Embed Size (px)
Citation preview
Prepared by Dr. Hoda Abed El
Azim
State common types of congenital anomalies in GIT.
Compare and contrast between cleft lip and palate (CL/CP).
Discus pre and postoperative care of CL/CP. Compare and contrast between the types of
hernias. Identify the clinical manifestation of
esophageal artesia (EA). Discus pre and postoperative care of
esophageal artesia (EA). Identify Anorectal malformations.
The most common anomalies are:
1. Cleft Lip or Cleft Palate2. Hernias3. Esophageal Atresia4. Anorectal malformations
CL and CP are facial malformations that occur during embryonic development and they are the most common congenital deformity of the head and neck.
They may appear separately or more often , together.
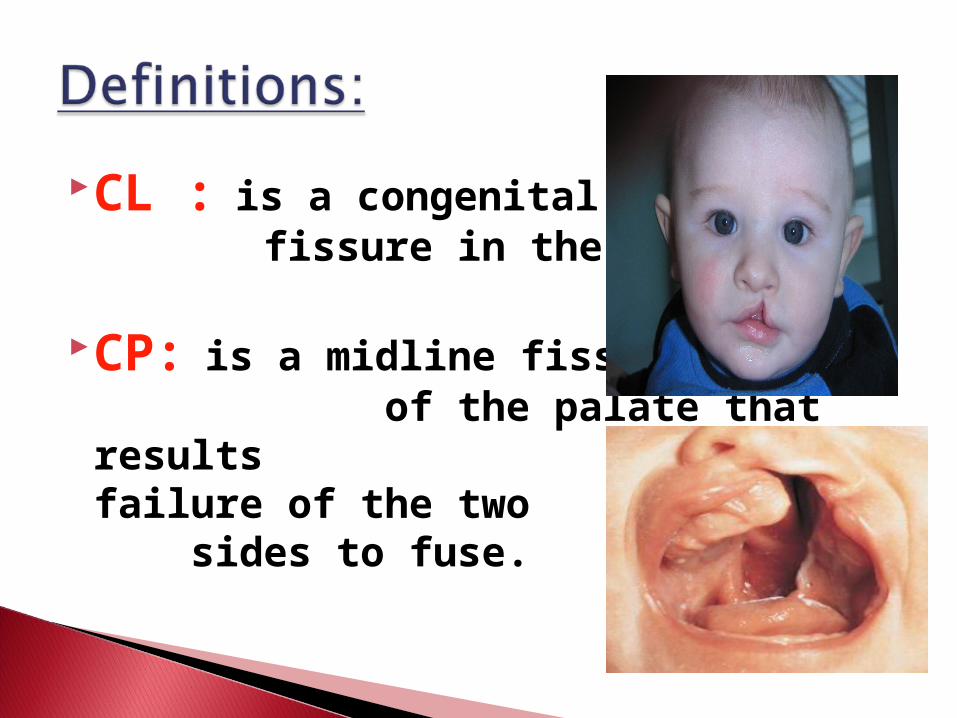
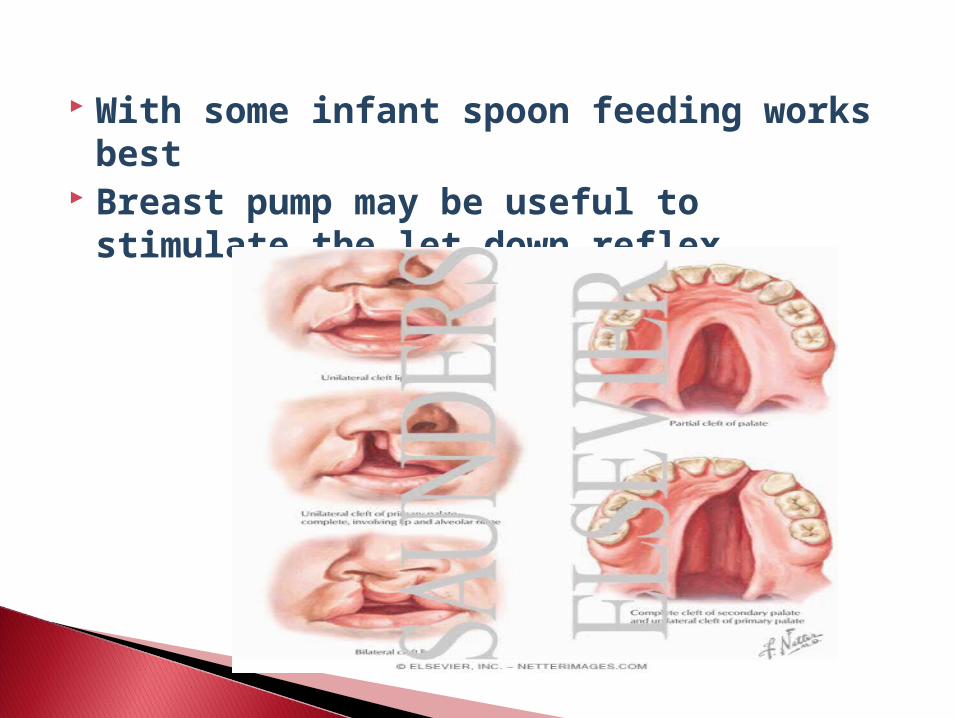
CL : is a congenital fissure in the upper lip.
CP: is a midline fissure of the palate that results from failure of the two sides to fuse.

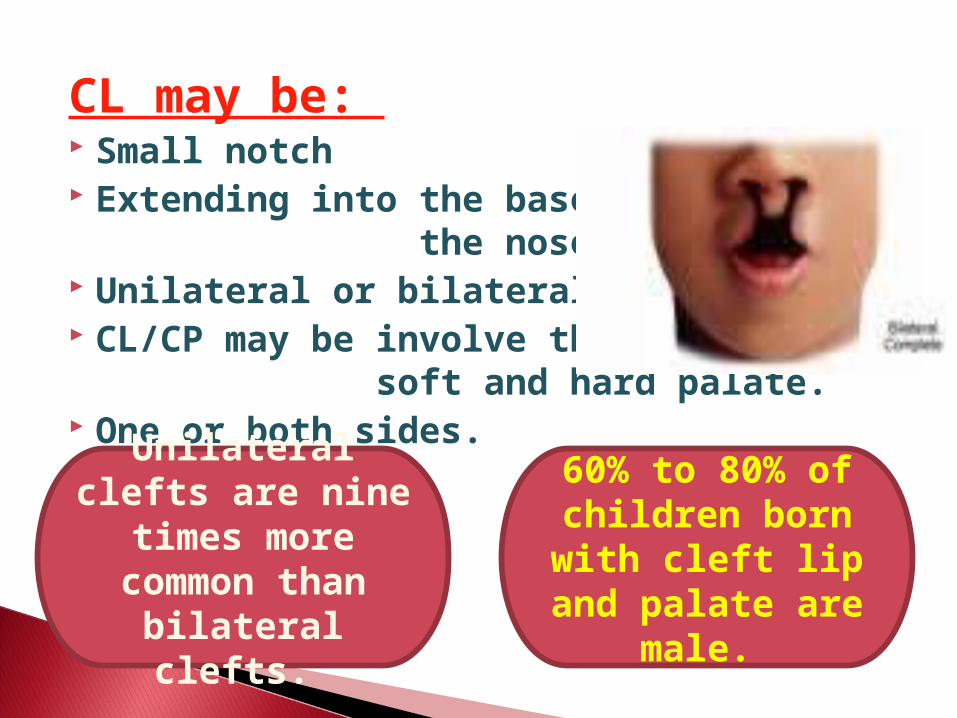
CL may be: Small notch Extending into the base of
the nose. Unilateral or bilateral. CL/CP may be involve the
soft and hard palate. One or both sides.
60% to 80% of children born with cleft lip
and palate are male.
Unilateral clefts are nine times more common than bilateral
clefts.
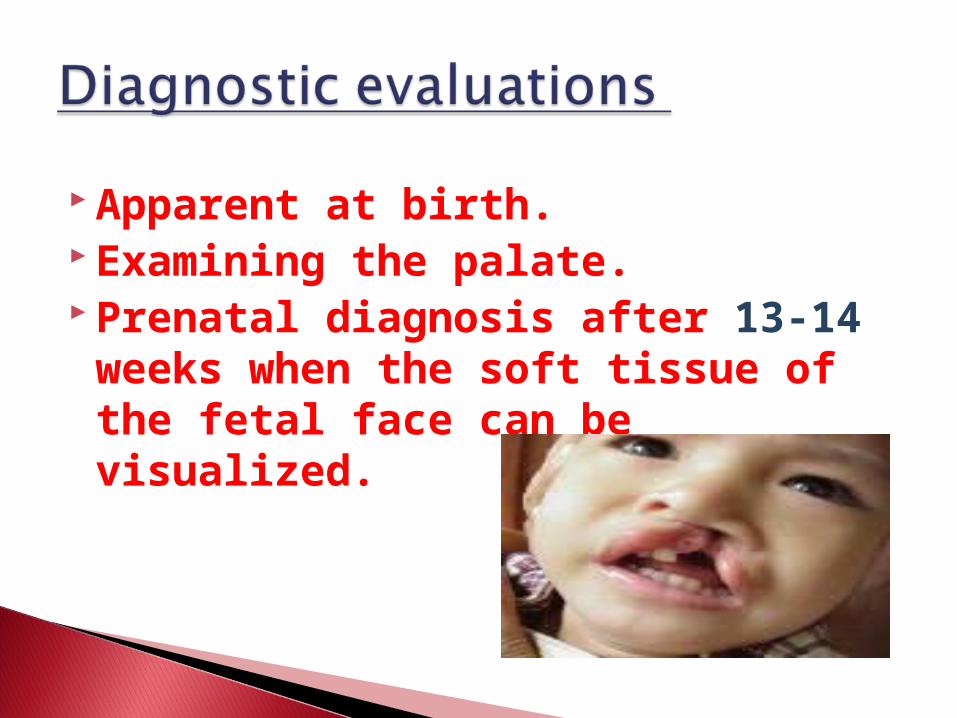
Apparent at birth. Examining the palate. Prenatal diagnosis after 13-14 weeks when the soft tissue of the fetal face can be visualized.
It interferes more with feeding and breathing, more
difficult to repair.
The management of CL involves the cooperative efforts of a multidisciplinary health care team.
Pediatrics Plastic surgery Speech/ language pathology Audiology Nursing and social work
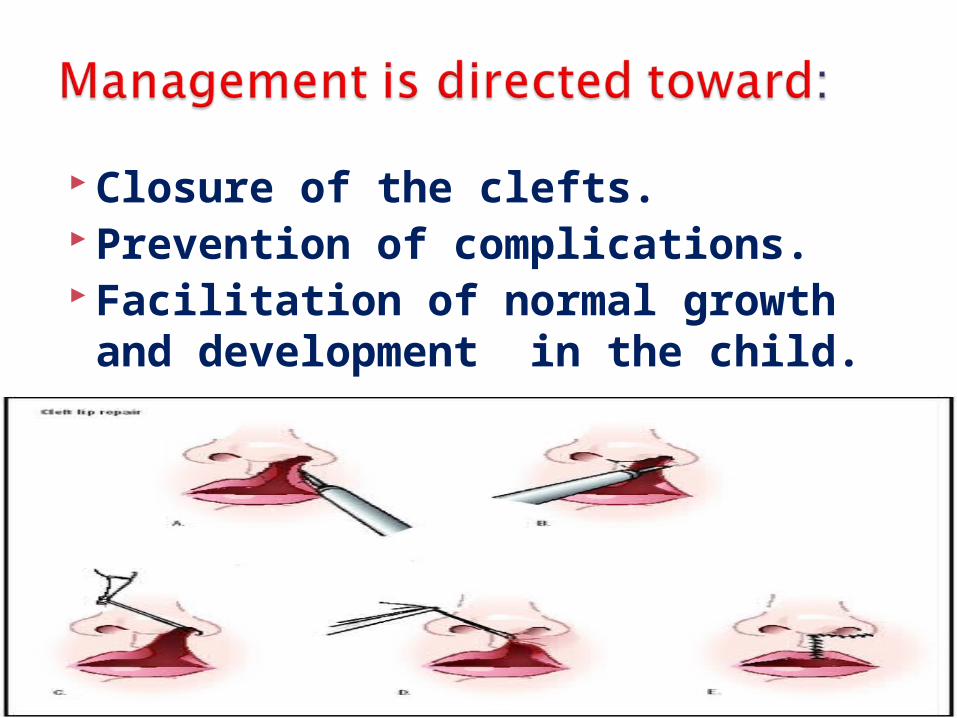
Closure of the clefts. Prevention of complications. Facilitation of normal growth and development in the child.
Even with good anatomic closure most children have:
Some degree of speech impairment . Inefficient functioning of the muscles
of the soft palate and nasopharynx. Improper tooth alignment. Varying degree of hear loss. Improper drainage of the middle ear. Recurrent Otitis media with scarring of
the tympanic membrane.
It is important for nurse to emphasis not only the infant’s physical needs but also on the parents emotional needs.
CL or CP reduces the infant’s ability to suck, interferes with compression of the areola.
Feeding is best with the infant’s head in upper right position.
Large , soft nipple with large holes have been advised and used.
Large syringe with soft rubber tubing can used.
With some infant spoon feeding works best
Breast pump may be useful to stimulate the let down reflex.
Elbow restrains are used to prevent the infant from rubbing or disturbing the suture line.
Older infants who roll over will require a jacket restraint to prevent rolling on the abdomen and rubbing the face on the sheet.
Adequate analgesia is required to relieve pain.
Clear liquids are offered when the infant has fully recovered from anesthesia.
The suture site are is carefully cleansed of formula.
A thin layer of antibiotic ointment. Genital aspiration of mouth and
nasopharyngeal secretions. An upright or infant set position.
Lie on the abdomen. Feeding by bottle, breast or cup. Oral packing, it is usually removed after 2
to3 days. Elbow restrains. Instruct the parents to keep the
restrained at home until palate is healed (2 to 6 weeks).
Opioids may be prescribed. Soft food in discharge plan until the
surgeon directs them otherwise.
Is a protrusion of a portion of an organ or organs through an abnormal opening.
through The diaphragm, The abdominal wall, or The inguinal canal.
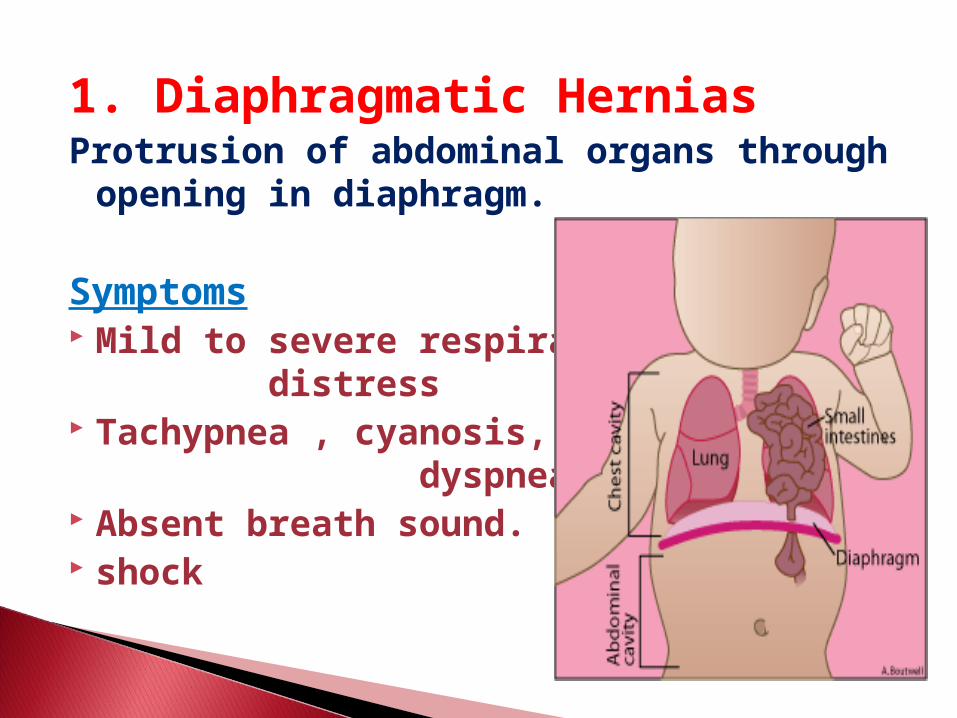
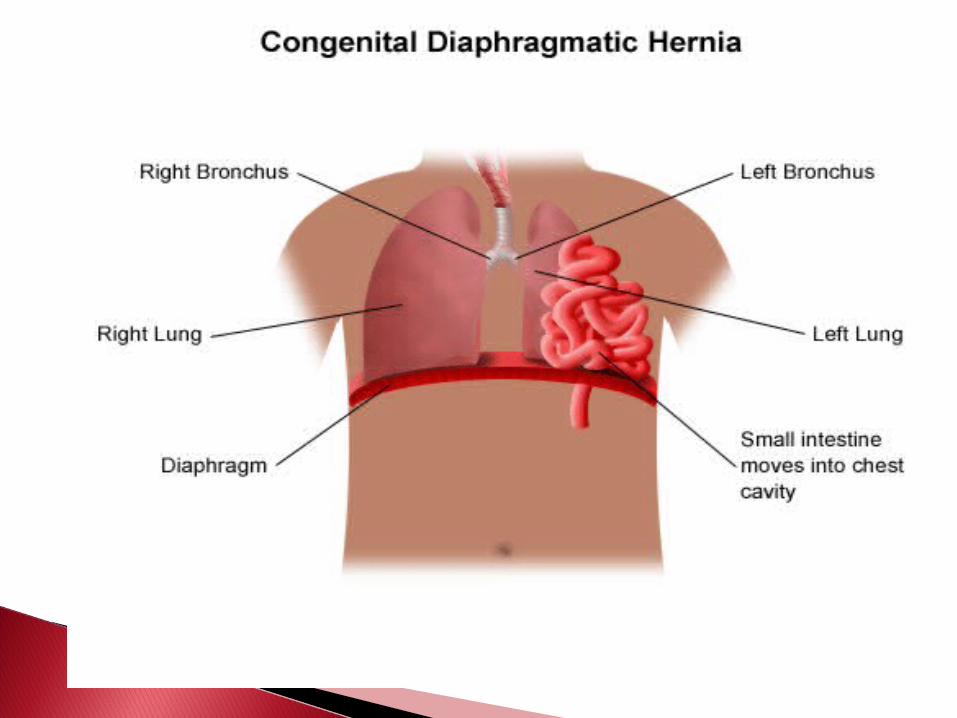
1. Diaphragmatic HerniasProtrusion of abdominal organs through
opening in diaphragm.
Symptoms Mild to severe respiratory
distress Tachypnea , cyanosis,
dyspnea Absent breath sound. shock
Diagnosis Symptoms Radiographic study. Prenatally as early as 25 week of gestation.
Therapeutic Supportive treatment of respiratory distress (Use of end tracheal intubation,
oxygenation). Prophylactic antibiotics. Surgical reduction of hernia and repair of
defect.
Preoperative Resuscitation, maintain suction, oxygen. IV fluids Positioning head up. Administer medication
Post operative Carry out routine postoperative care and
observation.
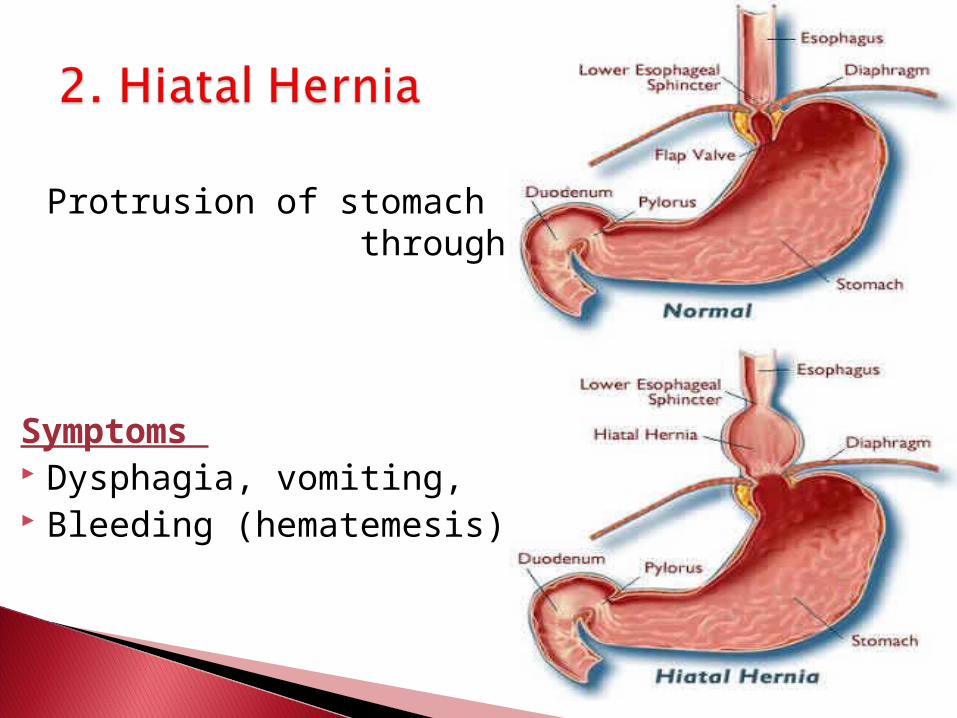
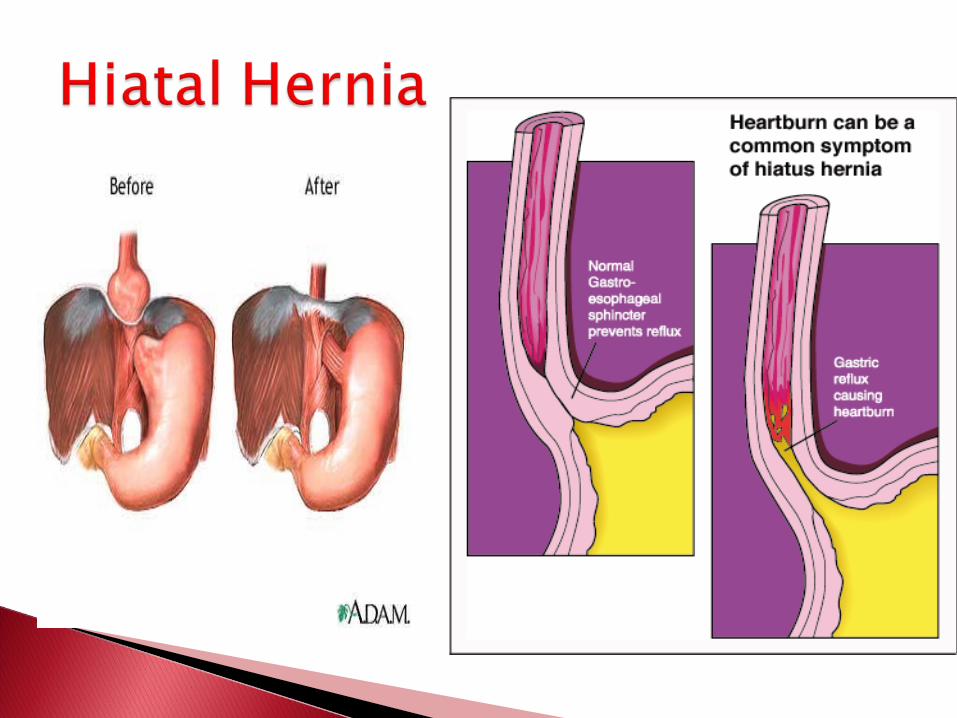
Protrusion of stomach through esophageal hiatus.
Symptoms Dysphagia, vomiting, Bleeding (hematemesis)
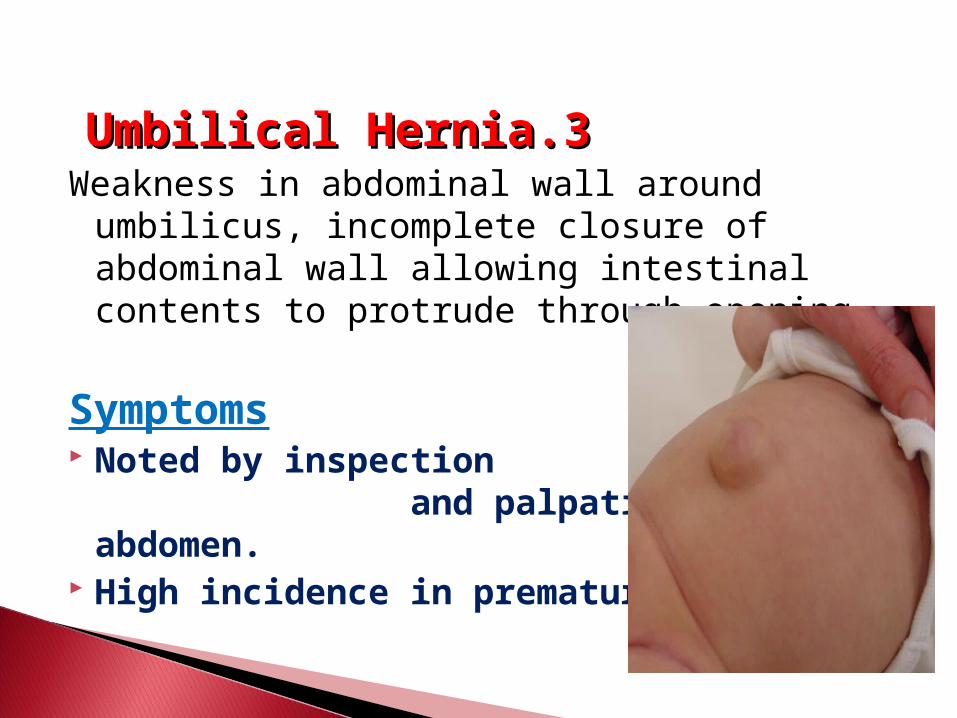
33..Umbilical HerniaUmbilical Hernia Weakness in abdominal wall around
umbilicus, incomplete closure of abdominal wall allowing intestinal contents to protrude through opening.
Symptoms Noted by inspection
and palpation of the abdomen. High incidence in premature.
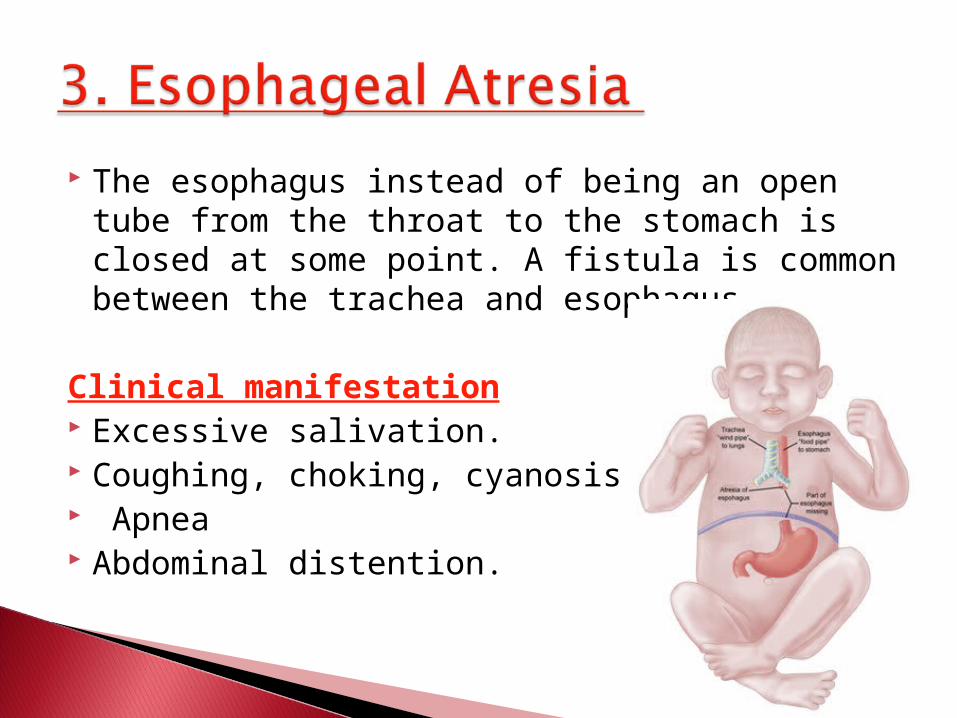
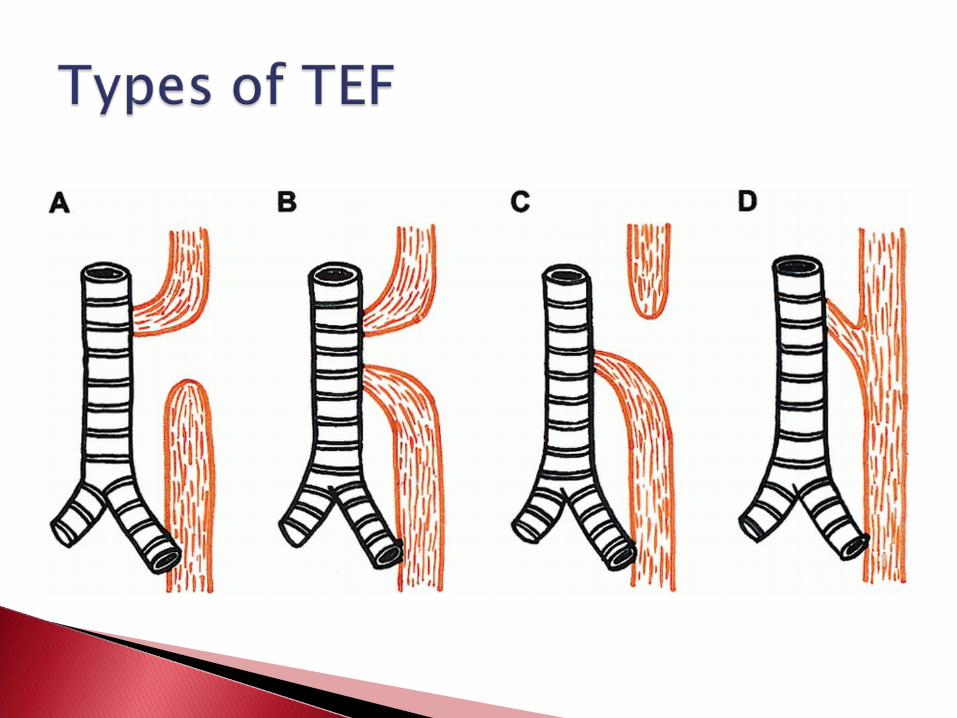
The esophagus instead of being an open tube from the throat to the stomach is closed at some point. A fistula is common between the trachea and esophagus.
Clinical manifestation Excessive salivation. Coughing, choking, cyanosis, Apnea Abdominal distention.
Any infant who has an excessive
amount of frothy saliva in the mouth
or difficulty with secretions and
unexplained episodes of cyanosis
should be suspected of having an
EA/TEF and referred immediately for
medical evaluation
Maintenance of a patent airway. Prevention of pneumonia. Surgical repair of the anomaly. Avoid oral intake, started IV fluids. Removal mouth secretion by suction. Broad spectrum antibiotic therapy. Gastrostomy AND ligation of the TEF.
`Nursing responsibility for detection of this malformation immediately after birth.
If feed the infant and swallows but suddenly coughs, and the fluid return through the nose or mouth, reported immediately.
The infant placed in incubator, oxygen is administer.
Intermittent or continuous suction of nose.
Oral fluid are withheld, the infant fluid met by IV fluid or gastrostomy.
The infant is returned to radiant heater or incubator.
The gastrostomy tube is connected to gravity drainage until the infant can tolerate feeding.
Tracheal suction with extreme caution to avoid injury to the suture line.
The initial attempt at oral feeding to make sure that the infant can swallow without choking.
Oral feedings are begun with sterile water, followed by frequent small feeding of formula.
Infants are usually not discharged until they are taking oral fluids well and the gastrostomy tube is removed.
The rectum and urinary tract separate completely by the seventh week of
gestation.
Abnormal development of genitourinary and
pelvic organs .
Is the most common congenital anomaly of GIT in newborn.
Diagnosis There is no anal opening. The nurse is unable to insert the
thermometer. No passage of meconium. Later on abdominal distention and pain
occur.
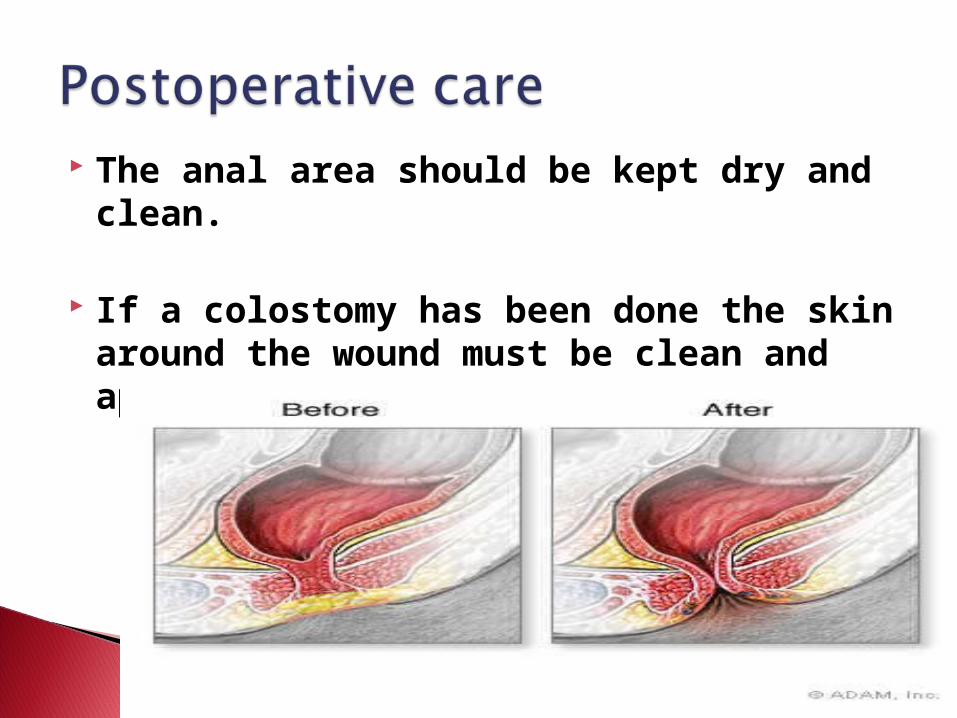
The anal area should be kept dry and clean.
If a colostomy has been done the skin around the wound must be clean and apply colostomy clean dressing.