Embed Size (px)
Citation preview

Preoperative Virtual Reality Preparation for children undergoing painful surgery
Bram DierckxJeroen LegersteeRobin EijlersChild and Adolescent Psychiatry/Psychology

ANXIETYPREOPERATIVE

Preoperative anxiety
Children: 50-70%
Peaks during induction of anesthesia
Negative consequences
Preoperative
Agitation
Less cooperation
Postoperative
Pain
Emergence delirium
Sleeping problems
Long term
Post traumatic stress
symptoms
PREPARATION

DISTRACTION

EXPOSURE

EXPOSURE

VR EXPOSURE

META-ANALYSISVR in Pediatrics

Records identified through database searchingApril 25, 2018 (n = 2889)
Records screened(n = 2,889)
Records excluded(n = 2,845)
Full text articles assessed for eligibility(n = 44)
Studies included (n = 17)
Records Excluded (n = 27)
No virtual reality (n = 11)Overlap with adults (n = 7)
Only adults (n = 3)No full text article (n = 3)
Pain or anxiety not an outcome (n = 2)No empirical study (n=1)
FLOWCHART

Dental care (n=2)
Burn care (n=6)
Oncological care (n=4)
Venous access (n=4)
Preoperative (n=1)
VR distraction
14 studies on pain7 studies on anxiety
VR exposure
1 study on anxiety
INCLUDED
STUDIES

RESULTS
PAIN
14 studies
698 patients
SMD = 1.3095% CI = 0.68–1.91, P < 0.001
SensitivityAnalysis 0,730 0,350 1,100 <0,001 OverallNo publication bias
Egger’s test p = 0,1

RESULTS
ANXIETY
7 studies
393 patients
SMD = 1.3295% CI = 0.21–2.44P = 0.02 SensitivityAnalysis 0,5 0,20 0,78 <0,001
Overall
No publication biasEgger’s test p = 0,3

VR is effective
In children and adolescents
For pain as well as anxiety
In a wide range of medical procedures
Limited focus on VR exposure (preparation) (n=1)
CONCLUSION

PREVIEW STUDY
Preop VR Exposure

PREVIEW
STUDY
AIMPsychological preparation (Exposure) of children undergoing day-care surgery: effects on anxiety and pain
DESIGN- Randomized Controlled Trial (RCT)- 200 children (4-12 yrs)- Elective day care surgery- Virtual Reality (VR) vs Care as Usual (CAU)- Single-blind
- Primary outcome: anxiety during induction- Secondary outcomes: pain, analgesia
VR promising for painful surgeryVirtual Reality exposure before elective day care
surgery to reduce anxiety and pain: an RCT
Eijlers, et al.
European Journal of Anaesthesiology, 2019

UNREALGAME ENGINE

THE MAKING
OFF
(Motion
Capture)
VR promising for painful surgery

VR promising for painful surgery
THE MAKING
OFF
(Motion
Capture)

THE MAKING
OFF
(Facial motion
capture)
VR promising for painful surgery

21


23

24

25

26

25
30
35
40
At admission In holding area During induction
VR
CAU
MyPasScore
RESULTS
Anxiety

RESULTS
Morphine use
55%
96%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
MORPHINE
VRCAU
adenoidectomy/tonsillectomy
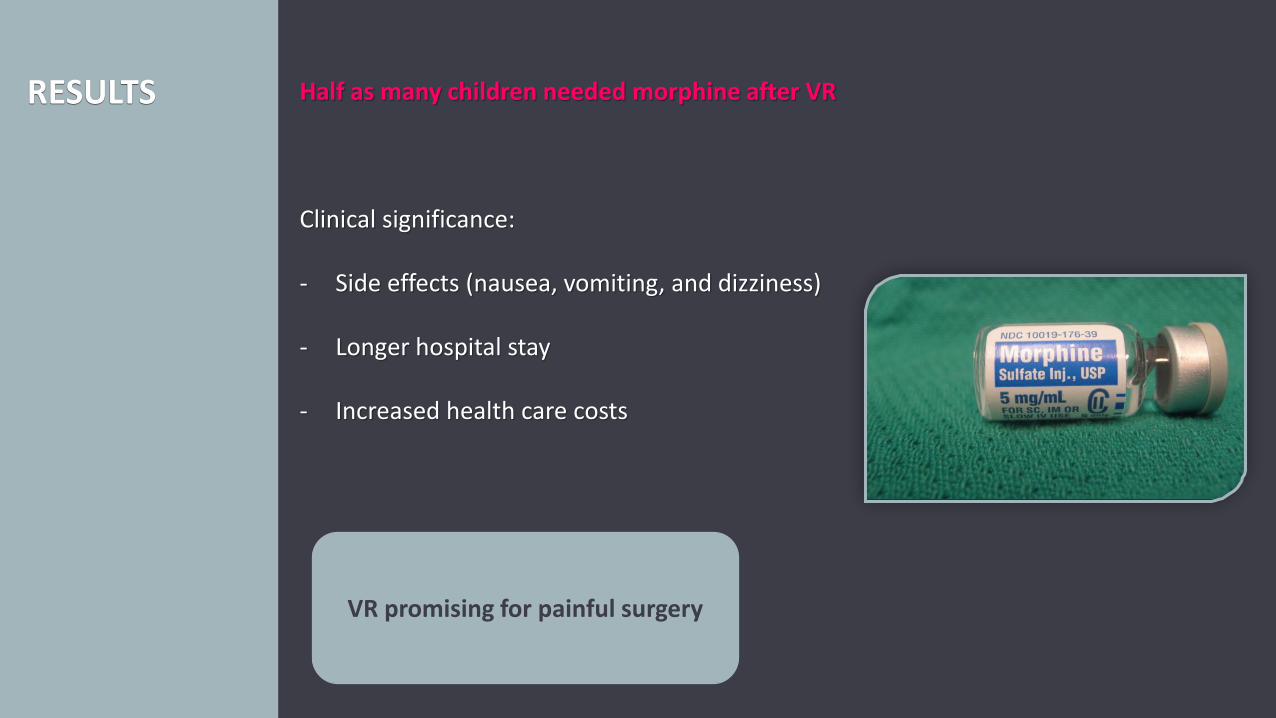
RESULTS Half as many children needed morphine after VR
Clinical significance:
- Side effects (nausea, vomiting, and dizziness)
- Longer hospital stay
- Increased health care costs
VR promising for painful surgery

RESULTS No differences in pain
- Only one postoperative assessment
- Not standardized in time
- Morphine had been administered before pain assessment
Pain measured more standardizedand more often

PREVIEW 2STUDY

SMARTPHONE VR APPLICATION
Advantages
- Easily accessible to all children
- At own pace and as often as needed
- Longer in advance, AT HOME
- No personnel needed
AIM 1

MORE PAINFUL SURGERY
SCOLIOSIS SURGERY
Advantages
- Even more benefit from VR
- Reduced pain
- Reduced need for morphine
- Shorter hospital stay
- Reduced health care costs
AIM 2

PAIN MEASURES
STANDARDIZED AND MORE OFTEN
Advantages
- More insight in effect of VR on pain
- Pain assessed before morphineadministration
AIM 3

36
AIM 4 EXPAND TO OTHER PROCEDURES


64 Patients(6-14 years)
64 Patients(6-14 years)
Sophia Children’s HospitalAmsterdam UMC
CAU
MRI
VR MRI
STUDY DESIGN
AnxietyImage QualityDuration of procedureNeed for anaesthesia

Erasmus MC, Rotterdam
Kinder-en Jeugdpsychiatrie
R. Eijlers
Prof. dr. E. Utens
Prof. dr. M. Hillegers
Anaesthesie
Dr. L. Staals
Kinderchirurgie
Prof. dr. R. Wijnen
ZNA, Anwerpen
Dr. J. Berghmans

THANK YOU FOR YOUR ATTENTION

41

EXTRA

43



Results: No effect on anxiety
46
VR (n = 94) CAU (n = 97) p-value
Child anxiety
mYPAS Induction observed 40.0 (28.3–58.3) 38.3 (28.3–53.3) 0.862
VAS Recovery room self-reported 0.0 (0.0–2.0) 0.0 (0.0–2.0) 0.735
Parental anxiety
VAS Induction observed 3.0 (2.0–5.0) 3.5 (2.0–5.0) 0.418
STAI (state) Induction self-reported 41.0 (34.5–
48.5)
40.5 (33.0–50.0) 0.753
Values are median (iqr)
mYPAS: modified Yale Preoperative Anxiety Scale
VAS: Visual Analogue Scale
STAI: State Trait Anxiety Inventory

Results: No effects on pain and emergence delirium
47
VR (n = 94) CAU (n = 97) p-value
Pain
FLACC Recovery room observed 0.0 (0.0–0.0) 0.0 (0.0–0.0) 0.669
FPS-r Recovery room self-reported 2.0 (0.0–4.0) 2.0 (0.0–2.5) 0.699
Emergence delirium
PAED Recovery room observed 7.0 (5.0–9.0) 6.0 (5.0–9.0) 0.266
Values are median (iqr)
FLACC: Face, Legs, Activity, Cry, and Consolability
FPS-r: Faces Pain Scale - revised
PAED: Pediatric Anesthesia Emergency Delirium

Anesthesia Protocol
First, anaesthetic preparation took place (i.e. placement of the electrocardiography electrodes, pulse oximeter, and blood pressure cuff).
Induction of anaesthesia was performed intravenously (IV) or by inhalation induction, if IV placement was not preferred or IV access was not successful.
For IV induction, a peripheral intravenous catheter was placed on the back of the hand, and propofol (2-4 mg kg-1 IV) and fentanyl (1-2 mcg kg-1 IV) were administered.
For inhalation induction, sevoflurane in a mixture of oxygen and air was administered by mask.
In these cases, IV placement took place after induction, after which fentanyl (1-2 mcg kg-1 IV) was administered.
Depending on the surgical procedure, a laryngeal mask (LMA) or an endotracheal tube (ETT) was placed.
In case of ETT placement, the child received a muscle relaxant beforehand.
Anaesthesia was maintained with sevoflurane (0.7-1.0 MAC) in O2/air.
During surgery, fentanyl (IV) was administered on discretion of the anaesthesiologist.
At the end of the procedure, first doses of IV paracetamol 20 mg kg-1 and diclofenac 1mg mg kg-1 were administered.
48

Scoliosis surgery (historical control study)
50 Patients(6-18 years)
Recovery
SmartphoneVRE
50 Patiens(6-18 years)
Sophia Children’s Hospital
CAU
Surgery
PREVIEW 2
STUDY DESIGN

Adenoidectomy/tonsillectomy (single-blind RCT)
50
CAU
Surgery Recovery
Sophia Children’s HospitalMaasstad Hospital
PREVIEW 2
STUDY DESIGN
100 Patients(6-18 years)