Embed Size (px)
Citation preview

PREOPERATIVE ASSESSMENTHossam M. Ajabnoor
Anesthesia & ICU Asistant ConsultantAnd Lecturer
School of Medicine, Taibah University

INTRODUCTION
Importance1. Reduce patient risk and morbidity associated
with surgery and coexisting diseases2. Promote efficiency and reduce costs3. Prepare the patient medically and
psychologically for surgery and anesthesia

ASA basic standards for preanesthetic care1. Determining the pt. medical status2. Developing an anesthetic care plan3. Reviewing with the pt. or a responsible adult
this plan

Who should perform the preoperative evaluation?
Ideally, the preoperative evaluation is performed by the person who will administer the anesthetic.

Goals:1. Inform the pt. of the risk → informed consent2. Educate the pt. regarding anesthesia Plan3. Answer pt. Q.s & reassure the pt. & family4. Prohibition of ingesting food5. Instruct the pt. about which medications to
take or to stop on the day of surgery

PREOPERATIVE EVALUATION
• It is important for the evaluation to be complete, accurate, and clear, not only to allow the information to be relayed to others who may care for the patient perioperatively, but also for medico legal purposes

COMPONANTS
• HISTORY• PHYSICAL EXAMINATION• LAB TESTS• CONSULTATIONS (if needed)• PLAN• DISCUSSION WITH PATIENT

HISTORY
1. State of health of pt. especially their • exercise tolerance• Present illness
2. Mental status3. Medication and substances use(e.g., cigarettes,
alcohol)4. Previous anesthesia and any complications5. Drug allergies and family Hx of MH6. review of medical records

SPECIFIC AREAS IN Hx
CNSStrokes - seizuresCVSAngina - old MI – HTN – rheumatic fever –
claudication – arrhythmiasPULMONARYSOB – cough/sputum – asthma – smoking – recent
UTI – pneumoniaGIGERD – alcohol – hepatitis

KIDNEYSDialysis – ch. Renal impairmentMUSCULOSKELETALArthritis – osteoporosis – weaknessENDOCRINEDM – thyroid/adrenal dysfunctionCOAGULATIONHistory of DVT/PE – bleeding tendencyPREGNANCY?DENTITION

PHYSICAL EXAMINATION
1. Vital signs2. CNS (LOC – evidence of S/M weakness)3. Airway4. CVS (heart sounds – BP – peripheral edema -
peripheral pulses – veins)5. Lungs (rales – wheezes – breathing pattern)

AIRWAY
• Cervical spine mobility• Short thick neck• Temporomandibular mobility• Large tongue• Prominent central incisors• Diseased or artificial teeth• Thyromental distance and tissue compliance• Ability to visualize the uvula (Mallampati
classification)

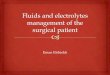
Mallampati classification
Mallampati found a correlation between higher oropharyngeal class and decreased glottic exposure at laryngoscopy. A higher oropharyngeal class combined with a mental space < 2 fingerbreadths may better predict increased difficulty with intubation
Performed by having patients in sitting position with their mouth widely open and protruding the tongue completely forward. (A tongue depressor is not used)

LARYNGOSCOPIC VIEW DIRECT VISUALIZATION, PATIENT SEATED
Entire glottic class I → soft palate, fauces, uvula, and pillars
Posterior commissure class II → soft palate, fauces, and a portion of the uvula
Tip of epiglottis class III → soft palate and base of the uvula
No glottal structures class IV → hard palate only


LAB TESTS
• No evidence supports the use of routine laboratory testing
• Use selected laboratory analysis based on the patient's preoperative history, physical examination, and proposed surgical procedure

Test IndicationsElectrocardiogram Cardiac and circulatory disease, respiratory
disease, advanced age†
Chest radiograph Chronic lung disease, history of congestive heart disease
Pulmonary function tests, including blood gas analysis and spirometry
Reactive airway disease, chronic lung disease, restrictive lung disease (e.g., scoliosis)
Hemoglobin/hematocrit Advanced age,† anemia, bleeding disorders, other hematologic disorders
Coagulation studies Bleeding disorders, liver dysfunction, anticoagulants
Serum chemistries (Na+, K+, Cl-, CO2, glucose) Endocrine disorders, medications, renal dysfunction
Pregnancy test Uncertain pregnancy history, history suggestive of current pregnancy

CONSULTATIONS
Preoperative consultations fall into two general categories:• Those cases that need more information or expertise to
establish or quantify a diagnosis that has implications for anesthetic management. An example is asking a cardiologist to evaluate a 50-year-old man with recent onset of exertional chest pain.
• Patients in whom the diagnosis is known, but further evaluation and treatment are needed to optimize their medical condition prior to surgery. Referring patients with poorly controlled diabetes, hypertension, or asthma to an internist are examples.

PLAN
Type of anesthesia• Awake• Sedation• Local• Regional• General anesthesiaTransfer postop• Home• Hospital room (day care / ward)• ICUPain control postop

Discussion With The Pt. Preop
1. Risks related to anesthesia• Nausea and vomiting• Myalgia• Dental injury• Peripheral neuropathy• Cardiac dysrhythmias• Atelectesis• Aspiration• Stroke• Allergic drug reactions• Death (very unlikely)

2. Preop insomnia and its treatment3. Time, route of administration & effects of
preop meds4. Time of transport to OR5. Duration of surgery

6. Awakening after surgery in PACU7. Probable presence of catheters on awakening8. Time to expected discharge from PACU9. Magnitude of postop discomfort and it
treatment

ASA PHYSICAL STATUS CLSSIFICATION
Created in 1940 purposes of statistical studies and hospital recordsIt is useful both for outcome comparisons and as a convenient means of
communicating the physical status of a patientUnfortunately, it is imprecise, and a patient often may be placed in different
classes by different anesthesiologiststhe higher ASA class only roughly predicts anesthetic risk• Class 1: Healthy patient, no medical problems • Class 2: Mild systemic disease • Class 3: Severe systemic disease, but not incapacitating • Class 4: Severe systemic disease that is a constant threat to life • Class 5: Moribund, not expected to live 24 hours irrespective of operation • An e is added to the status number to designate an emergency operation.
An organ donor is usually designated as Class 6.

How long should a patient fast before surgery?
• Healthy adults with no risk factors for aspiration include no solid food for a minimum of 6 hours, clear liquids up to 2 hours prior to an elective procedure, and oral preoperative medications up to 1-2 hours before anesthesia with sips of water.
• Pediatric patients are as follows:clear liquids up to 2 hours preoperativelybreast milk up to 4 hours preoperatively solid foods, including nonhuman milk and formula,
up to 6 hours preoperatively.

How long before surgery must A smoker patient quit smoking?
• Carbon monoxide (CO) from cigarette smoking diminishes oxygen delivery to tissues
• Nicotine increases heart rate and can cause peripheral vasoconstriction
• Within 12-24 hours of discontinuing cigarettes, CO and nicotine levels return to normal
• Bronchociliary function improves within 2-3 days of cessation• sputum volume decreases to normal levels within about 2
weeks• However, there may not be a significant decrease in
postoperative respiratory morbidity until after 6-8 weeks of abstinence.

List the major goals of premedication
• Sedation and anxiolysis • Analgesia and amnesia • Antisialagogue effect • To maintain hemodynamic stability, including
decrease in autonomic response • To prevent and/or minimize the impact of
aspiration • To decrease postoperative nausea and vomiting • Prophylaxis against allergic reaction

What factors should be considered in selecting premedication for a patient?
• Patient age and weight • Physical status • Levels of anxiety and pain • Previous history of drug use or abuse • History of postoperative nausea or vomiting or motion
sickness • Drug allergies • Elective or emergency surgery • Inpatient or outpatient status

List the most commonly used preop medications
• Diazepam Oral 5-20 Sedation • Midazolam IV 2.5-5 Sedation • Morphine IM 5-15 Analgesia • Meperidine IM 50-150 Analgesia • Ranitidine Oral, IV 150 mg and 50 mg, respectively Decrease
gastric pH • Metoclopramide Oral, IM, IV 5-20 Gastrokinetic• Glycopyrrolate IM, IV 0.1-0.3 Weak sedative, antisialagogue • Scopolamine IM, IV 0.3-0.6 Sedative, antisialagogue• Promethazine IM 25-50 Antiemetic • Ketamine IM, oral 1-2 mg/kg and 6 mg/kg, respectively
Sedation

A 3-year-old child presents for an elective tonsillectomy. His mother reports that for the past 3 days he has had a runny nose. Should you postpone surgery?

• Viral URI alters the quality and quantity of airway secretions and increases airway reflexes to mechanical, chemical, or irritant stimulation
• Some clinical studies have shown associated intraoperative and postoperative bronchospasm, laryngospasm, and hypoxia
• There is evidence that the risk of pulmonary complications may remain high for at least 2 weeks, and possibly 6-7 weeks, after a URI
• Infants have a greater risk than older children, and intubation probably confers additional risk

• However, as a practical matter, young children can average 5-8 URIs per year, mostly from fall through spring
• If a 4- to 7-week symptom-free interval were rigorously followed, an elective surgery might be postponed indefinitely
• Therefore, most anesthesiologists distinguish uncomplicated URI with chronic nasal discharge from nasal discharge associated with more severe URI with or without lower respiratory tract infection (LRI)
• Chronic nasal discharge is usually noninfectious in origin and caused by allergy or vasomotor rhinitis
• An uncomplicated URI is characterized by sore or scratchy throat, laryngitis, sneezing, rhinorrhea, congestion, malaise, nonproductive cough, and temperature > 38°C

• More severe URI or LRI may include severe nasopharyngitis, purulent sputum, high fever, deep cough, and associated auscultatory findings of wheezes or rales
• It is generally agreed that chronic nasal discharge poses no significant anesthesia risk
• In contrast, children with severe URI or LRI almost always have their elective surgery postponed
• Probably most anesthesiologists will proceed to surgery with a child with a resolving uncomplicated URI, unless the child has a history of asthma or other significant pulmonary disease

THANK YOU