Embed Size (px)
Citation preview

Problem Gamblers’ Harsh Gaze onCasino ServicesCatherine PrenticeSwinburne University
Arch G. WoodsideBoston College
ABSTRACT
This study provides a first look at the perspectives and profiles of casino problem gamblers. Thestudy proposes that problem gamblers (1) have unique antecedent conditions and (2) evaluate theircasino service more favorably than nonproblem gamblers. While first proposition receives support,the findings counter the second; surprisingly, problem gamblers view casino service with a harshgaze. The coverage here includes overall and specific findings from face-to-face interviews withgamblers (n = 348) inside seven casinos in the world’s largest gaming destination (Macau). Theinterviews included asking participants to complete the “Problem Gambling Severity Index”(identified to participants as “My gambling-related experiences”). The study includes both fit andpredictive validities of overall service quality models for each of the seven casinos—these findingssupport the nomological validity that specific patterns of antecedents and outcomes associate withproblem gambling. Policy and managerial implications inform how to go about creating uniquemarketing service designs to assist problem gamblers in managing their gambling behavior. C© 2013Wiley Periodicals, Inc.
LaRose (2001, p. 1) offers the following cogent sum-mary of early literature relevant to compulsive buyingand consumption behaviors: “Off-line, compulsive buy-ers account for between 1 and 8 percent of the popula-tion (Faber & O’Guinn, 1992), ninety percent of all con-sumers make impulse buys (Cobb & Hoyer, 1986), andtwo-fifths describe themselves as impulse buyers (Rook& Fisher, 1995).” The author emphasizes that thesebehaviors defy rational consumer choice processes, in-flating consumer prices and exacerbating abuse of con-sumer credit and personal bankruptcies and so haveimportant social effects.
Hirschman (1992) describes the connection acrossa broad range of consumption behaviors that havea common compulsive quality. These behaviors gobeyond the bounds of normalcy and also exceeda consumer’s ability to control them through rea-son and willpower. Hirschman concludes that thesebehaviors, unless restrained by the consumer orsome external intervention, lead to negative con-sequences, perhaps even death. Thus, some addic-tive behaviors are analogous to extreme compulsivebehaviors.
The present study provides a first report from in-side a retailing context (i.e., casinos) associated fre-quently in the literature with compulsive behavior (e.g.,
Afifi, Cox, Martens, Sareen, & Enns, 2010; Nower &Blaszczynski, 2010). The objectives of the study in-clude expanding knowledge of problem gambling andexamining antecedent and outcome conditions associ-ating with problem gambling through direct observa-tions of casino gamblers. The study is valuable uniquelyin gaining access to seven mega casino resorts in theworld’s largest gaming market and in including exten-sive meta-analyses of antecedent and outcome condi-tions and cross-validations of the predictive abilitiesof overall service quality models across the seven casi-nos. The study also aids in confirming and clarifyingthe identity of problem gamblers and provides clues forstrategies effective in managing issues involving prob-lem gambling.
Following this introduction is a brief review of therelevant literature on compulsive buying and problemgambling. Next, a model and hypotheses of antecedentsand consequences relating to problem gambling are pre-sented. What follows is a description of the method forour study, a report of the findings, and a general dis-cussion that includes conclusions, implications for con-trolling problem gambling relating to casino table gam-bling, and revisions to theory. In the final section, thestudy’s limitations and implications for future researchare presented.
Psychology and Marketing, Vol. 30(12): 1108–1123 (December 2013)View this article online at wileyonlinelibrary.com/journal/mar
C© 2013 Wiley Periodicals, Inc. DOI: 10.1002/mar.20670
1108

1. Compulsive in most contexts
2. Normal(Tense) 3. Normal
(Very Tense)
ControlLow Moderate High
Motive
High
Moderate
Low
4. Compulsivein some contexts 5. Normal
6. Normal(Control overrides motive intensity)
7. Normal inmost
contexts8. Normal(Relaxed)
9. Weak Consumer
(Miser)
a
cb
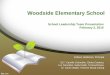
Figure 1. Categories of buyer behavior.Source: Adapted from Nataraajan and Goff (1991, p. 315).Note: The Venn diagram sitting on top of cell 1 is to indicate different compulsive behaviors (e.g., a = alcoholism, b = smoking, andc = gambling addictions) may overlap for some individuals; different sizes of overlapping circles indicate that time commitmentsvary for different compulsive behaviors. Sizes of rectangles in the figure vary by sizes to indicate varying shares of individuals ina population.
LITERATURE REVIEW
Compulsive Buying and Problem Gambling
Prior research on problem gambling focuses on the fol-lowing topics: (1) definition and characteristics of prob-lem gambling, (2) antecedent conditions and configura-tions of antecedent conditions associate with problemgambling, (3) the consequences, the outcomes, of prob-lem gambling, and (4) strategies effective in preventingand controlling/decreasing problem gambling.
What is Problem Gambling?
Compulsive buying receives substantial discussion inthe psychiatric nomenclature for almost 100 years (seeBlack, Shaw, & Blum, 2010). Kraepelin (1915) describesthe uncontrolled shopping and spending behavior asoniomania (“buying mania”) or buying maniacs (onio-maniacs) in whom even buying is compulsive and leadsto senseless contraction of debts with continuous delayof payment until a catastrophe clears the situation alittle—a little bit never altogether because they neveradmit all their debts. Kraepelin (1915) concludes thatthe particular element is impulsiveness; they cannothelp it, which sometimes even expresses itself in thefact that notwithstanding good school intelligence, the
patients are absolutely incapable of thinking differentlyand conceiving the senseless consequences of their actand the possibilities of not doing it (cf. Bleuler, 1930, p.540).
Nataraajan and Goff (1991) propose that impulsive,compulsive, and addictive buying lie along a contin-uum of purchase behavior characterized by deficientself-regulation—a continuum that includes normal im-pulsive consumer behavior at one extreme and deviantaddictive behavior at the other. The literature does notinclude agreement about the etiology of unregulatedbuying but learning theory models are common to manyexplanations of the course these disorders take as theyprogress from impulsive to repetitive and harmful com-pulsive behavior (LaRose, 2001).
Nataraajan and Goff (1991) identify two indepen-dent factors in compulsive buying as follows: buyingurge or desire and degree of control over buying; theyemphasize that in theory individuals are identifiable oncontinuums for each factor. In their model, compulsiveshoppers combine high urge with low control. This viewis consistent with clinical reports that compulsive buy-ers are preoccupied with shopping and spending; theywill try to resist their urges, though often with littlesuccess (Black, Shaw, & Blum, 2010).
Figure 1 is an adaptation of Nataraajan and Goff’s(1991) theory to incorporate empirical findings that be-tween 2% and 8% of general populations in the United
PROBLEM GAMBLERS’ HARSH GAZE 1109Psychology and Marketing DOI: 10.1002/mar

States engage in compulsive buying (Koran et al., 2006)and estimates of problem gambling includes 1–4% ofgeneral populations in the United States and Canada(Shaffer & Hall, 2001). Figure 1 here incorporatesFitzsimons’s (2008) “death to dichotomizing” perspec-tive by including nine cells, each of them varying insize to indicate shares of their respective populations;McClelland’s (1998) study by quintiles data analysisalso emphasizes that substantial differences among astudy’s participants only become apparent for the top20% of a sample. As Nataraajan and Goff suggest,“ . . . the majority of buyers will fall in categories [otherthan category 1] since the proportion of ‘normal’ buyersis expected to far exceed compulsiveness in any society”(1991, p. 314).
The overlapping circles on top of the first rectangu-lar cell in Figure 1 visualize the hypothesis and find-ings that some compulsive buying behaviors comple-ment one another for some consumers (Black, Shaw,& Blum, 2010). The different sizes of the a, b, and ccircles indicate daily-to-monthly time commitments tospecific compulsive buying behaviors are likely to vary.For example, daily smoking and alcohol addictions maybe prevalent for some problem gamblers who travel toa controlled casino area of a country (e.g., Macau inChina) for one full day of table gambling every week.
The present study adopts Nataraajan and Goff’s(1991) continuum proposal and provides substantial ev-idence supporting core propositions as follows: (1) pro-files of antecedent conditions are distinct for consumersexhibiting problem or addictive consumption behaviorand (2) consumer evaluations of their current in situservice providers vary consistently according to the con-sumers’ location on this consumption continuum.
Accepting the perspective that compulsive buyingcondition extends beyond retail shopping for products,problem gambling is regarded as a subcategory of com-pulsive buying. Afifi et al. (2010) observe that the Cana-dian population includes 2% who are problem gamblers,according to the Canadian Problem Gambling Index(CPGI; Marshall & Wynne, 2003, 2004). These statis-tics are similar to those reported in the United Stateswhere 78% of a nationally representative sample re-ported lifetime gambling activity and 3% are problemor pathological gamblers according to “Diagnostic andStatistical Manual of Mental Disorders, fourth edition”(DSM-IV) criteria (Kessler et al., 2008).
Similar to Afifi et al.’s (2010) study, instead meetingDSM-IV criteria for a disorder (i.e., pathological gam-bling), this research is focused on problem gambling asgambling behavior that has a negative impact on thegambler, the relevant others, or the community as de-scribed in the CPGI (Ferris & Wynne, 2001). Nataraa-jan and Goff (1991, p. 317) provide a similar perspec-tive, “The primary criterion to determine whether or notbuying behavior is innocuous or potentially compulsive(abnormal) buying is whether or not such behavior iscausing disruption in the normal life of the individual.”
While beyond the scope of the present study, “nega-tive impact” and “causing disruption” are viewable as
consequences of problem gambling rather than problemgambling per se. From the perspective of low control andhigh-intensity motive (see Figure 1), causing disruptionin an individual’s normal life is not a sufficient or nec-essary condition for problem gambling, which can beseemingly an innocuous activity for long time periods.This study adopts the view that examining configura-tions of formative, definitional, and reflective indica-tors are useful for theory building and measurementof problem gambling without measuring definitionalindicators.
Consistent with Nataraajan and Goff’s (1991) sug-gestion for compulsive buying, formative indicators ofproblem gambling include configurations of antecedentconditions that associate positively with problem gam-bling when viewing problem gambling as a continuumconstruct. The configuration of senior male with casinoreward membership is an example of a configuration ofantecedent conditions associating positively with prob-lem gambling.
Antecedent Conditions Associating withProblem Gambling
Meta-analyses of antecedent conditions associatingwith problem gambling are available in the literature.For example, Felicity, Lorains, Cowlishaw, and Thomas(2011) examine 11 eligible studies reporting on comor-bidity from the literature. Their findings from acrossthe studies indicate that problem and pathological gam-blers had high rates of other comorbid disorders. Thehighest mean prevalence was for nicotine dependence(60.1%), followed by a substance use disorder (57.5%),any type of mood disorder (37.9%) and any type of anxi-ety disorder (37.4%). However, moderate heterogeneityoccurs across studies, suggesting that rate estimatesdo not necessarily converge around a single populationfigure, and that weighted means should be interpretedwith caution, which suggest segmenting problem gam-blers by shares of comorbidity configurations.
In reviewing the literature on problem gambling,Black, Shaw, and Blum (2010) note that the rates ofproblem gambling are higher in senior males, adultswith mental health or substance-use disorders, personswho have been incarcerated, or those with low socioe-conomic status. Residency distance to casinos can bea factor of problem gambling too (NORC, 1991). Atfirst blush, household income may be thought to as-sociate positively with problem gambling since moneyavailability may be a prerequisite to gambling. How-ever, high gambling frequency occurs for similar sharesof households in the general population in the UnitedStates among the lowest and highest income categories(Woodside & Zhang, 2012).
Problem gambling is widely thought to be chronicand progressive (Cartwright, DeCaria, & Hollander,1998). Thus, the prevalence of problem gamblingis likely to occur among casino members. Cus-tomers in loyalty programs often receive special or
1110 PRENTICE AND WOODSIDEPsychology and Marketing DOI: 10.1002/mar

Age
Gender
Education
Income
Occupation
Casino rewardcard holder/user
Length-of-playeach visit, hours
Average bet size
Number of annualvisits
Problem Gambling
+
+F = 0, M = 1
_
0
-
+
+
+
+
Casino up-to-date, appealing facilities
Quality of serviceresponsiveness
This casino is my 1st choice
to visit
Casino has my best interests at heart &employees care
Quality of games
Food & beverageQuality
Overall servicequality
+ WOM for this casino
Ambience
Customer propensity to switch
+
+
+
+
+
+
+
+
+
_
+
+
+
+
+
+
Antecedents Immediate Outcomes
GlobalOutcomes
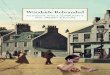
Figure 2. Theory of antecedents and casino outcomes of problem gambling.
complimentary gambling-related benefits designed forthem. Similar to airline frequent flyer programs, mem-bers receive free flights depending on the frequencyof use and expenditure levels of using these services.Some casino service and marketing promotions may beeffective in nurturing the development of problem gam-bling (e.g., 24-hour operation, casino membership pro-grams, complimentary accommodations including freefood and beverage service).
Outcome Conditions Associating withProblem Gambling
Research on consequences of problem gambling is ex-tensive. LaPlante, Nelson, LaBrie, and Shaffer (2009)indicate that depression and mood disorders followedby “spontaneous recovery” (i.e., without the use of pro-grammed intervention programs) are a common out-come of problem gambling). In their literature review,Black, Shaw, and Blum (2010, p. 177) conclude, “ . . . theperson with CB [compulsive buying] or PG [pathologicalgambling] finds the behaviors highly pleasurable, andonly wants to stop the behaviors when their deleterioussecondary consequences become overwhelming.” Thus,immediate, in-context, and high pleasure is thoughtto be a psychological outcome of problem gambling. If
present at all, such gambling-induced euphoria mayoccur only while the problem gambler engages in gam-bling. Concludes that the social and health costs ofproblem gambling are large at both individual and so-cietal levels. Personal costs can include irritability, ex-treme moodiness, problems with personal relationships(including divorce), absenteeism from work, neglect offamily, and bankruptcy; adverse health consequencesfor the gambler and his or her partner include de-pression, insomnia, intestinal disorders, migraine, andother stress-related disorders (Lorenz & Yaffee (1986).These are long-term consequences that the problemgambler may not associate directly with problem gam-bling per se.
Although numerous studies discuss consequences ofproblem gambling, none addresses the following out-comes. How do problem gamblers evaluate service ex-periences of the casinos? Do these evaluations differsubstantially from those of nonproblem gamblers? Thecurrent study attends to these issues and bridges theresearch void.
HYPOTHESES OF THE STUDY
Figure 2 presents the study’s model, and shows themain effect associations of the hypotheses. The model
PROBLEM GAMBLERS’ HARSH GAZE 1111Psychology and Marketing DOI: 10.1002/mar

Casino table gambling
Evaluations ofcasino service
experiences
Problem gambler
2 +
1 + 3 +
a. Original hypotheses b. Revised hypotheses
Casino gamblingOutcome (losses)
Problem gambler
Evaluations of casinoservice experiences
Casino tablegambling
2 -
3 +4 -
1 +
5 -
6 -
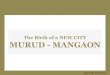
Figure 3. Heider’s balance theory applied to casino service evaluations by problem gamblers.
includes nine antecedent conditions. Based on the in-sights from reviewing the relevant literature, the modelincludes the following specific hypotheses.
Hypotheses for Antecedent Conditions
H1: Age associates positively with problem gam-bling.
H2: Male versus female gender associates posi-tively with problem gambling.
H3: Education associates negatively with prob-lem gambling.
H4: Income does not associate with problemgambling.
H5: Occupational status associates negativelywith problem gambling.
H6: Membership program associates positivelywith problem gambling.
H7: Length of play associates positively withproblem gambling.
H8: Average bet amount associates positivelywith problem gambling.
H9: Annual visitation associates positively withproblem gambling.
Hypotheses for Outcome Conditions
Given that the relevant literature proposes the prob-lem gambling provides high pleasure for problem gam-blers, casino customers with high problem gamblingscores should view their immediate casino service ex-
periences more favorably. Balance theory is helpful forexplaining why problem gamblers are likely to haveunique favorable evaluations of their immediate ser-vice experiences (see Figure 3a; the discussion of Fig-ure 3b is in the General Discussion section). Heider(1958, p. 201) explains, “By a balanced state is meanta situation in which the relations among the enti-ties fit together harmoniously; there is no stress to-ward change. A basic assumption is that sentimentrelations and unit relations tend toward a balancedstate.”
Given that it is uniquely highly pleasurable forthe problem gambler, the sentiment connection (bolddouble-headed arrow 1 in Figure 3a) with the ser-vice provider (2 in Figure 3a) will be most favorable—participating in an activity judged to be high plea-surable results in highly favorable evaluations of ser-vice experiences. The favorable connection between theservice experiences and the problem gambler (3 inFigure 3a) results in psychological balance—possiblya euphoric condition.
The model includes 10 outcome conditions that ap-pear in Figure 2 in two sets labeled immediate andglobal outcomes. These outcomes refer to evaluations ofa casino by customers with no, low, moderate, and highlevel of problem gambling indicator scores as the follow-ing method section describes. The model includes sixdimensions that influence four global outcomes: casinopreference, overall service quality, positive word-of-mouth communication about the casino, and propen-sity to switch to another casino. The model predictsthat casino service evaluations have direct influenceswhile problem gambling has an indirect influence onthe global outcome conditions—thus, the dotted lines inFigure 2 from problem gambling to the global outcomesindicate hypothesized main effects that are not signif-icant contributors to the immediate outcomes. Giventhat multiple combinations of immediate outcome con-ditions are nearly equal in explaining the global
1112 PRENTICE AND WOODSIDEPsychology and Marketing DOI: 10.1002/mar

outcome conditions, the study focuses on the main ef-fects in the model and proposes the following:
H10: High versus low or no problem gambling as-sociates with (1) more positive evaluationsof a casino’s physical facilities. High ver-sus low or no problem gambling associateswith more positive evaluations as follows:(H11) of a casino’s service responsiveness;(H12) a casino’s being the customer’s firstchoice; (H13) casino employees caring for thecustomer’s well-being; (H14) the customer’sperceptions about the quality of the gamesin the casino; (H15) of food and beveragequality evaluations; (H16) customers’ judg-ments of the overall service quality of thecasino; (H17) of word-of-mouth communi-cations about the casino; (H18) the ambi-ence of the casino; (H19) negatively withcustomers’ propensity to switch to anothercasino—switching behavior takes time andmoves the customer away from a highly plea-surable experience.
H20: The immediate outcomes of customer serviceevaluations have a direct major influenceon the global outcomes of most preferredcasino, overall service quality, positive Wordof Mouth (WOM), and propensity to switchcasinos. H21: While problem gambling doeshave a small direct influence on global out-comes, its influence is larger consistentlyon the immediate outcomes. H22: Overallservice quality is a lynchpin influence onthe other global outcomes of (1) propen-sity to switch, (2) positive word-of-mouthcommunications, and (3) first preference forthe present casino the customer is visiting.These final hypotheses relate to the nomo-logical validity (Peter, 1981) of the modeland are supported by prior work on modelingcustomer evaluations of specific service acts,overall satisfaction, and intentions about fu-ture visits to the service provider (Chang,Tseng, & Woodside, 2013; Woodside, Frey,& Daly, 1989).
METHOD
The section describes the measurement constructs,sampling plan, and procedure for data collection. Theresearchers opt for conducting the survey at casinosin Macau since this special administrative territory ofChina has become the world’s leading gaming desti-nation with an estimated US $44 billion in revenues
in 2013 (O’Keeffe, 2013). A face-to-face intercept witha self-report survey was conducted at Macau’s sevenlarge casino resorts.
Measures
Problem Gambling. According to research on theProblem Gambling Severity Index (PGSI, aka Cana-dian Problem Gambling Index), problem gambling isdefined as scoring three or more based on the endorse-ment of the gambling behaviors or concerns (Ferris &Wynne, 2001). The PGSI is a well-developed tool thatwas created specifically for assessing problem gamblingin general population samples and has been subjectto extensive psychometric testing (Ferris and Wynne,2001).
The PGSI has “good reliability” (α = 0.84) where“good” is above an α of 0.80 (Kline, 1999) and high cor-relation (r = 0.78) with test–retest reliability (Ferris& Wynne, 2001). The criterion-related validity deter-mined that the PGSI was highly correlated with DSM-IV criteria (r = 0.81) and with South Oaks GamblingScreen (SOGS; r = 0.80) indicating that the CPGI clas-sification of respondents is consistent with classifica-tion using other scales (Ferris & Wynne, 2001).
The PGSI uses the following self-report items to as-sess level of gambling problems: (1) wagered largeramounts to get the same feeling of excitement; (2) triedto win back losses; (3) borrowed money or sold some-thing to get money for gambling; (4) felt a gamblingproblem existed; (5) gambling caused health problemsincluding stress and anxiety; (6) been criticized for bet-ting or told a gambling problem exists; (7) gamblingcaused financial problems; (8) felt guilty about gam-bling; and (9) bet more than could be lost. Four choicesare available for answering each of the nine items 0 =never; 1 = sometimes; 2 = most of the time; 3 = almostalways.
In the present study the items were used to com-pute PGSI scores that measure problem gambling infive categories as follows: nonproblem gambler (scoreof zero), low risk gambler (score of 1–2), moderate riskgambler (score of 3–4), high risk (5–6), and severe riskgambler (score of 7 or more). Moderate and severe riskgamblers were combined into one group (referred to asproblem gamblers). Because scores of three to sevenreflect significant risk that may already have adverseconsequences related to gambling for the gambler (Fer-ris & Wynne, 2001).
Holtgraves (2009) examines the reliability and valid-ity of the PGSI across a national and six regional sam-ples of general populations of Canadians (integrated,n = 12,299). He reports a coefficient α equal to 0.86 forthe total sample and an α equal to 0.73 among the highscorers (i.e., >7) on the scale. Coefficient α for the PGSIis 0.92 for the total respondents to the present studyand 0.66 for the high scores (.i.e., 7+). The correcteditem to total correlations for the nine items in the scalefor the two studies indicates that the scale reliability
PROBLEM GAMBLERS’ HARSH GAZE 1113Psychology and Marketing DOI: 10.1002/mar

properties are adequate for the purposes of the currentstudy (correlations available upon request made to ei-ther author).
Findings for the nomological validity (Peter, 1981)indicate high validity of the scale in the patterns ofrelationships for the PGSI among the antecedent andoutcome conditions. For example, the share of high-PGSI scorers among once a year casino visitors shouldnot be the same as very frequent casino annual visitors.The findings indicate that high PGSI scores among oncea year casinos visitors is relatively rare in the sample(3/130), while the majority of customers visiting casinos7+ times have severe PGSI scores (8/14). For the rela-tionship of number of annual casino visits and PGSI,the ϕ2 = 0.368, p < 0.000, with ϕ2 > 0.25 indicates alarge effect size (see Cohen, 1977).
Antecedent Conditions. Depending on the question,two to eight responses were available to tick (
√)
for most of the antecedent conditions appearing inFigure 2. For example, the four-sided two-page surveyincluded two responses for gender, eight responses foreight household income ranges, seven ranges for typ-ical/average size of bet, and six age ranges (18–25 to61+). Open-ended responses were available to recordnumber of trips to visits casinos annually and numberof hours in the gaming area during each day of the visit.
Immediate and Global Outcomes. The outcomes fo-cus on customer evaluations of casino services, word-of-mouth communications, casino preference, and propen-sity to return. Four facets—game service product (orsimply game service), service environment, service de-livery, and food service—underline the casino servicequality conceptualization. Our conceptualization in-cludes measures of food and beverage service, but ex-cludes other nongaming aspects (e.g., shopping, musi-cal and special shows) to align with the aforementionedliterature, food and beverages have become an insep-arable component of the casino gambling experience(Prentice, 2013). Furthermore, our conceptualizationof casino service quality focuses on the performanceaspects of quality evaluation (i.e., service perceptions)rather than the gap score approach, since considerableevidence suggests that performance only measures aresuperior (Cronin & Taylor, 1992, 1994; Parasuramanet al., 1994).
The survey included six dimensions of service evalu-ations as appearing in Table 1 with two to seven itemsused to measure each dimension. Tests for the psycho-metric properties included both exploratory and con-firmatory factor analysis, and corrected item to totalreliability estimates. The exploratory and confirmatoryfactor analyses indicated unique factor structures forthe dimensions in Table 1. Details on the reliabilityestimations appear in Table 1.
The six immediate outcomes include customer eval-uations of service experiences relating uniquely to casi-nos. These six include the four dimensions and items
in Wong and Fong’s (2012) casino service quality scale(CASERV): casino patrons’ perceptions of service deliv-ery (e.g., “Staff give prompt service to customers”), ser-vice environment, food service (e.g., “The quality of foodand beverage is excellent”), and service product (e.g.,“The casino has sufficient number of table games avail-able”). The present study includes a separate uniquedimension relating to personal attention consisting oftwo items, “Casino has my best interests at heart” and“Employees care” as well an additional dimension re-lating to service experience evaluation: ambience.
Participants
The study’s participants were PRC adult residents ona holiday trip to Macau who were confirmed to be gam-bling in one of the seven largest casinos in Macau. Thiscustomer market is representative of more than 90% ofthe customers for each of the casinos in the study. Thesurvey instrument was a four-sided booklet containingthe questions.
Survey Instrument
The survey was a four-sided booklet written in the Chi-nese language and included all questions related to thestudy. The survey was pilot-tested twice (n = 30) forclarity. Eight questions were revised after the first pi-lot test and two were revised after the second pilot test.
Procedure
A request for a grant to conduct the survey was soughtand received from the Secretariat for Economy and Fi-nance of Macau. With assistance of the Macau govern-ment, all casinos contacted agreed to participate in thestudy. Data collections for the study were conducted inthe top seven casinos by total annual revenues.
For the data collection, three female master-levelstudents approached casino customers as they beganto exit the table gaming area of each casino withthe request to participate in a four-minute survey—approaching the fifth customer party following the com-pletion of a prior survey by a customer. Prospective par-ticipants were offered a choice of a US $25 food voucheror a collapsible umbrella for participation. A total of50% of customers approached agreed to participate inthe survey. Participants completed the survey whilebeing seated at a fold up table in an area nearby thegaming floor. Ninety-two percent of these customersanswered all questions in the survey. The survey wascompleted in two time periods per day: 2–5 pm and 7–10pm for three days per week in each of the seven casi-nos. The afternoon time period was used first and thenthe evening time period in the following weeks. Thedata were collected over one month in February 2013.Customer participation agreement levels did vary sys-tematically among the three interviews but customers’answers did not. The top interviewer had 60% coopera-tion and the bottom interviewer had 40% cooperation.
1114 PRENTICE AND WOODSIDEPsychology and Marketing DOI: 10.1002/mar

Table 1. Construct Scale Coefficient α (and Corrected Item to Total Correlations) (Decimal Points Omitted).
Immediate outcomes Global outcomes
Casino has up-to-date appealing facilities, α = 92 Casino is my first choice (single item)
The casino has up-to-date equipment (85)
The casino’s physical facilities are visually appealing(84)
The casino’s physical facilities are clean (82)
The appearance of the physical facilities of the casinois in keeping with the type of service provided (72)
I always consider this casino as my first choice to visit
Quality of service response, α = 86 Overall service quality, α = 83
When the casino promises to do something by acertain time, it does so (74)
The casino provides its services on time (80)
The casino tells its customers exactly when serviceswill be performed (67)
Overall service quality of the casino (71)
Overall how satisfied are you with the serviceprovided by the casino (71)
Casino has best interest at heart plus employees care, α =94
Positive word-of-mouth for this casino, α = 96
The casino has your best interest at heart (75)
When you have problems, the employees aresympathetic and reassuring (81)
The employees are dependable (81)
The employees are helpful (83)
The employees are polite (87)
The employees are aware of your needs (79)
I say positive things about the casino to other people(92)
I recommend the casino to other players who haven’tbeen here (92)
Quality of the games, α = 89 Propensity to switch from this casino, α = 87
The casino has sufficient number of table gamesavailable (75)
The casino has sufficient number of slot machinesavailable (78)
The casino provides a variety of games (85)
I will switch to other casino that offers better servicesand deal (78)
I will switch to another casino if I experience aproblem (78) with the casino service
Food and beverage quality, α = 83
The casino offers a variety of food and beverage (73)
The price of food and beverage is reasonable (66)
The quality of food and beverage is excellent (67)
Ambience, α = 86
The casino’s ambience is comfortable (76)
The casino’s decor and layout are stylish (76)
Survey cooperation levels did not vary systematicallyamong the seven casinos.
FINDINGS
In general, the hypotheses in the model relating to therelationship of antecedent conditions and problem gam-bling receive support. However, the findings indicate
negative relationships between problem gambling andcasino service performance consistently, contrary to theproposed positive relationships.
How the Antecedents Associate withProblem Gambling
Figure 4 is a summary of findings for the associations ofproblem gambling with the antecedent conditions and
PROBLEM GAMBLERS’ HARSH GAZE 1115Psychology and Marketing DOI: 10.1002/mar

Gender ProblemGambling
ß = .39
Ageß = .30
Educationß = -0.14
Incomeß = 0.19
Occupationphi2 = .24
Casino up-to-date,appealing facilities
Zero Low Mid High HighestProblem Gambling
ß = - .23
Quality of service
responsiveness
ß = - .22
Casino has my best interestsat heart plusemployees care
Casino rewardcard holder
ß = .46
Length-of-playEach visit, hours
ß = .22
Average bet1 phi2 = .09
Number of annual visits ß = .47
ß = - .21
Figure 4. Main effect paths (standardized β coefficients [βs], and ϕ2).aAverage bet size has a negative relationship with gambling problem.
three immediate outcomes conditions. All estimates ofrelationships in Figure 4 are significant statistically ex-cept for that education does not associate with problemgambling.
H1: Age. The findings support H1: increasing age asso-ciates with increases in problem gambling scores. Thestandard simple regression coefficient for age (β = 0.30)is significant statistically. However, the effect size isconsidered medium given that the significant overallage and problem gambling association does not occuramong all seven casinos.
The findings support the proposition that problemgambling is an age progressive difficulty except for thefinal age segment: the problem gambling mean (M) andstandard error (SE) of the mean for this segment (61+)are about the same as for the youngest segment (18–25): M = 0.60, SE = 0.60 for the five customers in the61+ age group and M = 0.62, SE = 0.24 for the 32 par-ticipants in the 18–25 segment. The average problemgambling score peaks for the 46–55 age group (n = 85):M = 2.92, SE = 0.40.
H2: Gender. The findings support the second hypoth-esis. The simple linear regression coefficient (β = 0.39),the consistent higher average scores for males versusfemales for all age segments, and the significant corre-lations between gender and problem gambling for sixof seven casinos indicate a large effect size for gender.Problem gambling is a male difficulty in particular.
The findings include a substantial relationship be-tween problem gambling and annual visitation amongmale versus female segments. For females, averagenumber of trips to casinos does not vary for low (1.7trips) versus high (2.0 trips) problem-gambling scores.For males, average number of trips increases dramati-cally among males (from 2.7 trips for zero to 5.0 trips)as problem gambling scores increases.
H3: Education. The findings support H3 that higherformal education associates with lower problem gam-bling. The M (SE) for problem gambling for high schooldiploma graduates was 0.95 (n = 84) versus 2.7 (0.29)for the 138 junior high school participants and 2.3 (0.26)for the 163 high school attendees. Among the 23 partic-ipants with schooling less than junior high, the average
1116 PRENTICE AND WOODSIDEPsychology and Marketing DOI: 10.1002/mar

problem gambling score was 1.6 (0.56). Thus, a curvilin-ear relationship occurs for education and problem gam-bling, few members of the lowest and high educationsegments experience problem gambling in comparisonto the two middle educational segments.
Formal educational training to avoid problem gam-bling may need to begin early in life to reach futureproblem gamblers—many problem gamblers will notbe around to receive such training in high school. Incomparison to the findings for the other antecedentconditions, the effect size for education’s influence onproblem gambling is small.
H4: Income. The findings do not support H4 that in-come level has no association with problem gambling. Ahighly significant positive relationship occurs betweenincome and problem gambling. Here are rather dra-matic findings: for the 123 participants with householdannual incomes below US $3000, the mean (and SE ofthe mean) for problem gambling is 1.67 (0.29); the mean(SE) for the 64 participants in the highest householdincome categories (>$20,000 annually) the average is3.45 (0.48). Low-income earners appear to have lessgambling problem. While the effect size is medium forincome’s influence on problem gambling, the impact ispositive and significant statistically. Additional detailsappear in Table 2.
H5: Occupational Status. The findings partially con-firm H5. The average problem gambling score (and SE)is lowest for the 53 participants in professional occupa-tions: M = 1.04 (0.31). The average (and SE) is high-est for the 19 participants identifying themselves to beworkers: 4.26 (1.06). However, the averages for man-agers (n = 40) and clerks (n = 53) are counter to the per-spective that occupational status has a negative rela-tionship with problem gambling: 3.33 (0.50) versus 1.00(0.26). For the 54 participants in customer service andsales, the problem gambling mean is 2.69 (SE = 0.45);the average is lower for agricultural and forestry work-ers: n = 14, M = 1.50 (SE = 0.65). Thus, for problemgambling, workers (i.e., laborers) and managers are at
Table 2. Respondents’ Income Distribution andAverage Problem Gambling Severity Index Scores(Standard Error of the Mean).
Income ($) 0 1–2 3–4 5–6 7+ Total (n) Mean (SE)
<3000 66% 9% 13% 3% 9% 123 1.7 (0.29)3001–6000 60 14 11 7 8 159 1.8 (0.23)6001–10,000 57 10 13 10 10 30 1.9 (0.47)10,001–15,000 25 7 32 36 0 28 3.1 (0.41)15,001–20,000 72 0 14 0 14 7 1.4 (1.02)20,001–25,000 33 0 22 33 11 9 3.6 (1.01)25,001–30,000 25 13 25 38 0 8 3.4 (0.86)30,000 0 0 0 33 67 3 7.3 (0.88
Total 57 11 14 10 8 367 2.0 (0.15)
ANOVA results combined: F = 3.011, df = 7/359, p < 0.004; linearitytest: F = 113.530, df = 1, 359, p. < 0.000.
η2 = 0.055, a moderate effect size.
risk in particular and clerks and agricultural/forestryworkers are not. Occupational categories rather than“occupational status” relates to problem gambling.
H6: Membership in Casino Reward Card Pro-grams. The association of membership in casino re-ward card programs with problem gambling is positiveand the effect size is large. The average problem gam-bling score among the 171 participants reporting notholding casino membership is 0.48 (SE = 0.10); theaverage among the 234 participants reporting mem-bership is 3.21 (SE = 0.23). Eliminating or curtailingcasino reward card membership programs are likelypositive steps in curtailing problem gambling. The largepositive effect of these programs on problem gamblingoccurs for each of the seven casinos.
H7: Hours of Playing Time per Day. The findingssupport H7: playing time gambling in casinos asso-ciates positively with problem gambling. The effect sizeis large and occurs consistently across the seven casi-nos. Limiting players time gambling in casinos to threehours or less during the daytime and the same at nightare steps likely to be effective in curtailing behaviorsrelating to problem gambling. Implementing such stepsare possible but should await confirmation by controlledtrue experiments with treatment and control group con-ditions that indicate doing so is effective in curtailingproblem gambling.
H8: Average Betting. H8 predicts a positive rela-tionship between average bet size and problem gam-bling. The findings do not support H8. The findings arecounter to H8: participants with high problem gam-bling scores (n = 38) all have average bets less than1000 MOP (Macau Pataca currency; 1000 MOP = US$125.41). None of the 16 participants reporting averagebet sizes at 1000 MOP or higher have problem gamblingscores equal to 7 or higher.
The perspective that problem gambling is not foundamong players in special casino rooms for high rollersreceives support in the present study. Problem gam-blers are concentrated in Macau among relatively low-stakes table gambles (i.e., where average bets are 100MOP).
H9: Annual Visitation. The number of annual visitsassociates positively with problem gambling. The β =0.47 (Figure 4) for the linear regression coefficient andthe ϕ2 coefficient equal to 0.25 indicate a large effectsize. While 2% of respondents taking one annual tripto a casino score in the severest level of problem gam-bling, the share of respondents taking 7+ annual tripsto casinos having the same severe level is 57%.
A large increase in share of severely high problemgambling scores occurs for six versus five trips. Limitingthe number of recreational trips to Macau five or feweris likely to be an effective control on problem gamblingin casinos.
PROBLEM GAMBLERS’ HARSH GAZE 1117Psychology and Marketing DOI: 10.1002/mar

How Problem Gambling Associates with theImmediate Service Evaluations
Consistently negative associations occur for problemgambling and evaluations of casino services. Figure 4presents visuals of these relationships for three imme-diate service dimensions. The consistent negative as-sociations were a surprise, which warrants a post hocexplanation. Problem gamblers are likely to recognizethat their casino gambling is unhealthy—and that theservice provider is at least partially (if not entirely) toblame for their behavior. Blaming the service providermay be preferable than blaming oneself for surrender-ing to a highly intense desire—the low control and highmotive state in Nataraajan and Goff (1991) typology.
This revisionist explanation expands on Urry’s(1990) “tourist gaze.” The tourist gaze in some impor-tant ways is a destructive process whereby both theservice provider and the tourist reflect upon each otherthe gaze of expectations of good times and positiveoutcomes—winning at the gaming tables for example—since reality infrequently matches these expectations,negative evaluations follow.
H10: Casino’s Physical Facilities. Problem gam-bling scores have a significant negative relationship(β =−0.23) with customers’ evaluations of the casino’sphysical facilities. Respondents with severely highproblem gambling scores (7+) offer less favorable eval-uations about the casino’s appearance. This finding forthe overall sample does not occur consistently for eachof the seven casinos.
Some correlations among the different casinos varysignificantly. The findings for Casino D support H10that a positive relationship occurs between casino prob-lem gambling and a casino’s physical facilities (r =0.242, p < 0.04, one-tailed test). The negative overallfinding for the total sample suggests the need to collectdata sufficiently among several casinos to clarify prob-lem gambling and customer evaluations of services.
H11: Quality of Service Responsiveness. Problemgambling scores have a significant negative relation-ship (β = −0.22) with the service responsiveness of thecasino. This finding occurs consistently for all sevencasinos. Casino patrons with severe problem gamblingreport substantially lower scores on service responsive-ness. The especially high relatively unfulfilled needfor response speed among problem gamblers matcheswith Nataraajan and Goff’s (1991) assessment of high-intensity motivation as a necessary condition of com-pulsive buying. The consistency of the findings for thisrelationship across the seven casinos supports this in-terpretation.
H12: First Choice. Problem gambling scores have asignificant negative relationship (β =−0.14) with cus-tomer evaluations of the casino as their first choice.This negative relationship occurs consistently thoughnot significantly among the seven casinos. The rela-
tionship is small in effect size. Its occurrence supportsthe belief that a problem gambler’s bad luck or lossesmay result in moving to another casino next time.
H13: Casino Has My Best Interests at Heart plusEmployees Care (Hereafter BIPEC). Problem gam-bling scores have a significant negative relationship(β =−0.21) with customer evaluations about the casinohaving their best interest at heart plus caring employ-ees. This negative finding holds consistently but notsignificantly for all seven casinos. The effect sizes ofthe relationship ranges from small to medium.
This BIPEC dimension associates strongly with pos-itive word-of-mouth advertising (r = 0.66). Given thatrelatively low scores on caring, the significant nega-tive relationship between problem gambling scores andWOM is unsurprising (r = −0.12, p < 0.01, two-tailedtest). The problem gambler is most likely to spread un-favorable messages about the casino that is perceivedto be uncaring and to have no heart.
H14: Game Service. The linear relationship be-tween game service and problem gambling is negative(β = −0.07) though significant statistically. Problemgamblers are more likely to conclude that game ser-vice is great at Casino “X” than other casino customers.The relationship for customer evaluations of game ser-vice and problem gambling is “U”-shaped. However,the effect size is small and the findings vary amongthe seven casinos, which support the conclusion thatproblem gambling does not have a substantial influ-ence on customer evaluations of game service. Whilethe U-shaped relationship is impressive for the overallfindings, the SE for the mean of game service is rel-atively large in the case of respondents with severelyhigh PGSI scores and the effect size is small.
H15: Food and Beverage Service. A significant neg-ative relationship occurs for problem gambling scoresand customer evaluations of the casino’s food and bever-age service (β = −0.27). The relationship is consistentlynegative across all seven casinos though the correlationis close to zero for Casino D. The overall effect size ismedium for this relationship.
H16: Overall Service Quality. A small effect sizebut significant negative relationship occurs for problemgambling scores and the casino’s overall service quality(β = −0.14). Casino D is an exception that a positive re-lationship is present between problem gambling scoresand overall service quality.
H17: Positive WOM. The relationship between prob-lem gambling scores and positive word-of-mouth com-munication is cubic: down, up, and down. The aver-age + WOM score for severely high PGSI scores is sig-nificantly below the +WOM average for respondentswith zero PGSI scores (details are available from theauthors). These findings confirm McClelland’s (1998)
1118 PRENTICE AND WOODSIDEPsychology and Marketing DOI: 10.1002/mar

Casino up-to-date, appealing facilitiesß = - .23
ß = - .22
Casino has my best interestsat heart + employees careProblem
Gambling
Quality of service responsiveness
ß= -.07 Quality of games
ß = -.21
Food & beverage qualityß = - .20
Overall servicequality of casino
ß = -.14
+WOM for this casinoadj. R2 = .41, d.f. = 2/407
ß1, ß2, ß3 = -.99, +2.64, -1.82
Casino switching propensity
ß = - .09
This casino is my first choice to visit(adj. R2 = .52, d.f. = 2/407) ß = - .14
ß = .32
ß = .48
ß = .55
ß = .16
ß = .25
ß = .13
(adj. R2 = .55, d.f. 5/404)
Ambienceß = - .09 ß = .26
ß = .17
ß = .15
r = .66
ß = .32, adj. R2 = .10
Figure 5. Problem gambling and evaluations of casino attributes and overall outcomes: Simple regression analyses and multiple(in bold) regression analyses for three overall outcomes.
recommendation to look beyond simple linear relation-ships when examining variables.
H18: Ambience. The relationship between ambienceand problem gambling is statistically significantly neg-ative for most casinos in the study, with an exception forCasino D. Ambience of Casino D appears to be more ap-pealing for problem gamblers. For the purposes of thestudy, the negative overall relationship runs counterand refutes H18 that a positive relationship occurs forproblem gambling and ambience. The findings serve toemphasize the value of self-replication in several places(contexts).
H19: Switching. While the effect size is small, thefindings do support H19—problem gambling associatesnegatively with switching to another casino (β = −0.09).The findings are inconsistent among the seven casi-nos. The overall appropriate conclusion is that problemgambling does not associate substantially with casinoswitching behavior. While increasing the hypothesizedproblem gambling continuum associates lower evalua-tions rather consistently, this influence does not trans-late into motive to switch casinos.
H20: Immediate and Global Outcomes. The find-ings support H20. Customer evaluations of the imme-diate service dimensions have substantial influences onthe global outcome measures. The results from perform-ing multiple regression analyses (MRA) for the global
outcomes appear in Figure 5. Problem gambling is aninsignificant effect on the global outcomes in the MRAwhen the models include the immediate service out-comes.
Figure 5 shows five immediate outcome variablescontribute significantly in influencing evaluations ofoverall quality of service: ambience, quality of games,food and beverage quality, facilities, and heart + car-ing. The effect size is large for this model.
Predictive validities for overall service quality wereestimated of individual casinos. The findings appearin Table 3. Every casino model serves to predict theoverall service quality scores across the seven casinos(see Table 3). All the effect sizes are large and supportthe conclusion that the immediate service outcomes areuseful in predicting overall service quality evaluations.
While this study focuses on antecedents and out-comes of problem gambling, the pattern of findings forimmediate and global outcomes provides nomologicalvalidity to estimate whether problem gambling has in-fluence on service quality evaluations.
H21 Receives Support. While problem gambling doeshave a small direct influence on global outcomes, itsinfluence is larger consistently on the immediate out-comes. For example, for predicting propensity to switch,while the beta, standardized partial regression coef-ficient (β), for problem gambling is −0.09, the betafor problem gambling influence on food and beveragequality is −0.20.
PROBLEM GAMBLERS’ HARSH GAZE 1119Psychology and Marketing DOI: 10.1002/mar

Table 3. Predictive Validities of Seven Overall Casino Service Quality and Satisfaction (OCAQS) Models:Correlations (rs) of Predicted and Actual Scores Using Individual Models for Each of the Seven Casino.
Casino: A B C D E F G
n = 69 68 62 53 60 40 60Casino A model: OCSQS = 1.989 + (.543 × Ambience) + (.070 × heart + service responsiveness), adj. R2 = 0.556, df = 2/66r = 76 57 71 82 55 62 71Casino B model: OCSQS = 3.079 + (.257 × Food Beverage) + (.150 × Facilities Quality), adj. R2 = 0.440, df = 2/64r = 66 68 73 80 61 77 69Casino C model: OCSQS = 2.411+ (.265 × Food Beverage)+(.162 × Facilities Quality), adj. R2 = 0.522, df = 2/59r = 66 68 73 80 62 77 70Casino D model: OCSQS = −.452 +(.650 × Ambience) + (.251 Food Beverage), adj. R2 = 0.714, df = 2,49r = 69 60 68 78 58 55 68Casino E model: OCSQS = 2.88 + (.214 × Food Beverage) + (.235 × Quality Games), adj. R2 = 0.434, df, = 2,57r = 60 62 71 77 67 72 67Casino F model: OCSQS = 1.175 + (.327 × Food Beverage) + (.199 × Facilities Quality), adj. R2 = 0.563, 2/37r = 66 68 73 80 62 77 70Casino G model: OSSQS = 1.207 + (.317 × Facilities Quality + (.084 × heart + employees care), adj. R2 = 0.54, 2/57r = 66 59 70 73 73 71 74
Note:: Decimal points omitted for r values.
H22 Receives Limited Support: Overall ServiceQuality as a Lynchpin. Overall service quality doesaffect +WOM separately in modeling the immediateand other global outcomes. However, “lynchpin” is prob-ably an inflated view on how overall service quality in-fluences other global outcomes. For H22a, customers’overall service quality perceptions do not have a directinfluence on propensity to switch in an MRA model, seeFigure 5. For H22b, customers’ overall service qual-ity perceptions do have a direct positive word-of-mouthcommunications in an MRA model and do not on havea direct influence on first preference for the presentcasino the customer is visiting in an MRA model asH22c predicts.
Meta-Analyses: Additional Findings. Table 4 pro-vides findings from a meta-analysis of the principalrelationships for antecedent and immediate outcomeconditions. The findings support the general conclusionthat problem gambling has a positive relationship withthe three antecedents: casino membership; annual vis-itation; and length of play each day.
The results also show that problem gambling hasnegative relationships substantially for six of the sevenimmediate service quality dimensions. The range ofthe estimates for each of the seven immediate servicedimensions is more negative than positive, which re-futes the original perspective that problem gamblingcontributes positively to casino service evaluations.
GENERAL DISCUSSION, CONTROLLINGPROBLEM GAMBLING STRATEGIES, ANDREVISING THEORY
Demographic Antecedent Conditions
The demographic and problem gambling findings forgamblers in Macau casinos are highly similar to find-
ings in Afifi et al.’s (2010) study of a 2002 Canadiannational health survey data (n = 18,913). However,the two studies are not highly comparable since thisstudy’s context is different. Afifi et al. (2010) compareonly subsamples of respondents with nonproblem gam-bling (zero scores on the PGSI) versus problem gam-bling scores (3–7), and combines moderate and severerisk gamblers into one group (referred to as problemgamblers) because scores of three to seven reflect sig-nificant risk that may or may not have adverse conse-quences related to gambling for the gambler.
The present study does not include combining mod-erate and severe risk gamblers but compares segmentsusing PGSI scores of zero, 1–2, 3–4, 5–7, and 7+ scores.Gender (male), age (middle-aged), occupation (man-agers and laborers), education (moderate), and income(high) have positive associations with problem gam-bling in the present study. However, association of de-mographic configurations with problem gambling doesnot occur among middle-aged male managers with mod-erate educations and high incomes. This finding indi-cates strategies to control (i.e., lessen the occurrenceand prevent) problem gambling would likely be focusedon specific customer segments that include middle-agedmen or younger in specific occupations with relativelymoderate to high incomes.
Behavioral Antecedent Conditions
In the present study casino membership, length of playper day and number of casino-related trips associatepositively with problem gambling. Average bet size incasino table games has a negative association withproblem gambling. However, this negative associationoccurs only for relatively high volume players.
The findings indicate that average betting volumedoes not associate with problem gambling. Hence, ac-tions that can be used to control problem gamblingshould be focused on reducing or eliminating the
1120 PRENTICE AND WOODSIDEPsychology and Marketing DOI: 10.1002/mar

Table 4. Meta-Analysis of Antecedents and Outcomes of Problem-Gambling across Seven Casinos.
r forTotal n
UnweightedMean r
StandardError
95%Confidence
Interval
Antecedents• Casino reward card +0.445 +0.448 0.037 +0.356 to
+0.539• Number of visits annually +0.411 +0.408 0.060 +0.260 to
+0.553• Length of play each day +0.220 +0.232 0.046 +0.120 to
+0.343Outcomes• The casino has your best interest at heart; services quality −0.275 −0.243 0.040 −0.340 to
−0.146• Quality of games −0.028 −0.103 0.103 −0.354 to
+0.149• Food and beverage quality −0.202 −0.250 0.070 −0.420 to
−0.080• Overall service quality/satisfaction −0.137 −0.183 0.075 −0.368 to
+0.001• Positive word-of-mouth −0.119 −0.114 0.076 −0.300 to
+0.073• This casino is my first choice −0.135 −0.139 0.041 −0.240 to
−0.038• Switch casino propensity −0.091 −0.085 0.066 −0.250 to
+.077
benefits of casino reward card programs, reducing thelength of play per day to six or fewer hours, and limitingthe number of annual trips to five or fewer.
Immediate and Global OutcomeConditions—Problem Gambling andService Provider Evaluations
For the most part, increases in the continuum ofproblem gambling (i.e., the PGSI scores) associates neg-atively with customer evaluations of their immediateexperiences and global service evaluations. The 95%confidence intervals for the estimates indicate that ifthe study was done 100 times, negative rather than pos-itive correlations for problem gambling and customerevaluations of casino services would occur.
Based on these findings, the original proposals forpositive-balanced relationships among problem gam-bling, casino game service, and evaluations of customerservice experiences need revising. The revision in Fig-ure 3b provides balance among four concepts while thestrong associations between problem gambling withcasino game service and gambling losses are still in-cluded.
From theory the problem gambler should associatelosses positively with casino services and negativelywith gambling per se, which aids in rationalizing thebehavior of continuing to gamble. What the problemgambler may perceive is a mix of conscious and uncon-scious rationalization that the losses attribute to thebad services in casinos but not to his or her gamblingbehavior. However, associations 2, 3, and 6 in Figure 3b
may be necessary for explaining the negative problemgambling and service evaluation associations.
Assuming major gambling losses represent a highlynegative experience that is likely to cause high cogni-tive dissonance for the problem gambler as Festinger(1957) suggests. Such cognitive dissonance leads prob-lem gamblers attributing gambling losses to casino ser-vice.
Given that gambling outcome (winning or losing) isunpredictable, and losses seems to be prevalent, blam-ing the quality of casino services may be more conve-nient for problem gamblers. Testing the applicabilityof this model and other relevant self-context outcometheories (e.g., Bem’s, 1967, self-perception theory) mayrequire direct measurement of problem gambling di-mensions based on Nataraajan and Goff’s (1991)motive-control continuum rather than on an index fo-cusing on consequences of problem gambling.
LIMITATIONS AND IMPLICATIONS FORFUTURE RESEARCH
While the use of a self-report nine-item index to esti-mate the extent of problem gambling is useful, mostitems (1, 3, 4, 6,7, and 8) in the index (i.e., the PGSI)measure consequences to problem gambling ratherthan problem gambling as a configuration of high mo-tive and low control as Nataraajan and Goff (1991) de-scribe compulsive buying. Use of self-reports, especiallyto measure a highly negative psychological state can beproblematic (see Nisbett & Wilson, 1977). The same
PROBLEM GAMBLERS’ HARSH GAZE 1121Psychology and Marketing DOI: 10.1002/mar

criticisms apply to using Faber and O’ Guinn’s (1992)clinical screener for compulsive buying.
Future research needs to include easy-to-administermetrics that overcome these twin limitations. Suchmetrics are likely to involve the use of small samples(n < 100) of different segments that do not exhibit lev-els of antecedent conditions to associate with problemgambling. Given that the difficulty is progressive andchronic, longitudinal studies rather than the dominat-ing cross-sectional method would be particularly usefulin problem gambling research.
The findings may not hold for casino customers inother Asian or Western markets. Additional studiesare necessary in other locations (e.g., Las Vegas andMonaco) to conform or refute the findings. The samplesizes for each casino in the study are quite small; largersample sizes for several daily and seasonal periods arenecessary for confirming the exploratory findings of thepresent study. Future studies should collect data onwinnings or losses of respondents at the time of theinterviews. Feelings of euphoria or despair from majorwinnings or losses, respectively, may affect evaluationsof immediate and global casino services.
REFERENCES
Afifi, T.O, Cox, B. J., Martens, P. J., Sareen, J., & Enns, M. W.(2010). Demographic and social variables associated withproblem gambling among men and women in Canada. Psy-chiatry Research, 178, 395–400.
Bem, D. J. (1967), Self-perception: An alternative interpre-tation of cognitive dissonance phenomena. PsychologicalReview, 74, 183–200.
Black, D. W., Shaw, M., & Blum, N. (2010). Pathologicalgambling and compulsive buying: Do they fall within anobsessive-compulsive spectrum? Dialogues in Clinical Neu-roscience, 12, 175–185.
Bleuler, E. (1930). Textbook of psychiatry. A. A. Brill (Trans.).New York, NY: Macmillan.
Budden, M. C., & Griffin, T. F. (1996). Explorations & ap-plications of aberrant consumer behaviour. Psychology &Marketing, 13(8), 739–740.
Cartwright, C., DeCaria, C., & Hollander, E. (1998). Patholog-ical gambling: A clinical review. Journal of Practical Psy-chiatry Behavior Health, 5, 277–286.
Chang, C.-W., Tseng, T.-H, & Woodside, A. G. (2013). Con-figural algorithms of patient satisfaction, participation indiagnostics, and treatment decisions’ influences on hospitalloyalty. Journal of Services Management, 27, 91–103.
Cobb, C. J., & Hoyer, W. D. (1986). Planned versus impulsepurchase behavior. Journal of Retailing, 62, 384–409.
Cohen, J. (1977). Statistical power analysis for the behavioralsciences. New York: Academic Press.
Cronin, J. J., & Taylor, S. A. (1992). Measuring service qual-ity: A reexamination and extension. Journal of Marketing,56(3), 55–68.
Cronin, J. J., & Taylor, S. A. (1994). SERVPERF ver-sus SERVQUAL: Reconciling performance-based andperceptions-minus-expectations measurements of servicequality. Journal of Marketing, 58(1), 125–131.
Dittmar, H., & Howard, S. (2004). Professional Hazards? Theimpact of models’ body size on advertising effectiveness and
women’s body-focused anxiety in professionals that do anddo not emphasize the cultural ideal of thinness. BritishJournal of Social Psychology. 43(4), 477–497.
Faber, R. J., & O’ Guinn, T. C. (1992). A clinical screenerfor compulsive buying. Journal of Consumer Research, 19,219–225.
Felicity, K., Lorains, F. K., Cowlishaw, S., & Thomas, S.A. (2011). Prevalence of comorbid disorders in problemand pathological gambling: Systematic review and meta-analysis of population surveys. Addiction, 106, 490–498.
Ferris, J., & Wynne, H. (2001). The Canadian problem gam-bling index: Final report. Ottawa, ON: Canadian Centre onSubstance Abuse.
Festinger, L. (1957). A theory of cognitive dissonance. Stan-ford, CA: Stanford University Press.
Fitzsimons, G. J. (2008). Death to dichotomizing. Journal ofConsumer Research, 35, 5–8.
Hirschman, E. C. (1992). The consciousness of addition: To-ward a general theory of compulsive consumption. Journalof Consumer Research, 19, 155–179.
Holtgraves, T. (2009). Evaluating the problem gamblingseverity index. Journal of Gambling Studies, 25:105–120.
Kessler, R. C., Hwang, I., LaBrie, R., Petukhova, M., Sampson,N. A., Winters, K. C., et al. (2008). DSM-IV pathologicalgambling in the National Comorbidity Survey Replication.Psychological Medicine 38, 1351–1360.
Kline, P. (1999). The handbook of psychological testing, 2nded. London: Routledge.
Koran, L. M., Faber, R. J., Aboujaoude, E., Large M. D., SerpeR. T. (2006). Estimated prevalence of compulsive buyingin the United States. American Journal of Psychiatry, 163,1806–1812.
Kraepelin, E. (1915). Psychiatrie, Vol. 15 (8th ed., pp. 408–409). Leipzig, Germany: Verlag Von Johann AmbrosiusBarth.
LaPlante, D. A., Nelson, S. E., LaBrie, R. A., & Shaffer, H. J.(2009). Stability and progression of disordered gambling:Lessons from longitudinal studies. Canadian Journal ofPsychiatry, 53, 52–60.
LaRose, P. (2001). On the negative effects of e-commerce:A sociocognitive exploration of unregulated on-line buy-ing. Journal of Computer-Mediated Communication, 6,1–12. LaRose, R. (2001). On the negative effects ofe-commerce: A sociocognitive exploration of unregu-lated on-line buying. Journal of Computer-MediatedCommunication, 6. Retrieved from http://jcmc.indiana.edu/vol6/issue3/larose.html.
Lorenz, V. C., & Yaffee, R. A. (1986). Pathological gambling:Psychosomatic, emotional and marital difficulties as re-ported by the gambler. Journal of Gambling Behavior, 2:40–45.
Marshall, K., & Wynne, H. (2003). Fighting the odds. Perspec-tives on Labour and Income, 4(12), 12–13.
Marshall, K., & Wynne, H., 2004. Against the odds: A profileof at-risk and problem gamblers. Canadian Social Trends,11, 25–29.
McClelland, D. C. (1998). Identifying competencies withbehavioral-event interviews. Psychological Science, 9, 331–339.
Nataraajan, R., & Goff, B. G. (1991). Compulsive buying: To-ward a reconceptualization. Journal of Social Behavior andPersonality, 6, 307–326.
Nisbett, R. E., & Wilson, T. D. (1977). Telling more than we canknow: Verbal reports on mental processes. PsychologicalReview, 84, 231–259.
1122 PRENTICE AND WOODSIDEPsychology and Marketing DOI: 10.1002/mar

National Opinion Research Center at the University ofChicago (NORC) (1991). Gambling Impact and BehaviorStudy, Report to the National Gambling Impact StudyCommission, April 1.
Nower, L., & Blaszczynski, A. (2010). Gambling motivations,money-limiting strategies, and precommitment preferencesof problem versus non-problem gamblers. Journal of Gam-bling Studies, 26, 361–372.
O’Keeffe, K. (2013). Macau gambling revenue up 25%on year in March to record MOP 31.34 billion.Dow Jones Business News, April 02. Retrieved fromhttp://www.nasdaq.com/article/macau-gambling-revenue-up-25-on-year-in-march-to-record-mop3134-billion-20130402-00043#.UV2i2TdPF0w. Accessed 1 April 2013.
Peter, J. P. (1981). Construct validity: A review of basic issuesand marketing practices. Journal of Marketing Research,18, 133–145.
Parasuraman, A., Zeithaml, V. A., & Berry, L. L. (1994).Reassessment of expectations as a comparison standardin measuring service quality: Implications for further re-search. Journal of Marketing, 58(1), 111–124.
Prentice, C. (2013). Who stays, who walks, and whyin high-intensity service contexts. Journal of Busi-ness Research. Retrieved from http://dx.doi.org/10.1016/j.jbusres.2013.02.044.
Rook, D. W., & Fisher, R. J. (1995). Normative influence onimpulsive buying behavior. Journal of Consumer Research,22, 305–313.
Shaffer, H. J., & Hall, M. N. (2001). Updating and refin-ing prevalence estimates of disordered gambling behavior
in the United States and Canada. Can Journal of PublicHealth, 92, 168–172.
Urry, J. (1990). The tourist gaze. Thousand Oaks, CA: Sage.Wong, I. K., & Fong, V. H. I. (2012). Development and valida-
tion of the casino service quality scale: CASERV. Interna-tional Journal of Hospitality Management, 31, 209–217.
Woodside, A. G., & Zhang, M. (2012). Identifying X-consumersusing causal recipes: ‘‘Whales’’ and ‘‘jumbo Shrimps’’ casinogamblers. Journal of Gambling Studies, 28:13–26.
Woodside, A. G., Frey, L. L., & Daly, R. T. (1989). Linkingservice quality, customer satisfaction, and behavioral in-tention. Journal of Health Care Marketing, 9, 5–17.
The field work for the study in this article was supported by agrant from the Secretariat for Economy and Finance of Macau;the authors express their gratitude for this support. The ap-pendices relevant for each casino and the entire set of datain this study do not appear in this copy of the paper but areavailable from the authors upon your request.
Correspondence regarding this article should be sent to: DrCatherine Prentice, Lecturer of Marketing, Professor ArchG. Woodside, Professor of Marketing, Faculty of Businessand Enterprise, Swinburne University, Melbourne, Australia([email protected]); Arch G. Woodside, Depart-ment of Marketing, Carroll School of Management, BostonCollege, 140 Commonwealth Avenue, Chestnut Hill, MA02467([email protected]).
PROBLEM GAMBLERS’ HARSH GAZE 1123Psychology and Marketing DOI: 10.1002/mar