Embed Size (px)
Citation preview
Pediatr Radiol (2006) 36: 138–140DOI 10.1007/s00247-005-0003-3
CASE REPORT
Ronit Agid . Sivan Lieberman . Michael Nadjari .John M. Gomori
Prenatal MR diffusion-weighted imaging in a fetuswith hemimegalencephaly
Received: 8 June 2005 / Accepted: 8 July 2005 / Published online: 16 November 2005# Springer-Verlag 2005
Abstract We report a case of hemimegalencephalydiagnosed by prenatal MRI with an emphasis on itsappearance on diffusion-weighted images. This case showsthat in this condition the enlarged hemisphere may showrestricted diffusion on prenatal MRI. In our opinion, thisfinding may result from a combination of increasedcellularity and advanced myelination in the affectedhemisphere. Restricted diffusion is an additional valuableindicator in the analysis of the fetal brain.
Keywords Fetus . Hemimegalencephaly . MRI .Diffusion-weighted MRI
Introduction
Hemimegalencephaly is a congenital malformation ofcortical development that consists of a unilateral enlargeddysplastic cerebral hemisphere. Patients present with earlyonset of intractable seizures, hemiplegia and moderate-to-severe developmental delay that depends on the extent ofhemispheric involvement [1].
Structural findings on MRI include moderate-to-markedenlargement of the involved hemisphere, and the involvedcortex is typically dysplastic, with broad gyri, shallow sulciand cortical thickening. The gyral pattern can range fromgrossly normal to frankly agyric. In severely affectedpatients, the usually sharp border between the cortex and
the subcortical white matter may be blurred or may havedisappeared altogether. The white matter usually showspatchy or diffuse mixed regions of prolonged andshortened T1 and T2 relaxation times [1, 2]. The ipsilaterallateral ventricle is typically enlarged with a characteristicconfiguration of its frontal horn, being almost straight andpointing superiorly and anteriorly [1].
Although prenatal US is quite accurate in the diagnosisof fetal brain anomalies, including hemimegalencephaly[3], MRI has an important role in further establishing thediagnosis and differentiating it from other conditions [4].While the MRI appearance of hemimegalencephaly is welldescribed [1], there are as yet no detailed reports of itsappearance on diffusion-weighted images (DWI).
Case report
A 22-year-old woman, 32 weeks into her first pregnancy,was referred for a prenatal MRI examination due tounilateral ventricular enlargement in the fetal brain. Theenlarged ventricle measured 24 mm and was found onroutine fetal US. MRI was performed on a 1.5-T MRsystem (Signa, GE, Milwaukee, Wis.) using single-shotfast spin-echo (SSFSE) sequences and spin-echo T1-weighted (T1-W) images in the axial, coronal and sagittalplanes. The SSFSE parameters were: TR/TE 1,522/91 mswith fat saturation and a slice width/gap of 4/1 mm. TheT1-W imaging parameters were: TR/TE 620/14 ms with anidentical slice prescription. Echoplanar DWI were obtainedwith TR/TE 10,000/123 ms with a B value of 1,000 s/mm2,also with an identical slice prescription. Apparent diffusioncoefficient (ADC) images were calculated by the vendor’ssoftware. MRI showed an enlarged dysmorphic leftcerebral hemisphere with abnormal sulcation. The frontallobe of the affected hemisphere showed T1 and T2shortening as well as restricted diffusion on DWI withcorresponding decreased ADC values (Fig. 1).
The patient was offered a termination, but refused onreligious grounds.
R. Agid (*) . S. Lieberman . J. M. GomoriDivision of Neuroradiology, Department of Radiology,Hadassah University Hospital,Kiryat Hadassah, Ein-Karem,P.O. Box 12000 Jerusalem, Israele-mail: [email protected].: +972-50-7874833Fax: +972-2-6419891
M. NadjariDepartment of Obstetrics and Gynecology,Hadassah University Hospital,Jerusalem, Israel
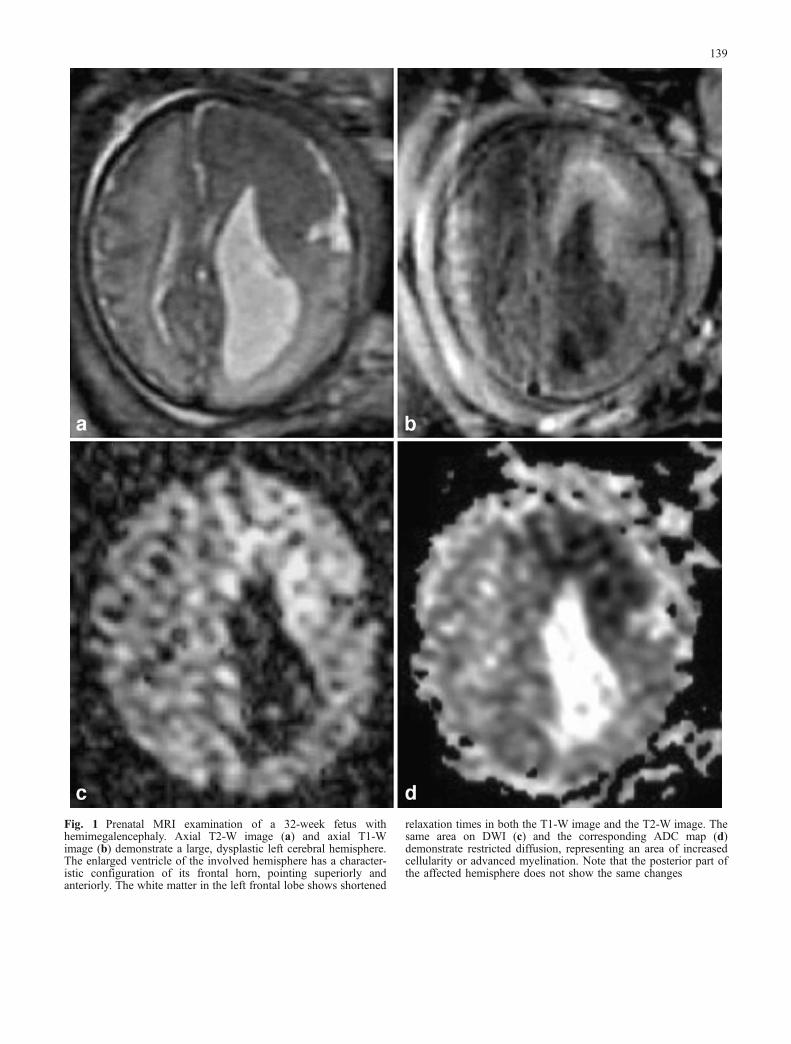
Fig. 1 Prenatal MRI examination of a 32-week fetus withhemimegalencephaly. Axial T2-W image (a) and axial T1-Wimage (b) demonstrate a large, dysplastic left cerebral hemisphere.The enlarged ventricle of the involved hemisphere has a character-istic configuration of its frontal horn, pointing superiorly andanteriorly. The white matter in the left frontal lobe shows shortened
relaxation times in both the T1-W image and the T2-W image. Thesame area on DWI (c) and the corresponding ADC map (d)demonstrate restricted diffusion, representing an area of increasedcellularity or advanced myelination. Note that the posterior part ofthe affected hemisphere does not show the same changes
139

Discussion
MRI diffusion images provide information on the mobilityof water molecules in tissues [5]. It is a widely accepted andutilized method for detecting acute ischaemic brain injury[5, 6]. During the early stage of arterial stroke, highlymobile extracellular water shifts into the intracellularcompartment generating cytotoxic oedema. Movement ofwater is more restricted in the intracellular environment,resulting in hyperintensity on DWI with low ADC values.Indeed, decreased ADC values reflect intracellular oedemaand increased ADC values correspond to an increase in theextracellular space (vasogenic oedema). Water diffusion inbiological tissue is highly dependent on the ratio ofextracellular to intracellular space [7, 8], and is greater inthe extracellular space than in the intracellular space [5].
Recent DWI findings of restricted diffusion in severalforms of viral encephalitis, such as West Nile virus andJapanese encephalitis, suggest cytotoxic oedema [9, 10].Later phase imaging shows higher ADC values indicatingconversion from cytotoxic to vasogenic oedema. A trans-membrane Na+/K+ pump malfunction, as seen in patientswith ischaemic stroke, is a viable explanation for diffusionrestriction in encephalitic conditions [6]. Alternatively, thepathophysiology of these encephalitides leading to re-stricted diffusion may be the result of brain infiltration byinflammatory cells leading to an increase in cellularity oftissue. This concept is similar to that proposed for lowADC values in highly cellular brain tumours, such aslymphoma [11]. Acute demyelination may rarely showrestricted diffusion, probably due to dense inflammatorycell infiltration with scant tissue destruction [12].
While no increase in intracellular water has been shownin hemimegalencephaly on pathological examination [13],it does demonstrate that the affected hemisphere containsareas of giant neurons, an increased nucleus-to-cell ratio,an increased number and size of astrocytes, and an increasein the number of glial cells [1, 14]. These findings amountto an increase in overall cellularity of the megalencephalictissue, and thus may cause restricted diffusion.
In addition, the normal myelination in the newbornreduces water motion in the developing brain [15]. Thewhite matter of hemimegalencephalic hemispheres showsadvanced myelination for age on MRI [16]. This earlymyelination is therefore another possible mechanism forthe restriction of water diffusion in hemimegalencephaly.
The shortening of T1 and T2 in the frontal portion of theaffected hemisphere in the case presented here, togetherwith water restriction in the same area, does not fitischaemic cytotoxic oedema, but supports either increasedcellularity or advanced myelination as the mechanismsresponsible for restricted diffusion in hemimegalencephaly.Alternatively, a combination of both mechanisms may beresponsible.
The signal changes and restriction of water diffusion wasseen only in part of the megalencephalic hemisphere in ourcase (frontal lobe). Prenatal MRI analysis of more fetuses isneeded in order to determine whether the extent of these
changes might be an indicator of the severity of clinicaloutcome in this dysplasia.
In conclusion, hemimegalencephalic hemispheres mayshow restricted diffusion on prenatal MR imaging inparallel to T1 and T2 shortening. These findings may resultfrom a combination of increased cellularity and advancedmyelination in the affected hemisphere. Restricted diffu-sion is an additional valuable indicator in the analysis of thefetal brain.
References
1. Barkovich AJ, Kuzniecky RI (1996) Neuroimaging of focalmalformations of cortical development. J Clin Neurophysiol13:481–494
2. Flores-Sarnat L (2002) Hemimegalencephaly: part 1. Genetic,clinical, and imaging aspects. J Child Neurol 17:373–384;discussion 384
3. Malinger G, Ben-Sira L, Lev D, et al (2004) Fetal brainimaging: a comparison between magnetic resonance imagingand dedicated neurosonography. Ultrasound Obstet Gynecol23:333–340
4. Nishimaki S, Endo M, Seki K, et al (2004) Hemimegalence-phaly misdiagnosed as a congenital brain tumor by fetalcerebral ultrasonography. Prenat Diagn 24:257–259
5. Le Bihan D, Breton E, Lallemand D (1986) MR imaging ofintravoxel incoherent motions: application to diffusion andperfusion in neurologic disorders. Radiology 161:401–408
6. Provenzale JM, Sorensen AG (1999) Diffusion-weighted MRimaging in acute stroke: theoretic considerations and clinicalapplications. AJR 173:1459–1467
7. Stejskal E, Tanner J (1965) Spin diffusion measurements: spinechoes in the presence of a time dependent field gradient. JChem Phys 42:288–292
8. Latour LL, Svoboda K, Mitra PP, et al (1994) Time-dependentdiffusion of water in a biological model system. Proc Natl AcadSci U S A 91:1229–1233
9. Agid R, Ducreux D, Halliday WC, et al (2003) MR diffusion-weighted imaging in a case of West Nile virus encephalitis.Neurology 61:1821–1823
10. Kalita J, Misra UK (2000) Comparison of CT scan and MRIfindings in the diagnosis of Japanese encephalitis. J Neurol Sci174:3–8
11. Stadnik TW, Chaskis C, Michotte A, et al (2001) Diffusion-weighted MR imaging of intracerebral masses: comparisonwith conventional MR imaging and histologic findings. AJNR22:969–976
12. Rovira A, Pericot I, Alonso J, et al (2002) Serial diffusion-weighted MR imaging and proton MR spectroscopy of acutelarge demyelinating brain lesions: case report. AJNR 23:989–994
13. Manz HJ, Phillips TM, Rowden G, et al (1979) Unilateralmegalencephaly, cerebral cortical dysplasia, neuronal hypertro-phy, and heterotopia: cytomorphometric, fluorometric cyto-chemical, and biochemical analyses. Acta Neuropathol (Berl)45:97–103
14. Townsend JJ, Nielsen SL, Malamud N (1975) Unilateralmegalencephaly: hamartoma or neoplasm? Neurology 25:448–453
15. Zhang L, Thomas KM, Davidson MC, et al (2005) MRquantitation of volume and diffusion changes in the developingbrain. AJNR 26:45–49
16. Yagishita A, Arai N, Tamagawa K, et al (1998) Hemimega-lencephaly: signal changes suggesting abnormal myelination onMRI. Neuroradiology 40:734–738
140





























