Embed Size (px)
Citation preview

Introduction
Arachnoid cysts are a rare central nervous system malfor-mation, representing only 1% of all intracranial masses innewborns [1]. Primary (congenital) arachnoid cysts arebenign accumulation of clear fluid between the dura andthe brain substance throughout the cerebrospinal axis inrelation to the arachnoid membrane and do not com-municate with the subarachnoid space [2]. Secondary(acquired) arachnoid cysts result from hemorrhage,trauma, and infection and usually communicate withthe subarachnoid space [1,3]. The common locations ofarachnoid cysts are the surface of the brain at the levelof main brain fissures, such as sylvian, rolandic and inter-hemispheric fissures, sella turcica, the anterior cranialfossa, and the middle cranial fossa [4]. Arachnoid cysts
may be associated with ventriculomegaly and dysgenesisof corpus callosum [5]. Prenatal ultrasound and mag-netic resonance imaging (MRI) have led to the increaseddiagnosis of central nervous system abnormalities ofthe fetuses (Figures 1–8: page 193–197, cases 1–3).
Prenatal Diagnosis
Fetal arachnoid cysts can be evaluated prenatally byultrasound and/or MRI [5–21]. To date, at least 27cases of fetal arachnoid cysts have been reported(Table). Among these, 9 cases had prenatal MRI evalu-ation in addition to ultrasound. The arachnoid cystcan appear as a hypoechoic lesion on prenatal ultra-sound. Most of fetal arachnoid cysts were first diag-nosed in the third trimester. In a few cases, the diagnosiswas made in the second trimester. Bretelle et al [18]reported the first-trimester diagnosis of a posterior fossaarachnoid cyst at 13 gestational weeks by transvaginalsonographic examination. The majority of arachnoidcysts are supratentorial with sylvian fissure cysts being
Taiwan J Obstet Gynecol • September 2007 • Vol 46 • No 3 187
PRENATAL DIAGNOSIS OF ARACHNOID CYSTS
Chih-Ping Chen*
Department of Obstetrics and Gynecology, Mackay Memorial Hospital, Taipei, and Department of Biotechnology, Asia University, Taichung, Taiwan.
SUMMARY
Arachnoid cysts are a rare central nervous system malformation, representing only 1% of all intracranial massesin newborns. Primary (congenital) arachnoid cysts are benign accumulation of clear fluid between the dura andthe brain substance throughout the cerebrospinal axis in relation to the arachnoid membrane and do not com-municate with the subarachnoid space. Secondary (acquired) arachnoid cysts result from hemorrhage, trauma,and infection and usually communicate with the subarachnoid space. The common locations of arachnoidcysts are the surface of the brain at the level of main brain fissures, such as sylvian, rolandic and interhemi-spheric fissures, sella turcica, the anterior cranial fossa, and the middle cranial fossa. Arachnoid cysts may beassociated with ventriculomegaly and dysgenesis of corpus callosum. Prenatal ultrasound and magnetic resonanceimaging have led to the increased diagnosis of fetal arachnoid cysts. This article provides a thorough review of fetalarachnoid cysts, including prenatal diagnosis, differential diagnosis and associated chromosomal abnormalities,as well as comprehensive illustrations of perinatal imaging findings of fetal arachnoid cysts. Prenatal diagnosisof intracranial hypoechoic lesions should include a differential diagnosis of arachnoid cysts and prompt geneticinvestigations. [Taiwan J Obstet Gynecol 2007;46(3):187–198]
Key Words: arachnoid cysts, MRI, prenatal diagnosis, ultrasound
*Correspondence to: Dr Chih-Ping Chen, Department ofObstetrics and Gynecology, Mackay Memorial Hospital, 92,Section 2, Chung-Shan North Road, Taipei 104, Taiwan.E-mail: [email protected]: June 28, 2007
■ REVIEW ARTICLE ■

Taiwan J Obstet Gynecol • September 2007 • Vol 46 • No 3188
C.P. Chen
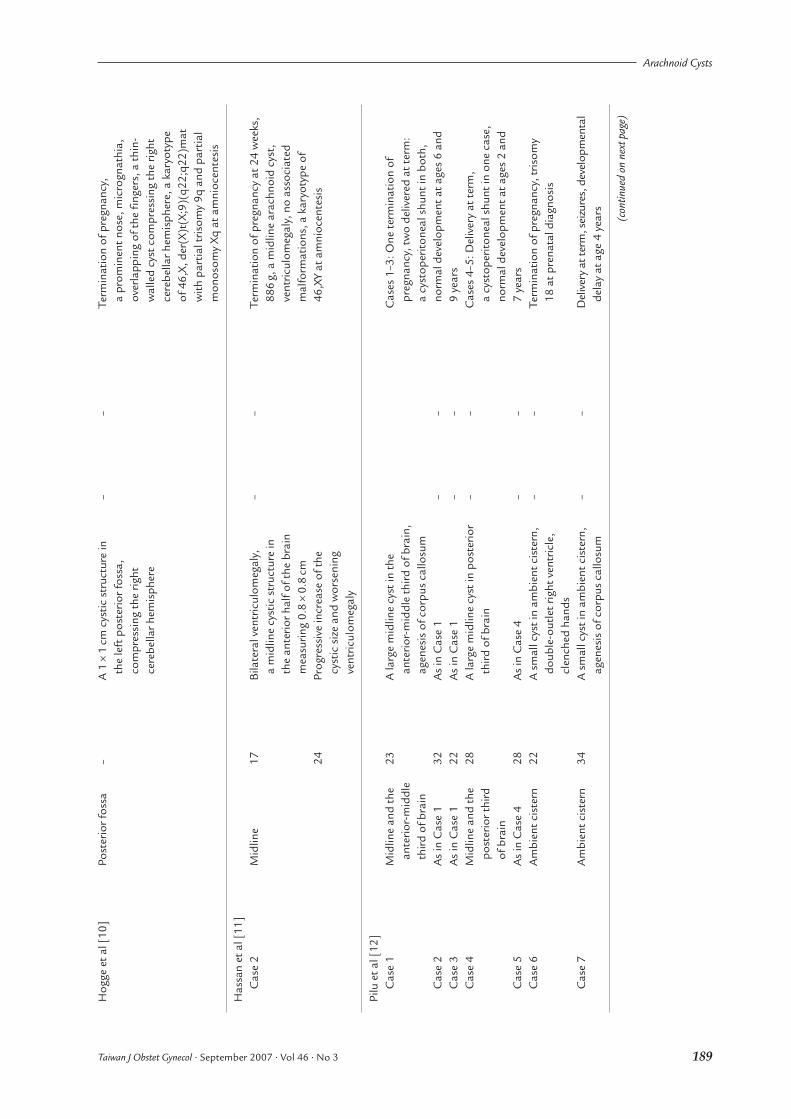
Tabl
e.R
epor
ted
case
s of
feta
l ara
chno
id c
ysts
dia
gnos
ed b
y ul
tras
ound
and
/or m
agne
tic r
eson
ance
imag
ing
(MR
I)
GW
at
GW
at
Pren
atal
MR
IA
utho
rspr
enat
alSo
nogr
aphi
c pr
enat
al M
RI
find
ings
inPe
rinat
al o
utco
me
[Ref
eren
ce]
Loca
tion
sono
grap
hic
find
ings
diag
nosi
sad
ditio
n to
cys
tdi
agno
sis
Dia
koum
akis
et a
l [6]
Supr
asel
lar
32
A 3
.5cm
sup
rase
llar c
ystic
–
–Va
gina
l del
iver
y at
37
wee
ks, 2
,654
g,
mas
sa
4.3
cm s
upra
sella
r ara
chno
id c
yst
35A
4cm
sup
rase
llar a
rach
noid
w
ith h
ydro
ceph
alus
, a s
olit
ary
seiz
ure
–cy
st w
ith h
ydro
ceph
alus
at a
ge 3
day
s, a
cys
tope
riton
eal s
hunt
at
age
19
days
Mei
zner
et a
l [7]
Parie
to-o
ccip
ital
22A
3.3
×3.
4cm
cys
tic m
ass
in
––
Vagi
nal d
eliv
ery
at 3
9 w
eeks
, 3,4
00g,
the
right
par
ieto
-occ
ipit
al lo
be
a 6
×7
cm a
rach
noid
cys
t, n
o of
the
brai
n, n
o hy
droc
epha
lus
hydr
ocep
halu
s, n
o de
fici
t or s
eizu
res,
38En
larg
emen
t of t
he c
yst u
p to
lo
st to
follo
w-u
p5
×4
cm
Ram
an e
t al [
8]Po
ster
ior f
ossa
24A
7.8
×9.
6cm
pos
terio
r cra
nial
–
–C
esar
ean
sect
ion
at 3
8 w
eeks
, 3,5
00g,
fo
ssa
cyst
, dila
tion
of th
e th
irda
post
erio
r fos
sa a
rach
noid
cys
t,
vent
ricle
vent
ricul
omeg
aly,
cys
tope
riton
eal a
ndve
ntric
ulop
erito
neal
shu
nts,
rec
urre
ntse
izur
es, d
eath
at a
ge 2
.5 m
onth
s
Lang
er e
t al [
9]C
ase
1Su
prat
ento
rial,
25A
3.0
×2.
2cm
ane
choi
c –
–Va
gina
l del
iver
y at
40
wee
ks, 3
,620
g,
mid
dle
cran
ial
supr
aten
toria
l mas
s w
ithin
the
an a
rach
noid
cys
t in
the
mid
dle
cran
ial
foss
arig
ht p
arie
to-o
ccip
ital
lobe
foss
a an
d rig
ht p
arie
to-o
ccip
ital
lobe
, 28
A s
light
incr
ease
in th
e di
amet
er
––
hydr
ocep
halu
s, a
cys
tope
riton
eal
of th
e cy
st (
4cm
),
shun
t at a
ge 2
mon
ths,
nor
mal
no
ven
tric
ulom
egal
yde
velo
pmen
t at a
ge 1
8 m
onth
sC
ase
2Su
prat
ento
rial,
32A
6cm
sup
rate
ntor
ial a
rach
noid
–
–C
esar
ean
sect
ion
at 4
0 w
eeks
, 3,0
80g,
m
idlin
ecy
st in
the
mid
line,
a
supr
asel
lar a
rach
noid
cys
t, m
ild
vent
ricul
ar d
ilatio
nve
ntric
ular
dila
tion,
cys
tope
riton
eal
and
vent
ricul
oper
itone
al s
hunt
s at
age
8 d
ays,
nor
mal
dev
elop
men
t at
age
20
days
Taiwan J Obstet Gynecol • September 2007 • Vol 46 • No 3 189
Arachnoid Cysts
Hog
ge e
t al [
10]
Post
erio
r fos
sa–
A 1
×1
cm c
ystic
str
uctu
re in
–
–Te
rmin
atio
n of
pre
gnan
cy,
the
left
pos
terio
r fos
sa,
a pr
omin
ent n
ose,
mic
rogn
athi
a,
com
pres
sing
the
right
ov
erla
ppin
g of
the
fing
ers,
a th
in-
cere
bella
r hem
isph
ere
wal
led
cyst
com
pres
sing
the
right
ce
rebe
llar h
emis
pher
e, a
kar
yoty
pe
of 4
6,X,
der
(X)t
(X;9
)(q2
2;q2
2)m
atw
ith p
artia
l tris
omy
9q a
nd p
artia
lm
onos
omy
Xq a
t am
nioc
ente
sis
Has
san
et a
l [11
]C
ase
2M
idlin
e17
Bila
tera
l ven
tric
ulom
egal
y,
––
Term
inat
ion
of p
regn
ancy
at 2
4 w
eeks
, a
mid
line
cyst
ic s
truc
ture
in
886
g, a
mid
line
arac
hnoi
d cy
st,
the
ante
rior h
alf o
f the
bra
in
vent
ricul
omeg
aly,
no
asso
ciat
ed
mea
surin
g 0.
8×
0.8
cmm
alfo
rmat
ions
, a k
aryo
type
of
24Pr
ogre
ssiv
e in
crea
se o
f the
46
,XY
at a
mni
ocen
tesi
scy
stic
siz
e an
d w
orse
ning
ve
ntric
ulom
egal
y
Pilu
et a
l [12
]C
ase
1M
idlin
e an
d th
e 23
A la
rge
mid
line
cyst
in th
e C
ases
1–3
: One
ter
min
atio
n of
an
terio
r-m
iddl
e an
terio
r-m
iddl
e th
ird o
f bra
in,
preg
nanc
y, tw
o de
liver
ed a
t ter
m:
third
of b
rain
agen
esis
of c
orpu
s ca
llosu
ma
cyst
oper
itone
al s
hunt
in b
oth,
C
ase
2A
s in
Cas
e 1
32A
s in
Cas
e 1
––
norm
al d
evel
opm
ent a
t age
s 6
and
Cas
e 3
As
in C
ase
122
As
in C
ase
1–
–9
year
sC
ase
4M
idlin
e an
d th
e 28
A la
rge
mid
line
cyst
in p
oste
rior
––
Cas
es 4
–5: D
eliv
ery
at t
erm
, po
ster
ior t
hird
th
ird o
f bra
ina
cyst
oper
itone
al s
hunt
in o
ne c
ase,
of
bra
inno
rmal
dev
elop
men
t at a
ges
2 an
d C
ase
5A
s in
Cas
e 4
28A
s in
Cas
e 4
––
7 ye
ars
Cas
e 6
Am
bien
t cis
tern
22A
sm
all c
yst i
n am
bien
t cis
tern
, –
–Te
rmin
atio
n of
pre
gnan
cy, t
risom
y do
uble
-out
let r
ight
ven
tric
le,
18 a
t pre
nata
l dia
gnos
iscl
ench
ed h
ands
Cas
e 7
Am
bien
t cis
tern
34A
sm
all c
yst i
n am
bien
t cis
tern
, –
–D
eliv
ery
at te
rm, s
eizu
res,
dev
elop
men
tal
agen
esis
of c
orpu
s ca
llosu
mde
lay
at a
ge 4
yea
rs (con
tinue
d on
nex
t pag
e)

Taiwan J Obstet Gynecol • September 2007 • Vol 46 • No 3190
C.P. Chen
Tabl
e.(c
ontin
ued)
GW
at
GW
at
Pren
atal
MR
IA
utho
rspr
enat
alSo
nogr
aphi
c pr
enat
al M
RI
find
ings
inPe
rinat
al o
utco
me
[Ref
eren
ce]
Loca
tion
sono
grap
hic
find
ings
diag
nosi
sad
ditio
n to
cys
tdi
agno
sis
Raf
fert
y et
al [
13]
Mid
dle
cran
ial
33M
acro
ceph
aly,
righ
t–
–C
esar
ean
sect
ion
at 3
9 w
eeks
, fo
ssa
vent
ricul
omeg
aly,
a 5
cm
an e
ndos
copi
c fe
nest
ratio
n of
the
mid
dle
cran
ial f
ossa
cy
st o
n da
y 1,
nor
mal
dev
elop
men
t ar
achn
oid
cyst
at a
ge 6
mon
ths
Levi
ne e
t al [
14]
Cas
e 1
–22
An
arac
hnoi
d cy
st–
Part
ial a
gene
sis
–31
of c
orpu
s ca
llosu
m w
ith
abse
nt b
ody
and
sple
nium
Cas
e 2
Mid
line
20A
mid
line
arac
hnoi
d cy
st–
Nor
mal
cor
pus
–ca
llosu
m th
at
was
not
vi
sual
ized
by
sono
grap
hyC
ase
3–
26A
larg
e ar
achn
oid
cyst
–Ex
tent
of m
ass
–27
effe
ct o
n 33
surr
ound
ing
36st
ruct
ures
Elbe
rs a
nd F
urne
ss [
15]
Supr
aten
toria
l18
.5A
larg
e m
idlin
e ar
achn
oid
cyst
––
Ces
area
n se
ctio
n at
38
wee
ks, n
orm
al
30D
ecre
ase
of th
e cy
st s
ize
deve
lopm
ent a
t age
2 y
ears
32C
ompl
ete
reso
lutio
n of
the
cyst
Bla
iche
r et a
l [5]
Cas
e 1
Left
-tem
pora
l, 39
A 6
×3.
8×
2.4
cm h
ypoe
choi
c 39
A p
eris
ylvi
an
Elec
tive
cesa
rean
sec
tion,
3,4
95g,
pe
risyl
vian
hom
ogen
eous
lesi
on in
the
arac
hnoi
d cy
st
no n
euro
logi
cal a
bnor
mal
ity, n
orm
al
left
par
ieta
l hem
isph
ere
with
no
deve
lopm
ent a
t age
6 m
onth
sco
mpr
essi
on
of s
urro
undi
ngst
ruct
ures
Cas
e 2
Third
ven
tric
le34
3×
5×
1.2
cm a
sym
met
ric
34C
allo
sal
Ces
area
n se
ctio
n at
39
wee
ks, 3
,300
g,

Taiwan J Obstet Gynecol • September 2007 • Vol 46 • No 3 191
Arachnoid Cysts
hypo
echo
ic h
omog
eneo
us
dysg
enes
is,
repe
ated
apn
eas
and
gene
raliz
ed
lesi
on in
the
third
ven
tric
le
norm
al fa
lx
seiz
ures
, ant
icon
vuls
ive
ther
apy
with
se
para
ting
the
basa
l gan
glia
, ce
rebr
i, co
rtic
al
phen
ytoi
n, s
light
ly a
bnor
mal
m
ild b
ilate
ral d
ilatio
n of
pa
tter
n,
deve
lopm
ent a
t age
5 m
onth
s w
ith
the
post
erio
r hor
nsce
rebe
llum
, di
min
ishe
d he
ad c
ontr
ol a
nd r
educ
ed
basa
l gan
glia
vi
sual
fix
atio
nan
d br
ain
stem
Gol
ash
et a
l [16
]Su
pras
ella
r17
A 2
.5cm
mid
line
cyst
ic le
sion
28Sl
ight
dila
tion
Elec
tive
cesa
rean
sec
tion
at 3
8 w
eeks
, 24
Cys
t siz
e 3.
2cm
of th
e oc
cipi
tal
vent
ricul
omeg
aly
and
mac
roce
phal
y,
28C
yst s
ize
3.2
cmho
rns
of th
e en
dosc
opic
cys
tove
ntric
ulos
tom
y la
tera
l an
d cy
stoc
iste
rnos
tom
y, n
orm
al
vent
ricle
sde
velo
pmen
t at a
ge 2
yea
rs
Nak
amur
a et
al [
17]
Prep
ontin
e-28
Mac
roce
phal
y, e
nlar
ged
28A
sup
ra a
nd
Vagi
nal d
eliv
ery
at 3
5 w
eeks
, su
pras
ella
rve
ntric
les
and
a m
idlin
e in
frat
ento
rial
impl
emen
tatio
n of
a c
yst-
perit
onea
l cy
stic
lesi
onfo
ssae
cys
t sh
unt o
n da
y 18
, end
osco
pic
com
pres
sing
cy
stov
entr
icul
osto
my
at a
ge
the
brai
n st
em2
mon
ths,
a 1
-mon
th d
elay
of
deve
lopm
ent a
t age
4 m
onth
s
Bre
telle
et a
l [18
]Po
ster
ior f
ossa
13A
n an
echo
ic m
ass
abov
e th
e –
–Te
rmin
atio
n at
15
wee
ks, 1
03g,
po
ster
ior f
ossa
and
bet
wee
n ka
ryot
ype
46,X
Y, a
pos
terio
r med
ian
the
two
occi
pita
l lob
esar
achn
oid
cyst
, no
othe
r ano
mal
ies
Sout
er e
t al [
19]
Cas
e 2
Mid
line
25Te
tral
ogy
of F
allo
t–
–C
esar
ean
sect
ion
at 3
7 w
eeks
, 1,9
61g,
34IU
GR
, a 1
.8×
2.0
cm m
idlin
e fa
cial
dys
mor
phis
m, i
ngui
nal h
erni
as,
intr
acra
nial
ara
chno
id c
yst,
te
tral
ogy
of F
allo
t with
a la
rge
post
erio
r and
sup
erio
r to
over
ridin
g ao
rta,
MR
I con
firm
ed
the
thal
ami
a 2
×1.
1×
1.2
cm m
idlin
e ar
achn
oid
cyst
, mar
ked
glob
al d
evel
opm
enta
l de
lay
at a
ge 1
3 m
onth
s, a
pos
tnat
al
kary
otyp
e of
46,
XY,d
er(1
4)t(
14;2
0)
(q32
.2;p
13)
with
a s
ubte
lom
eric
de
letio
n of
the
dist
al lo
ng a
rm o
f ch
rom
osom
e 14
. (con
tinue
d on
nex
t pag
e)

Taiwan J Obstet Gynecol • September 2007 • Vol 46 • No 3192
C.P. Chen
Tabl
e.(c
ontin
ued)
GW
at
GW
at
Pren
atal
MR
IA
utho
rspr
enat
alSo
nogr
aphi
c pr
enat
al M
RI
find
ings
inPe
rinat
al o
utco
me
[Ref
eren
ce]
Loca
tion
sono
grap
hic
find
ings
diag
nosi
sad
ditio
n to
cys
tdi
agno
sis
Kus
aka
et a
l [20
]Q
uadr
igem
inal
30
An
anec
hoic
mas
s in
the
31N
o ob
liter
atio
n N
orm
al v
agin
al d
eliv
ery,
no
cist
ern
quad
rigem
inal
cis
tern
of
the
cere
bral
hy
droc
epha
lus
at a
ge 1
yea
rw
ithou
t hyd
roce
phal
usaq
uedu
ct, n
o co
mm
unic
atio
nbe
twee
n th
e ve
ntric
ular
syst
em a
ndth
e cy
st
Fujim
ura
et a
l [21
]Su
pras
ella
r25
A 3
-cm
mid
line
cyst
ic le
sion
, 28
Con
firm
atio
n of
Va
gina
l del
iver
y at
37
wee
ks, 2
,844
g,
no v
entr
icul
omeg
aly
a su
pras
ella
r en
dosc
opic
cys
tove
ntric
ulos
tom
y at
ar
achn
oid
cyst
age
5 m
onth
s, n
orm
al d
evel
opm
ent
at a
ge 3
yea
rs
GW
=ge
stat
iona
l wee
ks; –
= no
info
rmat
ion;
IUG
R =
intr
aute
rine
grow
th re
stric
tion.

the most common. Arachnoid cysts may progressivelyenlarge in utero, causing ventriculomegaly. Elbers andFurness [15] reported an unusual case of presumedarachnoid cyst diagnosed at 18.5 weeks’ gestation.The cyst resolved at 32 weeks’ gestation. Serial prena-tal sonographic examinations are able to assess thesize of the cyst and the ventricles. Prenatal MRI helpsto demonstrate the anatomic details of other centralnervous system abnormalities, such as compression ofthe aqueduct, communication between the cyst andthe ventricles, and corpus callosum dysgenesis.
Differential Diagnosis
Prenatal diagnosis of intracranial hypoechoic cysticlesions should include a differential diagnosis of arach-noid cysts, porencephalic cysts, glioependymal cysts,choroid plexus cysts, aneurysms of the vein of Galen,schizencephaly, cystic neoplasms, and intracranialhemorrhage [12].
Taiwan J Obstet Gynecol • September 2007 • Vol 46 • No 3 193
Arachnoid Cysts
Figure 1. Prenatal ultrasound of an arachnoid cyst of case 1.Prenatal ultrasound at 32 weeks’ gestation revealed a 5.39 ×3.94 cm midline interhemispheric hypoechoic homogeneouslesion. Magnetic resonance imaging (MRI) at 33 gestationalweeks showed a left interhemispheric arachnoid cyst, markeddysgenesis of the corpus callosum, and colpocephaly. The kary-otype was 46,XY. A 2,788-g male baby was delivered at 37weeks’ gestation. Postnatal MRI confirmed the prenatal diag-nosis. A cystoperitoneal shunt was performed at age 7 months.The infant was doing well at age 1 year and 2 months.
A
C
B
Figure 2. (A) Sagittal, (B) axial and (C) coronalviews of magnetic resonance imaging of case 1 at33 weeks’ gestation.

Porencephalic cystsPorencephalic cysts are usually unilateral and communi-cate with the ventricular system with a cavity lined withwhite matter. Porencephalic cysts result from infarc-tion of the brain secondary to vascular insults, trauma,infection, hemorrhage, or monochorionic monozygotictwin–twin transfusion. In contrast, arachnoid cysts areusually asymmetric and smooth-walled; they do notcommunicate with the ventricular system and have amass effect.
Glioependymal cystsGlioependymal cysts are usually multilocular and locatedwithin the brain parenchyma. Glioependymal cysts havean ependymal lining, whereas, arachnoid cysts have
fibrous walls. Glioependymal cysts may have a masseffect and are often associated with agenesis of thecorpus callosum.
Choroid plexus cystsChoroid plexus cysts, unilateral or bilateral, are fre-quently detected in the second trimester. Choroid plexuscysts are sonolucent cysts within the choroids plexusof the lateral ventricle. Large choroid plexus cysts maybe associated with trisomy 18.
Aneurysms of the vein of GalenAneurysms of the vein of Galen are vascular anomaliesof the vein of Galen located in the brain deeply andposteriorly to the thalami and in the subarachnoidspace. Color Doppler is helpful for the diagnosis ofaneurysms of the vein of Galen. Prenatal sonographicdetection of fluid-filled lesions in the posterior third of the brain, which are found in association withhydrops fetalis, ventriculomegaly, porencephaly, singleumbilical artery, chorioangioma or limb reductiondefects, should raise the suspicion of aneurysms of thevein of Galen.
SchizencephalySchizencephaly or true porencephaly is characterizedby unilateral, asymmetric or bilateral congenital full-thickness clefts of the cerebral mantle. Schizencephalymay or may not communicate with the ventricular sys-tem and are lined by gray matter. Schizencephaly canbe associated with ventriculomegaly, polymicrogyria,heterotopias, agenesis of the corpus callosum, absentseptum pellucidum, and optic nerve hypoplasia.
Cystic neoplasmsCystic neoplasms, such as cystic teratoma and cysticastrocytoma, consist of solid and irregular cystic com-ponents and have a mass effect.
Taiwan J Obstet Gynecol • September 2007 • Vol 46 • No 3194
C.P. Chen
A B
Figure 3. (A) Sagittal and (B) axial views of postnatal magnetic resonance imaging of case 1 at age 3 days.
Figure 4. Prenatal ultrasound of an arachnoid cyst of case 2.Prenatal ultrasound of case 2 at 31 weeks’ gestation revealeda 1.97 × 2.87 cm left interhemispheric hypoechoic homoge-neous lesion. Magnetic resonance imaging (MRI) at 32 weeks’gestation showed a left interhemispheric arachnoid cyst andcolpocephaly. A 2,620-g male baby was delivered at term.Postnatal MRI confirmed the prenatal diagnosis. The size ofthe arachnoid cyst was measured about 6.81 × 3.71 cm.There was a left-to-right midline shift. A cystoperitonealshunt was performed at age 8 months. The child was doingwell at age of 3 years and 4 months.

Intracranial hemorrhageIntracranial hemorrhage usually occurs in the subependy-mal germinal matrix region and is associated withhypoxia, platelet disorders, coagulopathy, alterationsin cerebral blood pressure in the case of twin–twintransfusion or demise of a monozygotic co-twin, feto-maternal hemorrhage, and maternal medications. Intra-cranial hemorrhage may initially present echogenicblood clots in the ventricles and subsequently lead toventricular dilation.
Chromosomal Abnormalities Associatedwith Congenital Arachnoid Cysts
Fetal arachnoid cysts can be associated with chromo-somal abnormalities. Therefore, prenatal diagnosis of anarachnoid cyst, especially in association with structuralabnormalities, should prompt a cytogenetic investiga-tion. Various associated chromosomal abnormalitieshave been reported. For instance, Hogge et al [10]reported partial trisomy 9q (9q22 � qter) and partialmonosomy Xq (Xq22�qter) in a fetus with an infraten-torial arachnoid cyst. The fetus postnatally manifested
a prominent nose, micrognathia, overlapping of thefingers, and a thin-walled cyst compressing the rightcerebellar hemisphere. Souter et al [19] reported asubtelomeric deletion of the distal long arm of chro-mosome 14, i.e. monosomy 14q (14q32.3 � qter), in a fetus with tetralogy of Fallot, intrauterine growthrestriction, and a midline intracranial arachnoid cyst.The infant postnatally manifested facial dysmorphism,inguinal hernias, tetralogy of Fallot, a midline arach-noid cyst, and marked global developmental delay. Piluet al [12] reported trisomy 18 in a fetus with a smallarachnoid cyst in the ambient cistern, a double-outletright ventricle, and clenched hands. Elbers and Furness[15] additionally reported their experience of the asso-ciation of triploidy with a fetus with an arachnoid cyst.
Fetal Outcome
The prognosis of fetal arachnoid cysts is dependent onthe presence or absence of the corpus callosum, thepresence or absence of other congenital malformations,parenchymal hemorrhages, the rate of the growth ofthe cyst, and progression of ventriculomegaly. Fetal
Taiwan J Obstet Gynecol • September 2007 • Vol 46 • No 3 195
Arachnoid Cysts
A
C
B
Figure 5. (A) Sagittal, (B) axial and (C) coronalviews of magnetic resonance imaging of case 2at 32 weeks’ gestation.

arachnoid cysts without associated structural anomaliesor chromosomal abnormalities can have a favorableoutcome. In some cases with rapid progression of thelesion and ventriculomegaly, appropriate pediatric sur-gical therapy may be required in early infancy. Currently,postnatal endoscopic cystoventriculostomy and cysto-cisternostomy have become less invasive surgical alter-natives [16,17,21]. The prognosis of fetal intracranialcysts has been shown to rely on the brain integrityrather than the cyst volume or location [22]. Therefore,in order to establish the correct prognosis and intellec-tual outcome of fetuses with arachnoid cysts, MRI is animportant adjunct to ultrasound and helps to optimizeneonatal management by accurate determination ofthe fetal anatomy and objective perinatal counseling.
Conclusion
This article provides a thorough review of fetal arachnoidcysts, including prenatal diagnosis, differential diagnosisand associated chromosomal abnormalities, as well as
Taiwan J Obstet Gynecol • September 2007 • Vol 46 • No 3196
C.P. Chen
A
C
B
Figure 6. (A) Sagittal, (B) axial and (C) coronalviews of postnatal magnetic resonance imaging ofcase 2.
Figure 7. Prenatal ultrasound of an arachnoid cyst of case 3.Prenatal ultrasound of case 3 at 23 weeks’ gestation revealeda 1.45 × 3.03 cm midline interhemispheric hypoechoic homo-geneous lesion. The karyotype was 46,XY. Magnetic resonanceimaging (MRI) at 24 weeks’ gestation showed an interhemi-spheric arachnoid cyst and dysgenesis of the corpus callosum.Progression of the cyst was noted in late gestation. A 2,350-gmale baby was delivered prematurely at 28 weeks’ gestation.Postnatal MRI confirmed the prenatal diagnosis. A cysto-peritoneal shunt was performed at age of 1 week. The childwas doing well at age 4 years.

Taiwan J Obstet Gynecol • September 2007 • Vol 46 • No 3 197
Arachnoid Cysts
A
C
B
Figure 8. (A) Sagittal, (B) axial, and (C) coronalviews of magnetic resonance imaging of case 3at 24 weeks’ gestation.
comprehensive illustrations of perinatal imaging find-ings of fetal arachnoid cysts. Prenatal diagnosis ofintracranial hypoechoic lesions should include a differ-ential diagnosis of arachnoid cysts and prompt geneticinvestigations.
References
1. Robinson RG. Congenital cysts of the brain: arachnoidmalformations. Prog Neurol Surg 1971;4:133–74.
2. Pascual-Castroviejo I, Roche MC, Martinez Bermejo A,Arcas J, Garcia Blazquez M. Primary intracranial arach-noidal cysts: a study of 67 childhood cases. Childs Nerv Syst1991;7:257–63.
3. Oliver LC. Primary arachnoid cysts: report of two cases. Br Med J 1958;1:1147–50.
4. Wester K. Peculiarities of intracranial arachnoid cysts: loca-tion, sidedness, and sex distribution in 126 consecutivepatients. Neurosurgery 1999;45:775–9.
5. Blaicher W, Prayer D, Kuhle S, Deutinger J, Bernaschek G.Combined prenatal ultrasound and magnetic resonanceimaging in two fetuses with suspected arachnoid cysts.Ultrasound Obstet Gynecol 2001;18:166–8.
6. Diakoumakis EE, Weinberg B, Mollin J. Prenatal sonographicdiagnosis of a suprasellar arachnoid cyst. J Ultrasound Med1986;5:529–30.
7. Meizner I, Barki Y, Tadmor R, Katz M. In utero ultrasonicdetection of fetal arachnoid cyst. J Clin Ultrasound 1988;16:506–9.
8. Raman S, Rachagan SP, Lim CT. Prenatal diagnosis of a posterior fossa cyst. J Clin Ultrasound 1991;19:434–7.
9. Langer B, Haddad J, Favre R, Frigue V, Schlaeder G. Fetalarachnoid cyst: report of two cases. Ultrasound Obstet Gynecol1994;4:68–72.
10. Hogge WA, Schnatterly P, Ferguson JE 2nd. Early prenataldiagnosis of an infratentorial arachnoid cyst: associationwith an unbalanced translocation. Prenat Diagn 1995;15:186–8.
11. Hassan J, Sepulveda W, Teixeira J, Cox PM. Glioependymaland arachnoid cysts: unusual causes of early ventriculomegalyin utero. Prenat Diagn 1996;16:729–33.
12. Pilu G, Falco P, Perolo A, Sandri F, Cocchi G, Ancora G,Bovicelli L. Differential diagnosis and outcome of fetalintracranial hypoechoic lesions: report of 21 cases. UltrasoundObstet Gynecol 1997;9:229–36.
13. Rafferty PG, Britton J, Penna L, Ville Y. Prenatal diagnosis ofa large fetal arachnoid cyst. Ultrasound Obstet Gynecol 1998;12:358–61.
14. Levine D, Barnes PD, Madsen JR, Abbott J, Mehta T,Edelman RR. Central nervous system abnormalities assessedwith prenatal magnetic resonance imaging. Obstet Gynecol1999;94:1011–9.
15. Elbers SEL, Furness ME. Resolution of presumed arachnoidcyst in utero. Ultrasound Obstet Gynecol 1999;14:353–5.

16. Golash A, Mitchell G, Mallucci C, May P, Pilling D. Prenataldiagnosis of suprasellar arachnoid cyst and postnatalendoscopic treatment. Childs Nerv Syst 2001;17:739–42.
17. Nakamura Y, Mizukawa K, Yamamoto K, Nagashima T.Endoscopic treatment for a huge neonatal prepontine-suprasellar arachnoid cyst: a case report. Pediatr Neurosurg2001;35:220–4.
18. Bretelle F, Senat MV, Bernard JP, Hillion Y, Ville Y. First-trimester diagnosis of fetal arachnoid cyst: prenatal impli-cation. Ultrasound Obstet Gynecol 2002;20:400–2.
19. Souter VL, Glass IA, Chapman DB, Raff ML, Parisi MA,Opheim KE, Disteche CM. Multiple fetal anomalies associated
with subtle subtelomeric chromosomal rearrangements.Ultrasound Obstet Gynecol 2003;21:609–15.
20. Kusaka Y, Luedemann W, Oi S, Shwardfegar R, Samii M.Fetal arachnoid cyst of the quadrigeminal cistern in MRIand ultrasound. Childs Nerv Syst 2005;21:1065–6.
21. Fujimura J, Shima Y, Arai H, Ogawa R, Fukunaga Y. Man-agement of a suprasellar arachnoid cyst identified usingprenatal sonography. J Clin Ultrasound 2006;34:92–4.
22. Pierre-Kahn A, Hanlo P, Sonigo P, Parisot D, McConnell RS.The contribution of prenatal diagnosis to the understandingof malformative intracranial cysts: state of the art. Childs NervSyst 2000;16:619–26.
Taiwan J Obstet Gynecol • September 2007 • Vol 46 • No 3198
C.P. Chen












![A Cystic Mass in the Popliteal Fossa and Its Differential ......[2]. Therefore, surgeons may mistake ganglionic cysts in the popliteal fossa for Baker’s cysts or meniscal cysts](https://img.pdfslide.us/doc/110x75/5f8ba0d5beaa983e540e6dd7/a-cystic-mass-in-the-popliteal-fossa-and-its-differential-2-therefore.jpg)