Embed Size (px)
Citation preview

PRENATAL DIAGNOSISPrenat Diagn 2005; 25: 1084–1087.Published online 17 October 2005 in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/pd.1265
Prenatal detection of deletion 6q13q15 in a complexkaryotype
Min Yu1, Angela C. Obringer2, Melissa H. Fowler1, Marybeth Hummel3 and Sharon L. Wenger1*1Department of Pathology, West Virginia University, Morgantown, USA2Department of Obstetrics and Gynecology, West Virginia University, Morgantown, USA3Department of Pediatrics, West Virginia University, Morgantown, USA
Objectives Prenatal diagnosis of a pregnancy with elevated maternal serum alpha-fetoprotein identifieda karyotype with a complex chromosomal rearrangement, a Robertsonian translocation and a 6q deletioninvolving bands q13q15. Sonography identified mild IUGR, polyhydramnios and micrognathia. The infantpresented with multiple congenital anomalies, primarily limited to the head and neck, including hypertelorism,broad nose, micrognathia, cleft palate, microglossia and low-set ears with microtia.
Methods Amniocytes of the fetus and blood of the patient and her parents were analyzed by cytogeneticsand fluorescence in situ hybridization.
Results The karyotype on the fetus was 45,XX,t(3;21;20)(p12;q11.2;p11.2), del(6)(q13q15),der(13;14)(q10;q10)mat.
Conclusion The 13;14 Robertsonian translocation was inherited from the mother and the three-waytranslocation appeared to be balanced. The patient had facial dysmorphology similar to that which has beendescribed in 6 previously reported cases with the same deletion involving 6q13q15. There was no recognizableabnormality of limbs or digits, and the autopsy did not identify defects involving the internal organs. Copyright 2005 John Wiley & Sons, Ltd.
KEY WORDS: chromosome deletion; inherited Robertsonian translocation; 6q13q15 deletion; complex chromo-somal rearrangement
INTRODUCTION
More than 30 cases with proximal interstitial deletionof 6q have been reported (Gershoni-Baruch et al., 1996;Romie et al., 1996; Hopkin et al., 1997; Kumar et al.,1997; Gilhuis et al., 2000); however, to our knowl-edge, only 6 of these cases have involved only theq13q15 region (McNeal et al., 1977; Young et al., 1985;Yamamoto et al., 1986; Rose et al., 1992; Gershoni-Baruch et al., 1996).
The age of the probands in these 6 cases ranged fromseveral months to 13 years. The anomalies involvedmultiple organ systems, including facial dysmorphia,defects of brain, heart, lung, bone and joint, as wellas developmental delay in all patients. Here we reporta case diagnosed prenatally with a del(6)(q13q15),a complex chromosomal rearrangement involving 3chromosomes and a maternally inherited Robertsoniantranslocation.
CLINICAL REPORT
The female infant was the product of the first preg-nancy of a 22-year-old female. During pregnancy the
*Correspondence to: Sharon L. Wenger, Department of Pathology,West Virginia University, Morgantown, WV 26505, USA.E-mail: [email protected]
mother did not smoke or use drugs, and had no ill-nesses except for a urinary tract infection. The yearprior to her pregnancy, however, the mother had hadthree abdominal CT scans for diagnostic testing. Duringpregnancy, the routine maternal serum triple screeningindicated a 1 in 120 risk for Down syndrome. Amnio-centesis was performed at 25 weeks and amniotic fluidcells were cultured for cytogenetics, identifying a com-plex karyotype, including a three-way translocation, aRobertsonian translocation and a 6q deletion. Kary-otype of the father was 46,XY and the mother was45,XX,der(13;14)(q10;q10). Ultrasonography at the timeof amniocentesis documented polyhydramnios, absentstomach bubble, intrauterine growth retardation, two-vessel cord and distention of the left kidney. A follow-up ultrasound identified micrognathia as well. The fetalechocardiogram at 27 weeks showed no obvious intrac-ardiac pathology. The family elected to continue withthe pregnancy. At 30 weeks, the mother was hospital-ized in preterm labor. Sonography at this time showedpolyhydramnios and micrognathia. The mother receivedmagnesium sulfate tocolysis for several days. When con-tractions occurred again, she received terbutaline. Thefemale infant was born vaginally with vacuum assistanceat 33 1/7 weeks with a birth weight of 1780 g, length43 cm, and head circumference of 32 cm. There wasmeconium staining of the amniotic fluid. APGAR scorewas 4 at both 1 and 5 min due to minimal respiratoryeffort. The infant was bagged with air leaking throughthe ear canals. Intubation was difficult and identified
Copyright 2005 John Wiley & Sons, Ltd. Received: 28 September 2004Revised: 28 September 2004
Accepted: 28 September 2004Published online: 17 October 2005

PRENATAL DETECTION OF DELETION 6Q13Q15 1085
extremely anteriorly placed cords. The infant did not sur-vive despite aggressive resuscitation on the second dayof life. The cytogenetic findings from the amniocyteswere confirmed in a cord blood sample.
On physical examination, the patient had epican-thal folds, mild microphthalmia, hypertelorism, shortnose with inverted nares, micrognathia, cleft palate,microglossia and low-set ears (Figure 1). She was alsohypotonic. Autopsy showed mild left renal pelvis dila-tion without abnormalities of the kidneys, ureter or blad-der. No other internal defects were seen. There was atwo-vessel umbilical cord, and normal placenta. One ofthe maternal aunts is mentally retarded, the remainderof the family history is negative.
MATERIALS AND METHODS
Amniocytes on the fetus and peripheral blood lympho-cytes on the child and her parents were cultured and har-vested using routine cytogenetic techniques. G-bandedchromosomes were analyzed in metaphase cells from15 colonies in cultured amniocytes and 20 cells fromcultured lymphocytes. Further studies on the amnio-cytes included fluorescence in situ hybridization (FISH)probes for chromosome 6 telomeres to rule out a ter-minal deletion and spectral karyotyping, which con-firmed the reciprocal nature of the three-way translo-cation (Courtesy L. Sargent and J. Senft, NIOSH, notshown).
RESULTS AND DISCUSSION
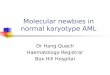
The karyotype of the amniocytes, which was confirmedon cord blood, was 45,XX,t(3;21;20)(p12;q11.2;p11.2),del(6)(q13q15),der(13;14)(q10;q10)mat (Figures 2 and3). The father’s karyotype was 46,XY, the mother’skaryotype was 45,XX,der(13;14)(q10;q10).
In addition to the 6q deletion and the maternallyinherited Robertsonian translocation, our patient had a de
Figure 1—Photograph of infant at autopsy, with parental consent,demonstrating the facial dysmorphology
1 2 3 4 5
6 7 98 10 11 12
13 14 1615 17
19 20 2221 x
18
Figure 2—Karyotype of infant showing maternally inherited 13;14Robertsonian translocation, the complex chromosomal rearrangement,which is an apparently balanced de novo three-way translocation, andde novo 6q deletion
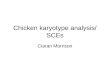
Figure 3—Ideogram showing the interstitial deletion of 6q13q15
novo complex chromosomal rearrangement. The spectralkaryotyping demonstrated the reciprocal nature of thethree-way translocation. Although the rearrangementappeared to be balanced, disruption of a gene at oneor more of the breakpoints cannot be ruled out. Ofinterest are the abdominal CT scans performed on themother within the year prior to her pregnancy, whichcould have caused DNA damage to the gametes of themother.
This is the first case of del(6)(q13q15) diagnosed pre-natally. Although intrauterine growth retardation (IUGR)was suspected and the multiple-marker screen wasabnormal, the birth weight and visceral developmentwere compatible with the stated gestational age. Incomparison with the previous 6 cases (Table 1), ourcase showed similar but milder anomalous externalfeatures of head, face, eye, ear, nose and orophar-ynx. There was no evidence of deformity of limbsor digits, and no signs of defects involving thebody wall. Previous reports have described that someclinical features might become recognizable or moreprominent with increasing age of the patient, such
Copyright 2005 John Wiley & Sons, Ltd. Prenat Diagn 2005; 25: 1084–1087.

1086 M. YU ET AL.
Table 1—Clinical presentation of patients with del(6)(q13q15)
McNeal(1977)
Young(1985)
Yamamoto(1986)
Rose(1992)
Gershoni(1996)
Passarge(2000) Present
Age at diagnosis 36 m 32 m 13 y 1.5 m 24 m 24 y PrenatalWeight at birth 2600 2420 3200 2812 2775 2650 1780Dolichocephaly + + + −Microcephaly + − − − + − −Upslanted palpebral fissure + + + + − −Epicanthic folds + + + + − +Hypertelorism + + + + Hypo- + +Short nose/broad nasal tip + + + + + − +Anteverted nares + + + + + − +Micrognathia − − − + − +Long philtrum + + + + −Thin upper lip + + + −Cleft palate + − +Microglossia + − +Large ears + + + + − −Low-set/dysplastic ears + + + + +Short neck + + + − + −Scoliosis + + + − −Clinodactyly + + − + − −Single palmar crease + + + + + −Umbilical hernia + − + + + −Inguinal hernia − + − − − −Pes planus + − + − − −Hypotonia + + − − + + +Hypermobile joint + + + + + −Umbilical cord Single A Single ACardiac anomalies PDA − PDA ASD PDA − −Other anomalies TE fistula Hiatal Scaphocephaly Ocular albinism Cryptorchidism Anterior
hernia TE fistula anus
+, present; —, absent; blank, unknown; ASD, atrial septal defect; PDA, patent ductus arteriosus, single A, single artery; TE, tracheoesophygeal.
as facial asymmetry, scoliosis and hernia (McNealet al., 1977; Young et al., 1985). This may be oneof the reasons that our patient had a milder presenta-tion.
Deletion of 6q13q15 is compatible with life. Becauseof the rarity of this deletion, there is no informationabout the life span of patients with this deletion. Thecause of death in our infant was respiratory distresssyndrome as documented by autopsy. While prematurityof birth may be related to the chromosomal abnormality,death was not due to physical defects resulting from the6q deletion.
Common abnormalities seen with the deletion6q13q15 include facial dysmorphy with epicanthalfolds, upslanted palpebral fissures, hypertelorism, shortnose with broad nasal tip and anteverted nares, longphiltrum, large low-set or dysplastic ears, and shortneck. Other common findings include single palmarcrease, umbilical hernia, hypotonia, hypermobile joints,heart defects (3 of 4 had patent ductus arteriosus)and scoliosis. Dolichocephaly was present in half thecases. Developmental delay and mental retardation wasreported in all cases; the 13-year-old had an IQ of 23(Yamamoto et al., 1986). We describe the sixth case ofdel(6)(q13q15), which is the first case diagnosed prena-tally.
ACKNOWLEDGEMENTS
We thank Ms. Jamie Senft and Dr Linda Sargent for theirhelp with spectral karyotyping analysis and Dr JonathanMcClain for photography.
REFERENCES
Gershoni-Baruch R, Mandel H, Bar ELH, Bar-Nizan N, Boro-chowitz Z. 1996. Interstitial deletion (6)q13q15. Am J Med Genet62: 345–347.
Gilhuis HJ, van Ravenswaaij CMA, Hamel BJC, Gabrels FJM. 2000.Interstitial 6q deletion with a Prader-Willi-like phenotype: a newcase and review of the literature. Eur J Paediatric Neurol 4(l):39–43.
Hopkin RJ, Schorry E, Bofinger M, et al. 1997. New insights into thephenotypes of 6q deletion. Am J Med Genet 70: 377–386.
Kumar R, Riordan D, Dawson AJ, Chudley AE. 1997. Proximalinterstitial 6q deletion. A recognizable syndrome. Am J Med Genet71: 353–356.
McNeal RM, Skoglund RR, Franke U. 1977. Congenital anomaliesincluding the VATER association in a patient with a del(6)qdeletion. J Pediatr 91: 957–960.
Passarge E. 2000. A distinctive phenotype associated with aninterstitial deletion 6q14 contained within a de novo pericentricinversion 6(p11.2q15). Cytogenet Cell Genet 91: 192–198.
Romie SS, Hartfield JK, Sutcliffe MJ, Dumont DP, Kousseff BG.1996. Monosomy 6q1 syndrome delineation. Am J Med Genet 62:105–108.
Rose NC, Menacker SJ, Schnur RE, et al. 1992. Ocular albinism in amale with del(6)(q13-q15): candidate region for autosomal recessiveocular albinism? Am J Med Genet 42: 700–705.
Copyright 2005 John Wiley & Sons, Ltd. Prenat Diagn 2005; 25: 1084–1087.

PRENATAL DETECTION OF DELETION 6Q13Q15 1087
Yamamoto Y, Okamoto N, Shiraishi H, Yanagisawa M, Kamoshita S.1986. Deletion of proximal 6q: a clinical report and review of theliterature. Am J Med Genet 25: 467–471.
Young RS, Fidone GS, Reider-Garcia PA, Hansen KL, McCombs JL,Moore CM. 1985. Deletion of the long arm of chromosome 6: twonew cases and review of the literature. Am J Med Genet 20: 21–29.
Copyright 2005 John Wiley & Sons, Ltd. Prenat Diagn 2005; 25: 1084–1087.