Embed Size (px)
Citation preview

www.elsevier.com/locate/earlhumdev
REVIEW
Prenatal assessment of foot deformity
Matthew Barry *
The Royal London Hospital, London E1 1BB, UK
0378-3782/$ - see front matter D 200doi:10.1016/j.earlhumdev.2005.06.013
* Tel.: +44 20 7377 7445; fax: +44 20E-mail address: matthew.barry@ba
KEYWORDSTalipes;Ultrasound;Prenatal diagnosis
Abstract Congenital talipes equinovarus (CTEV) and other skeletal abnormalitiescan be diagnosed prenatally by ultrasound scan. If diagnosed, clinicians should becautiously optimistic with the parents, particularly if the talipes diagnosed isisolated and not associated with other foetal abnormalities. There is no correlationbetween the prenatal appearance of the foot and the state of the foot at birth, norwith the necessity for surgical intervention.D 2005 Elsevier Ireland Ltd. All rights reserved.
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7931.1. What is CTEV? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7941.2. Prenatal assessment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 794
2. Method . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7942.1. Embryological development of the limbs [2,3]. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7942.2. Timing of scans . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7942.3. Incidence of talipes on USS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7942.4. Associated anomalies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7952.5. Amniocentesis — is it indicated? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7952.6. Correlation between prenatal diagnosis and post-natal appearance. . . . . . . . . . . . . . . . . . . 796
3. Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 796References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 796
1. Introduction
With advances in ultrasound scan (USS) technolo-gy, an increasing amount of anatomical detail ofthe foetus is now becoming available. Recent
5 Elsevier Ireland Ltd. All right
7377 7302.rtsandthelondon.nhs.uk.
developments such as 3D scanning further enhancethe quality of the images obtained. Anomaly scansare now routine and foot abnormalities areincreasingly being identified on these scans. Awide variety of musculoskeletal disorders can beidentified on these scans, including spinal abnor-malities such as spina bifida or hemivertebrae,limb reduction abnormalities such as proximalfemoral focal deficiency or finger abnormalities
Early Human Development (2005) 81, 793—796
s reserved.

M. Barry794
such as polydactyly. A common deformity that isreceiving much attention with regard to prenataldiagnosis is CTEV.
1.1. What is CTEV?
Congenital talipes equinovarus is a structuraldeformity of the lower leg characterised clinicallyby a combination of a high heel (equinus) andinward tilting of the hindfoot (varus). There areassociated deformities of the forefoot that are nowgenerally considered to represent an excessivepronation of the first ray with a variable degreeof cavus. In addition the calf may be hypoplastic.Spontaneous improvement does not occur, andtreatment , although generally successful, is pro-longed and may involve surgery.
This structural anomaly may appear superficial-ly similar to postural deformities commonly seenafter birth. These latter deformities are related tointra-uterine position and may be part of abpackagingQ problem. Spontaneous resolution isthe rule, and no active treatment is generallyrequired.
Differentiation between these two superficiallysimilar entities is therefore of extreme importance.
1.2. Prenatal assessment
Currently, the only method of prenatal diagnosis ofCTEV is by USS. Alternative imaging is not indicat-ed. Plain radiographs and CT scans result in anunacceptably high dose of radiation to the devel-oping foetus, and in addition, these imagingmodalities do not show soft tissues well. MagneticResonance Imaging (MRI) may show foot abnormal-ities but at the present time, the effects of MRI onthe developing foetus are not understood andtherefore routine MRI scans are probably notjustified.
2. Method
Ultrasound scanning of the foetus can be performedeither as a trans-abdominal scan (TAS) or a trans-vaginal scan (TVS). Early on in pregnancy, TVSresults in better image resolution (the foetus iscloser to the ultrasound probe) and as a result,musculoskeletal abnormalities can be detectedearlier by the TVS method, skeletal abnormalitiesmay be detected up to four weeks earlier [1] by theTVS method as compared to TAS.
As the pregnancy proceeds, the TVS methodbecomes less useful (the foetus moves further away
from the vaginal canal) and by about 17—18 weeksof gestation, the TAS method is preferable.
2.1. Embryological development of the limbs[2,3]
Limb buds appear at about week 4 of gestation,with the upper limb appearing a few daysearlier than the lower limb. At week 5, theupper limb has started to develop distinctregions and by week 6, the hand rays havestarted to develop. By this time, the lower limbhas developed a distinct thigh, lower leg andfoot. By the seventh week, the finger and toerays have started to develop and by 8—9 weeks,the toes and fingers have developed into sepa-rate digits.
As the limb buds develop and grow, the limbsrotate. The upper limb externally rotates and thelower limb internally rotates. This results in thefuture elbow and knee being rotated by 1808 withrespect to each other. This rotation is of primeimportance in the genesis of the CTEV deformity. Byweeks 10—11, the limb rotation process has fin-ished and limb development is largely complete.Primary ossification centres start to be seen in mostlong bones diaphyses by week 12.
2.2. Timing of scans
The optimum time to perform an USS to detectCTEV is between weeks 14 and 16 [4] of gestationalthough in many centres, anomaly scans are notperformed until 18—20 weeks [5,6]. Four types oftalipes have been described [1] on USS:
1. Early onset — diagnosed at 14—16 weeks andincludes most cases seen on USS.
2. Late onset — normal early scan but talipes notedat later scans after 20 weeks. (Many of these willnot be true CTEV but will be simple positionaldeformities in a structurally normal foot.)
3. Transient talipes — initial abnormality disap-pears and a normal foot is seen at later scans.
4. Incomplete — some abnormalities noted on USS.About 5% of this type will go on and develop trueCTEV.
2.3. Incidence of talipes on USS
The incidence of CTEV at birth is about 1 per 1000but there are racial variations, with, for example,up to 7 per 1000 births in the Maori population [4].On USS, the incidence varies from 0.1% [7,8] to0.4% [9].

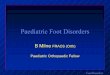
Figure 3 Appearance of foot at 10 days — plantar view.
Figure 1 18 week USS of unilateral isolated talipes —dorsal view.
Prenatal assessment of foot deformity 795
The sensitivity and specificity of USS detectionof talipes is not well reported in the literature.Tillett [6] reported a sensitivity of 0.95 (95% ofaffected feet were detected) but this paper was asmall group of selected patients and was not apopulation survey. Other authors [9] have sug-gested that talipes associated with other abnor-malities has a very low false positive rate (0%) but ifthe talipes is apparently isolated, the false positiverate is higher [9,10] especially if the USS isperformed in the third trimester [1].
2.4. Associated anomalies
A variety of associated abnormalities have beennoted [1,9]. Treadwell [9] found that in their study67% of the cases of talipes identified prenatally hadother abnormalities. These included CNS anomalies(36%), urogenital tract anomalies (29%) and skeletaldysplasias (10%). The remaining 33% of CTEV
Figure 2 18 week USS of unilateral isolated talipes —plantar view.
diagnosed prenatally appeared to have an isolatedfinding of talipes. At birth, a significant number ofthese apparently isolated talipes cases had normalfeet. However, in all cases of talipes associatedwith other abnormalities, talipes was presenteither at birth or termination. In other studies[7], up to 50% of talipes cases were associated withother abnormalities. It is likely that the talipesassociated with other abnormalities may be a moresevere bteratologicalQ club foot and so more easilyseen on USS [1].
2.5. Amniocentesis — is it indicated?
If an isolated abnormality is found, should an amnio-centesis be performed to obtain a karyotype of thefoetus? The literature is conflicting on this question.
Figure 4 Appearance of foot at 10 days — dorsal view.

M. Barry796
Shipp and Benacerraf [10] argue that amniocen-tesis should be performed as in his paper, 6% of theisolated talipes cases had an abnormal karyotype.Pagnotta et al. [11] found that 22% of their caseshad abnormal karyotypes although this includedisolated talipes and talipes associated with otherabnormalities on USS. In contrast, Malone et al.[12] found no abnormal karyotypes even in high riskmothers and therefore suggested that there was noindication for prenatal karyotyping, providing theUSS was otherwise normal, apart from the talipes.Katz et al. [13] found no abnormal karyotypes,although the number of cases was small.
As there appears to be a higher false positiverate in these isolated cases and the risks of anabnormal karyotype is low (6%) then amniocentesisis probably not indicated.
2.6. Correlation between prenatal diagnosisand post-natal appearance
Once diagnosed, there is poor correlation betweenthe prenatal appearance of the foot on USS and theseverity of the talipes at birth [1,4,6].
Tillett et al. [6] noted that in 26% of the talipesdiagnosed prenatally, the deformity was so mild atbirth that no treatment was required. In theirseries, 13% were treated with serial casts and 61%required surgery. Kerat et al. [4] quoted a figure of55% of prenatally diagnosed cases requiring surgery.Neither author could find any predictive factor inthe prenatal diagnosis with respect to the likeli-hood of structural abnormality of the foot requiringtreatment.
Experience in our practice would support thisobservation, making meaningful prenatal counsel-ling difficult. There is inevitably a risk of causingunnecessary concern for those prospective parentswho find that their baby has nothing more than apositional talipes that does not require treatment.Themost positive aspect of such counselling is that itraises awareness of the possibility of a true struc-tural deformity that requires immediate treatment.
Figs. 1 and 2 show an 18 week ultrasound scan ofan isolated unilateral true CTEV. Figs. 3 and 4 arethe same foot, ten days after birth and after oneweek in a plaster cast. In this case the foot wastreated by casting and Achilles tenotomy, asdescribed by Ponseti and Smoley [14].
3. Conclusion
Talipes can be diagnosed prenatally and if associ-ated with other foetal abnormalities, the false
positive rate appears to be low. This complex typeof talipes is probably a more rigid teratologicalcondition and may be associated with terminationof the pregnancy. In these complex cases, amnio-centesis may be indicated. However, in isolatedcases of talipes with no other foetal abnormalities,then the indication for amniocentesis is less clear.
When talipes is diagnosed as an isolated defor-mity, especially in the third trimester of pregnancy,the clinician should perhaps be more optimistic. Anumber of these feet may be normal at birth orhave only a mild deformity requiring no treatment.Neither the appearance of the foot on ultrasoundnor the stage of foetal development at which USSdiagnosis is made, is strongly correlated with thetrue nature of the deformity at birth. This placeslimitations on the usefulness of prenatal counsel-ling by the orthopaedic surgeon.
References
[1] Weintroub S, Keret D, Bronshtein M. Prenatal sonographicdiagnosis of musculoskeletal disorders. J Paed Orth1999;19:1–4.
[2] http://nmhm.washingtondc.museum/collections/hdac/index.htm.
[3] http://www.visembryo.com.[4] Kerat D, Ezra F, Lokiec F, Hayek S, Segev E, Weintroub S.
Efficacy of prenatal ultrasonography in confirmed clubfoot. J Bone Joint Surg 2002;84B:1015–9.
[5] Burgan HE, Furness ME, Foster BK. Prenatal ultrasounddiagnosis of clubfoot. J Paed Orth 1999;19:11–3.
[6] Tillett RL, Fisk NM, Murphy K, Hunt DM. Clinical outcome ofcongenital talipes equinovarus diagnoses antenatally byultrasound. J Bone Joint Surg 2000;82B:876–80.
[7] Bakalis S, Sairam S, Homfray T, Harrington K, Nicolaides K,Thilaganathan B. Outcome of antenatally diagnosed talipesequinovarus in an unselected obstetric population. Ultra-sound Obstet Gynecol 2002;20:226–9.
[8] Rijhsinghani A, Yankowitz J, Kamis AB, Mueller GM,Yankowitz DK, Williamson RA. Antenatal sonographic diag-nosis of club foot with particular attention to the implica-tions and outcomes of isolated club foot. Ultrasound ObstetGynecol 1998;12:103–6.
[9] Treadwell MC, Stanitski C, King M. Prenatal sonographicdiagnosis of club foot: implications for patient counselling.J Paed Orth 1999;19:8–10.
[10] Shipp TD, Benacerraf BR. The significance of prenatallyidentified isolated clubfoot: is amniocentesis indicated. AmJ Obstet Gynecol 1998;178:600–2.
[11] Pagnotta G, Maffulli N, Aureli S, Maggi E, Mariani M, Yip KM.Antenatal sonographic diagnosis of clubfoot: a six-yearexperience. J Foot Ankle Surg 1996;35:67–71.
[12] Malone FD, Marino T, Bianchi DW, Johnston K, D’Alton ME.Isolated clubfoot diagnosed prenatally: is karyotypingindicated? Obstet Gynecol 2000;95:437–40.
[13] Katz K, Meizner I, Mashiach R, Soudry M. The contributionof prenatal sonographic diagnosis of clubfoot to preventivemedicine. J Paed Orth 1999;19:5–7.
[14] Ponseti IV, Smoley EN. Congenital club foot: the results oftreatment. J Bone Joint Surg 1963;45A:261–5.