Embed Size (px)
Citation preview

Lichtman et al.
6. Palmer AK, Dobyns JH, Linscheid RL: Management of posttraumatic instability of the wrist secondary to ligament rupture. J HAND SURG 3:507-32, 1978
7. Lichtman DM, Schneider JR, Swafford AR, Mack GR: Ulnar midcarpal instability. Clinical and laboratory analysis. J HAND SURG 6:515-23, 1981
The Journal of HAND SURGERY
8. Watson HK: Limited wrist arthrodesis. Clin Orthop 149:126-36,1980
9. Watson HK, Goodman ML, Johnson TR: Limited wrist arthrodesis. Part II: Intercarpal and radiocarpal combinations. J HAND SURG 6:223-33, 1981
Preliminary study of the upper limb with the use of ultrasound transmission imaging
A biologically safe, noninvasive method for visualizing bone and soft tissue relationships has been developed recently. Termed the ultrasonic transmission imaging system, its advantages include visualization of soft tissues in real time while motion is underway. The image can be correlated to standard x-ray films, but since no ionizing radiation is involved, repeated risk-free visualization of extremities for either diagnostic assessment or biomechanical studies is permitted. Resolution of 1 mm and a depth of field of 8 mm are adequate for visualization of neurovascular bundles, tendons, ligaments, bones, and joints. The image can be digitized and stored for later analysis on computer graphic systems. Pilot studies have correlated the ultrasonic anatomy of normal and abnormal living and cadaver hands with known anatomic structures. The benefits to biomechani
cal analysis include the ability to visualize and accurately measure in a noninvasive manner the in vivo changes of position of tendons and other structures during movement. These initial efforts indicate the growing diagnostic and analytic capabilities of this instrument. (J HAND SURG
9A:188-92, 1984.)
Vincent R. Hentz, M.D., Kenneth W. Marich, M.B.A., and Parvati Dev, Ph.D., Stanford and Palo Alto, Calif.
Periodically, technical advances have a major impact on a clinical specialty. The development of ultrasonic techniques in medical diagnosis is but one example. In the 20 years since the introduction of ultrasonic techniques, their effectiveness as biologically safe, noninvasive diagnostic instruments has improved considerably. The use of pulse-echo or reflective ultrasound instruments is now widespread. Since nonionizing radiation is involved, reflective ultrasound studies have replaced radiography in prenatal fetal examinations. These instruments may supplant carotid angiog-
From Rehabilitation Research and Development, Palo Alto Veterans Administration Medical Center and the Schools of Medicine and Engineering, Stanford University, Stanford, Calif.
Received for publication Feb. 5, 1982; accepted in revised form April 22, 1983.
Reprint requests: Vincent R. Hentz, M.D., Stanford University Hospital, Ri03, Stanford, CA 94305.
188 THE JOURNAL OF HAND SURGERY
raphy as a screening tool for carotid artery stenosis. 1
The cross-sectional image derived from this reflective mode has only limited orthopedic applications at present, such as determining if a mass is fluid filled or solid or identifying, for example, abscess cavities. The detailed reflective image necessary for orthopedic examination is necessarily a static image because considerable time is needed to collect the reflective data sufficient to generate a high-resolution image. Far more applicable to the study of dynamic structures would be a focused ultrasonic system that would provide real-time, detailed images much like x-ray fluoroscopic techniques.
Ultrasonic transmission imaging (UTI)
A new instrument, the UTI camera, developed by Stanford Research Institute International (SRI), provides a unique perspective in soft and hard tissue diagnostic imaging. It has the following advantages over conventional x-ray and reflective ultrasonic methods:

Vol. 9A, No.2 March 1984
AUXILIARY
Study of upper limb with ultrasound transmission imaging 189
TRANSMISSION-MODE TRANSDUCER WITH
DIVERGING LENS TANK LENS/DEFLECTOR 192 ELEMENT RECEIVING ARRAY n PACKAGE
~L m TRANSMITTER
SIGNAL PROCESSING
ELECTRONICS
DISPLAY AND
RECORDING
COLLIMATING ~REPLECTION-MODE LENS FOCAL TRANSDUCER
PLANE
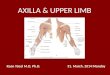
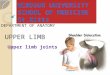
Fig. 1. The radio frequency generator and transmitting transducers (transmitter) produce pressure waves that are collimated and propagated through the water toward the target, which is placed in the focal plane of the system. The pressure waves are scattered in passing through the object, are collimated, and are focused by plastic lenses (lens / deflector package) onto 192 receiving transducers that produce a video signal that is digitally processed and stored on magnetic tape or converted into standard television format.
I. Real-time interactive display: The patient or the part can be examined while motion is underway and while localized palpation is being applied.
2. Soft tissue delineation: Tendons. ligaments. muscles. cartilage. blood vessels, and organ tissues can be examined while bone is presented in silhouette.
3. Correlation to radiography: Unlike conventional pulse-echo cross-sectional ultrasonic images, transmission images are presented in an orthographic format and can be directly correlated to x-ray methods.
4. Focusing: A depth of field about 1 cm allows objects of interest to be moved in and out of the focal plane. The position of the plane of focus is selected easily in much the same manner as microscopy by movement of the object being visualized.
5. Safety: No ionizing radiation is involved. An ultrasonic intensity of less than 1 m W / cm2 is sufficient for examining the extremities. Repeated and lengthy examinations present no risk to the patient. 2
The components of the SRI transmission imaging system are shown in Fig. 1. The legend briefly outlines the technique. The depth of field (8 mm) and resolution (1 mm) has proved suitable for detailed imaging of the upper limb without danger to the subject or observer.
Initial studies were performed by placing the object to be visualized in a small water tank (sound waves are poorly transmitted in air). These studies were designed to correlate the transmission ultrasonic image with known anatomic structures. Both cadaver and living hands were imaged. By moving the area or the object to be examined in and out of the focal plane, a three-
dimensional quality of the video image becomes apparent. Indeed the ability of the brain to reconstruct three-dimensional information from moving two-dimensional images greatly aids in the interpretation and identification of the anatomic studies. Unfortunately. this three-dimensional quality of the image is not transferred onto single frames in the video image or captured for illustrative photography. The accompanying photographs, while demonstrating the feasibility of the UTI technique. provide only a suggestion of what is seen in real time. Static photographic reproductions of these images result in an additional loss of detail, which is clearly observable in the real-time image.
Cadaver hands
The earliest studies used cadaver hands to provide a direct correlation of the acoustic image to known anatomic structures. Fresh cadaver hands appear to transmit more nearly accurate and better defined images than do older, frozen specimens. Preserved specimens are of little value because of the altered acoustic properties of the tissue caused by the preservation processes. In our initial studies. the cadaver hand was fixed first to a stabilizing platform and then scanned. Such anatomic structures as neurovascular bundles, tendons, collateral ligaments, and joint spaces can be seen in the fingers and intermetacarpal spaces (Fig. 2). Wire guides attached to various tendons allow these to be pulled and moved. Movement was observed easily. Selective palpation confirmed identification of many of the objects being imaged during real-time examination. Since no ionizing irradiation is involved, there is no danger to the observer as he manipulates or palpates with his own hand the object being observed.
A number of invasive techniques were used in the

190 Hentz et al .
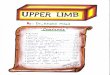
Fig. 2. Ultrasonic images of a fresh cadaver hand. The static image from the video monitor has been photographed and reproduced. A, Image demonstrates the anteroposterior projection of the intermetacarpal spaces just before injection of air into the ulnar artery at the wrist. B, Increased delineation of vascular anatomy after injection of 0.2 cc of air as a contrast agent. (Note arrows at the common digital arteries and their bifurcation .)
cadaver studies to confirm and correlate further the acoustic image with known anatomy. Contrast studies to assist in visualization of the vascular anatomy were performed. Visualization of the vascular anatomy was enhanced by the injection of air into the arterial system (Fig. 2,A andB). A suspension preparation of barium sulfate also proved to be an excellent ultrasonic as well as a radiologic contrast agent, allowing us to correlate and confirm some ultrasonic anatomic observations by standard radiography. To define tendon anatomy better,
The Journal of HAND SURGERY
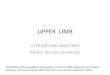
Fig. 3. Ultrasonic transmission images of a fresh cadaver hand. A, The first intermetacarpal space is visualized (note arrow at the flexor pollicis longus tendon). B, The flexor pollicis longus has been withdrawn , exposed to air, marked with a wire suture (arrow) , then returned to its normal tendon sheath.
and particularly the ultrasonic profile during motion, the movement of many tendons as observed on the ultrasonic image was recorded. The tendon was then removed from its synovial sheath, marked with a wire suture, replaced in its sheath, and moved again. Exposing the tendon caused some absorption of air that further acoustically altered its ultrasonic image. The wire marker could be seen clearly on the ultrasound image (Fig . 3). The empty tendon sheath had a recognizably different ultrasonic image when compared to the image of the tendon in its sheath. This has significant diagnostic implications . Other anatomic struc-

Vol. 9A, No . 2 March 1984
tures studied included the carpal bones and various collateral ligaments. The relationship of the movement of the various carpal bones could be visualized, but the image was not as well defined as with standard cinefluorographic images. However, resolution seemed sufficient to recognize, for example, a scapholunate dissociation . The larger collateral ligaments, particularly those about the metacarpophalangeal joints, were clearly visualized .
Living hands
Hands from living subjects were ultrasonically examined by having the subjects place their hands in the focal plane of the camera. Resolution seemed slightly better than in fresh cadaver hands . The hands were moved back and forth through the focal plane and were rotated to obtain the best position for imaging specific internal structures. In these hands , many tendons , muscles , ligaments , and bone were easily delineated. After some imaging experience, it became apparent that the position of the hand was important in visualizing specific anatomic structures, particularly the flexor and extensor tendons in the digits. Similarly, in movement these structures can be defined more clearly than when static. For example, the paths of both the superficialis and profundus flexor tendons can be visualized from the base of the finger to their insertions . Their palmar displacement as the finger was flexed could be visualized. The increased palmar displacement associated with resistance. to flexion could also be observed (Fig. 4).
Other applications in the hand
We believe that this instrument can be an exceptional tool for the in vivo study of the biomechanics of the hand . There are two major problems in the in vivo analysis of the forces required for movement and control of. for example , the finger. One is the inability to localize the trajectory of each tendon. Another is the inability to measure directly the force in each tendon. In vitro, these factors can be either controlled or observed by placing wire markers within various tendons and exerting a known force on these tendons, which is impossible in living hands. Whereas a number of indirect methods to measure various forces exist,5-8 until now , no safe, noninvasive method to measure the exact position of various tendons or their trajectories during movement has existed. With a resolution of 1 rom, UTI allows accurate measurement of the trajectory of tendons. Some resolution is lost when the digitally processed signals are converted to a video image. If the
Study of upper limb with uLtrasound transmission imaging 191
Fig. 4. UTI of a living hand . A, A plastic calibration grid is placed in the focal plane to align the transducers and check resolution. The dots in the center are 1 mrn in diameter. and the space between the lines is approximately 1 mrn. B, The index finger in the lateral projection (arrow shows the course profundus tendon from base of digit to tip of finger). C, The hand in the anteroposterior projection (the arrows point to collateral ligament of index finger and neurovascular bundle and i ntermetacarpal space) .
digital information taken directly from the magnetic tape is displayed onto a high-resolution computer graphic video system, resolution and detail are clearly improved. With the data obtained by UTI, we have performed several preliminary biomechanical investigations . We have been able to digitize the ultrasonic image and store this on magnetic tape for later processing by modem computer graphic systems . Such computer graphic systems can be programmed to enhance and analyze the image, producing a computer-derived two- or three-dimensional model or a simulation of the digit (Fig. 5). Any number of force or directional parameters can be altered on the computer simulation. The results of the computer simulation can be verified and correlated with the real-time transmission image obtained by similar manipulations of cadaver or living hands. Tendon trajectories, moment arms , and joint angles can be measured directly from the real-time ultrasonic video image . At the present time, for in vivo biomechanical studies , many of these parameters must , by necessity, be assumed. The noninvasive, bio-

192 Hentz et al. The Journal of
HAND SURGERY
Fig. 5. UTI as displayed directly onto a high-resolution computer graphic video system. A, The image has been photographed directly from the computer graphic video screen. The index finger is held in extension (note the course of the flexor tendon and its relationships to the adjacent osseous structures). The skin and skeleton are electronically highlighted. B, The bony skeleton and the course of the flexor tendon have been outlined electronically and the image has been photographed. C, The same index finger held in forcible flexion. The image is photographed directly from the computer graphic video screen without electronic enhancement of the outlines of skin or bone. D, The course of the flexor tendon is outlined. (Note that the palmar displacement of the flexor tendon and its angulation at the A4 pulley is well visualized. Compare its direction to that indicated in B with the finger held in extension.)
logically safe characteristics of the transmission ultrasound camera system allow repeated and lengthy examination of the living hand, seemingly without hazard to the subject or examiner.
Further modifications
The resolution and depth of focus can be altered by adding receiving arrays and by increasing the ultrasonic frequency to 5 or 10 MHz. SRI is now constructing a transmission ultrasound camera system with greater diagnostic capabilities than the present research instrument. With systems employing advanced design, we anticipate extending this technical advance to many diagnostic problems of the upper limb. For example, with UTI, it will be possible to locate the end of a divided flexor tendon, visualize a tom ulnar collateral ligament, diagnose intercarpal dissociations, and study the ultimate pathway of tendon transfers. Many other diagnostic or basic investigative studies can be performed. The use of this unique instrument will add measurably
to our understanding of the function and maladies of the hand.
REFERENCES
1. Evans TC Jr, Taenzer JC: Ultrasound imaging of atherosclerosis in carotid arteries. Appl Radiol 8: 106, 1979
2. Edmonds PD: Effects of ultrasound on biological structures. Review article, Stanford Research Institute International, Menlo Park, Calif., April, 1979
3. Marich KW, Green PS, Taenzer JC, Glick D, Mitchell AS, Stephens RJ, Stolzenberg SJ, Edmonds PD: Bioeffects of low-level ultrasound. In White DN, Brown RE, editors: Ultrasound in medicine, vol 3B. New York, 1977, Plenum Publishing Corp
4. Marich KW, Zatz LM, Suarez JR, Macovski A: Real-time imaging with a new ultrasonic camera: Part I. In vitro experimental studies on transmission imaging of biological structures. JCU 3:5-16, 1975
5. Ketchum LD, Wallingford DJ: An analysis of forces generated by the intrinsic muscles of the index finger and

Vol. 9A, No.2 March 1984
coordinating muscles of the hand. J HAND SURG 3:571. 1978
6. Hazelton Fr. Smidt GL. Flatt AE. Stephens RI: The influence of wrist position on the force produced by the finger flexors. J Biomech 8:301-6. 1975
7. Cooney WP. Chao EYS: Biomechanical analysis of static
Study of upper limb with ultrasound transmission imaging
forces in the thumb during hand function. J Bone Joint Surg [Am] 59:27-36. 1977
8. Brand PW. Beach RB: Relative tension and potential excursion of muscles in the forearm and hand. Paper presented at the Hand Society Meeting. San Francisco. February 1979
Atherosclerosis of the forearm and hand
Three patients were treated for severe atherosclerotic obstructive disease in the upper extremity. In all three, vein bypass grafts were placed from the forearm to the superficial palmar arch. The grafts have remained patent for the period of follow-up between 8 and 18 months, and significant palliation was achieved. (J HAND SURG 9A:193-6, 1984.)
H. Hollis Caffee, M.D., and Nalin T. Master, M.D., Gainesville, Fla.
Chronic arterial insufficiency of the hand is a relatively uncommon manifestation of atherosclerotic vascular disease. In contrast to the extremely common obstructive disease in the lower extremities or the coronary circulation, very little has been published about surgical experience with atherosclerosis in the hand. I. 2 Most of the literature on chronic arterial insufficiency of the hand relates to vasospastic disease or to thromboangiitis obliterans.3• 4
Over a 2-year period three patients were seen at the Gainesville Veterans Administration Hospital with signs and symptoms of chronic arterial insufficiency of one hand. All three patients presented with essentially the same clinical pattern. Symptoms began with a gradual onset of claudication and cold intolerance. This later progressed to severe constant pain and ischemic ulceration or gangrene. The diagnosis was readily established by the absence of both radial and ulnar pulses to either palpation or Doppler ultrasonic flow detector. However, demonstration of etiology and extent of disease required arteriography. In every case there was evidence of diffuse atherosclerotic involvement of the
From the Division of Plastic and Reconstructive Surgery. University of Florida College of Medicine, Gainesville, Fla.
Received for publication March 24, 1983; accepted in revised fonn May 8, 1983.
Reprint requests: H. Hollis Caffee, M.D., University of Florida College of Medicine, Division of Plastic and Reconstructive Surgery, Box J-286, J. Hillis Miller Health Center. Gainesville, FL 32610.
vessels of the forearm and hand with multiple levels of obstruction of both radial and ulnar arteries, the hand surviving on multiple small collateral vessels. All three patients had patent palmar arches and all three were successfully treated with a vein bypass graft from above the first obstruction to the superficial palmar arch.
Case reports
Case 1. A 58-year-old retired right-handed veteran was referred for amputation of a gangrenous left thumb. He had a 50 pack-year* history of cigarette smoking. Three months prior to admission he presented with claudication, cold intolerance, and absent pulses in the wrist. An arteriogram at that time showed diffuse atherosclerotic disease with complete obstruction of both the radial and ulnar arteries at the level of the elbow. The radial artery was reconstituted distally by collateral vessels from an enlarged median artery. The superficial palmar arch was well visualized, but segmental obstructions were seen in several digital arteries (Fig. 1). An attempt was made to bypass the proximal obstructions with a saphenous vein graft from the brachial artery to the radial artery. The graft occluded within a few days and was replaced with an expanded polytetrafluoroethylene graft, but this also failed. During the time of these operations the patient developed severe rest pain and gangrene of the thumb.
The patient was referred to the hand service for amputation of his gangrenous thumb, but the pain involved the entire hand and was sufficiently severe that he requested amputation
*Pack-year = number of packs smoked per day multiplied by the number of years patient has smoked.
THE JOURNAL OF HAND SURGERY 193