Embed Size (px)
Citation preview

tlRmctccTd
Medical Dosimetry, Vol. 36, No. 4, pp. 416-422, 2011Copyright © 2011 American Association of Medical Dosimetrists
doi:10.1016/j.meddos.2010.10.003
PRELIMINARY RESULTS OF HELICAL TOMOTHERAPY IN PATIENTSWITH COMPLEX-SHAPED MENINGIOMAS CLOSE TO THE
OPTIC PATHWAY
LUIS SCHIAPPACASSE, M.D., RICARDO CENDALES, M.D., KITA SALLABANDA, PH.D.,FRANCO SCHNITMAN, M.D., and JOSE SAMBLAS, M.D.
Neuro-Oncology Unit, Tomotherapy Department, Clinica La Milagrosa, IMO Group (Instituto Madrileno deOncologia), Madrid, Spain
(Received 13 August 2010; accepted 21 October 2010)
Abstract—Meningiomas are the most common benign intracranial tumor. Meningiomas close to the opticpathway represent a treatment challenge both for surgery and radiotherapy. The aim of this article is to describeearly results of helical tomotherapy treatment in complex-shaped meningiomas close to the optic pathway.Twenty-eight patients were consecutively treated. All patients were immobilized with a thermoplastic head maskand planned with the aid of a magnetic resonance imaging–computed tomography fusion. All treatmentsincluded daily image guidance. Pretreatment symptoms and acute toxicity were recorded. Median age was 57.5years, and 92.8% patients had Eastern Cooperative Oncology Group performance status scale <1. The mostcommon localizations were the sella turcica, followed by the cavernous sinus and the sphenoid. The most commonsymptoms were derived from cranial nerve deficits. Tomotherapy was administered as primary treatment in35.7% of patients, as an adjuvant treatment in 32.4%, and as a rescue treatment after postsurgical progressionin 32.1% patients. Most patients were either inoperable or Simpson IV. Total dose varied between 5000 and 5400cGy; fractionation varied between 180 and 200 cGy. Median dose to the planning target volume was 51.7 Gy(range, 50.2–55.9 Gy). Median coverage index was 0.89 (range, 0.18–0.97). Median homogeneity index was 1.05(range, 1–1.12). Acute transient toxicity was grade 1 and included headache in 35.7% patients, ocular pain/dryness in 28.5%, and radiation dermatitis in 25%. Thus far, with a maximal follow-up of 3 years, no late effectshave been seen and all patients have a radiological stabilization of the disease. Helical tomotherapy offered a safeand effective therapeutic alternative for patients with inoperable or subtotally resected complex-shaped menin-giomas close to the optic pathway. Acceptable coverage and homogeneity indexes were achieved with appropriatevalues for maximal doses delivered to the eyes, lenses, and chiasm, despite the proximity of the tumor to thesestructures. © 2011 American Association of Medical Dosimetrists.
Printed in the USA. All rights reserved0958-3947/11/$–see front matter
Key Words: Meningioma, Visual pathways, Radiotherapy, Intensity-modulated, Tomotherapy.
ti
naIisrtpo
aIr
INTRODUCTION
Meningiomas are the most common benign intracranialtumor; they account for 15% of all primary intracranialtumors. Approximately 90% are benign tumors, and theyoccur more frequently in females than in males, with a2:1 ratio.1 Although the preferred first treatment alterna-ive is surgery, it is not always possible because of tumorocalization or the clinical conditions of the patient.adiotherapy is effective as primary or adjuvant treat-ent in surgically inaccessible, recurrent, subtotally ex-
ised tumors, or in postsurgical relapses.2 Tumors closeo the optic pathway represent a surgical challenge be-ause they are in contact with critical structures, have aomplex shape, and can be moderately large in volume.hese difficulties also represent a challenge for the ra-iotherapy treatment, because it can be difficult to shape
Presented as an abstract at the TomoTherapy EMEA User Sym-posium held in Marbella (Malaga), Spain, May 6–8, 2010.
Reprint requests to: Luis Schiappacasse, M.D., TomotherapyDepartment, Clinica La Milagrosa, Modesto Lafuente 14, Madrid,
Spain, 28010. E-mail: [email protected]416
he dose distribution to the tumor while adequately spar-ng the organs at risk.
Radiotherapy techniques for the treatment of me-ingiomas include radiosurgery, conformal radiother-py, and intensity-modulated radiotherapy (IMRT).MRT has shown to be a safe and effective technologyn the treatment of intracranial meningioma, with re-ults comparable with those observed in conformaladiotherapy, both in the short3,4 and the intermediateerm,5 with some dosimetric advantages regarding tolanning target volume (PTV) coverage and sparing ofrgans at risk, even in complex-shaped tumors.6 To-
motherapy is a helicoidal IMRT treatment with highermodulation capabilities when compared with conven-tional IMRT, and the advantage of having an on-boardmegavoltage computed tomography (CT) imaging sys-tem capable of performing online image-guided radio-therapy.7 Tomotherapy has shown discrete dosimetricdvantages over some other modern techniques ofMRT in terms of coverage and sparing of organs atisk in the treatment of benign intracranial tumors8 and
greater dose uniformity in small brain tumors.9 Further

b
Meningiomas close to the optic pathway ● L. SCHIAPPACASSE et al. 417
clinical research has been recommended to validatethese preclinical, dosimetric findings.
In Spain, tomotherapy was first implemented at theInstituto Madrileno de Oncologia (IMO), in 2006. IMOhas accumulated an important number of patients withcomplex-shaped meningiomas close to or in direct con-tact with the optic pathway with indication of externalbeam radiotherapy treatment. This retrospective studydescribes our early treatment experience with tomo-therapy in this group of patients.
METHODS AND MATERIALS
Study design and patientsA descriptive, retrospective study was designed. All
patients with complex-shaped meningiomas close to orin direct contact with the optic pathway treated withhelical tomotherapy between January 2006 and March2009 at the Tomotherapy Unit, Clinica La Milagrosa, inMadrid, Spain, were included. The subset of eligiblepatients was identified from records of newly treatedpatients. Patients with multiple meningiomatosis orpreexistent or concomitant malignant diseases wereexcluded.
Tomotherapy treatmentAll patients were immobilized with a three-point
fixation thermoplastic head mask and planned using acomputed tomography–MRI (CT–MRI) fusion for thedefinition of tumor and organ at risk volumes. The CTaxial slice thickness was 3 mm; all CT and MRI imageswere imported into the Pinnacle treatment planning sys-tem (Philips Radiation Oncology Systems, Fitchburg,WI). Register and fusion were performed through thenormalized mutual information algorithm. Gross tumorvolume (GTV) was defined as the contrast-enhancingarea volume on MRI; PTV was defined as the GTV or thetumor bed plus a 2–3-mm margin. Areas of the PTV thatwere outside the skull were trimmed with a 0.3-cm innermargin to the body contour. Organs at risk included butwere not limited to the optic nerves, chiasm, lenses, eyes,brain, and brainstem. Datasets and structures were trans-ferred to the tomotherapy treatment planning software(TomoTherapy, Inc., Madison, WI) and an inverse treat-ment planning was performed.
The helical tomotherapy parameters definitionswere between 1 and 2.5 cm for the field size, 0.2–0.3 forpitch, and a planning modulation factor of 2–3. Alltreatments had a delivery quality assurance previous totreatment initiation. For PTV, the planning treatmentobjectives were to cover at least 95% of the PTV with the95% isodose, to have a minimum PTV dose of 90%, anda to have a maximum PTV dose of 105%. For organs atrisk, the planning objectives were maximal doses of 50Gy for optic nerves, 52 Gy for chiasm, 7 Gy for lenses,30 Gy for eyes, V-40 �30% for brain, and 52 Gy for
rainstem.All treatments were delivered through a 6-MV pho-tons helical TomoTherapy HiArt II system unit. Patientswere positioned by aligning the treatment room’s laserswith the marks drawn on the thermoplastic mask. Mega-voltage/CT images of the entire length of the PTV wereacquired before each fraction and co-registered with theplanning images based on bone anatomy. Patient setupbefore treatment was verified through the system’s soft-ware and according to the criteria of the radiation ther-apist. Patient setup deviations were detected in themedial-lateral, cranial-caudal, and anterior-posterior di-rections. Rotational deviations in the cranial-caudal axis(roll), anterior-posterior axis (pitch), and medial-lateralaxis (yaw) were also identified. Daily setup correctionsfor nonrotational deviations and roll were performed forall patients; rotational deviations for pitch and yaw weretaken into account only when subjectively consideredimportant.
Follow-upFollow-up with clinical examination was performed
weekly during the whole treatment and 3 months afterfinishing. MRI and clinical examination were performedevery 6 months during the remaining first year, andyearly thereafter. Clinical characteristics, pretreatmentsymptoms, and follow-up information were collectedfrom the clinical charts; acute neurological toxicity (until4 weeks after finishing treatment) was recorded accord-ing to Common Terminology Criteria for AdverseEvents v3.0 (CTCAE). Dose-volume histograms forPTV, optic nerves, chiasm, lenses, eyes, brain, and brain-stem were recorded from the dosimetric charts. Homo-geneity index was calculated dividing the maximal PTVdose by the prescription dose; the coverage index wascalculated dividing the minimum PTV dose by the pre-scription dose. Both indexes were calculated accordinglyto the recommendations established for evaluating tomo-therapy treatment plans.10
Statistical methodsMeasures of central tendency and dispersion were
used for numerical variables; simple frequencies andpercentages were used for categorical variables. Normal-ity assumptions were verified through the Shapiro-Wilktest. Exploration of factors associated with toxicity wasperformed by a traditional means comparison using theindependent-sample t-test or the Mann-Whitney U testaccording to the distributional assumptions. Two-tailedtests were always used and p values less than 0.05 wereconsidered statistically significant. All statistical analy-ses were performed using the SPSS version 12.0 soft-ware (SPSS, Inc., Chicago, IL).
Ethical considerationsThis study was classified as low risk; hence,
informed consent was not required. All procedures
followed were in accordance with good clinical prac-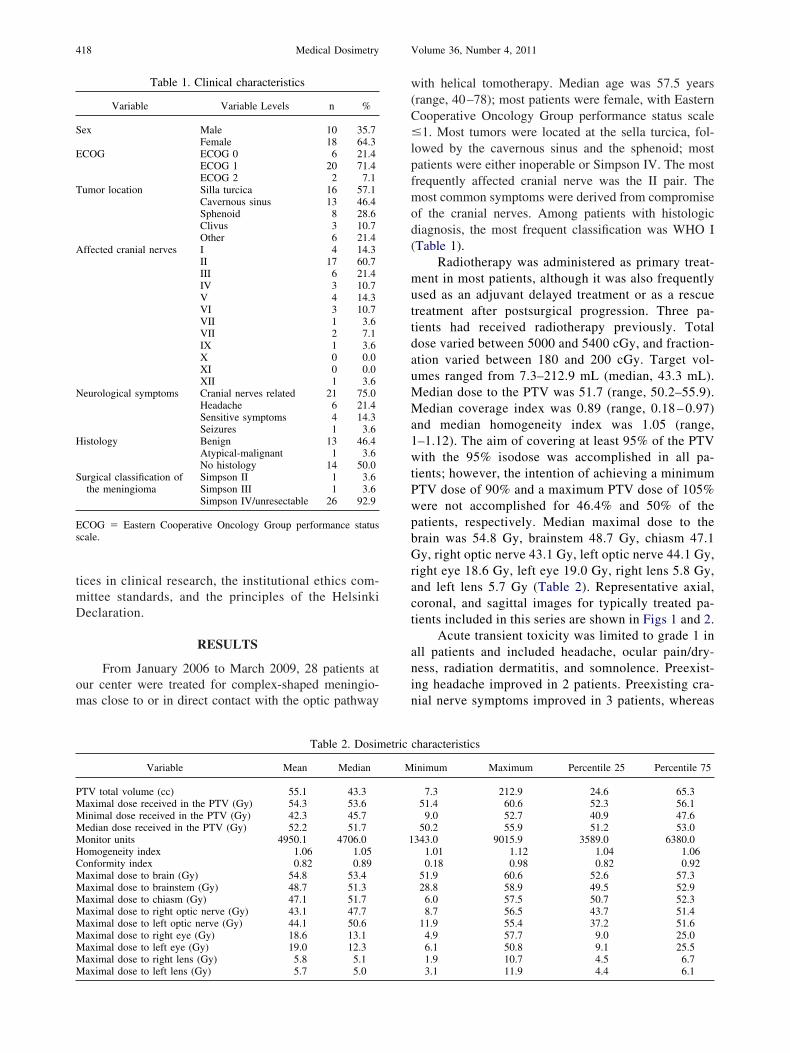
Medical Dosimetry Volume 36, Number 4, 2011418
tices in clinical research, the institutional ethics com-mittee standards, and the principles of the HelsinkiDeclaration.
RESULTS
From January 2006 to March 2009, 28 patients atour center were treated for complex-shaped meningio-mas close to or in direct contact with the optic pathway
Table 1. Clinical characteristics
Variable Variable Levels n %
Sex Male 10 35.7Female 18 64.3
ECOG ECOG 0 6 21.4ECOG 1 20 71.4ECOG 2 2 7.1
Tumor location Silla turcica 16 57.1Cavernous sinus 13 46.4Sphenoid 8 28.6Clivus 3 10.7Other 6 21.4
Affected cranial nerves I 4 14.3II 17 60.7III 6 21.4IV 3 10.7V 4 14.3VI 3 10.7VII 1 3.6VII 2 7.1IX 1 3.6X 0 0.0XI 0 0.0XII 1 3.6
Neurological symptoms Cranial nerves related 21 75.0Headache 6 21.4Sensitive symptoms 4 14.3Seizures 1 3.6
Histology Benign 13 46.4Atypical-malignant 1 3.6No histology 14 50.0
Surgical classification ofthe meningioma
Simpson II 1 3.6Simpson III 1 3.6Simpson IV/unresectable 26 92.9
ECOG � Eastern Cooperative Oncology Group performance statusscale.
Table 2. Dosim
Variable Mean Median
PTV total volume (cc) 55.1 43.3Maximal dose received in the PTV (Gy) 54.3 53.6Minimal dose received in the PTV (Gy) 42.3 45.7Median dose received in the PTV (Gy) 52.2 51.7Monitor units 4950.1 4706.0Homogeneity index 1.06 1.05Conformity index 0.82 0.89Maximal dose to brain (Gy) 54.8 53.4Maximal dose to brainstem (Gy) 48.7 51.3Maximal dose to chiasm (Gy) 47.1 51.7Maximal dose to right optic nerve (Gy) 43.1 47.7Maximal dose to left optic nerve (Gy) 44.1 50.6Maximal dose to right eye (Gy) 18.6 13.1Maximal dose to left eye (Gy) 19.0 12.3Maximal dose to right lens (Gy) 5.8 5.1
Maximal dose to left lens (Gy) 5.7 5.0with helical tomotherapy. Median age was 57.5 years(range, 40–78); most patients were female, with EasternCooperative Oncology Group performance status scale�1. Most tumors were located at the sella turcica, fol-lowed by the cavernous sinus and the sphenoid; mostpatients were either inoperable or Simpson IV. The mostfrequently affected cranial nerve was the II pair. Themost common symptoms were derived from compromiseof the cranial nerves. Among patients with histologicdiagnosis, the most frequent classification was WHO I(Table 1).
Radiotherapy was administered as primary treat-ment in most patients, although it was also frequentlyused as an adjuvant delayed treatment or as a rescuetreatment after postsurgical progression. Three pa-tients had received radiotherapy previously. Totaldose varied between 5000 and 5400 cGy, and fraction-ation varied between 180 and 200 cGy. Target vol-umes ranged from 7.3–212.9 mL (median, 43.3 mL).Median dose to the PTV was 51.7 (range, 50.2–55.9).Median coverage index was 0.89 (range, 0.18 – 0.97)and median homogeneity index was 1.05 (range,1–1.12). The aim of covering at least 95% of the PTVwith the 95% isodose was accomplished in all pa-tients; however, the intention of achieving a minimumPTV dose of 90% and a maximum PTV dose of 105%were not accomplished for 46.4% and 50% of thepatients, respectively. Median maximal dose to thebrain was 54.8 Gy, brainstem 48.7 Gy, chiasm 47.1Gy, right optic nerve 43.1 Gy, left optic nerve 44.1 Gy,right eye 18.6 Gy, left eye 19.0 Gy, right lens 5.8 Gy,and left lens 5.7 Gy (Table 2). Representative axial,coronal, and sagittal images for typically treated pa-tients included in this series are shown in Figs 1 and 2.
Acute transient toxicity was limited to grade 1 inall patients and included headache, ocular pain/dry-ness, radiation dermatitis, and somnolence. Preexist-ing headache improved in 2 patients. Preexisting cra-nial nerve symptoms improved in 3 patients, whereas
characteristics
inimum Maximum Percentile 25 Percentile 75
7.3 212.9 24.6 65.351.4 60.6 52.3 56.19.0 52.7 40.9 47.6
50.2 55.9 51.2 53.0343.0 9015.9 3589.0 6380.0
1.01 1.12 1.04 1.060.18 0.98 0.82 0.92
51.9 60.6 52.6 57.328.8 58.9 49.5 52.96.0 57.5 50.7 52.38.7 56.5 43.7 51.4
11.9 55.4 37.2 51.64.9 57.7 9.0 25.06.1 50.8 9.1 25.51.9 10.7 4.5 6.7
etric
M
1
3.1 11.9 4.4 6.1

with t
Meningiomas close to the optic pathway ● L. SCHIAPPACASSE et al. 419
they worsened in 1 patient (Table 3). The medianfollow-up was 7.5 months (range, 1–33.6). One patienthad a radiological partial response, and the remaining27 patients showed radiological stabilization of thedisease.
The maximal radiation dose among patients withacute ocular pain/dryness was significantly higher than inpatients without ocular pain/dryness: left eye 31.5 Gy vs13.6 Gy, respectively (Mann-Whitney p-value � 0.013)and right eye 25.6 Gy vs 15.6 Gy, respectively (Mann-Whitney p-value � 0.034). Headache as acute toxicitywas not associated with coverage index, homogeneityindex, or maximal doses to the brain or brainstem.
DISCUSSION
Clinical characteristics of this group of patients aresimilar to some other groups of patients with complex-
Fig. 1. Representative dosimetry in the axial, coronalsphenoidal wing, in close contact
shaped meningiomas of the skull base, cavernous sinus,
or surgically inaccessible meningiomas in regard to fe-male:male ratio, mean age, functional status, and tumorgrade. Tumor characteristics are also similar, with greatvariability in tumor volume, high use of radiotherapy asa primary treatment, and the presence of cranial nervesymptoms or headache as the most frequently observedsymptomatology.6,11,12
Total dose and fraction size were within the ther-apeutic range. An IMRT approach tends to administerdoses to the PTV somewhat higher than prescribed inconformal radiotherapy, with a median dose to thePTV of 51.7 Gy. Although fractionation for meningi-omas can be of 1.8 –2 Gy daily, in this group ofpatients given the proximity to the optic structures, a1.8-Gy fraction size is preferred to diminish toxicity tocritical structures.13
Acute toxicity was lower than reported in other
sagittal views, showing a meningioma located in thehe eye, optic nerve, and chiasm.
, and
series of conventional IMRT for ocular pain/dryness
md
T
I
T
T
C
A
S
Medical Dosimetry Volume 36, Number 4, 2011420
(28.6% vs 50%), nausea (0% vs 50%), and emesis (0%vs 10%).4 We did not evaluate the impact of the dosesadministered to the lacrimal glands or ocular surfacebecause we did not consider them primarily as organs atrisk, and we could not estimate the values retrospec-tively, because the tomotherapy planning software doesnot allow further modifications of approved plans. How-ever, we subjectively reviewed the isodoses curves onthe treatment planning, and we found that for mostpatients, the lacrimal glands were located near to theisodose curves of 30–35 Gy, but in affected patients thelacrimal gland/ocular surface was close to the 40–50-Gyisodose curves.
The incidence of xerophthalmia has been reportedwith doses to the lacrimal gland as low as 24 Gy,14
although the incidence of chronic dry eye increasessteeply with doses �40 Gy.15 The TD 5/50 defined asthe radiation dose that would result in a 50% proba-bility of developing severe complications within 5years after treatment, for severe dry eye for the lacri-
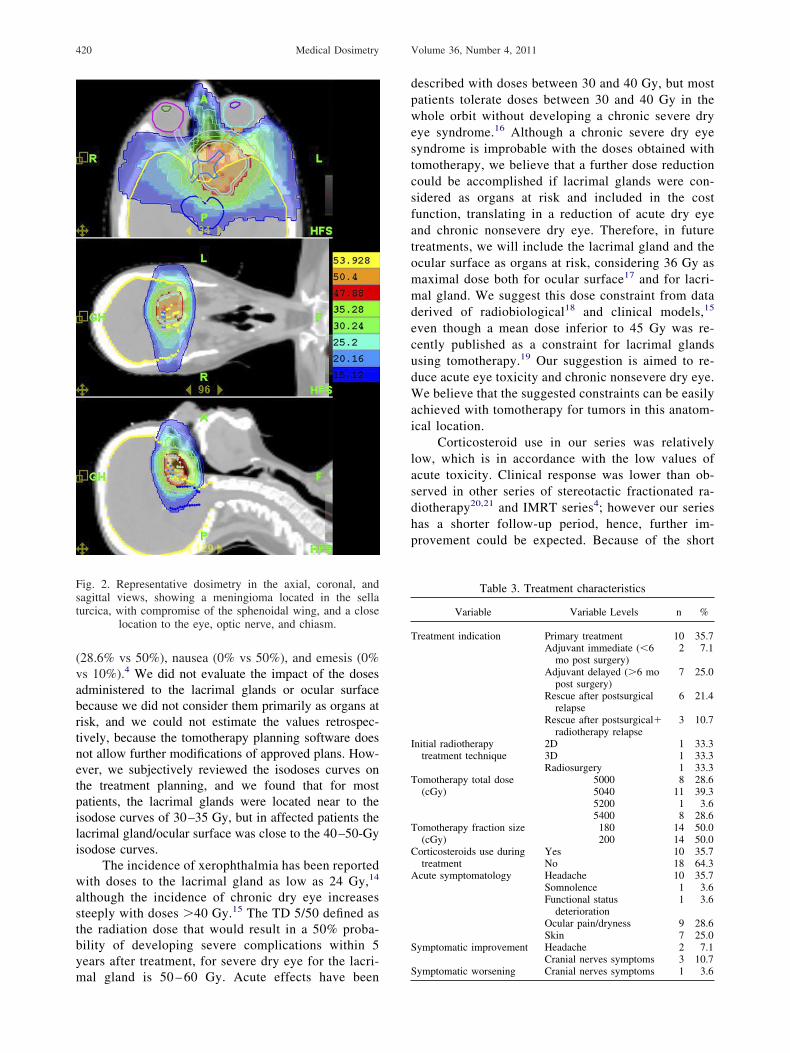
Fig. 2. Representative dosimetry in the axial, coronal, andsagittal views, showing a meningioma located in the sellaturcica, with compromise of the sphenoidal wing, and a close
location to the eye, optic nerve, and chiasm.
mal gland is 50 – 60 Gy. Acute effects have been S
described with doses between 30 and 40 Gy, but mostpatients tolerate doses between 30 and 40 Gy in thewhole orbit without developing a chronic severe dryeye syndrome.16 Although a chronic severe dry eyesyndrome is improbable with the doses obtained withtomotherapy, we believe that a further dose reductioncould be accomplished if lacrimal glands were con-sidered as organs at risk and included in the costfunction, translating in a reduction of acute dry eyeand chronic nonsevere dry eye. Therefore, in futuretreatments, we will include the lacrimal gland and theocular surface as organs at risk, considering 36 Gy asmaximal dose both for ocular surface17 and for lacri-
al gland. We suggest this dose constraint from dataerived of radiobiological18 and clinical models,15
even though a mean dose inferior to 45 Gy was re-cently published as a constraint for lacrimal glandsusing tomotherapy.19 Our suggestion is aimed to re-duce acute eye toxicity and chronic nonsevere dry eye.We believe that the suggested constraints can be easilyachieved with tomotherapy for tumors in this anatom-ical location.
Corticosteroid use in our series was relativelylow, which is in accordance with the low values ofacute toxicity. Clinical response was lower than ob-served in other series of stereotactic fractionated ra-diotherapy20,21 and IMRT series4; however our serieshas a shorter follow-up period, hence, further im-provement could be expected. Because of the short
Table 3. Treatment characteristics
Variable Variable Levels n %
reatment indication Primary treatment 10 35.7Adjuvant immediate (�6
mo post surgery)2 7.1
Adjuvant delayed (�6 mopost surgery)
7 25.0
Rescue after postsurgicalrelapse
6 21.4
Rescue after postsurgical�radiotherapy relapse
3 10.7
nitial radiotherapytreatment technique
2D 1 33.33D 1 33.3Radiosurgery 1 33.3
omotherapy total dose(cGy)
5000 8 28.65040 11 39.35200 1 3.65400 8 28.6
omotherapy fraction size(cGy)
180 14 50.0200 14 50.0
orticosteroids use duringtreatment
Yes 10 35.7No 18 64.3
cute symptomatology Headache 10 35.7Somnolence 1 3.6Functional status
deterioration1 3.6
Ocular pain/dryness 9 28.6Skin 7 25.0
ymptomatic improvement Headache 2 7.1Cranial nerves symptoms 3 10.7
ymptomatic worsening Cranial nerves symptoms 1 3.6

ctmpatttdciivdgdvu
ac
1
1
1
1
1
1
1
1
1
Meningiomas close to the optic pathway ● L. SCHIAPPACASSE et al. 421
follow-up period, the report of late morbidity is lim-ited on this series.
The lack of accomplishment of the planning ob-jectives reflects the balance we had to deal with toachieve the constraints for the organs at risk whiletrying to keep the prescription in the PTV in a groupof patients with tumors located very closely or eveninvading the organs at risk. Homogeneity index wasvery close to the ideal value (1), expressing a homo-geneous dose with low incidence of “hot spots” in theirradiated area. Excepting one previously irradiatedpatient, with a very complex volume and a coverageindex of 0.18, the coverage index was close to the unitfor most of the remaining patients, expressing a ho-mogeneous dose with low incidence of “cold spots” inthe treatment area. After excluding this value, themean coverage index increased from 0.81– 0.85, al-though the median value for coverage index remainedunchanged at 0.89.
Meningioma treatment requires a multidisciplinaryteam approach, including neurosurgeons, radiologists,and radiation oncologists. Surgery is the preferred treat-ment, but when a complete resection is unfeasible, thereis a high recurrence risk22; therefore, radiotherapy be-omes an option as primary or adjuvant treatment. Al-hough radiosurgery is the preferred radiotherapy treat-ent technique, in cases of tumors located in the
roximity of the optic pathway, it becomes impractical asresult of limiting doses of these visual structures added
o the fact of maximal tumor volume constraints of theechnique. Our study demonstrates that tomotherapy is aechnique with high capabilities of intensity modulation,espite the complexity of the tumor shape, with higheroverage and homogeneity indexes than those observedn conformal treatments23 and high capabilities for spar-ng the organs at risk. Daily image guidance with mega-oltage CT guarantees an accurate and precise treatmentelivery, providing a safe and effective alternative in thisroup of therapeutically challenging patients in whom,espite the facial mask use, it has been proved that setupariations range from 1–2 mm in translational errors andp to 1 degree in rotational errors.24,25
Technology advances have represented an im-provement in the treatment of meningiomas since theuse of CT and MRI for volume definition, enhancedconformal capabilities using conformal radiotherapyand IMRT, and, finally, tomotherapy as a techniquemerging advances in modulation capabilities and im-age guidance as an important component of a highlyconformal IMRT treatment administered in a criticalanatomical area.
CONCLUSION
Tomotherapy is a technique capable of deliveringwell-tolerated treatment with high homogeneity and
overage indexes and high capabilities for sparing the
organs at risk in patients with meningiomas close tothe optic pathway. Tomotherapy can be used as aprimary or adjuvant treatment when surgery or radio-surgery are not feasible. A longer follow-up is re-quired to appropriately evaluate late toxicity and tu-moral response.
This study was supported by the Instituto Madrilenode Oncologia (IMO) Foundation Group.
REFERENCES
1. Bondy, M.; Ligon, B.L. Epidemiology and etiology of intracranialmeningiomas: a review. J. Neurol. Oncol. 29:197–205; 1996.
2. Whittle, I.R.; Smith, C.; Navoo, P.; et al. Meningiomas. Lancet.363:1535–43; 2004.
3. Uy, N.W.; Woo, S.Y.; Teh, B.S.; et al. Intensity-modulated radi-ation therapy (IMRT) for meningioma. Int. J. Radiat. Oncol. Biol.Phys. 53:1265–70; 2002.
4. Pirzkall, A.; Debus, J.; Haering, P.; et al. Intensity modulatedradiotherapy (IMRT) for recurrent, residual, or untreated skull-base meningiomas: preliminary clinical experience. Int. J. Radiat.Oncol. Biol. Phys. 55:362–72; 2003.
5. Milker-Zabel, S.; Zabel-du Bois, A.; Huber, P.; et al. Intensity-modulated radiotherapy for complex-shaped meningioma of theskull base: long-term experience of a single institution. Int. J.Radiat. Oncol. Biol. Phys. 68:858–63; 2007.
6. Pirzkall, A.; Carol, M.; Lohr, F.; et al. Comparison of intensity-modulated radiotherapy with conventional conformal radiotherapyfor complex-shaped tumors. Int. J. Radiat. Oncol. Biol. Phys.48:1371–80; 2000.
7. Beavis, A.W. Is Tomotherapy the future of IMRT? Br. J. Radiol.77:285–95; 2004.
8. Fogliata, A.; Clivio, A.; Nicolini, G.; et al. Intensity modulationwith photons for benign intracranial tumours: a planning compar-ison of volumetric single arc, helical arc and fixed gantry tech-niques. Radiother. Oncol. 89:254–62; 2008.
9. Yartsev, S.; Kron, T.; Cozzi, L.; et al. Tomotherapy planning ofsmall brain tumours. Radiother. Oncol. 74:49–52; 2005.
0. Kantor, G.; Mahé, M.A.; Giraud, P.; et al. [Helical Tomo-therapy: general methodology for clinical and dosimetric eval-uation (national French project)]. Cancer. Radiother. 10:488 –91; 2006.
1. Metellus, P.; Batra, S.; Karkar, S.; et al. Fractionated conformalradiotherapy in the management of cavernous sinus meningiomas:long-term functional outcome and Tumor Control at a SingleInstitution. Int. J. Radiat. Oncol. Biol. Phys.; 2010 Febr 2 [Epubahead of print].
2. Korah, M.P.; Nowlan, A.W.; Johnstone, P.A.; et al. Radiationtherapy alone for imaging-defined meningiomas. Int. J. Radiat.Oncol. Biol. Phys. 76:181–6; 2010.
3. Mayo, C.; Martel, M.K.; Marks, L.B.; et al. Radiation dose-volumeeffects of optic nerves and chiasm. Int. J. Radiat. Oncol. Biol.Phys. 76(3 Suppl):S28–S35; 2010.
4. Kennerdell, J.S.; Flores, N.E., Hartsock, R.J. Low-dose radiother-apy for lymphoid lesions of the orbit and ocular adnexa. Ophthal.Plast. Reconstr. Surg. 15:129–33; 1999.
5. Parsons, J.T.; Bova, F.J.; Fitzgerald, C.R.; et al. Severe dry-eyesyndrome following external beam irradiation. Int. J. Radiat. On-col. Biol. Phys. 30:775–80; 1994.
6. Gordon, K.B.; Char, D.H., Sagerman, R.H. Late effects of radia-tion on the eye and ocular adnexa. Int. J. Radiat. Oncol. Biol. Phys.31:1123–39; 1995.
7. Durkin, S.R.; Roos, D.; Higgs, B.; et al. Ophthalmic and adnexalcomplications of radiotherapy. Acta Ophthalmol. Scand. 85:240–50; 2007.
8. Bhandare, N.; Moiseenko, V.; Song, W.; et al. 2498 poster.Severe dry-eye syndrome after radiation therapy: radiobiologi-cal modeling. Int. J. Radiat. Oncol. Biol. Phys. 78(Suppl):
S425– 6; 2010.
2
Medical Dosimetry Volume 36, Number 4, 2011422
19. Chen, A.M.; Sreeraman, R.; Mathai, M.; et al. Potential of helicalTomotherapy to reduce dose to the ocular structures for patientstreated for unresectable sinonasal cancer. Am. J. Clin. Oncol.; 2010May 3 [Epub ahead of print].
20. Brell, M.; Villà, S.; Teixidor, P.; et al. Fractionated stereotacticradiotherapy in the treatment of exclusive cavernous sinus menin-gioma: functional outcome, local control, and tolerance. Surg.Neurol. 65:28–33, discussion 33–4; 2006.
21. Milker-Zabel, S.; Zabel-du Bois, A.; Huber, P.; et al. Fractionatedstereotactic radiation therapy in the management of benign cav-
ernous sinus meningiomas: long-term experience and review of theliterature. Strahlenther. Onkol. 182:635–40; 2006.22. Simpson, D. The recurrence of intracranial meningiomas after surgicaltreatment. J. Neurol. Neurosurg. Psychiatry. 20:22–39; 1957.
23. Selch, M.T.; Ahn, E.; Laskari, A.; et al. Stereotactic radiotherapyfor treatment of cavernous sinus meningiomas. Int. J. Radiat.Oncol. Biol. Phys. 59:101–11; 2004.
24. Vaandering, A.; Lee, J.A.; Renard, L.; et al. Evaluation of MVCTprotocols for brain and head and neck tumor patients treated withhelical Tomotherapy. Radiother. Oncol. 93:50–6; 2009.
5. Schubert, L.K.; Westerly, D.C.; Tomé, W.A.; et al. A comprehen-sive assessment by tumor site of patient setup using daily MVCT
imaging from more than 3,800 helical Tomotherapy treatments.Int. J. Radiat. Oncol. Biol. Phys. 73:1260–9; 2009.