Embed Size (px)
Citation preview

Preliminary Evidence Of Anti Tumor Activity Of Selinexor (KPT-330) In a Phase I Trial Of a First-In-Class Oral
Selective Inhibitor Of Nuclear Export (SINE) In Patients With Relapsed / Refractory Non Hodgkin’s Lymphoma
(NHL) and Chronic Lymphocytic Leukemia (CLL) John Kuruvilla, MD1, Martin Gutierrez, MD2, Bijal D. Shah, MD3, Nashat Y. Gabrail, MD4, Peter de Nully Brown5, Richard M. Stone, MD6, Ramiro Garzon, MD7, Michael Savona, MD8, David S. Siegel, MD, PhD2, Rachid Baz, MD3, Morten Mau-Sorensen, MD5, Matthew S. Davids, MD6, John C. Byrd, MD7, Sharon Shacham, PhD, MBA9, Tami Rashal, MD9, Cindy YF Yau10, Dilara McCauley, PhD9, Jean-Richard Saint-Martin9, John McCartney, PhD9, Yosef Landesman, PhD9, Boris Klebanov9, Trinayan Kashyap9, Eran Shacham9, Greg Pond, PhD10, Amit M. Oza, MBBS, MD10, Michael Kauffman, MD, PhD9 and Mansoor R Mirza5
� a� h� t 2� � � �2 � 2 � � E) xX� � � � � t t 3�s � � � 0t � i� � a� h� t 2� � � � �2 �� Ph� 2 � � ad � a2u� d� � 2 � � �32 dai�
Copyright ©2013 American
Society of Hematology
Contact Us | Terms of Service |
Privacy Policy | RSS
Connect with us
1Princess Margaret Cancer Centre, University of Toronto, Toronto, ON, Canada 2John Theurer Cancer Center, Hackensack University Medical Center, Hackensack, NJ 3H. Lee Moffitt Cancer Center & Research Institute, Tampa, FL 4Gabrail Cancer Center, Canton, OH 5Copenhagen University Hospital, Copenhagen, Denmark 6Dana-Farber Cancer Institute, Harvard Medical School, Boston, MA 7The Ohio State University Comprehensive Cancer Center, Columbus, OH 8Sarah Cannon Research Institute, Nashville, TN 9Karyopharm Therapeutics Inc, Natick, MA 10Ozmosis Research, Toronto, ON, Canada

Presenter Disclosures
• Employment or Leadership Posi3on: None
• Consultant/Advisory Role: None
• Stock Ownership: None
• Honoraria: Hoffman LaRoche, Janssen, Celgene, Lundbeck, SeaFle Gene3cs
• Research Funding: Leukemia and Lymphoma Society
• Expert Tes3mony: None
• Other Remunera3on: None

Selective Inhibitors of Nuclear Export (SINE) o Cancer cells can inac5vate their
Tumor Suppressor Proteins (TSPs) via nuclear export
o Expor5n 1 (XPO1, CRM1) is the only nuclear exporter of most TSPs
o XPO1 is elevated in Non-‐Hodgkin’s Lymphoma (NHL), Chronic Lymphocy5c Leukemia (CLL) and other hematological malignancies
o Selinexor (KPT-‐330) is a covalent, oral selec5ve inhibitor of nuclear export (SINE) XPO1 antagonist that forces nuclear reten5on and ac5va5on of mul'ple TSPs
o Selinexor shows robust an5-‐cancer ac5vity in mul5ple preclinical models of NHL and CLL
o First in class, first in human phase 1 study of oral Selinexor (NCT01607892)

p73
Ki-67
SINE Reduce Growth of DLBCL in Vivo: Induction of p73 and Bax in p53mut DLBCL
*Azmi 2013 Department of Pathology, Wayne State University, Detroit, Michigan

KPT-330: Effects on TCL-1 CLL Leukemograft Model
*Lapalombella 2012 Department of Internal Medicine, The Ohio State University, Columbus Ohio
TCL1-SCID mice (N=10 each group) treated orally with: KPT-330 5 or 15 mg/kg or vehicle control twice per week (BIW; Monday and Tuesday). Treatment was initiated 14 days post engraftment
Peripheral blood count (PBL)

� � � � po� � 3� � � l � � ymld� � : � � � � �
� � 3� � h� � � h� � � � �
� � � � po� � 3� � � l � � ymld� � : � � � � �
� � � �
� � 3� � h� � � � � � � � � �
� mo� � � o� � � � emE� � m� mlyo� � mo� � � ap� Eo� mE� � m� mlyo�
� � y� � � d� � m� � � oe � � � � � � � � �
� : � � � � � � d p� m � �
� l � c �
� l � k�
� l � O�
� � 3� � h� � � h� � � � �� � 3� � h� � � h� � � � � � � 3� � h� � � � � � � � � �
� � � � po� � 3� � � l � � ymld� � : � � � � �
� � 3� � h� � � h� � � � �
� � � � po� � 3� � � l � � ymld� � : � � � � �
� � 3� � h� � � h� � � � �� � 3� � h� � � h� � � � �
C� � � u�
� � � � C� :� ml � � : � � � � u�� l � w�
� l � H�� � � � C� � � � � � l � y� � 3� � � oyu�
KPT-330 Phase 1 Haematological Malignancies Study Design (NCT01607892)�

KPT-330 Ph1 Study Design • Objec5ves (modified 3+3 design)
– Primary: Safety, tolerability and Recommended Phase 2 Dose (RP2D) of KPT-‐330;
– Secondary: Pharmacokine5cs (PK), pharmacodynamics (PDn), an5-‐tumor response; conforma5on of RP2D of KPT-‐330
• KPT-‐330 dosing – Oral on days 1, 3, 5 or days 1, 3 of each week – Doses 3mg/m2 – 45mg/m2
• Major eligibility criteria:
– Pa5ents (ECOG ≤1) with relapsed/refractory hematologic tumors with no available standard treatments
– Documented progression at study entry – ANC >1000/µL, Platelets >30,000/µL

KPT-330 Ph1: DLT Criteria • ≥ 3 missed doses in 28 days at target dose • Discontinuation of a patient due to a toxicity in Cycle 1 • Non Hematologic:
– Grade ≥3 (nausea/vomiting, electrolyte imbalances must be supported first and AST/ALT lasting more than 7 days)
– Grade ≥3 fatigue lasting ≥5 days while taking supportive care
• Hematologic: – Grade 4 neutropenia ≥7 days – Febrile neutropenia – Grade 4 thrombocytopenia that persists for ≥5 days, or
Grade ≥3 with bleeding

KPT-330 Ph1 Study: Patient Characteristics
Characteristic N=30
Median age (range) 65 years (32-‐79)
Male /Female 19 Males : 11 Females
Median prior lines of treatment (range) 4.5 (1-‐11)
ECOG performance status, 0/1 9 : 21
Non-Hodgkin’s Lymphoma -Follicular -Mantle Cell -Diffuse Large B Cell (DLBLC) -Transformed Chronic Lymphocytic Leukemia (CLL) Richter’s Syndrome
6 Patients 3 Patients 11 Patients 2 Patients
4 Patients
4 Patients

KPT-330 Ph1 Study: Dose Levels, DLT and MTD
Cohort #
Dose Level
(mg/m2)
Doses per cycle
DLT Evaluable Pa3ents (n=28)
Pa3ents with DLT
Dose Limi3ng Toxicity
1 3 10 2 0
2 6 10 3 0
3 12 10 5 0
4 16.8 10 7
1 MM: Grade 4 thrombocytopenia (pt con5nued on therapy >1 year)
5 23 10 7 1 FL: Grade 4 thrombocytopenia (pt con5nued on therapy 4 months)
6 30 10 5 0
7 35 8 3 0
8 45 8 2 0 Ongoing
Expansion 35 8 14 – DLBCL, MM, WM
All patients in Arm1 (NHL, CLL, MM and WM) were included for DLT evaluation

KPT-330 Ph1 Study: Hematological Drug Related Adverse Events
Grade&1 !! !! !! 1#(50%) !! !! !! 1#(33%) 7%Grade&2 !! !! !! !! !! 1#(17%) !! !! 3%Grade&3 !! !! 1#(33%) !! !! 2#(33%) !! !! 10%Grade&4 !! !! !! !! 2#(33%) 1#(17%) 1#(12.5%) 1#(33%) 17%Grade&1 !! !! !! !! 1#(17%) !! !! 3%Grade&2 !! !! !! !! !! !! !! 1#(33%) 3%Grade&3 !! 1#(100%) 1#(33%) !! !! 4#(67%) 1#(12.5%) !! 23%Grade&4 !! !! !! !! !! !! 2#(25%) !! 7%Grade&1 !! !! 1#(33%) !! !! !! !! !! 3%Grade&2 !! !! !! 1#(50%) 1#(17%) 1#(17%) !! 1#(33%) 13%
&Neutropenia
&Anemia
Thrombocytopenia
N=3
35 45
Hematological N=1 N=1 N=3 N=2 N=6 N=6 N=8
AE&NAME GRADESelinexor&(KPTL330)&Dose&Levels&(mg/m2)
All&N=30
3 6 12 16.8 23 30
KPT-330 related AEs occurring in ≥ 2 patients

KPT-330 Ph1 Study: Non Hematological Drug Related Adverse Events
KPT-330 related AEs occurring in ≥ 2 patients
Grade&1 1"(100%) '' 1"(33%) '' 1"(17%) 3"(50%) 2"(25%) 2"(67%) 33%Grade2 '' 1"(100%) 1"(33%) 1"(50%) 1"(17%) '' 2"(25%) 1"(33%) 23%Grade&1 1"(100%) '' 2"(67%) 1"(50%) 2"(33%) 3"(50%) 5"(62.5%) 2"(67%) 53%Grade2 '' 1"(100%) '' '' '' 1"(17%) '' 1"(33%) 10%Grade&1 1"(100%) '' 1"(33%) '' '' 1"(17%) 4"(50%) 1"(33%) 27%Grade2 '' 1"(100%) '' 1"(50%) 1"(17%) '' 2"(25%) 1"(33%) 20%Grade&3 '' '' '' '' 1"(17%) 2"(66%) '' '' 10%Grade&1 '' 1"(100%) '' '' 2"(33%) 2"(33%) 3"(37.5%) 1"(33%) 30%Grade2 '' '' '' '' '' 1"(17%) '' 1"(33%) 7%Grade&1 '' 1"(100%) 1"(33%) 1"(50%) 1"(17%) 2"(50%) 4"(50%) '' 33%Grade2 '' '' '' '' '' 1"(17%) '' '' 3%Grade&1 '' 1"(100%) 1"(33%) '' '' 1"(17%) '' '' 10%Grade2 '' '' 1"(33%) '' '' '' '' '' 3%Grade&1 '' 1"(100%) '' 1"(50%) '' '' '' '' 7%Grade2 '' '' 1"(33%) '' '' '' '' '' 3%
&Dizziness Grade&1 '' '' '' '' 1"(17%) '' 1"(12.5%) 1"(33%) 10%&Hyponatremia Grade&1 '' '' '' 1"(50%) '' '' 1"(12.5%) 1"(33%) 10%
Grade&1 '' '' '' 1"(50%) '' '' 2"(25%) '' 10%Grade2 '' '' '' '' '' 1"(17%) '' '' 3%
N=8
AE&NAME GRADESelinexor&(KPTG330)&Dose&Levels&(mg/m2)
3 6 12
N=1 N=3 N=2 N=6 N=6 N=3
&Anorexia
&Nausea
&Fatigue
&Vomiting
&Diarrhea
All&N=30
16.8 23 30 35 45
Gastrointestinal,&Constitutional,&and&Others& N=1
&Blurred&vision
&Weight&loss
&Malaise
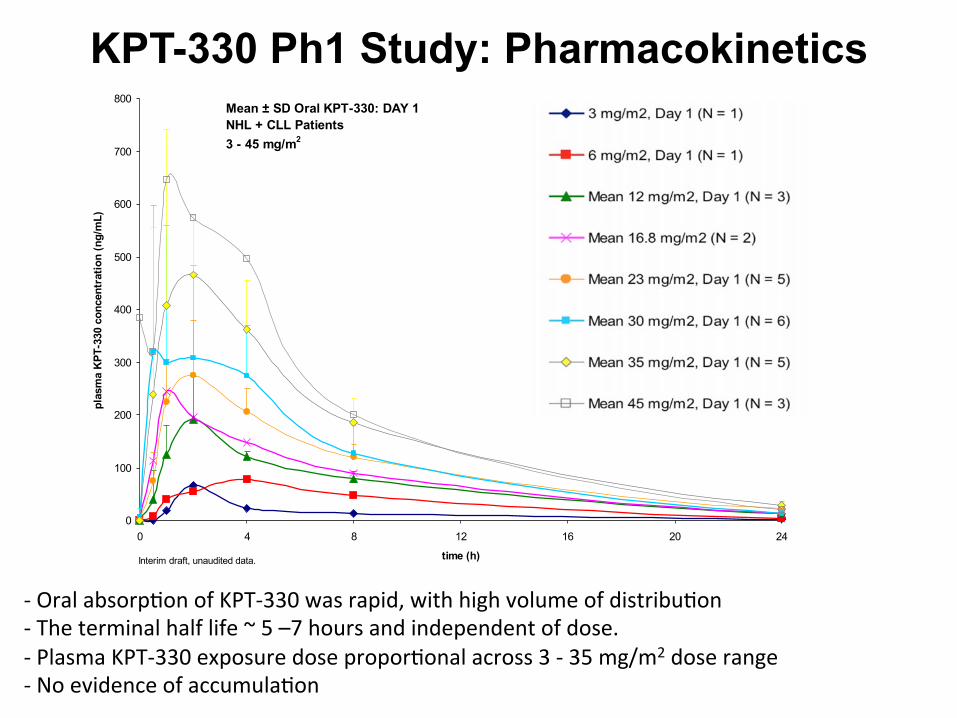
KPT-330 Ph1 Study: Pharmacokinetics
-‐ Oral absorp5on of KPT-‐330 was rapid, with high volume of distribu5on -‐ The terminal half life ~ 5 –7 hours and independent of dose. -‐ Plasma KPT-‐330 exposure dose propor5onal across 3 -‐ 35 mg/m2 dose range -‐ No evidence of accumula5on
0
100
200
300
400
500
600
700
800
0 4 8 12 16 20 24
time (h)
plas
ma
KPT
-330
con
cent
ratio
n (n
g/m
L)3 mg/m2, Day 1 (N = 1)
6 mg/m2, Day 1 (N = 1)
Mean 12 mg/m2, Day 1 (N = 3)
Mean 16.8 mg/m2 (N = 2)
Mean 23 mg/m2, Day 1 (N = 5)
Mean 30 mg/m2, Day 1 (N = 6)
Mean 35 mg/m2, Day 1 (N = 5)
Mean 45 mg/m2, Day 1 (N = 3)
Some subjects at doses > 12 mg/m2 dose levels receive a 1-week run-in at 12 mg/m2 before dose is escalated to target on Day 1.
Mean ± SD Oral KPT-330: DAY 1NHL + CLL Patients3 - 45 mg/m2
Interim draft, unaudited data.

KPT-330 Ph1 Study: Changes in XPO1 mRNA in Leukocytes
• XPO1 mRNA was measured in leukocytes from NHL patients using qRT-PCR
• Selinexor induced XPO1 expression at least 2-fold in 88% (15/17) of NHL patients
• XPO1 induction was time dependent and sustained for at least 48 h
12 4 8 24 480
1
2
3
4
5
6
7
Time (hours after KPT-330 administration)
XPO
1 ex
pres
sion
in le
ukoc
ytes
(F
old
pred
ose
leve
l)
XPO1 induction in leukocytes of NHL patients
Single oral dose of 30 mg/m2 KPT-330
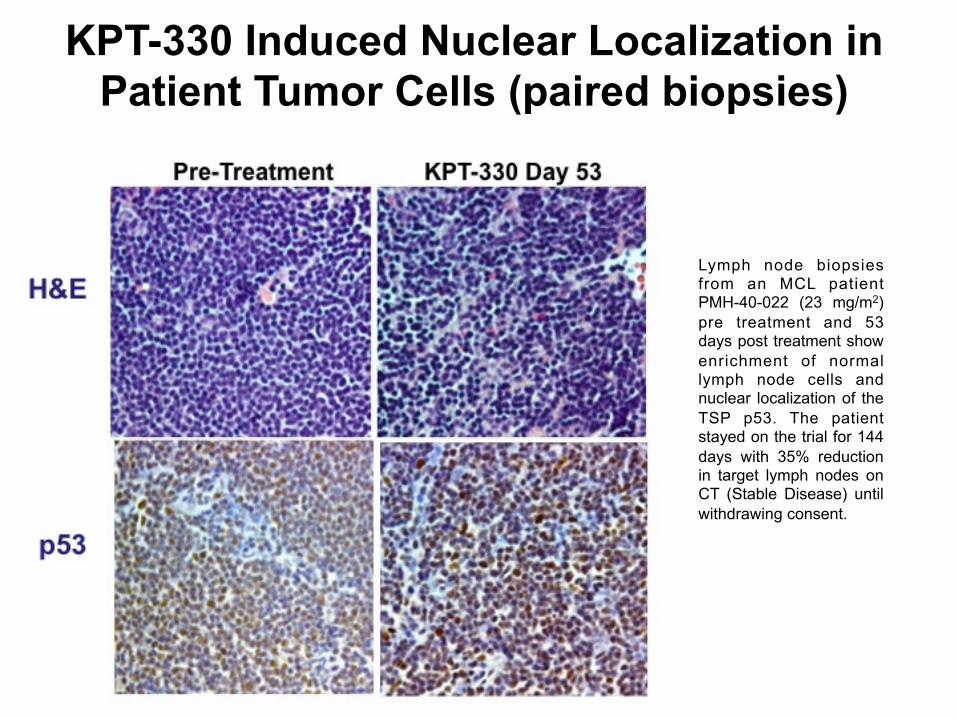
KPT-330 Induced Nuclear Localization in Patient Tumor Cells (paired biopsies)
Lymph node biopsies from an MCL patient PMH-40-022 (23 mg/m2) pre treatment and 53 days post treatment show enrichment of normal lymph node cells and nuclear localization of the TSP p53. The patient stayed on the trial for 144 days with 35% reduction in target lymph nodes on CT (Stable Disease) until withdrawing consent.
Pre-Treatment KPT-330 Day 53

KPT-330 Ph1 Study: Responses in Heavily Pretreated CLL & NHL
Responses in NHL/CLL/Ricther's Syndrome Pa5ents as of 4-‐Dec-‐2013
Cancer Number of Pts Evaluated
Total PRs and SDs (%) PR (%) SD (%) PD WC NE
CLL 4 4 (100%) 2 (50%) 2 (50%) -‐-‐ -‐-‐ -‐-‐
Richter's Syndrome 4 4 (100%) 1 (25%) 3 (75%) -‐-‐ -‐-‐ -‐-‐
NHL
DLBCL 11 10 (91%) 3 (27%) 5 (45%) 2 (18%) -‐-‐ 1 (9%)
MCL 3 2 (67%) 1 (33%) 1 (33%) -‐-‐ -‐-‐ 1 (33%)
FL 6 5 (83%) 1 (17%) 4 (66%) -‐-‐ 1 (17%) -‐-‐
Transformed 2 -‐-‐ -‐-‐ -‐-‐ 2 (100%) -‐-‐ -‐-‐
Total 30 24 (80%) 8 (27%) 15 (50%) 4 (13%) 1 (3.3%) 2 (6.7%)

KPT-330 Ph1 Study: Maximal % Change in Lymph Node from Baseline
� � � � � �
� � � � � �
� � �� � � �
� � � � � � � P� 2� avh�
� � � �� � � � � �
� � � � � � � P� 2� avh�
� � � �
� � � � � � � � � � � �
� � � �
� � � � � �yx) ) b �
y’ ) b �
yk) b �
y-‐ ) b �
yR) b �
y, ) b �
yO) b �
yX) b �
yE) b �
yx) b �
) b �
x) b �
E) b �
X) b �
O) b �
��a�
���F����
E����lm
���o���E��
Partial Response
Stable Disease
� � � � � �
Stable Disease
* Two patients with DLBCL and two patients with transformed FL had clinical progression in cycle 1

KPT-330 Ph1 : Patient Outcomes & Time on Study (n=28)
Transf'd NHL 35 mg/m2 BIW
FL 45mg/m2 BIW
Transf'd NHL 12 mg/m2
DLBCL 23 mg/m2
DLBCL 16.8 mg/m2
CLL/Richter's 30 mg/m2
CLL (Richter's transform) 23 mg/m2 Sched 4
CLL (Richter's transform) 23 mg/m2 Sched 4
DLBCL 35 mg/m2 BIW
DLBCL (Mediastinal) 35 mg/m2 BIW
DLBCL 35 mg/m2 BIW
CLL 30 mg/m2
DLBCL 35 mg/m2 BIW
CLL 35mg/m2 BIW ->QW
CLL 45mg/m2 BIW
DLBCL 23 mg/m2 Sched 4-> 30 mg/m2 Sched 3
FL 23 mg/m2
DLBCL 3 mg/m2
FL 12 mg/m2
FL 30 mg/m2
MCL 23 mg/m2-> BIW
FL 30 mg/m2 BIW (exp)
MCL 12 mg/m2
FL 35->25 mg/m2 BIW
DLBCL 30mg/m2
CLL 30-> BIW mg/m2
CLL 16.8->30 mg/m2
� � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � �
� � � � � �� � � � � �� � � � � �� � � � � �� � � � � �� � � � � � �� � � � � �� � � � � � �� � � � � �� � � � �� � � � �� � � � � �� � � � � �� � � � � � �� � � � � �� � � � � �� � � � � � �� � � � � � �� � � � � � �� � � � � �� � � � � � �� � � � � � �� � � � � �� � � � � � �� � � � � �� � � � � � �� � � � � � �� � � � � � �
� � � � � � � � � � �On Study (Stable Disease) Withdrew Consent Progression Partial Response
CLL (Richter's transform) 23 mg/m2 Sched 4
CLL/Richter's 30 mg/m2
Stem Cell Transplantation
CLL (Richter's transform) 23 mg/m2 Sched 4 (LN –36%)
(LN –60%)
(LN –40%) CLL 30 mg/m2
CLL 35mg/m2 BIW ->QW (LN –85%)
(LN –74%)
(LN –72%)
(LN –44%)
DLBCL 3 mg/m2 DLBCL 3 mg/m2
(LN –17%)
FL 30 mg/m2
(LN –17%)
(LN –36%)
(LN –32%)
(LN –57%)
(LN –55%)
(LN –11%)
(LN –64%)
DLBCL 471 days (LN –93%)
(LN –21%)
(LN –44%)
* 2 patients were non-evaluable

KPT-330 Ph1 : Progression Free Survival
0 60 120 180 240 300 3600
10
20
30
40
50
60
70
80
90
100
110
Time (Days)
Prog
ressio
n Free
Survi
val (P
FS)
Censored for Non-Progression
# Days On Study 7 15 20 23 30 32 38 52 58 60 86 113 143 144 158 168 179 186 273 445
# Pts On Study 29 27 26 22 19 18 17 15 14 13 10 9 8 6 5 4 3 2 1 0
# Pts At Risk 29 28 27 24 22 21 20 18 17 16 15 14 13 11 10 9 8 7 6 5
Details 1 2 3 3,5,5 6,4,2 5 2 5 2 2 2 4 5 3,5 5 5 5 5 2 2
Notes: 1= WC death unrelated 2= WC low grade tox 3= WC infection 4= Transplant 5= On Study 6= PD
Censored for Non-Progression and Death
Time on Study (Days)
Prog
ress
ion
Free
Sur
viva
l (PF
S)

Case Study: Patient 040-003: Refractory Diffuse Large B-Cell Lymphoma (DLBCL)
• 53 year old man with Primary Refractory DLBCL (Dec 2010) • Stage 4, IPI2 (elevated LDH), bulky disease • Refractory (PD) to primary therapy and transplant • Salvage radia5on to abdominal mass, PD to salvage (GDP) • Dec 2011-‐Aug 2012 – 20mg prednisone + weekly XRT
– Marked peripheral edema (3+) due to abd/pelvic mass, pancytopenia
• Response in Cycle 2; currently Cycle 16 – Began Selinexor Aug 20 2012: PR aler Cycle 2 (67% response) – 93% response on 12mg/m2 aler Cycles 12 -‐ 16 – Marked reduc5on in peripheral edema
– Minimal side effects, con5nues on single agent Selinexor

Patient 040-003 DLBCL
Baseline PET/CT Cycle 12 PET/CT (–93%)

Case Study 040-027: BTK Inhibitor Refractory CLL with Richter’s (DLBCL) Transformation
• Patient with CLL treated initially Jan 2010 with FCR • Recurred Dec 2010, treated with Bendamustine-Rituxan • Ofatumumab Feb 2011 (PD) • CHOP April 2011 (PD) • Revlimid + Flavoperidol Jul 2011 (NR) • Ibrutinib (BTK Inhibitor) Feb 2012 – Feb 2013 then PD with
Richter’s Transformation • Received Oxaliplatin, AraC, Fludarabine, Rituxan x 1 then PD • Began KPT-330 30mg/m2 (10X/cycle) – 60% PR in Cycle 1;
main side effect Grade 2 fatigue, anorexia • Following marked response to KPT-330, sent to transplant and
T-cell vaccine (experimental)

Case Study: Patient 040-046: Refractory Diffuse Large B-Cell Lymphoma (DLBCL)
• 73 year old man with Refractory DLBCL (Feb 2012) • Stage 4, bulky disease, possible CNS involvement
• CHOP-R initial therapy + intrathecal (CNS) metho-trexate + radiation to R arm with relapse in 10 months
• R-ICE treatment (Jan-Feb 2013) with relapse within 7 months
• Pain, marked edema in R arm (massive lesion)
• Sept 17, 2013 initiates Selinexor 20mg/m2 qd x 2
• Response within 2 weeks with marked reduction in pain and edema in arm
• MRI: 73% reduction in cycles 1 & 2
• Well tolerated (Remeron + Megace) with minimal side effects, increased dose in Cycle 3

Rel/Ref DLBCL 040-046: Rapid Partial Response (PR), bulky R arm lesion
R Arm Baseline: Sept 16, 2013 Cycle 1: October 13, 2013
6.89 x 4.73 cm (32.59cm2) 4.30 x 2.12 cm (9.12 cm2)

Conclusions
• Novel, oral SINE Selinexor (KPT-330) can safely be given as monotherapy to patients with advanced NHL/CLL – Main toxicities: fatigue, anorexia, nausea, thrombocytopenia – MTD has not been reached; currently dosing at 45mg/m2 BIW – Patients remaining on single agent Selinexor >9 months
• Selinexor has favorable PK and PD characteristics
• Signs of single-agent anti-tumor activity in heavily pre-treated patients with durable cancer control >9 months
• Expansion cohort in DLBCL (and MM) is ongoing, with future
trials in Richter’s syndrome and DLBCL planned

Acknowledgments • We would like to thank:
– Patients and their families – Investigators, co-investigators and the study
teams at each participating center • Princess Margaret Cancer Centre,
Toronto • Rigshospitalet, Copenhagen • Moffitt Cancer Centre, Tampa • Dana Farber Cancer Institute • Gabrail Cancer Center Research • Hackensack University Hospital • Sarah Cannon Research Institute • The Ohio State University • Tom Baker Cancer Centre • Washington University; St Louis, MO
The study was sponsored by Karyopharm Therapeutics Inc.






















![CD8+ Tumor-Infiltrating T Cells Are Trapped in the Tumor … · 2016. 12. 19. · tumor cells induces immunogenic cross-presentation of dying tumor cells [4,5] or sensitizing tumor](https://img.pdfslide.us/doc/110x75/5fbd8f04c0953e25272e83ca/cd8-tumor-infiltrating-t-cells-are-trapped-in-the-tumor-2016-12-19-tumor-cells.jpg)






![[PPT]TUMOR TRAKTUS UROGENITAL - FK UWKS 2012 C | … · Web viewTUMOR TRAKTUS UROGENITAL I. Tumor Ginjal A. Tumor Grawitz B. Tumor Wilms II. Tumor Urotel III. Tumor Testis IV. Karsinoma](https://img.pdfslide.us/doc/110x75/5ade93b87f8b9ad66b8bb718/ppttumor-traktus-urogenital-fk-uwks-2012-c-viewtumor-traktus-urogenital.jpg)