Embed Size (px)
Citation preview

Human Reproduction vol.7 no.5 pp.701-710, 1992
REVIEW
Pregnancy tests: a review
T.ChardDepartment of Reproductive Physiology, and Obstetrics andGynaecology, St Bartholomew's Hospital Medical College, and theLondon Hospital Medical College, London, UK
Pregnancy tests are widely used both by the public andby healthcare professionals. All tests depend on themeasurement of human chorionk gonadotrophin (HCG) inurine. Other pregnancy-specific materials have been proposedas pregnancy tests but none can better the sensitivity andconvenience offered by immunoassay of HCG. Ultrasounddetection is also not as sensitive as HCG measurement. Thecurrent generation of tests is based on monoclonal antibodiesto the beta-subunit of HCG; these virtually eliminate thepossibility of cross-reaction with pituitary hiteinizing hormone(LH) and it is this feature which permits the high sensitivity.However, it is important to recognize that the 'beta-subunit'antibody reacts with both intact HCG, which is the majorcomponent in pregnancy serum, and with fragments of thebeta-subunit (beta-core), which are the major form hi urine.Both the blood and urine of non-pregnant subjects containsmall amounts of HCG. HCG from the implanting blastocystfirst appears in maternal blood around 6—8 days followingfertilization; the levels rise rapidly to reach a peak at 7 -10weeks. With most current pregnancy test kits (sensitivity 25units per litre) urine may reveal positive results 3 - 4 daysafter implantation; by 7 days (the time of the expected period)98% will be positive. A negative result 1 week after the missedperiod virtually guarantees that the woman is not pregnant.With the present generation of test kits, false positive resultsdue to interfering materials are extremely unlikely. Pregnancytests have now reached a level of sensitivity and specificitywhich is unlikely to be surpassed either by better tests oralternative technology.Key words: HCG/pregnancy tests/ELISA
A pregnancy test is among the most widely used and valuableof tests in the whole field of clinical biochemistry. Furthermore,it is unique in that it is also used by non-professionals. One-thirdor more of all women buy and use a pregnancy test during theirreproductive lives (Jeng et al., 1991). Unlike the majority oflaboratory tests, the result may be die cause of immediate joyor anguish on die part of the consumer.
For the purposes of die present discussion a 'pregnancy test'is defined as a procedure intended simply to reveal die presenceor absence of a pregnancy.
Materials which might form the basis of a pregnancy test
All current pregnancy tests involve die qualitative determinationof die concentration of human chorionic gonadotrophin (HCG)by an immunoassay. Usually, diis is applied to a urine sample.However, die odier 'specific' fetoplacental products mightdieoretically be suitable provided diat diey appear at concen-trations which can be readily detected widiin die first 4weeks following fertilization. In practice, die only materials whichhave been evaluated in this context are Schwangerschaftsprotein1 (SP1), placental protein 14 (PP14) and 'early pregnancyfactor' (EPF) (Canfield and O'Connor, 1991).
Schwangerschaftsprotein 1 (SP1) is a glycoprotein of die samefamily as carcino-embryonic antigen (CEA). Substantial amountsare produced by me early trophoblast. Using a sensitiveradioimmunoassay, SP1 can be detected in maternal blood fromas early as 9 days following fertilization, and 2 days later inmaternal urine (Grudzinskas et al., 1978; Ho et at., 1988).However, altiiough measurement of SP1 might be equivalent tothat of HCG, it is in no way superior. The interesting possibilitydiat it might be a useful test in women receiving exogenous HCGhas not been exploited in clinical practice.
Placental protein 14 (PP14) was originally described by HansBohn as one of a group of proteins which could be isolated fromplacental extracts (Bohn et al., 1982). Subsequently, it was shownto be secreted by die maternal endometrium and decidua ratiiertiian die placenta (Bell et al., 1985) and to be a member of diebeta-lactoglobulin family (Julkunen et al., 1988). Small amountsare present in non-pregnant females, die highest levels beingfound at die time of menstruation. In early pregnancy, tiiere isa very rapid increase to a peak at 8 — 10 weeks, witfi a falldiereafter. This pattern is virtually identical to diat of HCG andsuggests that PPM could be used as a pregnancy test. As witiiSP1, however, there is no evidence diat it is superior to HCGin diis respect.
'Early pregnancy factor' (EPF) is a poorly characterizedmolecule which can be measured by a complex immunologicaltest (Morton et al., 1977). The great interest in diis compoundresults from the claim that it can be detected in maternalblood widiin hours of fertilization. If true, and if convenientmediodology were to be developed, dien estimation of EPFwould rapidly become the most popular of all pregnancy tests.Unfortunately, die test technology has proven difficult toreproduce, and a number of audiors have even doubted the actualexistence of EPF (Chard and Grudzinskas, 1987).
A rather more convincing 'early pregnancy factor' has beendemonstrated in the mouse (O'Neill et al., 1989). This is aphospholipid which, because of its main biological activity,
© Oxford University Press 701

T.Chard
is known as 'platelet activating factor' (PAF). A similarphenomenon (a reduction in platelet count within a few days offertilization) has also been noted in the human but, once again,the evidence for this is far from complete. It is worthremembering that the human embryo is approximately the samesize as the mouse embryo, but that its products will be dilutedinto a far larger maternal pool. This, together with the lack ofany direct contact between the early blastocyst and the maternalbloodstream, makes it inherently unlikely that there will ever bea reliable test of pregnancy in the human prior to the time ofimplantation (i.e before 6 - 7 days post-fertilization).
Development of HCG measurement as a pregnancy test
The development of the first biological assay for HCG, and hencepregnancy tests, can be attributed to Ascheim and Zondek (1927).A number of variations on their procedure were used for the next30 years (Table I). In the classic study by Tietz (1965), the frogtest showed 12% of positive results in the first week after themissed period, 58% during the second week and 93% in the thirdweek. Corresponding results for the more sensitive rabbit testwere 77%, 90% and 96%. Subsequent developments in bioassaysfor gonadotrophk activity (Rees et al., 1973) suggest that it wouldnot be difficult to devise tests with a higher level of accuracyin the first week after the missed period. However, the realdisadvantage of the bioassays as clinical tests was that theprocedures were cumbersome and expensive, and that it mightbe several days before results were available. As so oftenin practical medicine, convenience and cost determine theapplicability of a procedure and it is not surprising that thebioassays were rapidly overtaken in the 1960s when immuno-assays were introduced (Wide and Gemzell, 1960).
Biochemistry of HCG
Human chorionic gonadotrophin (HCG) is one of a family ofglycoprotein hormones, the other members being luteinizinghormone (LH), follicle stimulating hormone (FSH) andthyrotrophin-stimulating hormone (TSH). Each of these consistsof two subunits: an alpha-subunit (92 amino acids) which isvirtually identical in all four; and a beta-subunit which ischaracteristic of the individual hormone (Bahl et al., 1972;Morgan et al., 1975; Pierce and Parsons, 1981). The beta-subunitof HCG is a single chain of 145 amino acids. The first 121 N-terminal amino acids share 80% of the sequence with beta-LH;the C terminus of beta-HCG has a 24 amino acid extension whichis not present in beta-LH. Both subunits of the molecule areneeded for biological activity but the beta-subunit determines the
specificity of the action (Strickland and Puett, 1981). The alpha-subunit is coded by a single gene on chromosome 6 and the beta-subunit by a family of seven genes on chromosome 19; only twoof the latter genes appear to be active (Fiddes and Talmadge,1984).
In the circulation, the bulk of HCG is in the form of the intacthormone (a-/3 dimer) with only small amounts of free alpha- andbeta-subunit. In urine, by contrast, a large fraction of the materialwhich reacts in immunoassays for HCG is a metabolic fragmentof the hormone commonly known as 'beta-core' (Wehmannet al., 1989). This consists of two polypeptide chains derivedfrom the /3-subunit of HCG: the amino acid sequences 6 -40 and55-92 are joined by disulphide bridges (Birken et al., 1988).The fragment lacks the unique 30 amino acid carboxy-terminalpeptide but retains conformational immunological determinantsalso found in intact and free /3-subunit of HCG. Although largequantities are found in the urine of pregnant women and somepatients with cancer, it is virtually undetectable in serum. Someworkers believe that this fragment is secreted directly into thecirculation by the placenta and then rapidly excreted by thekidneys (Kardana et al., 1988); others consider that the majorsource is intracellular degradation of the intact and /3-subunit ofHCG in the renal parenchyma.
Functions of HCG
Chorionic gonadotrophin has biological activities identical withthose of pituitary luteinizing hormone. The trophoblastsurrounding the blastocyst begins secretion of HCG into thematernal circulation at the time of implantation, i.e. ~ 7 dayspost-conception. The rapidly rising levels of HCG in the motherprovide a stimulus to the corpus luteum (luteotrophic effect). Ina normal, non-pregnant menstrual cycle the corpus luteum wouldbegin to involute at this stage with a fall in secretion of oestradioland progesterone leading eventually to shedding of theendometrium. However, under the influence of HCG, the corpusluteum continues to grow and secrete increasing quantities ofsteroids. Thus, HCG is the principal signal from an earlypregnancy leading to 'rescue' of the corpus luteum, delay ofmenses and thus maintenance of the pregnancy.
Methods of measurement
The biological assays for HCG are now of only historical interest.For a time, considerable use was made of an assay using receptorsextracted from bovine corpora lutea (Saxena et al., 1974).However, since the 1960s virtually all assays have been im-munoassays.
TaWe I. Biological tests for early pregnancy*
Name of test (researcher)
Ascheim — ZondekFriedmanOvarian hyperaemia (Beck et al.)Frog test (Wiltberger, Miller)Toad test (Galli, Mainini, Shapiro)
'Modified from Pritchard et al. (1985).
702
Test animal
Mice or ratsRabbitsRatsFemale frogMale toad
Endpoint
Corpus luteumCorpus luteumHyperaemiaExtrusion of eggsExtrusion of spermatozoa
Time taken for test
5 days48 h12 — 18 h24 h2-5 h

Pregnancy tests
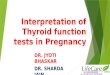
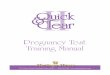
Several different forms of immunoassay have been used forqualitative pregnancy tests. The major variants are in the typeof label employed and in the specificity of the antibody. Theoriginal immunoassays used particles as the label—agglutinationassays (Figure 1). Agglutination techniques are still widely usedbecause of their familiarity and relatively low cost. The mostrecent generations of slide tests have a sensitivity of 500 IU/1and the tube tests of 200 IU/1. The later ELISA procedures(Figure 2) occur in a variety of different sorts of which 'dipsticks'(Norman etal., 1985) offer great user convenience and asensitivity between 25 and 50 IU/1. From the point of view ofthe consumer, professional or non-professional, it is difficult toenvisage any procedure which could offer a significant advanceover some of these devices. For example, Clearview (Unipath,UK) requires only the addition of five drops of urine to the'sample window' followed by the appearance of a line in the'result window' if the test is positive.
Similar procedures have been used for quantitativemeasurements in hospital laboratories. In the latter, extensive useis also made of radioimmunoassay with an isotope of iodine[125I] as the label.
The earlier assays used antibodies raised against the wholeHCG molecule. Most of these antisera reacted equally well withLH and HCG. The use of antibodies raised against the purifiedbeta-subunit was an important development; such antibodieswould react with HCG but not to a significant extent with LH(Vaitukaitis et al., 1972). The resulting ability to measure lowlevels of HCG in the presence of LH explains the great sensitivityof current pregnancy tests. A further development was the useof monoclonal antibodies. These have two important advantages:first, because of the method of selection it is possible to chooseonly those antibody-producing clones which have the desiredspecificity; second, they can be produced in large quantities
3 . ( P j - h C G Parties coated with hCG
Antibody to hCG with twocombining sites
(p)-hCGAgglutination
(?)-hCG
c. ©-©-
hCG
hCG
urbgwHh ( p ^ h C G hCG~
(^Pj-hCG
No agglutination
Fig. 1. The principle of the agglutination inhibition assay: (a) thetest reagents are particles (red cells or latex) coated with HCG, andan antibody to HCG; (b) when these are mixed with urinecontaining no HCG, the antibody binds adjacent particles thuscausing agglutination; (c) when the reagents are mixed with urinecontaining HCG, the latter combines with the antibody and thusprevents it from binding and agglutinating the particles. Theantibody is usually directed to the beta-subunit. The test can becarried out on slides or in tubes; in the latter a positive result isindicated by deposition of a ring at the bottom of the tube.
with total consistency from one batch to the next (unliketraditional polyclonal antibodies which vary with each individualantibody-producing animal).
What is measured by an assay for HCG?
The complex structure of HCG and its subunits and fragmentshas led to much confusion in both terminology and quantitation.For example, it is very common amongst clinicians to refer to'beta-subunit assay' or 'beta-subunit' levels. These terms maycorrectly refer to the specificity of the antibody. However, inblood the vast majority of the materials measured by a beta-subunit antibody is intact HCG (i.e. the assay is detecting thea-/3 dimer). The amount of free beta-subunit is very small, — 1 %or less of the total (Ozturk et al., 1987). In urine the bulk ofHCG-like material is beta-core (Kato and Braunstein, 1988),which again cannot properly be described as beta-subunit.
It is also commonly assumed that antibodies to the (3-subunitare directed to the unique C-terminal peptide. However, althoughhighly specific HCG assays have been developed using antibodiesto this peptide (Wehmann et al., 1981; Birken et al., 1982), suchantibodies are frequently of low affinity. In reality, many of thespecific beta-subunit antibodies used in pregnancy tests aredirected to other sites.
Although quantitation is not directly relevant to qualitativepregnancy testing, it may have an important bearing on the levelsof 'sensitivity' quoted for different assays. The problem is thatthe International Reference Preparation (IRP) on which theunitage is based is a preparation of highly purified HCG. Themost widely used standard at the present time is the FirstInternational Reference Preparation (IRP-HCG 75/537) providedby the World Health Organization (Stoning et al., 1980). Thishighly purified preparation still contains small quantities ofsubunits (Wehmann etal., 1988) and succeeded the SecondInternational Standard (2nd IS-HCG) which consisted of a mixtureof HCG and subunits. One unit of the 2nd IS is approximately
Sow-phaze
anl)-hCG Unnewith hCG
Enzyme-label ledanti-hCG
Fig. 2. The principle of the enzyme immunoassay [enzyme-linkedimmunosorbent assay (ELISA); also sometimes known as'sandwich' or 'immunometric' assays]. HCG in urine is capturedby a solid-phase antibody directed to one she on the HCGmolecule. The bound HCG is then identified by a second antibodyto a different site on the HCG molecule. This second antibodycarries an enzyme (®) as label: addition of an appropriatesubstrate yields a colour reaction. There are many variations onthis procedure, especially in the solid-phase support and the methodof developing the colour reaction: commercial pregnancy testsinvolve a range of dipsticks, pots, tubes, etc. The use of twoantibodies confers sensitivity because the capture antibodyconcentrates the HCG on the surface of the solid phase. It alsoconfers specificity because the two antibodies can be directed tosites which will only be found together in HCG. Thus in theclassical Hybritech format, the capture antibody is anti-a-subunitand the detection antibody is anti-/3-subunit. Other combinations canbe used, and the antibody may be monoclonal or polyclonal.
703

T.Chard
equivalent to 2 units of the 1st IRP, though this varies accordingto the assay used (Ooi et al., 1989). In this review, levels areusually stated in terms of the 1st IRP. Some authors report valuesas weight-by-volume; it is generally agreed that 1 ng of the highlypurified preparation CR 119 is equivalent to 56 mTU of IRP.
To understand the potential problems of basing the assay ona purified HCG preparation, consider two assays, one of whichis specific to free beta-subunit and reacts only slightly withintact HCG (assay 1), while the other shows the reverse (assay2). The IRP will show relatively little activity in assay 1.However, a urine sample from a pregnant woman, which containspredominantly beta-core, will show high levels in assay 1 andlow levels in assay 2. This illustrates why different assays cangive quite different results on the same clinical specimen. It alsoindicates why the sensitivity (minimum detection limit) of an assayin respect of the IRP could be different from that in respectof pregnancy urine.
HCG levels in normal pregnancy
Normal non-pregnant subjects have low circulating levels ofHCG: in males and pre-menopausal females the range is 0.02 —0.8 IU/1; in post-menopausal females it may sometimes rangemuch higher than this (Body et al., 1981; Borkowski et al., 1984;Armstrong et al., 1984; Lee et al., 1991).
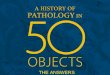
Cultured blastocysts secrete HCG into the medium from 7 dayspost-fertilization onwards (Fishel et al., 1984; Hay and Lopata,1988). Messenger RNA for HCG can also be detected in thetrophoblast at this time (Ohlsson et al., 1989). The earliest pointat which HCG can be detected in the maternal circulation is— 6—8 days post-conception, i.e. around the time of implantation(Braunstein et al, 1976; Lenton et al., 1981, 1982). It is likelythat the appearance of HCG in the mother is a combination ofcommencement of secretion by the trophoblast, together with theestablishment of direct contact between the trophoblast and thematernal circulation. Thereafter, the levels rise rapidly with adoubling time which has been variously estimated at between 1.3days (Lenton et al., 1982) and 2.3 days (Batzer et al., 1981;Lenton et al., 1981) (Figure 3). The increase is more rapid inthe earlier days of the rise (Pittaway et al., 1985; Daya, 1987;Fritz and Guo, 1987). Lenton and colleagues (1991) have shownthat the exponential rise can be resolved into two distinct phases:an initial faster component which they attribute to the actualprocess of implantation (up to 11 days post-LH surge); and aslower component, as trophoblast HCG and maternal circulatingHCG come into equilibrium. The rate of rising HCG is slightlyreduced in pregnancies which subsequently abort (clinical orsub-clinical 'biochemical' pregnancies) and in pregnanciesresulting from in-vitro conception (Smitz et al., 1988; Lentonetal., 1981).
The levels of HCG reach a peak at 7 - 1 0 weeks of pregnancy.At this time, the mean concentration is 50 000 U/l with a rangefrom 20 000 to 200 000 U/l; the secretion rate is over half amillion units (26 mg) per day (Rizkallah et al., 1969). The levelsof HCG in relation to various events in early pregnancy areshown in Table II.
Somewhat surprisingly, the levels of HCG in urine are verysimilar to those in blood (Marshall et al., 1968; Naryshkin et al.,1985; Norman et al., 1987; Lenton et al., 1991). The two fluids
are therefore virtually equivalent from the point of view ofpregnancy testing. Traditionally HCG is measured in the firstspecimen of urine passed in the morning. However, specificexperiment has failed to show any consistent variation of urinaryHCG concentrations over a 24-h period (Kent et al., 1991).
Detection of early pregnancy by a pregnancy test
For the user there are three main questions about a pregnancytest. What is the earliest time after conception when the testbecomes positive? How certain can a woman be that she is notpregnant on the basis of a negative result? How certain can awoman be that she is pregnant on the basis of a positive result?
How early does the test become positive?
Chorionic gonadotrophin first appears in maternal blood at6—7 days post-conception. Using a research assay (sensitivity0.1 -0 .3 IU/1), Lenton and colleagues (1982) found circulatingHCG in 5.3% of subjects by day 8 following the LH peak,15.8% by day 9, 53.2% by day 10 and 100% by day 11. Moststate-of-the-art pregnancy tests have a sensitivity of 25 IU/1. Atthis level it appears that some women will yield positive results3 or 4 days after implantation (Figure 4). Thereafter, therate of positive results increases rapidly, reaching an estimated
10,000 r
1.000hCG levels
(lu/l)
100
10
I I10 12 14 16 18 20
Days from LH peak
22
Fig. 3. The levels of HCG in early pregnancy based on the bloodHCG levels reported by Lenton and colleagues (1982) and Ooiet al. (1989). Surprisingly, there is no adequate quantitativeinformation on urinary HCG levels in the first 6 weeks ofpregnancy. However, the concentrations of HCG in blood andurine are very similar. The vertical lines show the means ( • ) andrange of values reported by Ooi et al. (1989). The means are verysimilar to those of Lenton and colleagues; the ranges are largerbecause the published results were aggregated into 4-day periods.
704

Pregnancy tests
98% by 7 days after implantation, i.e. at around the time ofthe expected period.
Clearly, the earliest time of detection is directly related to thesensitivity of the test. The bioassays and earlier immunoassayswith a sensitivity of 2000-2500 IU/1, only became positive at6 weeks post-LMP. Sometimes published results on sensitivitycan be confusing. For example, in a group of tests all of whichhad an estimated sensitivity of 200 IU/1, Asch and colleagues(1988) reported positive values at the time of the missed mensesof 70%, 88% and 95%. A possible reason for this type ofdiscrepancy is shown in Figure 5; relatively small differencesin sensitivity can make large differences in positivity rates ona given day of pregnancy.
How certain is a negative result?
It is generally recognized that pregnancy tests are unreliable (i.e.quite likely to give negative results) before the time of the firstmissed period (Jovanovic et al., 1987). However, given astate-of-the-art test with a sensitivity of 25—50 IU/1, a negativeresult > 1 week from the expected time of the missed period canvirtually guarantee that the woman is not pregnant. There muststill remain a small chance that the woman has levels at theextreme lower end of the normal range (and thus might beundetectable), or that conception took place later than expectedon the basis of the menstrual history. This residual uncertaintycan be excluded by repeating the test 1 week later. Several currenttest kits provide a second test for this purpose.
How certain is a positive result?
With current technology, a positive result is unlikely in theabsence of a pregnancy. However, 'false-positive' results canoccur, notably in post-menopausal women. There is little doubtthat these findings are attributable to low circulating levels ofauthentic HCG in non-pregnant subjects (Armstrong et al., 1984).In a study using five ELISA kits, there was a 1 - 2 % false-positiverate with three of the kits, while the remaining two yielded much
higher rates (10% and 25%) (Bandi et al., 1987a). Many of thesefalse-positive results appear to have been due to readings between5 and 25 IU/1; levels above the latter almost always proved tobe correct (Bandi et al., 1987b). Problems can also arise witha classical radioimmunoassay, even using an apparently highlyspecific antibody. Emancipator and Cadoff (1988) showed that8 out of 9 of women yielding a result between 10 and 30 IU/1in a radioimmunoassay were not pregnant on follow-up. In thelight of this information, the following general rules can be made(Bandi et al., 1989). A level of < 5 IU/1 can be confidently statedto be negative. A level > 25 IU/1 can equally confidently be statedas positive. Between these two is a 'doubtful' zone. At a practicallevel, a test result of this type should be repeated a minimumof 2 days later.
A wide variety of factors have at various times been describedas possible interfering agents in a pregnancy test (Table HI). Fewif any of these are significant with the current generation of testkits; there is no drug or physiological state which can interferewith a well-designed ELISA carried out on urine. An exceptionis the woman who has received HCG therapeutically, usually forinduction of ovulation. The serum half-life of injected HCGfollows a multiphase curve with initial rapid components of 5 hand 24 h (Rizkallah et al., 1969) followed by a further slowingto 2.3 days (Damewood et al., 1989). Exogenous HCG may stillappear in the urine up to 14 days after the last dose (Damewoodet al., 1989). Levels of HCG are higher following intramuscularthan subcutaneous injection (Saal et al., 1991). It has beenproposed that other tests may be useful under these circumstances(SP1; Grudzinskas et al., 1978) but the indication is so unusualthat it would hardly justify the resources needed to make thetechnology available. Following abortion in the first trimester,it may take as long as 60 days for HCG levels to return to zerofrom the very high values present at 7 -10 weeks (Steier et al.,1984). Another and exceedingly rare possibility is that the womanhas an HCG-secreting tumour: gestational trophoblastic disease(hydatidiform mole and choriocarcinoma); a gonadal teratoma;
Table n. Events in early pregnancy observed by ultrasound and the corresponding mean HCG levels. Note that most of these studies assayed serum ratherthan urine, but the levels in these two fluids are very similar. Daya et al (1991a,b) have published a very detailed table of HCG levels versus gestational sacsize
Author Event Days HCG (IU/1)*
Cacciatore et al (1990)
Goldstein el al. (1988)Bemaschek et al. (1988)Nyberg et al. (1988)
Fossum et al. (1988)
Daya et al. (I991a,b)
Gestational sac 1—3 mmYolk sac apparentHeart action seenGestational sac 1 cmGestational sac seenGestational sac seen:
20% of cases80% of cases
100% of casesGestational sac seenFetal pole seenFetal heart seenYolk sac first seenYolk sac always seenHeart action first seenHeart action always seen
313641
34.840.346936404146
± 2.2± 3.4± 6
730 (467-935)4103 (1120-7280)12 050 (5280-22 950)>6000>600
<10001000-2000>10001398 ± 1555113 ± 29817 208 ± 377219005800920024 000
"International Reference Preparation (IRP), if necessary converted by multiplying 2nd International Standard results by two.
705

T.Chard
10,000 r
1.000 -hCG levels
(lu/l)
10,000
100 -
10 12 14 16 18 20
Days from LH peak
22
Fig. 4. Levels of circulating HCG in early pregnancy (see Figure3), showing that an assay with a sensitivity of 25 IU/l wouldbecome positive in some subjects between 10 and 11 days after theLH peak and in most subjects 12 — 13 days after the peak.
or a carcinoma with ectopic secretion of HCG (lies et al., 1990).It is important to emphasize that a pregnancy and a positive
test do not guarantee a baby 9 months later. The total loss ofpregnancies between conception and term is substantial. Failureof the pregnancy is more common with the new than with theolder tests: the earlier the pregnancy is diagnosed, the more likelyit is to abort. Positive tests may even occur in the luteal phaseof an apparently normal cycle; the pregnancy implants but abortsbefore the term of the expected period. This is the so-called'occult' or 'biochemical' pregnancy (reviewed by Chard, 1991).
Dating of pregnancy
Since HCG levels are related to the stage of gestation, it is logicalthat a quantitative measurement of HCG in an individual womanmight be used to estimate the gestational age. Several authorshave shown that this prediction is possible (Lagrew et al., 1983;Westergaard et al., 1985). However, the error of the predictionin relation to the 'gold standard' of an unambiguous menstrualhistory is as high as ± 2 weeks. This is definitely inferior to datingby ultrasound (gestational sac diameter or crown-rump length)with an error of only 3 - 4 days (Johal et al., 1992).
It has also been suggested that a qualitative pregnancy test maybe used for dating. Thus, if serial tests are done on an individualwoman, the time at which they become positive defines the stageof gestation. However, this approach is fraught with possibleerrors and is entirely replaced by ultrasound dating.
1.000hCG levels
(lu/l)
100
10
I10 12 14 16 18 20
Days from LH peak
22
Fig. 5. Why different tests with the same quoted sensitivity maygive apparently very different results (Asch et al., 1988). Takethree tests with a sensitivity of '200 IU\ It is well-recognized thatthere may be substantial errors in the estimation of minimumdetection limits, such that the three kits might actually havesensitivities of 100, 200 and 400 IU/l. At 16 days of gestation thekit with the 100 IU limit will be positive in all cases; the 200 IUkit will be 80—90% positive; and the 400 IU kit will be positive inonly some 2% of cases.
Table m . Materials which have been described as interfering withpregnancy tests on urine. Most of these were described in connection withfirst generation assays and probably do not apply to current tests. Otherfactors, such as circulating antibodies to mouse immunoglobulins,rheumatoid factors, proteases and hyperlipidaemia can interfere with HCGassays on serum (Norman, 1991)
Acetylsalicylic acid (aspirin)CarbamazepineMethadoneBloodProteinHigh pHSeminal fluid
Other ways of detecting early pregnancy
The only significant current competitor to HCG as an earlypregnancy test is ultrasound. There are descriptions of changesassociated with the earliest stages of implantation and embryonicdevelopment, especially using transvaginal ultrasound (Table II).Clearly, the type of equipment and user skills needed to makethese observations are of a high order. The minimum level ofHCG below which a gestational sac cannot be visualized byultrasound is ~ 1000 IU/l (Fossum et al., 1988; Daya et al.,1991a,b). For practical purposes, however, routine clinicaldetection of an early pregnancy by ultrasound is not possible
706

Pregnancy tests
before 6 weeks of gestation. Measurement of HCG will continueto be the standard method of detecting an early pregnancy forthe foreseeable future.
Complications of pregnancy
Most pregnancy tests are performed simply to satisfy the curiosityof the woman and her relatives. There are also important medicalindications. These include situations in which the woman shouldconsider changing her lifestyle to avoid possible risks to the fetus:examples include smoking, drugs and excess alcohol. In addition,pregnancy might indicate the need for specific medical action,as in the mother with diabetes or heart disease. It has also beenrecommended that a pregnancy test should be performed on allwomen undergoing endometrial biopsy in the late luteal phaseof the cycle (Herbert et al., 1990).
An important medical indication is investigation of the womanwith abdominal symptoms which might or might not be associatedwith a pregnancy (Seppala et al., 1980). A positive pregnancytest (> 25 IU/1) is found in 95 % or more of women with ectopicpregnancy; false-negatives are rare (Taylor et al., 1988; Uribeand Dunn, 1990), although the rate becomes 11.9% if an assaywith a sensitivity of 200 IU/1 is used (Romero et al., 1985). Evenif the history seems unambiguously to exclude pregnancy, —10%of women may be pregnant (Ramoska et al., 1989). In one studyof females admitted as accident victims, random pregnancy testsrevealed that 2% were pregnant (Lippman et al., 1988). If thetest is negative, it can be safely assumed that pregnancy is nota feature of the case; if the test is positive then laparoscopy shouldbe performed to confirm or exclude an ectopic pregnancy. Thispolicy has led to a great improvement in the accuracy of diagnosisof ectopic pregnancy, with a substantial reduction in unnecessarylaparoscopies and other special investigations. The diagnosticapproach has been made possible by the widespread availabilityof simple and sensitive tests.
Evaluation of a pregnancy test
The main criteria for evaluating and comparing differentpregnancy tests are specificity, sensitivity, convenience and cost(Delfert etal., 1987; Lee and Hart, 1990).
Specificity refers to the cross-reaction with LH which shouldbe < 1 %. As already noted, specificity is vital to the achievementof a high level of sensitivity. A manufacturer would be mostunlikely to market a kit which performed less well than this. Thecriteria for assessment of specificity have been well describedby Porter et al. (1988). Testing should include substantialnumbers of samples from men and from non-pregnant women.
Sensitivity should be 50 IU/1 or better. Test kits with sensitivitylevels of > 100 IU are still on the market but it is difficult tosee any argument for their retention. They should definitely notbe used for specific clinical indications (abdominal pain), asituation in which a negative result from a poor test could beclinically misleading. The precision of the test at the detectionlimit should be examined by replicate determination on samplescontaining HCG levels 50% above and 50% below the limits(Delfert etal., 1987).
Convenience refers to simplicity such that any member of thegeneral public can perform the test without difficulty. Mostmembers of the medical profession can be considered in the samecategory since they are not usually trained in lab techniques.Simplicity of both procedure and instructions is especiallyimportant in the light of the fact that most 'over the counter'pregnancy tests are purchased on the basis of advertisementsrather than professional advice from a pharmacist (Coons, 1989).Another aspect of convenience is speed. It should be possibleto complete the test within 15 min, including any waiting periodfor delayed positive results.
Cost does not appear to be an issue in the 'over the counter'market where all tests are currently priced at around £8 — 10($14-18). Bulk purchases for hospital practice tend to be verycompetitive and prices of around £1.50 ($2.50) may be expected.AH these prices are very cost-effective in terms of the demandand the value achieved.
The ultimate evaluation of the performance of a pregnancytest should be a study on substantial numbers of very earlypregnancies (3 weeks post-LMP onwards) with a follow-up toidentify all false-positive and false-negative results. Ideal studiesof this type are few and far between. Where they have beenperformed, the results are sometimes disturbing. For example,Doshi (1986) found that only 56% of pregnancies were identifiedby kits with a claimed accuracy of 98-99%. This study referredto a previous generation of products, but it is still the case thatmany tests are judged solely on the basis of their specificity andsensitivity in the laboratory, with an extrapolation to their likelyperformance in clinic.
Conclusions
The current generation of immunoassay technologies formeasurement of HCG can detect or exclude a pregnancy at thetime of the missed period. Their simplicity and convenience issuch that the same procedures are applied in the hospital or thehome. Pregnancy tests have reached a level of sensitivity andspecificity which is unlikely to be surpassed either by bettertests or alternative technology. Pregnancy testing is remarkablein that it fulfils a strongly felt demand both from the public andthe healthcare professions.
ReferencesArmstrong.G., Ehrlich.P.H., Birken.S., Schlatterer.J.P., Siris.E.,
Hembree,C. and Canfield.R.E. (1984) Use of a highly sensitive andspecific immunoradiometric assay for detection of human chorionicgonadotropin in urine of normal, nonpregnant, and pregnantindividuals. J. Clin. Endocrinol. Metab., 59, 867-874.
Asch.R.H., Asch.G., Asch,M., Bray.R. and Rojas.F.J. (1988)Performance and sensitivity of modem home pregnancy tests. Int.J. Fertil, 33, 157-161.
Ascheim.S. and Zondek.B. (1927) Hypophysenvorderlappenhormon undovarialhormone im ham von schwangeren. Klin. Wochenschr., 6,1322.
Bahl.O.P., Carlson.R.B., Bellisario.R. and Swaminathan.N. (1972)Human chorionic gonadotropin amino acid sequence of the alpha andbeta subunits. Biochem. Biophys. Res. Commun., 48, 416-422.
Bandi.S.L., Schoen.I. and DeLara.M. (1987a) Enzyme-linked
707

T.Chard
immunosorbent urine pregnancy tests. Clinical specificity studies. Am.J. Clin. Pathoi, 87, 236-242.
Bandi.S.L., Schoen.I. and DeLara.M. (1987b) Highly sensitivequalitative methods for serum choriogonadotropin (hCG): clinicalspecificity studies. Clin. Chem., 33, 677-681.
Bandi.S.L., Schoen.I. and Waters.M. (1989) An algorithm for testingand reporting serum choriogonadotropin at clinically significantdecision levels with use of 'pregnancy test'. Clin. Chem., 35,545-551.
Batzer.F.R., Schlaff.S., Goldfarb.A.F. and Corson,S.L.(1981) Serialbeta subunit of human chorionic gonadotropin doubling time as aprognosticator of pregnancy outcome in an infertile population. Fertil.Steril., 35, 307-312.
Bell.S.C, Patel,S., Hales,H.W., Kirwan.P.H. and Dnfe.J.O. (1985)Immunochemical detection and characterization of pregnancy-associated endometrial alpha-1 and alpha-2 globulins secreted byhuman endometrium and decidua. J. Reprod. Fertil., 74, 261-270.
Bernaschek,G., Rudelstorfer.R. and Csaicsich,P.(1988) Vaginalsonography versus serum human chorionic gonadotropin in earlydetection of pregnancy. Am. J. Obstet. Gynecol., 1, 608—612.
Birken.S., Canfield.R., Agosto,G. and LewisJ. (1982) Preparation andcharacterization of an improved beta COOH-terminal immunogen forgeneration of specific and sensitive antisera to human chorionicgonadotropin. Endocrinology, 110, 1555—1563.
Birken.S., Armstrong,E.G., Kolks.M.A.G., Cole,L.A., Agosto.G.M.,Krichevsky.A., Vaitukaitis.J.L. and Canfield,R.E. (1988) Structureof human chorionic gonadotropin beta-subunit fragments frompregnancy urine. Endocrinology, 123, 572—583.
BodyJ.J., Muquardt.C. and Borkowski.A. (1981) The human chorionicgonadotropin-like substance in the plasma of normal nonpregnantsubjects is not modulated by the gonadotropin-releasing hormone. J.Clin. Endocrinol. Metab., 52, 1249-1252.
Bohn.H., Kraus.W. and Winckler,W. (1982) New soluble placentaltissue proteins: their isolation, characterization, localization andquantification. In Klopper.A. (ed.), Immunology of Human PlacentalProteins. Praeger Publishing, pp. 67 — 81.
Borkowski.A., Puttaert.V., Gyling.M., Murquardt.C. and Body.J.J.(1984) Human chorionic gonadotropin-like substances in plasma ofnormal nonpregnant subjects and women with breast cancer. J. Clin.Endocrinol. Metab., 58, 1171-1178.
Braunstein.G.D., RasorJ., Adler.D., Danzer,H. and Wade.M.E. (1976)Serum human chorionic gonadotropin levels throughout normalpregnancy. Am. J. Obstet. Gynecol, 126, 678-681.
Cacciatore3., Titinen.A., Stenman.U.H. and Ylostalo.P. (1990) Normalearly pregnancy: serum hCG levels and vaginal ultrasonographyfindings. Br. J. Obstet. Gynaecoi, 97, 899-903.
Canfield.R.E. and O'ConnorJ.F. (1991) Biological markers on humanpregnancy. Biomed. Environ. Sci., 4, 56—68.
Chard,T. (1991) Frequency of implantation and early pregnancy lossin natural cycles. Bailliere's Clin. Obstet. Gynaecoi., 5, 179-189.
Chard.T. and Grudzinskas,J.G. (1987) Early pregnancy factor. Biol.Res. Preg., 8, 53-56 .
Coons,S.J. (1989) A look at the purchase and use of home pregnancy-test kits. Am. Pharm., 29, 46-48 .
Damewood.M.D., Shen,W., Zacur,H.A., Schlaff,W.D., RockJ.A. andWallach.E.E. (1989) Disappearance of exogenously administeredhuman chorionic gonadotropin. Fertil. Steril., 52, 398—400.
Daya.S. (1987) Human chorionic gonadotropin increase in normal earlypregnancy. Am. J. Obstet. Gynecol., 156, 286-290.
Daya,S., Woods.S., Ward.S., Lappalainen.R. and Caco.C. (1991a)Early pregnancy assessment with transvaginal ultrasound scanning.Can. Med. Assoc., 144, 441-446.
Daya.S., Woods,S., Ward,S., Lappalainen,R. and Caco.C. (1991b)Transvaginal ultrasound scanning in early pregnancy and correlation
with human chorionic gonadotropin levels. J. Clin. Ultrasound, 19,139-142.
Delfert,D.M., Rea.M.R., Kessler.G., Siegfried.B.A. and Valdes.R.(1987) Criteria for evaluating nonquantitative assays: application toserum choriogonadotropin. Clin. Chem., 33, 150—153.
Doshi.M.A. (1986) Accuracy of consumer performed in-home tests forearly pregnancy detection. Am. J. Public Health, 76, 512—514.
Emancipator,K. and Cadoff.E.M. (1988) Analytical versus clinicalsensitivity and specificity in pregnancy testing. Am. J. Obstet.Gynecol., 1, 613-616.
FiddeSpJ.C. and Talmadge.K. (1984) Structure, expression and evolutionof the genes for the human glycoprotein hormones. Rec. Prog. Horn.Res., 40 ,43-53 .
Fishel.S.B., Edwards,R.G. and Evans.C.J. (1984) Human chorionicgonadotropin secreted by preimplantation embryos cultured in vitro.Science, 233, 816-818.
Fossum.G.T., Davajan.V. and Kletzky.O.A. (1988) Early detection ofpregnancy with transvaginal ultrasound. Fertil. Steril., 49, 788-791.
Fritz,M.A. and Guo,S. (1987) Doubling time of human chorionicgonadotropin (hCG) in early normal pregnancy: relationship to hCGand gestational age. Fertil. Steril., 47, 584-588.
Goldstein.S.R., Snyder,J.R., Watson.C. and Danon.M. (1988) Com-bined sonographic-pathological surveillance in elective first-trimestertermination of pregnancy. Obstet. Gynecol., 71, 747—750.
Grudzinskas,J.G., Gordon,Y.B., Jeffrey,D. and ChardJ. (1977)Specific and sensitive determination of pregnancy specific beta-1glycoprotein by radioimmunoassay: a new pregnancy test. Lancet,i, 333.
Hay.D.L. and Lopata,A. (1988) Chorionic gonadotropin secretion byhuman embryos in vitro. J. Clin. Endocrinol. Metab., 67,1322-1324.
Herbert.C.M., Hill.G.A., Maxson.W.S., Wentz.A.C. and Osteen.K.G.(1990) The use of a sensitive urine pregnancy test before endometrialbiopsies taken in the late luteal phase. Fertil. Steril., 53, 162-164.
Ho,P.-C., Chan,S.Y.W. and Tang.G.W.K. (1988) Diagnosis of earlypregnancy by enzyme immunoassay of Schwangerschafts-protein I.Fertil. Steril., 49, 76-80.
Ees,R.K., Purkis.E., Whitehead.P.C, Oliver.R.T.D., Leigh,!, andChard,T. (1990) Expression of beta human chorionic gonadotrophinby non-trophoblastic non-endocrine 'normal' and malignant epithelialcells. Br. J. Cancer, 61, 663-666.
Jeng.L.L., Moore.R.M. and Kaczmarek.R.G. (1991) How frequentlyare home pregnancy tests used? Results from the 1988 NationalMaternal and Infant Health Survey. Birth, 18, 11-13.
Johal.B., Setchell.M.E. and Chard,T. (1992) A comparison ofbiochemical and biophysical determination of gestational age in earlypregnancy. J. Obstet. Gynaecoi., in press.
Jovanovic.L., Singh.M., Saxena.B.B., Mills,J.L., Tulchinsky.D.,Holmes.L.B., SimpsonJ.L., Metzger.B.E., Labarbera.A., Aarons.J.and Van Allen,M.I. (1987) Verification of early pregnancy tests ina multicenter trial. Proc. Soc. Exp. Biol. Med., 184, 201-205.
Julkunen,M., Seppala,M. and Janne.O. (1988) Complete amino acidsequence of human placental protein 14. A progesterone-regulateduterine protein homologous to j3-lactoglobulin. Proc. Natl. Acad. Sci.USA, 85, 8845-8849.
Kardana.A., Taylor.M.E., SouthallJ.P., Boxer.G.M., Rowan.A.J. andBagshawe.K.D. (1988) Urinary gonadotropin peptide—isolation andpurification, and its immunohistochemical distribution in normal andneoplastic tissues.flr. J. Cancer, 58, 281-286.
Kato.Y. and Braunstein,G.D. (1988) Beta-core fragment is a major formof immunoreactive urinary chorionic gonadotropin human pregnancy.J. Clin. Endocrinol. Metab., 66, 1197-1201.
Kent,A., Kitau,M.J. and Chard, T. (1991) Absence of diurnal variationin urinary chorionic gonadotrophin excretion at 8—13 weeks gestation.
708

Pregnancy tests
Br. J. Obstet. GynaecoL, 98, 1180-1181.Lagrew.D.C, Wilson.E.A. and Jawad.M.J. (1983) Determination of
gestational age by serum concentrations of human chorionicgonadotropin. Obstet. Gynecol., 62, 37—42.
Lee.C. and Hart.L.L. (1990) Accuracy of home pregnancy tests. Ann.Pharmacother., 24, 712-713.
Lee.C.L., Hes,R., Shepherd,J.H., Hudson.C.N. and Chard.T. (1991)The purification and development of a radioimmunoassay for beta-core fragment of human chorionic gonadotrophin in urine: applica-tion as a marker of gynaecological cancer in premenopausal women.J. Endocrinol., 130, 481-489.
Lenton.E.A., GrudzinskasJ.G., Neal.L.M., Chard,T. and Cooke,I.D.(1981) Chorionic gonadotropin concentration in early humanpregnancy: comparison of specific and nonspecific assays. Fertil.Sterii, 35, 40-45.
Lenton.E.A., Neal,L.M. and Sulaiman.R. (1982) Plasma concentrationsof human chorionic gonadotropin from the time of implantation untilthe second week of pregnancy. Fertil. Sterii., 37, 773-778.
Lenton.E.A., Hooper.M., King.H., Kumar.A., Monks,N., Verma.S.and Osborn.J. (1991) Normal and abnormal implantation inspontaneous in-vivo and in-vitro human pregnancies. J. Reprod.Fertil., 92, 555-565.
Lippman.S., Bordador.B. and Shaltout.T. (1988) Detection of unknownearly pregnancy. A matter of safety. Postgrad. Med., 83, 129—131.
Marshall,J.R., Hammond,C.B., Ross.G.T., Jacobsen,A., Rayford.P.and Odell,W.D. (1968) Plasma and urinary chorionic gonadotropinduring early human pregnancy. Obstet. Gynecol., 32, 760—764.
Morgan,F.J.,Birken,S. and Canfield.R.E. (1975) The amino acidsequence of human chorionic gonadotropin. The alpha subunit andbeta subunit. J. Biol. Chem., 250, 5247-5258.
Morton,H., Rolfe,B., Clunie.G.J.A., Anderson,M.J. and Morrison,J.(1977) An early pregnancy factor detected in human serum by therosette inhibition test. Lancet, I, 394-397.
Naryshkin,S., Aw.T.C, Filstein.M., Murphy,J.G., Strauss.J.F.,Kiechie.F.L. and Jacobson.S. (1985) Comparison of the performanceof serum and urine hCG immunoassays in the evaluation ofgynecologic patients. Ann. Emerg. Med., 14, 1074 — 1076.
Norman,R.J. (1991) When a positive pregnancy test isn't. Med. J.Australia, 154, 718-719.
Norman,R.J., Lowings.C. and Chard,T. (1985) Dipstick method forhuman chorionic gonadotropin suitable for emergency use on wholeblood and other fluids. Lancet, i, 19-20.
Norman,R.J., Menabawey.M., Lowings.C., Buck,R.H. and Chard,T.(1987) Relationship between blood and urine concentrations of intacthuman chorionic gonadotropin and its free subunits in early pregnancy.Obstet. Gynecol., 69, 590-593.
Nyberg,D.A., Mack.L.A., Laing,F.C. and Jeffrey,R.B. (1988) Earlypregnancy complications: endovaginal sonographic findings correlatedwith human chorionic gonadotropin levels. Radiology, 167, 619-622.
O'Neill.C, Collier.M., Ryan.J.P. and Spinks.N.R. (1989) Embryo-derived platelet-activating factor. J. Reprod. Fertil. (Suppl.), 37,19-27.
Ohlsson.R., Nilsson.O., Larsson.E. and Lundstrom,P. (1989) Blastocystimplantation precedes activation of the IGF-2 gene in humantrophoblasts. Development, 206, 555-559.
Ooi,D.S., Perkins,S.L., Claman,P. and Muggah,H.F. (1989) Serumhuman chorionic gonadotrophin levels in early pregnancy. Clin. Own,Acta, 181, 281-292.
Ozturk.M., Bellet.D., Manil,L., Hennen,G., Frydman.R. and WandsJ.(1987) Physiological studies of human chorionic gonadotropin (hCG),alpha-hCG and beta-hCG as measured by specific monoclonalimmunoradiometric assays. Endocrinology, 120, 549-558.
Pierce.J.G. and Parsons,T.F. (1981) Glycoprotein hormones: structureand function. Anna. Rev. Biochem., 50, 465-468.
Pittaway.D.E., Reisch.M.S. and Wentz.A.C. (1985) Doubling timesof human chorionic gonadotropin increase in early viable intrauterinepregnancies. Am. J. Obstet. Gynecol., 152, 299-302.
Porter.P., Coley.J. and Gani.M. (1988) Immunochemical criteria forsuccessful matching of monoclonal antibodies to immunoassays ofpeptide hormones for assessment of pregnancy and ovulation. Prog.Clin. Biol. Res., 285, 181-200.
PritchanU.A., MacDonald.P.C. and Gant.N.F. (1985) WilliamsObstetrics, 17th edn. Norwalk, Connecticut: Appleton-Century-Crofts;Prentice/Hall International, Inc.
Ramoska.E.A., Sacchetti.A.D. and Nepp.M. (1989) Reliability of patienthistory in determining the possibility of pregnancy. Ann. EmergencyMed., 18, 48-50.
Rees.L.H., Holdaway.I.M., Kramer.R., McNeilly.A.S. and Chard.T.(1973) New bioassay for luteinizing hormone. Nature, 244, 232-234.
Rizkallah.T., Gurpide.E. and Vande.R.L. (1969) Metabolism of HCGin man. J. Clin. Endocrinol. Metab., 29, 92-103.
Romero.R., Kadar,N., CopeU.A., Jeanty.P., DeChemey.A.H. andHobbinsJ.C. (1985) The effect of different human chorionicgonadotropin assay sensitivity on screening for ectopic pregnancy.Am. J. Obstet. Gynecol., 153, 72-74.
Saal,W., Glowania.H.J. and Happ.J. (1991) Pharmacodynamics andpharmacokinetics after subcutaneous and intramuscular injection ofhuman chorionic gonadotropin. Fertil. Sterii., 56, 225-229.
Saxena,B.B., Hassan,S.H. and Haour.F. (1974) Radioreceptor assaysof HCG: detection of early pregnancy. Science, 184, 793-796.
SeppalS.M., Ranta.T., Tontti.K., Stenman.U.H. and Chard.T. (1980)Use of a rapid hCG-beta subunit radioimmunoassay in acutegynaecological emergencies. Lancet, i, 165-166.
Smitz.J., Devroey,P., Camus,M., DeschachtJ., Khan,L., Staessen,I.,Van Vaersberghe.L., Winsanto,A. and Van Steirteghem.A.C. (1988)The luteal phase and early pregnancy after combined GnRH-agonistHMG treatment for superovulation in IVF or GIFT. Hum. Reprod.,3, 585-590.
Steier.J.A., Bergsio.P.A. and Myking.O.L. (1984) Human chorionicgonadotrophin in maternal plasma after induced abortion, spontaneousabortion and removed ectopic pregnancy. Obstet. Gynecol., 64,391-934.
Storring.P.L., Gaines-Das.R.E. and Bangham,D.R. (1980) InternationalReference Preparation of human chorionic gonadotrophin forimmunoassay: potency estimates in various bioassay and proteinbinding systems; and International Reference Preparations of the alphaand beta-subunits of human chorionic gonadotrophin for immunoassay.J. Endocrinol., 84, 295-310.
Strickland.T.W. and Puett.D. (1981) Contribution of subunits to thefunction of luteinizing hormone/human chorionic gonadotropinrecombinants. Endocrinology, 109, 1933-1942.
Taylor.R.N., Padula,C. and Goldsmith,P.C. (1988) Pitfall in thediagnosis of ectopic pregnancy: immunocytochemical evaluation ina patient with false-negative serum beta hCG levels. Obstet. Gynecol.,71, 1035-1038.
Tietz.N.W. (1965) Comparative study of immunologic and biologicpregnancy tests in early pregnancy. Obstet. Gynecol., 25, 197—200.
Uribe.M.A. and Dunn,R.C. (1990) Tuba! pregnancy with normalhysterosalpingogram and negative serum pregnancy test. Obstet.Gynecol., 75, 483-485.
Vaitukaitis,J.L., Braunstein.G.D. and Ross.G.T. (1972) A RIA whichspecifically measures hCG in the presence of LH. Am. J. Obstet.Gynecol., 113, 751-757.
Wehmann.R.E., Harman.S.M., Birken,S., Canfield.R.E. andBruce,C.N. (1981) Convenient radioimmunoassay for urinary humanchoriogonadotropin without interference by urinary human lutropin.CUn. Chem., 27, 1997-2001.
Wehmann,R.E., Blithe.D.L., Akar.A.H. and Nisula.B.C. (1988) Beta-
709

T.Chard
core fragments are contaminants of the Worid Health OrganisationReference Preparations of human choriogonadotrophin and itsalpha-subunit. J. Endocrinol., 117, 147 — 152.
Wehmann.R.E., Blithe.D.L., Flack.M.R. and Nisula.B.C. (1989)Metabolic clearance rate and urinary clearance of purified beta-core.J. Clin. Endocrinol. Metab., 69, 510-517.
Westergaard,J.G., Teisner.B., Grudzinskas.J.G. and Chard.T. (1985)Single measurements of chorionk gonadotropin and schwangerschaftsprotein for assessing gestational age and predicting day of delivery.J. Reprod. Med., 30, 57-60.
Wide.L. and Gemzell,C.A. (1960) An immunological pregnancy test.Ada Endocrinol, 35, 261-267.
Received on October 18, 1991; accepted on January 9, 1992
710

本文献由“学霸图书馆-文献云下载”收集自网络,仅供学习交流使用。
学霸图书馆(www.xuebalib.com)是一个“整合众多图书馆数据库资源,
提供一站式文献检索和下载服务”的24 小时在线不限IP
图书馆。
图书馆致力于便利、促进学习与科研,提供最强文献下载服务。
图书馆导航:
图书馆首页 文献云下载 图书馆入口 外文数据库大全 疑难文献辅助工具