Embed Size (px)
Citation preview
8/3/2019 Pregest Risk
http://slidepdf.com/reader/full/pregest-risk 1/65
PRE-GESTATIONAL
CONDITIONS
MRS. CATHERINE V. STA.MONICA
8/3/2019 Pregest Risk
http://slidepdf.com/reader/full/pregest-risk 2/65
Pregnancy stresses your heart and
circulatory system.
During pregnancy, your blood
volume increases by 30 to 50
percent to nourish your growing
baby.
The amount of blood your heart
pumps each minute also increases
by 30 to 50 percent.Your heart rate increases as well.
These changes cause your heart to
work harder.
8/3/2019 Pregest Risk
http://slidepdf.com/reader/full/pregest-risk 3/65
Risks depend on the nature and severity of the underlyingheart condition
Heart rhythm issues. Minor abnormalities in heart rhythm
are common during pregnancy. Heart valve issues. If you have an artificial heart valve or
your heart or valves are scarred or malformed, you mightface an increased risk of complications during pregnancy.Mechanical artificial heart valves also pose serious risks
during pregnancy due to the need to adjust use of bloodthinners and the potential for life-threatening clotting(thrombosis) of heart valves.
Congestive heart failure. As blood volume increases,congestive heart failure can get worse.
Congenital heart defect. If you were born with a heartproblem, your baby has a greater risk of developing sometype of heart defect, too. You may also be at risk of premature delivery.
8/3/2019 Pregest Risk
http://slidepdf.com/reader/full/pregest-risk 4/65
EARLY DETECTION
Blood pressure monitoring
Urinalysis
C
BC
Echocardiogram, a test that
uses sound waves to produce
images of the heart
Electrocardiogram, a test that
records the heart's electrical
activity
8/3/2019 Pregest Risk
http://slidepdf.com/reader/full/pregest-risk 5/65
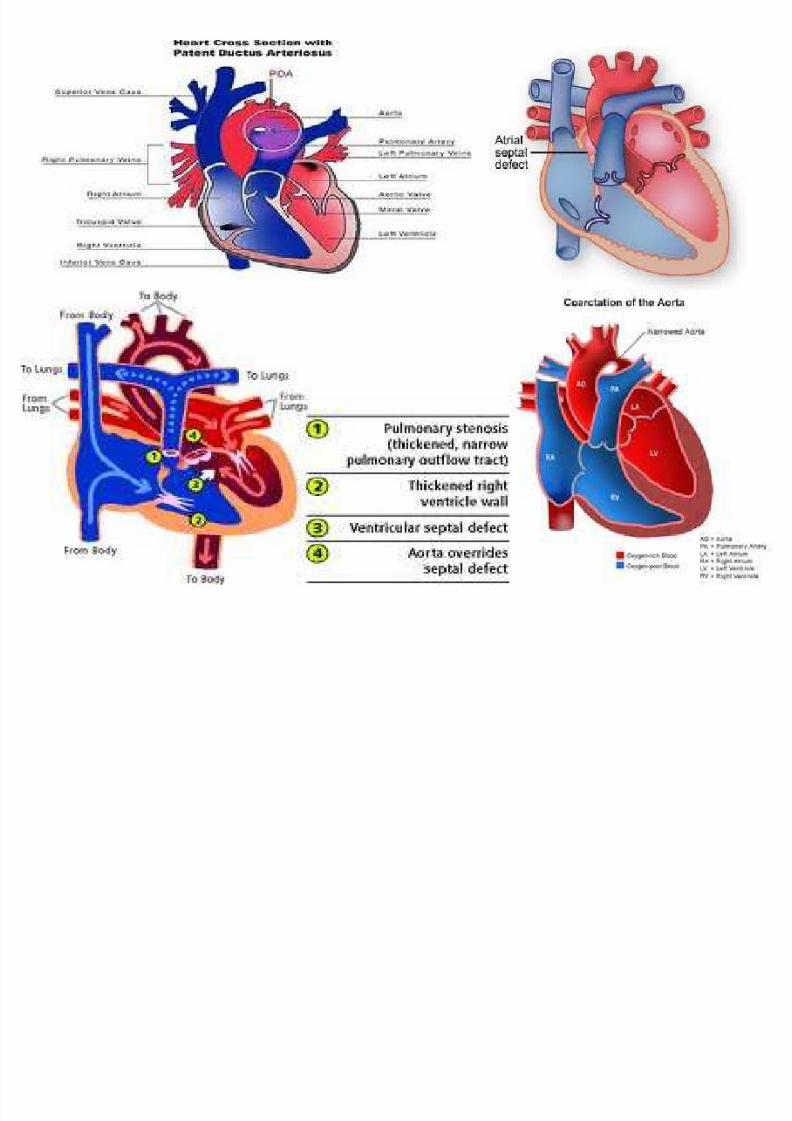
Congenital Heart Defects
Most commonly seen in pregnant women include:
Atrial septal defect
Patent ductus arteriosus
Coarctation of aorta
Tetralogy of fallot
impact of pregnancy depends on the specific defect.-if the heart has been surgically repaired & noevidence of heart disease remains, the woman may
undertake pregnancy with confidence.-woman withCHD who experience cyanosis should be counseled toavoid pregnancy because the risk to mother & fetus ishigh.
8/3/2019 Pregest Risk
http://slidepdf.com/reader/full/pregest-risk 6/65
8/3/2019 Pregest Risk
http://slidepdf.com/reader/full/pregest-risk 7/65
Rheumatic Heart Disease
Results from an infection (caused by the
bacteria,streptococci) known as rheumatic
fever, which starts with a sore throat & leads
to the scarring of one or more heart valves.
The injured valves are unable to open & close
normally, resulting in obstruction to the
flow of blood.
Is it possible to become pregnant?
8/3/2019 Pregest Risk
http://slidepdf.com/reader/full/pregest-risk 8/65
Laboratory tests for detecting RHD:
1. Throat cultures- for group A streptococcus usually arenegative by the time symptoms of rheumatic fever or RHDappear. Isolate the organism before the initiationof antibiotic therapy to help confirm a diagnosis of streptococcal pharyngitis & to allow typing of theorganism if it is isolated successfully.
2. Rapid Antigen- this test allows rapid detection of group Astreptococcal antigen & allows the diagnosis of streptococcal pharyngitis & the initiation of antibiotictherapy while the patient is still in the physicians office.
8/3/2019 Pregest Risk
http://slidepdf.com/reader/full/pregest-risk 9/65
3. Anti-streptococcal Antibodies
-this is useful for confirming previous
group A streptococcal infection. Antibody titer
should be checked @ 2-week intervals in
order to detect a rising titer.
8/3/2019 Pregest Risk
http://slidepdf.com/reader/full/pregest-risk 10/65
General measures to be followed once you becomepregnant:
Make sure to keep your follow-up appointments withyour obstetrician throughout your pregnancy.
Plan regular follow-up visits with your cardiologist.
Carefully follow all the recommendations of thecardiologist.
The diet should be nutritious & fluid & sodium intakeshould be restricted.
Take adequate rest.
Watch your weight.
Avoid alcohol.
Stop smoking.
8/3/2019 Pregest Risk
http://slidepdf.com/reader/full/pregest-risk 11/65
PRE-GESTATIONAL DIABETES
MELLITUS
8/3/2019 Pregest Risk
http://slidepdf.com/reader/full/pregest-risk 12/65
Diabetes Mellitus
An endocrine disorder of
carbohydrate metabolism, results
from inadequate production or
use of insulin.
Insulin- produced by B cells of
Islets of Langerhans in the
pancreas, lowers blood glucoselevels by enabling glucose to
move from the blood into muscle
& adipose tissue cells
8/3/2019 Pregest Risk
http://slidepdf.com/reader/full/pregest-risk 13/65
METABOLIC CHANGES DURING PREGNANCY
Caloric requirement for a pregnant womanis 300 kcal higher than the non-pregnantwomans basal needs
Placental hormones affect glucose and lipidmetabolism to ensure that fetus has ample
supply of nutrients Lipid metabolism:
± Increased lipolysis (preferential use of fat forfuel, in order to preserve glucose andprotein)
Glucose metabolism: ± Decreased insulin sensitivity
± Increased insulin resistance
8/3/2019 Pregest Risk
http://slidepdf.com/reader/full/pregest-risk 14/65
Increased insulin resistance Due to hormones secreted by the
placenta that are diabetogenic:
Growth hormone Human placental lactogen
Progesterone
Corticotropin releasing hormonE
Transient maternal hyperglycemia occurs aftermeals because of increased insulin resistance
Baseline hypoglycemia
Proliferation of pancreatic beta cells (insulin-secreting cells) leads to increased insulin secretion
Insulin levels are higher than in pregnant than
nonpregnant women in fasting and postprandial states
Hypoglycemia between meals and at night becauseof continuous fetal draw
Blood glucose levels are 10-20% lower
8/3/2019 Pregest Risk
http://slidepdf.com/reader/full/pregest-risk 15/65
Ist half of pregnancy: Increased
insulin production and increased
response to insulin
2nd half of pregnancy: Increased
insulin resistance and increased
glucose tolerance; mother may need2-3 times the insulin dosage
Fetus uses glucose from maternal
stores = increased disruption inmaternal carbohydrate metabolism
Increased maternal lipolysis and ketone
production
8/3/2019 Pregest Risk
http://slidepdf.com/reader/full/pregest-risk 16/65
MANAGEMENT OF PRE-GESTATIONAL
DM
All women screened at 24-28 weeks
Strict glycemic control
Oral agents are not recommended ;
after 1st trimester, glyburide may be
used
Lispro or Humalog insulin titrated to
caloric intake
Delivery at or around week 39; based
on BPP
8/3/2019 Pregest Risk
http://slidepdf.com/reader/full/pregest-risk 17/65
RISKS TO BABY AND MOTHER
Macrosomia
Hypoglycemia
Polycythemia and hyperbilirubinemia
Congenital anomalies
IUGRRespiratory Distress Syndrome
Hydramnios
Ketoacidosis
Retinopathies
Vaginitis, UTIs
8/3/2019 Pregest Risk
http://slidepdf.com/reader/full/pregest-risk 18/65
Three main types of Diabetes:
1.Type I diabetes
- results from the bodys failure to produceinsulin, & presently requires the person toinject insulin.
2.Type II diabetes
- results from insulin resistance, acondition in which cells fail to use insulinproperly, sometimes combined witan absolute insulin deficiency.
3.Gestational diabetes- is when pregnant women, who havenever had diabetes before, have a highblood glucose level during pregnancy.
8/3/2019 Pregest Risk
http://slidepdf.com/reader/full/pregest-risk 19/65
Diabetes on pregnancy outcome
The pregnancy of a woman
who has diabetes carries a
higher risk of complications,
especially perinatal mortality& congenital anomalies.
Tight metabolic control reducesthe risk.
8/3/2019 Pregest Risk
http://slidepdf.com/reader/full/pregest-risk 20/65
Management Antepartal
Prenatal care- using a team approach to
ensure an optimally healthy mother &newborn.
- woman needs clear explanations &
teaching to gain her cooperation inensuring a good outcome.
- the nurse-educator plays a major role inthis counseling.- the woman with
pregestational diabetes needs tounderstand what changes she can expectduring pregnancy.
8/3/2019 Pregest Risk
http://slidepdf.com/reader/full/pregest-risk 21/65
a. Dietary regulation
- the pregnant woman with diabetes needsto increase her caloric intake by300 kcal/day.- on the first trimester she needs about 35kcal/day of ideal body weight.Approximately 40% to 50% of the caloriescame from complex, highfiber carbohydrates,20% from protein, &30% to 40% from fats.
- the food is divided into 3 meals & 3 snacks.Bedtime snack is the most important &
should include both protein & complexcarbohydrates to prevent nightimehypoglycemia.
8/3/2019 Pregest Risk
http://slidepdf.com/reader/full/pregest-risk 22/65
b. Glucose monitoring
- is essential to determine the need for
insulin & to assess glucose control.
c. Insulin Administration- Many women
with gestational diabetes need insulin
to maintain normal glucose levels.Human insulin should be used because
it is the least likely to cause an allergic
reaction.- given either in multipleinjections or by continuous
subcutaneous infusion.
Oral hypoglycemics- not rarely used
8/3/2019 Pregest Risk
http://slidepdf.com/reader/full/pregest-risk 23/65
Intrapartal
a. Timing of birth- most pregnant women with
diabetes, regardless of the type are allowed to goto term, with spontaneous labor.
Some clinicians opt to induce labor in a woman at
term to avoid problems related to an agingplacenta.
Cesarean birth maybe indicated if signs of fetaldistress exist.
8/3/2019 Pregest Risk
http://slidepdf.com/reader/full/pregest-risk 24/65
b. Labor management- maternal glucose levels aremeasured hourly to determine insulin need.
Primary goal is to prevent neonatal hypoglycemia.
Often given two IV lines are used, one witH a50%dextrose solution & one with a saline solution.
The saline solution is for piggybacking insulin or if abolus is needed.
IV insulin is discontinued @ the end of the third stageof labor.
8/3/2019 Pregest Risk
http://slidepdf.com/reader/full/pregest-risk 25/65
Post partal Management
First 24 hours postpartum, women wit pre-existingdiabetes typically require very little insulin.
They are usually managed with a sliding scalespecifying dosage based on blood glucose levels.
Antihyperglycemics are contraindicated duringbreastfeeding.
The woman should be reassessed 6 weeks postpartum
to determine whether her glucose levels are normal. If the levels are normal, she should be reassessed at aminimum of 3 year intervals
8/3/2019 Pregest Risk
http://slidepdf.com/reader/full/pregest-risk 26/65
Rh INCOMPATIBILITY
8/3/2019 Pregest Risk
http://slidepdf.com/reader/full/pregest-risk 27/65
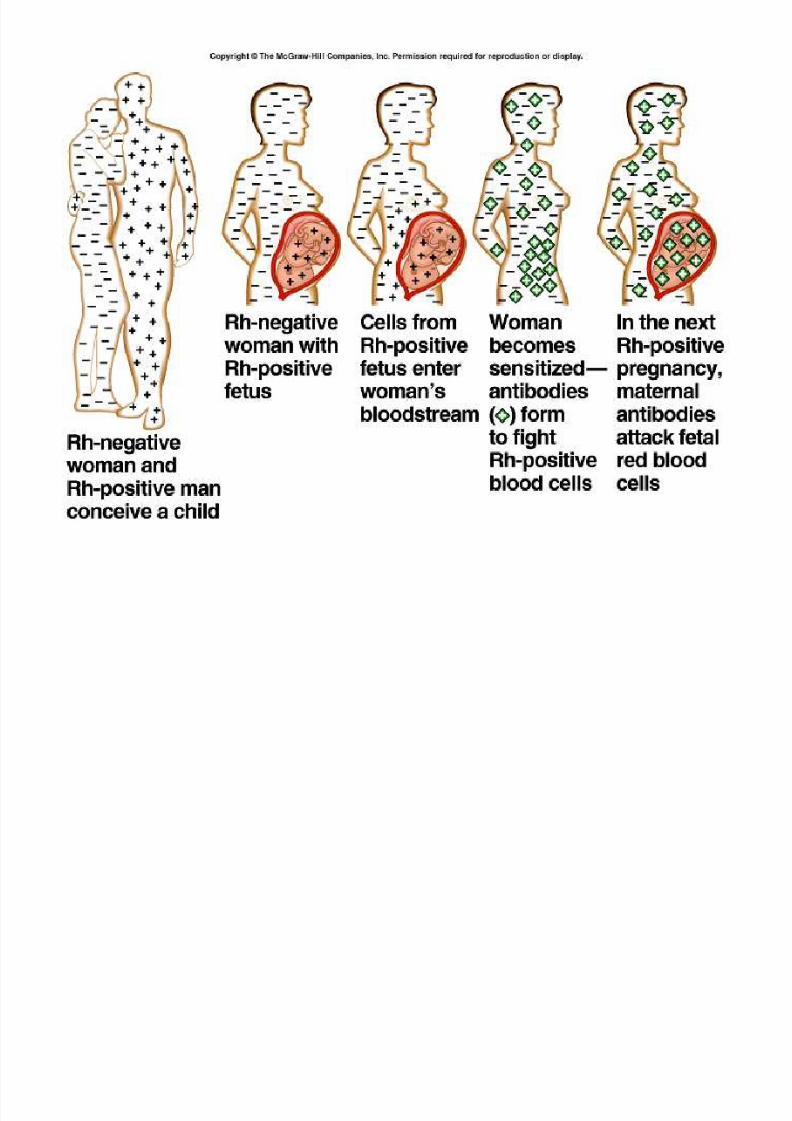
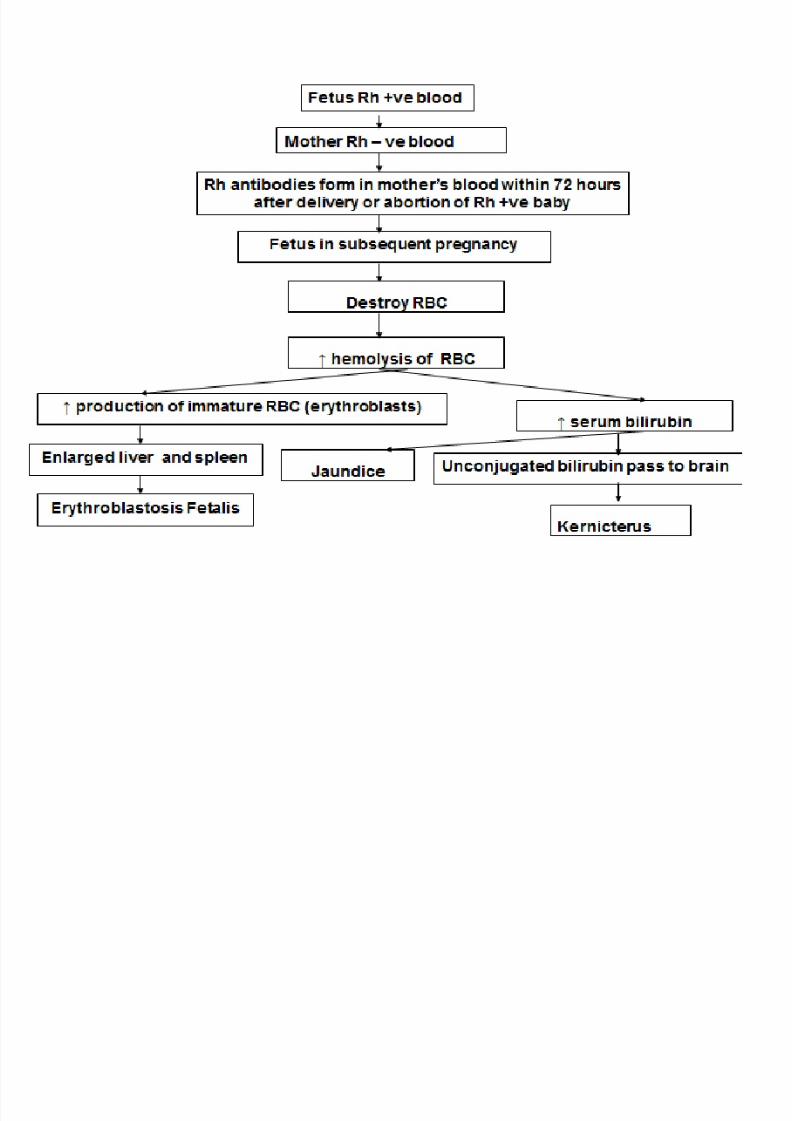
Rh incompatibility results from an antigen-
antibody reaction (alloimmunization).
The fetus develops anemia, jaundice, cardiac
failure (hydrops fetalis) and neurological
damage (kernicterus).
8/3/2019 Pregest Risk
http://slidepdf.com/reader/full/pregest-risk 28/65
8/3/2019 Pregest Risk
http://slidepdf.com/reader/full/pregest-risk 29/65
8/3/2019 Pregest Risk
http://slidepdf.com/reader/full/pregest-risk 30/65
Early Diagnosis Pregnancy f or Rh incompatibility
Hx previous blood transfusions
Blood group and Rh status of pregnant woman Rh antibody titer for Rh negative woman at the firstpregnancy visit and repeat at 32-38 weeks of pregnancy
Normal titer is 0Minimal ratio 1:8
Chorionic villus sampling in early pregnancy. Amniocentesis and amniotic fluid
spectrophotometry for biliribin Regular ultrasound from 14-18 weeks onwards look for fetal ascites and subcutaneous edema (hydropsfetalis)
8/3/2019 Pregest Risk
http://slidepdf.com/reader/full/pregest-risk 31/65
Prevention f or Rh incompatibility
Screening for the blood group of all
pregnant women. Arrange for further investigations if thewoman is Rh negative. Anti D (RhoD or RhoGAM) injection 300µg
IM for the mother at 28 weeks of gestation. Anti D (RhoD or RhoGAM) injection 300µgIM for the mother within 72 hours of anabortion, delivery of Rh positive baby or after
procedures like amniocentesis or chorionicvillus sampling.
8/3/2019 Pregest Risk
http://slidepdf.com/reader/full/pregest-risk 32/65
ANEMIA
8/3/2019 Pregest Risk
http://slidepdf.com/reader/full/pregest-risk 33/65
A low level of
hemoglobin (less than
10 gm/dl) duringpregnancy. Hemoglobin
carries oxygen to body
tissues via the red bloodcells
Anemia in pregnancy is
very common and is
present in almost 8o%
of pregnant women.
8/3/2019 Pregest Risk
http://slidepdf.com/reader/full/pregest-risk 34/65
CAUSES
Poor intake of iron in diet
Folic acid deficiency
Loss of blood from bleeding hemorrhoids orgastrointestinal bleeding.
Even if iron and folic acid intake are sufficient,a pregnant woman may become anemicbecause pregnancy alters the digestiveprocess.
Also the unborn child consumes some of theiron or folic acid normally available to themother's body.
8/3/2019 Pregest Risk
http://slidepdf.com/reader/full/pregest-risk 35/65
RISK FACTORS
Twin or multiple pregnancy
Poor nutrition, especially multiple vitamin
deficiencies
Smoking, which reduces absorption of
important nutrients
Excess alcohol consumption, leading to poor
nutrition
Any disorder that reduces absorption of
nutrient
8/3/2019 Pregest Risk
http://slidepdf.com/reader/full/pregest-risk 36/65
DIAGNOSIS
The blood tests determines the red blood cell
count, hemoglobin level ,iron and folic acid
levels in the blood.
8/3/2019 Pregest Risk
http://slidepdf.com/reader/full/pregest-risk 37/65
SIGNS AND SYMPTOMS
Comm
on Sympt
oms:
Tiredness, weakness or fainting.
Paleness
Breathlessness
Occasional Symptoms:
Headache
Nausea
Inflamed, sore tongue
Palpitations or an abnormal awareness of theheartbeat
Forgetfulness
Jaundice (rare)
Abdominal pain (rare)
8/3/2019 Pregest Risk
http://slidepdf.com/reader/full/pregest-risk 38/65
MEDICATIONS
Medications:
Iron deficiency anemia is treated with iron tablets, preferably as
ferrous sulphate 300 mg, to be taken no more than twice daily. Thisis because the side effects of iron tablets (stomach upset andconstipation) are increased if more than 2 tablets are taken.
About 20% of pregnant women fail to ingest or absorb adequateamount of iron and may need to be treated with intra-muscular ironinjections. Iron dextran is given every alternate day, in divided
doses, for a total of about 1000 mg. over a period of 3 weeks. Iron, folic acid and other supplements may be prescribed. For
better absorption, take iron supplements 1 hour before eating, orbetween meals. Iron will turn bowel movements black, and oftencauses constipation.
It is advisable that most pregnant women should be given
supplemental iron (ferrous sulphate 300 to 600mg per day). Eventhough the hemoglobin is normal at the beginning of pregnancy.This preventive measure prevents depletion of iron reserves andanemia that may occur in case of bleeding or with futurepregnancy.
Folic acid deficiency anemia is treated with folate tablets.
8/3/2019 Pregest Risk
http://slidepdf.com/reader/full/pregest-risk 39/65
PREVENTION
Eat foods rich in iron, such as liver, beef,
whole-grain breads and cereals, eggs anddried fruit.
Eat foods high in folic acid, such as wheatgerm, beans, peanut butter, oatmeal,mushrooms, collards, broccoli, beef liver andasparagus.
Eat foods high in vitamin C, such as citrus
fruits and fresh, raw vegetables. Vitamin Cmakes iron absorption more efficient.
Take prenatal vitamin and mineralsupplements, especially folic acid
8/3/2019 Pregest Risk
http://slidepdf.com/reader/full/pregest-risk 40/65
Activity:
No restrictions, except rest often until anemia
disappears.
Diet:
Eat well and take prescribed supplements
Increase fiber and fluid intake to prevent
constipation
8/3/2019 Pregest Risk
http://slidepdf.com/reader/full/pregest-risk 41/65
POSSIBLE COMPLICATIONS
Premature labor
Dangerous anemia from normal blood loss
during labor, requiring blood transfusions
Increased susceptibility to infection after
childbirth
8/3/2019 Pregest Risk
http://slidepdf.com/reader/full/pregest-risk 42/65
SUBSTANCE ABUSE
8/3/2019 Pregest Risk
http://slidepdf.com/reader/full/pregest-risk 43/65
Substance Abuse
Occurs when a person experiences difficulties
with work, family, social relations, & health as
a result of alcohol or drug use.
Drugs that are commonly misused includes:-
tobacco, alcohol, cocaine, marijuana,
amphetamines,barbiturates, hallucinogens,
club drugs, heroin andnarcotics.
8/3/2019 Pregest Risk
http://slidepdf.com/reader/full/pregest-risk 44/65
Substances commonly abused during pregnancy
1. Alcohol- is a central nervous system depressant& a potent teratogen.
The incidence of alcohol abuse is highest among
women ages 20 to 40 years although alcoholismis also seen in teenagers.
Chronic abuse of alcohol can undermine maternal
health by causing malnutrition, bone marrowsuppression, increased incidence of infections,& liver disease.
8/3/2019 Pregest Risk
http://slidepdf.com/reader/full/pregest-risk 45/65
Alcohol dependence-result is that a woman mayhavewithdrawal seizures in the intrapartal period
as early as 12 to 48 hours after se stops drinking.
Delirium tremens may occur in the postpartalperiod& the newborn may suffer a withdrawal
syndrome.
Care includes sedation to decrease irritability&tremors, seizure precautions, IV fluid therapyfor hydration & preparation foran addicted newborn.
8/3/2019 Pregest Risk
http://slidepdf.com/reader/full/pregest-risk 46/65
The effect of alcohol on the fetus may result in
a group of signs known as fetal alcohol
syndrome (FAS).
2. Cocaine & crack =Nearly 3% of pregnant
women use illicit drugs such as cocaine,marijuana, ecstasy, other amphetamines
&heroin.
Cocaine use during pregnancy tends to affectbetween1% & 5% of newborns
8/3/2019 Pregest Risk
http://slidepdf.com/reader/full/pregest-risk 47/65
Cocaine- acts as the nerve terminals to prevent
there uptake of dopamine & norepinephrine,
which in turn results in vasoconstriction,tachycardia, & hypertension.T his can be taken by
IV injection or by snorting the powdered form.
Crack- a form of freebase cocaine that is made
up of baking soda, water, and cocaine mixed into
a paste and microwaved to form a rock, can be
smoked. Smoking crack leads to a quicker, moreintense high because the drug is absorbed
through the large surface area of the lungs.
8/3/2019 Pregest Risk
http://slidepdf.com/reader/full/pregest-risk 48/65
Major adverse maternal effects of cocaine use
includes:
Hallucinations
Pulmonary edema
Cerebral hemorrhage
Respiratory failure
Heart problems
8/3/2019 Pregest Risk
http://slidepdf.com/reader/full/pregest-risk 49/65
Women who use cocaine have an increasedincidence of spontaneous abortion, abruptio
placentae, pretermbirth, and stillbirth.
Cocaine crosses into breastmilk and maycauses ymptoms in the breastfeeding infant,including extreme irritability, vomiting,diarrhea, dilated pupils, and apnea.
Thus, women who continue to use cocaineafte rchildbirth should avoid breastfeeding.
8/3/2019 Pregest Risk
http://slidepdf.com/reader/full/pregest-risk 50/65
3. Marijuana - is the most widely used illicit
drugs among women, both pregnant and non
pregnant. More than 25% womenof reproductive age admit to current or past
marijuana use. Marijuana use is associated
with impaired coordination, memory, andcritical thinking ability.
As a result, the pregnant women or new
mother who uses marijuana may be at risk
if she tries to perform tasks that
require complex mental activities.
8/3/2019 Pregest Risk
http://slidepdf.com/reader/full/pregest-risk 51/65
4. MDMA (Ecstasy)
Methylenedioxymethamphetamine (MDMA),
better known as Ecstasy, is the most
commonly used of a group of drugs referred
to as club drugs, so called because they have
become popular among adolescents andyoung adults who frequent dance clubs and
raves.
Is taken by mouth usually as a tablet. Itproduces euphoria and feelings of empathy
for others.
8/3/2019 Pregest Risk
http://slidepdf.com/reader/full/pregest-risk 52/65
5.Heroin - is an illicit CNS depressant narcotic that altersperception and produces euphoria. It is anaddictive drug that is generally administered IV.
Pregnancy in women who use heroin is consideredhighrisk because of the increased incidence in thesewomen of poor nutrition, iron deficiency anemia, andpreeclampsia.
The fetus of a heroin-addicted woman is at increasedrisk for IUGR, meconium aspiration, and hypoxia.
The newborn frequently show signs of heroin addictionsuch as restlessness; shrill, high-pitched cry; irritability;fist sucking, vomiting, and seizures.
8/3/2019 Pregest Risk
http://slidepdf.com/reader/full/pregest-risk 53/65
6.Methadone- is the most commonly usedtherapy for women dependent on opioids such asheroin.
Blocks withdrawal symptoms and reduces oreliminates the craving for narcotics.
Crosses the placenta and has been associatedwith preeclampsia, placental problems, andabnormal fetal presentation.
Prenatal exposure to methadone may result inreduced head circumference and lower birthweight.
8/3/2019 Pregest Risk
http://slidepdf.com/reader/full/pregest-risk 54/65
Management
A team approach to the care of the pregnantwoman with substance abuse problems ensuresthe management necessary to provide safelabor and birth for the woman and her child.
The management of drug addiction may includehospitalization if necessary to start detoxification.
Urine screening is also done regularly throughoutthe pregnancy if the woman has a known orsuspected substance abuse problem. This testinghelps to identify the type and amount of drugbeing abused.
8/3/2019 Pregest Risk
http://slidepdf.com/reader/full/pregest-risk 55/65
Little is yet known about the effects of MDMA
on pregnancy. However, the timing of ecstasy
used by the pregnant woman during fetalbrain development may be critical issue.
Infants exposed to ecstasy in uteromay experience some of the same risks as
infants exposed to other amphetamines
during pregnancy, including the possibility of withdrawal like symptoms such as drowsiness,
jitteriness, and breathing problems.
8/3/2019 Pregest Risk
http://slidepdf.com/reader/full/pregest-risk 56/65
IV. HIV/AIDS
Human immunodeficiency virus infection is
one of todays major health concerns.
It leads to a progressive disease that
ultimately results in acquiredimmunodeficiency syndrome (AIDS). Women
account for about 18% of cases in the U.S.
8/3/2019 Pregest Risk
http://slidepdf.com/reader/full/pregest-risk 57/65
Pathophysiology
HIV-1 enters the body through:Blood Blood Products Or other body fluids suchas semen, vaginal fluid and breastmilk
It affects T-cells, thereby decreasing the bodyssimmune responses.
This makes the affected person susceptible toopportunistic infections such as Pneumocystiscarinii
8/3/2019 Pregest Risk
http://slidepdf.com/reader/full/pregest-risk 58/65
Once infected with the virus, the individualdevelops antibodies that can be detected withthe enzyme-linked immunosorbent assay
(ELISA) & confirmed with the Western Blot test.
Can be detected within 6 mos after exposure.
Asymptomatic lasting from a few mos to as longas 17years.
Diagnosis of AIDS is made when a person isHIV positive & has one of several specificopportunistic infections.
8/3/2019 Pregest Risk
http://slidepdf.com/reader/full/pregest-risk 59/65
Maternal Risks
Many women who are HIV positive choose to avoid pregnancybecause of the risk of infecting the fetus &the possibility of dying beforethe child is raised.
Women who become pregnant should be advised that pregnancy isnot believed to accelerate the progression of HIV/AIDS, that the use of antiretroviral (ARV)therapy during pregnancy significantly reduces the riskof transmitting the HIV-1 to the fetus, and that most medications usedtreat HIV can be taken during the pregnancy.
Fetal-Neonatal Risks
HIV/AIDS may develop in infants whose mothers are seropositive,usually due to perinatal transmission. Perinatal transmissionoccurs transplacentally, at birth when the infant is exposed to maternalblood and vaginal secretions, via breastmilk.
anagemen
8/3/2019 Pregest Risk
http://slidepdf.com/reader/full/pregest-risk 60/65
g
Combination of ARV therapy suppresses viralreplication, helps preserve immune function,
and reduces the development of resistance.
Usually consists of two nucleoside analogues
reverse transcriptase inhibitors and a proteaseinhibitor
Zidovudine (ZDV) is perhaps the best known of
the nucleoside analogues
8/3/2019 Pregest Risk
http://slidepdf.com/reader/full/pregest-risk 61/65
Pregnant women who are currently on ARVtherapy should continue their provider-
recommended regimen and should receiveregular, careful monitoring for pregnancycomplications and possible toxicities.
Because the fetus is most susceptible toteratogenic effects during the first 10 weeks of pregnancy, and the risks of ARV therapy is not
well known, women in 1
st
trimester mightelect to delay therapy until after 12weeksgestation.
8/3/2019 Pregest Risk
http://slidepdf.com/reader/full/pregest-risk 62/65
To reduce the risk of perinatal transmission, all
pregnant women with HIV infection should be
offered the three-part ZDV prophylaxisregimen beginning after the first trimester.
This regimen includes:1.Oral ZDV daily
2.Intravenous ZDV during labor until birth
3.Oral ZDV for the infant starting 8 to 12 hoursafterbirth and continuing for 6 weeks.
8/3/2019 Pregest Risk
http://slidepdf.com/reader/full/pregest-risk 63/65
At each prenatal visit, asymptomatic, HIV infectedwomen are monitored for early signs of
complications, such as weight loss in the secondor third trimester or fever.
Each trimester the woman should have a visual
examination and examination of the retina todetect such complications as toxoplasmosis.
In addition to routine prenatal testing, the
woman who is HIV positive should be assessedregularly for serologic changes indicating thatHIV/Aids is progressing
8/3/2019 Pregest Risk
http://slidepdf.com/reader/full/pregest-risk 64/65
A pregnancy complicated by HIV infection,even if asymptomatic, is considered high risk,
and the fetus is monitored closely. Women who are HIV positive are at increased
risk for complications such as intrapartal orpostpartal hemorrhage, postpartal infection,
poor wound healing and infections of thegenitourinary tract.
Thus, they need careful monitoring andappropriate therapy as indicated.
HIV positive woman should be cautionedagainstbreast feeding her infant

8/3/2019 Pregest Risk
http://slidepdf.com/reader/full/pregest-risk 65/65





























