Embed Size (px)
Citation preview

Dear DoctorPublication of our Medical Digest is an effort to bring together some recent information and case studies from the KOLs in medical science. In this digest, we attempt to create a resource for the medical practitioners, physician assistant, and general practitioners to use to get a grasp on the issues and scope of problems that they confront in their day to day practice.
The Medical Digest contains a broad range of topics such as Hypertension in Adult, An Understanding of Cauda Equina Syndrome and Childhood mental problems: an overview. The articles in our medical digest are contributed by the physicians who are also the KOls in our country.
The authors are all practicing physicians The book has two sections and thirty two pages. As most of the articles are from our valued physicians we invite you all to read the digest and suggest us any improvements so as to enable us to serve you better.
In summary, we hope this book will enhance the practicing experience of all its users.
I hope you enjoy reading the “Medical Digest”.
Thanking you Best Regards
Dr. Afroza AkhterCell: 01713426579e-mail: [email protected]
Prefacekn
ow a
s yo
u go
1
CONTENTS
12
♦ An Understanding of Cauda Equina Syndrome
♦ Hypertension in Adult
♦ Childhood mental problems: an overview
21
Review Article
Series Article
03
2
Hypertension in AdultProf. Khan Abul Kalam Azad
MBBS, FCPS, MD, FACPProfessor and Head, Department of Medicine
Dhaka Medical College email: [email protected]
Hypertension is the most common condition seen in primary care and leads to myocardial infarction, stroke, renal failure, and death if not detected early and treated appropriately. The global age-standard prevalence of hypertension is 24.1% (21.4-27.1) in men and 20.1% (17.8-22.5) in women.
Defi ning Hypertension:The following defi nitions were suggested in 2003 by the seventh report of the Joint National Committee (JNC 7) and are based upon the average of two or more properly measured (table 2) readings at each of two or more offi ce visits after an initial screening:
Normal blood pressure: systolic <120 mmHg and diastolic <80 mmHg
Prehypertension: systolic 120 to 139 mmHg or diastolic 80 to 89 mmHg (see “Prehypertension”)
Series Article
3
Hypertension:
Stage 1: systolic 140 to 159 mmHg or diastolic 90 to 99 mmHgStage 2: systolic ≥160 mmHg or diastolic ≥100 mmHg
For most studies and in clinical practice, patients who are actively taking antihypertensive medications are usually defined as having hypertension regardless of their observed blood pressure.
Although definitions of hypertension (including stage 1 and stage 2 hypertension) and prehypertension were not specifically addressed in the 2014 Evidenced-Based Guidelines for Management of High Blood Pressure in Adults as reported by the panel members appointed to the eighth Joint National Committee (JNC 8), thresholds were adopted for the treatment of blood pressure that are generally consistent with these definitions.
European guidelines divide blood pressures below 140/90 mmHg into three categories (“optimal,” “normal,” and “high-normal”)
Isolated systolic hypertension is considered to be present when the blood pressure is ≥140/<90 mmHg, and isolated diastolic hypertension is considered to be present when the blood pressure is <140/≥90 mmHg.
Increasingly, the diagnosis of hypertension is made using ambulatory blood pressure monitoring (ABPM) or home blood pressure monitoring. The following diagnostic criteria were suggested by the 2013 ESH/ESC guidelines; meeting one or more of these criteria usingABPM qualifies as hypertension:• A 24-hour average of 130/80 mmHg or above• Daytime (awake) average of 135/85 mmHg or above• Nighttime (asleep) average of 120/70 mmHg or above
Diagnosis and evaluation of hypertension:Blood pressure measurement:At OPD set up care should be taken-• To allow the patients to sit for 3–5 minutes before beginning BP
measurements.• To take at least two BP measurements, in the sitting position,
4
spaced 1–2 min apart, and additional measurements if the first two are quite different. Consider the average BP if deemed appropriate.
• To take repeated measurements of BP to improve accuracy in p• To use a standard bladder (12–13 cm wide and 35 cm long),
but have a larger and a smaller bladder available for large (arm circumference >32 cm) and thin arms, respectively.
• To have the cuff at the heart level, whatever the position of the patient.
• When adopting the auscultatory method, use phase I and V (disappearance) Korotkoff sounds to identify systolic and diastolic BP, respectively.
• To measure the BP in the standing position in elderly subjects, diabetic patients, and in other conditions in which orthostatic hypotension may be frequent or suspected.
Identification of risk factors:• Age - Advancing age is associated with increased blood pressure,
particularly systolic blood pressure, and an increased incidence of hypertension.
• Obesity - Obesity and weight gain are major risk factors for hypertension and are also determinants of the rise in blood pressure that is commonly observed with aging
• Family history - Hypertension is about twice as common in subjects who have one or two hypertensive parents, and multiple epidemiologic studies suggest that genetic factors account for approximately 30 percent of the variation in blood pressure in various populations
• Race - Hypertension tends to be more common, be more severe, occur earlier in life, and be associated with greater target-organ damage in blacks.
• High-sodium diet - Excess sodium intake (eg, >3000 mg/day) increases the risk for hypertension, and sodium restriction lowers blood pressure.
• Excessive alcohol consumption• Physical inactivity - Physical inactivity increases the risk
for hypertension, and exercise is an effective means of lowering blood pressure.
• Diabetes and dyslipidemia - The presence of other cardiovascular risk factors, including diabetes and dyslipidemia, appear to be associated with an increased risk of developing hypertension.
5
• Personality traits and depression - Hypertension may be more common among those with certain personality traits, such as hostile attitudes and time urgency/impatience, as well as among those with depression.
Identification of secondary causes:• Medications:
♦ Oral contraceptives, particularly those containing higher doses of estrogen, which can often raise the blood pressure within the normal range but can also induce overt hypertension
♦ Nonsteroidal anti-inflammatory agents, particularly chronic use
♦ Antidepressants, including tricyclic antidepressants and selective serotonin reuptake inhibitors
♦ Glucocorticoids
♦ Decongestants, such as pseudoephedrine
♦ Weight loss medications
♦ Erythropoietin
♦ Cyclosporine
♦ Stimulants, including methylphenidate and amphetamines
♦ Illicit drug use – Drugs such as methamphetamines and cocaine
• Primary renal disease – Both acute and chronic kidney disease, particularly with glomerular or vascular disorders, can lead to hypertension.
• Primary aldosteronism – The presence of primary mineralocorticoid excess, primarily aldosterone, should be suspected in any patient with the triad of hypertension, unexplained hypokalemia, and metabolic alkalosis.
• Renovascular hypertension – Renovascular disease is a relatively common disorder. Renovascular hypertension is more often due to fibromuscular dysplasia in younger patients and more often due to atherosclerosis in older patients.
• Obstructive sleep apnea – Disordered breathing during sleep appears to be an independent risk factor for systemic
6
hypertension.• Pheochromocytoma – Pheochromocytoma is a rare cause of
secondary hypertension. About one-half of patients with pheochromocytoma have paroxysmal hypertension; most of the rest have what appears to be primary hypertension.
• Cushing’s syndrome – Cushing’s syndrome is a rare cause of secondary hypertension, but hypertension is a major cause of morbidity and death in patients with Cushing’s syndrome.
• Other endocrine disorders – Hypothyroidism, hyperthyroidism, and hyperparathyroidism may also induce hypertension.
• Coarctation of the aorta – Coarctation of the aorta is one of the major causes of secondary hypertension in young children, but it may also be diagnosed in adulthood.
Identification of complications:• Left ventricular hypertrophy (LVH) is a common and early
finding in patients with hypertension. LVH is associated with a higher incidence of subsequent heart failure, myocardial infarction, sudden death, and stroke.
• The risk of heart failure, both systolic (reduced ejection fraction) and diastolic (preserved ejection fraction), increases with the degree of blood pressure elevation. The pathogenesis of heart failure in patients with hypertension is both ischemic and nonischemic.
• Hypertension is the most common and most important risk factor for ischemic stroke, the incidence of which can be markedly reduced by effective antihypertensive therapy. It is also the most important risk factor for the development of intracerebral hemorrhage.
• Hypertension is a leading risk factor for ischemic heart disease, including myocardial infarction and coronary interventions.
• Hypertension is a risk factor for chronic kidney disease and end-stage renal disease. It can both directly cause kidney disease, which is called hypertensive nephrosclerosis, and accelerate the progression of a variety of other renal diseases.
Laboratory investigation:The following tests should be performed in all patients with newly
diagnosed hypertension:• Electrolytes and serum creatinine (to calculate the estimated
7
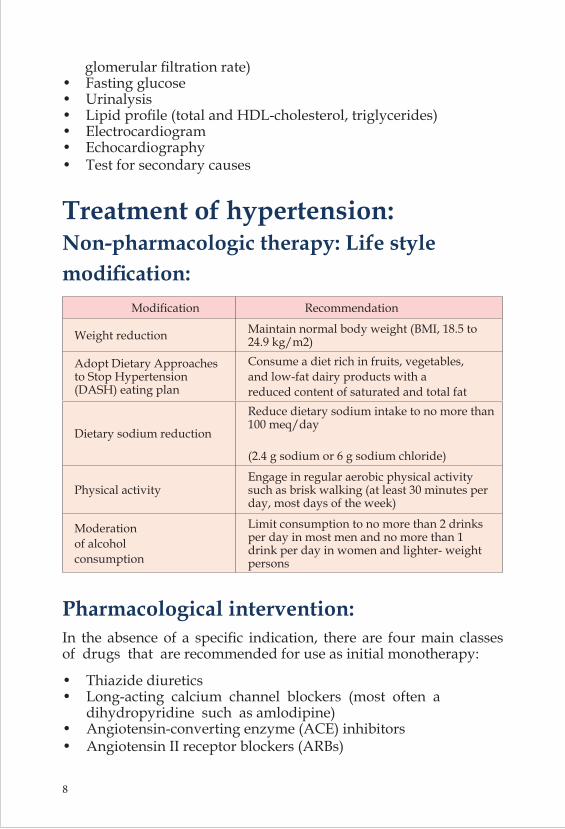
glomerular filtration rate)• Fasting glucose• Urinalysis• Lipid profile (total and HDL-cholesterol, triglycerides)• Electrocardiogram• Echocardiography• Test for secondary causes
Treatment of hypertension:Non-pharmacologic therapy: Life style modification:
Modification Recommendation
Weight reduction Maintain normal body weight (BMI, 18.5 to 24.9 kg/m2)
Adopt Dietary Approaches to Stop Hypertension (DASH) eating plan
Consume a diet rich in fruits, vegetables, and low-fat dairy products with a reduced content of saturated and total fat
Dietary sodium reduction
Reduce dietary sodium intake to no more than 100 meq/day
(2.4 g sodium or 6 g sodium chloride)
Physical activityEngage in regular aerobic physical activity such as brisk walking (at least 30 minutes per day, most days of the week)
Moderation of alcohol consumption
Limit consumption to no more than 2 drinks per day in most men and no more than 1 drink per day in women and lighter- weight persons
Pharmacological intervention:In the absence of a specific indication, there are four main classes of drugs that are recommended for use as initial monotherapy:
• Thiazide diuretics• Long-acting calcium channel blockers (most often a dihydropyridine such as amlodipine)• Angiotensin-converting enzyme (ACE) inhibitors• Angiotensin II receptor blockers (ARBs)
8
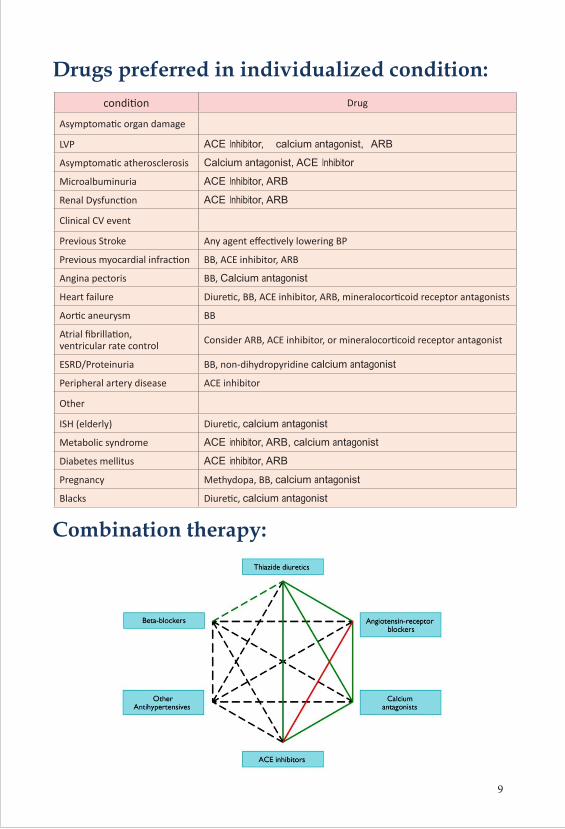
Drugs preferred in individualized condition:condition Drug
Asymptomatic organ damage
LVP ACE Inhibitor, calcium antagonist, ARB
Asymptomatic atherosclerosis Calcium antagonist, ACE Inhibitor
Microalbuminuria ACE Inhibitor, ARB
Renal Dysfunction ACE Inhibitor, ARB
Clinical CV event
Previous Stroke Any agent effectively lowering BP
Previous myocardial infraction BB, ACE inhibitor, ARB
Angina pectoris BB, Calcium antagonist
Heart failure Diuretic, BB, ACE inhibitor, ARB, mineralocorticoid receptor antagonists
Aortic aneurysm BB
Atrial fibrillation, ventricular rate control Consider ARB, ACE inhibitor, or mineralocorticoid receptor antagonist
ESRD/Proteinuria BB, non-dihydropyridine calcium antagonist
Peripheral artery disease ACE inhibitor
Other
ISH (elderly) Diuretic, calcium antagonist
Metabolic syndrome ACE inhibitor, ARB, calcium antagonist
Diabetes mellitus ACE inhibitor, ARB
Pregnancy Methydopa, BB, calcium antagonist
Blacks Diuretic, calcium antagonist
Combination therapy:
9
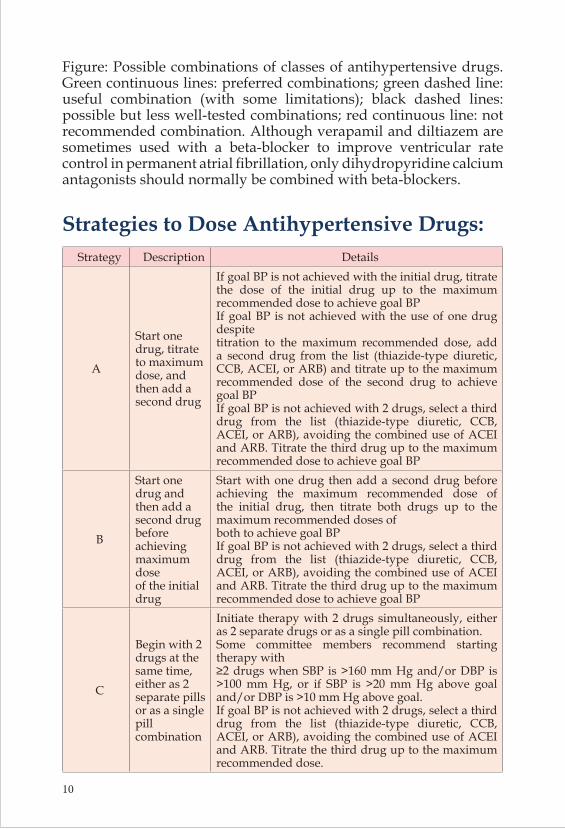
Figure: Possible combinations of classes of antihypertensive drugs. Green continuous lines: preferred combinations; green dashed line: useful combination (with some limitations); black dashed lines: possible but less well-tested combinations; red continuous line: not recommended combination. Although verapamil and diltiazem are sometimes used with a beta-blocker to improve ventricular rate control in permanent atrial fibrillation, only dihydropyridine calcium antagonists should normally be combined with beta-blockers.
Strategies to Dose Antihypertensive Drugs:Strategy Description Details
A
Start one drug, titrate to maximum dose, and then add a second drug
If goal BP is not achieved with the initial drug, titrate the dose of the initial drug up to the maximum recommended dose to achieve goal BPIf goal BP is not achieved with the use of one drug despitetitration to the maximum recommended dose, add a second drug from the list (thiazide-type diuretic, CCB, ACEI, or ARB) and titrate up to the maximum recommended dose of the second drug to achieve goal BPIf goal BP is not achieved with 2 drugs, select a third drug from the list (thiazide-type diuretic, CCB, ACEI, or ARB), avoiding the combined use of ACEI and ARB. Titrate the third drug up to the maximum recommended dose to achieve goal BP
B
Start one drug and then add a second drug beforeachieving maximum doseof the initial drug
Start with one drug then add a second drug before achieving the maximum recommended dose of the initial drug, then titrate both drugs up to the maximum recommended doses ofboth to achieve goal BPIf goal BP is not achieved with 2 drugs, select a third drug from the list (thiazide-type diuretic, CCB, ACEI, or ARB), avoiding the combined use of ACEI and ARB. Titrate the third drug up to the maximum recommended dose to achieve goal BP
C
Begin with 2 drugs at the same time,either as 2separate pills or as a singlepill combination
Initiate therapy with 2 drugs simultaneously, either as 2 separate drugs or as a single pill combination.Some committee members recommend starting therapy with≥2 drugs when SBP is >160 mm Hg and/or DBP is >100 mm Hg, or if SBP is >20 mm Hg above goal and/or DBP is >10 mm Hg above goal.If goal BP is not achieved with 2 drugs, select a third drug from the list (thiazide-type diuretic, CCB, ACEI, or ARB), avoiding the combined use of ACEI and ARB. Titrate the third drug up to the maximum recommended dose.
10
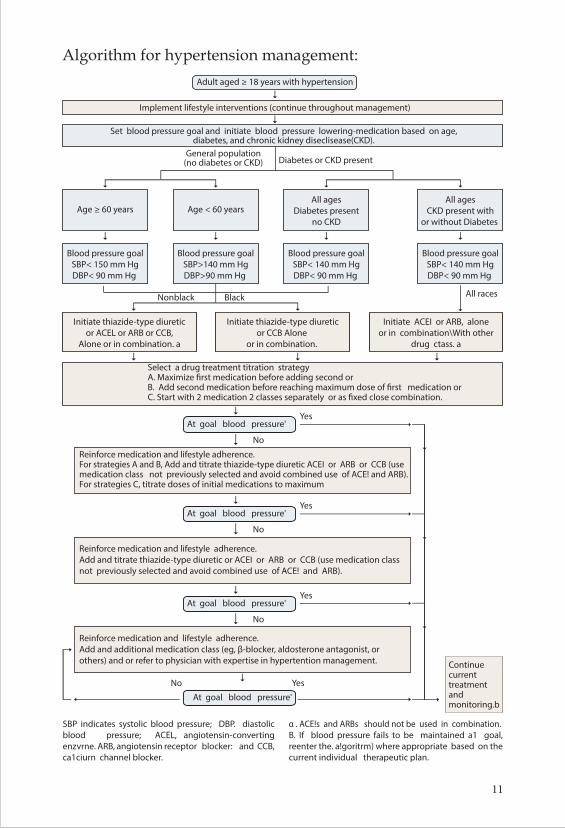
Algorithm for hypertension management:
11
An Understanding of Cauda Equina Syndrome
Sarkar S1, Mazumder U2 , Islam M M1, Dey A3, Dasgupta A1, Saha S1, Sazib SMF1
1. Department of Neurosurgery, Shaheed Suhrawardy Medical College, Dhaka, Bangladesh, 2. Dhaka Medical College Hospital, Dhaka, Bangladesh, 3. Bangabandhu Sheikh Mujib Medical University, Dhaka, Bangladesh,
1.Dr. Saumitra Sarkar, Associate Professor, Department of Neurosurgery, Shaheed Suhrawardy Medical College, Dhaka, Bangladesh. Email: [email protected]
2. Dr. Utpala Mazumder, Assistant Professor, Department of Gynae & Obs, Dhaka Medical College Hospital, Dhaka, Bangladesh
3. Dr. Md. Mohitul Islam, Assistant Professor, Department of Neurology, Shaheed Suhrawardy Medical College, Dhaka, Bangladesh
4. Dr. Avijit Dey, Resident, Department of Neurosurgery, Bangabandhu Sheikh Mujib Medical University, Dhaka, Bangladesh
5. Dr. Anindya Dasgupta, Resident, Department of Neurosurgery, Shaheed Suhrawardy Medical College Hospital, Dhaka, Bangladesh
6. Dr. Shuvro Saha, Resident, Department of Neurosurgery, Shaheed Suhrawardy Medical College Hospital, Dhaka, Bangladesh
7. Dr. S. M. Farhad Sazib, Resident, Department of Neurosurgery, Shaheed Suhrawardy Medical College Hospital, Dhaka, Bangladesh
Authors’ Disclosure StatementThe authors have no confl ict of interest in relation to this article.
Review Article
12
Background:Cauda equina syndrome (CES) is a serious neurologic condition in which neurological dysfunction affects the lumbar and sacral nerve roots within the vertebral canal. The nerves of the Cauda equine supply the muscles that control the bladder, bowel and the legs. Cauda equina syndrome is the symptoms which occur when the nerves of the Cauda equina are compressed. Recognition of CES is not only important to neurosurgeons and orthopaedic surgeons, but also to primary care practitioners, emergency room physicians, physiotherapists and allied health care professionals involved in management of back pain. It is an important diagnosis from a clinical and medico-legal perspective. Undiagnosed delays to diagnosis or a delay in treatment can have a disproportionate medico- legal impact. This article aims to provide an understanding of CES with illustrations of its common causes and mimics. CES results from dysfunction of the sacral and lumbar nerve roots within the vertebral canal producing impairment of bladder, bowel or sexual function and perianal or saddle numbness. Elucidation of these findings in the clinical examination is crucial. The number of potential aetiologies is vast but the most common causes are disc herniation, tumours, infection, spinal stenosis, inflammatory causes and vasculature occlusion. Early surgical decompression is advocated by most authors to best aid patient’s recovery and reduces long term disability.Key word: Cauda equina, saddle anaesthesia, disc herniation, early surgery.
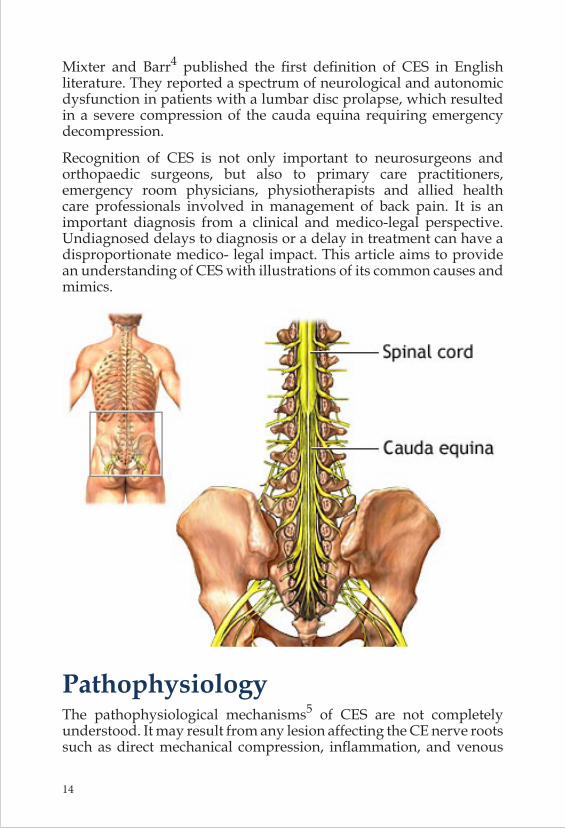
Introduction Cauda equina syndrome (CES) is a serious neurologic condition in which neurological dysfunction affects the lumbar and sacral nerve roots within the vertebral canal1.The spinal cord extends from the brain down through a canal inside the vertebral column. At each level of the spine nerves branch off from the spinal cord (nerve roots) and are responsible for sending signals to and from the muscles and other structures throughout the body. The spinal cord finishes just above the waist; below this is the group of nerves called the Cauda equina (CE). The nerves of the Cauda equine supply the muscles that control the bladder, bowel and the legs.
Cauda equina syndrome is the symptoms which occur when the nerves of the Cauda equina are compressed2. The term “cauda equina” was first applied by the French anatomist Lazarius3. In 1934,
13
Mixter and Barr4 published the first definition of CES in English literature. They reported a spectrum of neurological and autonomic dysfunction in patients with a lumbar disc prolapse, which resulted in a severe compression of the cauda equina requiring emergency decompression.
Recognition of CES is not only important to neurosurgeons and orthopaedic surgeons, but also to primary care practitioners, emergency room physicians, physiotherapists and allied health care professionals involved in management of back pain. It is an important diagnosis from a clinical and medico-legal perspective. Undiagnosed delays to diagnosis or a delay in treatment can have a disproportionate medico- legal impact. This article aims to provide an understanding of CES with illustrations of its common causes and mimics.
Pathophysiology The pathophysiological mechanisms5 of CES are not completely understood. It may result from any lesion affecting the CE nerve roots such as direct mechanical compression, inflammation, and venous
14
congestion or ischemia6. CE nerve roots are especially vulnerable to injury of compressive and tensile stresses. They are autonomic nerves and have nor schwann cell covering. Parke et al suggest there is an area of relative hypovascularity at the proximal portion of the root which is sensitive to neuroischemic manifestations concurrent with degenerative changes.
Delamarter et al7 analyzed evoked potentials and the pathology of cauda equina nerve root compression. They discovered that mild compression (25%) may not show signs of neurologic dysfunction, moderate compression (50%) may show signs of mild motor weakness with major changes in cortical evoked potentials and severe constriction (75%) may show signs of significant weakness, urinary incontinence and signs of complete nerve root atrophy at the level of the constriction. They found that chronic severe constriction blocked the axoplasmic flow, leading to distal motor Wallerian degeneration and proximal sensory Wallerian degeneration.
Incidence CES occurs in approximately 2% of cases of herniated lumbar discs and is one of the spinal surgical emergencies8. Following a lumbar disc prolapsed, Kostuik et al9 report an incidence of between 2-6%. Podnar et al10 reports an annual incidence rate of 1.5-3.4 million and period prevalence of 4.5-8.9 per 100,000 populations calculated.
SymptomsCauda Equina Syndrome presents as one or a combination of the following symptoms. Most commonly these symptoms develop suddenly and may worsen rapidly, within hours or days. However some people develop symptoms gradually11.
Saddle Anaesthesia• Loss of feeling between the legs• Numbness in or around the back passage and/or genitals• Inability to feel the toilet paper when wiping
15
Bladder disturbance• Inability to urinate (pass water)• Difficulty initiating urination (urinary hesitancy)• Loss of sensation when you pass urine.• Inability to stop or control urination (incontinence)• Loss of the full bladder sensation
Bowel disturbance• Inability to stop a bowel movement (incontinence)• Constipation• Loss of sensation when passing a bowel motion.
Sexual problems• Inability to achieve an erection or ejaculate (Males)• Loss of sensation during intercourse
Diagnosis: History and Clinical Examination There are no accepted criteria in the literature defining CES. Timely diagnosis and prompt treatment are however widely accepted. CES is a clinical diagnosis from the patient history and physical examination. Radiographic studies serve to confirm the diagnosis and define the pathological level of the lesion.
Gitelman et al reviewed 105 articles and proposed a single definition. For a diagnosis of CES, one or more of the following must be present: 1. Bladder and/or bowel dysfunction, 2. Reduced sensation in the saddle area, and 3. Sexual dysfunction, with possible neurologic deficit in the lower
limb (motor/sensory loss, reflex change).
Clinical scenarios for CES:1. Rapid onset without a previous history of back problems. 2. Acute bladder dysfunction with a history of low back pain and
sciatica.
16
3. Chronic backache and sciatica with gradually progressing CES often with canal stenosis.
ClassificationCES may be divided into complete or incomplete5.Incomplete cauda equina syndrome patients present with saddle anaesthesia and retention/incontinence of bladder or bowel.In incomplete CES there is saddle anaesthesia but bladder and bowel dysfunction has not progressed to full retention or incontinence.
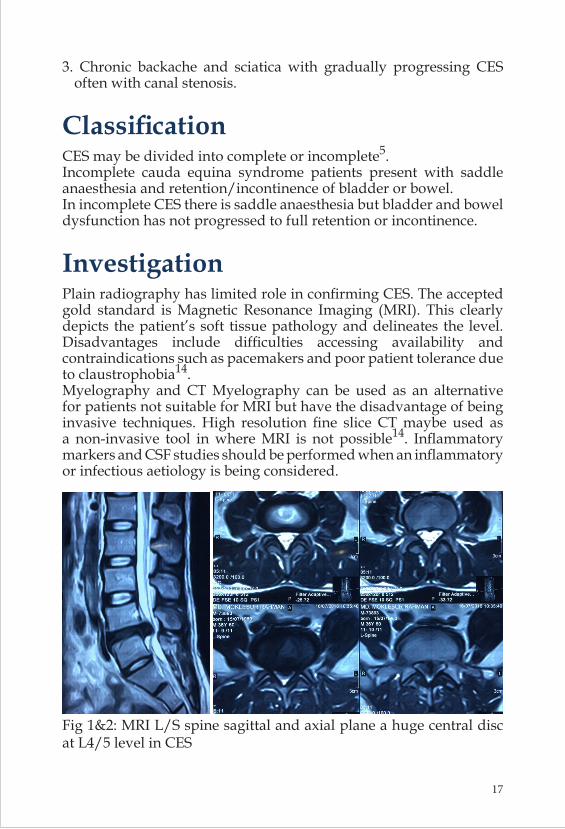
Investigation Plain radiography has limited role in confirming CES. The accepted gold standard is Magnetic Resonance Imaging (MRI). This clearly depicts the patient’s soft tissue pathology and delineates the level. Disadvantages include difficulties accessing availability and contraindications such as pacemakers and poor patient tolerance due to claustrophobia14.Myelography and CT Myelography can be used as an alternative for patients not suitable for MRI but have the disadvantage of being invasive techniques. High resolution fine slice CT maybe used as a non-invasive tool in where MRI is not possible14. Inflammatory markers and CSF studies should be performed when an inflammatory or infectious aetiology is being considered.
Fig 1&2: MRI L/S spine sagittal and axial plane a huge central disc at L4/5 level in CES
17
AetiologiesThe most common cause of CES is lumbar disc herniation atthe L4-L5 and L5-S1 level. Multiple other pathologies can damage the anatomical structures involved12,15.
Causes Lesions
Congenital Spinal dysraphismVertebral body malformations Dwarfing syndromes Congenital tumours
Acquired TraumaSpinal fracture or dislocation
Infective Bacterial abscess Tuberculosis
Neoplastic Primary tumourSecondary metastases
DegenerativeSpondylolisthesisSpinal stenosis Disc Prolapse
Inflammatory Rheumatoid arthritis Ankyolsing spondylitis
Vascular AV malformation Epidural or subdural haematoma
Iatrogenic Secondary to surgery
Management The aim of management for patients is to act as soon as possible to reduce the risk of permanent damage to the affected nerves. In acute compression of the conus medullaris or cauda equina, immediate surgical decompression is essential to reduce the pressure and increase the space in the vertebral canal. Traditionally, cauda equina syndrome has been considered a surgical emergency, with surgical decompression considered necessary within 48 hours after the onset of symptoms, and preferably performed within 6 h of injury15. Most authors advocate emergency surgical decompression to improve outcomes in CES, however there is controversy with regard to the timing of surgery. Although the majority of authors advocate early surgery within 24 hours to improve functional outcome, several
18
authors have shown little benefit to patients with complete cauda equina syndrome and early operative intervention. While there is debate about the exact timing of surgery in the literature, the consensus view is that those with incomplete cauda equina syndrome or indeterminate cases should be decompressed immediately as their neurologic and urologic outcomes are clearly improved if the patient does not progress to complete cauda equina syndrome16,17.Corticosteroid therapy may be beneficial in suppressing an inflammatory response but treatment must be started within eight hours of injury. If treatment begins after this time there appears to be no benefit and may even have detrimental effects18.
Surgical TechniqueThe accepted surgical technique for CES treatment is wide laminectomy and extensive decompression with foraminotomies as CES is often secondary to a large lumbar disc herniation. Several authors also aggressively remove disc space material after decompression. As for compressive hematomas or abscesses, tumours thorough evacuation becomes the mainstay of treatment15.
Key Learning Points1. Cauda equina syndrome (CES) is a pattern or neuromuscular and
urogenital symptoms resulting from compression of multiple spinal nerves.
2. Common symptoms are lower back pain, sciatica, saddle sensory disturbance, bladder & bowel dysfunction.
3. Narrowing of the spinal canal is responsible for the compression on the nerve roots.
4. Causes of CES include trauma, disc herniation, infection, neoplasm, spinal stenosis, and medical intervention.
5. Diagnosis is based on good clinical history and involves examination of muscle strength, tone, and tendon reflexes.
6. In most of the cases of CES is a clinical emergency, surgery is required to provide decompression in order to prevent permanent damage to the nerve roots.
7. Early surgical decompression is advocated by most authors to best aid patient’s recovery and reduces long term disability.
19
ConclusionConsidering the significant financial and social burden of this condition of a developing country, all primary care physicians have to be trained in identifying CES early among lot of nonspecific backaches. CES results from dysfunction of the sacral and lumbar nerve roots within the vertebral canal producing impairment of bladder, bowel or sexual function and perianal or saddle numbness. Elucidation of these findings in the clinical examination is crucial. The number of potential aetiologies is vast but the most common causes are disc herniation, tumours, infection, spinal stenosis, inflammatory causes and vasculature occlusion. Early surgical decompression is advocated by most authors to best aid patient’s recovery and reduces long term disability. There is evidence to suggest intervention within 24 hours significantly improves outcomes.
References:1. Fraser S, Roberts L, Murphy E. Caudae quina syndrome: a literature review of its definition and
clinical presentation. Arch Phys Med Rehabil. 2009:90(11);1964-68.2. Cohen MS, Wall EJ, Kerber CW, Abitbol JJ, Garfin SR. The anatomy of the cauda equina on CT
scans and MRI. J Bone Joint Surg Am. 1991;73(3):381-384. 3. Lazarius A. Historia anatomica humanicorporis. Frankfurt Germany: Becker; 1600: 178. 4. Mixter WJ, Barr JS. Rupture of the intervertebral disc with involvement of the spinal canal. N
Engl J Med 1934; 211: 210-215. 5. Wall EJ, Cohen MS, Massie JB, Rydevik B, Garfin SR. Caudaequina anatomy. I: intrathecal
nerve root organization. Spine.1990;15(12):1244-1247.6.. Parke WW, Gammell K, Rothman RH. Arterial vascularization of the cauda equina. J Bone Joint
Surg Am 1981; 63: 53-62. 7. Delamarter RB, Bohlman HH, Dodge LD, Biro C. Experimental lumbar spinal stenosis. Analysis
of the cortical evoked potentials, microvasculature, and histopathology. J Bone Joint Surg Am. 1990;72(1):110-120.
8. Shapiro S. Medical realities of cauda equina syndrome secondary to lumbar disc herniation. Spine. 2000;25(3):348-51.
9. Kostuik J. Medicolegal consequences of cauda equina syndrome: an overview. Neurosurgical focus. 2004;16(6):39--41
10. Podnar S. Epidemiology of cauda equina and conus medullaris lesions. Muscle Nerve 2007;35:529-31
11. Mooney V. Differential diagnosis of low back disorders: principles of classification. In: Frymore JW, editor. The adult spine: principles and practice. New York: Raven Press; 1991. p. 1559-60.
12. Gitelman A, Hishmeh S, Morelli BN, Joseph SA, Casden A, Kuflik P, et al. Cauda equina syndrome: a comprehensive review. Am J Orthop. 2008;37(11):556-62
13. Gleave JR, Macfarlane R. Cauda equina syndrome: what is the relationship between timing of surgery and outcome? Br J Neurosurg. 2002;16(4):325- 328
14. Sekiguchi M, Kikuchi S, Myers RR. Experimental spinal stenosis: relationship between degree of cauda equina compression, neuropathology, and pain. Spine.2004;29(10):1105-1111.
15. Ahn UM, Ahn Nu, Buchowski JM, Garrett ES, Siebert AN, Kostuik JP. Caudaequina syndrome secondary to lumbar disc herniation: a metaanalysis of surgical outcomes. Spine. 2000;25(12):1515-22
16. Hussain SA, Gullan RW, Chitnavis BP. Cauda equina syndrome: outcome and implications for management. Br J Neurosurg. 2003:17(2);164-7.
17. McCarthy MJ, Aylott CE, Grevitt MP, Hegarty J. Cauda equina syndrome: factors affecting long-term functional and sphincteric outcome. Spine. 2007;32(2):207-216.
18. Kohles SS, Kohles DA, Karp AP, Erlich VM, Polissar NL. Time-dependent surgical outcomes following cauda equina syndrome diagnosis: comments on a meta-analysis. Spine.2004;29(11):1281-1287.
20
Childhood mental problems: an overview
Helal Uddin Ahmed, M.D.Assistant Professor
Child Adolescent & Family PsychiatryNational Institute of Mental Health (NIMH), Dhaka, Bangladesh
IntroductionMental disorders in children are not very uncommon. Children have many developmental, emotional and behavioral problems, but every problem is not serious. In fact, many everyday stresses can cause changes in child’s behavior. Mental disorders of children have profound psychological, social and physical consequences. It is indicated that mental illnesses commonly have an onset early in life, continue during the years of an individual’s greatest potential for learning and productivity. If they remain untreated, they may lead to quite unproductive lives and poor social condition. Research shows that half of all lifetime cases of mental illness begin by age 14 years. (Kessler et al, 2005). Surveys have generally reported that psychiatric disorders are present in roughly 10-25% of children. In Bangladesh a community survey done on 2009 by National Institute of Mental Health with the collaboration of World Health Organization. That survey revealed the mental disorders among children in Bangladesh 18.4% [Figure 1].
Review Article
21
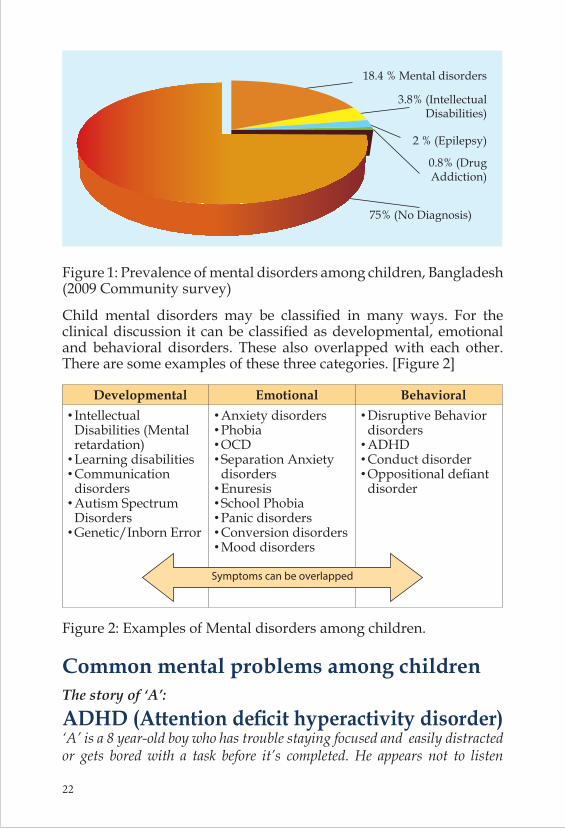
18.4 % Mental disorders
3.8% (IntellectualDisabilities)
2 % (Epilepsy)
0.8% (DrugAddiction)
75% (No Diagnosis)
Figure 1: Prevalence of mental disorders among children, Bangladesh (2009 Community survey)
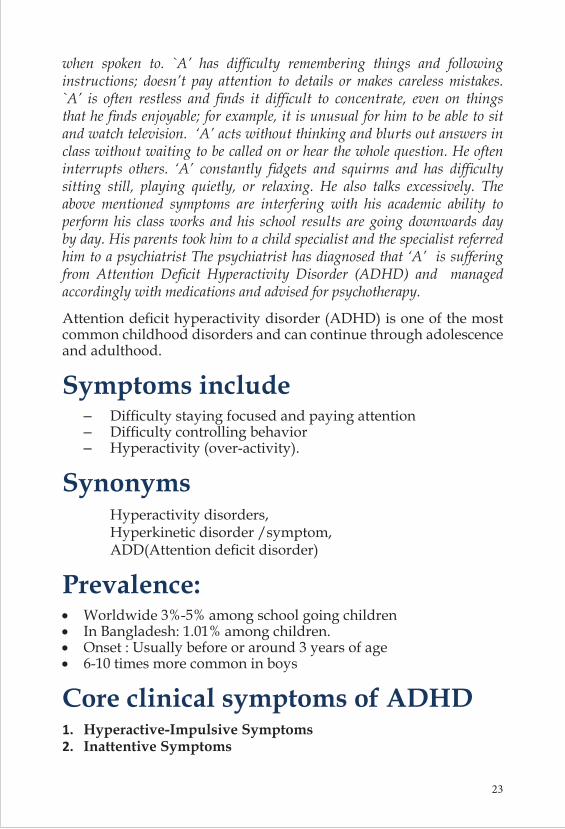
Child mental disorders may be classified in many ways. For the clinical discussion it can be classified as developmental, emotional and behavioral disorders. These also overlapped with each other. There are some examples of these three categories. [Figure 2]
Developmental Emotional Behavioral•Intellectual Disabilities (Mental retardation)•Learning disabilities•Communication disorders•Autism Spectrum Disorders•Genetic/Inborn Error
•Anxiety disorders•Phobia•OCD•Separation Anxiety disorders•Enuresis•School Phobia•Panic disorders•Conversion disorders•Mood disorders
Symptoms can be overlapped
•Disruptive Behavior disorders•ADHD•Conduct disorder•Oppositional defiant disorder
Figure 2: Examples of Mental disorders among children.
Common mental problems among childrenThe story of ‘A’:
ADHD (Attention deficit hyperactivity disorder)‘A’ is a 8 year-old boy who has trouble staying focused and easily distracted or gets bored with a task before it’s completed. He appears not to listen
22
when spoken to. `A’ has difficulty remembering things and following instructions; doesn’t pay attention to details or makes careless mistakes. `A’ is often restless and finds it difficult to concentrate, even on things that he finds enjoyable; for example, it is unusual for him to be able to sit and watch television. ‘A’ acts without thinking and blurts out answers in class without waiting to be called on or hear the whole question. He often interrupts others. ‘A’ constantly fidgets and squirms and has difficulty sitting still, playing quietly, or relaxing. He also talks excessively. The above mentioned symptoms are interfering with his academic ability to perform his class works and his school results are going downwards day by day. His parents took him to a child specialist and the specialist referred him to a psychiatrist The psychiatrist has diagnosed that ‘A’ is suffering from Attention Deficit Hyperactivity Disorder (ADHD) and managed accordingly with medications and advised for psychotherapy.
Attention deficit hyperactivity disorder (ADHD) is one of the most common childhood disorders and can continue through adolescence and adulthood.
Symptoms include – Difficulty staying focused and paying attention – Difficulty controlling behavior – Hyperactivity (over-activity).
Synonyms Hyperactivity disorders, Hyperkinetic disorder /symptom, ADD(Attention deficit disorder)
Prevalence:• Worldwide 3%-5% among school going children• In Bangladesh: 1.01% among children. • Onset : Usually before or around 3 years of age• 6-10 times more common in boys
Core clinical symptoms of ADHD1. Hyperactive-Impulsive Symptoms2. Inattentive Symptoms
23
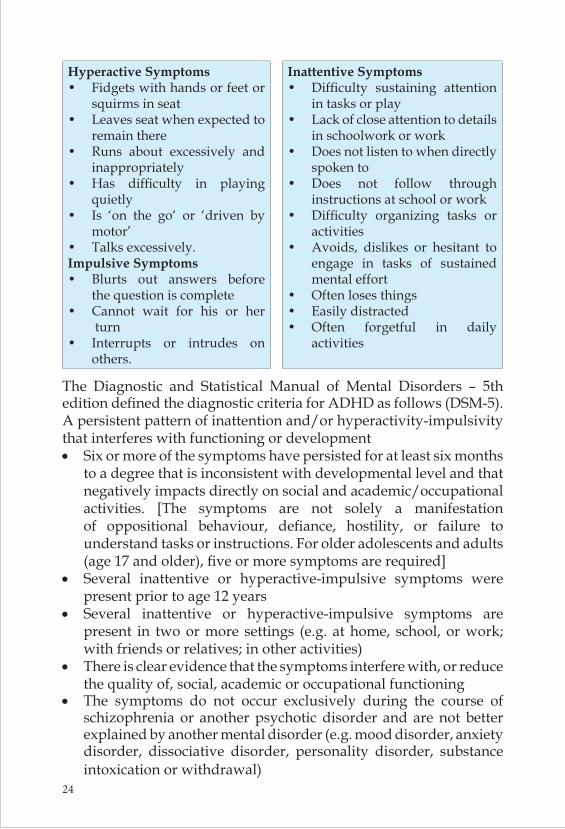
Hyperactive Symptoms• Fidgets with hands or feet or
squirms in seat • Leaves seat when expected to
remain there • Runs about excessively and
inappropriately• Has difficulty in playing
quietly• Is ‘on the go‘ or ‘driven by
motor’• Talks excessively.Impulsive Symptoms• Blurts out answers before
the question is complete • Cannot wait for his or her
turn • Interrupts or intrudes on
others.
Inattentive Symptoms• Difficulty sustaining attention
in tasks or play• Lack of close attention to details
in schoolwork or work• Does not listen to when directly
spoken to• Does not follow through
instructions at school or work• Difficulty organizing tasks or
activities• Avoids, dislikes or hesitant to
engage in tasks of sustained mental effort
• Often loses things• Easily distracted• Often forgetful in daily
activities
The Diagnostic and Statistical Manual of Mental Disorders – 5th edition defined the diagnostic criteria for ADHD as follows (DSM-5).A persistent pattern of inattention and/or hyperactivity-impulsivity that interferes with functioning or development • Six or more of the symptoms have persisted for at least six months
to a degree that is inconsistent with developmental level and that negatively impacts directly on social and academic/occupational activities. [The symptoms are not solely a manifestation of oppositional behaviour, defiance, hostility, or failure to understand tasks or instructions. For older adolescents and adults (age 17 and older), five or more symptoms are required]
• Several inattentive or hyperactive-impulsive symptoms were present prior to age 12 years
• Several inattentive or hyperactive-impulsive symptoms are present in two or more settings (e.g. at home, school, or work; with friends or relatives; in other activities)
• There is clear evidence that the symptoms interfere with, or reduce the quality of, social, academic or occupational functioning
• The symptoms do not occur exclusively during the course of schizophrenia or another psychotic disorder and are not better explained by another mental disorder (e.g. mood disorder, anxiety disorder, dissociative disorder, personality disorder, substance intoxication or withdrawal)
24
Subtype of ADHDCombined Inattentive Hyperactive/impulsive
All three core features are present and ADHD is diagnosed when ≥6 symptoms of hyperactivity/impulsivity and ≥6 symptoms of inattention have been observed for ≥6 months
Diagnosed if ≥6 symptoms of inattention (but <6 symptoms of hyperactivity/impulsivity) have persisted for ≥6 months
Diagnosed if ≥6 symptoms of hyperactivity/impulsivity (but <6 symptoms of inattention) have been present for ≥6 months
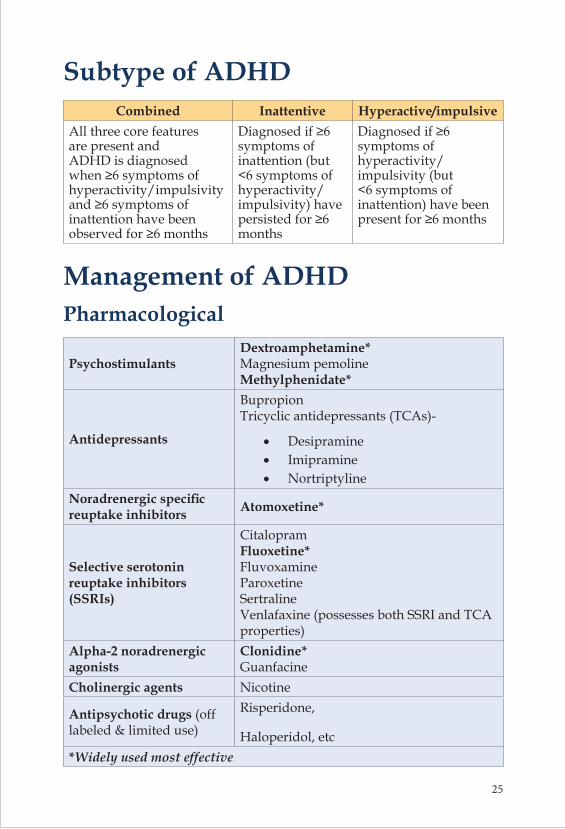
Management of ADHDPharmacological
Psychostimulants Dextroamphetamine* Magnesium pemoline Methylphenidate*
Antidepressants
Bupropion Tricyclic antidepressants (TCAs)-
• Desipramine• Imipramine• Nortriptyline
Noradrenergic specific reuptake inhibitors Atomoxetine*
Selective serotonin reuptake inhibitors (SSRIs)
Citalopram Fluoxetine* Fluvoxamine Paroxetine Sertraline Venlafaxine (possesses both SSRI and TCA properties)
Alpha-2 noradrenergic agonists
Clonidine* Guanfacine
Cholinergic agents Nicotine
Antipsychotic drugs (off labeled & limited use)
Risperidone,
Haloperidol, etc*Widely used most effective
25
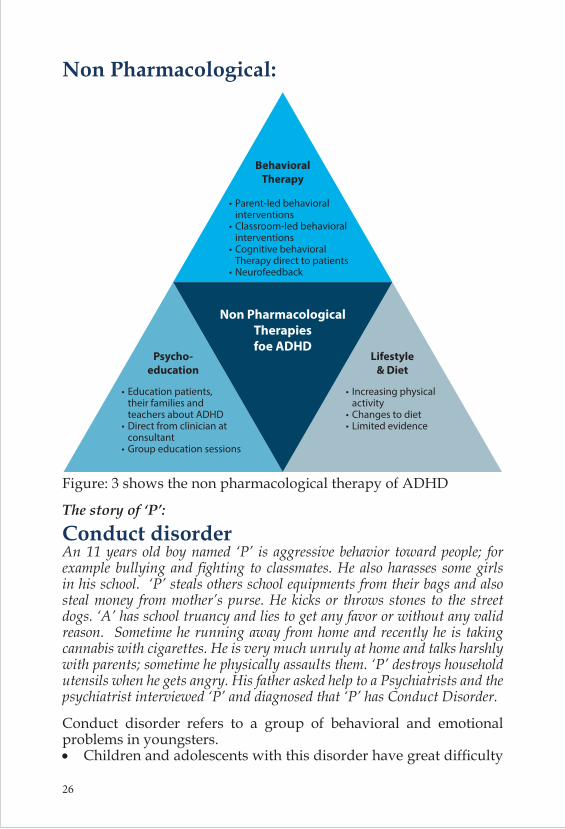
Non Pharmacological:
Figure: 3 shows the non pharmacological therapy of ADHD
The story of ‘P’:
Conduct disorderAn 11 years old boy named ‘P’ is aggressive behavior toward people; for example bullying and fighting to classmates. He also harasses some girls in his school. ‘P’ steals others school equipments from their bags and also steal money from mother’s purse. He kicks or throws stones to the street dogs. ‘A’ has school truancy and lies to get any favor or without any valid reason. Sometime he running away from home and recently he is taking cannabis with cigarettes. He is very much unruly at home and talks harshly with parents; sometime he physically assaults them. ‘P’ destroys household utensils when he gets angry. His father asked help to a Psychiatrists and the psychiatrist interviewed ‘P’ and diagnosed that ‘P’ has Conduct Disorder.
Conduct disorder refers to a group of behavioral and emotional problems in youngsters.• Children and adolescents with this disorder have great difficulty
26
following rules and behaving in a socially acceptable way. • They are often viewed by other children, adults and social
agencies as “bad” or delinquent, rather than mentally ill.
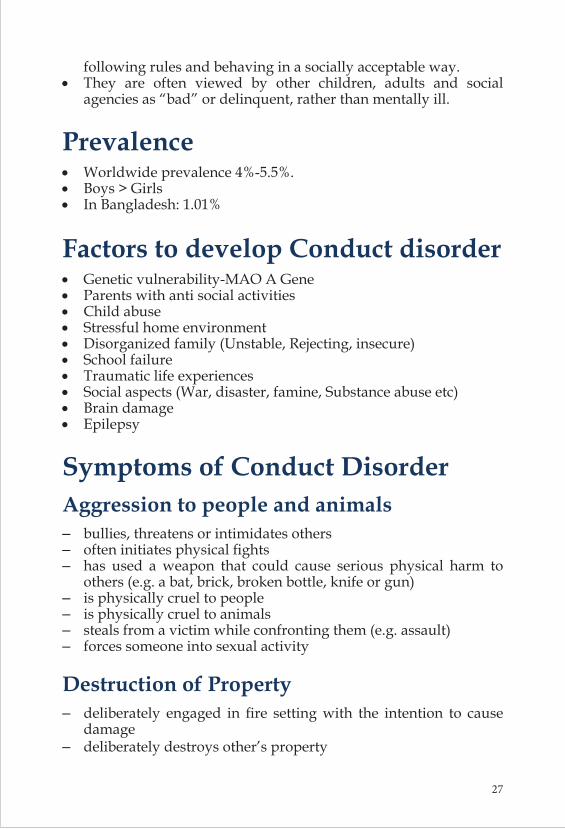
Prevalence • Worldwide prevalence 4%-5.5%.• Boys > Girls• In Bangladesh: 1.01%
Factors to develop Conduct disorder • Genetic vulnerability-MAO A Gene• Parents with anti social activities• Child abuse• Stressful home environment• Disorganized family (Unstable, Rejecting, insecure)• School failure• Traumatic life experiences• Social aspects (War, disaster, famine, Substance abuse etc) • Brain damage• Epilepsy
Symptoms of Conduct Disorder Aggression to people and animals – bullies, threatens or intimidates others – often initiates physical fights – has used a weapon that could cause serious physical harm to
others (e.g. a bat, brick, broken bottle, knife or gun) – is physically cruel to people – is physically cruel to animals – steals from a victim while confronting them (e.g. assault) – forces someone into sexual activity
Destruction of Property – deliberately engaged in fire setting with the intention to cause
damage – deliberately destroys other’s property
27
Deceitfulness, lying, or stealing – has broken into someone else’s building, house, or car – lies to obtain goods, or favors or to avoid obligations – steals items without confronting a victim (e.g. shoplifting, but
without breaking and entering)
Serious violations of rules – often stays out at night despite parental objections beginning
before age 13 years– runs away from home – often truant from school beginning before age 13 years
To diagnose the Conduct Disorder at least 3 out of above mentioned symptoms should be present for 12 months. The disturbance in behavior causes clinically significant impairment in social, academic, or occupational functioning.
Consequences of Conduct Disorder:• Mild Cases subside without formal treatment• Almost 50% develop antisocial behavior in adult life (Sociopathic
disorder)• Antisocial Personality disorder• Persistent social /interpersonal difficulties• Alcohol & other drug misuse• Criminality• Emotional Problems
Management of Conduct disorder• Assess severity and refer for treatment with a subspecialist as
needed.• Treat comorbid substance abuse first.• Describe the likely long-term prognosis without intervention to
caregiver.• Structure children’s activities and implement consistent behavior
guidelines.• Emphasize parental monitoring of children’s activities (where
28
they are, who they are with). Encourage the enforcement of curfews.
• Encourage children’s involvement in structured and supervised peer activities (e. organized sports, Scouting).
• Discuss and demonstrate clear and specific parental communication techniques.
• Help caregivers establish appropriate rewards for desirable behavior.
• Help establish realistic, clearly communicated consequences for noncompliance.
• Help establish daily routine of child-directed play activity with parent(s).
• Reinforcement of positive behavior• Psychotherapy: Family counseling, parental training, cognitive
therapy, cognitive behavior therapy • Consider pharmacotherapy for children who are highly
aggressive or impulsive, or both, or those with mood disorder. Mostly used mood stabilizers (Valproate, Lithium), Stimulant (Dextroamphetamine and methylphenidate ) antipsychotics (Risperidone, Haloperidol, Quitiapine etc) and/or antidepressants (Fluoxetine, Bupropion etc)
The story of ‘Z’:
Autism Spectrum Disorder‘Z’ is 4 years old boy. But he can’t speak properly. It is very difficult to express his thoughts or demand by using two or more words. Sometimes he repeats what other said to him. He has stereotype behaviors like flapping, moving hands etc. ‘Z’ not answers when call by his name and he has poor eye contact with others even with his parents. He likes to follow his own routine every day and any disruption of that routine makes him angry and sometime he bangs his head to the wall and crying and shouting inappropriately. His parents visited a child psychiatrist to know what problem ‘Z’ has. Psychiatrists comments that ‘Z’ has Autism Spectrum Disorder (ASD)
Autism Spectrum Disorder (ASD) is a lifelong Neuro-developmental condition that affects, among other things, the way an individual relates to his or her environment and their interaction with other people. The main areas of difficulty are in social communication, social interaction and restricted or repetitive behaviors and interests.
29
People on the autism spectrum may also have:• unusual sensory interests such as sniffing objects or staring
intently at moving objects• sensory sensitivities including avoiding everyday sounds and
textures such as hair dryers, vacuum cleaners and sand• intellectual impairment or learning difficulties
According to the Center of Disease control and prevention, (CDC) USA about 1 in 68 children has been identified with autism spectrum disorder (ASD). ASD is about 4.5 times more common among boys (1 in 42) than among girls (1 in 189). In Bangladesh there are some surveys on child mental health and revealed 1 in 125 children have autism spectrum disorder. (Rabbani, Alam, Ahmed 2009).Usually the symptoms appear near about 3 years of age.
The following signs may indicate the child is at risk for an autism spectrum disorder. If the child exhibits any of the following, need through evaluation by specialist:• No big smiles or other warm, joyful expressions by six months or
thereafter• No back-and-forth sharing of sounds, smiles or other facial
expressions by nine months• No babbling by 12 months• No back-and-forth gestures such as pointing, showing, reaching
or waving by 12 months• No words by 16 months• No meaningful, two-word phrases (not including imitating or
repeating) by 24 months• Any loss of speech, babbling or social skills at any ageCommon features of Autism Spectrum Disorder in Children:
Social Symptoms • Does not respond to name consistently when called • Tendency to avoid eye contact • Difficulty imitating the actions of others • Delays in imaginative play • Preference for solitary play • Limited back and forth play or interactions • Difficulty seeing things from another person’s perspective
30
• Failure to respond to social cues• Trouble understanding the perspective of others
Language Symptoms• Delayed speech language abilities/babbling • Delays in using gestures to communicate • Difficulty understanding body language• Trouble creating sentences• Tendency to repeat words or phrases
Behavioral Symptoms• Failure to seek comfort when upset • Frequent emotional outbursts or physical aggression
Common repetitive behaviors include:• Rocking• Twirling• Arranging objects in a particular order• Wiggling fingers• Flapping hands• Atypically intense or unusual interests
Management of ASD:Need early identification and intervention. Management includes education, training, and behavior shaping. Each person with autism is unique and, so, each intervention plan should be tailored to address specific needs. Early intensive behavioral intervention involves a child’s entire family, working closely with a team of professionals. Need speech therapy, occupational therapy and inclusive or special education. The target of management is to develop child’s social and learning skills. The Applied Behavior Analysis (ABA), Pivotal Response Therapy, Verbal Behavior Therapy is offered to the person with autism and his/her parents. Parents need training to learn how to deal with children with autism. Educational interventions, including behavioral strategies and habilitative therapies, are the
31

cornerstones of management of ASDs. These interventions address communication, social skills, daily-living skills, play and leisure skills, academic achievement, and maladaptive behaviors.Medication also indicated in autism to minimize the co-morbidity like seizure disorder, hyperactivity and sleep problems. Fewer antipsychotics (aripriprazole, risperidone) also approved to shape the behavioral problem of autism.
Conclusion:If we prevent and provide early intervention for mental disorders among children the overall mental health burden will be reduced. If child mental problems left untreated, mental disorders can impede all aspects of health, including emotional well-being and social development, leaving them socially isolated, stigmatized, and unable to optimize their social, vocational, and interpersonal contributions to society. In country like Bangladesh we have to raise our awareness in child mental health and need to reduced the stigma for a better nation.
References:1. Kessler RC, Chiu WT, Demler O, Merikangas KR, Walters EE. Prevalence, severity,
and comorbidity of 12-month DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry. 2005 Jun;62(6):617-27.
2. Rey JM. The epidemiologic catchment area (ECA) study: implications for Australia. The Med J Australia 1992; 156: 200-203.
3. Goodman R & Scott S, Child Psychiatry, 2nd Edition , Blackwell Publishing Ltd (2005)4. Rabbani MG, Alam MF, Ahmed HU, et al : Prevalence of mental disorders, mental
retardation, epilepsy and substance abuse in children. Bang J Psychiatry. 2009, 23 (1): 1-54.5. Cowen P, Harrison P, Burns T. Shorter Oxford textbook of psychiatry. 6th ed. Oxford:
Oxford University Press, 20126. American Psychiatric Association. (2013). Diagnostic and statistical manual of mental
disorders (5th ed.). Arlington, VA: American Psychiatric Publishing.7. https://www.autismspeaks.org/what-autism/treatment8. https://www.healthychildren.org/English/health-issues/conditions/Autism/Pages/
Early-Signs-of-Autism-Spectrum-Disorders.aspx9. http://www.adhd-institute.com/disease-management/non-pharmacological-therapy/10. https://www.cdc.gov/ncbddd/adhd/treatment.html
32





























