Embed Size (px)
Citation preview

PREDICTORS OF UNINTENTIONAL HOME INJURY
IN TODDLERS: AN EMPIRICAL TEST OF
A CAUSAL MODEL
JIRAWAN KLOMMEK
A DISSERTATION SUBMITTED IN PARTIAL FULFILLMENT OF
THE REQUIREMENTS FOR THE DOCTOR DEGREE OF PHILOSOPHY
IN NURSING SCIENCE
FACULTY OF NURSING
BURAPHA UNIVERSITY
JULY 2015
COPYRIGHT OF BURAPHA UNIVERSITY

ACKNOWLEDGEMENT
I would like to express my sincere gratitude toward persons and Asia Pacific
International University who provided educational financial support, gave advices, and
encouragement. These supports bring me to this precious moment, graduation.
First of all, I deeply thank Assoc. Prof. Dr. Nujjaree Chaimongkol who was
my major advisor for her knowledge and expertise, grace, teaching, guidance, and
affectionate relationship. I also would like to thank Assoc. Prof. Dr. Aporn Deenan
and Assoc. Prof. Dr. Pairatana Wongnam who were my co-advisors. They contributed
tremendous amount of knowledge and dedicated their personal time to be consultants
for students. Furthermore, I would like to give a special thank to Professor Dr. Louise
H. Flick who was an international co-advisor. She treated me with very friendly manner
and provided valuable guidance and ideas to fulfill my dissertation to be more completed
while I was in the USA. Moreover, I would like to thank Assoc. Prof. Adisak
Plitponkarnpim who provided financial support during data collection process. Special
thanks are given to all teaching faculties at Burapha University who gave this very
valued knowledge to me.
I sincerely thank Dr. Siriporn Tantipoovinai and Asia Pacific International
University (AIU) administrators who granted this scholarship. I also thank my colleagues
at Mission Faculty of Nursing at AIU who gave encouragement. Moreover, I would
like to give a special thanks to Dr. Jarurat Sriratanaprapat and Sucharit Yanissorn who
devoted their valued time and curtsey for supporting my study to be smooth throughout
these years. Indispensably, I thank all my friends in the doctoral program who gave
me encouragement and assistance in activities, as always.
I would like to thank Dr. Matthew L. Speltz, Dr. Deborah Glik, Dr. B. A.
Morrongiello, and Kieran J. Phelan and Assoc. Prof. Adisak Plitponkarnpim who
allowed me to use their measures without any charges in this study.
Lastly, I thank and appreciate my family, and husband, Virat Klommek, who
provided support in food and transportation, and gave me encouragement, always.
Jirawan Klommek

53810197: MAJOR: NURSING SCIENCE; Ph.D. (NURSING SCIENCE)
KEYWORDS: CAUSAL MODEL/ TODDLERS/ UNINTENTIONAL HOME
INJURY
JIRAWAN KLOMMEK: PREDICTORS OF UNINTENTIONAL HOME
INJURY IN TODDLERS: AN EMPIRICAL TEST OF A CAUSAL MODEL.
ADVISORY COMMITTEE: NUJJAREE CHAIMONGKOL, Ph.D., APORN
DEENAN, Ph.D. 151 P. 2015.
The purpose of this study was to test a causal model of unintentional home
injury in toddlers. Most of studies on unintentional home injury among toddlers have
shown complicated interactions among child attributes, parental supervisory
attributes, and home physical hazards. However, no study of predictors of
unintentional home injury has been empirically investigated. Samples of this study
consisted of 247 mothers of 1 - 3 year-old children living in Bangkok. Mothers were
interviewed by a package of questionnaires including Demographic Questionnaire,
Children’s Temperament for Injury Risk, Parental Protectiveness, Parental
Supervision, Parental Tolerance for Children’s Risk Taking, Parental Fate Belief, and
Unintentional Home Injury in Toddlers. Additionally, mothers’ homes were
naturalistically observed guided by The Home Physical Hazard Checklist.
Demographic characteristics of the sample were detailed using descriptive statistics.
Structural Equation Modeling was used to explore the magnitude of direct and
indirect effects of predicting variables on the unintentional home injury risk in
toddlers.
The results indicated that child temperament had the strongest significant
direct (positive) effect on unintentional home injury while parental supervision and
protectiveness had significant direct negative effects on unintentional home injury.
Parental supervision mediated the link between child temperament and parental
protectiveness and unintentional home injury. The model accounted for 37%
(R2 = .37) of the overall variance in the prediction of unintentional home injury in
toddlers. Findings suggest that health care providers should educate caretakers of
toddlers to prevent home injury by focusing these significant influencing factors.

CONTENTS
Page
ABSTRACT……………………………………………………………………… iv
CONTENTS……………………………………………………………………… v
LIST OF TABLES……………………………………………………………….. viii
LIST OF FIGURES………………………………………………………………. ix
CHAPTER
1. NTRODUCTION…………………………………………………………. 1
Significance of the problems………………………………………….. 1
Objective of the study…………………………………………………. 6
Research hypotheses…………………………………………………… 6
Conceptual framework………………………………………………… 7
Contribution to knowledge…………………………………………….. 12
Scope of the study……………………………………………………... 12
Definition of terms…………………………………………………….. 13
2. LITERATURE REVIEWS……………………………………………….. 14
Unintentional home injury in toddlers…………………………………. 14
Children’s gender is related to unintentional home injury in toddlers… 17
Children’s temperament is related to unintentional home injury in
toddlers....................................................................................................
19
Home physical hazards are related to unintentional home injury in
toddlers………………………………………………………………………………
22
Parental supervisory attributes are related to unintentional home injury
in toddles……………………………………………………………….
27
Concepts and models are related to unintentional home injury in
toddlers…………………………………………………………….......
32
3. RESEARCH METHODOLOGY…………………………………………. 44
Research design……………………………………………………....... 44
Population and sample…………………………………………………. 44
Setting of the study…………………………………………………….. 45
iv
V

CONTENTS (continued)
CHARPTER Page
Research instruments………………………………………………....... 48
A back-translation method…………………………………………...... 55
Psychometric properties of the measures……………………………… 57
Protection of human rights…………………………………………….. 59
Data collection procedures…………………………………………….. 59
Data analyses…………………………………………………………... 60
4. RESULTS…………………………………………………………………. 62
Description of the demographic information of the sample…………… 62
Description of home characteristics…………………………………… 64
Assumption tests for the SEM analysis………………………………... 66
Descriptive statistics for the continuous study of variables…………… 67
Hypothesized model testing…………………………………………… 68
Study findings related to research hypotheses………………………… 77
5. DISCUSSION AND CONCLUSION…………………………………….. 80
Summary of the study………………………………………………….. 80
Discussion of research findings………………………………………... 82
Limitations of the study………………………………………………... 89
Study strengths………………………………………………………… 90
Implications for nursing……………………………………………….. 90
Recommendations for future research Conclusion……………………. 91
Conclusion……………………………………………………………... 92
REFERENCES…………………………………………………………………… 93
APPENDICES……………………………………………………………………. 106
APPENDIX 1………………………………………………………………... 107
APPENDIX 2………………………………………………………………... 109
APPENDIX 3………………………………………………………………... 113
APPENDIX 4………………………………………………………………... 122
APPENDIX 5………………………………………………………………... 127
iv
V

CONTENTS (continued)
Page
APPENDIX 6………………………………………………………………... 129
BIOGHAPHY……………………………………………………………………. 151
iv
V

LIST OF TABLES
Tables Page
1. Sources and characteristics of the study variables…………………………... 53
2. Demographic characteristics of mothers…………………………………….. 63
3. Demographic characteristics of children…………………………………….. 64
4. Descriptive of home characteristics………………………………………….. 65
5. Descriptive statistics for the continuous study variables…………………….. 68
6. Statistics of model fit index between the hypothesize and modified model… 69
7. Standardized regression weights (Estimate), standard errors (S.E.), critical
ratio (C.R.), and p-value of the hypothesize model…………………………..
71
8. Parameter estimates of direct, indirect, and total effects of the hypothesized
model…………………………………………………………………………
73
9. Standardized regression weights (Estimate), standard errors (S.E.),
critical ratio (C.R.), and p-value of the modified model of UHI……………..
75
10. Direct, indirect, and total effects of causal variables on effect variables of
the modified model…………………………………………………………...
76
iv
V

LIST OF FIGURES
Figures Page
1. The hypothesized causal model of unintentional home injury in toddlers….. 11
2. The contributing factors to preschool unintentional injury model…………... 33
3. The conceptual model interactions between child, caregiver, and
environmental factors and sociocultural context influence child-injury risk...
36
4. The hypothesized mediated moderation model whereby temperament,
parenting, and ability overestimation predicted children’s unintentional
injury risk…………………………………………………………………….
37
5. The hypothesized mediated moderation model whereby gender, parenting,
and attribution of injury predicted children’s unintentional injury risk……...
39
6. The causal model of direct, indirect, and moderating effect on injuries in
preschool……………………………………………………………………..
40
7. The multi-stage stratified random sampling method use in this study……… 47
8. The process of back-translation in this study………………………………... 56
9. The hypothesized causal model of unintentional home injury in toddlers….. 72
10 The modified model of unintentional home injury in toddlers………………. 76
iv
V
CHAPTER 1
INTRODUCTION
Significance of the problems
Unintentional injury is defined as any injury from unspecified causes from
actions of a person or environment that make a wound or tissue damage to body parts
of human without purpose of harm (Hockenberry & Wilson, 2007; Sitthi-amorn et al.,
2006). Globally, unintentional injury is considered the foremost killer of young
children (National Injury Surveillance, Ministry of Publish Health [MOPH], Thailand,
2008; Safe kids USA, 2011). The World Health Organization [WHO] and United
Nations International Children's Emergency Fund [UNICEF] reported in 2004 that
unintentional injury has been ranked at the top of 15 leading causes of death among
1 - 4 years old children, and estimated that the mortality rate from unintentional injury
of this same age group was 45.8 per 100,000 populations (Bartolomeos, Mathers,
Oldenziel, Linnan, & Hyder, 2008; Towner & Scott, 2008). Unintentional injury is
not only depriving children of their lives but also leads to billions of dollars lost
annually in medical care costs, loss of children’s life quality, and parents’ loss of
productive work (Hutchings, Barnes, Maddocks, Lyons, & James-Ellison, 2010;
Schwebel & Gaines, 2007; Sitthi-amorn et al., 2006). In addition, unintentional injury
among young children is a significant global public health problem especially in low
and middle-income countries. It was reported in 2004 that the mortality rate from
unintentional injury among children aged 1 - 4 in low and middle-income countries
was nearly six times that of high-income countries (Towner & Scott, 2008).
Thailand is one of a group of low to - middle income countries, which have
had a high child mortality and morbidity rate due to unintentional injury (Linnan
et al., 2007; Sitthi-amorn et al., 2006). The prevalence of unintentional injury during
2003 to 2004 showed that more than 16 children died each day and around 6,000
children died annually (Sitthi-amorn et al., 2006). During 2008 - 2009, a report
showed that 8.2 % of injured children went to hospitals or clinics, and 1.9 % of them
were admitted in hospitals (Sangsupawanich, n.d.). Specifically, in children under five
years of age, during 2000 to 2003, another report showed that injury has been ranked

2
2
at top of five leading causes of death (MOPH & Ministry of Social Development and
Human Security [MSDHS], Thailand, 2008). In addition, unintentional injury caused
the highest mortality in children aged 1 - 4 years during 2003-2004. As a matter of
fact, morbidity from injury is more likely to be unintentional than intentional. Not
surprisingly, the leading cause of death was drowning, and when ranked from highest
to lowest, the leading causes of morbidity include: falls, animal bites, burns, transport
injuries, sharp objects, and poisonings (Sitthi-amorn et al., 2006). Unintentional injury
has led to death, permanent disability, hospitalization, and non-hospitalization in a
large group of young children worldwide.
As early as1949, Gordon (1949) proposed an understanding of unintentional
injury based on the interactions among the epidemiologic triad of agent, host, and
environment. The agent was described as various forms of energy that injure a person/
persons (e.g., thermal, radiant, chemical, electrical, and mechanical). The host was the
person/ persons hurt from the injury. The concept of environment included the
physical, biological, and socioeconomic surroundings that contributed to occurrence
of the injury (Gordon, 1949; Runyan, 2003). Gordon (1949) described the
demographics of the person/persons injured regarding their age, sex, race, and
economic status. The agent that could cause several types of injuries was specific; for
example, a glass door was the agent involved in cutting, collision, or crushing
injuries. The environment related to injury consisted of geographic characteristics
(such as climate, season, or topographical affairs), animals living with a person/
persons as pets or animals freely roaming in habitat such as rats, or snakes, and
included the structural environment, such as housing or buildings in rural or urban
areas. However, some researchers, i.e. Peterson, Farmer, and Mori (1987) and
Valsiner and Lightfoot (1987) considered that causal factors for injury are multi-
faceted and include both epidemiological and psychological characteristics which
might be co-occurring, leading to a deeper understanding of childhood injury risk.
Subsequently, Garzon (2005), Morrongiello (2005), Schwebel and Barton, (2005),
and Koulouglioti, Cole, and Kitzman (2009) suggested models of causal factors that
contribute to children’s unintentional injury and proposed interactions among risk
factors, and mediating or moderating factors leading to injury.
Garzon (2005) indicated that contributing factors to unintentional injury in

3
3
young children were three-fold: a child factor (e.g., development, physical, and
behaviors); an environmental factor (e.g., neighborhood, home physical hazards, and
the social environment); and an agent factor (e.g., automobile speed, sharp edged
toys, bullet velocity, heat of fire, and gravity). These risk factors interacted with one
another and with mediating factors, including parental recognition and modification
of the child, the environment, and the agent, while supervision interacted as a
mediating factor. Concurrently, Morrongiello (2005) suggested a model where
children, caregivers, and environmental hazards interacted and jointly influenced
injury as a dynamic system. This model also added that the socio-cultural context
could have direct influences on the model. Additionally, Schwebel and Barton (2005)
proposed two models related to child injury. Model-I showed that child temperament
and parenting had a direct effect on child injury risk. Assessment of the environmental
risk to children served as a mediator between child temperament and injury, and
between parenting and child injury. Model-II showed that child gender and parenting
had a direct effect on injury. Children’s attribution was also a mediator between child
gender and injury. Children’s attributions were both to their bad luck and to their
injury risk behavior. Boys tended to attribute their injuries to bad luck, whereas girls
tended to attribute their injuries to their own risky behavior. Recently, Koulouglioti
et al. (2009) studied factors that affected unintentional injury among toddlers. Their
causal model showed that maternal supervision had a direct effect on unintentional
injuries and that children’s everyday routines were a moderator between maternal
supervision and injuries. The investigators described children’s everyday routines as
being their daily activities in their home such as eating breakfast, going to bed, getting
up in the morning, having meals with their family, etc.
In addition, the Parental Monitoring Model, describing young children’s
safety and injury, described the relationship between parenting behavior and child’s
injury (Dishion & McMahon, 1998). The researchers indicated that parents increased
monitoring their child when in a high risk environment and decreased monitoring as
their child grew older. In addition, parental monitoring was described as supervision
which was influenced by parental beliefs and practices. Parents with high supervision
practices could reduce the rate of injury.
Accordingly, unintentional injury among young children has been of interest
4
4
for epidemiology, behavioral sciences, and psychosociology. The early studies
emphasized epidemiology including describing the characteristics of the host, the
kinds of agents, and the elements of environment which potentially influenced injury.
Knowledge was extended by the psychological approach that recognized the complex
interchanges between individual behaviors and environmental hazards related to
injury. In addition, an empirical study found that children’s attributes did not occur in
isolation but rather were influential within a complex set of parental supervisory
attributes, as well as the environmental and broader sociocultural contexts
(Morrongiello & Schwebel, 2008). Therefore, it is more likely that interrelated factors
among children’s attributes, parental supervisory attributes, and environmental
hazards would explain unintentional injury in young children.
Toddlers include children from one to three years old and are the most
vulnerable to the risk of injury at home. They are remarkable in their “heightened
sense of autonomy”, that is, they are discovering and experiencing their surroundings
on their own. However, they lack decision-making skills to differentiate what is
dangerous and what is safe (Cross, 2001; Hockenberry & Wilson, 2007). In addition,
toddlers’ characteristics, such as gender and temperament, could directly affect the
risk of injury. Boys tend to have more risk behaviors than girls, whereas girls were
more compliant with rules and were more easily managed than boys (Morrongiello,
Ondejko, & Littlejohn, 2004 a). Therefore, toddlers are particularly prone to
unintentional injury based on their developmental stage, gender, and temperament.
Most researchers show that boys are at greater risk of unintentional injury than girls,
especially in the home play area (Damashek et al., 2005; Morrongiello, Walpole, &
McArthur, 2009). Moreover, boys are more likely to have hyperactive behavior than
girls (Schwebel, Brezausek, Ramey, & Ramey, 2004). Children’s temperament refers
to specific expressive behaviors or emotional characteristics of children which
motivate them to interact with a specific situation or environment (Thomas & Chess,
1977). Numerous investigators have shown that children, who were rated as having
difficult temperaments, were at significantly greater risk of injury than those who
were rated as having easy temperaments (Dal Santo, Goodman, Gilk, & Jackson,
2004; Morrongiello, Corbett, McCourt, & Johnson; 2006 b; Schwebel et al., 2004).
On average boys had more difficult temperaments than girls (Schwebel, 2004).

5
5
Additionally, Goldsmith et al. (1987) suggested that the effect of temperament on
injury interacts with parental supervision. Children with difficult temperaments were
at particularly high injury risk when their parents provided less supervision
(Morrongirllo, Klemencic, & Corbett, 2008).
In addition to the toddlers’ attributes of gender and temperament, parental
supervisory attributes, and environmental hazards also contributed to unintentional
injury. Parental supervision has been described as watching, listening, and awareness
of the parent about their children’s whereabouts and monitoring their behaviors and
activities, either intermittently or constantly (Morrngiello, 2005; Saluja et al., 2004).
Researchers indicated that lack of, or inadequate, parental supervision was a risk
factor for unintentional home injury (Morrongiello, Ondejko, & Littlejohn, 2004 b;
Nakahara & Ichikawa, 2010). Morrongiello et al. (2008) argued that mothers who
spent less time with their children in view, such as watching or listening to what their
children were doing, had children who were exposed to more injury risk at home.
Although most parents closely supervised their children at home while they were
awake, around 20 % of mothers left their children alone at times (Morrongiello,
Corbett, & Brison, 2009; Morrongiello, Corbett, McCourt, & Johnson, 2006 a).
Additionally, parents, who tolerated children’s curiosity and allowed more of their
exploratory behavior, had children who were at higher risk than others. Inversely,
parents who had enough money and time to supervise their children could protect
even hyperactive children from injury (Schwebel et al., 2004). Morrongiello and
Corbett (2006) suggested that four parental supervision attributes were related to
unintentional injury risk: protectiveness, supervision, tolerance for child’s risk taking,
and fate beliefs. All of them were intercorrelated. For example, parental protectiveness
was positively related to supervision and both of them were negatively related to
tolerance for children’s risk taking and fate beliefs. Parental tolerance for children’s
risk taking was positively associated with fate beliefs. Additionally, they found that
parents who were more protective of their children had children with fewer injuries.
Similarly, parents who closely supervised their children had children who sustained
less injury (Morrongiello et al., 2008). Nevertheless, parents who tolerated their
children’s freedom of expression and exploration had children with less risk of injury
(Schwebel, 2004). Parents who believed injury related to bad luck (a fate belief) had

6
6
children who were prone to more injury (Morrongiello & Corbett, 2006). Although
most common hazardous environment has been demonstrated to be the home with
more than 60 % of unintentional injuries occurring in and around the home (Atak,
Karaoglu, Korkmaz, & Usubutun, 2010). The main locations in the home that
contributed to unintentional injuries included the kitchen, living room, bathroom,
child’s bedroom, and stairs (Atak et al., 2010; Phelan, Khoury, Xu, & Lanphear,
2009). Hard or sharp-edged furniture or substandard structures in the home were also
related to children’s injuries (Simpson, Turnbull, Ardagh, & Richardson, 2009).
Therefore, environmental or home physical hazards posed important and direct risks
for unintentional injuries to young children.
Most unintentional home injury risks to toddlers were preventable through
the effort of parents closely attending to children’s activities (Morrongiello et al.,
2008; Morrongiello et al., 2004 a) or through home design modifications to reduce
physical hazards (Dal Santo et al., 2004; Kendrick, Watson, Mulvaney, & Burton,
2005), the reviewed frameworks clearly revealed complicated interactions among
child factors, parental factors, environmental factors, and unintentional home injury.
Therefore, this study proposes the following causal model and aims to test the direct
and indirect effects among predictors of unintentional home injury to toddlers. Results
of this study can be used to guide development of a nursing intervention to prevent
unintentional children injury in the home and the community. Additionally, a better
understanding of the underlying causes of unintentional injury risk in toddlers at home
is essential.
Objective of the study
To test a causal model of unintentional home injury in toddlers
Research hypotheses
This study aims to test the following hypotheses, which were drawn from
the causal model depicted below:
1. Child gender (boy) has a direct positive effect on unintentional home
injury (UHI).

7
7
2. Child temperament has a direct positive effect on UHI.
3. Home physical hazards have a direct positive effect on UHI.
4. Parental protectiveness has a direct negative effect on UHI.
5. Parental supervision has a direct negative effect on UHI.
6. Parental tolerance for child’s risk taking has a direct positive effect on
UHI.
7. Parental fate beliefs have a direct positive effect on UHI.
8. Child gender, child temperament, and home physical hazards influence
UHI through parental protectiveness, supervision, tolerance for children’s risk taking,
and fate beliefs.
Conceptual framework
The conceptual framework of this study is guided by Garzon’s model
(Garzon, 2005). This model suggested that relationships among three main factors
contribute to the unintentional injury of toddlers including risk factors, mediating
factors, and outcomes.
Risk factors related to unintentional home injury in toddlers include child,
environment, and agent factors. Child factors were development, physical growth, and
behavioral characteristics. Toddlers’ developmental stage increased injury risk due to
their natural curiosity and exploration of new things within limited cognitive
understanding and physical ability. For example, they are at risk of a fall when they
try to reach the cookie jar on top of table but they do not realize the impact of their
weight on an unstable table. Toddlers’ physical growth also increases the risk of
falling and drowning injury due to their having larger and heavier heads in proportion
to their bodies than do older children or adults. The impulsiveness of toddlers also
increases injury risk. For example, children in this stage may try to put their fingers or
toys into electrical outlets and risk electrical injury. For environmental factors,
toddlers who live in and around hazardous homes, such as a home with unguarded
staircases, a poorly lit hallway, crowded spaces, or lead-substance contamination tend
to have higher injury rates than other children. The agent factors for toddler
unintentional home injuries include non-child-proof medicine containers, sharp edges
on toys, heat from fire, and effects of gravity in falling (Garzon, 2005). Additionally,

8
8
child gender, child difficult temperament, home physical hazard, and parental
supervision are proposed risk factors in Gordon’s (1949) hypothesized model and the
corresponding model proposed by Schwebel and Barton (2005). Child gender (boy),
child difficult temperament (i.e., aggressive, appositional, overactive, impulsive, and
uncontrolled behaviors), and low quality of housing are each associated with
unintentional home injury in toddlers. Boys are expected to have a higher rate of
activities, to be more impulsive, and approach physical hazards more quickly and with
less fear than girls. Parental close supervision is another facet that can reduce child
injury risk.
Mediating factors related to unintentional home injury in toddlers included
parental recognition and modification of hazards and a combination of parental
supervision, parental regonition and modification. Toddler injuries could be prevented
by parental recognition of their children’s specific high injury risk, potential severity
of injury, benefit of injury prevention, and their having fewer barriers to preventive
behavior. Moreover, toddler injuries could be decreased by parental modification of
the potential agents or environmental hazards such as safe storage of medication and
cleaning substances, or keeping floors dry. In addition, unintentional home injury in
toddlers was preventable by increasing parental close supervision on children, and
recognizing the high risk home locations (e.g., kitchen and bathroom) and modifying
these areas (Garzon, 2005). Moreover, including the influences from parental
supervisory attributes, particularly parental protectiveness, supervision, tolerance for
child’s risk taking, and fate beliefs, extend the model beyond Garzon’s by allowing
for mediated relationships between child gender, child difficult temperament, home
physical hazards and unintentional home injury in toddlers (Koulouglioti et al., 2009;
Morrongiello, 2005; Schwebel & Barton, 2005). Parents provided less close
supervision of boys than girls even when they exhibited the same injury-risk
behaviors. In addition, parents were more tolerable of risk taking of boys than girls
(Morrongiello, 2005). A difficult temperament child whose parents supervised closely
had less injury than an easy temperament child with less supervision (Schwebel &
Barton, 2005). Moreover, parents provided closer supervision to young children living
in high risk environments than those in low risk environments (Koulouglioti et al.
2009; Morrongiello, 2005).

9
9
Morrongiello and House (2004) and Morrongiello and Corbett (2006)
constructed the Parent Supervision Attribute Profile Questionnaire (PSAPQ), which
measures parental supervisory attributes related to unintentional home injury. The
PSAPQ consists of 29 items related to parental protectiveness, supervision, tolerance
for children’s risk taking, and fate beliefs. The using this questionnaire revealed that
parental protectiveness had the greatest positive relation to supervision. Inversely,
parental tolerance for children’s risk taking had the highest positive correlation with
parental fate beliefs. Parental tolerance for children’s risk taking and fate beliefs were
negatively associated with parental protectiveness and supervision. Moreover, the
Parental Monitoring Model (Dishion & McMahon, 1998) also provided a basic
understanding of a set of relationships among parenting behaviors, and children’s
activities, whereabouts, and adaptation. Parental monitoring was described in term of
supervision, and may serve as a protective factor for children living in high-risk
settings (Dishion & McMahon, 1998). Hence, all of these concepts are proposed to
have complex links rather than an individual or a direct link to risk of injury.
This study’s hypothesized causal model of unintentional home injury in
toddlers, which is based on the published literature, has four parental supervisory
attributes which are: 1) protectiveness, 2) supervision, 3) tolerance for child’s risk
taking, and 4) fate beliefs. They are related to child gender and temperament and the
home’s physical hazards. Boys are more prone to unintentional injury at home than
girls are (Morrongiello et al., 2004 a). Children with difficult temperament have
higher injury rates than children with easy temperaments (Damashek et al., 2005;
Ordoñana, Caspi, & Moffitt, 2008). Furthermore, children who live in environments
with more physical hazards have more injury than children who live in environments
with fewer physical hazards (Sirisamutr, 2008). In addition, high-protective-behavior
parents bring up children with less injury than low-protective-behavior parents.
Similarly, parents who closely supervise or provide constant supervision, bring up
their children with less injury than parents with inadequate supervision do
(Morrongiello & House, 2004). Inversely, parents who have more tolerance for their
children’s risk-taking expose their own children to more injury than parents who have
less tolerance for their children’s risk-taking. Lastly, parents who believe in fate have
children who are exposed to more injury risk than parents who believe that injury risk

10
10
is preventable (Morrongiello & Hogg, 2004). Therefore, this conceptual framework is
developed with an intention to identify key factors that are associated with
unintentional injury among toddlers at home. The hypothesized model is illustrated in
Figure 1.

11 11
Figure 1 The hypothesized causal model of unintentional home injury in toddlers
Child gender
(boy)
Unintentional
Home injury
in Toddlers
Parental
protectiveness
Parental
supervision
Parental
risk tolerance
Parental
fate beliefs
Child
temperament
Home
physical
hazard

12
12
Contribution to knowledge
1. In the nursing profession, pediatric nurses can create the educational
guidelines and risk assessment forms for toddler’s parents to assess the home’s
physical hazards and child temperament; as well as, recommend changing patterns of
supervision and modifying the environment to reduce injury risk. Pediatric nurses can
also give counseling routinely regarding parent’s management of toddlers’
temperament, patterns of supervision related to home physical hazards and its related
application.
2. In nursing education, nurses can utilize the new knowledge by teaching
and creating an awareness in nursing students, families, and communities about the
importance of child gender (boy) and difficult temperament, home physical hazards,
and parental supervisory attributes that can increase unintentional injuries among
toddlers at home. Especially, they can communicate the importance of parental
protectiveness and supervision that can prevent child injuries and that parental risk
tolerance and fate beliefs can increase child injuries.
3. In nursing administration, nurses can set safety standards for young
children in their homes that target toddlers’ unintentional injuries and for providing
support when homes are below the safety standards. Nurses can encourage nursing
managers, who are responsible for caring for the health of toddlers, to establish
strategies that will promote education to promote parental safety supervision; for
example, to identify each parent responsible for supervising their toddler and to
correct their supervision when there is inappropriate supervision.
4. In nursing research, nurses can create effective intervention programs
that foster the establishment of parental supervisory attributes. This may facilitate
parents’ supervision task and create an optimal environment in and around their
homes, which could lead to lower injury risk among toddlers.
Scope of the study
This study recruited 250 mothers who had children aged 1 to 3 years old,
currently residing in the Ratchathewee district of Bangkok Metropolitan, and
continuously taking care of their children for at least 6 months. Data were collected

13
13
from November 2013 to February 2014.
Definition of terms
Unintentional home injury to toddlers refers to children aged 1 - 3 years
old experiencing an incident of unintentional injury in the past six months inside or
around their home. It was measured by the likelihood of injury (Glik, Kronenfeld, &
Jackson, 1991).
Parental protectiveness refers to parents’ feelings, thoughts, and actions
that prevent or make sure their children are safe from all dangers both inside and
around their home. It was measured by the Parental Protectiveness subscale of the
PSAPQ (Morrongiello & Corbett, 2006; Morrongiello & House, 2004).
Parental supervision refers to parental watching, hearing, observing, or
controlling their children’s whereabouts or playing appropriately inside and around
their home. It was measured by the Parental Supervision subscale of the PSAPQ
(Morrongiello & Corbett, 2006; Morrongiello & House, 2004).
Parental tolerance for child’s risk taking refers to parents allowing or not
preventing their child’s having experiences or activities inside and around their home.
It was measured by the Parental tolerance for child’s risk taking subscale of the
PSAPQ (Morrongiello & Corbett, 2006; Morrongiello & House, 2004).
Parental fate beliefs refer to parents’ beliefs that children’s risk of injury is
a matter of good or bad luck. It was measured by the Parental Fate beliefs subscale of
the PSAPQ (Morrongiello & Corbett, 2006; Morrongiello & House, 2004).
Child temperament refer to the expression of a child’s risk-taking behavior
upon a situation or their attraction to an environment that motivates them to take risks
(e.g. “Jumps off furniture or other structures”, “Comes into contact with hot objects,
“Stands on chairs”). It was measured by the Injury Behavior Checklist (IBC) (Speltz,
Gonzales, Sulzbacher, & Quan, 1990).
Home physical hazards refers to structures, objects, equipments, chemical
products or furniture at home that could potentially be harmful to children and cause
injury. It was measured by the Home Injury Survey (Phelan et al., 2009) and Home
Observation Checklist (Plitapolkarnpim, n.d.).

CHAPTER 2
LITERATURE REVIEWS
This study aimed to test a causal model of unintentional home injury in
toddlers. This chapter describes a review of related literature regarding unintentional
home injury in toddlers; factors influences unintentional home injury in toddlers child
gender (boy), child temperament, parental supervisory attributes, and home physical
hazards; and concepts and models related to unintentional home injury in toddlers.
Unintentional home injury in toddlers
Toddlers are boys or girls from 1 - 3 years old. Numerous investigators
indicated that most unintentional injuries among toddlers occurred at home (Atak
et al., 2010; Simpson et al., 2009; Sirisamutr, 2008). The prevalence of fatal
unintentional home injury in the United States during 1992 - 1999 showed that death
rate of children 1 - 4 years old was around four times that of children 5 - 9 years old
and five times that of children 10 - 14 years old, respectively (Runyan et al., 2005).
Similarly in Germany, in 1995, the mortality rate from unintentional injury in and
around home was the highest among children at this age (Ellsäßer & Berfenstam,
2000). While in 2004, the rate of non-fatal unintentional home injury in Turkey was
the highest among children 0 - 4 years old (Alptekin, Uskun, Kisioglu, & Ozturk,
2008). In Canada, children younger than 4 years old visited an emergency room with
unintentional home injuries more than children older than aged 4 (Bernard-Bonnin
et al., 2003). A joint report between WHO and UNICEF in 2004 found that the
unintentional injury death rate among children 1 - 4 years old in low and middle
income countries was higher than those in high income countries (Towner & Scott,
2008). Particularly, a report from low and middle income countries in Asia during
2000 to 2005 found that mortality rate had rapidly changed from non-communicable
disease to unintentional injury at this age (Linnan et al., 2007).
Thailand was a developing country in which most people live in low to
middle income families (Linnan et al., 2007). Unintentional injury in and around the
home has been a major contributor to young Thai children’s death, disability, and

15
hospitalization rates. A report on the Second Thai Citizen Health Survey by Physical
Examination, during 1996 to 1997 found that nearly 20 % of children under 5 years of
age had experienced serious injuries and a Health Survey of Thai Citizen by Physical
Examination between 2008 to 2009 showed that the leading cause of serious injuries
to this age group of children was falls, while the second was traffic accidents,
followed by cuts from sharp objects (Sangsupawanich, n.d.). A survey during 2003 to
2004 found that nearly 50 % of all deaths in toddlers was caused by injury (Sitthi-
amorn et al., 2006). In 2004, a report indicated that the death rate from unintentional
injuries in toddlers was higher than children 5-14 years old. It found that boys’ death
rate was 47.2 per 100,000 children, and girls’ death rate was 44.3 per 100,000
children accordingly (Bartolomeos et al., 2008). Unintentional injury in toddlers is
still a major problem that occurs particularly in and around home (Linnan et al.,
2007). However, the pattern of children’s unintentional injuries suggests that it is
based on the developmental stage of children’s age-related development.
Toddlers have particular kinds of injury due to their developmental stage.
They are transitioning from total dependence on parents to autonomy and
independence (Colson & Dworkin, 1997). They have rapidly developing motor skills,
identity, autonomy, and self-esteem while their cognitive skills are still characterized
by preoperational thought (Dolan & Holt, 2008). By 1 to 2 years of age, children start
to walk, run, climb, jump, and increase their speed and strength but their visual acuity
has only reached about 20/ 100 feet, and only 20/ 30 by the age of 3. Their heads are
proportionally large compared to the size of their bodies making it difficult for them
to maintain their balance and stability when they move (Puckett & Black, 2005). As a
result, they are more likely to be injured on their faces and heads than are older
children. Children at this age are remarkable in their “heightened sense of autonomy,”
that is, they are discovering and experiencing their surroundings on their own.
However, they still lack knowledge, experience, and decision-making skills to make a
reasoned judgment about safety, thus adding to the toddlers’ risk of unintentional
injury (Cross, 2001; Hockenberry & Wilson, 2007).
Unintentional injury in toddlers is still a particular kind of injury and occurs
most commonly in and around home where they spent most of their time (Linnan
et al., 2007). Interestingly, most common types of unintentional home injury in

16
toddlers occur through a variety of injuries including drowning, falling, poisoning,
burning, puncturing with sharp objects, and animal biting (Garzon, Lee, & Homan,
2007; Morrongiello et al., 2004 a; Sitthi-amorn et al., 2006).
Drowning causes the highest death rate among toddlers both in Thailand
(reported during 2003 - 2004) and the United States (reported during 2005 - 2009). In
Thailand drowning causes nearly half (46 %) of all children’s death, and the mortality
rate was 40 per 100,000 children annually. The factors associated with drowning
were: lack of ability to swim, increasing mobility, lack of parental supervision, and
small bodies of water in or near home such as a bathtub, water bucket or open well
(Laosee, Gilchrist, & Rudd, 2012; Sitthi-amorn et al., 2006).
Falling, the next most common unintentional home injury, occurred when
toddlers injured themselves in accidents involving furniture, stairs, balconies, and
windows (Agran et al., 2003; Barker, Hockey, & Miles, 2004; Sitthi-amorn et al.,
2006). Toddlers who lived in urban areas experienced more high falls than those
living in rural areas. In addition, falling resulted in more moderate to severe injury,
such as open wounds, fracture, or intracranial injury, than in mortality (Barker et al.,
2004; Sitthi-amorn et al., 2006).
Poisoning mortality was found to occur less than all other types of
unintentional home injury among toddlers (Morrongiello et al., 2004 a; Sitthi-amorn
et al., 2006). Nonetheless, a report in Thailand found that during 2003 - 2004 the non-
fatal poisoning rate in toddlers was higher than found for children aged 5 - 9 and 10 -
14 (Sitthi-amorn et al., 2006). Examples of the most common causes of poisoning
injury were due to toddlers’ easy access to chemical substances and caretakers storing
hazardous household products such as dishwasher products, soaps, and detergents in
unsafe and reachable places to toddlers and children (Patel, Groom, Prasad, &
Kendrick, 2008; Sitthi-amorn et al., 2006).
Burn morbidity or burn hospitalization also contributes to a high rate of
unintentional home injury among toddlers’ (Čelko, Grivna, Dáňová, & Barss, 2009;
Sitthi-amorn et al., 2006). The majority of non-fatal burn cases occurring inside the
home were from scalding by hot water followed by scalding from other hot liquids
(soups or foods), mostly in the kitchen or bathroom (Čelko et al., 2009; Drago, 2005).
Examples of common causes of scald burn in children were children reaching out and

17
pulling down hot objects and the contents of hot objects splashing onto them, or
grabbing onto hot objects themselves (Drago, 2005).
Significantly, sharp object injury was remarkably more frequent than bumps,
bruises, crushes, burns, and poisons among toddlers in Canada (Morrongiello et al.,
2004 a) while in Thailand, it had the lowest morbidity rate in toddlers. Additionally,
the most common instruments causing injuries were knives following by broken glass,
plastics, and nails. In Thailand, a report during 2003 to 2004 found that animal biting
injuries were much more likely to cause mortality among toddlers than older children
and the occurrence of this accidental injury in toddlers was ranked as third leading
cause of non-fatal animal injury when compared to children up-to 17 years old age
group. Besides it was found that in-house dogs and cats as well as snakes, and insects
such as bees or wasps were the most common sources of non-fatal animal biting
injury. These injuries often occurred because the toddlers disturbed these animals in
or around home (Sitthi-amorm et al., 2006). Therefore, toddlers are prone to injuries
due to their development stage. Reducing toddlers’ risk factors requires an
understanding of causal factors related to unintentional home injury.
Children’s gender is related to unintentional home injury in toddlers
There have been many studies with different designs and populations which
have examined the effect of gender on unintentional home injury (Collins et al., 2013;
Damashek et al., 2005; Morrongiello et al., 2009). Investigators reported that boys’
experienced more injuries than girls to as much as one to three times greater (Bernard-
Bonnin et al., 2003; Morrongiello et al., 2004 a; Sorenson, 2011). Boys have a higher
unintentional injury rate from falls and burns (Shenassa, Stubbendick, & Brown,
2004), drowning (Laosee et al., 2012), poisoning (Kanchan, Menezes, & Monteiro,
2009), and animal bites (Sitthi-amorn et al., 2006) but lower injury from punctures
and cuts (Morrongiello et al., 2004 a). However, there appear to be several factors that
contribute to boys being at greater unintentional home injury.
Studies of boys’ unintentional injury risk behavior indicated that boys have
greater risk taking, and have more active, intense, and sensation seeking behavior than
girls (Morrongiello et al., 2008; Morrongiello et al., 2004 a). Morrongiello and
Dawber (1998) consistently found that boys approached more hazards than girls and

18
exhibited more risk behavior than girls after approaching hazards. Boys did more
touching-retrieving of burn, cut, and poison hazards than girls while girls did more
looking and pointing at these same hazards than boys. Granié (2010) indicated that the
behavior of boys created higher rates of injuries than that of girls due to the natural
condition that boys were born more masculine than girls and girls were born more
feminine than boys. Moreover, the masculinity of boys showed as a predictor of risk
behavior. Children’s risk behaviors were also positively related to their injury rate
(Damashek et al., 2005). Additionally, Morrongiello et al. (2004 a) found that boys
had more injuries than girls in playrooms or children’s bed rooms and fewer injuries
in non-play areas (i.e., kitchen, bathroom, or and lower than girls between lunch and
dinner. living room) wherein boys’ experienced of injury was higher than girls’
during dinnertime Boys’ injuries more affected the head and neck than did injuries to
girls. However, Morrongiello and Hogg (2004) suggested that characteristics of boys’
behavior would result in greater risk even in the presence of equal supervision.
Parental supervisory attributes are a factor. Morrongiello et al. (2009), in a
study of adult supervisory practices, suggested that parents provided less supervision
for boys than girls. Perhaps parents of boys perceived that boys were less compliant
and more difficult to manage than girls. However, when parents viewed their children
to be at high injury, their boys experienced fewer injuries (Morrongiello et al., 2004 a).
Morrongiello and Rennie (1998) found there was less vigilance and injury risk
monitoring for boys than girls in high risk situations. Also, there was a belief that
boys’ injuries were more associated with bad luck whereas girls’ injuries were more
associated with poor choices. Some parents supervised their boys with more emphasis
on discipline than safety whereas they supervised their girls with more emphasis on
safety than discipline. According to parents’ strategies, greater non-injury risk was
due to the strategy of discipline than the safety strategy. Parents also emphasized that
boys’ risk of injuries were entwined with bad luck more than girls’ and they did not
make any more environmental changes, rules or took any more punitive action for the
boys than they did for girls to prevent recurrent injury risk. However, they showed
more anger to boys than to girls when their children engaged in behavior placing them
at risk of injury (Morrongiello & Hogg, 2004). Furthermore, parents believed that
they are less able to control and protect boys from injury risk than girls even though

19
boys were more prone to injury risk (Morrongiello et al., 2004 a).
In conclusion, child gender has direct and indirect effects on unintentional
home injury. Boys have much higher rates of injury than girls for most unintentional
injury types except punctures and cuts. Also, boys have riskier behaviors and greater
risk of injury than girls. Both boys and girls experienced different injury types, at
different times of day, different places in the home, and bodily injury locations.
Besides, parents supervised their boys less than girls. And, believed that boys hardly
listened to their parents’ warnings, as well as, that boys’ injuries were more connected
with bad luck than girls injuries and that boys were expected to be more likely to be
injured than girls. Additionally, parents resorted to rules, discipline, and punishment
of their children to prevent injury and its recurrence. Reasonably, children’s gender,
specifically, male gender was a significant variable in prediction of unintentional
injury occurrence. Nonetheless, there were still other child characteristics involved
such as children’s temperament, which related with children’s injury.
Children’s temperament is related to unintentional home injury in
toddlers
Children’s temperament was defined as a relatively specific inborn
characteristic or behavior children that could not be easily altered. Children responded
differently in different situations or environments when they interacted with an
environment that motivated them (Goldsmith et al., 1987; Thomas & Chess, 1977). In
the classic early work of Thomas and Chess (1977) children’s temperament was
described as having three clinical categories: 1) the difficult temperament, which
referred to children who had an irregular rhythm, low approach and adaptability, and
high intense and negative moods; 2) the easy temperament which referred to children
who were regular rhythmic, positive approach and adaptability, mild intensity, and
positive in mood; and 3) the slow to warm-up temperament which referred to children
who were low in activity level, approachability, and adaptability, mild intensity,
negative mood, and variable rhythmicity.
There was empirical evidence illustrating that children’s temperament was
associated with unintentional injury in young children (Rowe & Maughan, 2009;
20
Schwebel, 2004). Difficult temperament had been conceptualized and measured in a
variety of ways but findings consistently show that more difficult characteristics, such
as being hard to manage (Dal Santo et al., 2004), having a high level of sensation
seeking and a high degree of behavioral intensity (Morrongiello et al., 2008),
delinquent and aggressive behavior (Ordoñana et al., 2008), having a higher activity
level, oppositional behavior, immaturity, emotional instability (Damashek et al.,
2005), having a higher level of risk taking and less inhibitory control (Morrongiello
et al., 2006 b) were each associated with greater injury. Furthermore, the effects of a
difficult temperament on injury also interacted with parental supervision.
Numerous investigators indicated that children who had difficult
temperaments (having high sensation seeking, risk taking behavior, intensity, high
activity level, and impulsivity) had parents who closely supervised them whereas
children who had high self-control had parents who provided less supervision
(Morrongiello et al., 2006 b; Morrongiello et al., 2008). Additionally, children’s
temperament interacted with parental supervision in its contribution to injury.
Morrongiello et al. (2008) pointed out that children who had high scores in behavioral
intensity were more exposed to injury when they were not supervised at a moderate or
high degree, than children with low scores. Consequently, children’s temperament is
an important child characteristic to measure and include in a predictive model for
unintentional injury. There have been many studies using questionnaire methods to
measures of child temperament. These measures include:
1. The Toddler Temperament Scale (TTS) by Fullard, McDevitt, and Carey
(1984), which measures all nine categories of temperament. This is a 97-item measure
designed for use among children 1-3 years old and has mothers rate their children in
comparison with other children. Analyses produced 5 categories had an acceptable
alpha coefficient of more than .70: activity, rhythmicity, distractibility, approach, and
persistence whereas adaptability, threshold, and intensity were below the .70
threshold.
2. The Toddler Behavior Assessment Questionnaire (TBAQ) by Goldsmith
(1996) was constructed to assess temperamental categories of activity level (e.g.,
“When playing on a movable toy, how often did your child attempt to go as fast as
he/she could?”), tendency to express pleasure (e.g., “When in the bathtub, how often

21
did your child babble or talk happily?”), social fearfulness (e.g., “When your child
was being approached by an unfamiliar adult while shopping or out-walking, how
often did your child show distress or cry?”), anger/ proneness (e.g., “When you did
not allow your child to do something for her/ himself, for example, dressing or getting
into the car seat, how often did your child try to push you away?”), and interest/
persistence (e.g., “How often did your child play alone with his/ her favorite toys for
30 minutes or longer?”). The internal consistency of each categories was higher than
.80.
3. The Early Childhood Behavior Questionnaire (ECBQ) by Putnam,
Garstein, and Rothbart (2006) was designed to assess emotion, motor, and sensory
system of toddler. It contained 18 categories and 201 items in 7-point Likert-scale
ranging from never to always. There were only 3 categories had internal consistency
lower than .70 (impulsitivity, α = .57, activity level α = .66, and inhibitory control
α = .62 respectively) when measure at children 18 months. However, internal
consistency of impulsitivity, activity level, and inhibitory control increased to .70, .71,
and .73 respectively at aged 36 months.
4. The Injury Behavior Checklist by Speltz et al. (1990), which measures
temperament through risky behavior of children 2 to 5 years old by parents report. It
contains 24 behaviors on a 5-point scale, such as “Jumps down stairs” and “Plays with
fire”. The IBC total scores showed good reliability with a Cronbach’s alpha of .87.
5. The Child Injury Risk Scale (CIRS) by Damashek et al. (2005) was
designed to measure child behavior characteristics such as aggression, high activity
level, behavior problem, and emotional reactivity. The CIRS showed high Cronbach’s
alpha reliability (α = .82).
To serve the purposes of this study, child temperament will be operationally
defined using the Injury Behavior Checklist (IBC) developed by Speltz et al. (1990).
This instrument was selected because it was designed as a measurement of children’s
temperamental characteristics as reflected through risky behaviors for the purpose of
understanding young children’s unintentional injuries. IBC had 24 items on a 5-point
Likert scale, ranging from 0 to 4 and total score range from 0 to 96. It is filled out by
parents to rate their children’s frequency of each behavior during the previous 6
months. The IBC had been shown to have good psychometric properties as

22
demonstrated by test-retest reliability, internal consistency reliability, and construct
validity. Particularly, this measure’s psychometrics have been evaluated with Thai
toddlers and used in relation to unintentional home injury. It has also demonstrated
good internal consistency (α = .94) (Sirisamutr, 2008).
To summarize, the in-born temperament of children is exhibited through
their behaviors or emotions/ feelings and is molded by the environment while they are
growing up. Each child expresses his/her response differently. Children’s
temperaments are classified into three categories: difficult temperament, easy
temperament, and slow to warm-up temperament. Children’s temperament is a risk
factor in children’s unintentional injury. The difficult temperament child experienced
injury more often than the easy temperament child. Parents supervise difficult
temperament children more than easy temperament children. In addition, the difficult
temperament children’s behaviors interacted with inadequate parental supervision and
further affected increasing injury. Undoubtedly, both temperament and parental
supervision are risk factors for unintentional home injury.
Home physical hazards are related to unintentional home injury in
toddlers
Descriptive data and cross sectional studies done in the United States and
Thailand describe the common risk factors as well as associations between home
characteristics and unintentional home injury. Physical hazards included poor quality
structures, dangerous and sharp objects, non-functioning equipment, accessible
poisonous cleaning or chemical products, as well as hard furniture at home that could
potentially be harmful and cause unintentional injury to children (Garzon, 2005;
Phelan et al., 2011; Sirisamutr, 2008). More than 60 % of unintentional injury
occurred in and around home (Atak et al., 2010). The most common places for
unintentional injuries in the home were children’s bedrooms, living rooms, kitchens,
bathrooms, and stairs (Morrongiello et al., 2004 a; Sirisamutr, 2008).
Physical hazards to toddlers that contributed to unintentional injuries in the
United States were found in very old homes or homes that needed repairs (Dal Santo
et al., 2004; Shenassa et al., 2004). They could also consist of chemical containers

23
without child-proof lids or caps (LeBlanc et al., 2006), non-gated stairways,
accessible sharp instruments, the absence of functioning smoke detectors, hot water
tap temperatures of over 49oC (Kendrick et al., 2005; Phelan et al., 2011), hard
flooring, and sharp corners on furniture or other structures in home (Simpson et al.,
2009). Some researchers specified home physical hazards directly related to the
likelihood of specific types of injury. For example, children in homes that: lacked
safety stair-gates, used a rolling baby walker, had open windows with low window
sills and no barriers, and with slippery polished floors as well, were particularly risky
for injury from falling (LeBlanc et al., 2006; Munro, van Niekerk, & Seedat, 2006);
non-functioning or lack of use of recommended safety equipment such as: absent
carbon monoxide or smoke alarms, uncovered electrical outlets and wires. Also, hot
substances lying on the floor or otherwise accessible hot liquids/ objects all around,
were the causes of burns (Drago, 2005; Munro et al., 2006). Sharp objects lying on
the floor (i.e. broken glass, needles, knives, tin cans, or nails), sharp corners, barbed
wire, and zinc plates on heaters presented potential puncture cutting or burning
injuries. Another safety concern was the storing of chemical substances in food
containers of any kind or having non child proof lids or caps on bottles, cans or any
type of packages of chemical products increased poisoning (Munro et al., 2006).
Kitchens provided specific hazards from the heat source used in cooking as well as
potential injuries from contact with hot objects or liquids with particular danger from
spills of hot liquids onto the child (Drago, 2005).
Studies of home physical hazards related to unintentional injury among
young children in Thailand found that children living in poorly maintained houses had
4.5 times higher risk of unintentional injuries than children in well-maintained homes
(OR = 4.5, 95 % CI = 2.76 - 7.34). Children who lived in houses with high numbers
of hazards both inside and outside their houses, had more than 48 times the risk of
injury than those living in households with lower numbers of hazards (OR = 48.19,
95 % CI = 20.23-144.80) (Sirisamutr, 2008). A study by Pooltawee (2000) found that
children who lived in town houses or had more than one room in the house
experienced injuries more than children who lived in detached or row/brick houses or
in one room (OR = 3.06, 95 % CI = 1.20 - 7.81; OR = 2.61, 95 % CI = 1.48 - 4.62
respectively). In addition, it was found that the physical condition of houses were also

24
risk factors for child injury around this age and they were as follows: houses with out-
of-order doors or non-equipped door barrel bolts, damaged balusters of balconies,
steep stairways with high risers and no handrails or with out-of-order handrails, and
unkempt home equipment and kitchenware or keeping of house pets (Tiempathom,
1994). Consequently, toddlers in a home with many kinds of these hazards tend to be
at increased risk of unintentional injuries (Alptekin et al., 2008). All in all, parents
were the key to home injury protection for toddlers.
An excess of home hazards, which exposed toddlers to unintentional injury,
may come from the inability of parents to identify the risk of injury, lack of
knowledge, and not following safety recommendations (LeBlanc et al., 2006; Munro
et al., 2006). Though parents spent much time with their children and knew every
corner of their homes, in a study by Gaines and Schwebel (2009) parents were able to
identify less than half of the hazards in each room of their house. Parents, who were
under-educated, unemployed, low-income, had toddler-aged children, had lived their
lives in their extended family, and were unable to assess the danger from hazards in
their homes had more child injuries than parents with higher education, were
employed, and had more financial resources (Atak et al., 2010). Conversely, parents
in homes with safety equipment such as smoke detectors, cupboard locks, or electrical
outlet covers were able to provide information about all potential home physical
hazards such as blocking accessibility to poisons, using fireguards and safe medicine
storage, and other methods to decrease home physical hazard risk (Clamp &
Kendrick, 1998; Johnston, Britt, D’Ambrosio, Mueller, & Rivara, 2000).
However, while the physical characteristics of the environment, such as
those described above, provided the exposure to objects that could cause injury, there
were other important factors that contributed to whether or not a particular child was
likely to be injured by a home physical hazard. These factors included characteristics
of the child and those of the parent. Gender effected both the location in the
household where the injury occurred and the type of injury. Studies, such as the one
by Morrongiello et al. (2004 a) pointed out that boys’ injuries occurred in the
playroom or children’s bedroom whereas girls’ injuries happened in the kitchen,
bathroom, or living room. Others documented that boys were also at greater risk than
girls for falling, being poisoned, or burned (Hjern, Ringbäck-Weitoft, & Andersson,

25
2001). Parents tended to leave boys alone in living/ family room while girls were
more likely to be unsupervised in the bedroom than any other rooms (Morrongiello
et al., 2006 a).
Numerous intervention studies had targeted reducing children injuries in the
home. Recent studies tested interventions to reduce home unintentional injury by
means of home modification, countering home physical hazards such as installation of
stair gates, cabinet locks, and smoke detectors and they found that reducing home
physical hazards could decrease the injuries (Phelan et al., 2011). Furthermore, one
study developed an intervention through a hospital emergency department, focusing
on caregivers who brought their 5 years old or younger children to the emergency
department for treatment from accidental injuries occurring in the home. The
intervention group received information from the ED staff on safety practices and
home safety devices such as cabinet and drawer latches, electric outlet covers, bath
water thermometer etc., while the usual care group did not. The authors concluded
that caregivers who received knowledge and safety devices have higher sustainable
safety behavior than caregivers who did not (Posner, Hawkins, Garcia-Espana, &
Durbin, 2004). Therefore, providing knowledge about home physical hazards and
ways of prevention can increase knowledge and safety behaviors to reduce injury.
Measures of home injuries and measures of physical hazards to young
children in homes are essential to studying the factors that influence unintentional
injury in toddlers. A variety of approaches have been taken to measurement. These
include observational surveys and questionnaires (Jordaan, Atkins, van Niekerk, &
Seedat, 2005; Phelan et al., 2009; Williams et al., 2003) and assessment surveys with
illustrations depicting risky situations (Tymchuk, Lang, Sewards, Lieberman, & Koo,
2003). Most of these measures relied on observation by a data collector rather than
participant self report or interview. In the next section the major measures will be
discussed and evaluated for their relevance and psychometric properties.
First, the Home Injury Survey by Phelan et al. (2009) was designed for
observation of the number and density of home hazards related to unintentional injury
among 163 households with US children aged 1-3. These injuries were from cutting/
piercing, having been struck, falling, poisoning, and being burned. This instrument
consists of 55 items describing things observed in the kitchen, main activity room,

26
child’s bathroom, child’s bedroom, and stairways. Inter-rater reliability reached a
mean of .81.
Second, the Thai-translated HOME inventory (Infant/ Toddler version) by
Williams et al. (2003). This measure was back-translated from The Infant/ Toddler
(IT) Home Observation for Measurement of the Environment (HOME) of Caldwell
and Bradley (1984 cited in Williams et al., 2003) in English version into Thai version.
The measure was used to study 36 low income mothers and their children aged 13 to
35 months in northeast Thailand. The translated scale, like the original, included 45
items and 6 subscales covering 1) emotional and verbal responsibility of mother,
2) avoidance of restriction and punishment, 3) organization of the environment,
4) provision of appropriate play material, 5) maternal involvement with the child, and
6) opportunity for variety in daily stimulation. The total alpha coefficient of the Thai
version was .81 but the subscales of “opportunity for variety in daily stimulation” and
“organization of environment” were .14 and -.15 respectively.
The third measure, is the Home Inventory of Dangers and Safety Precautions
- Illustrated Version (HIDSP-IV) by Tymchuk et al. (2003). This measure allowed
identification of home hazards and precautions one could take by using six colored
pictures of the kitchen, bedroom, bathroom, living room, stairway, and yard/ street.
It had 101 items in all six areas. For example, one question was set in a kitchen for a
hazard “Metal utensil in plugged in toaster” and for a precaution “Hook cord on wall
hook”. The measure was tested among 62 US parents with children aged less than 3.
Total internal consistency of home hazards and precautions demonstrated an alpha
coefficient of .89 and .87 respectively, but only .07 for the set of 12 items describing
danger of the stairway.
Lastly, in Thailand, Plitapolkarnpim (n.d.) developed the Home Observation
Checklist from natural environment observations in and around homes of Thai
children aged 0 to 14 years. This instrument was used with more than 300 households
in both urban and rural areas in Thailand. It consisted of 40 items covering
characteristics such as house structure and location, characteristics of stairway,
balcony, toilets/restrooms, and furniture, in and out of home water body, number and
location of electrical plug outlets, and chemical and poisonous substances etc. This
checklist has not been published. However, it was constructed by experienced experts
27
in child injury prevention and revised after it had been utilized in a survey of at least
50 Thai households.
This study will use the Home Injury Survey by Phelan et al. (2009) and the
Home Observation Checklist by Plitapolkarnpim (n.d.). These instruments assess
physical hazards related to home injury occurring among toddlers in the kitchen, main
activity room, children’s bathrooms, children’s bedrooms, and stairways. Most of the
population in this study lives in the capital of Thailand, the same population targeted
in the current study. Furthermore, this instrument was found to have good
psychometric properties when assessing test-retest reliability, replicability, and
external validity.
In summary, the common risk factors of home physical hazards associated
with unintentional injury in toddlers both in Thailand and the United States of
America were as the followings: dangerous areas around home, under-standard home
structures, and all the house-wares and substances (for examples, out-of-order
equipments, chemical substances, and dangerous and unsafe furniture). The parental
factors that effected children injury from home physical hazards were lack of
knowledge and inability to identify hazards, non-abiding by safety recommendations,
less supervision, and safety behavior while children gender was related to locations
and types of home injury.
Parental supervisory attributes are related to unintentional home
injury in toddlers
A dictionary definition of supervision states that it is “to direct and watch
over the work and performance of others” (Kleinedler & Spitz, Eds., 2005).
Morrongiello describes supervision related to child injury risk as:
“…behaviors that index attention (watching and listening) in interaction
with those that reflect a state of readiness to intervene (touching/ within arm’s each/
beyond arm’s reach), with both types of behaviors judged over time to index
continuity in attention and proximity (constant/ intermittent/ not at all)”
(Morrongiello, 2005).
In this definition, parental supervision consists of 3 behaviors: 1) attention

28
which referred to a parent’s interaction with their children through watching and
listening, 2) proximity which referred to a parent being within an arm’s reach of the
child or beyond reach of the child’s whereabouts and activities, and 3) continuity of
attention and proximity which referred to parent’s constant/ intermittent/ absent
supervision of their children (Morrongiello & Schell, 2009; Saluja et al., 2004;
Schwebel & Kendrick, 2009).
Consistent with the above definition, researchers indicate that parental
supervision is a risk factor for unintentional home injury in toddlers (Morrongiello
et al., 2008; Morrongiello et al., 2004 b; Nakahara & Ichikawa, 2010). According to
Morrongiello et al. (2006 b), mothers who closely supervised their child such as
frequently checking on them, had children with fewer medically attended injuries.
Inversely, mother who lacked or inadequately supervised their child had more injuries
to that child (Morrongiello et al., 2004 a). Consistent with Morrongiello and Hogg
(2004) studied the relation between mother’s supervision, children’s risk-taking
behavior and injury and found that parents who left their high risk-taking children
playing alone had children who experienced injuries. Inversely, parents who
constantly and closely supervised their high risk-taking children while they played,
experienced fewer injuries occurring to their children. However, recent research
showed that the parental supervisory attributes related to unintentional child home
injury were: parental protectiveness, supervision, tolerance of children’s risk taking,
and fate beliefs (Morrongiello & Corbett, 2006; Morrongiello & House, 2004).
Parental protectiveness has been described as the ability of parents, and their
specific behaviors, and attitudes that focus on keeping their children safe from injuries
(Morrongiello & Corbett, 2006). Parental protectiveness and its relationship with
unintentional injury was examined in a group of children aged 2-5. In this study,
parents’ reports showed that parents who possessed strong attributes of protectiveness
had children who experienced fewer injuries (Morrongiello & Corbett, 2006;
Morrongiello & House, 2004). Another study found that parents of non-injured
children had higher protectiveness than parents of injured children (Morrongiello
et al., 2009). Similarly, parents, who showed a tendency to protect their children from
unintentional injuries in their homes could save their children from dangerous
environments, and fewer had children who were exposes to injury (Garling & Garling,

29
1993; Morrongiello et al., 2004 a). For example, parents who applied a top guard on
their oven window can prevent burn injuries (Wortel, De Geus, & Kok, 1995).
Inversely, parents who did not provide adequate protection, has children with greater
risk of injury deaths; for example, in Alaska and Louisiana, it was found that parents
who left their young children home alone or did not inspect smoke alarms regularly,
were more likely to experience child deaths from drowning, pedestrian accidents, and
fire (Landen, Bauer, & Kohn, 2003). Therefore, parental protectiveness is an
important parental role in preventing unintentional child injuries at home.
Parental supervision has been defined as parental judgments about whether
or not they need to supervise their child more closely or to provide directed or
undirected supervision, or intermittent supervision of their children in each situation
(Morrongiello & Corbett, 2006; Morrongiello et al., 2004 a). Numerous studies found
that parents who had high scores for close supervision exposed their children to fewer
injuries (Morrongiello & Corbett, 2006; Morrongiello et al., 2004 a; Morrongiello et
al., 2008). Similarly, the results of other studies of parental beliefs related to time of
supervision found that mothers who could not constantly supervise their young
children at home, but frequently checked on their children, had children who
experienced fewer unintentional injuries requiring medical attention (Morrongiello
et al., 2006 b). In other work Morrongiello, studied the frequency of checking on
children in non-risk and risk situations in and around home environment. He found
that a group of parents believed that children needed more frequent checking-on in
risky environments (checking on every 9.30 minutes) than in non-risky environment
(checking on every 11.01 minutes). For example, a risky environment in-and-around
home was depicted as “the child is playing with toys on the floor of his/ her bedroom
and there is a medicine container with pills left open on the top of the dresser” A non-
risk environment was portrayed as “the child is playing with toys on the floor of his/
her bedroom” (without any hazardous setting existing) (Morrongiello et al., 2009).
Other findings indicated that parents provided closer supervision of their toddlers than
their older children (Morrongiello et al., 2009). Thus, parental supervision beliefs
were strongly associated with unintentional home injury to toddlers.
Parental tolerances for children’s risk taking was described as parents
encouraging or letting their children approach new environments or enjoy doing

30
something they were not supposed to do (Morrongiello & Corbett, 2006). Research on
the relationship between parental tolerance of child risk-taking and unintentional
injuries among children found that parents who permitted their child to freely
experiment with and explore their environment instead of focusing on their children’s
misbehavior and imposing discipline on them, had children who were exposed to
more injuries (Morrongiello & Hogg, 2004; Schwebel et al., 2004). Similarly, a study
in simulated hazardous settings (e.g., the settings displayed an unplugged coffee pot,
shaving razor without blade, cleaner substance bottles filled with water, and pill
bottles contained small candies) found that injured children possessed riskier
behaviors (e.g., disruptive behavior, contact with hazards, inappropriate behaviors)
than uninjured children and parents of injured children allowed their children play by
themselves more than parents of uninjured children (Cataldo et al., 1992).
Additionally, reasons given by parents who tolerated their child’s risk-taking which
resulted in unintentional injuries were to gain the benefits from minor child injuries
that would teach their child about risky behavior (Lewis, DiLillo, & Peterson, 2004).
Some parents did not implement proactive hazards removal precautions to prevent
their children’s injuries even though their children (especially boys) possessed risk
taking behaviors, approached hazards and had had injury experiences (Morrongiello
& Dawber, 1998). Parental tolerance to children’s risk taking behaviors is mainly
related to toddlers’ unintentional injury at home.
Parental fate beliefs were defined as parents who believed that the injury
status of their children was predominantly determined by luck or fate (Morrongiello
& House, 2004). Parental fate beliefs were extended from the Parent Health Locus of
Control (PHLOC), which measured the perception that parents could or could not
influence the status of their children’s health and injury. According to these
perceptions, parents who believed their children’s health and injury status was
predominantly driven by luck or fate, had children who experiences more injuries
than parents who believed that they could control their children’s health and injury
status (Morrongiello & House, 2004; Morrongiello et al., 2004 a). In addition, the
influence of parental fate beliefs on unintentional injury risk among young children
was confirmed through testing the psychometric properties of the Parent Supervision
Attributes Profile Questionnaire (PSAPQ) and demonstrating that parental fate beliefs

31
had an effect on child injury risk (Morrongiello & Corbett, 2006).
The instruments that can be used to explore the relationship between the
parental supervisory patterns and unintentional home injury among young children
include: 1) the Parent Protection Scale (PPS) by Thomasgard, Shonkoff, Metz, and
Edelbrock (1995) which measures parenting behaviors intended to protect their
children (aged 2 - 10) regarding supervision, separation problems, dependency, and
control 2) The Beliefs About Supervision Questionnaire by Morrongiello and Hogg
(2004) which measures parental beliefs about non-supervision and indirect
supervision in different domains for toddlers and 3) the Parent Supervision Attributes
Profile Questionnaire (PSAPQ) by Morrongiello and Corbett (2006) which measures
parental behaviors, beliefs, and attitudes that were associated with risk of injuries
among children aged 2 - 5. This instrument consists of 4 subscales, which include
parental protectiveness, parental supervision beliefs, parental tolerance of risk-taking
children, and parental fate beliefs.
Morrongiello and Corbett (2006) constructed this instrument for measuring
parental supervisory attributes related to unintentional home injury and while it is a
relatively new measure, reliability and validity information was available from early
studies. A recent study by the authors’ reported data from the Parent Supervision
Attributes Profile Questionnaire (PSAPQ) on parental behaviors, beliefs, and attitudes
that were associated with injuries among children aged 2-5 and showed good
psychometric properties. One month test-retest reliability was acceptably good for all
subscales and has a range from r = .72 (p < .001) to r = .80 (p < .001) with good
internal consistency which ranges from α = .77 to α = .79. The PSAPQ had good
constructive validity as well as high convergent and discriminatory validity for each
of the four subscales. It was a unique scale and the author’s showed that the
intercorrelation between parental protectiveness and parental supervision was strong
and positive (r = .62, p < .001) and it was negatively related to parental tolerance of
risk-taking in children (r = -.37, p < .001). Parental supervision was negatively
correlated with both tolerance of risk-taking children (r = -.55, p < .001) and fate
beliefs (r = -.21, p < .05). Hence, these subscales showed strong psychometric
properties and were able to predict unintentional injury.
To sum up, parental supervision consists of attention (watching and

32
listening), proximity (within versus beyond), and continuity of attention and
proximity (constant/ intermittent/ not at all). Parental supervision is long-standing in
that adequate parental supervision serves a protective role and prevents injuries from
occurring in and around home. It was also found that the parental supervisory
attributes related to unintentional children home injury were protectiveness,
supervision, tolerance of children risk-taking, and fate belief. Therefore, all these
supporting findings highlight the challenge of exploring which parenting attributes
can identify children at risk for unintentional home injury.
Concepts and models are related to unintentional home injury in
toddlers
The next section reviews the concepts pertaining to children’s unintentional
home injury based on existing models, included Gordon (1949), Garzon (2005),
Morrongiello (2005), Schwebel and Barton (2005), Koulouglioti et al. (2009), and the
Parental Monitoring Model of Dishion and McMahon (1998). They were reviewed,
integrated, and a model developed to be this study’s conceptual framework.
In 1949, Gordon proposed the concept of injury epidemiology which related
to injury based on an understanding of basic causes of disease that included three
fundamental interacting factors: the host, agent, and environment. The host was the
person who got hurt especially young children, males, and children of color. Agents
were various kinds of physical, chemical, biological and mechanical vectors that
cause injuries such as scalding or unguarded poison. Each agent produces a different
kind or type of injury; for example, a glass-paneled door is an agent for a cutting
injury or a faulty ladder is an agent of fall injury. Environment could be described as
including both animate and inanimate things around a person that may cause personal
injury including physical, biological, and socioeconomic one. The physical
environment affecting on injury includes differences in geography, climate, and
seasons, such as home, cold temperature, and summer. The biological environment,
described as animate, were pets, snakes, or insects that live around a person and
leading to injury. The socio-economic environment referred to any causes of injury
such as the quality of housing, amount of income, and occupation. However, Peterson

33
et al. (1987) extended epidemiology of causes to include psychological causes of
injury by using process analysis of the injury situation. They focused on linkage
between the physical environment and the behavior of children and their caretaker.
For example, if a child falls from a bicycle riding, the physical environment may
come from the road condition or traffic, the behavior of children may be that of
excitement, and the behavior of caretaker may be that of lack of parental supervision.
Consistent with Valsiner and Lightfoot (1987), they used the psychological theory
perspective for conceptualizing and undertaking a study of unintentional injuries in
childhood using the socio-ecological approach. This concept viewed the relationship
between a child’s action and the environmental setting under conditions of caregiver.
Garzon (2005) proposed a model explaining interactions among contributing
factors to preschooler unintentional injury (PUI) as including a) risk factors (the child,
environment, and agent), b) mediating factors (parent’s recognition and modification
of the child, environmental, agent factors and parent supervision) and c) outcome. The
contributing factors to preschool unintentional injury model are illustrated in Figure 2.
Figure 2 The contributing factors to preschool unintentional injury model
(Garzon, 2005, p. 442)
Risk factors Outcomes Mediating factors
Child factors
Environmental
factors
Agents factors
Adult
recognition and
modification of
child, agent and
environmental
factors
Adult
supervision
Preschool
unintentional
injury
No preschool
unintentional
injury

34
1. Risk factors: The three categories of risk factors contributing to PUI risk
and their interaction with one another and mediating factors are as follow:
1.1 The child: These include developmental, physical, and behavioral
characteristics (e.g., impulsiveness). A natural development in preschoolers is
curiosity and exploration that drives them to explore new environments and
potentially hazardous objects; consequently, it increases injury risk. Besides, normal
physical growth of preschoolers includes a large and heavy head, which increases the
risk of falls, head injury, and drowning from being top-heavy. Preschoolers also have
frequent impulsive thoughts and limited cognitive abilities. They like to climb onto
stacked objects and get them. Unfortunately, they could not comprehend their weight
and forces of gravity. In addition, many parents misunderstand children’s normal
development, physical ability, and behavior. Hence, not only does child development
interact constantly with environment, but these predispositing factors also lead to the
PUI.
1.2 Environment: Environmental characteristics contributing to the injury
rate include neighborhood (e.g., traffic volume, safe or unsafe play area, and access to
emergency care); home physical hazards (e.g., unguarded staircases, poorly lit
hallway, crowding, lead contamination, and absence of working fire prevention
equipment); and social environment (e.g., caregiver’s work or hobbies, parental
supervision practice, and caregiver’s parental skill). For example, some parents do not
realize the danger of poison injuries when their child swallows cosmetics, cough and
cold medicines, cleaning substances, plants, and personal-care products.
1.3 Agent: The agents of risk include any environmental, physical, or
thermal force that potentially makes specific tissue damage or injury such as
automobile’s speed, toy’s sharp edges, velocity of bullet, heat of fire, and gravity. For
example, many parents do not realize that safeguards for stairs or window screens can
prevent preschoolers from serious falls. At the same time, the preschoolers themselves
do not know that such preventive equipment cannot support their weight.
2. Mediating factors: These factors include a parent’s recognition of risks
and modifications of any child, environmental, or agent factors. The concepts
included are based on the Health Belief Model. Garzon believed that parents, who
perceived the high risk of injury, severity of injury, benefits of protective behavior,

35
and less barriers of change behavior, recognized and modified the risk factors of
injury. Preschoolers had to rely on parental recognition and modification of the
children’s environment including the injury agents in order to prevent children from
exposing themselves to the risk factors of injury. Moreover, parental supervision was
a mediating factor that interacted with parental recognition and modification related to
injury. Parents who paid closer supervision to their children in areas perceived as a
risky environment such the kitchen, were able to prevent the injury better than those
who did not.
3. Outcome: There are two main outcomes after parents’ supervision. Either
that a PUI occurs or one does not occur.
The child’s development interacts with the environment and agents
continuously. And, if any risk factor out of these three exists, parents can recognize
and modify the risk to prevent PUI by using supervision. However, being effective in
preventing any PUI depends on the parents’ ability to recognize risk factors and be
able to modify them into a safer situation, which determines an outcome.
Morrongiello (2005) provided a conceptual model that focused on children,
caregivers, and environmental factors (e.g., noise, hazards, chaos) which interacted
jointly within the socio-cultural context (e.g., norms about safety, economic status,
ethnicity) as a system which influenced child injury risk in the natural environment.
This system was a complex process that focused on the interaction of a person and an
environment in the real world and could not separate each factor that can contribute to
child injury. The child and caregiver factors that contribute to child injury consisted
of: attitude (e.g., towards safety gear), behaviors (e.g., risk taking), cognitions (e.g.,
vulnerability for injury), distractibility, expectations for self and others (e.g.,
expectations regarding behavior, injuries, etc), feeling (e.g., excited, fearful,
depressive state), goal (immediate, long term), hazard awareness (perception of risk),
and individual’s traits (personality, temperament). The conceptual model with its
interactions between child, caregiver, environmental factors and the sociocultural
contexts that influence child injury risk is illustrated in Figure 3.

36
Figure 3 The conceptual model interactions between child, caregiver, and
environmental factors and sociocultural context influence child-injury risk
(Morrongiello, 2005, p. 547)
This conceptual model describes interaction among child factors, caregiver
factor, and environmental factors, which were shaped, directed, and constrained by
the sociocultural context, and jointly and continuously effect child injury. The
researcher also indicated that caregiver supervision serves as a protective function to
reduce injury and the pattern of supervision that they provided varies depending on
environmental hazards, social context, child attributes, and child development.
Schwebel and Barton (2005) proposed two models that related to child
unintentional injury. Model I illustrated the combination of three risk factors that
included child temperament, child’s estimation of environment risk, and parenting.
They had a direct and indirect effect to child injury. The researchers described direct
effect on child injury that was the child temperament, parenting, and child’s
estimation of environment risk. For child temperament, children who had aggressive,
overactive, oppositional, impulsive, and uncontrolled behavior predicted an increased
injury. On parenting, a parent providing close supervision reduced child risk-taking.
Lastly, child’s estimation of environmental risk, children who overestimated their
ability had an increased risk of injury. In addition, child’s estimation of the
environmental risk could be a mediator in the relationship between temperament and
CHILD-INJURY RISK
Child-based variables Caregiver-based variables
Environment-based variables
(e.g., noise, hazards, chaos)
Sociocultural-based context
(e.g., norms about safety)

37
child injury, and between parenting and child injury. The temperamentally impulsive
and under-controlled children could not judge appropriately what about their
environment could lead to injury. Moreover, parents support the risk-taking behavior
of boys more than girls; therefore, boys have more injuries than girls. The researchers
also proposed an interaction between temperament and parenting as moderating the
effect between temperament and injury. Their reviewed literature supported the idea
that parents who had difficult temperament children provided more supervision, and
their children had less injury than children without difficult temperament. Lastly,
there is an interaction between temperament and parenting that had an indirect effect
on child injury through child estimation of environment risk. The difficult
temperament children were encouraged to be cautious in their judgments of
environment and they were prevented from injury by parents’ close supervision. The
hypothesized mediated moderation model whereby temperament, parenting, and
ability overestimation predicts children’s unintentional injury risk is illustrated in
Figure 4.
Figure 4 The hypothesized mediated moderation model whereby temperament,
parenting, and ability overestimation predicted children’s unintentional
injury risk (Schwebel & Barton, 2005, p. 554)
Model II proposed the direct, mediating, moderating, and mediated
moderation effect among child gender, child’s attributions of injury, and parenting
Child
temperament
Child temperament
x parenting
Child estimation of
environmental risk
Parenting
Child injury
risk

38
behavior on unintentional injury (UI). There were three direct effects on UI: 1) boys
had more injury than girls (children gender); 2) parental proximity to the children was
related with decrease children risk-taking (parenting behavior); and 3) children who
attribute their injury to bad luck, they were more engaged to risky behavior
(children’s attributions of injury). Furthermore, two mediating effect were proposed.
First, child’s attribution was a mediator between child gender and injury. Boys
attributed their injury to bad luck while girls attributed injury to their own behavior.
The researchers believed this caused boys to be more prone to injury. Second, child’s
attribution was a mediator between parenting and injury. The child attributed injury to
bad luck from their parent attribution, beliefs, and thoughts. The moderating effect
was gender which interacted with parenting to influence injury. Parents of boys
encouraged them to be in risky environments whereas parents of girls cautioned and
closely supervision them in risky environments. The researchers also proposed a
mediated moderation effect that was gender by parenting (moderator) which
influences injury through the child’s attribution (mediator). Parents selected
appropriate instruction for their child’s gender about risky situations including
socialization and child attributed to risk from a situation from socialization. The
hypothesized mediated moderation model whereby gender, parenting, and attributions
of injury predicted children’s unintentional injury risk is illustrated in Figure 5.

39
Figure 5 The hypothesized mediated moderation model whereby gender, parenting,
And attribution of injury predicted children’s unintentional injury risk
(Schwebel & Barton, 2005, p. 557)
Models I and II showed relationship between child factor and parental
factors. A child’s decision making about estimation of environmental risk or a child’s
attribution of injury are direct effects and mediating factors to injury. The children can
make judgments about their surroundings and what the risky or safe environment look
slike does but they depended on the parenting style of their parent that shaped them
through socialization.
Koulouglioti et al. (2009) illustrated a causal model from a study of risk
factors that contribute to unintentional injury among toddlers. The predictors were
maternal supervision, maternal fatigue, children’s temperament, children’s routine,
and children’s sleep. The outcome was children’s unintentional injuries. The sample
was 264 mothers who completed 6 questionnaires during 2002-2004. Maternal
supervision refered to the number of minutes that mother did not supervise their child
in each od 4 environments including: 1) bedroom/ living room at home 2) bathroom,
garage, and kitchen at home 3) sidewalk by home and 4) driveway in front of the
home. Maternal fatigue refered to a parent’s perceived symptoms of fatigue.
Children’s temperament refered to children’ behaviors of their activity level, intensity,
pleasure, impulsivity, and inhibitory control. Children’s routines refered to the daily
living routine activities. Children’s sleep refered to the mother’s perception of the
Child gender
Child gender
x parenting
Child attribution
of injury
Parenting
Child injury
risk

40
amount their children usually sleep. Children’s injuries refered to the total number of
unintentional injuries that had required medical treatment. The results supported a
causal model where maternal fatigue was negatively associated with children’s
routine and positively associated with maternal lack of supervision. In addition,
maternal lack of supervision was positively correlated with injury. Children’ routines
were a moderator between maternal supervision and injury. The result also showed
that an increase in the number of maternal unsupervised minutes was correlated with
an increase injury in the low routines score. Moreover, children’s lack of sleep was a
predictor of injuries and was a mediator between children’s routines and injuries.
The this study’s results showed that maternal fatigue had an effect on
maternal supervision and child routine. Mother did not provide supervision and could
not supervise their children’s frequent and regular activities if they were fatigued.
Moreover, mothers who did not have adequate time to supervise their children, had
children who were unable to do everyday activities. As a result, the children were
injured. The causal model of direct, indirect, and moderating effects on the number of
injuries in preschoolers is illustrated in Figure 6.
Figure 6 The causal model of direct, indirect, and moderating effect on injuries in
preschoolers (Koulouglioti et al., 2009, p. 524)
In conclusion, all models of unintentional injury to young children
illustrated the interaction between person and environment rather than describing
isolated events. Children’s characteristics (such as gender, temperament,and ability to
estimate injuries) interacted with parental supervision attributes (time of supervision,
b = 0.11*
Maternal
fatigue
Supervision
Child’s Routines
Child’s Sleep
Injuries
b = -0.003*
b = -0.046**
b = -0.174*

41
characteristic of parents, and safety behavior) and environmental hazards in and
around the home. However, all of these models can not be utilized in order to assess
the specific style of the parental supervision provided for toddlers. In this study, the
safety of toddlers has to depend on their parent’s supervision strategies. The Parental
Monitoring Model was a process model of parent-child interaction that pertains to
safety and injury (Dishion & McMahon, 1998)
The Parental Monitoring Model provides the partial frame for the study’s
conceptual framework. The Parental Monitoring Model focuses on both parental
tracking of children’s behavior and structuring the children’s environment, both of
which were based on the age of children. Parental monitoring was a part of the
relationship quality for a parent-child dyad. A positive parent-child relationship
enhanced the parent’s motivation to monitor their child and was used for management
purposes. The Parental Monitoring Model also describes the relationship between
parenting behavior, children’s activities, and adaptation. In general, the majority of
parents monitor young children in the home setting. Parental monitoring involved
supervision of children’s development. In the beginning, parents fulfilled all of the
infant’s basic physical and emotional needs. Then, when infants developed into
toddlers, they increased their mobility, curiosity, and interacted with the surrounding
environment up to the limit that parents allowed. Parents had to increase their
supervision of their toddlers’ activities and whereabouts to prevent home injury.
There were three areas of parental monitoring related to children’s behavior, which
were injury and safety, antisocial behavior, and substance abuse. However, in the area
of injury and safety, parental monitoring served as a protective factor for children who
live in high-risk settings that could easily led to injury (Dishion & McMahon, 1998).
Several investigators indicated that increased parental monitoring decreased
children’s injury risk (Garling & Garling, 1993; Harrell & Reid, 1990; Peterson,
Ewigman, & Kivlahan, 1993).
Another important study describes parental supervisory attributes, which
include parental protectiveness, supervision, tolerance for child’s risk taking, and fate
belief, which relate to unintentional home injury to toddlers. These conceptual
approaches of parents’ supervisory behaviors, attitudes, and beliefs were examined in
relation to naturalistic observations of parental supervisory attributes and children’s

42
injury history (Morrongiello & Corbett, 2006). The investigators pointed out that the
four parental supervisory attributes were significantly related to children’s injury
history and were inter-correlated. Parental protectiveness had a positive correlation
with risk of child injury as well as supervision beliefs. Inversely, parents who
believed in fate as well as those who tolerated children’s risk taking behavior had
children who were involved in injury risk. The meaningfulness of protectiveness,
supervision, tolerance for child’s risk taking, and fate beliefs reflected on parental
tracking and structuring of their children’s behavior in varied environments. For
example, “I am a very protective mother of my child” (protectiveness), “I make sure
that I know my child whereabouts and what he/she is doing” (supervision belief),
“I encourage my child to try on new things” (risk tolerance), and “When my child gets
injured it is due to bad luck” (fate beliefs). These parental supervision attributes may
have direct and indirect effects on unintentional home injury to toddlers.
The previous models have come from literature reviews of injury among
young children from epidemiology, behavioral sciences, and psychosociology.
However, Garzon’s model considers not only the child, environment, and parental
factors but also agent factors related to unintentional injury. It is difficult for parents
to modify the agent factors. Modifying the agent requires product redesign from
producer of the product or policy changes limiting what producers can make.
Morrongiello’s model is not clear which variable in each factor is the most influential
to toddlers’ risk of injury. The fact is that not all environments and behaviors of
toddlers and caregivers can be modified to prevent injury. Researchers need to
consider which variables (children, parents, and environments) have direct and
indirect impacts on unintentional home injury risk for toddlers. In addition, Schwebel
and Barton’s model is more appropriate for older children who can make judgments
about their surroundings than for younger children. Since this research investigates
unintentional home injury in toddlers, who lack decision-making skills to make the
right judgment regarding a risky or safe environment. They depend on their parent’s
supervision and perception about the injury risk. Finally, in Koulouglioti, Cole, and
Kitzman’s model, mothers were asked only about the amount of time without
supervision that they think is safe for their children. This has some limitation because
in reality child injury can occur at anytime. In fact, multiple studies showed that

43
parental supervision attributes such as fate beliefs, protectiveness, tolerance of
children’s risk taking behavior, and positive parenting were related to unintentional
injuries in toddlers (Morrongiello & Corbett, 2006; Schwebel et al., 2004). Therefore,
this model can not be used to assess the style of parental supervisory attributes in
parents of toddlers.
Consequently, a conceptual model has been developed for this study that
was constructed by selecting seven significant concepts shown in prior work to
contribute to toddlers’ unintentional home injury risk. These include: 1) child gender
(boy) 2) child temperament 3) home physical hazard 4) parental protectiveness 5)
parental supervision 6) parental tolerance for child’s risk taking and 7) parental fate
beliefs. This conceptual model and the relationships between these concepts were
presented by the hypothesized causal model of unintentional home injury in toddlers
(page 10).

CHAPTER 3
RESEARCH METHODOLOGY
The aim of this study was to test a causal model of unintentional home
injury in toddlers. This chapter presents the research methodology including the
research design, population and sample, setting of the study, research instruments,
protection of human rights, data collection, and data analyses.
Research design
A descriptive model-testing, cross-sectional design was used in the study.
Population and sample
The target population was mothers of 12-36 month old children currently
residing in Ratchathewee district, Bangkok Metropolitan. There were a total of 1,664
mothers with an eligible child living in these communities (Ratchathewee Institute,
2011). The target sample of 250 mothers of 12 - 36 month old children residing in this
district were drawn from the target population using a multi-stage stratified random
sampling technique. Inclusion criteria were as follows:
Child
1. Healthy in general, no congenital anomalies or genetic disorders, and
2. Currently residing in Ratchathewee district, Bangkok Metropolitan
Mother
1. Aged 18 years old or older and currently residing in Ratchathewee
district, Bangkok Metropolitan, for at least 6 months,
2. Being the primary caretaker and continuously rearing her child for at
least the most recent 6 months, and
3. Being able to read and write in Thai, and willing to participate in the
study
Sample size
Structural Equation Modeling, the most complex analyses used in this study,
often requires sample sizes that are between 250 and 500 subjects to maintain power

45
and obtain stable parameter estimates and standard errors (Schumacker & Lomax,
2010). Therefore, this study was conducted with 250 subjects for the minimum
number using the Structural Equation Modeling.
Setting of the study
Ratchathewee district is one of the 50 administrative districts governed by
Bangkok Metropolitan. It is located in the inner group of districts in the city of
Bangkok and is a highly populated area packed with housing and government offices.
The general profile of the district is commercial and direct services area.
The Community Development and Social Welfare of Ratchathewee
(Ratchathewee Institute, 2011) surveyed the national demographics of the
Ratchathewee district in 2011 and found that it had a population of 22,243, consisting
of 4,694 households, and 5,752 families, and covered an area of 7.73 square
kilometers with a population density of 10,230.14 per square kilometer. Ratchathewee
district is divided into four zones, which are grouped into 25 communities according
to the geographical area. Each zone consists of one to fourteen communities. The
communities are classified into three types according to population density and the
condition of dwellings (i.e. congested one-story wooden houses as type one, two-story
wooden or half solid structure, half wooden houses with fences around them as type
two, and apartments as type three). Each community sampled for this study belonged
to type one or two.
Most of the population is Buddhist or Muslim and works as laborers earning
daily or monthly incomes. Some make a living by trading, with their families either
working at home or outside their homes. Generally, their incomes are not sufficient
and families have no savings. The highest education level completed for most parents
in the communities was grade-six or grade nine (Prathomsuksa six or Mathayomsuksa
three). Residences in the poor areas are typically either small one-story wooden
houses with one to two rooms or families rent single rooms. The buildings are
structurally weak, sitting side by side and have no fences. Walkways are narrow
cement-pathways bordered by ditches with wooden-walking bridges laid over open
drain channels at some locations or small-width concrete passages on concrete
retaining walls alongside canals. Some communities are very crowded, poorly

46
arranged and inaccessible by vehicles. Some have sport playgrounds. In higher
income areas, the residences are structurally stable, one-story or two-story
wooden or half brick, half wood houses with surrounding fences.
There are a total of 1,664 children aged 1-3 years old living in these
communities. Most of the children are cared for by unemployed parents or
grandparents. At two and a half to six years of age, their parents enroll them in a
preschool development center. Four of these centers are located nearby in one of the
previously described communities in Ratchathewee. These centers have children’s
services and volunteer workforces to supervise the children. Accordingly, the
Ratchathewee resident group is considered to affirmatively represent the population
group that is exposed to unintentional home injury in toddlers.
Sampling
A multi-stage stratified random sampling technique was carried out to
achieve a sample of 250 subjects in the Ratchathewee district of Bangkok
Metropolitan. Ratchathewee district is divided into 4 zones: A) Thung Phaya Thai
consists (14 communities), B) Thanon Phaya Thai (1 community), C) Thanon
Phetchaburi (4 communities), and D) Makkasan (6 communities) (Ratchathewee
Institute, 2011). Procedures for sampling were as follows:
Stage 1: To obtain a homogenous sample in this study, 6 communities in
zone-A were excluded from sampling since there were police and army housing in
these communities which have higher education and income than is characteristic of
the rest of this zone and other zones. This left 8 communities remaining in zone A.
Stage 2: The number of communities to be randomly sampled from each
zone was determined by using a ratio of 1:2, and that was proportional to the number
of communities in that zone. Each community of each zone was given a number on a
piece of paper, all numbers from a zone were placed in a bowl, they were mixed well,
and then a designated person picked one number out of the bowl to obtain a sample.
Each number must be replaced before the next number is picked. In Zone - A each
community was given a number from 1 - 8 and then a random sample of 4 out of the
8 were selected, zone - B included only 1 community and that was selected, zone - C
had 4 communities and 2 were selected, and zone - D consisted of 6 communities and
3 of these were selected. This yielded 4, 1, 2 and 3 communities from Zones A to D

47
for a total of 10 communities. The community was the unit of analysis at this stage.
Stage 3: With a total desired sample of 250, each of 10 communities was
targeted to provide 25 participants. Zone A with 4 communities provided 4 times 25
or 100 participants, using the same process, zone B, C and D provided participants
numbering 25, 50, and 75, respectively. Convenience sampling was used to recruit the
sample at this stage, applying the inclusion criteria. If any family had more than one
toddler, names of the children were randomly selected by writing each name on a
piece of paper, placing in the container, shaking well, and then, drawing one name out
of container to identify the target child. Details of this sampling process are shown in
Figure 7.
Figure 7 The multi-stage stratified random sampling method used in this study
Family/
Participant
Community
Zone
Ratchathewee district
(4 zones)
Thung Phaya Thai Zone-A
(8 communities)
4
communities 2
communities 3
communities
1
community
100
families 25
families 50
families 75
families
Thanon Phaya Thai Zone-B
(1 community)
Thanon Phetchaburi Zone-C
(4 communities)
Makkasan
Zone-D
(6 communities)

48
Research instruments
Eight questionnaires were completed by the child’s mother or by a data
collector based on an interview of the target child’s and by the data collector’s home
observation. These included:
1. A Demographic Questionnaire developed by the researcher. This
questionnaire was to collect information about children’s age, gender, birth date, birth
order, and the number of children under 15 years of age who were in the same
household. Mother’s characteristics included age, marital status, education,
occupation, and family income. The researcher interviewed the mother and filled out
the information on the questionnaire.
2. The Child’s Temperament for Injury Risk was measured by the Injury
Behavior Checklist (IBC). This measure was derived from a questionnaire assessing
unintentional injury risk behaviors by Speltz et al. (1990). The initial items included
in the IBC were derived from histories of children who had injuries treated at an
emergency department and a review of injuries among young children. The IBC’s
psychometric properties were tested by Speltz et al. (1990). The IBC consists of 24
items, which relate to child temperament and risky behavior of children aged 2 - 5
years. Parents rate their child on each behavior situation based on the past 6 months.
Cronbach’s alpha and a one-month test-retest reliability coefficient for the scale,
tested with a sample of 253 middle-class U.S. families with children aged 2 to 5 years,
were .87 and .81 respectively (Speltz et al., 1990). In addition, high internal
consistency reliability (Cronbach’s alpha of .94) has been reported with a sample of
414 Thai preschool children (Sirisamutr, 2008).
A total of 23 items were used in this study. One item of the IBC was not
used because it pertained to risky behavior in a car which was not relevant for this
population. Each item of the IBC requests a selection from among 5 choices ranging
from 1 (not at all) to 5 (very often). The total sum of the scores ranged from 23 to
115, with a high score indicating a high level of risk taking behavior or a difficult
temperament child and a low score indicating a low level of risk taking behavior or an
easy or slow to warm up temperament child.
3. The Home Physical Hazard Checklist was measured by adaptation of the
Home Injury Survey and the Home Observation Checklist. The Home Injury Survey

49
was created from an observational survey of home injury hazards by Phelan et al.
(2009). It was used to assess the number and density of injury hazards observed by a
researcher in the homes of toddlers in the United States, particularly in the kitchen,
the main activity room, children’s bedrooms, bathrooms, and stairways. The Home
Injury Survey consists of 52 items and covers five types of unintentional injuries
which include cutting/ piercing, being struck/ striking, falling, poisoning, and burns.
The inter-rater reliability among seven research assistants using The Home Injury
Survey to score 100 randomly assigned rooms was .81 (Phelan et al., 2009).
The Home Observation Checklist was developed from an environmental
assessment in and around the homes of Thai children aged 0 to 14 years by
Plitapolkarnpim (n.d.). This instrument was used with more than 300 households in
both urban and rural areas in Thailand. It consists of 40 items covering characteristics
such as house structure and location, characteristics of stairways, balconies, toilets/
restrooms, and furniture, areas with water in and outside of the home, the number and
location of electrical outlets, as well as chemical and poisonous substances etc. This
checklist has not been published. However, it was constructed by experienced experts
in child injury prevention and revised after it had been utilized in a survey of at least
50 Thai households.
The Home Injury Survey (Phelan et al., 2009) was adapted by deleting four
items regarding smoke and carbon monoxide detectors which are not normally
installed in Thai homes. Moreover, three items about near drowning (such as water
well/ ditch or ponds near home or sink, and water containers in the home) of the
Home Observation Checklist (Plitapolkarnpim, n.d.) were added to be more relevant
to the Thai home context. Finally, the assessment used in this study consisted of 2
parts. In Part I, the observer assessed the general characteristics of home on 10 items.
For Part II, the observer assessed a series of 51 home physical hazards using a yes/ no
format. The total sum of the scores on Part II, ranged from 0 to 51, with high scores
indicated a high risk for child injury, and low scores indicated a low risk.
4. Parental Protectiveness was measured by the Parental Protectiveness
subscale of the Parental Supervision Attributes Profile Questionnaire (PSAPQ). This
subscale was derived from a questionnaire measuring parental supervision attributes
relevant to children’s risk of unintentional injury by Morrongiello and House (2004)
50
and Morrongiello and Corbett (2006). The Parental Protectiveness subscale was
initially constructed by Morrongiello and House (2004) and consists of 21 items.
It was used to describe the behaviors of 48 parents and children aged 2 - 5 years
related to injury risk. Its Cronbach’s alpha coefficient was .70. Subsequently,
Morrongiello and Corbett (2006) modified the PSAPQ and the Parental Protectiveness
subscale by reducing it to 9 items. Its psychometric properties were tested with a
sample of 192 U.S. parents of developmentally normal children aged 2 to 5 years.
Cronbach’s alpha and one month test-retest reliability coefficients were .78 and .72,
respectively.
This nine-item subscale of the Parental Protectiveness Questionnaire was
used in this study. Mothers were asked to rate items on a 5-point rating scale, ranging
from 1 (not true) to 5 (strongly true). The total sum of the scores ranged from 9 to 45.
Higher scores indicated that mothers had a high ability to protect their children from
injury and lower scores indicated that mothers had little ability to protect their
children from injury.
5. Parental Supervision were measured by the Parental Supervision Belief
subscale of the PSAPQ. This subscale was derived from a questionnaire measuring
parental supervision attributes relevant to children’s risk of unintentional injury and
was developed by Morrongiello and House (2004) and Morrongiello and Corbett
(2006). In this study, mothers were asked to rate all 9 items on a 5-point rating scale
ranging from 1 (not true) to 5 (strongly true). Items # 4 and # 6 were negative in
meaning and were reverse scored. The total sum of scores ranged from 9 to 45, with
higher scores indicating that mothers more closely supervised their children and lower
scores indicating that mothers provided less or inadequate supervision of their
children.
The Parental Supervision belief subscale had been tested for psychometric
properties with a sample of 192 U.S. parents of developmentally normal children aged
2 to 5 years. Cronbach’s alpha and the one month test-retest reliability coefficient
were .77 and .76, respectively (Morrongiello & Corbett, 2006).
6. The Parental Tolerance for Child’s Risk Taking was measured by the
Parental Tolerance for Children’s Risk Taking subscale of the PSAPQ. It was derived
from a questionnaire to measure parental supervision attributes which consisted of

51
parental behaviors, attitudes, and beliefs related to children’s risk of unintentional
injury by Morrongiello and House (2004) and Morrongiello and Corbett (2006).
Mothers were asked to rate all of 8 items on a 5-point rating scale ranging from 1 (not
true) to 5 (strongly true). The total sum of the scores ranged from 8 to 40. High scores
indicated parents who allowed or encouraged their children to do or to play with
objects or environment around them and low scores were parents who did not allow or
encourage their children to do or to play with objects or environment around them.
The Parental Tolerance for Children’s Risk Taking subscale was tested for
its psychometric properties with a sample of 192 U.S. parents of developmentally
normal children aged 2 to 5 years. Cronbach’s alpha and one month test-retest
reliability coefficient were .79 and .76, respectively.
7. The Parental Fate Beliefs were measured by the Parental Fate Beliefs
subscale of the PSAPQ. It was derived from a questionnaire to measure parental
supervision attributes consisting of parental behaviors, attitudes, and beliefs related to
children’s risk of unintentional injury by Morrongiello and House (2004) and
Morrongiello and Corbett (2006). The initial content of the Parental Fate Beliefs
subscale was extended to include an item indicating the parental belief that the health
and injury status of their child is predominantly a matter of luck or fate. This item was
taken from the Parent Health Locus of Control (PHLOC) scale by Morrongiello and
House (2004). Later, Morrongiello and Corbett (2006) modified the PSAPQ so that
the Parental Fate Beliefs included 3 items. Mothers were asked to rate all of 3 items
on a 5-point rating scale ranging from 1 (not true) to 5 (strongly true). Its total scores
ranged from 3 to 15, with higher scores indicating that parents believed that their
children getting hurt was more due to fate and lower scores indicating that parents did
not believe their children get hurt was due to fate.
The Parental Fate Beliefs subscale was tested for psychometric properties
with a sample of 192 U.S. parents of developmentally normal children aged 2 to 5
years. Cronbach’s alpha and one month test-retest reliability coefficients for the scale
were .78 and .80, respectively.
8. The Unintentional Home Injury in Toddlers (UHI) was measured by the
Likelihood of an Injury questionnaire. It was derived from a questionnaire measuring
Perception of Risk developed by Glik et al. (1991). It measures the chances of an

52
injury occurring to a child in its home. The original Likelihood of an Injury
questionnaire consisted of 17 items covering unintentional home injuries from falls,
burns, and poisoning. Its internal consistency reliability was tested with a sample of
1,247 U.S mothers rating their 6 - 60 months old children and yielded a Cronbach’s
alpha of .71.
In this study, the Unintentional Home Injuries in Toddlers consisted of 14
items. Four items from the Perception of Risk of Injury Questionnaire were not used
because the items overlapped with measures of the seriousness of the injury (e.g.,
bruises, cuts, puncture wound, broken bone). Moreover, one item about traffic injury
was added which consisted of type of traffic injury such as car or motorcycle crash, or
falls from a motorcycle. Mothers were asked to rate all 14 items on a 5-point rating
scale ranging from 0 (least likely) to 4 (most likely). The total sum of the scores
ranged from 0 to 56, with higher scores indicating that children had a greater risk of
injuries and lower scores indicating that children had a lower risk of injuries.
The summary of sources and characteristics of variables for analysis are
shown in Table 1.

53
Table 1 Sources and characteristics of the study variables
Variable Variable
source
No.
of
items
Rating
scale and
interpretation
Level of
variable
Psychometric
properties
Independent variables
1. Child Gender Demographic
questionnaire
1 1 = boy
2 = girl
Dicho-
tomous
n/ a
2. Child’s
Temperament
for Injury Risk
Score
The Injury
Behavior
Checklist (IBC)
(Speltz et al.,
1990)
23 Items: 1 (not at all) to
5 (very often)
Scoring: Simple sum of
rating scales = 23 – 115
Higher score = a
difficult temperament
child
Interval α = .87
test-retest,
r = .81, p <.01
(253 U.S
mothers of
child aged
2 -5)
Thai samples,
α = .94 (414 of
mothers of
child aged 24
to 71 months)
3. Home
Physical Hazard
Checklist
Score
- The Home
Injury Survey
(Phelan et al.,
2009)
- Home
Observation
Checklist
(Plitapolkarnpim,
n.d.)
51 0 = No
1 = Yes
Scoring: Simple sum of
rating scale = 0 – 51
Higher scores = high
home hazards
Interval The inter-rater
reliability
= .81
(7 research
assistants
observed in
the home of
children from
birth through
3 years of age
in the US)

54
Table 1 (continued)
Variable Instruments’
source/authors
No.
of
items
Rating
Scale and
interpretation
Level of
Variable
Psychometric
properties
Mediating variables
4. Parental
Protectiveness
Score
The
Protectiveness
subscale of the
PSAPQ
(Morrongiello &
House, 2004)
and
(Morrongiello &
Corbett, 2006).
9 1 (not true) to
5 (strongly true)
Scoring: Simple sum of
rating scale = 9 – 45
Higher score = greater
protection from injury
Interval α = .78,
test-retest,
r = .72,
p < .001
(192 parents
of children
aged 2-5
years in
Canada)
5. Parental
Supervision
Score
The Supervision
belief subscale
of the PSAPQ
9 1 (not true) to
5 (strongly true)
Scoring: Simple sum of
rating scale = 9 – 45
Higher scores = more
close parental
supervision
Interval α = .77,
test-retest,
r = .76,
p < .001
6. Parental
tolerance for
Child’s Risk
Taking Score
The Tolerance
for Children’s
Risk Taking
subscale of the
PSAPQ
8 1 (not true) to
5 (strongly true)
Scoring: Simple sum of
rating scale = 8 – 40
Higher scores = parents
allow more risk taking
Interval α = .79,
test-retest,
r = .76,
p < .001
7. Parental Fate
Beliefs Score
The Fate Beliefs
subscale of the
PSAPQ
3 1 (not true) to
5 (strongly true)
Scoring: Simple sum of
rating scale = 3 – 15
Higher scores = parents
believe in their child
getting hurt due to fate
Interval α = .78,
test-retest,
r = .80,
p < .001

55
Table 1 (continued)
Variable Instruments’
source/authors
No.
of
items
Rating
Scale and
interpretation
Level of
Variable
Psychometric
properties
Dependent variable
8. Unintentional
Home Injury in
Toddlers Score
(UHI)
The likelihood
of injury
subscale of the
Perception of
Risk (Glik
et al.,1991)
14
0 (least likely) to
4 (most likely)
Scoring: Simple sum of
rating scale = 0 – 56
Higher score = greater
risk of injury
Interval α = .71
(1,247 U.S
mothers rating
their child
ages 6 - 60
months)
A back- translation method
A method of back-translation is necessary for the cross-cultural application
of existing measures and is recommended for translating instruments from the original
language into the target language (Brislin, 1970; Cha, Kim, & Erlen, 2007; Hilton &
Skrutkowski, 2002; Sousa, Zauszniewski, Mendes, & Zanetti, 2005). Hence, this
study employed the following back-translation method.
First, the original English measures were translated independently into Thai
by two bilingual translators who were Thai native speakers. The two individuals were
a nursing faculty member at Asia-Pacific International University and a pediatrician at
Mission Hospital Bangkok. They translated the contents to convey the precise
meanings, statements from the original measures. Thai linguistic usages were applied
in a way that captured and clearly relayed the main subjects or ideas from the English
originals.
Second, each translated Thai version was translated independently back into
English language by two additional proficient bilingual linguists who had not seen the
original English version. They were an English teacher at the faculty of Business
Administration of Asia-Pacific International University and a faculty member from
the School of Humanities and Social Science at Burapha University.
Finally, the PI and the major advisor who are both bilingual, native Thai
speakers and knowledgeable about child injuries reviewed and compared the contents
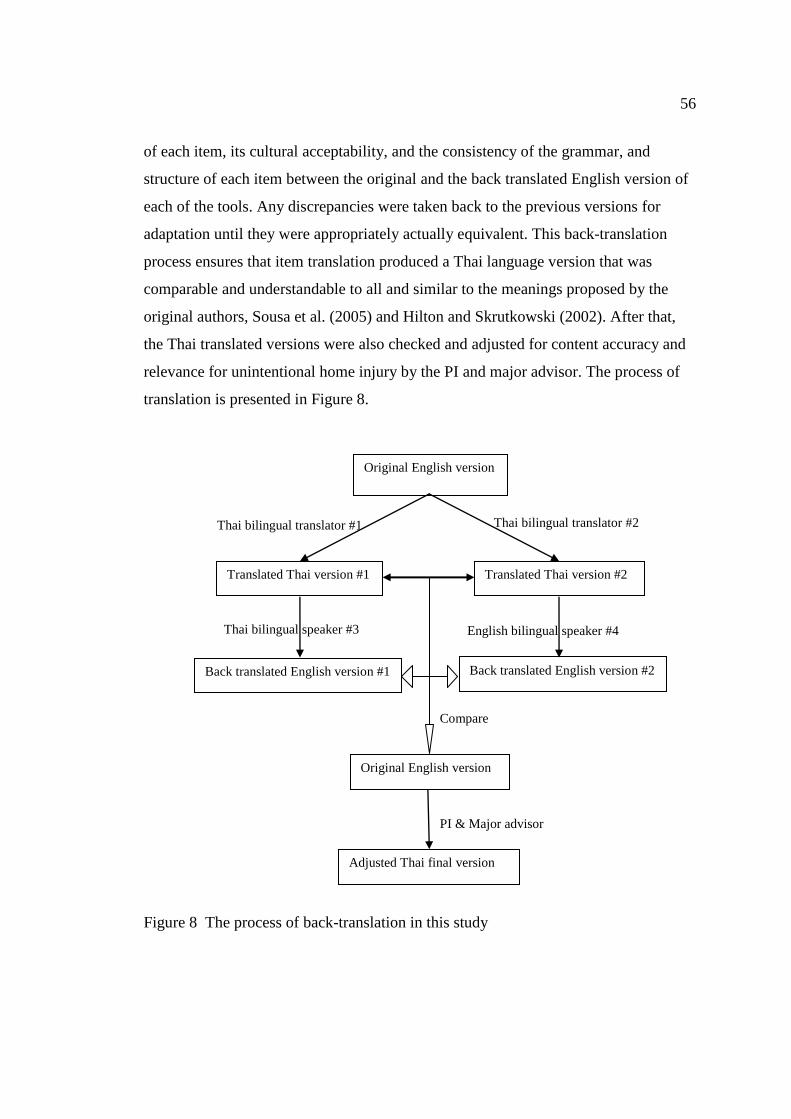
56
of each item, its cultural acceptability, and the consistency of the grammar, and
structure of each item between the original and the back translated English version of
each of the tools. Any discrepancies were taken back to the previous versions for
adaptation until they were appropriately actually equivalent. This back-translation
process ensures that item translation produced a Thai language version that was
comparable and understandable to all and similar to the meanings proposed by the
original authors, Sousa et al. (2005) and Hilton and Skrutkowski (2002). After that,
the Thai translated versions were also checked and adjusted for content accuracy and
relevance for unintentional home injury by the PI and major advisor. The process of
translation is presented in Figure 8.
Figure 8 The process of back-translation in this study
Compare
Translated Thai version #2
PI & Major advisor
English bilingual speaker #4 Thai bilingual speaker #3
Thai bilingual translator #2 Thai bilingual translator #1
Original English version
Translated Thai version #1
Back translated English version #1 Back translated English version #2
Adjusted Thai final version
Original English version

57
Psychometric properties of the measures
Validity
The questionnaires of the Child’s Temperament for Injury Risk, the Home
Physical Hazard Checklist, the Parental Protectiveness, the Parental Supervision, the
Parental Tolerance for Children’s Risk Taking, the Parental Fate Belief, and the UHI
were originally developed in English. After the instrument owners’ permissions were
granted, the instruments were translated into the Thai by using the back-translation
method described previously to ensure the validity of these tools.
In the content validity process, one item on the Child’s Temperament for
Injury Risk was deleted, leaving 23 items. The deleted item (# 10) was “refuses to use
seat belt or stay seated in car” which was about behavior in cars, but not relevant to
the concept of UHI. Four items from the Home Injury Survey (Phelan et al., 2009)
were deleted, regarding smoke and carbon monoxide detectors which are not normally
installed in Thai homes. This left 48 items. Moreover, three items about near
drowning (such as in a water well/ ditch or ponds near home or in a sink, or water
container in the home) of the Home Observation Checklist (Plitapolkarnpim, n.d.)
were added to be more relevant to the Thai home context. Finally, the Home Physical
Hazard Checklist consisted of 51 items before it was validated by four professors.
Four items overlapped with the UHI. These were about the kind of wound (e.g.,
puncture wound, bruise, gashes and cut, head injury) and were deleted. An item was
added about a traffic injury from a car or motorcycle crash, or a fall from a
motorcycle. This left a total of 14 items remaining.
Subsequently, content validity and language suitability in the Thai versions
were verified by four experts. These experts included a director of Child Safety
Promotion and Injury Prevention Research Center and three nursing faculty members.
The instruments were revised according to the recommendations of the experts and
then a Content Validity Index (CVI) calculated. The original UHI consisted of 17
items. Three of them (# 9 - 11) contained similar and overlapping meanings, and were
deleted and its CVI was 1.00 (14 items). The CVI of the Child’s Temperament for
Injury Risk, Home Physical Hazard Checklist, Parental Protectiveness, Parental
Supervision, Parental Tolerance for Children’s Risk Taking, and Parental Fate Beliefs
were .91, .94, 1.0, .89, .88, and 1.00 respectively. According to Lynn (1986) and

58
Davis (1992), assessment of the quality of data collection instruments should be based
on experts with relevant experience in the topic area and a high CVI is required that is
based on using a minimum of three experts and a minimum CVI of .80. Thus, content
validity of all Thai versions was acceptable.
Reliability
The reliability of study instruments was tested using internal consistency and
interobserver reliability. A pilot study was performed using 40 participants who have
children aged 1 to 3 years and resided in the Ratchathewee district of Bangkok
Metropolitan and met the inclusion criteria, but lived in a different community that
those from which the study sample was drawn. According to Hertzog (2008), 30 – 40
participants in a case study is adequate to evaluate instrumentation.
Cronbach’s alpha of the Unintentional Home Injury in Toddlers was .82, the
Child’s Temperament for Injury Risk was .91, the Parental Protectiveness was .79, the
Parental Supervision was .67, the Parental Tolerance for Child’s Risk Taking was .84,
and the Parental Fate Beliefs was .75. The rule of thumb for acceptable internal
consistency reliability is a Cronbach’s alpha of .70 or above (Hair, Black, Babin, &
Anderson, 2010).
Although the Cronbach’s alpha of the Parental Supervision scale was lower
than .70, and when item # 6 (about negative supervision of mother that their child can
play safely by his/ herself) was deleted, the Cronbach’s alpha went up to .83, this item
was retained in the scale since its meaning pertained strongly to the parental
supervision concept for unintentional home injury in toddler.
In addition, the interobserver reliability of the Home Physical Hazard
Checklist was tested by calculating the Pearson Correlation coefficient between scores
produced by two observers. They both observed 30 cases in their homes but worked
independently to do the ratings. Based on this, the interobserver reliability of the
Home Physical Hazard Checklist was r = .93, p < .01.
This study also tested the reliability of study instruments from a final sample
of 247 mothers with children aged from 1 to 3. The findings showed that the
Cronbach’s alpha for the Unintentional Home Injury in Toddlers scale decreased from
.82 to .66, the Child’s Temperament for Injury Risk also decreased from .91 to .88,
Parental Protectiveness remained the same at .79, Parental Supervision increased from

59
.67 up to .74, Parental Tolerance for Child’s Risk Taking increased from .84 up to .85,
and Parental Fate Beliefs increased from .75 up to .77.
Protection of human rights
The study proposal was approved by the Institutional Review Board (IRB) at
the Faculty of Nursing, Burapha University prior to data collection. Each potential
subject was fully notified in writing and given a participative permission request.
Potential participants could agree or refuse to join the study without any imposed
consequences. They were given the opportunity to discuss the purposes of the study
and assured of the confidentiality of their answers. Identity concealment was
accomplished by the assignment of code numbers to each participant and each
questionnaire. The list showing the correspondence between the code numbers and
participants’ identifiers was kept separate from the data and will be completely
destroyed after publication of the study findings.
Data collection procedures
1. After receiving IRB approval from the committee of the Faculty of
Nursing, Burapha University, the researcher selected research assistants who were
employees at the Child Safety Promotion and Injury Prevention Research Center and
Health Centre 2. There were three research assistants in order to easily establish and
maintain reliability and consistency among the observers. They collected data after
their office hours and on their days off.
2. The research assistants were provided instruments, all study procedures,
and received a full-day training on completing the research protocol provided by the
researcher. First, the researcher reviewed and discussed all procedures and
instruments with the research assistants. Second, there was a presentation of each
room interior and the surroundings of demonstration homes. The home presentation
included examples of both one and two-storey houses. After the end of the home
illustration, the research assistants immediately completed the homes’ physical
hazards observation tool and rated the home hazards. Third, the percent agreement
among the three research assistants was calculated. Discrepancies were discussed and
60
the research assistants repeatedly watched the video and scored the Survey tool until
80-100 percent agreement was achieved.
3. A data-collection permission letter from the Faculty of Nursing, Burapha
University was provided and submitted to the leaders of the communities in the
research target areas prior to the beginning of data collection.
4. The researcher and research assistants performed the random selection
following the methods described earlier and determined whether the participants met
the household study criteria. They recruited the eligible families by convenience
sampling. The researcher or the research assistants contacted community leaders and
explained the criteria for participation. Then community leaders took the researcher or
research assistants to meet with the family in order to make an appointment with the
mother. After that they conducted a home visit at a mutually agreed upon time and
date and explained to them the purposes of the research study, the potential benefits,
their expected participation in the study, and the elements of protection of human
subjects. They also obtained written informed consent from the participants.
5. After researcher or research assistants completed an interview, they asked
permission from the mother for home observation by using home observation
checklist. While observing the home, if researcher or research assistants had any
questions, they could ask the mother.
6. The researcher and research assistants took approximately 1 hour for data
collection in a given home. While answering the questionnaires, if any participants
did not understand certain questions, they would be given a clarification of the
question so they could answer to the best of their knowledge. At the end of data
collection time period, the researcher and research assistant checked that all the
answers on questionnaires were completed. If it was incomplete, the researcher
returned the questionnaire to participants in order to complete the questionnaire.
Data analyses
The Analysis of Moment Structure (AMOS) program of SPSS Version 20
was used for data analyses. Statistical significance level was set throughout the
analyses at p < .05. Methods of data analyses were as follows:
1. Data were reviewed and edited and then entered into a computer software

61
program database. Double entry was done with a later comparison to identify
inconsistencies to ensure accuracy of data entry.
2. The data were reviewed for missing data, and outliers.
3. Data were tested to assure they met the underlying assumptions necessary
for multivariate analysis. That is that they met the assumptions of normality, linearity,
and multicolinearity.
4. The demographic characteristics of the sample were summarized
descriptive statistics.
5. The relationships between pairs of continuous predictors and with the
unintentional home injury score were examined using Pearson’s correlation
coefficients.
6. The magnitude of causal effects, both direct and indirect, on UHI in
toddlers was analyzed with Structural Equation Modeling (SEM) using the AMOS
program.

CHAPTER 4
RESULTS
This chapter presents the results of data analyses to determine whether the
proposed causal model of unintentional home injury (UHI) in toddlers fits the data.
The results include a description of the sample’s demographic and home
characteristics, diagnostic tests for the Structural Equation Modeling (SEM) analyses,
descriptive statistics of the continuous study variables, and tests of the research
hypotheses.
Description of the demographic information of the sample
The sample included 250 mothers of 12 - 36 month-old children. Mother’s
demographic characteristics are presented in Table 2. Mothers ranged in age from 18
to 46 years with a mean of 28.35 (SD = 6.50). About fifty-one per cent of mothers
(51.2 %) were aged 21 - 30 years old, followed by 30.8 % who were 31 - 40 years old.
Most were married (85.2 %). More than one half of the mothers had completed their
education below the high-school level (54.0 %). There were 38.4 % who were
unemployed or a housewife. Among employed mothers, most were laborers (36.8 %),
followed by working in trade or private business (18.4 % and 3.6 %). Approximately,
80 % of the mothers had adequate family income, but 50 % had no savings and 30 %
had some savings.
The children’s demographic characteristics are presented in Table 3. The
ages of the children ranged from 12 to 41 months with an average of 25.52
(SD = 7.99). Forty-six per cent were between 24 - 36 months, and 44% were 12-24
months. Slightly more than half were boys (52.8 %) and 47.2 % were girls. First-born
children comprised 45.6 % of the sample and 32.8 % were the second-born. Mostly,
there were one (36 %) or two (36 %) children younger than 15 years living in the
sampled homes.

63
63
Table 2 Demographic characteristics of mothers (n = 250)
Mother n %
Age (years) (M = 28.35, SD = 6.50, range = 18 - 46)
≤ 20 34 13.6
> 20 - 30 128 51.2
> 30 - 40 77 30.8
> 40 - 50 11 4.4
Marital status
Married 213 85.2
Divorce/ Separated 33 13.2
Widowed 4 1.6
Education
≤ Elementary 53 21.2
Secondary school 82 32.8
High school/ Vocational 66 26.4
Diploma 14 5.6
Bachelor’s degree or more 35 14.0
Occupation
Unemployed/ House wife 96 38.4
Labor 92 36.8
Trading 46 18.4
Private business 9 3.6
Civil servant/ State enterprise 7 2.8
Family income
Inadequate 49 19.6
Adequate but not saving 126 50.4
Adequate and saving 75 30.0
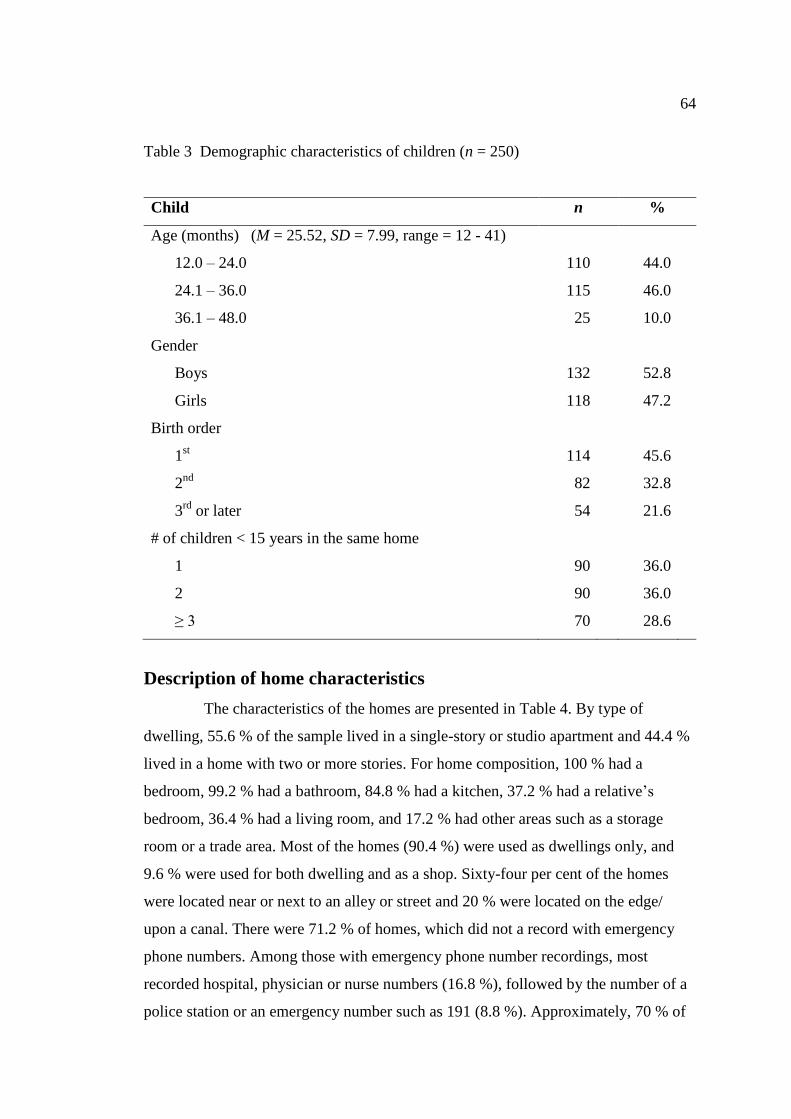
64
64
Table 3 Demographic characteristics of children (n = 250)
Child n %
Age (months) (M = 25.52, SD = 7.99, range = 12 - 41)
12.0 – 24.0 110 44.0
24.1 – 36.0 115 46.0
36.1 – 48.0 25 10.0
Gender
Boys 132 52.8
Girls 118 47.2
Birth order
1st
114 45.6
2nd
82 32.8
3rd
or later 54 21.6
# of children < 15 years in the same home
1 90 36.0
2 90 36.0
≥ 3 70 28.6
Description of home characteristics
The characteristics of the homes are presented in Table 4. By type of
dwelling, 55.6 % of the sample lived in a single-story or studio apartment and 44.4 %
lived in a home with two or more stories. For home composition, 100 % had a
bedroom, 99.2 % had a bathroom, 84.8 % had a kitchen, 37.2 % had a relative’s
bedroom, 36.4 % had a living room, and 17.2 % had other areas such as a storage
room or a trade area. Most of the homes (90.4 %) were used as dwellings only, and
9.6 % were used for both dwelling and as a shop. Sixty-four per cent of the homes
were located near or next to an alley or street and 20 % were located on the edge/
upon a canal. There were 71.2 % of homes, which did not a record with emergency
phone numbers. Among those with emergency phone number recordings, most
recorded hospital, physician or nurse numbers (16.8 %), followed by the number of a
police station or an emergency number such as 191 (8.8 %). Approximately, 70 % of

65
65
the homes had no baby walker, but about 30 % had baby walkers where the wheels
had not been removed (26.8 %). About 82.0 % of the sample had a vehicle and the
majority of these were parked near the home (50.8 %), followed by being parked at a
community/ relative’s home (18 %) and inside the home (13.2 %).
Table 4 Descriptive of home characteristics (n = 250)
Home n %
Type of dwelling
Single story/ studio 139 55.6
Two stories or more 111 44.4
Room/ area in home
Bedroom 250 100.0
Bathroom 248 99.2
Kitchen 212 84.8
Relative’s bedroom 93 37.2
Living room and other 91 36.4
Other (such as trade area or storage room) 43 17.2
Functions of home
Dwelling only 226 90.4
Dwelling and shop 24 9.6
Location
Near/ next to alley or street 160 64.0
On the edge/ upon a canal 50 20.0
Near/ next to a railroad 18 7.2
Near/ next to a roadway 17 6.8
Near/ next to a market 5 2.0

66
66
Table 4 (continued)
Home n %
Emergency phone number recording
None 178 71.2
Hospital, physician, or nurse 42 16.8
Police or 191 22 8.8
Ambulance 8 3.2
Baby walkers
No baby walker 174 69.6
Did not remove wheels 67 26.8
Removed wheels 9 3.6
Vehicle parking
No vehicle 45 18.0
Around home 127 50.8
Community/ relative’s house 45 18.0
In home 33 13.2
Assumption tests for the SEM analysis
The commonly used assumption tests in SEM analysis are tests for outliers,
normality, linearity, and multicolinearity (Tabachnick & Fidell, 2007). Results of
these diagnostic tests can have effects on the parameter estimates for testing the
hypothesized model (Schumacker & Lomax, 2010). All major variables were tested
with the diagnostic tested in order and the results demonstrated that all assumptions of
the SEM met criteria.
According to Tabachnick and Fidell (2007), univariate outliers are cases
with an extreme value or large standardized scores on one or more variables. If it is in
excess of 3.29 standard deviations or less than -3.29 standard deviations, it is an
outlier. The test results showed that there were 3 univariate outliers, including,
parental protectiveness (1 outlier) and UHI (2 outliers) (Table 11, Appendix 6). One
recommended remedial action is to delete them and to reanalyze the remaining data
(Cohen, Cohen, West, & Aiken, 2003). Consequently, three cases of outliers were
67
67
deleted from raw data. Therefore, 247 cases were tested for multivariate outliers,
normality of distribution, linearity, and multicolinearity.
The multivariate outliers were examined using Mahalanobis’ distance,
which can be measured for each case using the Chi-square distribution. A distance
with a probability value of the Chi-square statistic less than .001 is considered an
outlier. The results showed that there were no multivariate outliers for any of the
tested variables (Table 12, appendix 6). Next, multivariate normality was tested by
calculating statistics and using graphical methods. The statistics of normality were
skewness and kurtosis. A symmetric distribution of skewness and a peakiness
distribution of kurtosis are zero and the critical ratio for both of them is between -
1.96 and 1.96 (Hair et al., 2010). For this study, these tests were combined with
Blunch’s (2013) recommended use of graphical methods to judge a variable’s
normality. Thus, the dependent variable (UHI) was tested by calculating these
statistics and evaluating a histogram showing the frequency distribution of UHI. The
results showed that the variable UHI has a normal distribution (Table 13 and Figure
11 - 18, Appendix 6).
A linear, or straight-line, relationship between continuous variable and one
another is assessed by demonstrating a non-zero correlation of the Pearson correlation
coefficient (Shumacker & Lomax, 2010). The results for the relationship between
child gender and home physical hazards, and child temperament and parental
protectiveness proved to be nonlinear (Table 14, Appendix 6). However, this linearity
assumption could be ignored for the SEM analyses (Shumacker & Lomax, 2010).
Finally, multicolinearity, which refers to high correlations among
independent variables (r ≥ .90), was evaluated. Multicolinearity was tested by using a
correlation matrix (Tabachnick & Fidell, 2007), with tolerances value (< .2), and a
Variance Inflation Factor (VIF > 4). The results show no evidence of multicolinearity
among the predictors variables. The correlation matrix is presented in Table 14
(Appendix 6), and tolerance and VIF are presented in Table 15 (Appendix 6).
Descriptive statistics for the continuous study variables
Descriptive statistics for all continuous study variables are presented in
Table 5, which included child temperament, home physical hazards, parental
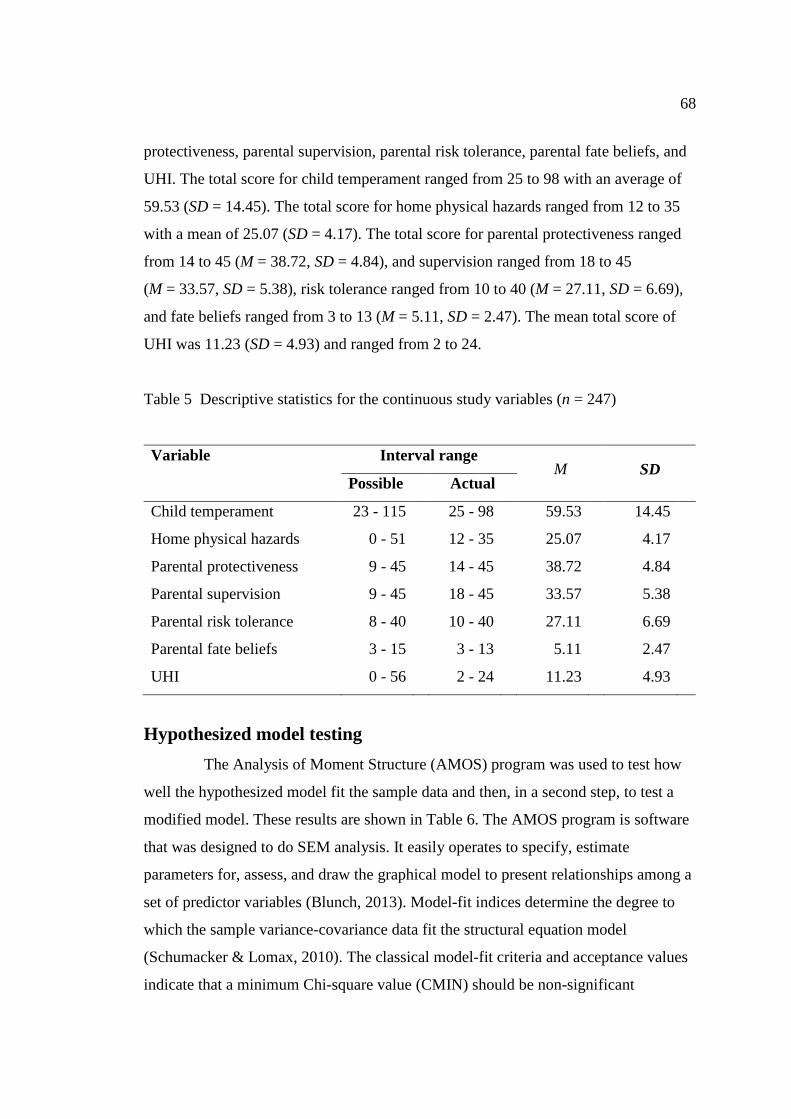
68
68
protectiveness, parental supervision, parental risk tolerance, parental fate beliefs, and
UHI. The total score for child temperament ranged from 25 to 98 with an average of
59.53 (SD = 14.45). The total score for home physical hazards ranged from 12 to 35
with a mean of 25.07 (SD = 4.17). The total score for parental protectiveness ranged
from 14 to 45 (M = 38.72, SD = 4.84), and supervision ranged from 18 to 45
(M = 33.57, SD = 5.38), risk tolerance ranged from 10 to 40 (M = 27.11, SD = 6.69),
and fate beliefs ranged from 3 to 13 (M = 5.11, SD = 2.47). The mean total score of
UHI was 11.23 (SD = 4.93) and ranged from 2 to 24.
Table 5 Descriptive statistics for the continuous study variables (n = 247)
Variable Interval range M SD
Possible Actual
Child temperament 23 - 115 25 - 98 59.53 14.45
Home physical hazards 0 - 51 12 - 35 25.07 4.17
Parental protectiveness 9 - 45 14 - 45 38.72 4.84
Parental supervision 9 - 45 18 - 45 33.57 5.38
Parental risk tolerance 8 - 40 10 - 40 27.11 6.69
Parental fate beliefs 3 - 15 3 - 13 5.11 2.47
UHI 0 - 56 2 - 24 11.23 4.93
Hypothesized model testing
The Analysis of Moment Structure (AMOS) program was used to test how
well the hypothesized model fit the sample data and then, in a second step, to test a
modified model. These results are shown in Table 6. The AMOS program is software
that was designed to do SEM analysis. It easily operates to specify, estimate
parameters for, assess, and draw the graphical model to present relationships among a
set of predictor variables (Blunch, 2013). Model-fit indices determine the degree to
which the sample variance-covariance data fit the structural equation model
(Schumacker & Lomax, 2010). The classical model-fit criteria and acceptance values
indicate that a minimum Chi-square value (CMIN) should be non-significant

69
69
(p > .05), with CMIN/ degrees of freedom (df) less than 2 (Tabachnick & Fidell,
2007), the root-mean square residual (RMR) (based on correlations) should be less
than .05, the Goodness-of-fit index (GFI) should be between .90 to 1.00, the adjusted
goodness-of-fit index (AGFI) between .90 to 1.00, and the root-mean-square error of
approximation (RMSEA) should be less than .05 (a value close to zero indicate a
good fit) (Blunch, 2013; Schumacker & Lomax, 2010).
The scores for the hypothesized model showed that the CMIN was equal to
7.76 (p >.05, df = 3), CMIN/ df was 2.59, RMR was .69, GFI was .99, AGFI was .99,
and RMSEA was .08. These findings indicate the hypothesized model was not
supported by the sample data. Subsequently, the hypothesized model was modified by
deleting parameters, one at a time, until the remaining estimated parameters achieve
the criteria for model goodness of fit (Schumacker & Lomax, 2010). After eliminating
some parameters to arrive at a well fitting model, the results for the modified model
showed CMIN was 4.98 (p >.05, df = 4), CMIN/ df was 1.25, RMR was .97, GFI was
.91, AGFI was .97, RMSEA was .03.
Table 6 Statistics of model fit index between the hypothesize and modified model
(n = 247)
Model fit criterion Acceptable score Hypothesized model Modified model
CMIN p > .05
χ2 = 7.76
p = .051 (df = 3)
χ2 = 4.98
p = .29 (df = 4)
CMIN/ df < 2 2.59 1.25
RMR < .05 .69 .97
GFI .90 – 1.00 .99 .91
AGFI .90 – 1.00 .99 .97
RMSEA < .05 .08 .03
Note CMIN = minimum Chi-square, RMR = root-mean square residual,
GFI = good-of-fit index, AGFI = adjusted goodness-of-fit index,
RMSEA = root-mean-square error of approximation

70
70
A path diagram of the hypothesized causal model of UHI in toddlers was
tested using parameter estimates and is displayed in Table 7 and Figure 9. The
hypothesized model proposed relationships among exogenous, mediator, and
endogenous variables. The exogenous variables included child gender, child
temperament, and home physical hazards. The mediators contained parental
protectiveness, parental supervision, parental risk tolerance, and parental fate beliefs.
The endogenous variables were parental protectiveness, parental supervision, parental
risk tolerance, parental fate beliefs, and UHI. The tested path of the hypothesized
model showed the parameter estimates and their directions were significant at a
probability level of less than .05.
The relationships between exogenous and endogenous variables: There was
a significant parameter estimate with a path from child temperament to parental
supervision in a negative direction ( = -.18, p < .01), which accounted for 5 % of the
variance in UHI (R2
= .05). The significant parameter estimates from child
temperament to parental risk tolerance was = .25 (p < .001) and accounted for 7 %
of variance (R2 = .07), and the estimate to parental fate beliefs was = .13 (p < .05)
and accounted for 3 % of variance (R2 = .03), and to UHI was = .53 (p < .001). In
addition, child temperament in combination with parental supervision accounted for
37 % (R2 = .37) in the variance prediction of UHI. However, the parameter estimate
from child temperament to parental protectiveness was not significant ( = .00,
p > .05). Moreover, none of the parameter estimates from child gender to parental
protectiveness ( = -.04, p > .05), supervision ( = -.11, p > .05), risk tolerance
( = .07, p > .05) fate belief ( = .07, p > .05) and UHI ( = -.01, p > .05) were
significant. The parameter estimates from home physical hazards to parental
protectiveness ( = .07, p > .05), supervision ( = .07, p > .05), risk tolerance
( = .08, p > .05) fate belief ( = -.10, p > .05) and UHI ( = .02, p > .05) were also
not significant.
The relationships between mediator and endogenous variables: There was a
significant parameter estimate from parental supervision to UHI in a negative
direction ( = -.17, p < .01). However, the parameter estimates from parental
protectiveness, risk tolerance, and fate belief to UHI were not significant ( = -.11,

71
71
p > .05, = -.00, p > .05, and = .03 p > .05 respectively).
A summary of the direct, indirect, and total effects of hypothesized model of
UHI from the parameter estimates is presented in Table 8.
Table 7 Standardized regression weights (Estimate), standard errors (SE), critical
ratio (C.R.), and p-value of the hypothesized model (n = 247)
Path Estimate SE C.R. p-value
Child gender
Parental protectiveness -.04 .62 -.57 .570
Parental supervision -.11 .67 -1.71 .087
Parental risk tolerance .07 .83 1.19 .235
Parental fate belief .07 .31 1.16 .246
UHI -.01 .50 -.21 .829
Child temperament
Parental protectiveness .00 .02 .02 .985
Parental supervision -.18 .02 -2.90 **
Parental risk tolerance .25 .03 3.99 ***
Parental fate belief .13 .01 2.03 *
UHI .53 .02 9.83 ***
Home physical hazards
Parental protectiveness .07 .07 1.11 .268
Parental supervision .07 .08 1.04 .300
Parental risk tolerance .08 .10 1.37 .171
Parental fate belief -.10 .04 -1.51 .132
UHI .02 .06 .33 .742
Parental protectiveness
UHI -.11 .06 -1.90 .058
Parental supervision
UHI -.17 .05 -2.83 **
Parental risk tolerance
UHI -.00 .04 -.04 .966
Parental fate belief
UHI .03 .10 .61 .539
Note SE = standard error, C.R. = critical ratio
* = p < .05, ** = p < .01, *** = p < .001

72 72
Unintentional
Home injury
in Toddlers
Parental
protectiveness
Parental
supervision
Parental
risk tolerance
Parental
fate beliefs
Child
temperament
Child gender
(boy)
Home
physical
hazards
2R = .01
2R = .05
2R = .07
2R = .03
ns
ns ns ns
ns
ns
ns ns
ns
ns
ns
ns ns
ns
2R = .37 -.18**
.53***
.25***
.13*
-.17**
Figure 9 The hypothesized causal model of unintentional home injury in toddlers
Note ns = non-significant, * = p < .05, ** = p < .01, *** = p < .001

73 73
Table 8 Parameter estimates of direct, indirect, and total effects of the hypothesized model (n = 247)
Causal
variable
Parental
protectiveness
Parental
supervision
Parental
risk tolerance
Parental
fate belief
Unintentional
home injury
DE IE TE DE IE TE DE IE TE DE IE TE DE IE TE
Child gender -.04 - -.04 -.11 - -.11 .07 - .07 .07 - .07 -.01 .02 .01
Child
temperament
.00 - .00 -.18** - -.18** .25*** - .25*** .13* - .13* .53*** .03*** .56***
Home physical
hazard
.07 - .07 .07 - .07 .08 - .08 -.10 - -.10 .02 -.02 -.00
Parental
protectiveness
- - - - - - - - - - - - -.11 - -.11
Parental
supervision
- - - - - - - - - - - - -.17** - -.17**
Parental
risk tolerance
- - - - - - - - - - - - -.00 - -.00
Parental fate
belief
- - - - - - - - - - - - .03 - .03
R2 = .01 R
2 = .05 R
2 = .07 R
2 = .03 R
2 = .37
* p < .05, ** p < .01, *** p < .001
Note DE = Direct effect, IE = Indirect effect, TE = Total effect

74
74
The path analysis of modified model
The final modified model was determined by deleting parameter estimates
with non-significant paths in the original hypothesized model until the revised model
achieved significant goodness of fit coefficients and specified parameters
(Schumacker & Lomax, 2010). The process followed was to remove the parameter
estimate with the highest probability value, then test the model-fit criteria to
determine if the new reduced model met the acceptance value. If the model indicated
values for the model-fit criteria that did not show a good fit to the data, the parameter
estimate with the highest probability value in the reduced model was removed and the
model fit tested again. This procedure was followed, removing the parameters with
the highest fit one by one, until the desired model-fit was achieved.
There were 14 non-significant parameters removed from the hypothesized
model (Table 7). The highest to the lowest probability value was deleted until the
parameter estimates of the modified model fit the model criteria well (Table 6). Paths
were deleted in the following order: 1) the path from child temperament to parental
protectiveness (p = .985), 2) the path from parental risk tolerance to UHI (p = .966),
3) the path from child gender to UHI (p = .829), 4) the path from home physical
hazards to UHI (p = .742), 5) the path from child gender to parental protectiveness
(p = .570), 6) the path from parental fate belief to UHI (p = .539), 7) the path from
home physical hazards to parental supervision (p = .300), 8) the path from home
physical hazards to parental protectiveness (p = .268), 9) the path from child gender to
parental fate belief (p = .246), 10) the path from child gender to parental risk
tolerance (p = .235), 11) the path from home physical hazards to parental risk
tolerance (p = .171), 12) the path from home physical hazards to parental fate belief
(p = .132), 13) the path from child gender to parental supervision (p = .087), and the
path from parental protectiveness to UHI (p = .058)
The path diagram and parameter estimates for the modified model are
presented in Table 9 and Figure 10. In this model, Exogenous variables are child
temperament and parental protectiveness, Mediators are parental supervision. And the
Endogenous variables are parental supervision and UHI. The relationships among all
variables were as follows.
There were significant parameters from child temperament to parental

75
75
supervision in a negative direction ( = -.17, p < .01) and to UHI in a positive
direction ( = .53, p < .001). That is, children with temperaments indicating greater
risk taking, had parents who provided less supervision and had a greater risk of UHI.
There were also significant parameter estimates in a positive direction from parental
protectiveness to parental supervision ( = .46, p < .01) and to UHI in a negative
direction ( = -.11, p < .05). The significant parameter estimate from parental
supervision to UHI was also negative ( = -.17, p < .01). In addition, child
temperament in combination with parental protectiveness accounted for 24 %
(R2
= .24) of the variance in parental supervision. Moreover, child temperament, in
combination with parental protectiveness and supervision, accounted for 37 %
(R2
= .37) of the variance in UHI.
Child temperament had a positive direct effect ( = .53, p < .001), indirect
effect ( = .03, p < .001), and total effect ( = .56, p < .001) on UHI. Parental
protectiveness had a negative direct effect ( = -.11, p < .05), indirect effect ( = -.08,
p < .05), and total effect ( = -.19, p < .05) on UHI (Table 10).
Table 9 Standardized regression weights (Estimate), standard errors (SE), critical
Ratio (C.R.), and p-value of the modified model of UHI (n = 247)
Path Estimate SE C.R. p-value
Child temperament
Parental supervision -.17 .02 -3.10 **
Unintentional Injury .53 .02 10.30 ***
Parental protectiveness
Parental supervision .46 .06 8.40 ***
Unintentional Injury -.11 .06 -2.00 *
Parental supervision
Unintentional Injury -.17 .05 -2.87 **
* p < .05, ** p < .01, *** p < .001

76
76
Figure 10 The modified model of unintentional home injury in toddlers
Note * = p < .05, ** = p < .01, *** = p < .001
Table 10 Direct, indirect, and total effects of causal variables on effect variables of
the modified model (n = 247)
Causal variable Parental supervision Unintentional injury
DE IE TE DE IE TE
Child temperament -.17** - -.17** .53*** .03*** .56***
Parental protectiveness .46*** - .46*** -.11* -.08* -.19*
Parental supervision - - - -.17** - -.17**
R2 = .24 R
2 = .37
* p < .05, ** p < .01, *** p < .001
Note DE = Direct Effect, IE = Indirect Effect, TE = Total Effect
Parental
supervision
R2 = .24
R2 = .37
-.17** -.17**
.53***
.46*** -.11*
Child
temperament
Parental
protectiveness
Unintentional
Home Injury

77
77
Study findings related to research hypotheses
The inferential findings of this study are described here for each research
hypothesis. The magnitude of causal effects, both direct and indirect, on UHI in
toddlers was analyzed with Structural Equation Modeling (SEM) using the AMOS
program, with a significance level set at p < .05 for all analyses.
Hypothesis one: Child gender (boy) has a direct positive effect on UHI.
The path coefficient between child gender and UHI was non-significant
( = -.01, p > .05) in the hypothesized model. Therefore, child gender did not have a
direct effect on UHI and was deleted from the modified model.
Hypothesis two: Child temperament has a direct positive effect on UHI.
Based on the hypothesized model and the modified model, the parameter
estimate for child temperament had a statistically significant direct positive effect on
UHI ( = .53, p < .001). Thus, the causal relationship proposed in the hypothesized
model of UHI in toddler was supported.
Hypothesis three: Home physical hazards have a direct positive effect on
UHI.
The study findings did not support this hypothesis. The direct effect of home
physical hazards on UHI was not statistically significant ( = .02, p > .05). The
measure of home physical hazards was deleted from the modified model.
Hypothesis four: Parental protectiveness has a direct negative effect on
UHI.
The estimate for parental protectiveness had a non-significant direct effect
on UHI ( = -.11, p > .05) in the initial hypothesized model. However, in the modified
model, the estimate was significant showing that parental protectiveness had a direct
negative effect on UHI ( = -.11, p < .05) and a direct positive effect on parental
supervision ( = .46, p < .001). Therefore, parental protectiveness, which had been
hypothesized to be a mediator in the initial hypothesized model, proved to be an
exogenous or independent variable in the modified model. This hypothesis was
supported.
Hypothesis five: Parental supervision has a direct negative effect on UHI.
The findings showed that the parameter estimate for parental supervision

78
78
had a significantly negative direct effect on UHI both in the hypothesized model and
the modified model ( = -.17, p < .01). Hence, the results support this hypothesis.
Hypothesis six: Parental tolerance for child’s risk taking has a direct
positive effect on UHI.
The parameter estimate for the hypothesized model revealed that parental
risk tolerance did not have a significant direct effect on UHI ( = -.00, p > .05). Thus,
the modified model did not include a relationship between parental risk tolerance and
UHI. This hypothesis was not supported.
Hypothesis seven: Parental fate beliefs have a direct positive effect on UHI.
Testing the hypothesized model revealed that parental fate beliefs did not
have a significant direct effect on UHI ( = .03, p > .05). Thus, the modified model
did not show a relationship between parental risk tolerance and UHI. Hypothesis
seven was not supported.
Hypothesis eight: Child gender (boy), child temperament, and home
physical hazards influences UHI through parental protectiveness, supervision,
tolerance for child’s risk taking, and fate beliefs.
Child gender and home physical hazards were not statistically associated
with UHI ( = .02, p > .05, = -.02, p > .05 respectively). However, child
temperament influenced UHI through parental supervision ( = .03, p < .001) both in
the hypothesized model and the modified model. The total effect of child
temperament was positive ( = .56, p < .001). Moreover, parental protectiveness had a
significant indirect negative effect on UHI through parental supervision ( = -.08,
p < .05) and its total effect was negative ( = -.19, p < .05). As a result, this
hypothesis was partially supported.
In summary, the results of this study testing a causal model of UHI in
toddlers were presented. Descriptive statistics indicated the characteristics of mothers,
their children, and their homes. Outliers, normality, linearity, and multicolinearity of
were tested in the preliminary analyses and found acceptable regarding the
assumptions for the statistics used. The hypothesized model was tested using model-
fit criteria compared to specific acceptance values and modified based on the results.
The paths of the modified model of unintentional home injury in toddlers fit the

79
79
sample data well. The modified model did not include paths to unintentional home
injury in toddlers from child gender, home physical hazards, parental risk tolerance,
and parental fate beliefs as hypothesized. But, the predicting factors in the modified
model showed strong relationships with unintentional home injury in toddlers. After
modification, the model indicated that child temperament had a direct positive effect
on UHI and influenced UHI through parental supervision. Additionally, parental
protectiveness had a statistically significant negative direct effect and indirect effect
on UHI through parental supervision. The total effect of child temperament was
positive ( = .56, p < .001) while the total effect of parental protectiveness was
negative ( = -.19, p < .05). That is, children whose difficult temperaments reflect
greater risk taking behavior had greater risk of UHI. Finally, the combination of child
temperament and parental protectiveness accounted for 24 % of the variance in
parental supervision and the combination of child temperament, parental
protectiveness, and parental supervision accounted for 37 % (R2 = .37) of the variance
observed for the measure of unintentional home injury risk in toddlers.

CHAPTER 5 DISCUSSION AND CONCLUSION
This chapter is presented in three main parts. The first part includes a
summary of the study, the second a discussion of the research findings related to each
research hypothesis and the resulting modified model. In the third and final section,
the study limitations and study strengths are presented and recommendations made for
future research and nursing practice.
Summary of the study
The purpose of this study was to determine the direct and indirect
relationships among predictors of unintentional home injury (UHI) in toddlers. These
predictors were based on a framework of interactions among child, parental, and
environmental factors. The child factors included gender and temperament. The
parental factors were comprised of protectiveness, supervision, tolerance for child’s
risk taking, and fate beliefs. The environmental factor included home physical
hazards.
A multi-stage stratified random sampling technique was employed to
identify 10 communities in the Ratchathewee district of Bangkok Metropolitan. A
sample group of 250 families from these communities were then selected by using
convenience sampling with inclusion criteria. These families are living in congested
one-story wooden houses or two-story wooden or half solid-structure and half wooden
houses surrounded with fences, and they have currently been residing in their houses
solely owned or rented in Ratchathewee district, Bangkok Metropolitan, for at least 6
months. There were eight questionnaires, including the Demographic Questionnaire
for mothers and their children, the Child’s Temperament for Injury Risk, Home
Physical Hazard Checklist, Parental Protectiveness, Parental Supervision, Parental
Tolerance for Child’s Risk Taking, Parental Fate Beliefs, and Unintentional Home
Injury in Toddlers. Additionally, these questionnaires were translated from their
original English version into the Thai language using the back-translation method.
Subsequently, their Content Validity Indices (CVI) and reliabilities were tested and

81
demonstrated as acceptable with CVIs for the Child’s Temperament for Injury Risk,
Home Physical Hazard Checklist, Parental Protectiveness, Parental Supervision,
Parental Tolerance for Child’s Risk Taking, Parental Fate Belief, and UHI of .91, .94,
1.0, .89, .88, 1.0, and 1.0 respectively. The Cronbach’s alpha coefficients for those
measures were .91, .75, .79, .67, .84, and .82 respectively. For Home Physical Hazard
Checklist, interobserver reliability was r = .93, p < .01 based on two observers ratings
of the same households.
Characteristics of mothers, children, and the mother’s home in this study
resemble those of the whole population sampled. Most of mothers were young adults,
married and living with their families, they had graduated from the upper elementary
school level, were unemployed/ house wives and labor, and had adequate family
income but no savings. More than half of their toddlers were boys. In their families,
the index toddlers were more often first-born rather than second-born. The sampled
children were younger than 15 years old and came from homes with one to two
children. Most of their homes were single story/ studio, which consisted of a bed
room, a bathroom, and a kitchen. Additionally, most of their homes were used for
dwelling only, and located near/ next to alley’s street. Only in a minority of homes,
did the mother’s have the following emergency numbers recorded near the phone:
hospital, police station, or ambulance. Only a minority of the homes had baby
walkers. Most of the walkers had not had the wheels removed. A majority of the
families’ vehicles were parked near their homes followed by parking in the home or
around neighborhood.
Data screening and assumption testing for the SEM analysis were used to
detect the accuracy of the data and whether the assumptions of the statistical method
were met. The initial sample of 250 participants was tested univariate outliers and
three cases were deleted because their standardized scores for either parental
protectiveness or UHI were higher than 3.29, indicating the scores were more than 3
standard deviations from the sample mean. Consequently, the final sample of 247
participants was tested for multivariate outliers for the characteristics of normality,
linearity, and multicolinearity. The results indicated that the assumptions for SEM
were met.
The hypothesized causal model of UHI in toddlers was tested by using the
82
AMOS program and the findings indicated the model did not fit the data. There were
14 non-significant parameter estimates for the hypothesized model, which were
removed by using a process of deleting non-significant paths with the highest
probability value one by one. Then, testing of the model-fit criteria was repeated until
the values of criteria were acceptable. Consequently, the final modified model was
identified by reaching one that met the goodness of fit criteria. There were 5
significant parameter estimates in the final modified model including: 1) the
parameter estimates from child temperament to parental supervision, 2) the parameter
estimates from child temperament to UHI, 3) the parameter estimates from parental
protectiveness to parental supervision, 4) the parameter estimates from parental
protectiveness to UHI, and 5) the parameter estimates from parental supervision to
UHI. The strongest direct predictor of UHI in toddlers was child temperament
followed by parental supervision and parental protectiveness. The indirect effects on
UHI through parental supervision were child temperament and parental
protectiveness. Surprisingly, child gender (boy) and home physical hazards did not
predict UHI.
Discussion of research findings
The research findings of this study are discussed in the next section
including those for the modified model and for each research hypothesis:
Hypothesis one: Child gender (boy) has a direct positive effect on UHI.
This hypothesis was not supported by the findings based on the parameter
estimate indicating a lack of correlation between gender (boy) and UHI. Results
indicated that boys did not experience more unintentional home injuries (UHI) than
did girls. This finding was inconsistent with evidence from numerous studies which
noted that, among toddlers, boys experienced UHI more often than girls (Barker et al.,
2004; Drago, 2005; Morrongiello et al., 2004 a; Sorenson, 2011). In addition, boys
were found to have more severe unintentional home injuries than girls, especially
injuries to their heads and necks, and boys were more likely to be risk-takers and
sensation-seekers than girls, while both behaviors were positively related to UHI
(Morrongiello et al., 2004 a). Nevertheless, two studies, one in Turkey (Atak et al.,
2010) and one in Thailand (Sirisamutr, 2008), found that gender was not significantly

83
associated with UHI. One potential explanation could be that parents or child
caregivers provide very good child rearing and protection equally to boys or girls,
possibly because families tend to be small. According to UNICEF, Thailand (2014),
the total fertility rate in Thailand 2012 was 1.4 %, and there were 1 - 2 children per
family.
Hypothesis two: Child temperament has a direct positive effect on UHI.
This hypothesis was supported by the findings based on the estimated
parameter which indicated a correlation between child temperament and UHI. This
correlation showed a significant direct positive effect on UHI. It indicated that a child
with difficult temperament or a high level of risk taking behavior was more exposed
to UHI. Consistent with this finding, numerous prior studies demonstrated that
children’s hyperactivity, aggressiveness, opposition, intensity, negative moods, and
irregular rhythmic expressions were highly, positively, correlated with unintentional
injuries (van Aken, Junger, Verhoeven, van Aken, & Dekovic, 2007; Dal Santo et al.,
2004; Morrongiello et al., 2008; Sirisamutr, 2008). Additionally, a study by Thomas
and Chess (1977) elaborated a clearer description of child temperament and UHI.
They analyzed temperament in five year old children and found that about 40 %
showed an easy temperament, 15 % were slow to warm up, and 10 % were classified
as having a difficult temperament. The rest of the sample (35 %) showed mixed
characteristics with some evidence of difficult temperament, while also being slow to
warm up, and having some evidence of easy temperament. For example, a child might
have hyperactivity and high resistance but be slowly adaptive as well. They also
described that children with difficult temperament showed withdrawal responses to
new things, non-adaptability to changes, frequent and negative intense mood
expression, and hyperactivity, each of which are associated with greater risk of
unintentional injuries than found for children with easy or slow to warm up
temperaments. Therefore, having a difficult temperament child predicts a higher risk
of UHI.
Child temperament also had a direct negative effect on parental supervision.
It could be implied that children with difficult temperament are less closely
supervised. This finding seemed inconsistent with prior studies which found that
parents of young children with difficult temperaments provided closer supervision

84
than did parents of easier temperament children (Morrongiello et al., 2006 b;
Morrongiello et al., 2008).
Hypothesis three: Home physical hazards have a direct positive effect on
UHI.
This hypothesis was not supported because of finding a non-significant
correlation for the estimated parameter describing the relationship between home
physical hazards and UHI. Children who lived in homes with more physical hazards
did not have higher risk of UHI. This was inconsistent with prior studies. For
example, Sirisamutr (2008) found that children who lived in a house, which was
structurally unstable, in need of repair, and had a high hazards level had higher UHI
than children who lived in a stable house with a low hazards level. In addition, UHI
could be reduced by installing safety devices in the homes such as smoke detectors,
stair gates, and safe storage for sharp objects, and cleaning products (Kendrick et al.,
2005; Phelan et al., 2011). However, there was one study indicating that children
whose homes had more physical hazards did not have higher UHI that required
medical attention (Watson et al., 2004). Similarly, the present findings found that the
total sum of home physical hazards produced a score that ranged from 12 to 35 with
an average of 25.07 (SD = 4.17) which represents a high number of hazards and a
somewhat high risk for child injury both within the home, especially in the kitchen,
bedroom, bathroom, as well as around the home or home vicinity including the alley’s
street. Interestingly, most participants reported that while their homes exposed
children to high numbers of physical hazards their children had never experienced
severe UHI, especially from poisoning, sharp object injury, and motorcycle accidents.
This may have evidence for a link between supervision and hazards. There was
evidence that parental close supervision in homes with high physical hazards resulted
in lower rates of UHI among toddlers in Canada (Morrongiello et al., 2009) and in
Thailand (Chatsantiprapa, Chokkanapitak, & Pinpradit, 2001). The closer supervision
and mothers frequently checking on their children were associated with fewer and the
less severe UHI even in the presence of high physical hazards. Child rearing practices
of Thai children’s parents include being highly protective. For example, at meal time,
parents hold children sitting in their laps or on their chair for feeding and parents have
their children sleep in the same bed with them. On the contrary, parents in western

85
countries train their children to sit separately and to feed themselves at younger ages
and to sleep in separate bedrooms from early in infancy. Additionally, it also could be
that there is a higher adult to young child ratio in the Thai home. This would mean
greater support and respite for the mother without reducing supervision. The number
of children are fewer and the Thai home is also more likely to be intergenerational
than homes in western culture. For these reasons, young Thai children were in their
parent arms and under direct supervision at all times. Consequently, children could
stay away from unintentional home injury even with hazardous things present in the
house. This finding is consistent with the study of Pichayapinyo, Pawwatana and
Thongvichaen (2008) that Thai parents’ were more protective and less authoritative,
authoritarian, and permission in their parenting style.
Hypothesis four: Parental protectiveness has a direct negative effect on
UHI.
This hypothesis was supported by findings an estimated parameter
indicating correlation between parental protectiveness and UHI. Parental
protectiveness showed a significant direct negative effect on UHI. This indicates that
mothers with high protectiveness had toddlers who experienced less UHI. This
characteristic was consistent with the prior research (Garling & Garling, 1993;
Morrongiello et al., 2006 a; Peterson et al., 1993). Mothers provided more attention to
their children’s activities when their children were in locations in their homes with
greater risk such as the kitchen, dining room, or bath room. Additionally, some
parents gave verbal warnings and offered direct physical assistance to their children
when concerned about injury protection while their children used play equipment
(Morrongiello & Dawber, 1999). In addition, the study of Morrongiello et al. (2004 a)
reported that mothers who had high scores for being protective were more likely to
protect their toddlers (e.g., “ keep a close watch on a child”; “know exactly what a
child is doing) and had toddlers who experienced fewer unintentional injuries at
home.
The estimated parameters and correlation coefficients for parental
protectiveness also showed a direct positive effect on parental supervision. The
evidence showed that mothers’ who were protective of their children or who thought
about their children’s injury risks, demonstrated closer supervision by protective

86
mothers than neglecting mothers. It revealed that parental protectiveness might be the
cause of increased parental supervision. However, there was little literature supporting
the idea that parental protectiveness had a direct positive effect on parental
supervision. There is a finding of Morrongiello and Corbett (2006), which
demonstrated a relationship between parental protectiveness and supervision among
children aged 2 to 5. They found that parental protectiveness was the characteristic
most positively associated with parental supervision. Therefore, the next study should
reconfirm causal association between these two variables.
Hypothesis five: Parental supervision has a direct negative effect on UHI.
This hypothesis was supported by the findings of the estimated parameters
and correlation between parental supervision and UHI. There was a statistically
significant direct negative effect between parental supervision and UHI. Parental
supervision of toddlers acted as direct reaffirmation of their children’s current activity
and parents’ exhibited continuity of supervision so that supervision continually
preceded their children’s behaviors (constant/intermittent/ not at all) (Morrongiello &
Schell, 2009; Saluja et al., 2004). Inversely, parents who reported inadequate
supervision had their children exposed to more injury risk and UHI (Landen et al.,
2003; Morrongiello et al., 2009; Munro et al., 2006). Practically, most parents cannot
be closely with their children at all times, but if they frequently check on their
children they will have less UHI.
Hypothesis six: Parental tolerance for child’s risk taking has a positive
direct effect on UHI.
This hypothesis was not supported by the findings based on the estimated
parameter between parental tolerance for children’s risk taking and UHI. Parents who
toleration of their children’s risk taking behavior was not associated with children’s
risk of UHI. This was inconsistent with previous studies which pointed out that
parents who had tolerance for their children’s injury risk taking, such as freely
allowing their children’s self-expression, experimentation, or exploration, had
children who experienced more injuries (Morrongiello, Corbett, & Kane, 2011;
Schwebel et al., 2004). One study found that parental tolerance of children’s risk
taking behavior indicated that mothers allowed their children to engage in greater risk
taking activities (such as climbing on a playground climber, swimming in a pool, etc.)

87
because they believed that their children should have a high level of experience in
these activities and that there were adequate safety measures in place to prevent injury
(Marrongiello & Major, 2002). In view of toddler development, because children aged
1 to 3 have limited physical and cognitive skills (Hockenberry & Wilson, 2007;
Puckett & Black, 2005) their mothers may not tolerate risk behaviors at their very
young age that they might tolerate when they are older. Turning to the family’s
developmental tasks, the family’s task during the toddler period is not only to provide
a safe environment, but it is also to help the child develop a positive self-concept, to
handle aggressive behavior as well as preventing injuries (Duvall, 1977; Phuphaibul,
Tachachhong, Kongsuktrakul, & Ooon-sawai, 2002).
Hypothesis seven: Parental fate beliefs have a direct positive effect on UHI.
This hypothesis was not supported by the findings. Parents belief in fate as a
determinate of injury had no relationship with children’s risk of UHI. This finding
was inconsistent with the prior studies which found that parents who believed their
child’s injuries were predominantly a matter of luck or fate, had children with an
increased risk of injury (Morrongiello & House, 2004; Morrongiello et al., 2004 a).
One potential explanation for the current study’s contrary findings could be that they
are evidence of the success of Thailand’s instituting new policies, education and skill
training related to accidental injury prevention and first aid for children, parents, and
caregivers (Office of Promotion and Protection of Children, Youth, the Elderly, and
Vulnerable Groups, 2007). These policies were developed after Thailand participated
as one of the 193 United Nations’ member nations to establish The National Policy
and Strategies on child development as a topic in “A World Fit for Children” (2007-
2016) whereby parents would be educated on what causes child injuries and how to
prevent them. Numerous studies have shown that parents who have a high degree of
knowledge or education about injury prevention have children with fewer injuries
(Hjern et al., 2001; Jordan, Duggan, & Hardy, 1993; Laursen & Nielsen, 2008). In
other words, parents who obtained more information on injuries, retained more of
safety precaution behaviors (Nansel, Weaver, Jacobsen, Glasheen, & Kreuter, 2008;
Posner et al., 2004; Tertinger, Greene, & Lutzker, 1984) and were better able to
protect their children from injury. When parents believed that most injuries were
preventable, then UHI would be rare (Coffman, Martin, Prill, & Langley, 1998;

88
Hooper, Coggan, & Adams, 2003).
Hypothesis eight: Child gender, child temperament, and home physical
hazards influence UHI through parental protectiveness, supervision, tolerance for
children’s risk taking, and fate beliefs.
This hypothesis can be discussed in terms of mediators/ moderators of the
relationships between predictors and UHI.
Child temperament: The estimated parameter from child temperament to
UHI had a significant positive indirect effect on UHI through parental supervision
( = .03, p < .001). The total effect of child temperament was positive ( = .56,
p < .001). Furthermore, correlation analyses showed that child temperament was
negatively associated with parental supervision and positively associated with UHI
(r = -.17, p < .01 and r = .56, p < .01 respectively). It indicated that difficult
temperament children accounted for more UHI when their mother provided low levels
of supervision, a finding consistent with previous studies (Morrongiello & Hogg,
2004; Morrongiello et al., 2008). Practically, hyperactive children are rarely left
unsupervised and their mothers supervised them more closely than mothers of
children with normal active levels (Morrongiello et al., 2008). Interestingly, the
estimated parameter from child temperament did not show an indirect effect on UHI
through parental protectiveness, parental tolerance for children’s risk taking, and
parental fate beliefs. Hence, the findings only partially supported this hypothesis
because child temperament proved to be the only
significant predictor of UHI through parental supervision.
Parental protectiveness proved to have a negative indirect effect on UHI
through parental supervision and the total effect was negative a relationship which
was not hypothesized. This finding indicated that parents who had more ability to
closely supervise their children, had children who experienced less UHI.
In summary, the findings partially supported the relationships hypothesized
in the modified model. The strongest to the weakest significant direct predictors of
UHI were child temperament, parental supervision, and parental protectiveness,
respectively. Child temperament and parental protectiveness also had a direct effect
on parental supervision. As for indirect effects, there were two predictors that had a
significant indirect effect on UHI, which were child temperament and parental

89
protectiveness, which operated through parental supervision. The predictors that did
not have the hypothesized direct effects on UHI were child gender (boy), home
physical hazards, parental tolerance for child’s risk taking, and parental fate beliefs.
Additionally, child gender (boy) and home physical hazards had no indirect effects on
UHI through parental protectiveness, supervision, tolerance for child’s risk taking,
and fate beliefs.
The present findings provide a context of causal relationship between the
significant predictors and unintentional injuries which occurred to toddlers in and
around home in Thailand. The finding pointed that the significant causal predictor of
UHI was not only children temperament but also protectiveness and supervision of
mothers. In fact, difficult temperament child predicted more UHI exposure when
his/her mother did not closely supervise and inversely, UHI could decrease when
his/her mother had more protectiveness and more adequate supervision on her child.
Limitations of the study
There are three limitations to this study. First, generalizability to other
different populations may be need to be considered. Participant recruitment and data
collection was limited by the location of participants’ homes in urban area
communities. While sampling procedures provided a representative sample of
communities in the region from which the families were drawn, a significant strength
of the design, the findings can only be generalized to similar urban areas. The
characteristics of home physical hazards and parental supervisory attributes may be
different in rural areas. Second, the research instruments were originally designed in
English and were translated into Thai for the first time for use in this study. Even
though back translation was performed and the back-translated version carefully
examined for conceptual consistency, translation can never be absolutely perfect and
not all concepts have counter parts in another culture and language. Another
important limitation is that the cross-sectional design of this study precludes proving
causal relationships. This study provides data that provides strong support for the
modified causal model but it cannot provide proof of causal relationships.
A prospective design where data on the risk factors are collected first, and the
outcome, Unintentional Home Injury, is measured at a later time would provide the

90
next level of evidence for cause.
Study Strengths
This study has four strengths. First, is the sampling of the geographic area.
The Ratchathewee district is located in the inner group of districts of Bangkok and it
is a highly populated area clustered with community housing. The communities are
classified into three types according to population density and the condition of
dwellings (i.e. Type one: congested one-story wooden houses, Type two: two-story
wooden or half solid structures, including half wooden houses with fences around
them, and Type three: apartments). Each sampled community for this study belonged
to type one or two. The characteristics of the community in Ratchathewee district
could represent the identity for many communities in other inner group districts of
Bangkok. Second, a proportional sample was drawn from each community by using a
multi-stage stratified random sampling technique. This method can reduce sampling
error and ensure more precise estimations of the population parameters in order to
obtain a homogenous sample in this study (Burns & Grove, 2005; Polit & Beck,
2012). Third, the sample size of 250 subjects was adequate to maintain power and to
obtain stable parameter estimates and standard errors for the Structural Equation
Modeling (SEM) (Schumacker & Lomax, 2010). Finally, SEM was selected to
analyze the proposed causal model for UHI in this study because it explicitly takes
measurement error into account and as data is processed statistically the equations
work simultaneously (Schumacker & Lomax, 2010). Additionally, SEM can evaluate
causal models where all predictor variables are related to each other and it uses
maximum likelihood to calculate the path coefficients in order to estimate the values
of the parameters of the model that would result in the highest likelihood of
reproducing the actual data (Meyers, Gamst, & Guarino, 2006).
Implications for nursing
Pediatric, educator, and public health nurses should gain understanding of
the associations between child temperament, parental protectiveness, parental
supervision, and UHI in toddlers. Particularly, a child with a difficult temperament is

91
at greater risk for UHI and professional nurses should assist parents to recognize
characteristics of their children that represent difficult temperament and to understand
their children’s behavior well in order to decrease injury risk behaviors. Furthermore,
nurses should identify parental supervisory attributes of parents such as parental
tolerance for children’s risk taking and parental fate beliefs. In addition, nurses should
be in tune with parental supervisory behaviors and provide support and guidance to
give appropriate protections and close supervision.
In some cases, parents of some toddlers with difficult temperaments may
report that they could not supervise their children adequately around the clock
because they have to work and their children are very naughty. To promote
appropriate parental supervision to prevent UHI, professional nurses have to
emphasize the importance of close supervision of children in both risk and non-risk
environments, while sleeping and while awake, and during play with friends or
playing toys or with play equipment. Additionally, clinical nurse administrators need
to develop policies for close supervision of toddlers in hospital wards and playrooms
during hospitalization in order to prevent injuries.
However, close supervision is not enough to prevent children’s injuries in
some situations because children are unable to differentiate between safe and
dangerous things. Protection by parents, that is appropriate for the toddler’s level of
development, can help their children feel more secure and be safer as they explore the
world. It is an obligation that nurses and the public health sector have to provide
knowledge of various UHI situations and child protection to parents.
Recommendations for future research
There are several recommendations for future research suggested by this
study. First, the instruments used in this study were derived from English measures
developed in Euro-American cultures. Although, the psychometric properties of the
measures were tested by using a back-translation process and content validity, and
reliability yielded acceptable results, it would be more valuable to develop measures
that can ensure accuracy of concepts related to unintentional injury in Thai toddlers.
The findings from testing the hypothesized causal model of unintentional
home injury in toddlers provide new information about Thai mothers of toddlers

92
residing in urban communities. It would be useful to replicate this cross-sectional
design in rural communities and to include children and their parents from high
economic circumstances. Additionally, longitudinal and qualitative designs should be
implemented for stronger evidence of cause and for deeper understanding of complex
interactions between parental supervisory attributes and unintentional home injury.
Furthermore, it would be beneficial to design, conduct and evaluate
interventions to prevent UHI based on the three predictors of unintentional home
injury identified in this study as well as information from the literature. Experimental
interventions should target patterns of parental supervision in combination with
children’s risk taking behaviors in order to reduce unintentional home injuries.
Conclusion
This research study tested a model of UHI in Thai toddlers and provides an
understanding of the causal pathways linking predictors and UHI. Child temperament,
parental supervision, and parental protectiveness are significant contributing factors to
risk of UHI. This model met the model-fit criteria for the data collected from a final
sample of 248 mothers with a target child aged from1 to 3. The findings suggest a
new direction for education and preventive interventions targeting the caretakers of
toddlers which has relevance to the nursing profession and health care administrators.

REFERENCES
Agran, P. F., Anderson, C., Winn, D., Trent, R., Walton-Haynes, L., & Thayer, S.
(2003). Rates of pediatric injuries by 3-month intervals for children 0 to 3
years of age. Pediatrics, 111(6), e683-e692.
Alptekin, F., Uskun, E., Kisioglu, A. N., & Ozturk, M. (2008). Unintentional
non- fatal home-related injuries in Central Anatolia, Turkey: Frequencies,
characteristics, and outcomes. Injury, International Journal of the Care of
the Injuried, 39(5), 535-546.
Atak, N., Karaoglu, L., Korkmaz, Y., & Usubutun, S. (2010). A household survey:
Unintentional injury frequency and related factors among children under
five years in Malatya. The Turkish Journal of Pediatrics, 52(3), 285-293.
Barker, R., Hockey, R., & Miles, E. (2004, February). Toddler falls from baconies &
windows. Injury Bulletin, 80, 1-4.
Bartolomeos, K., Mathers, C. D., Oldenziel, K., Linnan, M., & Hyder, A. A. (2008).
Statistical annex. In M. Peden, K. Oyegbite, J. Ozanne-Smith, A. A. Hyder,
C. Branche, AKH. F. Rahman, F. Rivara, & K. Bartolomeos (Eds.), World
Report on Child Injury Prevention (pp. 157-202). Geneva: WHO Press.
Bernard-Bonnin, A. C., Pless, I. B., Robitaille, Y., Leblanc, J., King, W. J.,
Tenenbein, M., & Klassen, T. P. (2003). Home injury patterns in children:
A comparison by hospital sites. Paediatr Child Health, 8(7), 433-437.
Blunch, N. J. (2013). Introduction to structural equation modeling using IBM SPSS
statistics and Amos (2nd
ed.). Los Angeles: SAGE.
Brislin, R. W. (1970). Back-translation for cross-cultural research. Journal of Cross-
Cultural Psychology, 1(3), 185-216.
Burn, N., & Grove, S. K. (2005). The practice of nursing research: Conduct, critique,
and utilization (5th
ed.). St. Louis: Elsevier.
Cataldo, M. F., Finney, J. W., Richman, G. S., Riley, A. W., Hook, R. J., Brophy,
C. J., & Nau, P. A. (1992). Behavior of injured and uninjured children and
their parents in a simulated hazardous setting. Journal of Pediatric
Psychology, 17(1), 73-80.
94
Čelko, A. M., Grivna, M., Dáňová, J., & Barss, P. (2009). Severe childhood burns in
the Czech Republic: Risk factors and prevention. Bulletin of the World
Health Organization, 87(5), 374-381.
Cha, E-S., Kim, K. H., & Erlen, J. A. (2007). Translation of scales in cross-cultural
research: Issues and techniques. Journal of Advanced Nursing, 58(4),
386-395.
Chatsantiprapa, K., Chokkanapitak, J., & Pinpradit, N. (2001). Host and environment
factors for exposure to poisons: A case-control study of preschool children
in Thailand. Injury Prevention, 7(3), 214-217.
Clamp, M., & Kendrick, D. (1998). A randomised controlled trial of general
practitioner safety advice for families with children under 5 years. British
Medical Journal, 316(7144), 1576-1579.
Coffman, S., Martin, V., Prill, N., & Langley, B. (1998). Perceptions, safety
behaviors, and learning needs of parents of children brought to an
emergency department. Journal of Emergency Nursing, 24(2), 133-139.
Cohen, J., Cohen, P., West, S. G., & Aiken, L. S. (2003). Applied multiple regression/
correlation analysis for the behavioral sciences (3rd
ed.). Mahwah, NJ:
Lawrence Erlbaum Associates.
Collins, N. C., Molcho, M., Carney, P., McEvoy, L., Geoghegan, L., Phillips, J. P., &
Nicholson, A. J. (2013). Are boys and girls that different? An analysis of
traumatic brain injury in children. Emergency Medicine Journal, 30(8),
675-678.
Colson, E. R., & Dworkin, P. H. (1997). Toddler development. Pediatrics in Review,
18(8), 255-259.
Cross, T. L. (2001). Gifted children and Erikson’s theory of psychosocial
development. Gifted Child Today, 24(1), 54-62.
Dal Santo, J. A. D., Goodman, B. M., Gilk, D., & Jackson, K. (2004). Childhood
unintentional injuries: Factors predicting injury risk among preschoolers.
Journal of Pediatric Psychology, 29(4), 273-283.
Damashek, A. L., Williams, N. A., Sher, K. J., Peterson, L., Lewis, T., &
Schweinle, W. (2005). Risk for minor childhood injury: An investigation of
maternal and child factors. Journal of Pediatric Psychology, 30(6), 469-480.

95
Davis, L. L. (1992). Instrument review: Getting the most from your panel of experts.
Applied Nursing Research, 5(4), 194-197.
Dishion, T. J., & McMahon, R. J. (1998). Parental monitoring and prevention of child
and adolescent problem behavior: A conceptual and empirical formulation.
Clinical Child and Family Psychology Review, 1(1), 61-75.
Dolan, B., & Holt, L. (2008). Accident & emergency theory into practice (2nd
ed.).
Edinburgh: Bailliere Tindall Elsevier.
Drago, D. A. (2005). Kitchen scalds and thermal burns in children five years and
younger. Pediatrics, 115(1), 10-16.
Duvall, E. M. (1977). Marriage and family development (5th
ed.). Philadelphia: J. B.
Lippincott Company.
Ellsäßer, G., & Berfenstam, R. (2000). International comparisons of child injuries and
prevention programs: Recommendations for an improved prevention
program in Germany. Injury Prevention, 6(1), 41-45.
Fullard, W., McDevitt, S. C., & Carey, W. B. (1984). Assessing temperament in
one-to three-year-old children. Journal of Pediatric Psychology, 9(2),
205-217.
Gaines, J., & Schwebel, D. C. (2009). Recognition of home injury risks by novice
parents of toddlers. Accident Analysis and Prevention, 41(5), 1070-1074.
Garling, A., & Garling, T. (1993). Mothers’ supervision and perception of young
children’s risk of unintentional injury in the home. Journal of Pediatric
Psychology, 18(1), 105-114.
Garzon, D. L. (2005). Contributing factors to preschool unintentional injury. Journal
of Pediatric Nursing, 20(6), 441-447.
Garzon, D. L., Lee, R. K., & Homan, S. M. (2007). There's no place like home: A
preliminary study of toddler unintentional injury. Journal of Pediatric
Nursing, 22(5), 368-375.
Glik, D., Kronenfeld, J., & Jackson, K. (1991). Predictors of risk perception of
childhood injury among parents of preschool. Health Education Quarterly,
18(3), 285-301.
Goldsmith, H. H. (1996). Studying temperament via construction of the toddler
behavior assessment questionnaire. Child Development, 67(1), 218-235.
96
Goldsmith, H. H., Buss, A. H., Plomin, R., Rothbart, M. K., Thomas, A., & Chess, S.
(1987). Roundtable: What is temperament? Four approaches. Child
Development, 58(2), 505-529.
Gordon, J. E. (1949). The epidemiology of accidents. American Journal of Public
Health, 39(4), 504-515.
Granié, M. A. (2010). Gender stereotype conformity and age as determinants of
preschoolers' injury-risk behaviors. Accident Analysis and Prevention,
42(2), 726-733.
Hair, J. F., Black, W. C., Babin, B. J., & Anderson, R. E. (2010). Multivariate data
analysis a global perspective (7th
ed.). Boston: Pearson Education.
Harrell, W. A., & Reid, E. E. (1990). Safety of children in grocery stores: The impact
of cartseat use in shopping carts and parental monitoring. Accident Analysis
and Prevention, 22(6), 531-542.
Hertzog, M. A. (2008). Considerations in determining sample size for pilot studies.
Research in Nursing & Health, 31(2), 180-191.
Hilton, A., & Skrutkowski, M. (2002). Translating instruments into other languages:
Development and testing process. Cancer Nursing, 25(1), 1-7.
Hjern, A., Ringbäck-Weitoft, G., & Andersson, R. (2001). Socio-demographic risk
factors for home-type injuries in Swedish infants and toddlers.
Acta paediatrica, 90(1), 61-68.
Hockenberry, M. J., & Wilson, D. (2007). Wong’s nursing care of infants and
children (8th
ed.). St. Louis, Missouri: Elservier.
Hooper, R., Coggan, C. A., & Adams, B. (2003). Injury prevention attitudes and
awearness in New Zealand. Injury Prevention, 9(1), 42-47.
Hutchings, H., Barnes, P. M., Maddocks, A., Lyons, R., & James-Ellison, M. Y.
(2010). Burns in young children: A retrospective matched cohort study of
health and developmental outcomes. Child: Care, Health and Development,
36(6), 787-794.
Johnston, B. D., Britt, J., D'Ambrosio, L., Mueller, B. A., & Rivara, F. P. (2000).
A preschool program for safety and injury prevention delivered by home
visitors. Injury Prevention, 6(4), 305-309.

97
Jordaan, E. R., Atkins, S., van Niekerk, A., & Seedat, M. (2005). The development of
an instrument measuring unintentional injuries in young children in low-
income settings to serve as an evaluation tool for a childhood home injury
prevention program. Journal of Safety Research, 36(3), 269-280.
Jordan, E. A., Duggan, A. K., & Hardy, J. B. (1993). Injuries in children of adolescent
mothers: Home safety education associated with decreased injury risk.
Pediatrics, 91(2), 481-487.
Kanchan, T., Menezes, R. G., & Monteiro, F. N. (2009). Fatal unintentional injuries
among young children - a hospital based retrospective analysis. Journal of
Forensic and Legal Medicine, 16(6), 307-311.
Kendrick, D., Watson, M., Mulvaney, C., & Burton, P. (2005). How useful are home
safety behaviors for predicting childhood injury? A cohort study. Health
Education Research, 20(6), 709-718.
Kleinedler, S. R., & Spitz, S. I. (Eds.). (2005). Webster's II new college dictionary.
New York: Houghton Miffin.
Koulouglioti, C., Cole, R., & Kitzman, H. (2009). The role of children's routines of
daily living, supervision, and maternal fatigue in preschool children's injury
risk. Research in Nursing & Health, 32(5), 517-529.
Laosee, O. C., Gilchrist, J., & Rudd, R. A. (2012). Drowning-United States,
2005-2009. Morbidity and Mortality Weekly Report, 61(19), 344-347.
Landen, M. G., Bauer, U., & Kohn, M. (2003). Inadequate supervision as a cause of
injury deaths among young children in Alaska and Louisiana. Pediatrics,
111(2), 328-331.
Laursen, B., & Nielsen, J. W. (2008). Influence of sociodemographic factors on the
risk of unintentional childhood home injuries. European Journal of Public
Health, 18(4), 366-370.
LeBlanc, J. C., Pless, I. B., King, W. J., Bawden, H., Bernard-Bonnin. A-C.,
Klassen, T., & Tenenbein, M. (2006). Home safety measures and the risk of
unintentional injury among young children: A multicentre case-control
study. Canadian Medical Association Journal, 175(8), 883-887.
98
Lewis, T., DiLillo, D., & Peterson, L. (2004). Parental beliefs regarding
developmental Benefits of childhood injuries. American Journal of Health
Behavior, 28(Supplement 1), S61-S68.
Linnan, M., Giersing, M., Cox, R., Linnan, H., Williams, M. H., Voumard, C., &
Hatfield, R. (2007). Child mortality and injury in Asia: An overview,
innocenti working paper 2007-04, special series on child injury no. 1.
Florence: UNICEF Innocenti Research Centre.
Lynn, M. R. (1986). Determination and quantification of content validity. Nursing
Research, 35(6), 382-386.
Meyers, L. S., Gamst, G., & Guarino, A. J. (2006). Applied multivariate research:
Design and interpretation. London: SAGE Publications.
Ministry of Public Health [MOPH] & Ministry of Social Development and Human
Security [MSDHS], Thailand. (2008). Country report Thailand, the 6th
ASEAN & Japan high level officials meeting on caring societies: “Healthy
next generation” under the tight collaboration between health and of social
welfare. Retrieved from http://www.mhlw.go.jp/bunya/.../asean//…/h20_
thailand.pdf
Morrongiello, B. A. (2005). Caregiver supervision and child-injury risk: I. Issues in
defining and measuring supervision; II. Findings and directions for future
research. Journal of Pediatric Psychology, 30(7), 536-552.
Morrongiello, B. A., & Corbett, M. (2006). The parent supervision attributes profile
questionnaire: A measure of supervision relevant to children’s risk of
unintentional injury. Injury Prevention, 12(1), 19-23.
Morrongiello, B. A., Corbett, M., & Brison, R. J. (2009). Identifying predictors of
medically-attended injuries to young children: do child or parent behavioral
attributes matter? Injury Prevention, 15(4), 220-225.
Morrongiello, B. A., Corbett, M., McCourt, M., & Johnston, N. (2006 a).
Understanding unintentional injury-risk in young children I. The nature and
scope of caregiver supervision of children at home. Journal of Pediatric
Psychology, 31(6), 529-539.

99
Morrongiello, B. A., Corbett, M., McCourt, M., & Johnston, N. (2006 b).
Understanding unintentional injury risk in young children II.
The contribution of caregiver supervision, child attributes, and parent
attributes. Journal of Pediatric Psychology, 31(6), 540-551.
Morrongiello, B. A., Corbett, M. R., & Kane, A. (2011). A measure that relates to
Elementary school children’s risk of injury: The supervision attributes and
Risk-taking questionnaire (SARTQ). Injury Prevention, 17(3), 189-194.
Morrongiello, B. A., & Dawber, T. (1998). Toddlers' and mothers' behaviors in an
injury-risk situation: Implications or sex differences in childhood injuries.
Journal of Applied Developmental Psychology, 19(4), 625-639.
Morrongiello, B. A., & Dawber, T. (1999). Parental influences on toddlers’ injury-risk
behaviors: Are son and daughters socialized differently?. Journal of Applied
Developmental Psychology, 20(2), 227-251.
Morrongiello, B. A., & Hogg, K. (2004). Mothers’ reactions to children misbehaving
in ways that can lead to Injury: Implications for gender differences in
children’s risk taking and injuries. Sex Role, 50(1-2), 103-117.
Morrongiello, B. A., & House, K. (2004). Measuring parent attributes and supervision
behaviors relevant to child injury risk: Examining the usefulness of
questionnaire measures. Injury Prevention, 10(2), 114-118.
Morrongiello, B. A., Klemencic, N., & Corbett, M. (2008). Interactions between child
behavioral patterns and parent supervision: Implications for children’s risk
of unintentional injury. Child Development, 79(3), 627-638.
Morrongiello, B. A., & Major, K. (2002). Influence of safety gear on parental
perceptions of injury risk and tolerance for children’s risk taking. Injury
Prevention, 8(1), 27-31.
Morrongiello, B. A., Ondejko, L., & Littlejohn, A. (2004 a). Understanding toddlers'
in-home injuries: I. Context, correlates, and determinants. Journal of
Pediatric Psychology, 29(6), 415-431.
Morrongiello, B. A., Ondejko, L., & Littlejohn, A. (2004 b). Understanding toddlers’
in-home injuries: II. Examining parental strategies, and their efficacy, for
managing child injury risk. Journal of Pediatric Psychology, 29(6), 433-446.

100
Morrongiello, B. A., & Rennie, H. (1998). Why do boys engage in more risk taking
than girls? The role of attributions, beliefs, and risk appraisals. Journal of
Pediatric Psychology, 23(1), 33-43.
Morrongiello, B. A., & Schwebel, D. C. (2008). Gaps in childhood injury research
and prevention: What can developmental scientists contribute?. Child
Development Perspectives, 2(2), 78-84.
Morrongiello, B. A., & Schell, S. L. (2009). Child injury: The role of supervision in
prevention. American Journal of Lifestyle Medicine, 4(1), 65-74.
Morrongiello, B. A., Walpole, B., & McArthur, B. A. (2009). Brief report: Young
children’s risk of unintentional Injury: A comparison of mothers’ and
fathers’ supervision beliefs and reported practices. Journal of Pediatric
Psychology, 34(10), 1063-1068.
Munro, S. A., van Niekerk, A., & Seedat, M. (2006). Childhood unintentional
injuries: The perceived impact of the environment, lack of supervision and
child characteristics. Child: Care, Health and Development, 32(3), 269-279.
Nakahara, S., & Ichikawa, M. (2010). Care giver supervision and child injuries:
consideration of different contexts when translating knowledge into practice.
Injury Prevention, 16(5), 293-295.
Nansel, T. R., Weaver, N. L., Jacobsen, H. A., Glasheen, C., & Kreuter, M. W.
(2008). Preventing unintentional pediatric injuries: A tailored intervention
for parents and providers. Health Education Research, 23(4), 656-669.
National Injury Surveillance, Ministry of Public Health [MOPH], Thailand. (2008).
Child injury prevention in the South-East Asia Region. New Deihi: World
Health Organization, Regional Office for South-East Asia. Retrieved from
http://www.who.int/violence_injury_ prevention/child/injury/world report/
CIP_SEARO.pdf
Office of Promotion and Protection of Children, Youth, the Elderly, and Vulnerable
Groups. (2007). A World Fit for Children. Bangkok: Office of Promotion
and Protection of Children, Youth, the Elderly, and Vulnerable Groups.
Ordoñana, J. R., Caspi, A., & Moffitt, T. E. (2008). Unintentional injuries in a twin
study of preschool children: Environmental, not genetic, risk factors.
Journal of Pediatric Psychology, 33(2), 185-194.

101
Patel, B., Groom, L., Prasad, V., & Kendrick, D. (2008). Parental poison prevention
practices and their relationship with perceived toxicity: Cross-sectional
study. Injury Prevention, 14(6), 389-395.
Peterson, L., Ewigman, B., & Kivlahan, C. (1993). Judgments regarding appropriate
child supervision to prevent injury: The role of environmental risk and child
age. Child Development, 64(3), 934-950.
Peterson, L., Farmer, J., & Mori, L. (1987). Process analysis of injury situations:
A complement to epidemiology methods. Journal of Social Issues, 43(2),
33-44.
Phelan, K. J., Khoury, J., Xu, Y., & Lanphear, B. (2009). Validation of a HOME
injury survey. Injury Prevention, 15(5), 300-306.
Phelan, K. J., Khoury, J., Xu, Y., Liddy, S., Hornung, R., & Lanphear, B. P. (2011).
A randomized controlled trial of home injury hazard reduction. Archives of
Pediatric & Adolescent Medicine, 165(4), 339-345.
Phuphaibul, R., Tachachhong, A., Kongsuktrakul, C., & Ooon-sawai, J. (2002).
Family developmental tasks in childrearing families: From infancy to
adolescence. The Journal of Faculty of Nursing Burapha University, 10(1),
1-14.
Pichayapinyo, P., Pawwatana, A., & Thongvichaen, S. (2008). Parenting styles,
Emotional intelligence, and Intelligence quotients in Thai school-aged
children in Tukdang community, Bangkok Metropolis. Journal of Public
Health, 38(1), 59-70.
Plitapolkarnpim, A. (n.d.). Home Observation Checklist. Bangkok: Child Safety
Promotion and Injury Prevention Research Center.
Polit, D. F., & Beck, C. T. (2012). Nursing research: Generating and assessing
evidence for nursing practice (9th
ed.). Philadelphia: Wolters Kluwer Health
Lippincott Williams & Wilkins.
Pooltawee, S. (2000). Risk factors of unintentional injury at home in children one to
four years of age. Master’s thesis, Department of Epidemiology, Faculty of
Graduate Studies, Mahidol University.

102
Posner, J. C., Hawkins, L. A., Garcia-Espana, F., & Durbin, D. R. (2004).
A randomized, clinical trial of a home safety intervention based in an
emergency department setting. Pediatrics, 113(6), 1603-1608.
Puckett, M. B., & Black, J. K. (2005). The young child: Development from prebirth
through age eight (4th
ed.). New Jersey: Pearson Merrill Prentice Hall.
Putnam, S. P., Gartstein, M. A., & Rothbart, M. K. (2006). Measurement of fine-
grained aspects of toddler temperament: The early childhood behavior
questionnaire. Infant Behavior & Development, 29(3), 386-401.
Ratchathewee Institute. (2011). The general information of community development
and social welfare. Bangkok: Ratchathewee Institute.
Rowe, R., & Maughan, B. (2009). The role of risk-taking and errors in children's
liability to unintentional injury. Accident Analysis and Prevention, 41(4),
670-675.
Runyan, C. W. (2003). Introduction: Back to the future-revisiting Haddon’s
conceptualization of injury epidemiology and prevention. Epidemiologic
Reviews, 25(1), 60-64.
Runyan, C. W., Casteel, C., Perkis, D., Black, C., Marshall, S. W., Johnson, R. M.,
Coyne-Beasley, T., Waller, A. E., & Viswanathan, S. (2005). Unintentional
injuries in the home in the United States Part I: Mortality. American Journal
of Preventive Medicine, 28(1), 73-79.
Safe Kids USA. (2011). Unintentional injury risk for children. Retrieved from
http://www.safekids.org/assets/docs/ourwork/research/2011-high-risk-fact-
sheet.pdf
Saluja, G., Brenner, R., Morrongiello, B. A., Haynie, D., Rivera, M., & Cheng, T. L.
(2004). The role of supervision in child injury risk: Definition, conceptual
and measurement issues. Injury Control and Safety Promotion, 11(1), 17-22.
Sangsupawanich, P. (n.d.). General health status. In Report on the fourth Thai citizen
health survey by physical examination, 2551-2552 (B.C.) (pp. 81-88).
Nonthaburi: NHESO.
Schumacker, R. E., & Lomax, R. G. (2010). A beginner’s guide to structural equation
modeling (3rd
ed.). New York: Routledge Taylor & Francis Group.

103
Schwebel, D. C. (2004). Temperamental risk factors for children’s unintentional
injury: The role of impulsivity and inhibitory control. Personality and
Individual Differences, 37(3), 567-578.
Schwebel, D. C., & Barton, B. K. (2005). Contributions of multiple risk factors to
child injury. Journal of Pediatric Psychology, 30(7), 553-561.
Schwebel, D. C., Brezausek, C. M., Ramey, S. L., & Ramey, C. T. (2004).
Interactions between child behavior patterns and parenting: Implications for
children's unintentional injury risk. Journal of Pediatric Psychology, 29(2),
93-104.
Schwebel, D. C., & Gaines, J. (2007). Pediatric unintentional injury: Behavioral risk
factors and implications for prevention. Journal of Developmental &
Behavioral Pediatrics, 28(3), 245-254.
Schwebel, D. C., & Kendrick, D. (2009). Caregiver supervision and injury risk for
young children: Time to re-examine the issue. Injury Prevention, 15(4),
217-219.
Shenassa, E. D., Stubbendick, A., & Brown, M. J. (2004). Social disparities in
housing and related pediatric injury: A multilevel study. American Journal
of Public Health, 94(4), 633-639.
Schumacker, R. E., & Lomax, R. G. (2010). A beginner’s guide to structural equation
modeling (3ed
ed.). New York: Taylor and Francis Group.
Simpson, J. C., Turnbull, B. L., Ardagh, M., & Richardson, S. (2009). Child home
injury prevention: Understanding the context of unintentional injuries to
preschool children. International Journal of Injury Control and Safety
Promotion, 16(3), 159-167.
Sirisamutr, T. (2008). Prevalence and risk factors of unintentional home injury in
preschool children, Roi et province. Master’s thesis, Department of Public
Health, Faculty of Graduate Studies, Mahidol University.
Sitthi-amorn, C., Chaipayom, O., Udomprasertgul, V., Linnan, M., Dunn, T.,
Beck, L., Cardenas, V., Irvine, K., Forsgate, D., & Cox, R. (2006).
Child injury in Thailand: A report on the Thai national injury survey.
Bangkok: Chulalongkorn University.
104
Sorenson, S. B. (2011). Gender disparities in injury mortality: Consistent, persistent,
and larger than you'd think. American Journal of Public Health, 101(S1),
S353-S358.
Sousa, V. D., Zauszniewski, J. A., Mendes, I. A., & Zanetti, M. L. (2005). Cross-
cultural equivalence and psychometric properties of the Portuguese version
of the Depressive Cognition Scale. Journal of Nursing Measurement, 13(2),
87-99.
Speltz, M. L., Gonzales, N., Sulzbacher, S., & Quan, L. (1990). Assessment of injury
risk in young children: A preliminary study of the injury behavior checklist.
Journal of Pediatric Psychology, 15(3), 373-383.
Tabachnick, B. G., & Fidell, L. S. (2007). Using multivariate statistics pearson
international edition (2nd
ed.). Boston: Pearson/Allyn & Bacon.
Tertinger, D. A., Greene, B. F., & Lutzker, J. R. (1984). Home safety: Development
and validation of one component of an ecobehavioral treatment program for
abused and neglected children. Journal of Applied Behavior Analysis, 17(2),
159-174.
Thomas, A., & Chess, S. (1977). Temperament and development. New York:
Brunner/Mazel.
Thomasgard, M., Shonkoff, J. P., Metz, W. P., & Edelbrock, C. (1995). Parent-child
relationship disorders. Part II. The vulnerable child syndrome and its relation
to parental overprotection. Journal of Developmental and Behavioral
Pediatrics, 16(4), 251-256.
Tiempathom, S. (1994). Factors associated with home accidents in preschool
children of Bangbuathong district Nonthaburi province. Master’s thesis,
Department of Public Health, Graduate School, Mahidol University.
Towner, E., & Scott, I (2008). Child injuries in context. In M. Peden, K. Oyegbite, J.
Ozanne-Smith, A. A. Hyder, C. Branche, AKH. F. Rahman, F. Rivara, & K.
Bartolomeos (Eds.), World Report on Child Injury Prevention (pp. 1-30).
Geneva: WHO Press.

105
Tymchuk, A. J., Lang, C. M., Sewards, S. E., Lieberman, S., & Koo, S. (2003).
Developmental and validation of the illustrated version of the home
inventory for dangers and safety precautions: Continuing to address learning
needs of parents in injury prevention. Journal of Family Violence, 18(4),
241-252.
United Nations International Children's Emergency Fund [UNICEF], Thailand
(2014). Statistic. Retrieved from http://www.unicef.org/infobycountry/
Thailand_statistics.html.
Valsiner, J., & Lightfoot, C. (1987). Process structure of parent-child-environment
relations and the prevention of children's injuries. Journal of Social Issues,
43(2), 61-72.
van Aken, C., Junger, M., Verhoeven, M., van Aken, M. A. G., & Dekovic, M.
(2007). Externalizing behaviors and minor unintentional injuries in toddlers:
Common risk factor?. Journal of Pediatric Psychology, 32(2), 230-244.
Watson, M., Kendrick, D., Coupland, C., Woods, A., Futers, D., & Robinson, J.
(2004). Providing child safety equipment to prevent injuries: Randomised
controlled trial. BMJ, 330(7484), 1-6.
Williams, P., Piamjariyakul, U., Williams, A., Hornboonherm, P., Meena, P.,
Channukool, N., Singhala, K., Hosakulthai, M., Klunkarndee, K.,
Mahasiripun, T., Pusatum, P., Tuebpo, C., Pranprai, P., & Chamusri, S.
(2003). Thai mothers and children and the home observation for
measurement of the environment (home inventory): Pilot study.
International Journal of Nursing Studies, 40(3), 249-258.
Wortel, E., De Geus, G. H., & Kok, G. (1995). Behavioral determinants of mothers’
safety measures to prevent injuries of preschool children. Scandinavian
Journal of Psychology, 36(3), 306-322.

APPENDICES

107
APPENDIX 1
Institutional Review Board

108

109
APPENDIX 2
Participant information and Consent form

110
เอกสารชแจงผเขารวมการวจย
การวจยเรอง ปจจยท ำนำยกำรบำดเจบแบบไมตงใจทบำนในเดกวยหดเดน: กำรทดสอบเชง ประจกษของแบบจ ำลองเชงสำเหต รหสจรยธรรมการวจย 03 – 11 - 2556 ชอผวจย นำงจรำวรรณ กลอมเมฆ กำรวจยครงนท ำขน เพอทดสอบแบบจ ำลองเชงสำเหตกำรบำดเจบแบบไมตงใจกบบตรของทำนทมอำยระหวำง 1 ถง 3 ป ทบำน ซงทำนไดรบเชญใหเขำรวมกำรวจยครงน เนองจำกทำนเปนผทมคณสมบตตรงกบกำรศกษำครงน คอ ทำนอำยมำกกวำ 19 ป เลยงบตรอำยระหวำง 1 ถง 3 ปตอเนองมำอยำงนอย 6 เดอน บตรมสขภำพแขงแรงสมบรณ อำศยอยในชมชนเขตรำชเทวมำอยำงนอย 6 เดอน อำนและเขยนภำษำไทยได และสมครใจเขำรวมงำนวจย ซงกำรวจยนตองกำรมำรดำเขำรวมวจย จ ำนวน 250 ทำน ระยะเวลำทใชในกำรเกบขอมลในกำรท ำวจยครงนอยระหวำง เดอน มกรำคม ถง เมษำยน พ.ศ. 2557 เมอทำนเขำรวมกำรวจยแลว สงททำนจะตองปฏบตคอ ตอบแบบสอบถำมตำมควำมเปนจรงดวยตวทำนเอง หรอใหผวจยอำนใหฟงในกรณททำนมปญหำเรองสำยตำ เชน ตำเจบ ตำพรำมว แบบสอบถำมมจ ำนวน 4 ชด คอ 1) ขอมลสวนตวของบตรและของทำน เชน เพศ อำยของบตร อำชพ ระดบกำรศกษำ รำยไดของทำน เปนตน 2) พฤตกรรมของบตรทอำจเสยงตอกำรบำดเจบ เชน กระโดดจำกโตะ เกำอ หกลม เลนสงของมคม เปนตน 3) ลกษณะกำรเลยงดบตรของทำน เชน วธกำรปกปองบตรจำกกำรบำดเจบ กำรดแลอยำงใกลชดขณะบตรท ำกจกรรมตำงๆ กำรปลอยใหบตรเรยนรประสบกำรณกำรกำรบำดเจบ และควำมเชอเรองโชคชะตำของทำนตอกำรบำดเจบของบตร และ4) โอกำสเกดกำรบำดเจบของบตรทงในและบรเวณรอบๆบำน ใชเวลำทงหมดประมำณ 30 นำท และผวจยขออนญำตสงเกตสงแวดลอมทกอใหเกดกำรบำดเจบส ำหรบบตรอำย 1 – 3 ป ทบำน โดยใชเวลำประมำณ 1 ชวโมง ประโยชนททำนจะไดรบคอ ทำนจะไดรบค ำแนะน ำในกำรจดสงแวดลอมทปลอดภย ใน และบรเวณรอบบำน และวธกำรเลยงบตรอำย 1 ถง 3 ป อยำงปลอดภย นอกจำกนผลกำรวจยครงน

111
ยงมประโยชนตอสงคมคอ สำมำรถน ำไปหำแนวทำงกำรปฏบตในกำรปองกนและลดกำรบำดเจบ แบบไมตงใจทบำนในเดกอำย 1 ถง 3 ป และกำรวจยนไมมควำมเสยงใดๆ กำรเขำรวมกำรวจยของทำนครงนเปนไปดวยควำมสมครใจ ทำนมสทธปฏเสธกำรเขำรวม วจย หรอถอนตวออกจำกกำรวจยไดตลอดเวลำโดยไมมผลกระทบใดๆทงสน โดยไมตองแจงใหผวจย ทรำบลวงหนำ ผวจยจะเกบรกษำควำมเปนสวนตวของทำนและบตร โดยกำรใชรหสตวเลขแทนกำรระบ ชอ-สกล บำนเลขท และสงใดๆ ทอำจอำงองหรอทรำบไดวำขอมลนเปนของทำนและบตร ขอมลของทำนและบตรทเปนกระดำษแบบสอบถำมจะถกเกบอยำงมดชด และปลอดภยในแฟม ใสตเกบเอกสำร และลอกกญแจตลอดเวลำ ผวจยเทำนนทสำมำรถเปดตเอกสำรได ส ำหรบขอมลทเกบในคอมพวเตอรของผวจย จะถกใสรหสผำน และผวจยเทำนนทสำมำรถเขำถงขอมลนได ผวจยจะรำยงำนผลกำรวจยและกำรเผยแพรผลกำรวจยในภำพรวม โดยไมระบขอมลสวนตวทำนและบตร ดงนนผอำนงำนวจยนจะทรำบเฉพำะสำเหตกำรบำดเจบของเดกเทำนน สดทำยหลงจำกผลกำรวจยไดรบกำรตพมพในวำรสำรเรยบรอยแลว ขอมลทงหมดจะถกท ำลำย หำกทำนมปญหำหรอขอสงสยประกำรใด สำมำรถสอบถำมไดโดยตรงจำกผวจยในวนท ำกำรรวบรวมขอมล หรอสำมำรถตดตอสอบถำมเกยวกบกำรวจยครงนไดตลอดเวลำท จรำวรรณ กลอมเมฆ หมำยเลขโทรศพท 08-9816-7175 หรอท รศ. ดร.นจร ไชยมงคล อำจำรยทปรกษำหลก หมำยเลขโทรศพท 038-102863 นำงจรำวรรณ กลอมเมฆ
ผวจย หากทานไดรบการปฏบตทไมตรงตามทไดระบไวในเอกสารชแจงน ทำนจะสำมำรถแจงใหประธำนคณะกรรมกำรพจำรณำจรยธรรมฯ ทรำบไดท เลขำนกำรคณะกรรมกำรจรยธรรมฯ ฝำยวจย คณะพยำบำลศำสตร มหำวทยำลยบรพำ โทร. 038-102823
ในเอกสารนอาจมขอความททานอานแลวยงไมเขาใจ โปรดสอบถามผวจยหรอผแทนใหชวยอธบายจนกวาจะเขาใจด ทานอาจจะขอเอกสารนกลบไปทบานเพออานและท าความเขาใจ หรอปรกษาหารอกบญาตพนอง เพอนสนท แพทยประจ าตวของทาน หรอแพทยทานอน เพอชวยในการตดสนใจเขารวมการวจยครงนได

112
ใบยนยอมเขารวมการวจย ..........................................
หวขอวทยานพนธ ปจจยท ำนำยกำรบำดเจบแบบไมตงใจทบำนในเดกวยหดเดน: กำรทดสอบเชงประจกษของแบบจ ำลองเชงสำเหต วนใหค ำยนยอม วนท …………… เดอน ………………… พ.ศ. ………………. กอนทจะลงนำมในใบยนยอมเขำรวมกำรวจยน ขำพเจำไดรบกำรอธบำยจำกผวจยถงวตถประสงคของกำรวจย วธกำรวจย ประโยชนทจะเกดขนจำกกำรวจยอยำงละเอยด และมควำมเขำใจดแลว ขำพเจำยนดเขำรวมโครงกำรวจยนดวยควำมสมครใจ และขำพเจำมสทธทจะบอกเลกกำรเขำรวมในโครงกำร วจยน เมอใดกได และกำรบอกเลกกำรเขำรวมกำรวจยนจะไมมผลกระทบใดๆตอขำพเจำ ผวจยรบรองวำจะตอบค ำถำมตำงๆ ทขำพเจำสงสยดวยควำมเตมใจ ไมปดบง ซอนเรน จนขำพเจำพอใจ ขอมลเฉพำะเกยวกบตวขำพเจำจะถกเกบเปนควำมลบและจะเปดเผยในภำพรวมทเปนกำรสรปผลกำรวจย ขำพเจำไดอำนขอควำมขำงตนแลว และมควำมเขำใจดทกประกำร และไดลงนำมในใบยนยอมนดวยควำมเตมใจ ลงนำม……………………………………………ผยนยอม (…………………………………………) ลงนำม……………………………………………พยำน (…………………………………………) ลงนำม……………………………………………ผวจย (…………………………………………)

113
APPENDIX 3
Questionnaires

114
ชอชมชน ……………………..
แบบสอบถามส าหรบมารดา เลขท ………….
วนท……….เดอน…………….พ.ศ…………
แบบสอบถามท 1 ขอมลสวนตวของบตรและของมารดา ค าชแจง: กรณำเขยนรำยละเอยด หรอ กำเครองหมำย ลงในชอง ตำมควำมเปนจรงมำกทสด ขอมลสวนตวของบตร 1. เกดวนท …………. เดอน …….…………………. พ.ศ. .................. อำย ……………………... 2. เพศ 1. ผชำย 2. ผหญง 3. ล ำดบทเกด 1. คนแรก 2. คนท 2
3. คนท 3 4. มำกกวำคนท 3 ระบ ........................... 4. จ ำนวนเดกทอำศยอยในบำนเดยวกนทมอำยนอยกวำ 15 ป 1. หนงคน 2. สองคน 3. มำกกวำสองคนระบ .................................................................................. ขอมลสวนตวของมารดา 5. อำย ......................... ป 6. สถำนภำพสมรส 1. อยดวยกน 2. หยำ/แยกกนอย 3. หมำย 7. ระดบกำรศกษำ 1. นอยกวำประถมศกษำปท 6 2. ประถมศกษำปท 6 3. มธยมศกษำตอนตน 4. มธยมศกษำตอนปลำย/ ปวช. 5. ปวส/ ประกำศนยบตร 6. ปรญญำตร/ หรอสงกวำ 8. อำชพ 1. ไมไดท ำงำน/ แมบำน 2. คำขำย 3. รบจำง 4. รบรำชกำร 5. ธรกจสวนตว 6. อนๆระบ ............................... 9. รำยไดครอบครว 1. ไมเพยงพอ 2. เพยงพอแตไมมเหลอเกบ 3. เพยงพอและมเหลอเกบ

115
แบบสอบถามท 2 พฤตกรรมเสยงตอการบาดเจบของบตร (23 ขอ) ค าชแจง: กรณำใสเครองหมำย ในชองททำนคดวำบตรของทำนมความถของพฤตกรรมเสยงตอการบาดเจบในและบรเวณรอบบานมากนอยเพยงใดในชวง 6 เดอนทผานมา กรณำเลอกค ำตอบในชองทตรงกบควำมเปนจรงมำกทสดเพยงค ำตอบเดยวในแตละขอ โดยใหคะแนน ดงน 5 หมำยถง มพฤตกรรมเสยงบอยมำก (มำกกวำสปดำหละครง) 4 หมำยถง มพฤตกรรมเสยงบอย (ประมำณสปดำหละครง) 3 หมำยถง มพฤตกรรมเสยงบำงครง (ประมำณเดอนละครง) 2 หมำยถง มพฤตกรรมเสยงนอย (ประมำณ 1 ถง 2 ครง) 1 หมำยถง ไมมพฤตกรรมเสยง
ขอท ขอความ พฤตกรรมเสยงตอการบาดเจบของบตร
บอยมาก (5)
บอย (4)
บางครง (3)
นอย (2)
ไมม (1)
1 วงออกไปท… 2 กระโดดจำกท… 3 กระโดดลงจำกบนได… . . .
21 หยบจบของรอน หรอเลนใกล เตำ … 22 เลนใกล หรอปนบอน ำ อำงน ำ… 23 แกลงหรอแหยสตว เชน สนขหรอ
แมว…

116
แบบสอบถามท 3 คณลกษณะการดแลบตรของมารดาตอการบาดเจบ (29 ขอ) ค าชแจง: แบบสอบถำมนมวตถประสงคเพอ ตองกำรเรยนรพฤตกรรม ทศนคต ควำมเชอในกำรเลยงบตรของมำรดำตอกำรบำดเจบ ใน 4 คณลกษณะ คอ 1) กำรปกปองของมำรดำ 2) กำรเฝำระวง/ กำรดแลอยำงใกลชดของมำรดำ 3) กำรอนญำตหรอรอใหบตรเรยนรประสบกำรณกำรท ำกจกรรมตำงๆ หรอกำรบำดเจบของมำรดำ และ 4) ควำมเชอเรองโชคชะตำของมำรดำตอกำรบำดเจบของบตร กรณำอำนขอควำมแตละขอควำมอยำงละเอยดแลวพจำรณำวำแตละขอควำมขำงลำงนตรงกบควำมเปนจรงมำกทสดของทำนและใสเครองหมำย เพยงค ำตอบเดยวในชองของแตละขอ โดยใหคะแนน ดงน 5 หมำยถง เปนจรงมำกทสด 4 หมำยถง เปนจรงมำก 3 หมำยถง เปนจรงครงหนง 2 หมำยถง เปนจรงบำงครง 1 หมำยถง ไมเปนจรง
ขอท ขอความ
การปกปองของมารดาตอการบาดเจบของบตร
เปนจรง มากทสด
(5)
เปนจรงมาก (4)
เปนจรง ครงหนง
(3)
เปนจรงบางครง
(2)
ไมเปน จรง (1)
1 ฉนใหลกอยหำง… 2 ฉนเฝำดลก… 3 ฉนรสกวำ… 4 ฉนเตอนลกเกยวกบ… 5 ฉนสอนลกท ำกจกรรม… 6 ฉนรสกกลววำ… 7 ฉนรสกถงควำมรบผดชอบ… 8 ฉนนกถงเกยวกบอนตรำย… 9 ฉนหำมลกเลนเกมสทรนแรง...

117
ขอท ขอความ
การปกปองของมารดาตอการบาดเจบของบตร
เปนจรง มากทสด
(5)
เปนจรงมาก (4)
เปนจรง ครงหนง
(3)
เปนจรงบางครง
(2)
ไมเปนจรง (1)
1 ฉนอยใกลๆ ทจะชวยลก… 2 ฉนเฝำดลกอยำงใกลชด… 3 ฉนแนใจวำฉนรวำลก… 4 ฉนไวใจใหลกเลนคนเดยว… 5 ฉนอยใกลชดลก… 6 ฉนเชอวำลกสำมำรถ… 7 ฉนปวนเปยน… 8 ฉนอยใกลชดลกมำก… 9 ฉนแนใจวำลก…
ขอท ขอความ
การอนญาตหรอรอใหบตรเรยนรประสบการณ การท ากจกรรมตางๆ หรอการบาดเจบของมารดา
เปนจรง มากทสด
(5)
เปนจรงมาก (4)
เปนจรง ครงหนง
(3)
เปนจรงบางครง
(2)
ไมเปนจรง (1)
1 ฉนปลอยใหลกเรยนร… 2 ฉนใหลกบำดเจบ… 3 ฉนเฝำดลกท ำสงตำงๆ… 4 ฉนปลอยใหลก… 5 ฉนใหลกตดสนใจ… 6 ฉนใหลกลองท ำสงตำงๆ… 7 ฉนใหลกท ำสงตำงๆ… 8 ฉนสงเสรมใหลก…

118
ขอท ขอความ
ความเชอเรองโชคชะตาของมารดาตอการบาดเจบของบตร
เปนจรง มากทสด
(5)
เปนจรงมาก (4)
เปนจรง ครงหนง
(3)
เปนจรงบางครง
(2)
ไมเปนจรง (1)
1 กำรทลกไดรบบำดเจบ… 2 เมอลกไดรบบำดเจบ… 3 กำรดดวงท ำนำยโชคชะตำ…

119
แบบสอบถามท 4 การบาดเจบแบบไมตงใจทบานส าหรบเดกวยหดเดน (14 ขอ) ค าชแจง: กรณำใสเครองหมำย ในชองททำนคดวำบตรของทำนมโอกาสเกดการบาดเจบในและบรเวณรอบบานไดมากนอยเพยงใดในชวง 6 เดอนทผานมา กรณำเลอกค ำตอบในชองทตรงกบควำมเปนจรงมำกทสดเพยงค ำตอบเดยวในแตละขอ โดยใหคะแนน ดงน 4 หมำยถง มโอกำสเกดบอยทสด 3 หมำยถง มโอกำสเกดบอย 2 หมำยถง มโอกำสเกดบำงครง 1 หมำยถง มโอกำสเกดนอย 0 หมำยถง ไมมโอกำสเกด
ขอท ขอความ โอกาสเกดการบาดเจบ
บอยทสด (4)
บอย (3)
บางครง (2)
นอย (1)
ไมม (0)
1 พลดตก หกลม 2 ไฟไหม น ำรอนลวก 3 ตดในชอง หรอวสด… . . .
12 สตวกด เชน สนข… 13 แมลงกด ตอย เชน… 14 เดกอนท ำรำยรำงกำย…

120
แบบสงเกตสงทกอใหเกดการบาดเจบในและบรเวณรอบบานของบตร ค าชแจง: แบบสงเกตนผวจยเปนผส ำรวจลกษณะบำนของเดกทอำศยอยกบมำรดำอยำงนอย 6 เดอนทผำนมำ โดยผวจยจะใสเครองหมำย ในชอง หนำขอควำมหรอระบสงทพบจรงตำมขอควำมในแบบสงเกตน ซงแบบสงเกตนแบงเปน 2 ตอน คอ ตอนท 1 แบบสงเกตลกษณะบำนทวไป ตอนท 2 แบบสงเกตสงอนตรำยในและบรเวณรอบบำน 4.1 แบบสงเกตลกษณะบานทวไป (10 ขอ) 1. ชนดทอยอำศย 1. บำนชนเดยว 2. บำนสองชน 3. หอง/ แฟลต 4. อนๆ ระบ ........................................... 2. ในบำนประกอบดวยหองอะไรบำง 1. หองครว 2. หองน ำ 3. หองนอน 4. หองนงเลน 5. หองเกบของ 6. หองรวม 7. อนๆระบ ................................................................................................................ . . . 10. ทจอดรถ 1. ม 1.1 หนำบำน 1.2 ในบำน 1.3 ทจอดรถประจ ำชมชน 1.4 อนๆ ระบ ............................
0. ไมม

121
4.2 แบบสงเกตสงอนตรายในและบรเวณรอบบาน (51 ขอ) ของมคม 1. มองเหนสงของมคมบนเคำเตอร ชนวำงของ โตะ หรออนๆ (ไมรวมในกลองเกบมด) 1. ม ระบบรเวณ ………………………………........................................................ 0. ไมม 2. มองเหนสงของมคมวำงบนโตะ ต ชนวำงของ หรอทอนๆทมความสงจากพนนอยกวา 1 เมตร 1. ม ระบบรเวณ ………………………………........................................................ 0. ไมม 3. มสงของมคมอยในลนชก ตเกบของ ตเสอผำ หรอทอนๆโดยทลอคเสยหรอไมมทลอคและอย
สงจากพนนอยกวา 1 เมตร 1. ม ระบบรเวณ ………………………………...................................................... 0. ไมม . . . 50. ปนอยในกลองหรอตทลอคไว 1. ไมใช 0 ใช 51. กระสนอยในกลองหรอตทลอคอย 1. ไมใช 0 ใช

122
APPENDIX 4
Permission instruments

123
124

125

126

127
APPENDIX 5
Content validators

128
Content validators
1. Associate Professor Dr. Adisak Plitponkarnpim, MD
Department of Pediatrics, Faculty of Medicine, Ramathibodi Hospital,
Mahidol University
2. Associate Professor Dr. Wannee Deoisres
Faculty of Nursing, Burapha University
3. Associate Professor Dr. Ratsiri Thato
Faculty of Nursing, Chulalongkorn University
4. Assistant Professor Dr. Renu Pookboonmee
Department of Nursing, Faculty of Medicine, Ramathibodi Hospital,
Mahidol University

129
APPENDIX 6
Additional analyses

130
Table 11 Standardized scores of continuous variables for testing univariate outliers
(n = 250)
ID Ztem Zhazards Zpro Zsuper Ztol Zfate Zinjury
1 -1.08631 .46545 -.34527 .27079 -1.66901 -.45297 -.81857
2 .36302 .70389 1.10369 -.47725 .42548 1.96503 -.09160
3 -.39615 -.72679 .89670 -1.78632 -1.96823 -.85597 -1.18206
4 .57007 -.48834 -.96625 .64481 .12627 .35303 .45363
5 -.12009 .22700 -.34527 -.47725 -2.26744 -.04997 -.09160
6 2.15743 -.24989 .68970 -.47725 .87430 -.45297 1.54409
7 1.74334 -.24989 -.13827 .45780 .87430 2.36804 .99886
8 -1.01729 .70389 .27572 1.76687 .57509 -.85597 -1.36380
9 -.12009 -.24989 .89670 1.20584 -.32255 -.85597 -.81857
10 -.12009 -.72679 .48271 .45780 .57509 1.56203 -.45508
11 1.46727 .94234 -.13827 -1.97333 .27587 -.04997 1.90757
12 1.26023 -.24989 .68970 -.29024 .42548 -.85597 1.36234
13 -.74123 1.18079 .06872 1.57986 -.32255 -.85597 -.81857
14 .98416 -1.44213 .48271 -2.34735 1.62234 -.85597 -1.18206
15 -.18910 -.72679 .68970 -.29024 1.47273 2.77104 .63537
16 -1.29335 -1.44213 .06872 -.10323 .87430 .75603 -.27334
17 -.25812 1.18079 -.55226 -.47725 .27587 .35303 -.45508
18 -.46517 -.72679 -1.58723 -.47725 .87430 .35303 -.81857
19 -.46517 -.72679 -2.00122 -.10323 .27587 -.45297 -1.00031
20 .36302 -1.20368 .89670 -.29024 -.47216 -.85597 .09014
21 -.74123 .46545 -2.00122 -.10323 -.62177 .35303 .63537
22 -.87926 -.96523 .89670 .08378 .87430 -.85597 .27189
23 .36302 -.96523 .68970 .45780 -.77137 -.85597 -.27334
24 .57007 -1.20368 .68970 -1.78632 .57509 -.85597 -.45508
25 -.81024 -.24989 .48271 .45780 -.47216 -.45297 -1.18206
26 -1.08631 -1.20368 .89670 1.76687 -.32255 3.17404 -.81857
27 2.29546 -.48834 .89670 -.47725 -.32255 .75603 1.36234
28 -.05107 -.24989 .06872 1.95388 -1.51941 -.85597 -.63683
29 1.19121 1.41923 -.55226 .45780 -.02334 -.85597 .99886
30 2.43349 .46545 .89670 .08378 .12627 -.85597 1.54409
31 -1.77646 -.72679 -.96625 .27079 .27587 -.85597 -1.18206
32 .36302 -.96523 .89670 .83182 .42548 -.85597 .81712

131
Table 11 (continued)
ID Ztem Zhazards Zpro Zsuper Ztol Zfate Zinjury
33 -.12009 -.72679 .06872 -1.03828 .87430 .35303 .27189
34 -.53418 -.24989 .89670 1.39285 -2.26744 -.85597 .27189
35 .70810 .22700 .89670 .27079 1.77194 -.85597 -.45508
36 .70810 1.18079 -2.82919 -1.59931 -.32255 1.56203 1.90757
37 1.46727 -.72679 .27572 1.20584 -.92098 -.45297 .45363
38 -.46517 -.24989 1.10369 .45780 1.47273 1.56203 -1.36380
39 -1.36237 -.24989 .48271 -.85127 -1.07059 -.85597 -.45508
40 -.46517 -.72679 -.96625 -.29024 -.32255 -.04997 -.27334
41 .43204 -.24989 .48271 .45780 .72470 -.04997 -.45508
42 .63909 1.89613 .27572 -.29024 -.47216 -.04997 .27189
43 -1.63843 1.41923 .27572 .27079 1.02391 -.04997 -.63683
44 1.05318 .46545 .27572 .64481 .27587 -.85597 -.63683
45 1.19121 -.24989 .89670 2.14089 -.47216 -.85597 1.18060
46 1.67432 -.96523 -1.58723 -.29024 .42548 1.56203 2.08932
47 -1.29335 -.01145 -1.17324 1.01883 -.62177 -.85597 -.63683
48 -.18910 -1.91902 -1.58723 .83182 .12627 1.96503 -.27334
49 .91515 .22700 -1.38024 -.29024 1.32312 -.04997 4.99720*
50 -.81024 .22700 -.55226 -2.53436 -.02334 -.45297 -1.00031
51 .22499 1.18079 .48271 1.01883 1.17352 1.56203 .09014
52 -.39615 1.65768 .48271 .27079 -1.96823 -.45297 -.45508
53 .15598 1.89613 -1.58723 -1.97333 -.47216 -.85597 .99886
54 .08696 1.41923 1.31069 1.76687 -.62177 -.04997 -1.36380
55 -1.29335 1.65768 .48271 -.66426 1.02391 -.45297 -1.36380
56 .50105 -.24989 -.13827 -1.03828 -.47216 1.56203 -.09160
57 .98416 -.24989 -.34527 -.29024 1.17352 -.04997 1.90757
58 2.22645 .22700 .06872 -2.34735 1.62234 .75603 1.18060
59 -.67221 .22700 1.10369 .64481 .42548 -.85597 -1.00031
60 1.05318 -.96523 -.96625 -1.03828 -.47216 .75603 1.18060
61 .50105 -.48834 .48271 -.66426 -.47216 -.85597 .09014
62 -.18910 .70389 .89670 .83182 1.92155 1.56203 -.81857
63 -1.36237 .70389 .68970 .27079 -.32255 2.36804 -1.36380
64 -.32713 -.24989 -1.58723 -.29024 -1.22019 1.96503 -.09160
65 .36302 -.96523 -1.58723 -.10323 -.02334 -.85597 -.45508

132
Table 11 (continued)
ID Ztem Zhazards Zpro Zsuper Ztol Zfate Zinjury
66 .22499 1.18079 .48271 -.29024 .72470 2.36804 1.90757
67 -.60320 1.41923 -.55226 -1.03828 -.32255 -.04997 -.27334
68 1.81235 -.24989 1.31069 -.29024 -.92098 .75603 1.72583
69 .98416 -.48834 -1.58723 -1.22529 .12627 1.56203 1.72583
70 -.67221 .70389 -1.38024 .45780 -1.66901 -.04997 -.63683
71 .22499 1.65768 .89670 .27079 .12627 -.85597 -.27334
72 -1.29335 -.01145 .27572 1.20584 -1.51941 -.45297 -1.72728
73 -.67221 -.96523 1.10369 .83182 -.92098 -.85597 -.63683
74 -.74123 .70389 -2.41521 -1.03828 .42548 1.15903 -.27334
75 -.53418 -1.68057 1.31069 .45780 .87430 -.85597 -1.00031
76 2.08842 1.18079 .89670 .27079 1.47273 -.04997 .99886
77 .77712 1.18079 .27572 -2.90838 1.92155 -.85597 2.27106
78 .57007 -.48834 1.10369 1.20584 1.17352 -.85597 .27189
79 -1.15532 -1.91902 .48271 .45780 -.47216 -.45297 -1.00031
80 -.74123 .46545 -1.79422 .27079 .72470 -.85597 .63537
81 -.12009 -.96523 -.75925 -.66426 -.32255 -.85597 .27189
82 -.67221 -1.91902 1.31069 1.01883 -2.11783 -.85597 -.63683
83 -.46517 -.01145 -.55226 -1.03828 -.02334 -.85597 -.45508
84 -2.05253 -1.20368 1.31069 .45780 -2.56665 1.56203 -.81857
85 -1.84548 -1.44213 -5.10613* -.47725 -2.11783 -.45297 -.81857
86 .84613 .94234 1.10369 1.57986 .87430 .35303 -.45508
87 -.74123 -.48834 -.96625 .08378 -1.07059 .35303 -.27334
88 -.39615 -.48834 .48271 1.01883 1.77194 .35303 -.27334
89 -.53418 .94234 .27572 .45780 -1.51941 -.85597 -.63683
90 -1.29335 .70389 -1.38024 -.29024 -1.81862 -.85597 -1.18206
91 -1.15532 .46545 -.34527 .08378 -1.81862 -.85597 -.63683
92 -.94828 .70389 1.10369 .08378 -1.81862 -.04997 -1.36380
93 .36302 1.18079 1.31069 1.01883 1.32312 -.85597 .81712
94 .36302 -1.44213 -.55226 -.66426 -.32255 .35303 .45363
95 1.19121 -3.11125 .48271 .08378 .27587 -.85597 .45363
96 .01794 -1.44213 .89670 1.01883 1.77194 -.85597 -.27334
97 -.60320 -1.68057 .89670 1.39285 -.47216 -.85597 -.27334
98 -1.77646 -1.20368 .68970 .45780 .27587 .75603 -1.18206

133
Table 11 (continued)
ID Ztem Zhazards Zpro Zsuper Ztol Zfate Zinjury
99 -1.50040 -.72679 .89670 -.10323 -1.22019 -.04997 -.45508
100 .29401 -.24989 -.13827 -.85127 .12627 1.15903 -.81857
101 -.87926 .22700 -.55226 -1.22529 -.32255 1.96503 -.81857
102 .77712 -.96523 -.55226 .08378 .72470 .75603 -.63683
103 .29401 1.18079 .48271 .08378 .87430 -.85597 -.27334
104 .77712 -1.44213 .68970 .27079 -.17295 .75603 -.81857
105 -.12009 1.65768 .89670 -.47725 .27587 -.85597 -.09160
106 -1.70745 1.18079 .48271 1.39285 -1.07059 -.04997 -1.36380
107 .57007 -.24989 1.31069 2.14089 -.62177 .75603 .81712
108 -.32713 1.41923 .27572 .27079 1.02391 -.85597 -.63683
109 -.12009 .70389 1.31069 1.76687 -.32255 .35303 -.27334
110 -.05107 .94234 -1.38024 -.29024 .57509 1.15903 .27189
111 1.53629 -.72679 -.55226 -1.97333 1.32312 -.85597 .45363
112 -1.50040 .94234 .27572 1.39285 -.02334 -.85597 -.63683
113 -.67221 -.48834 1.31069 -.66426 1.47273 -.85597 .63537
114 -.39615 -1.20368 .89670 -.10323 -1.07059 -.45297 -.45508
115 .36302 1.41923 -.34527 -.10323 1.32312 -.04997 -.27334
116 -.39615 .46545 -.34527 .83182 -.17295 -.85597 -1.18206
117 .84613 .70389 .48271 1.39285 1.62234 .75603 -.09160
118 -.67221 .70389 1.10369 .64481 .72470 -.45297 -.09160
119 .43204 .70389 1.31069 2.14089 -1.66901 -.85597 -.63683
120 -.60320 .94234 -.75925 .45780 -.17295 -.45297 .27189
121 .50105 -.24989 .27572 .08378 .27587 -.85597 -.09160
122 1.05318 -.01145 -1.79422 -1.22529 -1.07059 1.15903 1.54409
123 -.39615 1.18079 .89670 .45780 -.02334 -.45297 -.45508
124 1.53629 .46545 -.13827 -.66426 .12627 -.85597 -.09160
125 -1.50040 -.24989 -.34527 -1.78632 .12627 1.15903 -.63683
126 .43204 -1.68057 -.55226 .27079 .57509 -.04997 .81712
127 .15598 -1.68057 -2.82919 -1.41230 -1.22019 .75603 1.54409
128 .29401 -.01145 -.96625 .64481 .87430 .35303 -.27334
129 -.12009 -.96523 -1.17324 -.47725 -.62177 -.45297 -.09160
130 -2.39761 1.41923 1.31069 .64481 -1.22019 -.85597 -1.18206
131 -.25812 .22700 -.34527 -.66426 -.77137 .35303 -.63683

134
Table 11 (continued)
ID Ztem Zhazards Zpro Zsuper Ztol Zfate Zinjury
132 .22499 .46545 .89670 .27079 .72470 -.45297 -.81857
133 -.12009 1.41923 -.34527 -.47725 .87430 -.04997 -1.00031
134 -.53418 1.89613 -.55226 -.66426 .12627 -.45297 -.09160
135 -1.01729 .70389 1.31069 .83182 .72470 -.04997 .81712
136 .63909 1.18079 .06872 .64481 .42548 -.85597 .09014
137 .29401 -.01145 .06872 -1.59931 .12627 .75603 -.27334
138 -.05107 .22700 -1.17324 -1.03828 -.02334 -.85597 1.18060
139 -1.84548 -.01145 .89670 .64481 -1.81862 -.85597 -.81857
140 -.18910 .46545 .27572 -.47725 -.17295 -.85597 1.36234
141 .98416 1.18079 .48271 -.66426 1.62234 1.15903 1.18060
142 1.81235 .70389 -.55226 .45780 1.02391 2.36804 .09014
143 .15598 -.01145 .89670 .64481 -1.81862 -.85597 -1.00031
144 -.67221 .22700 .68970 1.01883 -.62177 -.85597 -.45508
145 .36302 1.89613 .27572 -1.78632 -.47216 -.85597 -.27334
146 .91515 1.41923 .68970 .08378 .57509 1.56203 -.09160
147 -.87926 -.24989 -.34527 -1.22529 .72470 -.85597 -.09160
148 -.18910 .94234 .89670 .27079 .12627 -.45297 -.27334
149 .63909 -.72679 1.10369 1.01883 .72470 .35303 -.81857
150 -.46517 .94234 .27572 .45780 1.17352 -.85597 -.09160
151 -.53418 -1.44213 -2.00122 -1.22529 .27587 1.56203 -1.18206
152 -.25812 .70389 -2.20821 -1.03828 -.47216 .75603 1.18060
153 -.81024 1.41923 .68970 .27079 1.32312 -.04997 -1.00031
154 1.32924 -.48834 .89670 -1.03828 1.02391 1.96503 .09014
155 .22499 .22700 1.10369 -1.41230 1.17352 -.85597 .81712
156 .57007 .70389 -.34527 .08378 .42548 1.56203 -.45508
157 .84613 .94234 -.75925 .45780 .72470 .35303 .27189
158 -1.36237 -1.20368 .27572 .08378 -.02334 -.45297 -.81857
159 -1.08631 .94234 -.96625 -.29024 -.02334 -.85597 -.63683
160 2.50251 -.24989 -.96625 1.20584 -1.36980 -.85597 1.72583
161 .98416 -.48834 -.96625 -1.03828 1.02391 1.56203 1.54409
162 1.05318 1.41923 -.13827 -.29024 .72470 .35303 -.27334
163 .57007 2.37302 -.13827 .83182 -1.07059 -.85597 -1.54554
164 -.25812 .22700 -.75925 -.10323 .72470 -.85597 -.81857

135
Table 11 (continued)
ID Ztem Zhazards Zpro Zsuper Ztol Zfate Zinjury
165 2.64054 -.48834 -1.17324 -1.41230 .87430 -.04997 2.27106
166 1.88137 -.01145 -1.17324 -1.41230 -.47216 -.45297 2.27106
167 -1.43139 1.18079 .06872 -1.03828 -1.22019 1.15903 1.36234
168 -.81024 .46545 -.34527 -.85127 -.92098 2.77104 .45363
169 -1.91450 -.24989 1.31069 2.14089 -2.56665 -.85597 -1.18206
170 -.81024 -.72679 -.55226 -.10323 -.77137 -.85597 -.27334
171 .98416 -.72679 -.55226 -.66426 -.47216 -.45297 .45363
172 .08696 1.18079 .48271 1.20584 .42548 -.85597 -.09160
173 -1.22434 -2.15747 -.34527 -.47725 .87430 .35303 -.09160
174 -1.01729 1.41923 1.31069 2.14089 -.02334 -.85597 -1.00031
175 -.60320 .22700 -.96625 .08378 .87430 2.77104 -1.18206
176 -.67221 1.41923 1.31069 1.01883 -.02334 -.85597 .45363
177 -.87926 -.48834 .06872 1.01883 1.32312 2.36804 -.81857
178 .57007 -1.44213 -.55226 -.47725 -.47216 .35303 .27189
179 2.43349 -.01145 .89670 .45780 -.32255 -.04997 .45363
180 1.32924 -.48834 .27572 -.66426 .57509 1.56203 .45363
181 -.46517 -.72679 .48271 2.14089 -1.81862 -.85597 .81712
182 -1.15532 -1.20368 .48271 1.39285 -.47216 .75603 .45363
183 .01794 .46545 -1.17324 -1.22529 -1.22019 .75603 .63537
184 .50105 -1.20368 -1.58723 -1.03828 .57509 1.56203 -1.00031
185 -.12009 -.72679 -.13827 -1.22529 .12627 1.56203 .27189
186 -.53418 .70389 -.55226 -.47725 -.32255 -.85597 -.81857
187 .77712 -.24989 .89670 -.29024 1.02391 -.45297 .09014
188 .43204 -.01145 -.75925 -1.03828 -.02334 .35303 .81712
189 1.19121 -1.20368 -.13827 -1.22529 .72470 -.45297 .63537
190 -1.91450 .94234 .06872 .45780 .27587 -.85597 .63537
191 .63909 .70389 .48271 -.29024 .57509 -.85597 -.27334
192 -.53418 -.96523 1.31069 1.57986 -2.26744 -.85597 .63537
193 1.19121 1.41923 1.31069 2.14089 .42548 -.85597 .63537
194 -.67221 -.24989 -1.38024 .27079 .27587 2.36804 -.27334
195 -.94828 -.01145 1.31069 1.76687 -.17295 -.85597 -1.54554
196 -1.29335 .46545 1.31069 .83182 1.32312 -.85597 -1.54554
197 .50105 .94234 -.55226 -1.03828 .72470 .35303 -.09160

136
Table 11 (continued)
ID Ztem Zhazards Zpro Zsuper Ztol Zfate Zinjury
198 1.26023 .94234 .48271 -.29024 1.47273 -.04997 2.08932
199 2.43349 -.01145 .06872 .64481 1.47273 2.77104 .27189
200 -.25812 -.96523 .48271 .64481 -2.41705 -.85597 -1.00031
201 -1.63843 -.72679 .48271 -1.03828 .72470 .75603 -1.00031
202 -.18910 -1.44213 .48271 .64481 .57509 .75603 .27189
203 .50105 -.72679 -.13827 -.29024 1.32312 .75603 .27189
204 .50105 -.96523 -.75925 -1.03828 -.92098 -.45297 1.90757
205 -.18910 -.72679 -1.17324 -1.59931 -.47216 -.85597 -.27334
206 .22499 -.48834 -.96625 -.10323 -.17295 -.45297 -.09160
207 -.05107 -1.68057 .68970 .64481 .87430 .75603 -.27334
208 -.87926 .94234 -2.62220 -.29024 -.47216 -.85597 -.81857
209 .15598 .94234 1.10369 .27079 -.47216 -.85597 -.81857
210 .63909 -.96523 .06872 -.29024 1.62234 -.85597 -.45508
211 -1.63843 .94234 1.31069 .45780 .87430 -.45297 .27189
212 .98416 -.96523 .48271 .64481 1.02391 -.85597 -.27334
213 .77712 .94234 .68970 .45780 -1.81862 -.45297 -.81857
214 1.88137 .22700 .48271 1.20584 -1.81862 .35303 -.45508
215 -.39615 .94234 -.34527 .08378 .87430 -.45297 .45363
216 -.25812 -.96523 -.34527 -.29024 -.17295 .35303 -.27334
217 -.74123 .46545 -.34527 1.76687 -.17295 -.85597 -.09160
218 1.39826 -.72679 1.31069 1.01883 -.62177 -.04997 .63537
219 .29401 1.65768 .06872 1.01883 .27587 -.85597 -.27334
220 -.74123 .46545 -2.00122 .45780 -1.66901 -.85597 -.09160
221 -1.01729 .22700 -.96625 -.10323 -.32255 -.85597 -.27334
222 -.60320 -.48834 .68970 -.47725 .12627 -.45297 -1.00031
223 .98416 .70389 -.55226 -.47725 .72470 1.96503 4.27023*
224 -.53418 .70389 .06872 .64481 -1.07059 -.85597 -.09160
225 .36302 .22700 -.34527 -1.97333 -1.07059 -.45297 .63537
226 -1.43139 .46545 .27572 -.85127 -.02334 -.45297 -1.54554
227 .98416 .22700 .68970 -.10323 .12627 -.04997 .45363
228 -1.36237 -1.20368 .06872 .27079 .57509 -.85597 -1.00031
229 -1.08631 -.01145 -.55226 -.10323 -1.81862 -.04997 -1.54554
230 .01794 -.72679 .68970 .45780 -1.51941 -.45297 -.27334

137
Table 11 (continued)
ID Ztem Zhazards Zpro Zsup Ztol Zfate Zinjury
231 -.25812 -.48834 -1.17324 -.85127 .12627 1.15903 .81712
232 -.18910 -2.87280 -.34527 -1.78632 -.77137 -.45297 .63537
233 1.60531 -2.15747 -.55226 -.10323 -.17295 -.85597 2.81629
234 .22499 -1.20368 .48271 -.29024 1.77194 -.85597 .09014
235 -.60320 1.18079 .06872 -.47725 .42548 1.15903 .45363
236 -.60320 .22700 .48271 -.66426 .57509 -.85597 -.81857
237 .57007 .22700 -.75925 -1.78632 -.02334 .35303 .81712
238 .43204 -1.91902 .68970 .64481 -.02334 .35303 -.63683
239 .08696 -1.91902 .68970 1.20584 -.32255 -.85597 -.63683
240 .22499 .70389 -1.17324 -1.59931 -.62177 -.85597 -.81857
241 -1.22434 -.24989 .68970 .83182 1.62234 .75603 -1.00031
242 -.05107 -.01145 -.55226 -.29024 .87430 1.56203 1.90757
243 -.18910 .46545 .06872 -.10323 -.32255 .75603 .09014
244 -1.01729 .70389 .68970 .27079 .12627 -.85597 -.45508
245 -.67221 1.65768 .89670 1.01883 .87430 -.85597 -.45508
246 1.53629 -.24989 .68970 1.20584 .72470 -.04997 -.63683
247 .98416 -.96523 -3.24318 -2.16034 -1.07059 -.85597 1.18060
248 2.08842 -1.44213 .27572 -1.03828 -1.36980 1.56203 .99886
249 -.87926 -.24989 -.34527 -.66426 .12627 -.45297 1.36234
250 .57007 .22700 .06872 .08378 -.02334 -.85597 1.90757
Note ID = number of sample
Ztem = Z – score of child temperament
Zhazards = Z – score of home physical hazards
Zpro = Z – score of parental protectiveness
Zsup = Z – score of parental supervision
Ztol = Z – score of parental tolerance for child’s risk taking
Zfate = Z – score of parental fate beliefs
Zinjury = Z – score of unintentional home injury in toddlers
* outlier (ID # 49, # 85, # 223)

138
Table 12 Test of multivariate outliers by using mahalanobis distanced (n =247)
ID MAH_1 ID MAH_1 ID MAH_1 ID MAH_1
1 3.40759 35 5.76323 70 1.51544 104 2.49996
2 7.01898 36 10.95964 71 5.05320 105 4.74883
3 15.34439 37 5.92840 72 2.70579 106 8.91233
4 3.17090 38 7.78557 73 8.03969 107 2.75943
5 6.01725 39 5.79809 74 3.73323 108 4.14902
6 6.25177 40 1.25382 75 6.28063 109 3.45102
7 8.97689 41 1.49334 76 18.68963 110 8.84820
8 6.27651 42 1.16532 77 4.60078 111 4.59149
9 2.37156 43 4.92776 78 1.75962 112 8.93894
10 3.49870 44 4.42488 79 9.38179 113 2.91943
11 7.17875 45 9.47853 80 1.82817 114 2.76695
12 4.16508 46 8.55493 81 6.97766 115 3.37316
13 3.75051 47 6.07428 82 2.73168 116 6.48466
14 17.04234 48 9.30334 83 18.87674 117 2.79855
15 11.09186 50 10.45637 84 34.58470 118 8.59228
16 3.91085 51 5.07081 85 5.18820 119 2.33999
17 1.02134 52 4.50537 86 2.47025 120 1.33844
18 5.64528 53 6.54981 87 5.25768 121 7.33087
19 7.98336 54 5.57380 88 2.83466 122 1.02816
20 2.56413 55 5.87009 89 6.77130 123 5.21455
21 5.99665 56 4.96805 90 4.18115 124 8.48159
22 4.61456 57 4.88922 91 7.14282 125 1.91136
23 2.05803 58 10.97226 92 5.88729 126 10.46616
24 8.10811 59 2.64213 93 .87574 127 4.43739
25 1.63100 60 3.33303 94 2.56939 128 2.02464
26 17.24591 61 2.60787 95 5.85881 129 8.65582
27 8.42595 62 7.80550 96 2.80128 130 2.04850
28 6.71399 63 10.61706 97 5.07446 131 2.35308
29 4.15350 64 7.83589 98 5.65209 132 3.03029
30 8.30334 65 5.85587 99 4.06106 133 1.32607
31 6.34064 66 11.22646 100 7.61715 134 7.59191
32 3.24278 67 1.83933 101 3.99739 135 2.26341
33 2.19803 68 6.01202 102 2.09819 136 4.52235
34 8.38277 69 5.36063 103 3.99121 137 4.36188

139
Table 12 (Continued)
ID MAH_1 ID MAH_1 ID MAH_1 ID MAH_1
138 6.96082 172 3.64960 206 2.04251 241 2.20953
139 4.74076 173 5.56787 207 10.75824 242 3.42444
140 4.77353 174 11.75888 208 2.83381 243 7.08297
141 11.30680 175 4.66277 209 5.35995 244 14.96039
142 6.05549 176 10.30983 210 8.71494 245 13.01092
143 1.95077 177 1.13530 211 4.17478 246 6.25654
144 6.80871 178 8.55952 212 7.29432 247 5.52712
145 4.29525 179 4.53613 213 13.48859 248 3.42833
146 4.67264 180 10.69942 214 2.52983 249 1.87715
147 .97064 181 6.58526 215 .44829 250 2.33309
148 3.89608 182 4.36946 216 6.02051 234 6.96738
149 3.36482 183 9.00313 217 5.53880 235 6.62042
150 9.47146 184 4.26159 218 2.60572 236 7.82681
151 6.33604 185 2.23847 219 8.50497 237 .99288
152 3.73161 186 2.69337 220 2.91137 238 2.20953
153 8.91141 187 1.50018 221 2.61196 239 3.42444
154 7.99708 188 3.35614 222 2.00376 240 7.08297
155 3.95468 189 9.42744 224 6.70214 241 14.96039
156 3.18181 190 2.38318 225 5.32561 242 13.01092
157 2.18068 191 11.12591 226 1.59448 243 6.25654
158 3.32357 192 8.23361 227 3.61636 244 5.52712
159 16.50362 193 8.72295 228 5.70410 245 3.42833
160 4.92597 194 4.77710 229 3.25539 246 1.87715
161 2.66678 195 6.98215 230 3.24481 247 2.33309
162 7.76602 196 2.08101 231 5.35022
163 3.94189 197 6.52642 232 4.72441
164 9.55982 198 16.14468 233 3.12729
165 8.26738 199 7.22797 234 3.42833
166 14.06776 200 7.44599 235 1.87715
167 12.32767 201 1.90539 236 2.33309
168 12.14081 202 2.09212 237 6.96738
169 1.88528 203 6.06431 238 6.62042
170 2.24986 204 4.76378 239 7.82681
171 2.59814 205 1.74018 240 .99288
Note ID = number of sample
MAH_1 = p-value of Chi-square

140
Table 13 Test of normality of study variables (n = 247)
Variable Skewness C.R. of
Skewness Kurtosis
C.R. of
Kurtosis
Child gender .105 .676 -1.989 -6.380
Children temperament .331 2.124 -.174 -.559
Home physical hazards -.184 -1.178 -.428 -1.373
Parental protectiveness -1.172 -7.522 2.367 7.595
Parental supervision -.144 -.926 -.179 -.575
Parental risk tolerance -.403 -2.585 -.357 -1.145
Parental fate belief 1.091 6.999 .268 .860
Unintentional injury .622 3.989 -.209 -.671
Note C.R. of skewness = Critical ratio of skewness
C.R. of kurtosis = Critical ratio of kurtosis

141
Figure 11 The histogram of child gender
Figure 11 The histogram of child gender
141

142
Figure 12 The histogram of child temperament
142

143
Figure 13 The histogram of home physical hazards
143

144
Figure 14 The histogram of parental protectiveness
144

145
Figure 15 The histogram of parental supervision
145
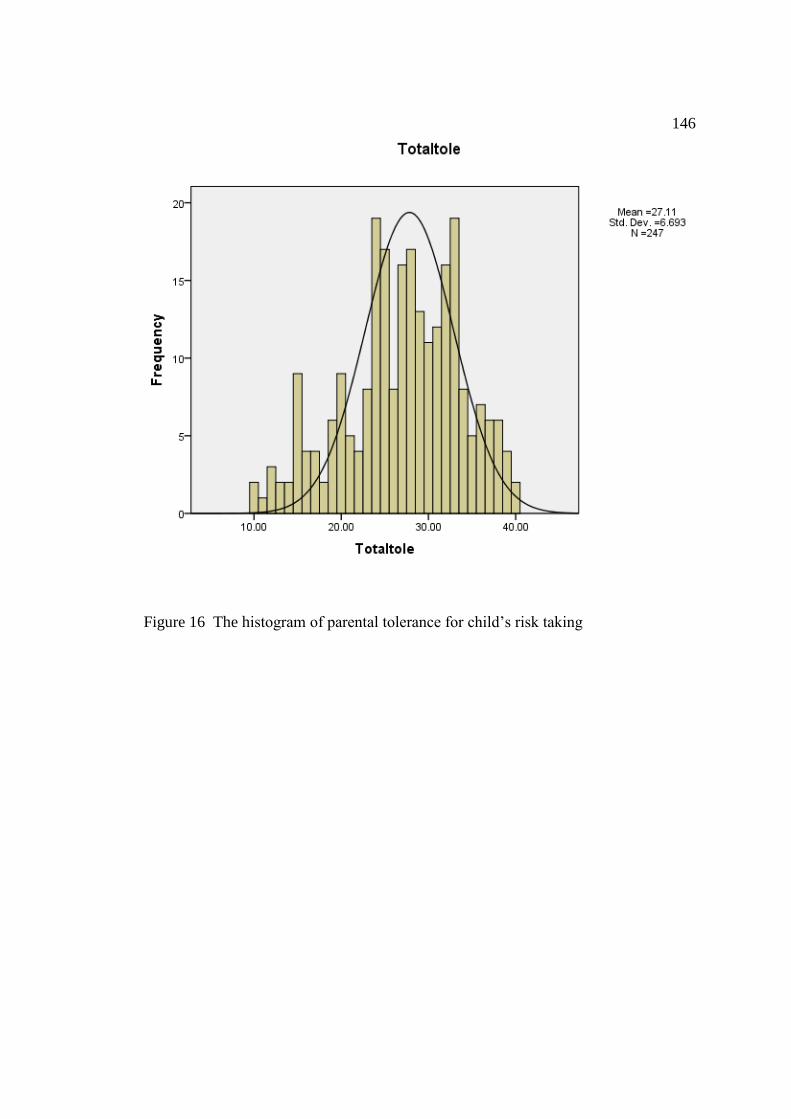
146
Figure 16 The histogram of parental tolerance for child’s risk taking
146
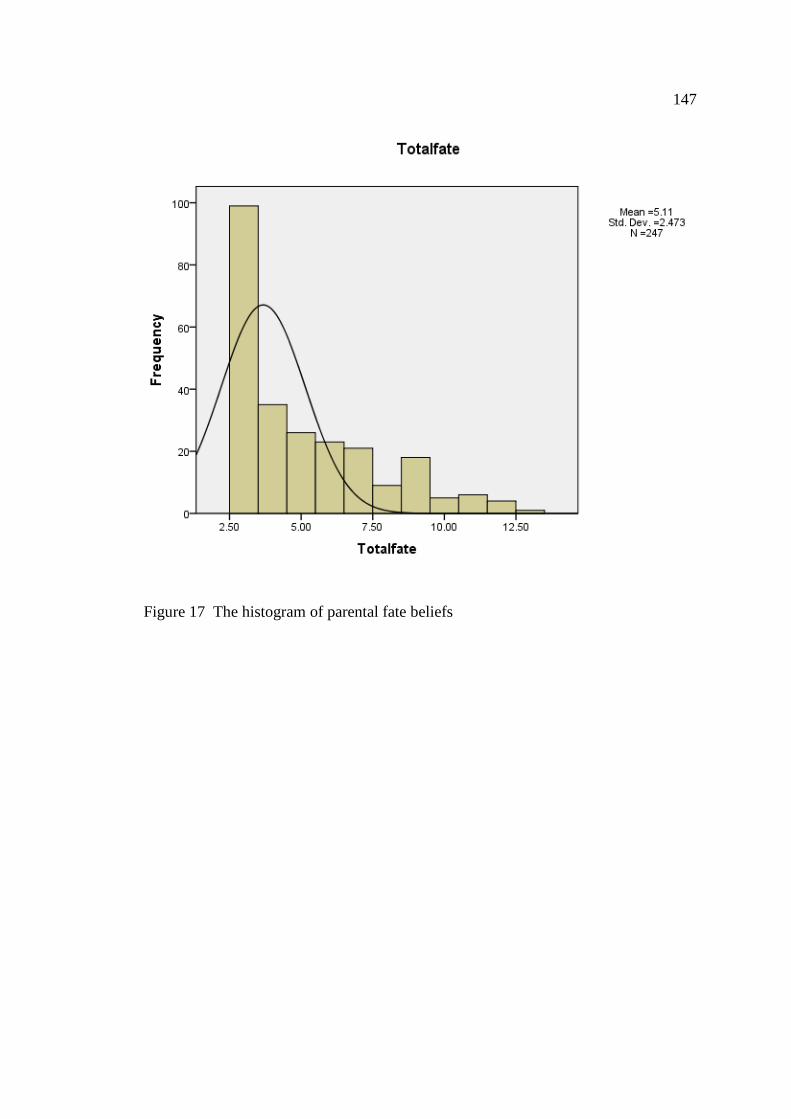
147
Figure 17 The histogram of parental fate beliefs
147
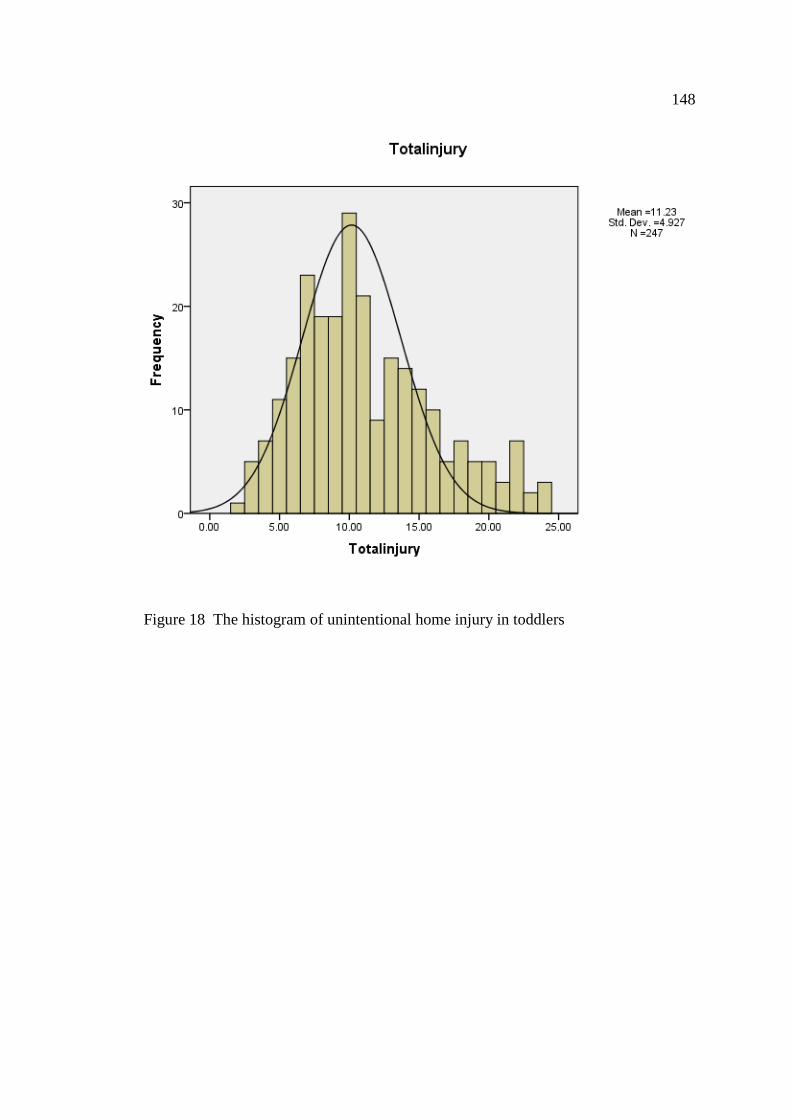
148
Figure 18 The histogram of unintentional home injury in toddlers
148

149
Table 14 Correlation matrix of study variables (n = 247)
Variable CG CT HPH PP PS PR PF UI
Child’s gender 1.00
Child
temperament
-.12 1.00
Home physical
hazards
.00 -.04 1.00
Parental
protectiveness
-.04 .00 .07 1.00
Parental
supervision
-.09 -.17** .07 .45** 1.00
Parental
risk tolerance
.05 .24** .07 .12 -.12 1.00
Parental
fate belief
.06 .12 -.10 -.17** -.14* .19** 1.00
Unintentional
injury
-.05 .56** -.03 -.19** -.31** .14* .14* 1.00
* p < .05, ** p < .01
Note CG = Child’s gender, CT = Child temperament, HPH = Home physical
hazards, PP = Parental protectiveness, PS = Parental supervision belief,
PR = Parental risk tolerance, PF = Parental fate belief, UHI = Unintentional
home injury

150
Table 15 Testing for multicolinearity of predictor variables (n = 247)
Variable Tolerance Variance Inflation Factor
(VIF)
Child’s gender .967 1.034
Child temperament .893 1.119
Home physical hazards .974 1.026
Parental protectiveness .746 1.340
Parental supervision .742 1.348
Parental risk tolerance .864 1.157
Parental fate belief .910 1.099

151
BIOGRAPHY
Name Mrs. Jirawan Klommek
Date of birth January 21, 1962
Place of birth Bangkok, Thailand
Present address 878/17 Soi. Makkasan Pittaya school
Petchaburi Rd. Ratchathewee district,
Bangkok 10400
Position held
1984 - 1988 Register Nurse
Mission Hospital
1990 - 1991 Instructor
Boromrajchonnani College of Nursing,
Ratchaburi Province
1991 - 1992 Register Nurse
Mission Hospital
1992 - present Senior lecturer
Mission Faculty of Nursing,
Asia-Pacific International University
Education
1981 - 1984 Certificate of Nursing and Midwifery
Bangkok Adventist Hospital, School of
Nursing, Thailand
1988 - 1990 Bachelor of Nursing Education,
Srinakharinwirot University, Thailand
1998 - 2000 Master of Nursing Science
(Pediatric Nursing),
Mahidol University, Thailand
2010 - 2015 Doctoral of Philosophy (Nursing Science),
Burapha University, Thailand