Embed Size (px)
Citation preview
Cancer Investigation, 31:287–308, 2013ISSN: 0735-7907 print / 1532-4192 onlineCopyright C© 2013 Informa Healthcare USA, Inc.DOI: 10.3109/07357907.2013.789899
REVIEW
Predictors of Long-Term Survival in Patients With GlioblastomaMultiforme: Advancements From the Last Quarter Century
Nauman S. Chaudhry, Ashish H. Shah, Nicholas Ferraro, Brian M. Snelling, Amade Bregy,Karthik Madhavan, and Ricardo J. Komotar
Department of Neurological Surgery, University of Miami Miller School of Medicine, Miami, FL, USA
Over the last quarter century there has been significantprogress toward identifying certain characteristics andpatterns in GBM patients to predict survival times andoutcomes. We sought to identify clinical predictors of survivalin GBM patients from the past 24 years. We examined patientsurvival related to tumor locations, surgical treatment,postoperative course, radiotherapy, chemotherapy, patientage, GBM recurrence, imaging characteristics, serum, andmolecular markers. We present predictors that may increase,decrease, or play no significant role in determining a GBMpatient’s long-term survival or affect the quality of life.
Keywords: Glioblastoma multiforme, Brain tumors, CNSmalignancy, Prognosis and response, Cancer biomarkers,Treatment, systematic analysis
INTRODUCTION
Glioblastoma multiforme (GBM) is the most common pri-mary brain tumor comprising approximately 12–15% of allintracranial neoplasms and 50–60% of all astrocytomas (1).In the United States of America (USA), the incidence ofGBM is 2–3 new cases per 100,000 people appear everyyear (1). Palliative care involving surgery, radiotherapy, andchemotherapy remains to be the standard treatment ap-proach, which extends the median survival time (MST) forpatients who receive such treatment to 12 months comparedwith 3 months for those who do not receive any treatment.
Traditionally, prognosis of a patient with GBM is de-termined with histology. Today’s advancements in geneticsand imaging technology have surfaced more patient-specificmolecular associations and therapies for these patients. Thisis continuing to lead both doctors and patients toward a bet-ter understanding of GBM and improving quality of care.
Each GBM tumor is unique. The distinct nature of eachpatient’s GBM is what makes the tumor elusive to most ther-apies and difficult to target. In addition, the timeline of dis-ease will vary from patient to patient. This presents difficulty
Correspondence to: Ricardo J. Komotar, M.D., Assistant Professor of Neurological Surgery, Director of Neurooncology, University of MiamiHospital, Co-Director of Neurooncology, Sylvester Comprehensive Cancer Center, Co-Director of Neurooncology, Department of NeurologicalSurgery, University of Miami Health Clinics, University of Miami, 1095 NW 14th Terrace, 2nd Floor, Miami, FL, USA, e-mail:[email protected]
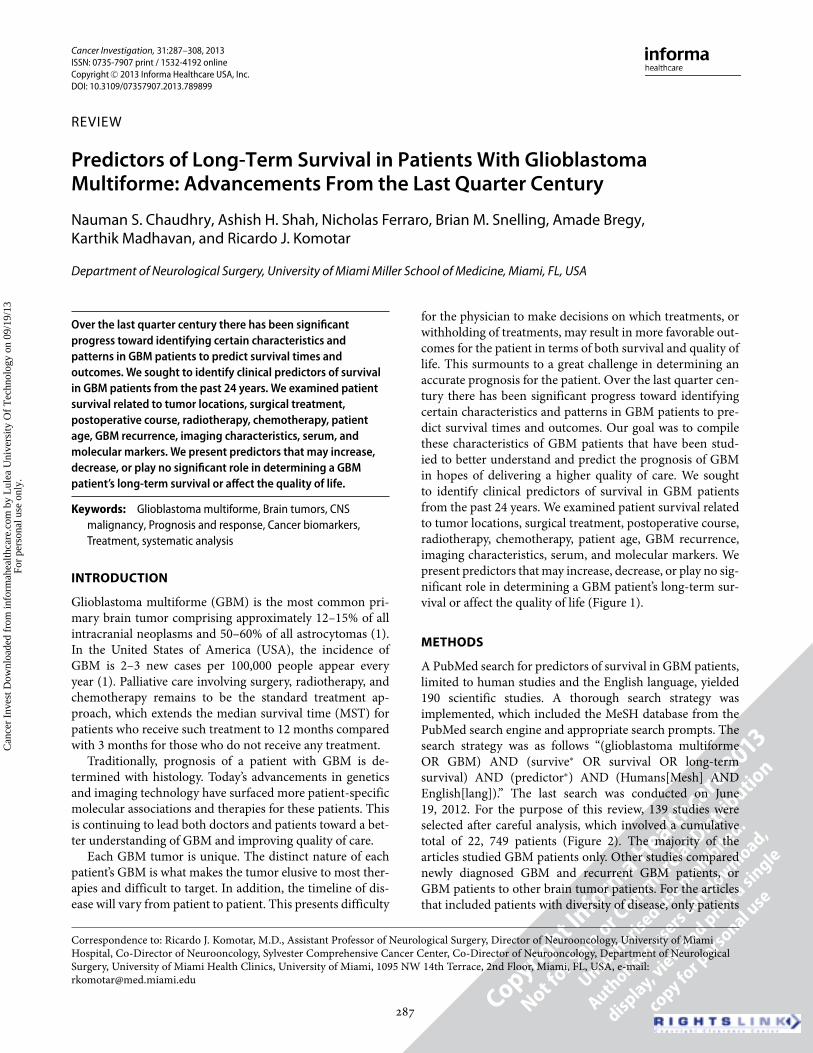
for the physician to make decisions on which treatments, orwithholding of treatments, may result in more favorable out-comes for the patient in terms of both survival and quality oflife. This surmounts to a great challenge in determining anaccurate prognosis for the patient. Over the last quarter cen-tury there has been significant progress toward identifyingcertain characteristics and patterns in GBM patients to pre-dict survival times and outcomes. Our goal was to compilethese characteristics of GBM patients that have been stud-ied to better understand and predict the prognosis of GBMin hopes of delivering a higher quality of care. We soughtto identify clinical predictors of survival in GBM patientsfrom the past 24 years. We examined patient survival relatedto tumor locations, surgical treatment, postoperative course,radiotherapy, chemotherapy, patient age, GBM recurrence,imaging characteristics, serum, and molecular markers. Wepresent predictors that may increase, decrease, or play no sig-nificant role in determining a GBM patient’s long-term sur-vival or affect the quality of life (Figure 1).
METHODS
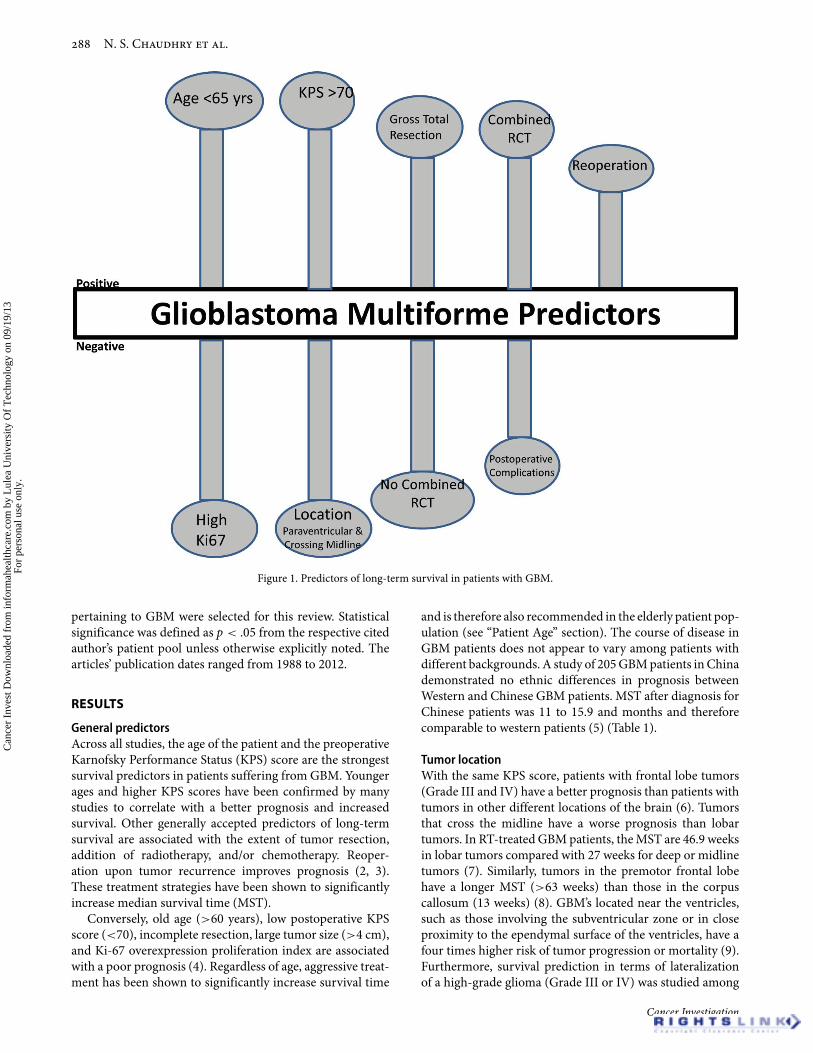
A PubMed search for predictors of survival in GBM patients,limited to human studies and the English language, yielded190 scientific studies. A thorough search strategy wasimplemented, which included the MeSH database from thePubMed search engine and appropriate search prompts. Thesearch strategy was as follows “(glioblastoma multiformeOR GBM) AND (survive∗ OR survival OR long-termsurvival) AND (predictor∗) AND (Humans[Mesh] ANDEnglish[lang]).” The last search was conducted on June19, 2012. For the purpose of this review, 139 studies wereselected after careful analysis, which involved a cumulativetotal of 22, 749 patients (Figure 2). The majority of thearticles studied GBM patients only. Other studies comparednewly diagnosed GBM and recurrent GBM patients, orGBM patients to other brain tumor patients. For the articlesthat included patients with diversity of disease, only patients
Can
cer
Inve
st D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y L
ulea
Uni
vers
ity O
f T
echn
olog
y on
09/
19/1
3Fo
r pe
rson
al u
se o
nly.
N. S. Chaudhry et al.
Figure 1. Predictors of long-term survival in patients with GBM.
pertaining to GBM were selected for this review. Statisticalsignificance was defined as p < .05 from the respective citedauthor’s patient pool unless otherwise explicitly noted. Thearticles’ publication dates ranged from 1988 to 2012.
RESULTS
General predictorsAcross all studies, the age of the patient and the preoperativeKarnofsky Performance Status (KPS) score are the strongestsurvival predictors in patients suffering from GBM. Youngerages and higher KPS scores have been confirmed by manystudies to correlate with a better prognosis and increasedsurvival. Other generally accepted predictors of long-termsurvival are associated with the extent of tumor resection,addition of radiotherapy, and/or chemotherapy. Reoper-ation upon tumor recurrence improves prognosis (2, 3).These treatment strategies have been shown to significantlyincrease median survival time (MST).
Conversely, old age (>60 years), low postoperative KPSscore (<70), incomplete resection, large tumor size (>4 cm),and Ki-67 overexpression proliferation index are associatedwith a poor prognosis (4). Regardless of age, aggressive treat-ment has been shown to significantly increase survival time
and is therefore also recommended in the elderly patient pop-ulation (see “Patient Age” section). The course of disease inGBM patients does not appear to vary among patients withdifferent backgrounds. A study of 205 GBM patients in Chinademonstrated no ethnic differences in prognosis betweenWestern and Chinese GBM patients. MST after diagnosis forChinese patients was 11 to 15.9 and months and thereforecomparable to western patients (5) (Table 1).
Tumor locationWith the same KPS score, patients with frontal lobe tumors(Grade III and IV) have a better prognosis than patients withtumors in other different locations of the brain (6). Tumorsthat cross the midline have a worse prognosis than lobartumors. In RT-treated GBM patients, the MST are 46.9 weeksin lobar tumors compared with 27 weeks for deep or midlinetumors (7). Similarly, tumors in the premotor frontal lobehave a longer MST (>63 weeks) than those in the corpuscallosum (13 weeks) (8). GBM’s located near the ventricles,such as those involving the subventricular zone or in closeproximity to the ependymal surface of the ventricles, have afour times higher risk of tumor progression or mortality (9).Furthermore, survival prediction in terms of lateralizationof a high-grade glioma (Grade III or IV) was studied among
Cancer Investigation
Can
cer
Inve
st D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y L
ulea
Uni
vers
ity O
f T
echn
olog
y on
09/
19/1
3Fo
r pe
rson
al u
se o
nly.
Predictors of Long-Term Survival in GBM Patients
Figure 2. Patient data gathered for various predictors of survival with GBM.
280 right-handed patients. These patients were separatedinto dominant (control of speech) and nondominant (con-tralateral hemisphere to the control of speech) hemisphericgroups; the study found that lateralization of a tumor isneither a prognostic factor for survival nor for the outcomein a patient. Therefore, the study concluded that surgery
should not be dissuaded for a resectable tumor solely on fearof lateralization (10)(Table 1).
SurgeryThe diagnosis of GBM is generally followed by surgery, ra-diotherapy (RT), chemotherapy, or combined radiotherapy
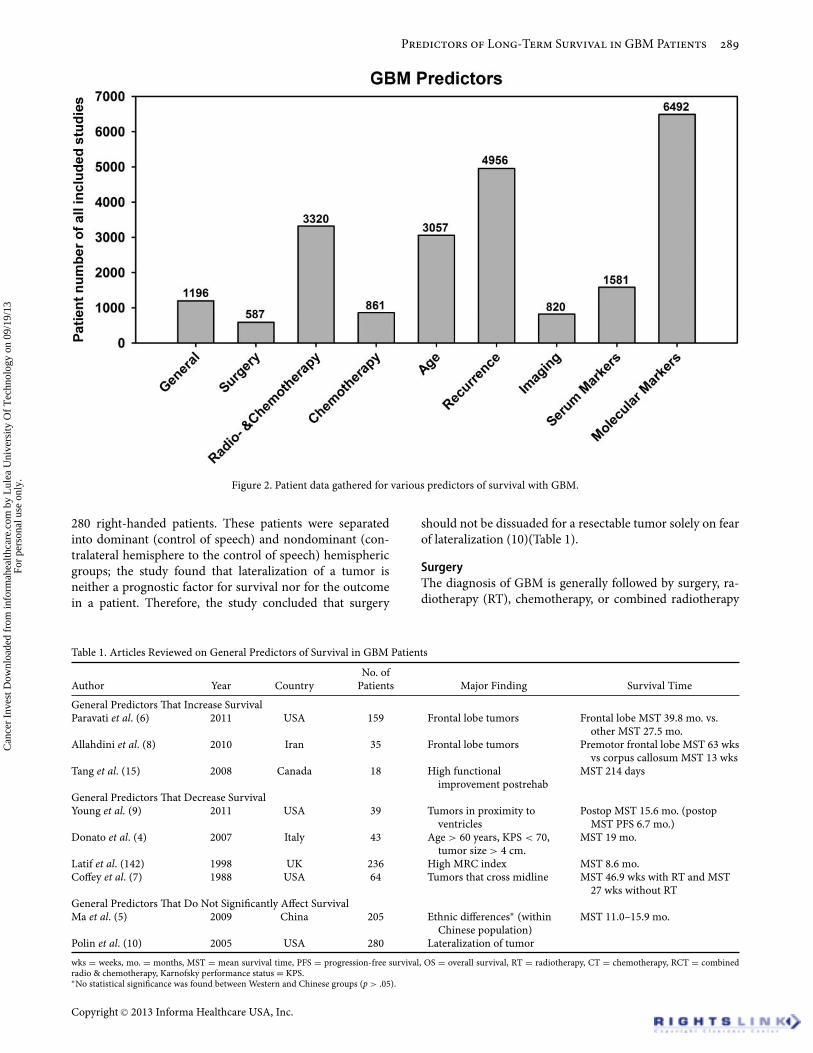
Table 1. Articles Reviewed on General Predictors of Survival in GBM Patients
Author Year CountryNo. of
Patients Major Finding Survival Time
General Predictors That Increase SurvivalParavati et al. (6) 2011 USA 159 Frontal lobe tumors Frontal lobe MST 39.8 mo. vs.
other MST 27.5 mo.Allahdini et al. (8) 2010 Iran 35 Frontal lobe tumors Premotor frontal lobe MST 63 wks
vs corpus callosum MST 13 wksTang et al. (15) 2008 Canada 18 High functional
improvement postrehabMST 214 days
General Predictors That Decrease SurvivalYoung et al. (9) 2011 USA 39 Tumors in proximity to
ventriclesPostop MST 15.6 mo. (postop
MST PFS 6.7 mo.)Donato et al. (4) 2007 Italy 43 Age > 60 years, KPS < 70,
tumor size > 4 cm.MST 19 mo.
Latif et al. (142) 1998 UK 236 High MRC index MST 8.6 mo.Coffey et al. (7) 1988 USA 64 Tumors that cross midline MST 46.9 wks with RT and MST
27 wks without RTGeneral Predictors That Do Not Significantly Affect SurvivalMa et al. (5) 2009 China 205 Ethnic differences∗ (within
Chinese population)MST 11.0–15.9 mo.
Polin et al. (10) 2005 USA 280 Lateralization of tumor
wks = weeks, mo. = months, MST = mean survival time, PFS = progression-free survival, OS = overall survival, RT = radiotherapy, CT = chemotherapy, RCT = combinedradio & chemotherapy, Karnofsky performance status = KPS.∗No statistical significance was found between Western and Chinese groups (p > .05).
Copyright C© 2013 Informa Healthcare USA, Inc.
Can
cer
Inve
st D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y L
ulea
Uni
vers
ity O
f T
echn
olog
y on
09/
19/1
3Fo
r pe
rson
al u
se o
nly.

N. S. Chaudhry et al.
Table 2. Articles Reviewed on Surgical Predictors of Survival in GBM Patients
Author Year CountryNo. of
Patients Major Finding Survival Time
Surgical Predictors That Increase SurvivalAllahdini et al. (8) 2010 Iran 35 Maximal resection Max resection MST 13 mo. vs.
subtotal resection MST 8.8 mo.Lacroix et al. (13) 2001 USA 416 Age, KPS score, maximal
resectionMax resection MST 27 mo. vs.
subtotal resection MST 33 mo.Kowalczuk et al. (12) 1997 USA 75 Maximal extent of resectionSurgical Predictors That Decrease SurvivalJakola et al. (14) 2011 Norway 61 Postop early deterioration in
HRQOL
wks = weeks, mo. = months, MST = mean survival time, PFS = progression-free survival, OS = overall survival, RT = radiotherapy, CT = chemotherapy, RCT = combinedradio & chemotherapy, HRQOL = health-related quality of living, Karnofsky performance status = KPS.
and chemotherapy (RCT). Intervention can increase MSTand quality of life in eligible patients. A major autopsy studyshowed GBM patients who do not receive any treatmentfor their condition die most commonly due to herniation(11). Surgical resection is the primary treatment modalityand the extent of resection significantly impacts MST andprogression-free survival (PFS). A study consisting of high-grade astrocytoma patients (Grade III and IV) showed pa-tients who underwent subtotal or total resection had an MSTof at least 27 months versus 13 months for those who onlyhad a biopsy performed (12). Maximal resection of the GBMin patients is associated with longer survival times and im-proved outcomes and is highly recommended, barring otherrisk factors (8,13) (Table 2).
Postoperative coursePostoperative complications of surgery correlate with a worseprognosis. One study looked at survival in terms of GBM pa-tients’ self-reported health quality of life (HQOL) deteriora-tion after surgery. Patients who reported early deteriorationin the postoperative period were significantly associated withdecreased survival (14). High functional improvement afterrehabilitation therapy is also a prognostic indicator of sur-vival. Survival improved in those patients who presented tothe rehabilitation center with a higher score on Function In-dependence Measure (FIM) and a low dose of dexametha-sone (<8 mg/day) upon admission (15). See Table 1.
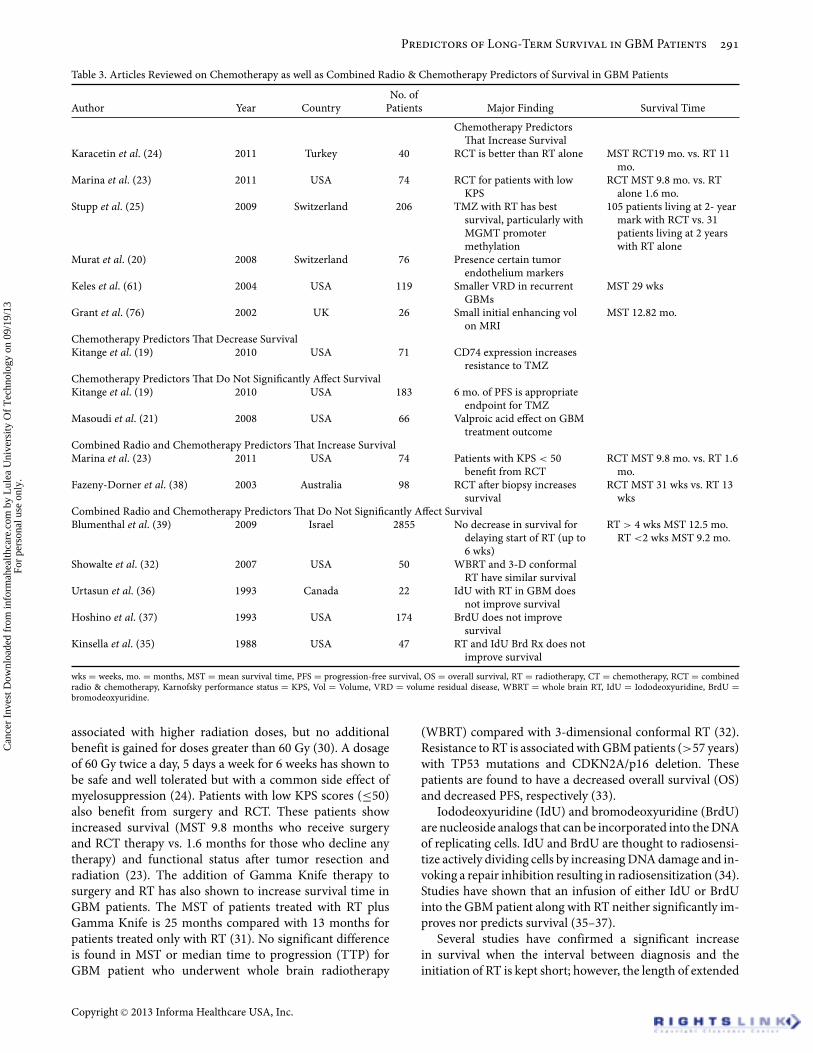
ChemotherapyTemozolamide (TMZ) is a widely used protocol forchemotherapeutic treatment in patients with GBM; however,its efficacy varies according to the molecular makeup of theGBM tumors. TMZ acts to alkylate/methylate DNA at N-7 orO-6 guanine residues in tumor cells to trigger apoptosis (16).Studies have shown that certain patients with GBM tumorsexpressing the O(6)-methylguanine-DNA methyltransferase(MGMT) enzyme are resistant to TMZ therapy. MGMTexpressing tumors are believed to possess the ability to repairthe alkylating effects on the DNA caused by the TMZ ther-apy. Patients in which the MGMT promoter is epigeneticallymethylated have increased sensitivity to TMZ therapy andtherefore a significantly better prognosis and increased sur-vival time (17, 18). There are other different tumor markers
that also vary in their sensitivity to TMZ therapy such asCD74, which has also been implicated with TMZ resistance(19). Similarly, one study found that increased expressionof particular cluster of HOX genes, G28 and CD133, areassociated with worse outcome and resistance to RT andTMZ therapy. Conversely, better prognosis was indicatedwith other gene clusters involving the vascularization, celladhesion, and innate immune response (20).
Valproic acid, an antiepileptic therapy for seizures, isthought to induce tumor cell differentiation because it alsoacts as a histone deacetylase (HDAC) inhibitor. HDAC in-hibitors sensitize malignant cells to RCT, but this was notfound to be true in GBM patients. A study found that pe-diatric anaplastic astrocytoma (AA) and GBM patients re-ceiving RCT and valproic acid together for seizure controlreported no beneficial or even adverse effects from concomi-tant antiseizure treatments (21).
The duration of chemotherapy for a patient to receivea significant benefit is not clearly defined. One study with183 patients showed significant survival outcomes in pa-tients who received chemotherapy for periods of 2, 4, and6 months. They recommended a 6-month progression-freesurvival (PFS) period as an appropriate endpoint for TMZtherapy (22). Patients who revealed early signs of progressionduring treatment were found to have a significantly higherrisk of early death.
Combined RCT comprises a significant role in GBM ther-apy. The best outcomes were found in patients who con-comitantly receive TMZ as chemotherapy and RT. One studyshowed that MST for patients receiving RCT was 9.8 monthsversus 1.7 months for those receiving RT alone (23). A simi-lar study revealed RCT patients lived 19 months versus 11.5months for patient who received RT only (24). Another studypresented data revealing 105 of their patients receiving RCTwere alive at the 2-year mark compared with 31 patients alivethat only received RT (25)(Table 3).
Combined radiotherapy & chemotherapyA high KPS score (≥70) is the best predictor for response toRT in patients with GBM (26). RT increases survival time inpatients after a maximum total resection (27, 28), and it hasbeen shown to increase survival in patients with GBM butalso in other malignant gliomas (29). Adequate RT is neededfor optimal outcomes. Increased survival is significantly
Cancer Investigation
Can
cer
Inve
st D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y L
ulea
Uni
vers
ity O
f T
echn
olog
y on
09/
19/1
3Fo
r pe
rson
al u
se o
nly.
Predictors of Long-Term Survival in GBM Patients
Table 3. Articles Reviewed on Chemotherapy as well as Combined Radio & Chemotherapy Predictors of Survival in GBM Patients
Author Year CountryNo. of
Patients Major Finding Survival Time
Chemotherapy PredictorsThat Increase Survival
Karacetin et al. (24) 2011 Turkey 40 RCT is better than RT alone MST RCT19 mo. vs. RT 11mo.
Marina et al. (23) 2011 USA 74 RCT for patients with lowKPS
RCT MST 9.8 mo. vs. RTalone 1.6 mo.
Stupp et al. (25) 2009 Switzerland 206 TMZ with RT has bestsurvival, particularly withMGMT promotermethylation
105 patients living at 2- yearmark with RCT vs. 31patients living at 2 yearswith RT alone
Murat et al. (20) 2008 Switzerland 76 Presence certain tumorendothelium markers
Keles et al. (61) 2004 USA 119 Smaller VRD in recurrentGBMs
MST 29 wks
Grant et al. (76) 2002 UK 26 Small initial enhancing volon MRI
MST 12.82 mo.
Chemotherapy Predictors That Decrease SurvivalKitange et al. (19) 2010 USA 71 CD74 expression increases
resistance to TMZChemotherapy Predictors That Do Not Significantly Affect SurvivalKitange et al. (19) 2010 USA 183 6 mo. of PFS is appropriate
endpoint for TMZMasoudi et al. (21) 2008 USA 66 Valproic acid effect on GBM
treatment outcomeCombined Radio and Chemotherapy Predictors That Increase SurvivalMarina et al. (23) 2011 USA 74 Patients with KPS < 50
benefit from RCTRCT MST 9.8 mo. vs. RT 1.6
mo.Fazeny-Dorner et al. (38) 2003 Australia 98 RCT after biopsy increases
survivalRCT MST 31 wks vs. RT 13
wksCombined Radio and Chemotherapy Predictors That Do Not Significantly Affect SurvivalBlumenthal et al. (39) 2009 Israel 2855 No decrease in survival for
delaying start of RT (up to6 wks)
RT > 4 wks MST 12.5 mo.RT <2 wks MST 9.2 mo.
Showalte et al. (32) 2007 USA 50 WBRT and 3-D conformalRT have similar survival
Urtasun et al. (36) 1993 Canada 22 IdU with RT in GBM doesnot improve survival
Hoshino et al. (37) 1993 USA 174 BrdU does not improvesurvival
Kinsella et al. (35) 1988 USA 47 RT and IdU Brd Rx does notimprove survival
wks = weeks, mo. = months, MST = mean survival time, PFS = progression-free survival, OS = overall survival, RT = radiotherapy, CT = chemotherapy, RCT = combinedradio & chemotherapy, Karnofsky performance status = KPS, Vol = Volume, VRD = volume residual disease, WBRT = whole brain RT, IdU = Iododeoxyuridine, BrdU =bromodeoxyuridine.
associated with higher radiation doses, but no additionalbenefit is gained for doses greater than 60 Gy (30). A dosageof 60 Gy twice a day, 5 days a week for 6 weeks has shown tobe safe and well tolerated but with a common side effect ofmyelosuppression (24). Patients with low KPS scores (≤50)also benefit from surgery and RCT. These patients showincreased survival (MST 9.8 months who receive surgeryand RCT therapy vs. 1.6 months for those who decline anytherapy) and functional status after tumor resection andradiation (23). The addition of Gamma Knife therapy tosurgery and RT has also shown to increase survival time inGBM patients. The MST of patients treated with RT plusGamma Knife is 25 months compared with 13 months forpatients treated only with RT (31). No significant differenceis found in MST or median time to progression (TTP) forGBM patient who underwent whole brain radiotherapy
(WBRT) compared with 3-dimensional conformal RT (32).Resistance to RT is associated with GBM patients (>57 years)with TP53 mutations and CDKN2A/p16 deletion. Thesepatients are found to have a decreased overall survival (OS)and decreased PFS, respectively (33).
Iododeoxyuridine (IdU) and bromodeoxyuridine (BrdU)are nucleoside analogs that can be incorporated into the DNAof replicating cells. IdU and BrdU are thought to radiosensi-tize actively dividing cells by increasing DNA damage and in-voking a repair inhibition resulting in radiosensitization (34).Studies have shown that an infusion of either IdU or BrdUinto the GBM patient along with RT neither significantly im-proves nor predicts survival (35–37).
Several studies have confirmed a significant increasein survival when the interval between diagnosis and theinitiation of RT is kept short; however, the length of extended
Copyright C© 2013 Informa Healthcare USA, Inc.
Can
cer
Inve
st D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y L
ulea
Uni
vers
ity O
f T
echn
olog
y on
09/
19/1
3Fo
r pe
rson
al u
se o
nly.

N. S. Chaudhry et al.
time that was considered significant remains subjective to acertain degree. Minimizing waiting time after stereotacticbiopsy to begin treatment has been shown to increase sur-vival in patients. Treatment with RCT (MST 31 weeks) as op-posed to RT only (MST 13 weeks) further increases survivaltimes (38). A major retrospective study consisting of 2,855GBM patients found that there is no significant decrease insurvival for delaying the start of RT within 6 weeks of diag-nosis. Interestingly, the authors noted there was a significantincrease in survival for those patients who waited until 4weeks after diagnosis to receive treatment compared withthose patients with shorter delays after surgery (39) (Table 3).
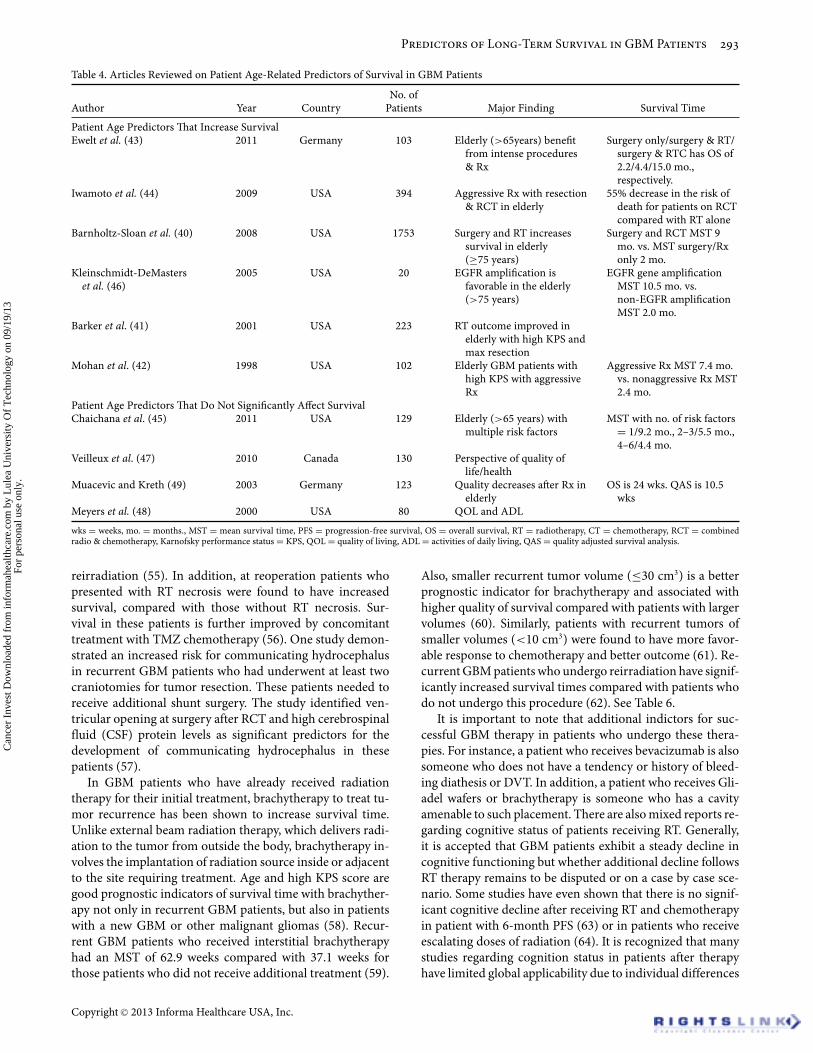
Patient ageAge and KPS score are very important prognostic indicators,which also hold true in the elderly population. Althoughyounger ages and higher KPS scores are associated withbetter prognosis, this should not serve as definitive groundsagainst providing aggressive multimodal care to elderly GBMpatients. A major study of treatment in the elderly GBMpopulation (n = 1,753) revealed patients over ≥75 yearsold had 2.5-fold increased odds of being treated with biopsyonly, 1.5-fold increased odds of undergoing surgery only,and 0.31 decreased odds of having both radiation andsurgery compared with patients younger than 75 years.Subsequently, those elderly patients who solely receivedeither biopsy or surgery had an MST of 2 months comparedwith 9 months for older GBM patients treated with RCT(40). Elderly patients are known to benefit from aggressiveprocedures and therapy, especially those with higher KPSscores. Higher KPS scores and maximal resection result inbetter outcomes in these patients (41). Furthermore, elderlypatients (>70 years) treated with surgery and RCT had amedian survival of 7.4 months compared with 2.4 months inthose not receiving multimodal treatment (42). Overall sur-vival (OS) differed significantly among elderly patients whoreceived varying treatments: 2.2 months in patients receivingsurgery only and 4.4 months in patients receiving surgeryand RT compared with 15 months in patients receivingsurgery and RCT. Along with OS, elderly patients undergo-ing surgery and RCT were also found to have significantlyincreased PFS (43). Another major study (n = 394) found a55% decreased risk of death in patients receiving surgery andRCT compared with those who only received RT (44). Thus,cases in which elderly patients are not receiving optimalaggressive care due to age alone are prone to have a worseprognosis. However, one study looked at factors to provideinsight as to whether or not elderly patients (>65 years)should receive aggressive surgery. They found that amongpatients who undergo aggressive surgery, those with riskfactors, including low KPS scores, COPD, tumor size >4 cm,and motor, language, and cognitive deficits have worseprognosis. Patients with 0–1, 2–3, or 4–6 of these risk factorshad MSTs of 9.2, 5.5, and 4.4 months, respectively (45).
Biomarkers may also play a role in the elderly involvingthe presence of the epidermal growth factor receptor (EGFR).Contrary to the nonelderly population, one study showedEGFR amplification to be associated with increased survival.
MST in elderly GBM patients (>75 years) was 8.3 monthscompared with 3.2 months for those elderly patients withoutEGFR amplification (46).
Hesitation in the execution of aggressive multimodal ther-apy in the elderly patient largely concerns issues regardingquality of life. Perspective of quality of life (QOL) amongGBM patients is different depending on the age of the group.One study compared predictors of QOL in age groups of<40 years and >40 years. In younger patients, the predictorfor QOL was the “support of friends,” whereas “enjoying life”was the predictor for QOL in older patients. Negative impactson quality of health (QOH) in younger patients were physicalpain versus difficulty concentrating for older patients (47).QOL and activities of daily living (ADL) do not predict sur-vival (48). Although aggressive treatment has shown to sig-nificantly increase survival time in elderly patients, one studynoted that QOL does decrease after treatment, which pro-vides little functional improvement, in the elderly. Althoughthis study’s sample population did not show prognostic sig-nificance with age, unlike many other studies, the authordoes indeed recommend consideration of supportive treat-ment for patients with low KPS (<70) (49) (Table 4).
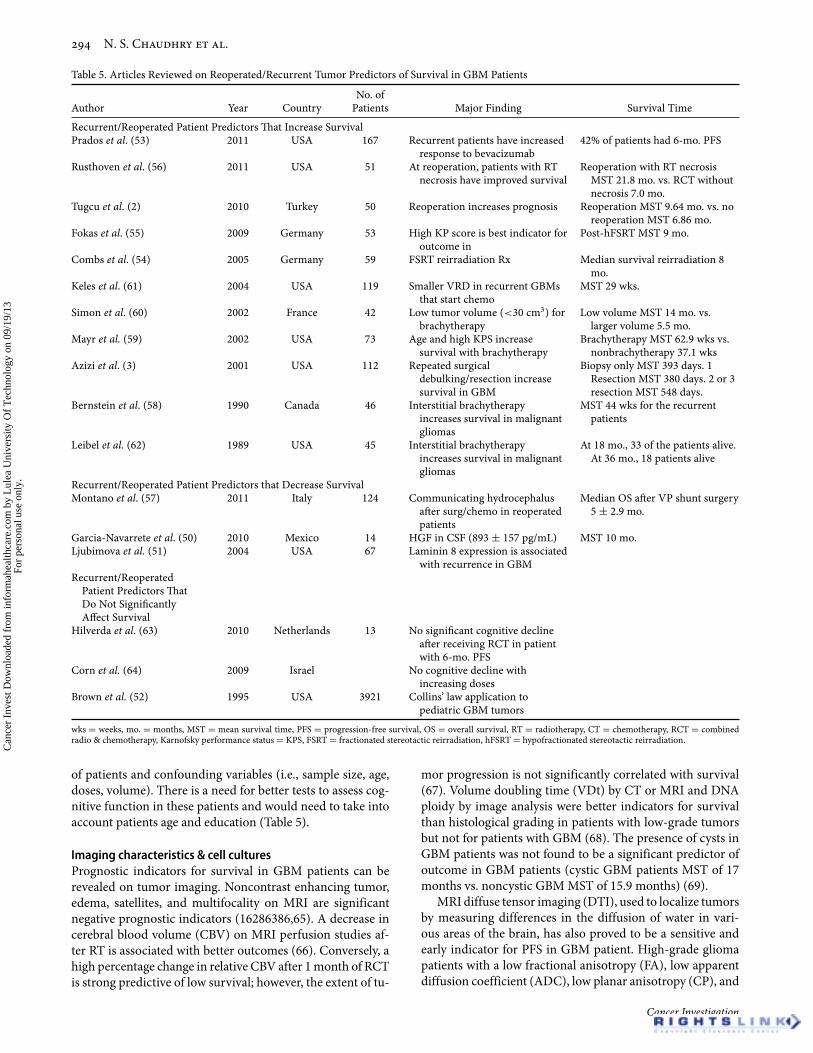
GBM recurrence in patientsTumor recurrence in GBM patients is not a rare find-ing, and although it is associated with higher risk of mor-bidity, additional therapy is favorable predictor of positiveoutcomes. GBM patients with high concentrations (893 ±157 pg/mL) of hepatocyte growth factor (HGF) in CSF arefound to have a shorter tumor-free survival period aftertreatment, more rapid recurrence, and increased mortalityrates (50). Laminin-8, a vascular basement membrane com-ponent, is also a marker for recurrence. Overexpression oflaminin-8 in GBM is associated with a shorter time of re-currence and decreased survival time compared with lowergrade glioma patients that showed higher expressions levelsof laminin-9 (51). One study found tumor recurrence in pe-diatric (<21 years) GBM patients to correlate with the child’sage plus 9 months, a pattern also displayed in Wilms’ tumorknown as Collins’ law (52). Patients with recurrent GBM tu-mors have an increased response to bevacizumab, a mono-clonal antibody that inhibits vascular endothelial growth fac-tor (VEGF) resulting in angiogenesis inhibition. One studywith 167 recurrent GBM patients treated with bevacizumabdemonstrated over 75% of them lived past the 26-week land-mark. Patients who responded to bevacizumab therapy had ahigher predictor of survival and PFS (53).
Repeated surgical resection in recurrent GBM patientssignificantly increases prognosis and survival. Patients withrecurrent GBM who underwent reoperation had an MST of9.64 months compared with 6.56 months in those who didnot (2). Patients who underwent one resection had an MSTof 380 days compared with 548 days in those patients whohad two or three resections (3). Fractionated stereotactic reir-radiation therapy (FSRT) also improves survival in recurrentGBM patients with one study showing MST after reirradi-ation to be 8 months (54). High KPS score is a significantindicator of outcome in recurrent GBM patients undergoing
Cancer Investigation
Can
cer
Inve
st D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y L
ulea
Uni
vers
ity O
f T
echn
olog
y on
09/
19/1
3Fo
r pe
rson
al u
se o
nly.
Predictors of Long-Term Survival in GBM Patients
Table 4. Articles Reviewed on Patient Age-Related Predictors of Survival in GBM Patients
Author Year CountryNo. of
Patients Major Finding Survival Time
Patient Age Predictors That Increase SurvivalEwelt et al. (43) 2011 Germany 103 Elderly (>65years) benefit
from intense procedures& Rx
Surgery only/surgery & RT/surgery & RTC has OS of2.2/4.4/15.0 mo.,respectively.
Iwamoto et al. (44) 2009 USA 394 Aggressive Rx with resection& RCT in elderly
55% decrease in the risk ofdeath for patients on RCTcompared with RT alone
Barnholtz-Sloan et al. (40) 2008 USA 1753 Surgery and RT increasessurvival in elderly(≥75 years)
Surgery and RCT MST 9mo. vs. MST surgery/Rxonly 2 mo.
Kleinschmidt-DeMasterset al. (46)
2005 USA 20 EGFR amplification isfavorable in the elderly(>75 years)
EGFR gene amplificationMST 10.5 mo. vs.non-EGFR amplificationMST 2.0 mo.
Barker et al. (41) 2001 USA 223 RT outcome improved inelderly with high KPS andmax resection
Mohan et al. (42) 1998 USA 102 Elderly GBM patients withhigh KPS with aggressiveRx
Aggressive Rx MST 7.4 mo.vs. nonaggressive Rx MST2.4 mo.
Patient Age Predictors That Do Not Significantly Affect SurvivalChaichana et al. (45) 2011 USA 129 Elderly (>65 years) with
multiple risk factorsMST with no. of risk factors
= 1/9.2 mo., 2–3/5.5 mo.,4–6/4.4 mo.
Veilleux et al. (47) 2010 Canada 130 Perspective of quality oflife/health
Muacevic and Kreth (49) 2003 Germany 123 Quality decreases after Rx inelderly
OS is 24 wks. QAS is 10.5wks
Meyers et al. (48) 2000 USA 80 QOL and ADL
wks = weeks, mo. = months., MST = mean survival time, PFS = progression-free survival, OS = overall survival, RT = radiotherapy, CT = chemotherapy, RCT = combinedradio & chemotherapy, Karnofsky performance status = KPS, QOL = quality of living, ADL = activities of daily living, QAS = quality adjusted survival analysis.
reirradiation (55). In addition, at reoperation patients whopresented with RT necrosis were found to have increasedsurvival, compared with those without RT necrosis. Sur-vival in these patients is further improved by concomitanttreatment with TMZ chemotherapy (56). One study demon-strated an increased risk for communicating hydrocephalusin recurrent GBM patients who had underwent at least twocraniotomies for tumor resection. These patients needed toreceive additional shunt surgery. The study identified ven-tricular opening at surgery after RCT and high cerebrospinalfluid (CSF) protein levels as significant predictors for thedevelopment of communicating hydrocephalus in thesepatients (57).
In GBM patients who have already received radiationtherapy for their initial treatment, brachytherapy to treat tu-mor recurrence has been shown to increase survival time.Unlike external beam radiation therapy, which delivers radi-ation to the tumor from outside the body, brachytherapy in-volves the implantation of radiation source inside or adjacentto the site requiring treatment. Age and high KPS score aregood prognostic indicators of survival time with brachyther-apy not only in recurrent GBM patients, but also in patientswith a new GBM or other malignant gliomas (58). Recur-rent GBM patients who received interstitial brachytherapyhad an MST of 62.9 weeks compared with 37.1 weeks forthose patients who did not receive additional treatment (59).
Also, smaller recurrent tumor volume (≤30 cm3) is a betterprognostic indicator for brachytherapy and associated withhigher quality of survival compared with patients with largervolumes (60). Similarly, patients with recurrent tumors ofsmaller volumes (<10 cm3) were found to have more favor-able response to chemotherapy and better outcome (61). Re-current GBM patients who undergo reirradiation have signif-icantly increased survival times compared with patients whodo not undergo this procedure (62). See Table 6.
It is important to note that additional indictors for suc-cessful GBM therapy in patients who undergo these thera-pies. For instance, a patient who receives bevacizumab is alsosomeone who does not have a tendency or history of bleed-ing diathesis or DVT. In addition, a patient who receives Gli-adel wafers or brachytherapy is someone who has a cavityamenable to such placement. There are also mixed reports re-garding cognitive status of patients receiving RT. Generally,it is accepted that GBM patients exhibit a steady decline incognitive functioning but whether additional decline followsRT therapy remains to be disputed or on a case by case sce-nario. Some studies have even shown that there is no signif-icant cognitive decline after receiving RT and chemotherapyin patient with 6-month PFS (63) or in patients who receiveescalating doses of radiation (64). It is recognized that manystudies regarding cognition status in patients after therapyhave limited global applicability due to individual differences
Copyright C© 2013 Informa Healthcare USA, Inc.
Can
cer
Inve
st D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y L
ulea
Uni
vers
ity O
f T
echn
olog
y on
09/
19/1
3Fo
r pe
rson
al u
se o
nly.
N. S. Chaudhry et al.
Table 5. Articles Reviewed on Reoperated/Recurrent Tumor Predictors of Survival in GBM Patients
Author Year CountryNo. of
Patients Major Finding Survival Time
Recurrent/Reoperated Patient Predictors That Increase SurvivalPrados et al. (53) 2011 USA 167 Recurrent patients have increased
response to bevacizumab42% of patients had 6-mo. PFS
Rusthoven et al. (56) 2011 USA 51 At reoperation, patients with RTnecrosis have improved survival
Reoperation with RT necrosisMST 21.8 mo. vs. RCT withoutnecrosis 7.0 mo.
Tugcu et al. (2) 2010 Turkey 50 Reoperation increases prognosis Reoperation MST 9.64 mo. vs. noreoperation MST 6.86 mo.
Fokas et al. (55) 2009 Germany 53 High KP score is best indicator foroutcome in
Post-hFSRT MST 9 mo.
Combs et al. (54) 2005 Germany 59 FSRT reirradiation Rx Median survival reirradiation 8mo.
Keles et al. (61) 2004 USA 119 Smaller VRD in recurrent GBMsthat start chemo
MST 29 wks.
Simon et al. (60) 2002 France 42 Low tumor volume (<30 cm3) forbrachytherapy
Low volume MST 14 mo. vs.larger volume 5.5 mo.
Mayr et al. (59) 2002 USA 73 Age and high KPS increasesurvival with brachytherapy
Brachytherapy MST 62.9 wks vs.nonbrachytherapy 37.1 wks
Azizi et al. (3) 2001 USA 112 Repeated surgicaldebulking/resection increasesurvival in GBM
Biopsy only MST 393 days. 1Resection MST 380 days. 2 or 3resection MST 548 days.
Bernstein et al. (58) 1990 Canada 46 Interstitial brachytherapyincreases survival in malignantgliomas
MST 44 wks for the recurrentpatients
Leibel et al. (62) 1989 USA 45 Interstitial brachytherapyincreases survival in malignantgliomas
At 18 mo., 33 of the patients alive.At 36 mo., 18 patients alive
Recurrent/Reoperated Patient Predictors that Decrease SurvivalMontano et al. (57) 2011 Italy 124 Communicating hydrocephalus
after surg/chemo in reoperatedpatients
Median OS after VP shunt surgery5 ± 2.9 mo.
Garcia-Navarrete et al. (50) 2010 Mexico 14 HGF in CSF (893 ± 157 pg/mL) MST 10 mo.Ljubimova et al. (51) 2004 USA 67 Laminin 8 expression is associated
with recurrence in GBMRecurrent/Reoperated
Patient Predictors ThatDo Not SignificantlyAffect Survival
Hilverda et al. (63) 2010 Netherlands 13 No significant cognitive declineafter receiving RCT in patientwith 6-mo. PFS
Corn et al. (64) 2009 Israel No cognitive decline withincreasing doses
Brown et al. (52) 1995 USA 3921 Collins’ law application topediatric GBM tumors
wks = weeks, mo. = months, MST = mean survival time, PFS = progression-free survival, OS = overall survival, RT = radiotherapy, CT = chemotherapy, RCT = combinedradio & chemotherapy, Karnofsky performance status = KPS, FSRT = fractionated stereotactic reirradiation, hFSRT = hypofractionated stereotactic reirradiation.
of patients and confounding variables (i.e., sample size, age,doses, volume). There is a need for better tests to assess cog-nitive function in these patients and would need to take intoaccount patients age and education (Table 5).
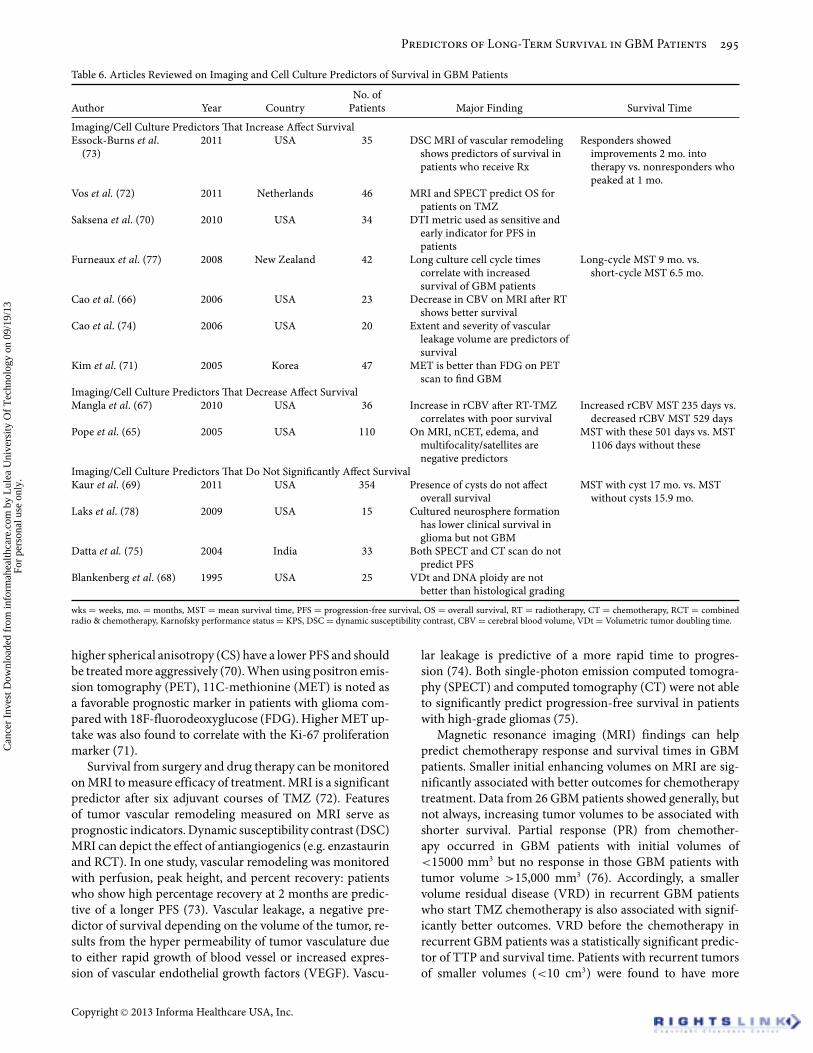
Imaging characteristics & cell culturesPrognostic indicators for survival in GBM patients can berevealed on tumor imaging. Noncontrast enhancing tumor,edema, satellites, and multifocality on MRI are significantnegative prognostic indicators (16286386,65). A decrease incerebral blood volume (CBV) on MRI perfusion studies af-ter RT is associated with better outcomes (66). Conversely, ahigh percentage change in relative CBV after 1 month of RCTis strong predictive of low survival; however, the extent of tu-
mor progression is not significantly correlated with survival(67). Volume doubling time (VDt) by CT or MRI and DNAploidy by image analysis were better indicators for survivalthan histological grading in patients with low-grade tumorsbut not for patients with GBM (68). The presence of cysts inGBM patients was not found to be a significant predictor ofoutcome in GBM patients (cystic GBM patients MST of 17months vs. noncystic GBM MST of 15.9 months) (69).
MRI diffuse tensor imaging (DTI), used to localize tumorsby measuring differences in the diffusion of water in vari-ous areas of the brain, has also proved to be a sensitive andearly indicator for PFS in GBM patient. High-grade gliomapatients with a low fractional anisotropy (FA), low apparentdiffusion coefficient (ADC), low planar anisotropy (CP), and
Cancer Investigation
Can
cer
Inve
st D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y L
ulea
Uni
vers
ity O
f T
echn
olog
y on
09/
19/1
3Fo
r pe
rson
al u
se o
nly.
Predictors of Long-Term Survival in GBM Patients
Table 6. Articles Reviewed on Imaging and Cell Culture Predictors of Survival in GBM Patients
Author Year CountryNo. of
Patients Major Finding Survival Time
Imaging/Cell Culture Predictors That Increase Affect SurvivalEssock-Burns et al.
(73)2011 USA 35 DSC MRI of vascular remodeling
shows predictors of survival inpatients who receive Rx
Responders showedimprovements 2 mo. intotherapy vs. nonresponders whopeaked at 1 mo.
Vos et al. (72) 2011 Netherlands 46 MRI and SPECT predict OS forpatients on TMZ
Saksena et al. (70) 2010 USA 34 DTI metric used as sensitive andearly indicator for PFS inpatients
Furneaux et al. (77) 2008 New Zealand 42 Long culture cell cycle timescorrelate with increasedsurvival of GBM patients
Long-cycle MST 9 mo. vs.short-cycle MST 6.5 mo.
Cao et al. (66) 2006 USA 23 Decrease in CBV on MRI after RTshows better survival
Cao et al. (74) 2006 USA 20 Extent and severity of vascularleakage volume are predictors ofsurvival
Kim et al. (71) 2005 Korea 47 MET is better than FDG on PETscan to find GBM
Imaging/Cell Culture Predictors That Decrease Affect SurvivalMangla et al. (67) 2010 USA 36 Increase in rCBV after RT-TMZ
correlates with poor survivalIncreased rCBV MST 235 days vs.
decreased rCBV MST 529 daysPope et al. (65) 2005 USA 110 On MRI, nCET, edema, and
multifocality/satellites arenegative predictors
MST with these 501 days vs. MST1106 days without these
Imaging/Cell Culture Predictors That Do Not Significantly Affect SurvivalKaur et al. (69) 2011 USA 354 Presence of cysts do not affect
overall survivalMST with cyst 17 mo. vs. MST
without cysts 15.9 mo.Laks et al. (78) 2009 USA 15 Cultured neurosphere formation
has lower clinical survival inglioma but not GBM
Datta et al. (75) 2004 India 33 Both SPECT and CT scan do notpredict PFS
Blankenberg et al. (68) 1995 USA 25 VDt and DNA ploidy are notbetter than histological grading
wks = weeks, mo. = months, MST = mean survival time, PFS = progression-free survival, OS = overall survival, RT = radiotherapy, CT = chemotherapy, RCT = combinedradio & chemotherapy, Karnofsky performance status = KPS, DSC = dynamic susceptibility contrast, CBV = cerebral blood volume, VDt = Volumetric tumor doubling time.
higher spherical anisotropy (CS) have a lower PFS and shouldbe treated more aggressively (70). When using positron emis-sion tomography (PET), 11C-methionine (MET) is noted asa favorable prognostic marker in patients with glioma com-pared with 18F-fluorodeoxyglucose (FDG). Higher MET up-take was also found to correlate with the Ki-67 proliferationmarker (71).
Survival from surgery and drug therapy can be monitoredon MRI to measure efficacy of treatment. MRI is a significantpredictor after six adjuvant courses of TMZ (72). Featuresof tumor vascular remodeling measured on MRI serve asprognostic indicators. Dynamic susceptibility contrast (DSC)MRI can depict the effect of antiangiogenics (e.g. enzastaurinand RCT). In one study, vascular remodeling was monitoredwith perfusion, peak height, and percent recovery: patientswho show high percentage recovery at 2 months are predic-tive of a longer PFS (73). Vascular leakage, a negative pre-dictor of survival depending on the volume of the tumor, re-sults from the hyper permeability of tumor vasculature dueto either rapid growth of blood vessel or increased expres-sion of vascular endothelial growth factors (VEGF). Vascu-
lar leakage is predictive of a more rapid time to progres-sion (74). Both single-photon emission computed tomogra-phy (SPECT) and computed tomography (CT) were not ableto significantly predict progression-free survival in patientswith high-grade gliomas (75).
Magnetic resonance imaging (MRI) findings can helppredict chemotherapy response and survival times in GBMpatients. Smaller initial enhancing volumes on MRI are sig-nificantly associated with better outcomes for chemotherapytreatment. Data from 26 GBM patients showed generally, butnot always, increasing tumor volumes to be associated withshorter survival. Partial response (PR) from chemother-apy occurred in GBM patients with initial volumes of<15000 mm3 but no response in those GBM patients withtumor volume >15,000 mm3 (76). Accordingly, a smallervolume residual disease (VRD) in recurrent GBM patientswho start TMZ chemotherapy is also associated with signif-icantly better outcomes. VRD before the chemotherapy inrecurrent GBM patients was a statistically significant predic-tor of TTP and survival time. Patients with recurrent tumorsof smaller volumes (<10 cm3) were found to have more
Copyright C© 2013 Informa Healthcare USA, Inc.
Can
cer
Inve
st D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y L
ulea
Uni
vers
ity O
f T
echn
olog
y on
09/
19/1
3Fo
r pe
rson
al u
se o
nly.

N. S. Chaudhry et al.
Table 7. Articles Reviewed on Serum Marker Predictors of Survival in GBM Patients
Author Year CountryNo. of
Patients Major Finding Survival Time
Serum Marker Predictors That Increase SurvivalCrocker,et al. (82) 2011 UK 36 Low TIMP1Colin et al. (90) 2009 France 69 Cathepsin B, PAI-1, MMP9Petrik et al. (91) 2008 UK 72 Normal levels of serum AHSG
predict survival in GBMHormigo et al. (84) 2006 USA 76 Low YKL40 and MMP9Serum Marker Predictors That Decrease SurvivalBorg et al. (81) 2011 UK 549 Preoperative hypoalbuminemia
(<30 g/L)Postop hypoalbuminemia MST 2.3
mo. vs. normal albumin levelMST 5.6 mo.Also, with normal albumin, lower
levels (30–40 g/L) MST 5.1 mo.vs. upper levels (40–50 g/L)MST 8.8 mo.
Hoke et al. (79) 2011 Austria 23 High d-dimerGarcia-Navarrete et al. (50) 2010 Mexico 52 HGF in CSF MST 10 mo. 893 ± 157 pg/mL of
HGF in GBMBrockmann et al. (80) 2007 Germany 153 Preop thrombocytosis (>400
platelets/nL)Thrombocytosis is platelets >400
platelets/nLFlannery et al. (87) 2006 UK 51 Cathepsin SPelloski et al. (83) 2005 USA 287 YKL40Fukuda et al. (86) 2005 Japan 87 Cathepsin DPeles et al. (88) 2004 Israel 26 bFGF & VEGF in CSFStrojnik et al. (85) 1999 Slovenia 100 Cathepsin B
wks = weeks, mo. = months, MST = mean survival time, PFS = progression-free survival, OS = overall survival, RT = radiotherapy, CT = chemotherapy, RCT = combinedradio & chemotherapy, Karnofsky performance status = KPS.
favorable response to chemotherapy and better outcome.Data revealed that for every 1 cm3 of residual disease therewas a 1.04-fold higher risk of death (61) (Table 6).
Cell cultures of tumor samples taken from GBM patientsmay also reveal survival predictors. Tumors appear to retaincytokinetic characteristic when transferred to culture. Onestudy showed short-term GBM culture samples that tookgreater than 10 days to grow correlated with longer survivalin certain gliomas (77). Also, cultures that formed neuro-spheres were predictive of low clinical survival. Neurospheresare likened to neural stem cells from brain tumors, such asGBM, that are able to self-replicate. Grade I, II, and III glialtumors of patients capable of producing neurospheres in cellculture resulted in decreased time to progression and in-creased risk of death for the patient, but no significance wasfound for GBM samples (78) (Table 6).
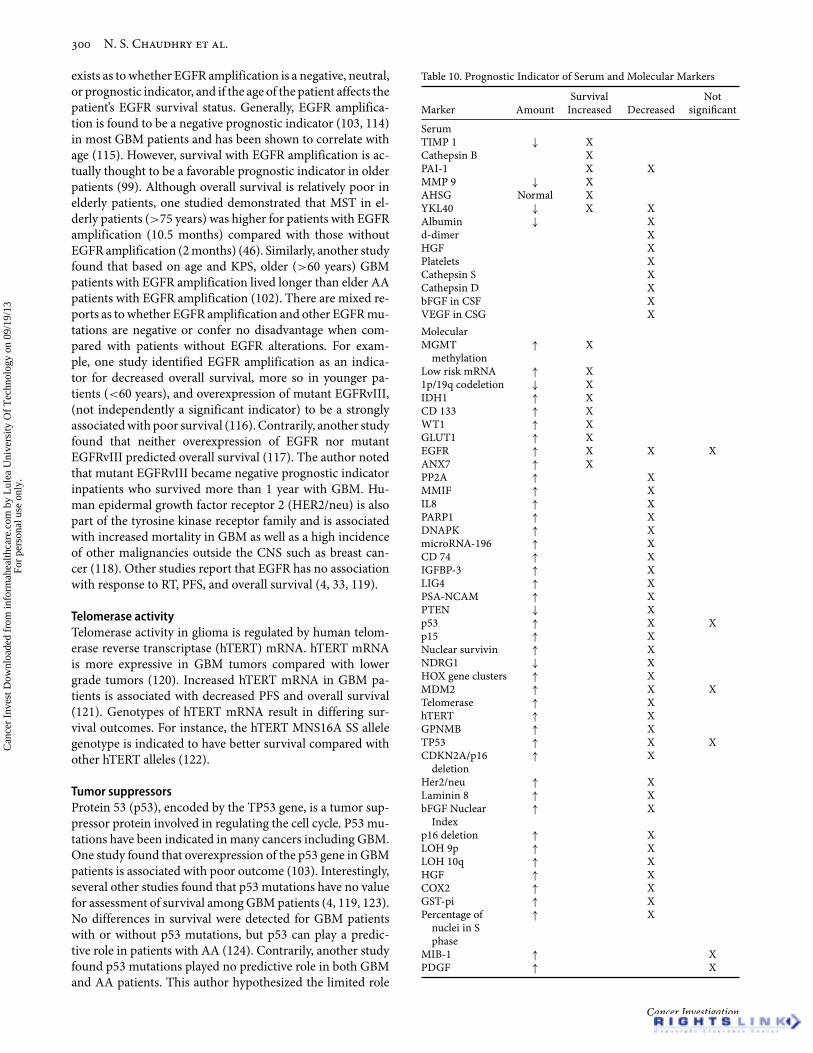
Serum markersAlthough not specific, the concentration of certain sub-stances in the serum of GBM patients can serve as markersfor predicting survival (Table 7). Elevation of D-dimers, pro-tein degradation products from fibrinolysis of blood clots, isfrom the hypercoagulable state in GBM patients. D-dimersare associated with increased risk of thromboembolism andmortality compared with GBM patients with normal lev-els of d-dimers (79). Preoperative thrombocytosis (>400platelets/nL) is also associated with poor survival (80). GBMpatients with hypoalbuminemia (<30 g/L) have a lower sur-vival (MST of 5.1 months) compared with patients with albu-min in the upper normal range (40–50 g/L; MST 8.8 months)(81).
TIMP 1Tissue inhibitor of metalloproteinases (TIMP1) inhibitsmatrix metalloproteinases (MMP) in an effort to promotecellular proliferation and antiapoptotic activities. Interest-ingly, low serum TIMP1 is associated with longer survivalin GBM patients (82). This significant inverse relationshipbetween TIMP1 and MMPs suggests that TIMP1 may play arole beyond solely inhibiting MMPs, and for some reason alow concentration of TIMP1 in patients plays a stronger rolein increasing survival. GBM patients with no radiographicevidence of disease have lower levels of MMP9 and YKL40compared with patients with active disease. YKL40 is alsoassociated with poor response to radiation, chromosome 10qloss, and poor survival (83). MMP9 and YKL40 are highlyexpressed in malignant gliomas thus low levels of thesesubstances can be used to assay the absence of disease (84).
CathepsinsCathepsins are proteases overexpressed in cancerous statesand involved in destructive activity. High-grade gliomashave higher levels of cathepsins. Cathepsin B (85), cathepsinD (86), and cathepsin S (87) are found to be highly expressedin GBM patients and serve as significant predictors forshorter survival. One study compared GBM patients withGrade 1 pilocytic astrocytoma patients and found cathepsinB and plasminogen activator inhibitor 1 (PAI1) significantlymore expressed in the GBM patients. Cathepsin B, a cysteineendopeptidase, heavily stains endothelial cells of the GBMtumor, which suggests a role in angiogenesis and invasion.It also has cytokines and growth factors that allow for
Cancer Investigation
Can
cer
Inve
st D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y L
ulea
Uni
vers
ity O
f T
echn
olog
y on
09/
19/1
3Fo
r pe
rson
al u
se o
nly.

Predictors of Long-Term Survival in GBM Patients
communication between the tumor and environment toprovide drug resistance.
Other proteinsHigh concentrations of basic fibroblast growth factor (bFGF)and VEGF in the CSF is found in high-grade glioma patientsand associated with negative outcomes compared with low-grade gliomas (88). Similarly, nuclear accumulation of bFGFhas a negative influence on survival rate, and its presenceis significantly indicated in recurrence of pituitary adenoma(89).
PAI1 was found in microvascular proliferating cells andpseudopalisading cells near necrotic tissue. MMP9, but notp53 suppressor MMP2, is also a biomarker of poor outcomefor GBM patients in this study (90).
Levels of B-chain of alpha 2-Heremans–Schmid glycopro-tein (AHSG) inversely correlate with tumor grade. Patientswith normal, as opposed to low levels, of AHSG are predictedto live longer (91).
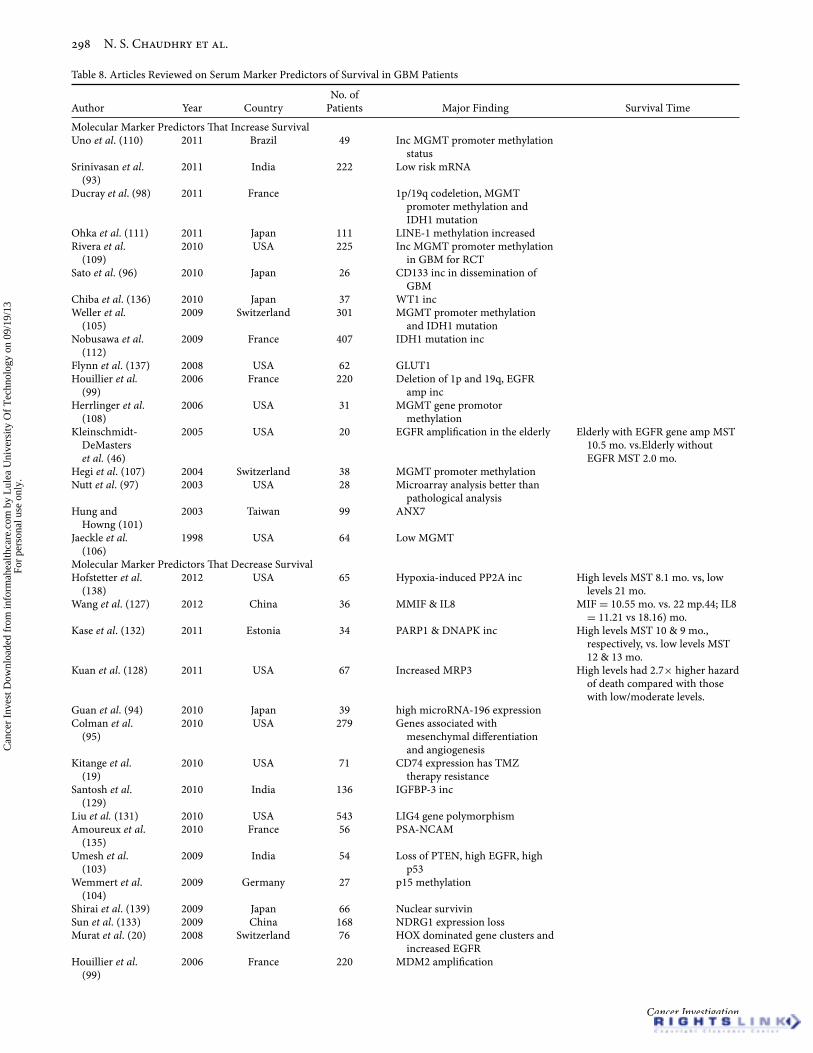
Molecular markersAdvances in genetic technology have led to the discoveryof many biological markers that are either overexpressed orunderexpressed in disease processes (Table 8). Traditionally,GBM prognosis has been predicted by outcomes from his-tological grading, surgery, response to RCT, MRI features,and serum plasma and/or CSF proteins. However, patientswith GBM are also found to express certain genes and otherbiomarkers distinct from lower grade gliomas and otherpathologies. For instance, one study found a higher percent-age of nuclei in the S phase of DNA in GBM patients cor-related with poor survival (92). Microarray analysis of GBMhas revealed there are certain microRNA (miRNA) expres-sions unique to GBM. One study claimed that certain sub-sets of miRNAs, when expressed in GBM, correlate to highersurvival than other miRNA subsets (93). Another study asso-ciated a high expression of miRNA-196 expression in GBMpatients to be with poor survival when compared with AAand normal brain patients (94). Also, overexpression of mi-croarray gene sets associated with mesenchymal differenti-ation and angiogenesis in GBM patients are indicative of apoor prognosis (95). HOX dominated gene clusters, includ-ing those with prominin-1 (CD133), are poor predictors ofsurvival in patients (20). CD133 is also predictive of dissem-ination in GBM, a rare entity with increasing incidence per-haps due to longer survival in GBM patients (96). One studygathered data on 28 diagnostically challenging glioma pa-tients and found that molecular profiling with microarrayanalysis was more predictive of survival than when the samepatients were analyzed pathologically (97).
Chromosomal alterationsAside from microRNA expressions, there are many otherbiomarkers that have been indicated as predictors of survivalfor GBM patients. We will discuss various markers that pre-dict survival published in the literature dating from 1993 tothe December 2011 (Table 9).
Alterations of chromosome 1, 9, 10, and 19 are associ-ated with survival indicators in GBM patients. Patients withcodeletion of 1p and 19q have an increased response to treat-ment (98) and favorable outcomes (99). Decreased survival isassociated with loss of heterozygosity (LOH) in chromosome9p and 10q (100). Annexin VII (ANX7), a gene on chromo-some 10q21 related to the function of tumor suppressors, isassociated with longer survival (101). Phosphate and tensinhomolog (PTEN) is a tumor suppressor gene also found onchromosome 10. One role of PTEN is to inhibit pathwaysleading to formation of antiapoptotic bcl2. PTEN mutation,also found in prostate cancer, occurs more often in GBM thanlower grade gliomas (102) and is a predictor of poor outcome(103). Furthermore, deletion of chromosome 10q occurs sig-nificantly more often in GBM compared with AA, but it doesnot solely predict survival (102). One study also found cyclic-dependent kinase inhibitor 2B or multiple tumor suppressor2 (CDKN2B/p15/MTS2) methylation to be a poor predictorfor survival in GBM patients; however, contrary to severalother studies, this author’s findings indicate no significancefor MST in patients with MGMT methylation treated withTMZ therapy (104). Other tumor suppressors such as p53and CDKN2A/p16/MTS1 play a role in regulating the cellcycle but have not been shown as significant predictors forsurvival (33, 100,105).
Gene methylations & mutationsA high level of MGMT in GBM patients is correlated withpoor survival compared with patients with low levels ofMGMT (106). As discussed earlier, presence of MGMT inGBM patients makes them resistant to TMZ therapy. Thus in-activation by promoter methylation of the MGMT gene is as-sociated with longer survival in patients (107, 108) as well asincreased sensitivity to TMZ therapy and RT. NonmethylatedMGMT tumors progress twice as fast during RT than thosepatients with promoter methylated MGMT tumors (109).MGMT promoter methylation status is a more significantand reliable prognostic indicator than MGMT gene or pro-tein expression levels for adjuvant therapy (110). Long inter-spersed nuclear element-1 (LINE1) methylation status is an-other marker of DNA methylation. LINE1 hypomethylationhas been implicated with a poor prognosis in various cancers.Higher levels of LINE1 methylation are found in lower gradegliomas compared with higher grade gliomas and GBM.LINE1 is directly proportional to MGMT methylation, thushigher levels of LINE1 methylation in GBM patients corre-late with a favorable prognosis and increased overall survival(111). Isocitrate dehydrogenase 1 (IDH1) mutations are alsoindicated in increased survival in GBM patients. IDH1 mu-tations can be used to classify patients because they are com-monly found in secondary GBM patients, who seem to beyounger patients compared with those with EGFR amplifica-tion (112). Patients MGMT promoter methylation and IDH1mutation have increased PFS and overall survival (98, 105).
Mutations leading to the overexpression of EGFR, a tyro-sine kinase cell membrane receptor, are implicated in a vari-ety of cancers including GBM (113); however, its prognosticrole in the clinical realm is unclear and debated. Controversy
Copyright C© 2013 Informa Healthcare USA, Inc.
Can
cer
Inve
st D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y L
ulea
Uni
vers
ity O
f T
echn
olog
y on
09/
19/1
3Fo
r pe
rson
al u
se o
nly.
N. S. Chaudhry et al.
Table 8. Articles Reviewed on Serum Marker Predictors of Survival in GBM Patients
Author Year CountryNo. of
Patients Major Finding Survival Time
Molecular Marker Predictors That Increase SurvivalUno et al. (110) 2011 Brazil 49 Inc MGMT promoter methylation
statusSrinivasan et al.
(93)2011 India 222 Low risk mRNA
Ducray et al. (98) 2011 France 1p/19q codeletion, MGMTpromoter methylation andIDH1 mutation
Ohka et al. (111) 2011 Japan 111 LINE-1 methylation increasedRivera et al.
(109)2010 USA 225 Inc MGMT promoter methylation
in GBM for RCTSato et al. (96) 2010 Japan 26 CD133 inc in dissemination of
GBMChiba et al. (136) 2010 Japan 37 WT1 incWeller et al.
(105)2009 Switzerland 301 MGMT promoter methylation
and IDH1 mutationNobusawa et al.
(112)2009 France 407 IDH1 mutation inc
Flynn et al. (137) 2008 USA 62 GLUT1Houillier et al.
(99)2006 France 220 Deletion of 1p and 19q, EGFR
amp incHerrlinger et al.
(108)2006 USA 31 MGMT gene promotor
methylationKleinschmidt-
DeMasterset al. (46)
2005 USA 20 EGFR amplification in the elderly Elderly with EGFR gene amp MST10.5 mo. vs.Elderly withoutEGFR MST 2.0 mo.
Hegi et al. (107) 2004 Switzerland 38 MGMT promoter methylationNutt et al. (97) 2003 USA 28 Microarray analysis better than
pathological analysisHung and
Howng (101)2003 Taiwan 99 ANX7
Jaeckle et al.(106)
1998 USA 64 Low MGMT
Molecular Marker Predictors That Decrease SurvivalHofstetter et al.
(138)2012 USA 65 Hypoxia-induced PP2A inc High levels MST 8.1 mo. vs, low
levels 21 mo.Wang et al. (127) 2012 China 36 MMIF & IL8 MIF = 10.55 mo. vs. 22 mp.44; IL8
= 11.21 vs 18.16) mo.Kase et al. (132) 2011 Estonia 34 PARP1 & DNAPK inc High levels MST 10 & 9 mo.,
respectively, vs. low levels MST12 & 13 mo.
Kuan et al. (128) 2011 USA 67 Increased MRP3 High levels had 2.7× higher hazardof death compared with thosewith low/moderate levels.
Guan et al. (94) 2010 Japan 39 high microRNA-196 expressionColman et al.
(95)2010 USA 279 Genes associated with
mesenchymal differentiationand angiogenesis
Kitange et al.(19)
2010 USA 71 CD74 expression has TMZtherapy resistance
Santosh et al.(129)
2010 India 136 IGFBP-3 inc
Liu et al. (131) 2010 USA 543 LIG4 gene polymorphismAmoureux et al.
(135)2010 France 56 PSA-NCAM
Umesh et al.(103)
2009 India 54 Loss of PTEN, high EGFR, highp53
Wemmert et al.(104)
2009 Germany 27 p15 methylation
Shirai et al. (139) 2009 Japan 66 Nuclear survivinSun et al. (133) 2009 China 168 NDRG1 expression lossMurat et al. (20) 2008 Switzerland 76 HOX dominated gene clusters and
increased EGFRHouillier et al.
(99)2006 France 220 MDM2 amplification
Cancer Investigation
Can
cer
Inve
st D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y L
ulea
Uni
vers
ity O
f T
echn
olog
y on
09/
19/1
3Fo
r pe
rson
al u
se o
nly.
Predictors of Long-Term Survival in GBM Patients
Boldrini et al.(121)
2006 Italy 42 Telomerase activity and hTERTmRNA
Wang et al. (122) 2006 USA 299 Certain hTERT mRNA have worsesurvival outcomes than others
hTERT MNS16A SS allele genotypehas better survival than otheralleles
Kuan et al. (134) 2006 USA 50 Increased GPNMB (3× > normal)Shih et al. (33) 2005 USA 75 TP53 mutations and
CDKN2A/p16 deletion inresponse to RT
Potti et al. (118) 2004 USA 347 HER2/neu overexpressionLjubimova et al.
(51)2004 USA 67 Laminin 8
Shinojima et al.(116)
2003 Japan 87 EGFRvIII mutation with EGFRamplification
Tchirkov et al.(120)
2003 France 70 Increased hTERT mRNA
Fukui et al. (89) 2003 Japan 52 High bFGF Nuclear IndexRasheed et al.
(100)2002 USA 100 p16 deletion, LOH 9p, and LOH
10qArrieta et al.
(126)2002 Mexico 62 HGF
Smith et al. (102) 2001 USA 174 Loss of PTEN, p53 mutation, 10qdeletion
Shono et al.(140)
2001 USA 66 Increased COX2
Frederick et al.(113)
2000 USA 48 EGFR mutations with EGFRamplification
Etienne et al.(115)
1998 France 79 EGFR amplification
Ali-Osman et al.(130)
1997 USA 61 high GST-pi
Zhu et al. (114) 1996 USA 71 EGFR amplificationMcKeever et al.
(92)1990 USA 9 Increased % of nuclei with S phase
Molecular Marker Predictors That Do Not Significantly Affect SurvivalChiba et al. (136) 2010 Japan 37 MIB-1Donato et al. (4) 2007 Italy 43 P53, PDGF, and EGFRHeimberger
et al. (117)2005 USA 196 Neither wild-type EGFR nor
mutant EGFRvIII predictsurvival
Shih et al. (33) 2005 USA 75 EGFR has no association withresponse to RT, PFS, or OS
Stark et al. (119) 2003 Germany 143 p53, EGFR, MDM2 have no effecton survival
Rasheed et al.(100)
2002 USA 100 TP53 mutations
Smith et al. (102) 2001 USA 174 EGFR amplificationKyritsis et al.
(124)1995 USA 122 p53
Ellison et al.(123)
1995 UK 68 p53
Chozick et al.(125)
1994 USA 149 p53
wks = weeks, mo. = months, MST = mean survival time, PFS = progression-free survival, OS = overall survival, RT = radiotherapy, CT = chemotherapy, RCT = combinedradio & chemotherapy, Karnofsky performance status = KPS, amp = amplification, inc = increase, dec = decrease.
Table 9. Molecular Markers Reviewed
ANX7 DNAPKBiomarkers
hTERT LINE1 p15 PSA-NCAM
BrdU EGFR IDH1 MDM2 p16 PTENCD133 GLUT1 idU MGMT p53 SF2CD74 GST-pi IGFBP3 MIB1 PARP1 TP53CDKN2A HER2 Laminin 8 MRP3 PDGF WT1COX2 HGF LIG4 Msh2 PP2A Ch deletion (1, 9, 10, 19)
Copyright C© 2013 Informa Healthcare USA, Inc.
Can
cer
Inve
st D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y L
ulea
Uni
vers
ity O
f T
echn
olog
y on
09/
19/1
3Fo
r pe
rson
al u
se o
nly.
N. S. Chaudhry et al.
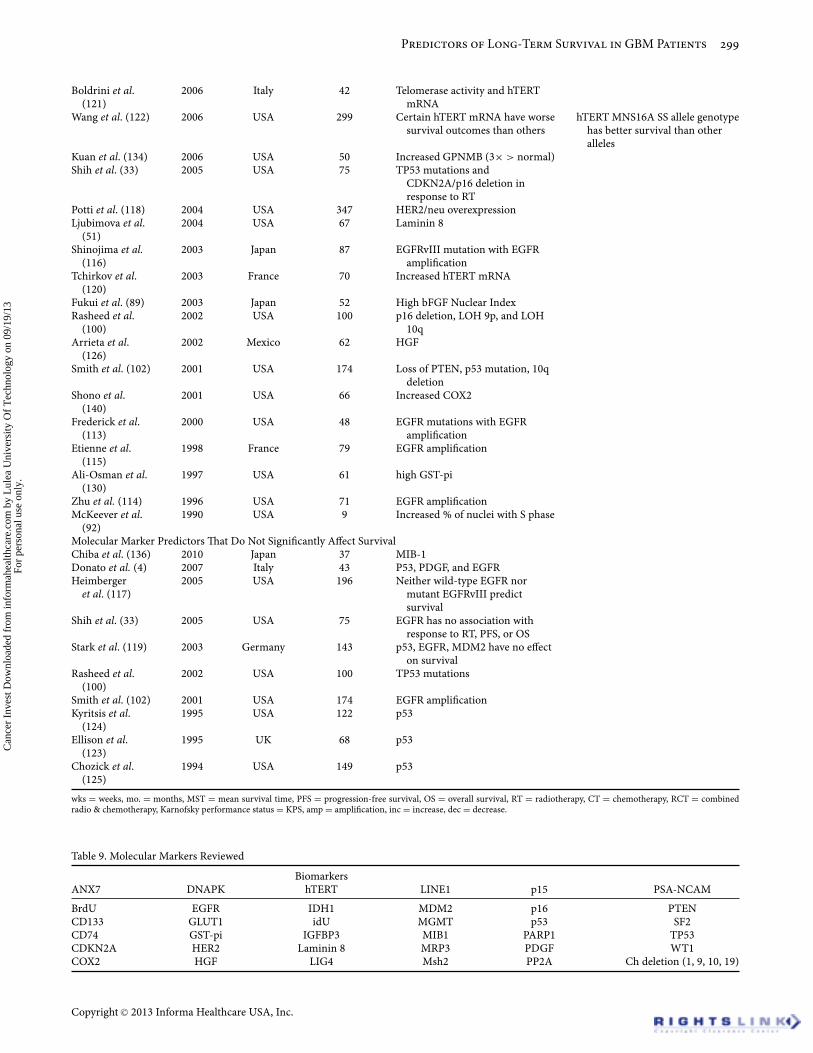
exists as to whether EGFR amplification is a negative, neutral,or prognostic indicator, and if the age of the patient affects thepatient’s EGFR survival status. Generally, EGFR amplifica-tion is found to be a negative prognostic indicator (103, 114)in most GBM patients and has been shown to correlate withage (115). However, survival with EGFR amplification is ac-tually thought to be a favorable prognostic indicator in olderpatients (99). Although overall survival is relatively poor inelderly patients, one studied demonstrated that MST in el-derly patients (>75 years) was higher for patients with EGFRamplification (10.5 months) compared with those withoutEGFR amplification (2 months) (46). Similarly, another studyfound that based on age and KPS, older (>60 years) GBMpatients with EGFR amplification lived longer than elder AApatients with EGFR amplification (102). There are mixed re-ports as to whether EGFR amplification and other EGFR mu-tations are negative or confer no disadvantage when com-pared with patients without EGFR alterations. For exam-ple, one study identified EGFR amplification as an indica-tor for decreased overall survival, more so in younger pa-tients (<60 years), and overexpression of mutant EGFRvIII,(not independently a significant indicator) to be a stronglyassociated with poor survival (116). Contrarily, another studyfound that neither overexpression of EGFR nor mutantEGFRvIII predicted overall survival (117). The author notedthat mutant EGFRvIII became negative prognostic indicatorinpatients who survived more than 1 year with GBM. Hu-man epidermal growth factor receptor 2 (HER2/neu) is alsopart of the tyrosine kinase receptor family and is associatedwith increased mortality in GBM as well as a high incidenceof other malignancies outside the CNS such as breast can-cer (118). Other studies report that EGFR has no associationwith response to RT, PFS, and overall survival (4, 33, 119).
Telomerase activityTelomerase activity in glioma is regulated by human telom-erase reverse transcriptase (hTERT) mRNA. hTERT mRNAis more expressive in GBM tumors compared with lowergrade tumors (120). Increased hTERT mRNA in GBM pa-tients is associated with decreased PFS and overall survival(121). Genotypes of hTERT mRNA result in differing sur-vival outcomes. For instance, the hTERT MNS16A SS allelegenotype is indicated to have better survival compared withother hTERT alleles (122).
Tumor suppressorsProtein 53 (p53), encoded by the TP53 gene, is a tumor sup-pressor protein involved in regulating the cell cycle. P53 mu-tations have been indicated in many cancers including GBM.One study found that overexpression of the p53 gene in GBMpatients is associated with poor outcome (103). Interestingly,several other studies found that p53 mutations have no valuefor assessment of survival among GBM patients (4, 119, 123).No differences in survival were detected for GBM patientswith or without p53 mutations, but p53 can play a predic-tive role in patients with AA (124). Contrarily, another studyfound p53 mutations played no predictive role in both GBMand AA patients. This author hypothesized the limited role
Table 10. Prognostic Indicator of Serum and Molecular Markers
Marker AmountSurvival
Increased DecreasedNot
significant
SerumTIMP 1 ↓ XCathepsin B XPAI-1 X XMMP 9 ↓ XAHSG Normal XYKL40 ↓ X XAlbumin ↓ Xd-dimer XHGF XPlatelets XCathepsin S XCathepsin D XbFGF in CSF XVEGF in CSG XMolecularMGMT
methylation↑ X
Low risk mRNA ↑ X1p/19q codeletion ↓ XIDH1 ↑ XCD 133 ↑ XWT1 ↑ XGLUT1 ↑ XEGFR ↑ X X XANX7 ↑ XPP2A ↑ XMMIF ↑ XIL8 ↑ XPARP1 ↑ XDNAPK ↑ XmicroRNA-196 ↑ XCD 74 ↑ XIGFBP-3 ↑ XLIG4 ↑ XPSA-NCAM ↑ XPTEN ↓ Xp53 ↑ X Xp15 ↑ XNuclear survivin ↑ XNDRG1 ↓ XHOX gene clusters ↑ XMDM2 ↑ X XTelomerase ↑ XhTERT ↑ XGPNMB ↑ XTP53 ↑ X XCDKN2A/p16
deletion↑ X
Her2/neu ↑ XLaminin 8 ↑ XbFGF Nuclear
Index↑ X
p16 deletion ↑ XLOH 9p ↑ XLOH 10q ↑ XHGF ↑ XCOX2 ↑ XGST-pi ↑ XPercentage of
nuclei in Sphase
↑ X
MIB-1 ↑ XPDGF ↑ X
Cancer Investigation
Can
cer
Inve
st D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y L
ulea
Uni
vers
ity O
f T
echn
olog
y on
09/
19/1
3Fo
r pe
rson
al u
se o
nly.

Predictors of Long-Term Survival in GBM Patients
of p53 in GBM tumors may be because pathogenesis in GBMoccurs downstream of the p53 mutation (125). There aremixed reports regarding the prognostic abilities of the TP53gene. TP53 mutations are frequent in younger patients buthave neither an effect on survival (100) nor prediction to re-sponse to therapy (105); however, one study found older pa-tients who undergo RT with TP53 mutation have a worseprognosis (33). MDM2 is a negative regulator of p53 and alsohas mixed reports on survival predictability. MDM2 ampli-fication in GBM patients also presents mixed findings; it isfound to be a predictor of poor outcome (99) as well as tohave no significant effect on survival (119). The author whofound MDM2 not to have an effect on survival also did notfind p53 and EGFR to significantly influence survival but in-stead showed GBM patients with increased Msh2 expressionto have prolonged survival (119).
Growth & inhibitory factorsHepatocyte growth factor (HGF) is a neurotropic factor as-sociated with cellular growth. HGF is implicated in brain tu-mors, including GBM. It modulates activity through tyrosinekinase activity and interacts with the proto-oncogene c-MET.Presence of HGF in the CSF is indicative of a worse prog-nosis in GBM patients when compared with patients withother brain tumors (MST 10 month; 893 ± 157 pg/mL ofHGF in GBM). HGF is associated with increased recurrenceof GBM in patients (50). Patients with HGF in their CSFhave increased mortality and poor prognosis in GBM, re-current GBM, as well as an increased likelihood to developa relapse meningioma in patients with prior meningioma(126).
Macrophage migratory inhibition factor (MMIF) is a cy-tokine, which has been shown to induce cell proliferation,corrupt apoptotic activity, and high vascular density tumors.In GBM, MMIF promotes tumor angiogenesis and is upreg-ulated during hypoxia and hypoglycemia. Although the ex-act mechanism is unknown, MMIF mediates activity via IL8possibly through an autocrine process. IL8 concentration di-rectly correlates with MMIF levels. High-grade (III & IV) tu-mors with increased expression of MMIF (10.55 months) orIL8 (11.21 months) significantly correlate with decreased sur-vival compared with high-grade tumors with lower expres-sion of MMIF (22.4 months) or IL8 (18.16 months). Presenceof MMIF also has a direct correlation with tumor recurrencein low-grade glioma but not in Grade III or IV glioma (127).
Other protein & gene markersAdvances in genetics have allowed for many other molecu-lar markers to be identified and studied. Results vary as towhether the presence or absence of certain markers improvesor declines GBM patient survival. Relative findings from sev-eral other studies that were revealed from our PubMed searchare discussed.
GBM patients are found to have more RNA and pro-tein levels of human multidrug-resistance protein 3 (MRP3).MRP3 expression is a strong predictor of survival. Patientswith high levels of MRP3 RNA had a higher risk of death
(2.7 times higher hazard of death) compared with those withmoderate to low levels of MRP3 (128).
Insulin like growth factor binding protein (IGFBP) is sig-nificantly more highly expressed in GBM patients comparedwith AA patients. IGFBP 2, 3, and 5 are relevant forms inGBM and AA. These are associated with shorter survival inGBM patients compared with AA and controls (129).
Glutathione S transferase (GST)-pi gene is found tobe overexpressed in many cancers, including GBM. GBMpatients with overexpression of this gene are resistant tochemotherapy. High expression of GST-pi gene in tumors isassociated with more aggressive tumors and poor survival(130).
Polymorphisms in genes involved in double strand repairof DNA are strong predictors for survival in GBM patients.Short-term survival is predicted in patients (>50 years) withpolymorphisms in LIG4 and BTBD2 (MST 1.2 years). Long-term survival was found in younger (<50 years) patients withCCDC26, HMGA2, and RTEL1 genes (131). However, a highexpression of DNA repair enzymes is thought to decrease sur-vival in GBM patients. Patients with low expressions withpoly-ADP ribose polymerase-1 (PARP1) and DNA proteinkinase (DNAPK) expression had higher MST (12 months and13 months, respectively) compared with patients with highlevels of these enzymes (10 months and 9 months, respec-tively) (132).
Protein NDRG1 is involved in control cellular growth anddifferentiation. Expression of NDRG1 decreases from GradeI glioma to Grade IV glioma. GBM patients with a loss ofNDRG1 expression have lower survival rates compared withglioma patients with higher NDRG1 expression (133).
Human transmembrane glycoprotein nonmetastaticmelanoma protein B (GPNMB) is either found in very lowquantity or not expressed at all in normal brain tissue. Ithas been identified in glioma, melanoma, and breast cancer.GBM patients with mRNA levels of GPNMB greater thanthree times normal have a higher risk of death comparedwith patients with normal or nonexistent levels of GPNMB(134).
Polysialic acid neural cell adhesion molecule protein(PSA-NCAM) is involved in neuronal and glial developmentand formation. PSA-NCAM is found to be overexpressed inmany cancers. GBM patients with overexpression of PSA-NCAM have a poor overall survival and disease-free survival(135).
Wilms’ tumor is a cancer of the kidneys due to mutation ofthe Wilms’ tumor 1 (WT1) gene. Interestingly, the WT1 genemay also play a role in GBM. GBM patients with expressionof the normal WT1 gene have a higher progression-free sur-vival and overall survival (MST 54.4 weeks) compared withpatients expressing low levels of the WT1 gene (28.4 weeks)(136).
One author aimed to find if any markers for hypoxia-related proteins had any survival predictability in GBM pa-tients. Four markers for hypoxia inducible factor 1 (HIF-1alpha) and carbonic anhydrase 9 (CA IX) were not foundto have any survival predictability. Interestingly, markersfor VEGF and glucose transporter 1 (GLUT1) significantly
Copyright C© 2013 Informa Healthcare USA, Inc.
Can
cer
Inve
st D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y L
ulea
Uni
vers
ity O
f T
echn
olog
y on
09/
19/1
3Fo
r pe
rson
al u
se o
nly.

N. S. Chaudhry et al.
correlated with survival (137). Another study found thathypoxia-induced protein phosphatase 2A (PP2A), a cell cy-cle regulator, in GBM patients correlates with poor reducessurvival. PP2A acts to decrease metabolic demand of stem-cell like cells. Patients with high activity of PP2A had shorterMST (8.1 months) compared with patients with low activities(21 months) (138).
Survivin is a member of the inhibitor of apoptosis familythat inhibits caspase activity. This negatively regulates apop-tosis. Patients with malignant tumors, including GBM, whoexpress nuclear survivin have a poor prognosis (139).
Cyclooxygenase 2 (COX2) is a marker of inflammation.COX2 expression increases in higher grade gliomas. High ex-pression of COX2 in GBM patients is significantly correlatedwith poor survival compared with patients with lower gradebrain tumors (140).
Laminins are a group of proteins involved in the vascu-lar basement membrane of cells. Overexpression of laminin 8is significant for recurrence in GBM patients compared withpatients with lower grade tumors, which are found to havemore expression of laminin 9. GBM patients with high ex-pression of laminin 8 also have decreased survival time (51).Interestingly, PDGF, a protein with a tyrosine kinase recep-tor involved in blood vessel formation, plays no role in pre-dictability for survival in GBM (4).
DISCUSSION
Glioblastoma multiforme (GBM) is a malignant and fataldisease. Although no cure yet exists, advances in treatmentfor GBM have extended the patients lifespan from weeks tomonths. Current GBM treatment modalities include surgicalresection followed by radiotherapy, chemotherapy, and reha-bilitative services. Advances in genetics have allowed iden-tification of numerous gene markers in GBM patients thatcan help developing potentially individualized therapy andtherefore result in better treatment options with fewer sideeffects. These advances have not only allowed physicians toextend the lives of patients, but also helped to predict over-all survival, progression-free survival, and time to progres-sion. This has allowed both physicians and patients to betterunderstand an individual’s GBM and course of disease. Allfindings discussed were found to be significant by respectivestudies unless otherwise stated.
Generally, GBM tumors that cross the midline of the brainare more highly associated with negative outcomes (7), as arethose tumors in proximity to the ventricles (9). Frontal lobetumors demonstrate the best outcome (6). There is no sig-nificant difference in survival in patients where the tumorexists in the dominant hemisphere compared with the non-dominant hemisphere, thus hesitation is not warranted in re-moving resectable tumors solely on lateralization of the tu-mor (10). Western and Eastern GBM patients have similarprognosis of disease (5).
In all situations, age and KPS score have conclusively beenstrong survival predictors in GBM patient management.Younger patients and higher preoperative KPS scores areassociated with the best outcomes, whereas older patients
and lower KPS have the most unfavorable outcomes. Oldage solely should not be used as evidence against providingappropriate therapy in older patients, especially in thosewho have high KPS scores (>70). Although old age is nota favorable prognostic indicator, the elderly should notbe excluded from aggressive treatment (combined grosstotal resection with radiation and chemotherapy) if theyare otherwise healthy and show good KPS. Elderly patientsbenefit from such therapies and withholding of aggressivetreatment in capable patients is associated with negativeoutcomes (40–44, 47). Quality of life and activities of dailyliving (ADL) are not predictive of survival in GBM patients(48) and the perspective of quality of life is different forpatients older patients compared with younger patients (47).
Lifespan can be significantly extended in patients whochoose to undergo surgery and combined radiation andchemotherapy (RCT). GBM patients who do not receivetreatment usually die from herniation (11). In addition to ageand KPS score, survival is increased with maximal tumor re-section and smaller tumor volume (4, 8, 12, 13, 23, 26). Pa-tients with low KPS scores are also found to benefit from re-section (23); therefore, it is important to balance the benefitversus the risk of the surgery for each individual patient. RTincreases survival in patients who undergo maximal resec-tion (27–29, 38). The addition of Gamma Knife therapy to ex-ternal beam radiotherapy also increases survival (31). Thereis no difference in survival outcome between 3-D conformalRT and whole brain radiotherapy (WBRT), thusly WBRT isnot recommended over 3-D conformal RT (32). Increasingtotal radiation dose up to 60 years to the tumor bed increasessurvival (30). There is no decrease in survival for delayingRT up to 6 weeks, with longest survival found when start-ing RT at 4 weeks postdiagnosis (39). There is no significantcognitive decline after receiving RT and chemotherapy in pa-tient with 6-month PFS (63) or in patients who receive es-calating doses of radiation (64). Also, GBM patients on RTwho receive infusions of either IdU or BrdU have neithershown to significantly improve nor predict survival (35–37).In addition, patients with TP53 mutations and CDKN2A/p16deletion do not respond well to RT, especially older patients(33).
Best outcomes in patients are found in those who un-dergo maximal tumor resection with concomitant RCT (25).TMZ is a commonly used chemotherapeutic agent for GBM.Patients who express MGMT are resistant to TMZ ther-apy. TMZ therapy has the highest survival outcomes in pa-tients whose MGMT promoter is methylated (16–18,98, 105,108,109). TMZ therapy for 6 months without interruptedprogression-free survival is beneficial. Early progression isassociated with negative outcomes (22). Smaller initial en-hancing volume on MRI for primary GBM patients (76) aswell as smaller volume residual disease for recurrent GBMpatients (61) responds better to chemotherapy. Chemother-apy outcomes are improved in patients with certain endothe-lial markers such as those involving vascularization, cell ad-hesion, and innate immune response and negative outcomesin patients expressing HOX-dominated gene clusters (20).In addition, concurrent treatment for seizures using valproic
Cancer Investigation
Can
cer
Inve
st D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y L
ulea
Uni
vers
ity O
f T
echn
olog
y on
09/
19/1
3Fo
r pe
rson
al u
se o
nly.

Predictors of Long-Term Survival in GBM Patients
acid, which is also an HDAC inhibitor, has no beneficial oradversary effects in GBM pediatric patients.
Patients with recurrent GBM benefit from additional ther-apy in terms of survival. Repeat surgical resection (2, 3) andfractionated stereotactic radiotherapy (FSRT) (54) increasesmedian survival time compared with patients who do notelect for repeat therapy. A high KPS score is associated witha better outcome with repeat RT (55). At reoperation, pa-tients who present with RT necrosis from previous treatmenthave better outcomes (56). Communicating hydrocephaluscan occur with recurrent craniotomies that involve ventricu-lar opening. These patients will require additional VP shuntsurgery (57). Recurrent GBM patients also respond betterto the angiogenesis inhibitor bevacizumab (53). Interstitialbrachytherapy increases survival in patients recurrent GBM(58, 62). Age, high KPS score, and low tumor volume are as-sociated with favorable outcomes from brachytherapy treat-ment (59, 60). Presence of HGF (19856144 50) in the CSF andoverexpression of laminin 8 (51) is significantly correlatedwith recurrence of GBM. Collins’ law, a formula used to mea-sure estimate the recurrence of Wilms’ tumor in children, isalso appreciated for use in estimating time to recurrence inGBM patients.
In addition to monitoring treatment and progression ofthe tumor, MRI findings in GBM patients also have a predic-tive role in determining survival for GBM patient manage-ment. MRI can predict overall survival in patients on TMZ(72). SPECT and CT are not predictive of PFS (75). If usingPET scan, MET is more adept than FDG at locating cellu-lar proliferation due to GBM (71). On MRI, a decrease incerebral blood volume (CBV) after RCT is associated withincreased survival (66, 67), whereas noncontrast enhancingtumor, edema, and multifocality is associated with decreasedsurvival (65). On MRI, diffuse tensor imaging metrics aresensitive and early indicators for PFS. DTI metrics in high-grade glioma patients yielding high CS and low FA, ADC,and CP are unfavorable predictors of outcome, with CP beingthe most indicative (70). Presences of cysts on MRI do nothold any significant predictive value for outcomes in GBMpatients (69). The extent of tumor vascular leakage on MRI ispredictive of survival (74). Similarly, vascular tumor remod-eling after antiangiogenic treatment can also be measured viaMRI to not only determine drug efficacy but also predict sur-vival (73). In addition, cell cultures using patient GBM sam-ples can also predict survival in patients. Long cell culturetimes (>10 days) (77) and neurosphere formation (78) havelower clinical outcomes.
A plethora of molecular markers have been identified andanalyzed in terms of long-term survival predictability. Am-plification, inhibition, or even expression of certain mark-ers can result in favorable, unfavorable, or neutral outcomesin patients (Table 10). From the data, of particular note areEGFR and TP53. There are mixed reports regarding the prog-nostic ability of EGFR amplification and TP53 mutations.EGFR amplification is thought to be a negative prognostic in-dicator (103, 113–115), especially with concurrent EGFRvIIImutation (116). Other authors suggest EGFR amplificationis beneficial in GBM patients (99), beneficial only in the el-
derly (46) or has no significance in terms of survival (33,102) with or without EGFRvIII (117). Similarly, TP53 muta-tions are found to be either negative predictor for outcome inpatients who undergo RT (33), predict no response therapy(105), or not have any effect on survival (100).
CONCLUSION
Histological classification is currently the major criteria forguiding therapeutic treatment and determining survivalusing factors such as size and location. Limitations to currenttherapy largely are due to lack of specific targeted therapy.Greater understanding of molecular genetics and pathwayswill allow for identification of more markers that may helpdetermine treatment. Microarray analysis has identifiednumerous genetic markers that are predictive of survivalin GBM patients; however, a specific tumor marker forGBM remains to be discovered. This may be due to theheterogeneity of GBM tumors across patients, which resultsin nonuniform outcomes. Given this heterogeneous natureof GBM, future management will place greater emphasis onmolecular classification of tumors. This will allow for moreindividualized and targeted therapies, which will ideally leadto better outcomes in both the quantity and quality of life.From the new molecular findings, the goal will be to identifykey driving genes, downstream of the more broad regulatorygenes (e.g. p53) that specifically lead the pathogenesis inGBM. Targeting these key genes with a combined cocktailregimen consisting of a few drugs that elicit a synergistictherapy will perhaps prove to be more beneficial than currentmodalities. Future treatments may include improved tumorvaccines, angiogenesis inhibitors, growth factor inhibitors,hypoxic cell sensitizers, and electric treatment fields (141).
DECLARATION OF INTEREST
The authors report no conflicts of interest. The authors aloneare responsible for the content and writing of the paper.
REFERENCES
1. Bruce J, Benjamin K. Glioblastoma multiforme: Medscape Ref-erence, 2011.
2. Tugcu B, Postalci LS, Gunaldi O, Tanriverdi O, Akdemir H. Ef-ficacy of clinical prognostic factors on survival in patients withglioblastoma. Turk Neurosurg 2010;20(2):117–125.
3. Azizi A, Black P, Miyamoto C, Croul SE. Treatment of malignantastrocytomas with repetitive resections: a longitudinal study. IsrMed Assoc J 2001;3(4):254–257.
4. Donato V, Papaleo A, Castrichino A, Banelli E, GiangasperoF, Salvati M, Delfini R. Prognostic implication of clinical andpathologic features in patients with glioblastoma multiformetreated with concomitant radiation plus temozolomide. Tumori2007;93(3):248–256.
5. Ma X, Lv Y, Liu J, Wang D, Huang Q, Wang X, Li G, Xu S, Li X.Survival analysis of 205 patients with glioblastoma multiforme:clinical characteristics, treatment and prognosis in China. J ClinNeurosci 2009;16(12):1595–1598.
6. Paravati AJ, Heron DE, Landsittel D, Flickinger JC, Mintz A,Chen YF, Huq MS. Radiotherapy and temozolomide for newlydiagnosed glioblastoma and anaplastic astrocytoma: validationof Radiation Therapy Oncology Group-Recursive Partitioning
Copyright C© 2013 Informa Healthcare USA, Inc.
Can
cer
Inve
st D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y L
ulea
Uni
vers
ity O
f T
echn
olog
y on
09/
19/1
3Fo
r pe
rson
al u
se o
nly.
N. S. Chaudhry et al.
Analysis in the IMRT and temozolomide era. J Neurooncol2011;104(1):339–349.
7. Coffey RJ, Lunsford LD, Taylor FH. Survival after stereotacticbiopsy of malignant gliomas. Neurosurgery 1988;22(3):465–473.
8. Allahdini F, Amirjamshidi A, Reza-Zarei M, Abdollahi M. Eval-uating the prognostic factors effective on the outcome of pa-tients with glioblastoma multiformis: does maximal resectionof the tumor lengthen the median survival? World Neurosurg2010;73(2):128–134; discussion e16.
9. Young GS, Macklin EA, Setayesh K, Lawson JD, Wen PY, Nor-den AD, Drappatz J, Kesari S. Longitudinal MRI evidence fordecreased survival among periventricular glioblastoma. J Neu-rooncol 2011;104(1):261–269.
10. Polin RS, Marko NF, Ammerman MD, Shaffrey ME, Huang W,Anderson FA, Jr., Caputy AJ, Laws ER. Functional outcomes andsurvival in patients with high-grade gliomas in dominant andnondominant hemispheres. J Neurosurg 2005;102(2):276–283.
11. Silbergeld DL, Rostomily RC, Alvord EC, Jr. The cause of death inpatients with glioblastoma is multifactorial: clinical factors andautopsy findings in 117 cases of supratentorial glioblastoma inadults. J Neurooncol 1991;10(2):179–185.
12. Kowalczuk A, Macdonald RL, Amidei C, Dohrmann G, 3rd, Er-ickson RK, Hekmatpanah J, Krauss S, Krishnasamy S, MastersG, Mullan SF, Mundt AJ, Sweeney P, Vokes EE, Weir BK, Woll-man RL. Quantitative imaging study of extent of surgical re-section and prognosis of malignant astrocytomas. Neurosurgery1997;41(5):1028–1036; discussion 36–38.
13. Lacroix M, Abi-Said D, Fourney DR, Gokaslan ZL, Shi W,DeMonte F, Lang FF, McCutcheon IE, Hassenbusch SJ, HollandE, Hess K, Michael C, Miller D, Sawaya R. A multivariate analysisof 416 patients with glioblastoma multiforme: prognosis, extentof resection, and survival. J Neurosurg 2001;95(2):190–198.
14. Jakola AS, Gulati S, Weber C, Unsgard G, Solheim O. Postopera-tive deterioration in health related quality of life as predictor forsurvival in patients with glioblastoma: a prospective study. PLoSOne 2011;6(12):e28592.
15. Tang V, Rathbone M, Park Dorsay J, Jiang S, Harvey D. Rehabil-itation in primary and metastatic brain tumours: impact of func-tional outcomes on survival. J Neurol 2008;255(6):820–827.
16. Jacinto FV, Esteller M. MGMT hypermethylation: aprognostic foe, a predictive friend. DNA Repair (Amst)2007;6(8):1155–1160.
17. Mason WP, Cairncross JG. Drug insight: temozolomide as atreatment for malignant glioma – impact of a recent trial. NatClin Pract Neurol 2005;1(2):88–95.
18. Weller M, Steinbach JP, Wick W. Temozolomide: a mile-stone in the pharmacotherapy of brain tumors. Future Oncol2005;1(6):747–754.
19. Kitange GJ, Carlson BL, Schroeder MA, Decker PA,Morlan BW, Wu W, Ballman KV, Giannini C, Sarkaria JN.Expression of CD74 in high grade gliomas: a potential role intemozolomide resistance. J Neurooncol 2010;100(2):177–186.
20. Murat A, Migliavacca E, Gorlia T, Lambiv WL, Shay T, HamouMF, de Tribolet N, Regli L, Wick W, Kouwenhoven MC, Hain-fellner JA, Heppner FL, Dietrich PY, Zimmer Y, CairncrossJG, Janzer RC, Domany E, Delorenzi M, Stupp R, Hegi ME.Stem cell-related “self-renewal” signature and high epidermalgrowth factor receptor expression associated with resistance toconcomitant chemoradiotherapy in glioblastoma. J Clin Oncol2008;26(18):3015–3024.
21. Masoudi A, Elopre M, Amini E, Nagel ME, Ater JL,Gopalakrishnan V, Wolff JE. Influence of valproic acid onoutcome of high-grade gliomas in children. Anticancer Res2008;28(4C):2437–2442.
22. Polley MY, Lamborn KR, Chang SM, Butowski N, Clarke JL,Prados M. Six-month progression-free survival as an alterna-tive primary efficacy endpoint to overall survival in newly diag-nosed glioblastoma patients receiving temozolomide. Neuro On-col 2010;12(3):274–282.
23. Marina O, Suh JH, Reddy CA, Barnett GH, Vogelbaum MA,Peereboom DM, Stevens GH, Elinzano H, Chao ST. Treat-ment outcomes for patients with glioblastoma multiformeand a low Karnofsky Performance Scale score on presenta-tion to a tertiary care institution. Clinical article. J Neurosurg2011;115(2):220–229.
24. Karacetin D, Okten B, Yalcin B, Incekara O. Concomitant temo-zolomide and radiotherapy versus radiotherapy alone for treat-ment of newly diagnosed glioblastoma multiforme. J BUON2011;16(1):133–137.
25. Stupp R, Hegi ME, Mason WP, van den Bent MJ, TaphoornMJ, Janzer RC, Ludwin SK, Allgeier A, Fisher B, Belanger K,Hau P, Brandes AA, Gijtenbeek J, Marosi C, Vecht CJ, MokhtariK, Wesseling P, Villa S, Eisenhauer E, Gorlia T, Weller M,Lacombe D, Cairncross JG, Mirimanoff RO. Effects of radiother-apy with concomitant and adjuvant temozolomide versus radio-therapy alone on survival in glioblastoma in a randomised phaseIII study: 5-year analysis of the EORTC-NCIC trial. Lancet On-col 2009;10(5):459–466.
26. Watanabe T, Katayama Y, Yoshino A, Fukaya C, Yamamoto T.Human interferon beta, nimustine hydrochloride, and radiationtherapy in the treatment of newly diagnosed malignant astrocy-tomas. J Neurooncol 2005;72(1):57–62.
27. Jubelirer SJ. A review of the treatment and survival ratesof 138 patients with glioblastoma multiforme. W V Med J1996;92(4):186–190.
28. Barker FG, 2nd, Prados MD, Chang SM, Gutin PH,Lamborn KR, Larson DA, Malec MK, McDermott MW,Sneed PK, Wara WM, Wilson CB. Radiation response and sur-vival time in patients with glioblastoma multiforme. J Neurosurg1996;84(3):442–448.
29. Sarkaria JN, Mehta MP, Loeffler JS, Buatti JM, Chappell RJ, LevinAB, Alexander E, 3rd., Friedman WA, Kinsella TJ. Radiosurgeryin the initial management of malignant gliomas: survival com-parison with the RTOG recursive partitioning analysis. Radi-ation Therapy Oncology Group. Int J Radiat Oncol Biol Phys1995;32(4):931–941.
30. Miller PJ, Hassanein RS, Giri PG, Kimler BF, O’Boynick P, EvansRG. Univariate and multivariate statistical analysis of high-gradegliomas: the relationship of radiation dose and other prognosticfactors. Int J Radiat Oncol Biol Phys 1990;19(2):275–280.
31. Nwokedi EC, DiBiase SJ, Jabbour S, Herman J, Amin P, ChinLS. Gamma knife stereotactic radiosurgery for patients withglioblastoma multiforme. Neurosurgery 2002;50(1):41–6; dis-cussion 46–47.
32. Showalter TN, Andrel J, Andrews DW, Curran WJ, Jr, DaskalakisC, Werner-Wasik M. Multifocal glioblastoma multiforme: prog-nostic factors and patterns of progression. Int J Radiat Oncol BiolPhys 2007;69(3):820–824.
33. Shih HA, Betensky RA, Dorfman MV, Louis DN, LoefflerJS, Batchelor TT. Genetic analyses for predictors of radia-tion response in glioblastoma. Int J Radiat Oncol Biol Phys2005;63(3):704–710.
34. Wang Y, Pantelias GE, Iliakis G. Mechanism of radiosensitizationby halogenated pyrimidines: the contribution of excess DNA andchromosome damage in BrdU radiosensitization may be mini-mal in plateau-phase cells. Int J Radiat Biol 1994;66(2):133–142.
35. Kinsella TJ, Collins J, Rowland J, Klecker R, Jr., Wright D, Katz D,Steinberg SM, Glastein E. Pharmacology and phase I/II study ofcontinuous intravenous infusions of iododeoxyuridine and hy-perfractionated radiotherapy in patients with glioblastoma mul-tiforme. J Clin Oncol 1988;6(5):871–879.
36. Urtasun RC, Cosmatos D, DelRowe J, Kinsella TJ, Lester S,Wasserman T, Fulton DS. Iododeoxyuridine (IUdR) combinedwith radiation in the treatment of malignant glioma: a compari-son of short versus long intravenous dose schedules (RTOG 86-12). Int J Radiat Oncol Biol Phys 1993;27(2):207–214.
37. Hoshino T, Ahn D, Prados MD, Lamborn K, Wilson CB. Prog-nostic significance of the proliferative potential of intracranial
Cancer Investigation
Can
cer
Inve
st D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y L
ulea
Uni
vers
ity O
f T
echn
olog
y on
09/
19/1
3Fo
r pe
rson
al u
se o
nly.
Predictors of Long-Term Survival in GBM Patients
gliomas measured by bromodeoxyuridine labeling. Int J Cancer1993;53(4):550–555.
38. Fazeny-Dorner B, Wenzel C, Veitl M, Piribauer M, Rossler K,Dieckmann K, Ungersbock K, Marosi C. Survival and prognos-tic factors of patients with unresectable glioblastoma multiforme.Anticancer Drugs 2003;14(4):305–312.
39. Blumenthal DT, Won M, Mehta MP, Curran WJ,Souhami L, Michalski JM, Rogers CL, Corn BW. Shortdelay in initiation of radiotherapy may not affect out-come of patients with glioblastoma: a secondary analy-sis from the radiation therapy oncology group database.J Clin Oncol 2009;27(5):733–739.
40. Barnholtz-Sloan JS, Williams VL, Maldonado JL, Shahani D,Stockwell HG, Chamberlain M, Sloan AE. Patterns of care andoutcomes among elderly individuals with primary malignant as-trocytoma. J Neurosurg 2008;108(4):642–648.
41. Barker FG, 2nd, Chang SM, Larson DA, Sneed PK, Wara WM,Wilson CB, Prados MD. Age and radiation response in glioblas-toma multiforme. Neurosurgery 2001;49(6):1288–1297; discus-sion 97–8.
42. Mohan DS, Suh JH, Phan JL, Kupelian PA, Cohen BH, BarnettGH. Outcome in elderly patients undergoing definitive surgeryand radiation therapy for supratentorial glioblastoma multi-forme at a tertiary care institution. Int J Radiat Oncol Biol Phys1998;42(5):981–987.
43. Ewelt C, Goeppert M, Rapp M, Steiger HJ, Stummer W, Sabel M.Glioblastoma multiforme of the elderly: the prognostic effect ofresection on survival. J Neurooncol 2011;103(3):611–618.
44. Iwamoto FM, Cooper AR, Reiner AS, Nayak L, AbreyLE. Glioblastoma in the elderly: the Memorial Sloan-Kettering Cancer Center Experience (1997–2007). Cancer2009;115(16):3758–3766.
45. Chaichana KL, Chaichana KK, Olivi A, Weingart JD, BennettR, Brem H, Quinones-Hinojosa A. Surgical outcomes for olderpatients with glioblastoma multiforme: preoperative factors as-sociated with decreased survival. Clinical article. J Neurosurg2011;114(3):587–594.
46. Kleinschmidt-DeMasters BK, Lillehei KO, Varella-GarciaM. Glioblastomas in the older old. Arch Pathol Lab Med2005;129(5):624–631.
47. Veilleux N, Goffaux P, Boudrias M, Mathieu D, Daigle K, FortinD. Quality of life in neurooncology – age matters. J Neurosurg2010;113(2):325–332.
48. Meyers CA, Hess KR, Yung WK, Levin VA. Cognitive functionas a predictor of survival in patients with recurrent malignantglioma. J Clin Oncol 2000;18(3):646–650.
49. Muacevic A, Kreth FW. Quality-adjusted survival after tumorresection and/or radiation therapy for elderly patients withglioblastoma multiforme. J Neurol 2003;250(5):561–568.
50. Garcia-Navarrete R, Garcia E, Arrieta O, Sotelo J. Hepatocytegrowth factor in cerebrospinal fluid is associated with mortal-ity and recurrence of glioblastoma, and could be of prognosticvalue. J Neurooncol 2010;97(3):347–351.
51. Ljubimova JY, Fugita M, Khazenzon NM, Das A, Pikul BB, New-man D, Sekiguchi K, Sorokin LM, Sasaki T, Black KL. Associa-tion between laminin-8 and glial tumor grade, recurrence, andpatient survival. Cancer 2004;101(3):604–612.
52. Brown WD, Tavare CJ, Sobel EL, Gilles FH. The applicability ofCollins’ Law to childhood brain tumors and its usefulness as apredictor of survival. Neurosurgery 1995;36(6):1093–1096.
53. Prados M, Cloughesy T, Samant M, Fang L, Wen PY, MikkelsenT, Schiff D, Abrey LE, Yung WK, Paleologos N, Nicholas MK,Jensen R, Vredenburgh J, Das A, Friedman HS. Response asa predictor of survival in patients with recurrent glioblastomatreated with bevacizumab. Neuro Oncol 2011;13(1):143–151.
54. Combs SE, Thilmann C, Edler L, Debus J, Schulz-Ertner D.Efficacy of fractionated stereotactic reirradiation in recurrentgliomas: long-term results in 172 patients treated in a single in-stitution. J Clin Oncol 2005;23(34):8863–8869.
55. Fokas E, Wacker U, Gross MW, Henzel M, Encheva E,Engenhart-Cabillic R. Hypofractionated stereotactic reirra-diation of recurrent glioblastomas: a beneficial treatmentoption after high-dose radiotherapy? Strahlenther Onkol2009;185(4):235–240.
56. Rusthoven KE, Olsen C, Franklin W, Kleinschmidt-DeMastersBK, Kavanagh BD, Gaspar LE, Lillehei K, Waziri A, Damek DM,Chen C. Favorable prognosis in patients with high-grade gliomawith radiation necrosis: the University of Colorado reoperationseries. Int J Radiat Oncol Biol Phys 2011;81(1):211–217.
57. Montano N, D’Alessandris QG, Bianchi F, Lauretti L, Doglietto F,Fernandez E, Maira G, Pallini R. Communicating hydrocephalusfollowing surgery and adjuvant radiochemotherapy for glioblas-toma. J Neurosurg 2011;115(6):1126–1130.
58. Bernstein M, Laperriere N, Leung P, McKenzie S. Interstitialbrachytherapy for malignant brain tumors: preliminary results.Neurosurgery 1990;26(3):371–379; discussion 79–80.
59. Mayr MT, Crocker IR, Butker EK, Williams H, Cotsonis GA, Ol-son JJ. Results of interstitial brachytherapy for malignant braintumors. Int J Oncol 2002;21(4):817–823.
60. Simon JM, Cornu P, Boisserie G, Hasboun D, Tep B, HardimanC, Valery CA, Delattre JY, Dormont D, Baillet F, Mazeron JJ.Brachytherapy of glioblastoma recurring in previously irradiatedterritory: predictive value of tumor volume. Int J Radiat OncolBiol Phys 2002;53(1):67–74.
61. Keles GE, Lamborn KR, Chang SM, Prados MD, BergerMS. Volume of residual disease as a predictor of outcomein adult patients with recurrent supratentorial glioblastomasmultiforme who are undergoing chemotherapy. J Neurosurg2004;100(1):41–46.
62. Leibel SA, Gutin PH, Wara WM, Silver PS, Larson DA, EdwardsMS, Lamb SA, Ham B, Weaver KA, Barnett C, et al. Survivaland quality of life after interstitial implantation of removablehigh-activity iodine-125 sources for the treatment of patientswith recurrent malignant gliomas. Int J Radiat Oncol Biol Phys1989;17(6):1129–1139.
63. Hilverda K, Bosma I, Heimans JJ, Postma TJ, Peter Vandertop W,Slotman BJ, Buter J, Reijneveld JC, Klein M. Cognitive function-ing in glioblastoma patients during radiotherapy and temozolo-mide treatment: initial findings. J Neurooncol 2010;97(1):89–94.
64. Corn BW, Wang M, Fox S, Michalski J, Purdy J, Simpson J,Kresl J, Curran WJ, Jr., Diaz A, Mehta M, Movsas B. Healthrelated quality of life and cognitive status in patients withglioblastoma multiforme receiving escalating doses of confor-mal three dimensional radiation on RTOG 98–03. J Neurooncol2009;95(2):247–257.
65. Pope WB, Sayre J, Perlina A, Villablanca JP, Mischel PS, Clough-esy TF. MR imaging correlates of survival in patients with high-grade gliomas. AJNR Am J Neuroradiol 2005;26(10):2466–2474.
66. Cao Y, Tsien CI, Nagesh V, Junck L, Ten Haken R, Ross BD,Chenevert TL, Lawrence TS. Survival prediction in high-gradegliomas by MRI perfusion before and during early stage of RT[corrected]. Int J Radiat Oncol Biol Phys 2006;64(3):876–885.
67. Mangla R, Singh G, Ziegelitz D, Milano MT, Korones DN,Zhong J, Ekholm SE. Changes in relative cerebral blood vol-ume 1 month after radiation-temozolomide therapy can helppredict overall survival in patients with glioblastoma. Radiology2010;256(2):575–584.
68. Blankenberg FG, Teplitz RL, Ellis W, Salamat MS, Min BH, HallL, Boothroyd DB, Johnstone IM, Enzmann DR. The influenceof volumetric tumor doubling time, DNA ploidy, and histologicgrade on the survival of patients with intracranial astrocytomas.AJNR Am J Neuroradiol 1995;16(5):1001–1012.
69. Kaur G, Bloch O, Jian BJ, Kaur R, Sughrue ME, Aghi MK, Mc-Dermott MW, Berger MS, Chang SM, Parsa AT. A critical eval-uation of cystic features in primary glioblastoma as a prognosticfactor for survival. J Neurosurg 2011;115(4):754–759.
70. Saksena S, Jain R, Narang J, Scarpace L, Schultz LR, LehmanNL, Hearshen D, Patel SC, Mikkelsen T. Predicting survival in
Copyright C© 2013 Informa Healthcare USA, Inc.
Can
cer
Inve
st D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y L
ulea
Uni
vers
ity O
f T
echn
olog
y on
09/
19/1
3Fo
r pe
rson
al u
se o
nly.
N. S. Chaudhry et al.
glioblastomas using diffusion tensor imaging metrics. J MagnReson Imaging 2010;32(4):788–795.
71. Kim S, Chung JK, Im SH, Jeong JM, Lee DS, Kim DG, Jung HW,Lee MC. 11C-methionine PET as a prognostic marker in patientswith glioma: comparison with 18F-FDG PET. Eur J Nucl MedMol Imaging 2005;32(1):52–59.
72. Vos MJ, Berkhof J, Hoekstra OS, Bosma I, Sizoo EM, HeimansJJ, Reijneveld JC, Sanchez E, Lagerwaard FJ, Buter J, Noske DP,Postma TJ. MRI and thallium-201 SPECT in the prediction ofsurvival in glioma. Neuroradiology 2012;54(6):539–546.
73. Essock-Burns E, Lupo JM, Cha S, Polley MY, Butowski NA,Chang SM, Nelson SJ. Assessment of perfusion MRI-derived pa-rameters in evaluating and predicting response to antiangiogenictherapy in patients with newly diagnosed glioblastoma. NeuroOncol 2011;13(1):119–131.
74. Cao Y, Nagesh V, Hamstra D, Tsien CI, Ross BD, Chenevert TL,Junck L, Lawrence TS. The extent and severity of vascular leak-age as evidence of tumor aggressiveness in high-grade gliomas.Cancer Res 2006;66(17):8912–8917.
75. Datta NR, Pasricha R, Gambhir S, Phadke RV, Prasad SN. Post-operative residual tumour imaged by contrast-enhanced com-puted tomography and 201Tl single photon emission tomog-raphy: can they predict progression-free survival in high-gradegliomas? Clin Oncol (R Coll Radiol) 2004;16(7):494–500.
76. Grant R, Walker M, Hadley D, Barton T, Osborn C. Imagingresponse to chemotherapy with RMP-7 and carboplatin in ma-lignant glioma: size matters but speed does not. J Neurooncol2002;57(3):241–245.
77. Furneaux CE, Marshall ES, Yeoh K, Monteith SJ, Mews PJ, SansurCA, Oskouian RJ, Sharples KJ, Baguley BC. Cell cycle times ofshort-term cultures of brain cancers as predictors of survival. BrJ Cancer 2008;99(10):1678–1683.
78. Laks DR, Masterman-Smith M, Visnyei K, Angenieux B, OrozcoNM, Foran I, Yong WH, Vinters HV, Liau LM, Lazareff JA, Mis-chel PS, Cloughesy TF, Horvath S, Kornblum HI. Neurosphereformation is an independent predictor of clinical outcome in ma-lignant glioma. Stem Cells 2009;27(4):980–987.
79. Hoke M, Dieckmann K, Koppensteiner R, Schillinger M, MarosiC, Mlekusch W. Prognostic value of plasma d-dimer levels in pa-tients with glioblastoma multiforme - Results from a pilot study.Wien Klin Wochenschr 2011;123(7–8):199–203.
80. Brockmann MA, Giese A, Mueller K, Kaba FJ, Lohr F, Weiss C,Gottschalk S, Nolte I, Leppert J, Tuettenberg J, Groden C. Pre-operative thrombocytosis predicts poor survival in patients withglioblastoma. Neuro Oncol 2007;9(3):335–342.
81. Borg N, Guilfoyle MR, Greenberg DC, Watts C, Thomson S.Serum albumin and survival in glioblastoma multiforme. J Neu-rooncol 2011;105(1):77–81.
82. Crocker M, Ashley S, Giddings I, Petrik V, Hardcastle A, Ah-erne W, Pearson A, Bell BA, Zacharoulis S, Papadopoulos MC.Serum angiogenic profile of patients with glioblastoma identifiesdistinct tumor subtypes and shows that TIMP-1 is a prognosticfactor. Neuro Oncol 2011;13(1):99–108.
83. Pelloski CE, Mahajan A, Maor M, Chang EL, Woo S, Gilbert M,Colman H, Yang H, Ledoux A, Blair H, Passe S, Jenkins RB, Al-dape KD. YKL-40 expression is associated with poorer responseto radiation and shorter overall survival in glioblastoma. ClinCancer Res 2005;11(9):3326–3334.
84. Hormigo A, Gu B, Karimi S, Riedel E, Panageas KS, EdgarMA, Tanwar MK, Rao JS, Fleisher M, DeAngelis LM, HollandEC. YKL-40 and matrix metalloproteinase-9 as potential serumbiomarkers for patients with high-grade gliomas. Clin CancerRes 2006;12(19):5698–5704.
85. Strojnik T, Kos J, Zidanik B, Golouh R, Lah T. Cathepsin B im-munohistochemical staining in tumor and endothelial cells is anew prognostic factor for survival in patients with brain tumors.Clin Cancer Res 1999;5(3):559–567.
86. Fukuda ME, Iwadate Y, Machida T, Hiwasa T, Nimura Y, NagaiY, Takiguchi M, Tanzawa H, Yamaura A, Seki N. Cathepsin D is
a potential serum marker for poor prognosis in glioma patients.Cancer Res 2005;65(12):5190–5194.
87. Flannery T, McQuaid S, McGoohan C, McConnell RS,McGregor G, Mirakhur M, Hamilton P, Diamond J, Cran G,Walker B, Scott C, Martin L, Ellison D, Patel C, NicholsonC, Mendelow D, McCormick D, Johnston PG. Cathepsin Sexpression: An independent prognostic factor in glioblastomatumours – a pilot study. Int J Cancer 2006;119(4):854–860.
88. Peles E, Lidar Z, Simon AJ, Grossman R, Nass D, Ram Z. An-giogenic factors in the cerebrospinal fluid of patients with astro-cytic brain tumors. Neurosurgery 2004;55(3):562–567; discus-sion 67–8.
89. Fukui S, Nawashiro H, Otani N, Ooigawa H, Nomura N, Yano A,Miyazawa T, Ohnuki A, Tsuzuki N, Katoh H, Ishihara S, ShimaK. Nuclear accumulation of basic fibroblast growth factor in hu-man astrocytic tumors. Cancer 2003;97(12):3061–3067.
90. Colin C, Voutsinos-Porche B, Nanni I, Fina F, Metellus P, Intagli-ata D, Baeza N, Bouvier C, Delfino C, Loundou A, Chinot O,Lah T, Kos J, Martin PM, Ouafik L, Figarella-Branger D. Highexpression of cathepsin B and plasminogen activator inhibitortype-1 are strong predictors of survival in glioblastomas. ActaNeuropathol 2009;118(6):745–754.
91. Petrik V, Saadoun S, Loosemore A, Hobbs J, Opstad KS,Sheldon J, Tarelli E, Howe FA, Bell BA, Papadopoulos MC.Serum alpha 2-HS glycoprotein predicts survival in patients withglioblastoma. Clin Chem 2008;54(4):713–722.
92. McKeever PE, Feldenzer JA, McCoy JP, Laug M, Gebarski S,Chandler WF, Greenberg HS, Junck L, D’Amato CJ, Varani J.Nuclear parameters as prognostic indicators in glioblastoma pa-tients. J Neuropathol Exp Neurol 1990;49(1):71–78.
93. Srinivasan S, Patric IR, Somasundaram K. A ten-microRNA ex-pression signature predicts survival in glioblastoma. PLoS One2011;6(3):e17438.
94. Guan Y, Mizoguchi M, Yoshimoto K, Hata N, Shono T, SuzukiSO, et al. MiRNA-196 is upregulated in glioblastoma but notin anaplastic astrocytoma and has prognostic significance. ClinCancer Res 2010;16(16):4289–4297.
95. Colman H, Zhang L, Sulman EP, McDonald JM, Shooshtari NL,Rivera A, et al. A multigene predictor of outcome in glioblas-toma. Neuro Oncol 2010;12(1):49–57.
96. Sato A, Sakurada K, Kumabe T, Sasajima T, Beppu T,Asano K, et al. Association of stem cell marker CD133 ex-pression with dissemination of glioblastomas. Neurosurg Rev2010;33(2):175–183; discussion 83–84.
97. Nutt CL, Mani DR, Betensky RA, Tamayo P, Cairncross JG, LaddC, Pohl U, Hartmann C, McLaughlin ME, Batchelor TT, BlackPM, von Deimling A, Pomeroy SL, Golub TR, Louis DN. Geneexpression-based classification of malignant gliomas correlatesbetter with survival than histological classification. Cancer Res2003;63(7):1602–1607.
98. Ducray F, Idbaih A, Wang XW, Cheneau C, Labussiere M, San-son M. Predictive and prognostic factors for gliomas. Expert RevAnticancer Ther 2011;11(5):781–789.
99. Houillier C, Lejeune J, Benouaich-Amiel A, Laigle-Donadey F,Criniere E, Mokhtari K, Thillet J, Delattre JY, Hoang-Xuan K,Sanson M. Prognostic impact of molecular markers in a series of220 primary glioblastomas. Cancer 2006;106(10):2218–2223.
100. Rasheed A, Herndon JE, Stenzel TT, Raetz JG, Kendelhardt J,Friedman HS, Friedman AH, Bigner DD, Bigner SH, McLendonRE. Molecular markers of prognosis in astrocytic tumors. Cancer2002;94(10):2688–2697.
101. Hung KS, Howng SL. Prognostic significance of annexin VII ex-pression in glioblastomas multiforme in humans. J Neurosurg2003;99(5):886–892.
102. Smith JS, Tachibana I, Passe SM, Huntley BK, Borell TJ, Iturria N,O’Fallon JR, Schaefer PL, Scheithauer BW, James CD, BucknerJC, Jenkins RB. PTEN mutation, EGFR amplification, and out-come in patients with anaplastic astrocytoma and glioblastomamultiforme. J Natl Cancer Inst 2001;93(16):1246–1256.
Cancer Investigation
Can
cer
Inve
st D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y L
ulea
Uni
vers
ity O
f T
echn
olog
y on
09/
19/1
3Fo
r pe
rson
al u
se o
nly.
Predictors of Long-Term Survival in GBM Patients
103. Umesh S, Tandon A, Santosh V, Anandh B, Sampath S, Chan-dramouli BA, Sastry Kolluri VR. Clinical and immunohisto-chemical prognostic factors in adult glioblastoma patients. ClinNeuropathol 2009;28(5):362–372.
104. Wemmert S, Bettscheider M, Alt S, Ketter R, Kammers K, Fei-den W, Steudel WI, Rahnenfuhrer J, Urbschat S. p15 promotermethylation – a novel prognostic marker in glioblastoma pa-tients. Int J Oncol 2009;34(6):1743–1748.
105. Weller M, Felsberg J, Hartmann C, Berger H, Steinbach JP,Schramm J, Westphal M, Schackert G, Simon M, Tonn JC,Heese O, Krex D, Nikkhah G, Pietsch T, Wiestler O, Reifen-berger G, von Deimling A, Loeffler M. Molecular predictorsof progression-free and overall survival in patients with newlydiagnosed glioblastoma: a prospective translational study ofthe German Glioma Network. J Clin Oncol 2009;27(34):5743–5750.
106. Jaeckle KA, Eyre HJ, Townsend JJ, Schulman S, Knudson HM,Belanich M, Yarosh DB, Bearman SI, Giroux DJ, Schold SC. Cor-relation of tumor O6 methylguanine-DNA methyltransferaselevels with survival of malignant astrocytoma patients treatedwith bis-chloroethylnitrosourea: a Southwest Oncology Groupstudy. J Clin Oncol 1998;16(10):3310–3315.
107. Hegi ME, Diserens AC, Godard S, Dietrich PY, Regli L, Os-termann S, Otten P, Van Melle G, de Tribolet N, StuppR. Clinical trial substantiates the predictive value of O-6-methylguanine-DNA methyltransferase promoter methylationin glioblastoma patients treated with temozolomide. Clin Can-cer Res 2004;10(6):1871–1874.
108. Herrlinger U, Rieger J, Koch D, Loeser S, Blaschke B, KortmannRD, Steinbach JP, Hundsberger T, Wick W, Meyermann R, TanTC, Sommer C, Bamberg M, Reifenberger G, Weller M. Phase IItrial of lomustine plus temozolomide chemotherapy in additionto radiotherapy in newly diagnosed glioblastoma: UKT-03. J ClinOncol 2006;24(27):4412–4417.
109. Rivera AL, Pelloski CE, Gilbert MR, Colman H, De La Cruz C,Sulman EP, Bekele BN, Aldape KD. MGMT promoter methy-lation is predictive of response to radiotherapy and prognosticin the absence of adjuvant alkylating chemotherapy for glioblas-toma. Neuro Oncol 2010;12(2):116–121.
110. Uno M, Oba-Shinjo SM, Camargo AA, Moura RP, Aguiar PH,Cabrera HN, Begnami M, Rosemberg S, Teixeira MJ, Marie SK.Correlation of MGMT promoter methylation status with geneand protein expression levels in glioblastoma. Clinics (Sao Paulo)2011;66(10):1747–1755.
111. Ohka F, Natsume A, Motomura K, Kishida Y, Kondo Y, AbeT, Nakasu Y, Namba H, Wakai K, Fukui T, Momota H, IwamiK, Kinjo S, Ito M, Fujii M, Wakabayashi T. The global DNAmethylation surrogate LINE-1 methylation is correlated withMGMT promoter methylation and is a better prognostic factorfor glioma. PLoS One 2011;6(8):e23332.
112. Nobusawa S, Watanabe T, Kleihues P, Ohgaki H. IDH1 muta-tions as molecular signature and predictive factor of secondaryglioblastomas. Clin Cancer Res 2009;15(19):6002–6007.
113. Frederick L, Wang XY, Eley G, James CD. Diversity and fre-quency of epidermal growth factor receptor mutations in humanglioblastomas. Cancer Res 2000;60(5):1383–1387.
114. Zhu A, Shaeffer J, Leslie S, Kolm P, El-Mahdi AM. Epidermalgrowth factor receptor: an independent predictor of survival inastrocytic tumors given definitive irradiation. Int J Radiat OncolBiol Phys 1996;34(4):809–815.
115. Etienne MC, Formento JL, Lebrun-Frenay C, Gioanni J, Cha-tel M, Paquis P, Bernard C, Courdi A, Bensadoun RJ, Pig-nol JP, Francoual M, Grellier P, Frenay M, Milano G. Epider-mal growth factor receptor and labeling index are indepen-dent prognostic factors in glial tumor outcome. Clin Cancer Res1998;4(10):2383–2390.
116. Shinojima N, Tada K, Shiraishi S, Kamiryo T, Kochi M,Nakamura H, Makino K, Saya H, Hirano H, Kuratsu J, Oka K,Ishimaru Y, Ushio Y. Prognostic value of epidermal growth fac-
tor receptor in patients with glioblastoma multiforme. CancerRes 2003;63(20):6962–6970.
117. Heimberger AB, Hlatky R, Suki D, Yang D, Weinberg J, GilbertM, Sawaya R, Aldape K. Prognostic effect of epidermal growthfactor receptor and EGFRvIII in glioblastoma multiforme pa-tients. Clin Cancer Res 2005;11(4):1462–1466.
118. Potti A, Forseen SE, Koka VK, Pervez H, Koch M, FraimanG, Mehdi SA, Levitt R. Determination of HER-2/neu overex-pression and clinical predictors of survival in a cohort of 347patients with primary malignant brain tumors. Cancer Invest2004;22(4):537–544.
119. Stark AM, Hugo HH, Witzel P, Mihajlovic Z, Mehdorn HM. Age-related expression of p53, Mdm2, EGFR and Msh2 in glioblas-toma multiforme. Zentralbl Neurochir 2003;64(1):30–36.
120. Tchirkov A, Rolhion C, Kemeny JL, Irthum B, Puget S, KhalilT, Chinot O, Kwiatkowski F, Perissel B, Vago P, Verrelle P.Clinical implications of quantitative real-time RT-PCR analy-sis of hTERT gene expression in human gliomas. Br J Cancer2003;88(4):516–520.
121. Boldrini L, Pistolesi S, Gisfredi S, Ursino S, Ali G, Pier-acci N, Basolo F, Parenti G, Fontanini G. Telomerase activ-ity and hTERT mRNA expression in glial tumors. Int J Oncol2006;28(6):1555–1560.
122. Wang L, Wei Q, Wang LE, Aldape KD, Cao Y, Okcu MF, HessKR, El-Zein R, Gilbert MR, Woo SY, Prabhu SS, Fuller GN,Bondy ML. Survival prediction in patients with glioblastomamultiforme by human telomerase genetic variation. J Clin On-col 2006;24(10):1627–1632.
123. Ellison DW, Steart PV, Bateman AC, Pickering RM, Palmer JD,Weller RO. Prognostic indicators in a range of astrocytic tu-mours: an immunohistochemical study with Ki-67 and p53 an-tibodies. J Neurol Neurosurg Psychiatry 1995;59(4):413–419.
124. Kyritsis AP, Bondy ML, Hess KR, Cunningham JE, Zhu D, AmosCJ, Yung WK, Levin VA, Bruner JM. Prognostic significance ofp53 immunoreactivity in patients with glioma. Clin Cancer Res1995;1(12):1617–1622.
125. Chozick BS, Pezzullo JC, Epstein MH, Finch PW. Prognostic im-plications of p53 overexpression in supratentorial astrocytic tu-mors. Neurosurgery 1994;35(5):831–837; discussion 37–38.
126. Arrieta O, Garcia E, Guevara P, Garcia-Navarrete R, OndarzaR, Rembao D, Sotelo J. Hepatocyte growth factor is associatedwith poor prognosis of malignant gliomas and is a predictor forrecurrence of meningioma. Cancer 2002;94(12):3210–3218.
127. Wang XB, Tian XY, Li Y, Li B, Li Z. Elevated expression ofmacrophage migration inhibitory factor correlates with tumorrecurrence and poor prognosis of patients with gliomas. J Neu-rooncol 2012;106(1):43–51.
128. Kuan CT, Wakiya K, Herndon JE, 2nd, Lipp ES, Pegram CN, Rig-gins GJ, Rasheed A, Szafranski SE, McLendon RE, Wikstrand CJ,Bigner DD. MRP3: a molecular target for human glioblastomamultiforme immunotherapy. BMC Cancer 2010;10:468.
129. Santosh V, Arivazhagan A, Sreekanthreddy P, Srinivasan H,Thota B, Srividya MR, Vrinda M, Sridevi S, Shailaja BC,Samuel C, Prasanna KV, Thennarasu K, Balasubramaniam A,Chandramouli BA, Hegde AS, Somasundaram K, KondaiahP, Rao MR. Grade-specific expression of insulin-like growthfactor-binding proteins-2, -3, and -5 in astrocytomas: IGFBP-3 emerges as a strong predictor of survival in patients withnewly diagnosed glioblastoma. Cancer Epidemiol BiomarkersPrev 2010;19(6):1399–1408.
130. Ali-Osman F, Brunner JM, Kutluk TM, Hess K. Prognostic sig-nificance of glutathione S-transferase pi expression and subcel-lular localization in human gliomas. Clin Cancer Res 1997;3(12Pt 1):2253–2261.
131. Liu Y, Shete S, Etzel CJ, Scheurer M, Alexiou G, ArmstrongG, Tsavachidis S, Liang FW, Gilbert M, Aldape K, ArmstrongT, Houlston R, Hosking F, Robertson L, Xiao Y, Wiencke J,Wrensch M, Andersson U, Melin BS, Bondy M. Polymorphismsof LIG4, BTBD2, HMGA2, and RTEL1 genes involved in the
Copyright C© 2013 Informa Healthcare USA, Inc.
Can
cer
Inve
st D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y L
ulea
Uni
vers
ity O
f T
echn
olog
y on
09/
19/1
3Fo
r pe
rson
al u
se o
nly.

N. S. Chaudhry et al.
double-strand break repair pathway predict glioblastoma sur-vival. J Clin Oncol 2010;28(14):2467–2474.
132. Kase M, Vardja M, Lipping A, Asser T, Jaal J. Impact ofPARP-1 and DNA-PK expression on survival in patients withglioblastoma multiforme. Radiother Oncol 2011;101(1):127–131.
133. Sun B, Chu D, Li W, Chu X, Li Y, Wei D, Li H. Decreased ex-pression of NDRG1 in glioma is related to tumor progression andsurvival of patients. J Neurooncol 2009;94(2):213–219.
134. Kuan CT, Wakiya K, Dowell JM, Herndon JE, 2nd, Reardon DA,Graner MW, Riggins GJ, Wikstrand CJ, Bigner DD. Glycopro-tein nonmetastatic melanoma protein B, a potential moleculartherapeutic target in patients with glioblastoma multiforme. ClinCancer Res 2006;12(7 Pt 1):1970–1982.
135. Amoureux MC, Coulibaly B, Chinot O, Loundou A, Metellus P,Rougon G, Figarella-Branger D. Polysialic acid neural cell adhe-sion molecule (PSA-NCAM) is an adverse prognosis factor inglioblastoma, and regulates olig2 expression in glioma cell lines.BMC Cancer 2010;10:91.
136. Chiba Y, Hashimoto N, Tsuboi A, Rabo C, Oka Y, Kinoshita M,Kagawa N, Oji Y, Sugiyama H, Yoshimine T. Prognostic value ofWT1 protein expression level and MIB-1 staining index as pre-dictor of response to WT1 immunotherapy in glioblastoma pa-tients. Brain Tumor Pathol 2010;27(1):29–34.
137. Flynn JR, Wang L, Gillespie DL, Stoddard GJ, Reid JK, OwensJ, Ellsworth GB, Salzman KL, Kinney AY, Jensen RL. Hypoxia-regulated protein expression, patient characteristics, and preop-erative imaging as predictors of survival in adults with glioblas-toma multiforme. Cancer 2008;113(5):1032–1042.
138. Hofstetter CP, Burkhardt JK, Shin BJ, Gursel DB, Mubita L, Gor-repati R, Brennan C, Holland EC, Boockvar JA. Protein phos-phatase 2A mediates dormancy of glioblastoma multiforme-derived tumor stem-like cells during hypoxia. PLoS One2012;7(1):e30059.
139. Shirai K, Suzuki Y, Oka K, Noda SE, Katoh H, Itoh J, Itoh H, Ishi-uchi S, Sakurai H, Hasegawa M, Nakano T. Nuclear survivin ex-pression predicts poorer prognosis in glioblastoma. J Neuroon-col 2009;91(3):353–358.
140. Shono T, Tofilon PJ, Bruner JM, Owolabi O, Lang FF.Cyclooxygenase-2 expression in human gliomas: prognos-tic significance and molecular correlations. Cancer Res2001;61(11):4375–4381.
141. American Cancer Society. Brain and Spinal Cord Tumors inAdults. Atlanta, Ga: American Cancer Society 2013.
142. Latif AZ, Signorini D, Gregor A, Grant R, Ironside JW, Whit-tle IR. Application of the MRC brain tumour prognostic indexto patients with malignant glioma not managed in randomisedcontrol trial. J Neurol Neurosurg Psychiatry 1998;64(6):747–750.
Cancer Investigation
Can
cer
Inve
st D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y L
ulea
Uni
vers
ity O
f T
echn
olog
y on
09/
19/1
3Fo
r pe
rson
al u
se o
nly.