Embed Size (px)
Citation preview

Int. J. Radiation Oncology Biol. Phys., Vol. 79, No. 3, pp. 724–731, 2011Copyright � 2011 Elsevier Inc.
Printed in the USA. All rights reserved0360-3016/$–see front matter
jrobp.2009.11.044
doi:10.1016/j.iCLINICAL INVESTIGATION Prostate
PREDICTORS OF ANDROGEN DEPRIVATION THERAPY EFFICACY COMBINEDWITH PROSTATIC IRRADIATION: THE CENTRAL ROLE OF TUMOR STAGE AND
RADIATION DOSE
SCOTT WILLIAMS, M.D., F.R.A.N.Z.C.R.,* MARK BUYYOUNOUSKI, M.D.,y LARRY KESTIN, M.D.,z
GILLIAN DUCHESNE, M.D., F.R.A.N.Z.C.R.,* AND TOM PICKLES, M.D.x
*Peter MacCallum Cancer Centre and University of Melbourne, Melbourne, Australia; yFox Chase Cancer Center, Philadelphia,Pennsylvania; zWilliam Beaumont Hospital, Royal Oak, Michigan; and xBritish Columbia Cancer Agency, Vancouver, Canada
ReprinDivisionLocked B9656 111petermac.
Purpose: To evaluate the response of clinically localized prostate cancer to various durations of planned androgendeprivation therapy (ADT) and to investigate subgroups predicting response.Methods and Materials: Data of 3,666 prostate cancer patients treated with either combined ADT and externalbeam radiotherapy (EBRT) or EBRTalone at four institutions were examined. ADT consisted of neoadjuvant, con-current, or adjuvant ADT or combinations of these regimens. The primary endpoint was time to biochemical fail-ure (nadir plus 2 ng/ml), assessed from the end of therapy. Factors predictive for the need for ADT were examinedwith interaction analyses.Results: The impact of increasing ADT duration was nonlinear with, on average, 6 months of adjuvant ADTresult-ing in a reduction of the risk of biochemical failure by 38% (95% confidence interval [CI], 29%–46%), while 12, 24,and 36 months of ADT resulted in a 58% (95% CI, 47%–67%), 66% (95% CI, 55%–75%), and 66% (95% CI,51%–77%) relative failure reduction, respectively. Patients with higher T stage cancers and those treated withlower radiation doses had a significantly greater benefit for increasing ADT duration (interaction, p = 0.016and p = 0.007, respectively). Pretreatment prostate-specific antigen values, Gleason score, age, and risk groupdid not modify the response to ADT.Conclusions: The known ADT efficacy derived from randomized studies can be generalized to patients with differ-ent features, and individual predictions of potential benefit from ADT use and duration may be calculated to aidpatient and physician decision making. Tumor stage and radiation dose variations were related to significantly dif-ferent ADT duration effects. The validity of these predictive factors requires prospective evaluation. � 2011Elsevier Inc.
Prostate cancer, Radiotherapy, Androgen deprivation, Outcomes.
INTRODUCTION
Durations of androgen deprivation therapy (ADT) varying
from 4 months to 3 years or longer have been shown in ran-
domized trials to result in improved outcomes for patients
with locally advanced or high-grade prostate cancer treated
with radiation therapy, including improved survival (1–4).
On the basis of this high-level evidence, ADT has become
widely used in intermediate and high-risk patients concurrent
with radiation, combined with various ADT durations, neo-
adjuvantly or adjuvantly, or both (5). Previous data have sug-
gested that ADT duration should be selected based on broad-
risk criteria, with those at highest failure risk having longer
term ADT, while those with intermediate risk disease are
treated with briefer courses (6–8).
t requests to: Dr. Scott Williams, M.D., F.R.A.N.Z.C.R.,of Radiation Oncology, Peter MacCallum Cancer Centre,ag 1 A’Beckett St., Victoria 8006, Australia. Tel: (61) 31; Fax: (61) 3 9656 1424; E-mail: scott.williams@org
724
The use of planned adjuvant ADT has to be balanced
against the significant toxicity it carries in many patients.
ADT-induced metabolic syndrome is relatively common,
with a substantial risk of diabetes (40% increased risk) and
cardiac disease, including fatal myocardial infarction (16%
increased risk) (9). Weight gain, muscle loss, and osteoporo-
sis may occur (10). These and other toxicities typically pre-
cipitate a quality-of-life detriment that can worsen with
longer ADT durations (11).
In counseling patients regarding the potential benefit of
planned ADT or potential loss, as in the case of a man con-
templating early ADT cessation due to toxicity, an under-
standing of the factors responsible for response are required
for the individual. The aims of this study were to define the
Conflict of interest: none.Received Oct 3, 2009, and in revised form Nov 14, 2009.
Accepted for publication Nov 16, 2009.

Androgen deprivation duration effect d S. WILLIAMS et al. 725
relative efficacy of ADT over time and to examine in detail
the role of individual factors in predicting this response. To
maximize the power available to identify interactions be-
tween variables and generate hypotheses, the primary focus
was the use of a biochemical endpoint free from the influ-
ences of salvage therapies.
METHODS AND MATERIALS
Patient selectionPatients included in this study were required to have clinically
localized prostate adenocarcinoma. The distinction of disease risk
was made according to NCCN criteria (12), with high risk having
any one of the following features: a clinical stage T3 or higher,
a prostate-specific antigen concentration at presentation (iPSA) of
>20 ng/ml, or a Gleason score (GS) of 8 to 10; with low risk being
T2a or less, an iPSA concentration of #10 ng/ml, and a GS of # 6;
and intermediate risk being all the remainder.
A total of 3,666 eligible cases treated between 1989 and 2000
were identified from a collaborative database from four institutions
(British Columbia Cancer Agency, Fox Chase Cancer Center, Peter
MacCallum Cancer Center, and William Beaumont Hospital).
Radiation treatment methods have been previously published
(13–16). In summary, radiation was given via computed tomogra-
phy (CT)-planned conformal or intensity-modulated techniques
without image guidance, and whole-pelvis radiation was not rou-
tinely employed. ADT, which was initiated prior to or concurrent
with radiotherapy and continued for less than 1 month after radio-
therapy, was classified as neoadjuvant ADT (NAADT), with any
continuation beyond this point classified as adjuvant ADT
(AADT). The rate of ADT usage among institutions varied from
7% to 46%, with the two US-based centers using less ADT and hav-
ing fewer tumors with high-risk features than the Canadian or Aus-
tralian centers (Table 1). ADT, when given, was almost universally
begun prior to radiotherapy, with pure adjuvant scheduling in less
than 2% of cases in any center.
Follow-up was calculated from the date of completion of therapy;
therefore, for those receiving radiotherapy only or pure NAADT, the
date on which radiation was finished was the index date, while for
those who received a component of AADT, the calculated date of
finishing the hormone therapy became the start of follow-up. The
primary endpoint was biochemical failure (bF), defined by using
the Phoenix definition (17), where the date of a PSA rise to 2 ng/ml
or more above the lowest level to date indicated failure. Secondary
analyses were done for the time to distant metastatic failure (free-
dom from distant metastases), death from prostate cancer (cause-
specific survival), and death from any cause. There were 1,198 bF
events, 211 episodes of distant metastatic failure, 172 deaths from
prostate cancer, and 664 deaths from any cause at a median
follow-up of 75 months (Table 1).
StatisticsDescriptive data were expressed as either a median value with as-
sociated interquartile range (representing the values at the 25th and
75th centiles) or as counts with associated percentages. Modeling
was based on a proportional hazards model. Restricted cubic splines
were used to investigate nonlinearity of continuous variables (18).
Interactions between prognostic covariates (predictive variables)
were tested by including an additional product term between the
continuous range of ADT duration and a respective covariate of in-
terest within the model (19). A statistically significant interaction
term, then, suggests that the factor of interest modulates ADT dura-
tion effect and is a predictive factor for ADT duration response. To
reduce the potential for over-fitting bias, confidence intervals (CI) of
all p values were determined by bootstrap resampling (n = 1,000).
Treatment center was a stratification factor in all analyses.
The impact of individual variables was determined by the contri-
bution it makes to the model fit as shown by the equation c2 minus
degrees of freedom (c2 � df). Discrimination was assessed via the
concordance index (analogous to the area under the receiver opera-
tor characteristic curve) via bootstrap resampling (n = 150). The
ability to predict the likely rate of failure for an individual (calibra-
tion) was internally validated using bootstrap resampling (n = 150).
Analyses and the derived nomogram depicting the final model
based on bF were performed in R statistical language (R Foundation
for Statistical Computing, Vienna, Austria). Statistical significance
was denoted at the p value level of #0.05 and was always
two-sided.
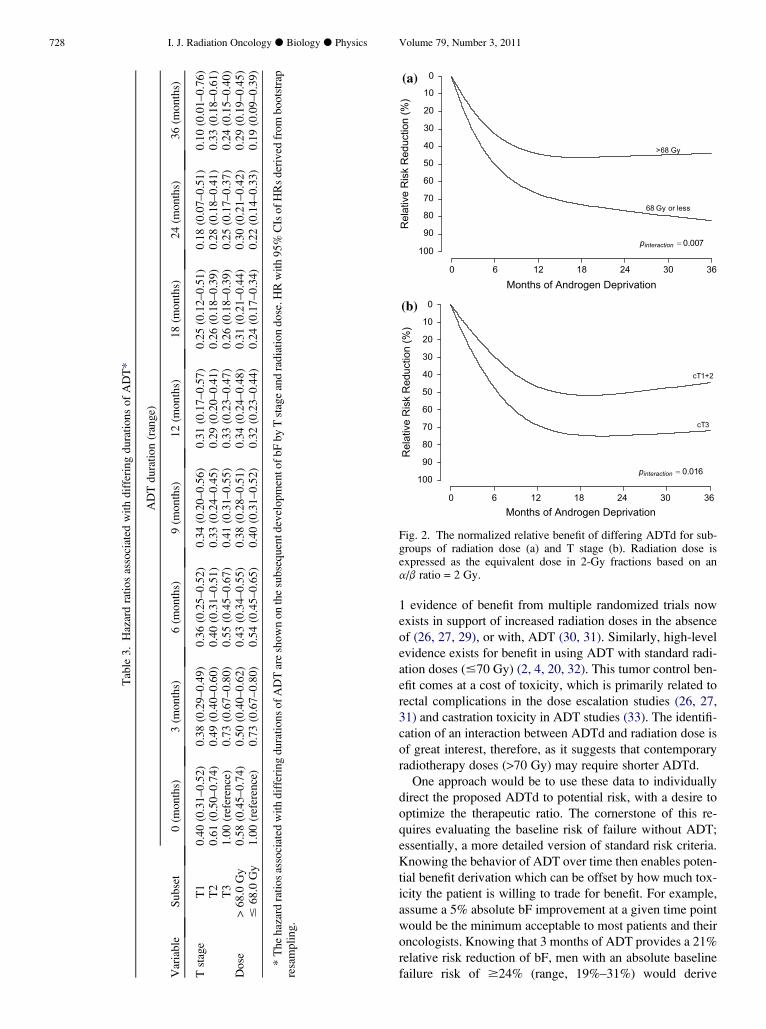
RESULTS
Defining the functional form of ADT duration effectAlong with PSA (p < 0.0001), GS (p < 0.0001), stage
(p < 0.0001), age (p = 0.010), and radiotherapy dose (p =
0.0002), ADT duration (ADTd) (p <0.0001) had a statistically
significant impact on freedom from bF (FFbF). Strong non-
linearity of the response to increasing ADTd was demon-
strated by including a restricted cubic spline transformation
of ADTd within the model (p < 0.0001). The nonlinear re-
sponse appeared to show asymptotic behavior with minimal
additional ADTd effect beyond approximately 18 months of
therapy (Fig. 1). Using the benefit obtained from a 3-year
course of ADT as a reference for comparison (a 66% risk re-
duction), the average patient in this cohort received 56%
(95% CI, 45%–77%) of this potential total benefit in the first
6 months of ADT, 86% (95% CI, 73%–114%) by the end of
the first year, and 99% (95% CI, 92%–119%) by completing
2 years of therapy (Table 2). We were unable to correlate
ADTd with time to distant metastasis, death from prostate
cancer, or death from any cause due to an insufficient number
of events (p = 0.11, 0.20, and 0.85, respectively).
The subset of patients who received ADT only prior to or
concurrent with radiotherapy (NAADT) showed results qual-
itatively similar to those of the overall cohort. The predomi-
nant effect of NAADT was seen in the first 6 months of ADT,
with a reduction in the risk of bF of 30.2% (95% CI,
19.5%–39.5%), 46.6% (95% CI, 32.4%–57.8%), and
47.6% (95% CI, 33.4%–58.8%) associated with 3, 6, and 9
months, respectively, of ADT use prior to and concurrent
with radiotherapy.
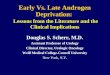
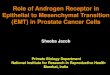
Investigation of ADTd interactionsClinical stage and radiation dose had statistically signifi-
cant interactions with ADTd. When we used the bF endpoint,
dose dichotomization at the median biologically equivalent
dose (68 Gy) showed lower doses had a higher baseline fail-
ure rate coupled with a prominent effect to prolonged ADT
administration, which was less pronounced in those treated
with higher doses (p = 0.007). This translated into a 46%
(95% CI, 35%–54%), 76% (95% CI, 66%–83%), and 82%

Table 1. Demographics of the total cohort*
Center
Variable Subgroup BCCA (n = 992) FCCC (n = 1007) PMCC (n = 608) WBH (n = 1059) Combined (n = 3,666)
Age (years) 71 (56–80) 68 (52–78) 70 (54–79) 73 (57–84) 71 (54–82)iPSA (ng/ml) 9.4 (1.6–46.1) 8.3 (3.1–41.0) 11.5 (2.7–60.8) 8.3 (2.0–90.8) 9.1 (2.2–58.6)Gleason Score 2–5 298 (30%) 89 (9%) 79 (13%) 258 (24%) 724 (20%)
6 291 (29%) 565 (56%) 255 (42%) 484 (46%) 1595 (44%)7 289 (29%) 282 (28%) 215 (35%) 211 (20%) 997 (27%)
8–10 114 (11%) 71 (7%) 59 (10%) 106 (10%) 350 (10%)Clinical Stage 1a–c 183 (18%) 436 (43%) 72 (12%) 290 (27%) 981 (27%)
2a–b 396 (40%) 389 (39%) 156 (26%) 531 (50%) 1472 (40%)2c 107 (11%) 112 (11%) 147 (24%) 193 (18%) 559 (15%)3a 171 (17%) 49 (5%) 134 (22%) 17 (2%) 371 (10%)
3b–4 135 (14%) 21 (2%) 99 (16%) 28 (3%) 283 (8%)Risk group Low 89 (9%) 242 (24%) 24 (4%) 158 (15%) 513 (14%)
Intermediate 479 (48%) 552 (55%) 278 (46%) 646 (61%) 1960 (53%)High 424 (43%) 208 (21%) 306 (50%) 255 (24%) 1193 (33%)
ADT Duration(months)
10.1 (1.2–38.8) 8.0 (1.1–41.0) 5.9 (1.8–38.0) 7.0 (2.7–33.7) 8.0 (1.1–39.0)
ADT type None 539 (54%) 816 (81%) 349 (57%) 1010 (95%) 2714 (74%)NAAD/C 283 (29%) 105 (10%) 195 (32%) 47 (4%) 630 (17%)
NAAD/C/AAD 165 (17%) 83 (8%) 56 (9%) 2 (0%) 306 (8%)AAD 5 (1%) 3 (0%) 8 (1%) 0 (0%) 16 (0%)
Dose (Gy) 66.0 (52.5–70.0) 75.8 (70.5–82.1) 70.0 (66.0–74.0) 66.6 (66.0–77.4) 68.4 (64.0–82.1)BED (Gy) 66.0 (59.1–70.0) 72.8 (67.8–78.6) 70.0 (66.0–74.0) 64.7 (63.4–78.6) 68.0 (63.2–78.6)Follow-up (months) 85.0 (42.4–127.6) 66.7 (38.6–122.4) 62.2 (38.1–97.8) 83.7 (37.9–156.7) 75.2 (38.5–134.8)
Abbreviations: BCCA = British Columbia Cancer Agency; FCCC = Fox Chase Cancer Center; PMCC = Peter MacCallum Cancer Center;WBH = William Beaumont Hospital; iPSA = initial prostate specific antigen; NAAD = neoadjuvant androgen deprivation; C = concurrent;AAD = adjuvant androgen deprivation; BED = biologically effective dose in 2-Gy fractions estimated using an a/b ratio = 2 Gy.
* Table shows demographics of the total cohort divided by treating centre. Numbers are counts (percentage) for categorical data and median(95% CI) for continuous data.
726 I. J. Radiation Oncology d Biology d Physics Volume 79, Number 3, 2011
(95% CI, 65%–92%) reduction in relative risk of bF related to
6, 18, or 36 months of ADT (Table 3), respectively, in those
treated to equivalent doses of 68 Gy or less and a 27% (95%
CI, 12%–44%), 50% (95% CI, 25%–68%), and 49% (95%
CI, 19%–67%) reduction, respectively, in those treated to
higher doses (Fig. 2).
The addition of a term interacting trichotomous clinical
stage category with ADT duration significantly improved
Months of Androgen Deprivation
Rel
ativ
e R
isk
Red
uctio
n (%
)
0 6 12 18 24 30 36
100
90
80
70
60
50
40
30
20
10
0
Fig. 1. The relative effect of increasing durations of ADT on bF, in-creasing from 0 to 36 months duration along with 95% CIs. Graylines represent the relative risk reduction curves of 20 random boot-strap resampled values used to calculate the CIs.
a model already independently utilizing these covariates
(p = 0.016). Compared to the risk of failure in those receiving
no ADT, the respective relative risk of failure associated with
6, 18, or 36 months of ADT was reduced by 34% (95% CI,
21%–46%), 58% (95% CI, 41%–71%), and 48% (95% CI,
19%–71%), respectively, for cT2 cancers (Table 3), and
45% (95% CI, 35%–55%), 74% (95% CI, 63%–82%), and
76% (95% CI, 56%–84%) for cT3 cancers (Fig. 2). Estimates
beyond 6 months of ADTd were unreliable with cT1 cancers
due to low numbers of events with which to model (risk re-
duction at 6 months of ADTd, 10%; 95% CI,�25% to 41%).
To assess the relative predictive power afforded by consid-
ering the interactions, comparison of the individual predic-
tors, c2 � df, showed the interactive variables to have
considerably less impact than the primary ADTd effect (c2
� df of 9.6 and 8.8 for ADTd interactive with dose and stage,
respectively, and 41.4 for ADTd alone) and much less than
the impact of iPSA (c2� df = 274.9). Examining other prog-
nostic variables for interaction effect, classification by risk
(low, intermediate, or high) showed no impact on ADT dura-
tion effect (p = 0.25) nor did age, PSA, or GS (p = 0.22, 0.81,
0.47, respectively).
For the NAADT subset, statistically significant interac-
tions were seen between NAADT duration and both radio-
therapy dose (p = 0.027) and clinical T stage (p = 0.01),
which were functionally similar to those seen in the complete
cohort. There was not enough information about pure AAD

Table 2. The relative benefit to various ADT durations*
Proposed total ADT duration
ADT duration alreadyreceived (months)
3 months(range)
6 months(range)
9 months(range)
12 months(range)
18 months(range)
24 months(range)
36 months(range)
None 21 (16–26) 38 (29–46) 50 (39–59) 58 (47–67) 65 (54–74) 66 (55–75) 66 (51–77)3 16 (13–19) 27 (22–30) 34 (29–37) 41 (36–44) 44 (37–48) 45 (29–54)6 11 (9–11) 17 (15–19) 25 (21–27) 28 (21–33) 29 (11–39)9 7 (6–7) 14 (11–17) 17 (10–22) 18 (1–28)
12 7 (5–9) 10 (4–15) 8 (7–14)18 3 (�1 to �5) 4 (�10 to �12)24 1 (�9 to �6)
Abbreviations: as in Table 1.* The relative benefit to various ADT durations is shown in comparison to the ADT duration so far received. A man with a baseline failure
risk of 50% would have this risk reduced by an absolute 25% by completing 9 months of ADT. At the end of that 9 months, should he consideranother 9 months of ADT, then his failure risk would potentially be further reduced by 14% in relative terms by reaching the end of that du-ration, equating to an absolute benefit of 7% (with a plausible range of 5.5 to 8.5%).
Androgen deprivation duration effect d S. WILLIAMS et al. 727
for a reliable evaluation of duration effect or evaluation of the
timing of ADT relative to that for radiation therapy.
Predictions of the absolute ADT effect in the individualA nomogram which graphically summarizes the multivari-
able model is shown in Fig. 3. This figure shows the baseline
absolute risk of failure without the use of ADT. The absolute
benefit potentially gained by differing durations of ADT can
then be directly calculated using the appended values. Cali-
bration of this model using internal bootstrap validation
was excellent (Fig. 4), with all levels of expected outcomes
having confidences intervals covering the expected levels.
DISCUSSION
The seminal randomized studies (2–4, 20, 21) that proved
the efficacy of ADT combined with radiation have led to
a massive increase in the use of leutinizing hormone-releas-
ing hormone over the last decade (22, 23), although this trend
may be declining somewhat recently (24). While extrapola-
tion of these results to the contemporary clinic could be
expected to improve survival and other endpoints, there
will be a significant toxicity burden, which for some men
limits their acceptance of this therapy.
Clinically, it is often difficult to determine the correct bal-
ance between expected efficacy and the countering toxicity
for an individual patient. As the randomized studies that
guide our clinical decisions all had differences in ADTd,
treatment technique, patient characteristics, and endpoints,
it is unlikely that randomized data will be available to guide
us for all clinical scenarios. For those patients with high-risk
cancers, a prolonged (at least 2 years) ADTd is recommended
(25), based largely on an overall survival advantage that was
seen in one European ADT study performed prior to the PSA
era, where most patients had bulky tumors (20). With a moti-
vation similar to that of the current study, a meta-analysis of
the Radiation Therapy Oncology Group (RTOG) studies
from a similar era (6) used predefined risk strata based on
stage and grade (including pathological node-positive cases).
Although the iPSA levels were only available in <20% of
cases, there was the undoubted advantage of central pathol-
ogy review and long follow-up. Subgroup evaluation showed
that patients with bulky, high-grade, or node-positive cancers
most often benefited from long-term ADT, while those with
low-risk features (GS, 2–6; stage T1–T2, and unknown PSA)
showed no benefit from ADT. Where less advanced tumors
predominated in a study performed in the PSA era, an overall
survival benefit was limited to Gleason scores of 8 to 10 cases
(2). Further confounding our ability to rationalize the need for
ADT are the increased radiation doses used in contemporary
radiation oncology, which are known to improve clinical out-
comes (but not overall survival, as yet) in diverse risk groups
without ADT use (26, 27).
At the other end of the spectrum, the use of ADT in pa-
tients with low-risk cancers may lead to a survival detriment
(28) and is not a recommended intervention, especially when
dose escalation advantages are considered (26, 27). Interme-
diate risk patients present a more difficult decision-making
scenario, where both ADTd (none or short-term therapy)
and radiotherapy dose (conventional or escalated) are recom-
mended options, either in unison or in combination (25). Pre-
dictive variables which can be used to determine the need for
ADT in an individual within this group of patients are pres-
ently lacking.
With these data, we present a unifying approach to ratio-
nalize many of these issues in the individual patient. The re-
sults show the impact of ADT on risk of bF to be significant,
predictable, and highly nonlinear, with increasing benefits
until the impact reached an apparent zenith at approximately
18 months. In biological terms, these data suggest that apart
from the small but significant interaction with the primary
tumor bulk, the response to various durations of ADT is in-
dependent of conventional prognostic factors and therefore,
whether low, intermediate, or high risk, all cancers have
similar biological responses where increasing ADT durations
always result in greater effect.
The other interaction of significance, and the only one
open to a clinician’s control, was that of radiation dose. Level
Tab
le3
.H
azar
dra
tio
sas
soci
ated
wit
hd
iffe
rin
gd
ura
tio
ns
of
AD
T*
AD
Td
ura
tio
n(r
ang
e)
Var
iab
leS
ub
set
0(m
on
ths)
3(m
on
ths)
6(m
on
ths)
9(m
on
ths)
12
(mo
nth
s)1
8(m
on
ths)
24
(mo
nth
s)3
6(m
on
ths)
Tst
age
T1
0.4
0(0
.31
–0
.52
)0
.38
(0.2
9–
0.4
9)
0.3
6(0
.25
–0
.52
)0
.34
(0.2
0–
0.5
6)
0.3
1(0
.17
–0
.57
)0
.25
(0.1
2–
0.5
1)
0.1
8(0
.07
–0
.51
)0
.10
(0.0
1–
0.7
6)
T2
0.6
1(0
.50
–0
.74
)0
.49
(0.4
0–
0.6
0)
0.4
0(0
.31
–0
.51
)0
.33
(0.2
4–
0.4
5)
0.2
9(0
.20
–0
.41
)0
.26
(0.1
8–
0.3
9)
0.2
8(0
.18
–0
.41
)0
.33
(0.1
8–
0.6
1)
T3
1.0
0(r
efer
ence
)0
.73
(0.6
7–
0.8
0)
0.5
5(0
.45
–0
.67
)0
.41
(0.3
1–
0.5
5)
0.3
3(0
.23
–0
.47
)0
.26
(0.1
8–
0.3
9)
0.2
5(0
.17
–0
.37
)0
.24
(0.1
5–
0.4
0)
Do
se>
68
.0G
y0
.58
(0.4
5–
0.7
4)
0.5
0(0
.40
–0
.62
)0
.43
(0.3
4–
0.5
5)
0.3
8(0
.28
–0
.51
)0
.34
(0.2
4–
0.4
8)
0.3
1(0
.21
–0
.44
)0
.30
(0.2
1–
0.4
2)
0.2
9(0
.19
–0
.45
)#
68
.0G
y1
.00
(ref
eren
ce)
0.7
3(0
.67
–0
.80
)0
.54
(0.4
5–
0.6
5)
0.4
0(0
.31
–0
.52
)0
.32
(0.2
3–
0.4
4)
0.2
4(0
.17
–0
.34
)0
.22
(0.1
4–
0.3
3)
0.1
9(0
.09
–0
.39
)
*T
he
haz
ard
rati
os
asso
ciat
edw
ith
dif
feri
ng
du
rati
on
so
fA
DT
are
sho
wn
on
the
sub
seq
uen
td
evel
op
men
to
fb
Fb
yT
stag
ean
dra
dia
tio
nd
ose
.HR
wit
h9
5%
CIs
of
HR
sd
eriv
edfr
om
bo
ots
trap
resa
mp
lin
g.
Months of Androgen Deprivation
Rel
ativ
e R
isk
Red
uctio
n (%
)
0 6 12 18 24 30 36
100
90
80
70
60
50
40
30
20
10
0
68 Gy or less
>68 Gy
(a)
pinteraction 0.007
Months of Androgen Deprivation
Rel
ativ
e R
isk
Red
uctio
n (%
)
0 6 12 18 24 30 36
100
90
80
70
60
50
40
30
20
10
0
cT1+2
cT3
(b)
pinteraction 0.016
Fig. 2. The normalized relative benefit of differing ADTd for sub-groups of radiation dose (a) and T stage (b). Radiation dose isexpressed as the equivalent dose in 2-Gy fractions based on ana/b ratio = 2 Gy.
728 I. J. Radiation Oncology d Biology d Physics Volume 79, Number 3, 2011
1 evidence of benefit from multiple randomized trials now
exists in support of increased radiation doses in the absence
of (26, 27, 29), or with, ADT (30, 31). Similarly, high-level
evidence exists for benefit in using ADT with standard radi-
ation doses (#70 Gy) (2, 4, 20, 32). This tumor control ben-
efit comes at a cost of toxicity, which is primarily related to
rectal complications in the dose escalation studies (26, 27,
31) and castration toxicity in ADT studies (33). The identifi-
cation of an interaction between ADTd and radiation dose is
of great interest, therefore, as it suggests that contemporary
radiotherapy doses (>70 Gy) may require shorter ADTd.
One approach would be to use these data to individually
direct the proposed ADTd to potential risk, with a desire to
optimize the therapeutic ratio. The cornerstone of this re-
quires evaluating the baseline risk of failure without ADT;
essentially, a more detailed version of standard risk criteria.
Knowing the behavior of ADT over time then enables poten-
tial benefit derivation which can be offset by how much tox-
icity the patient is willing to trade for benefit. For example,
assume a 5% absolute bF improvement at a given time point
would be the minimum acceptable to most patients and their
oncologists. Knowing that 3 months of ADT provides a 21%
relative risk reduction of bF, men with an absolute baseline
failure risk of $24% (range, 19%–31%) would derive

Fig. 3. A nomogram used to derive 60- and 90-month predicted probability of bF following completion of therapy incor-porating the ADTd.
Androgen deprivation duration effect d S. WILLIAMS et al. 729
$5% benefit (5/0.213 = 3.8). Similarly, those patients with
$13% failure risk would have this absolute improvement
in bF risk if $6 months of ADT was used. Correspondingly,
having defined the benefit to incremental increases in ADT
duration, we can see that a man who has already had 6 months
of ADT would gain at least another 5% absolute benefit by
completing another 3 months of ADT if he had a $45% base-
line risk. Alternatively, if his failure risk was 17% at baseline,
he would require an additional 30 months of therapy to see
a 5% benefit, which may not be a compelling argument. If
a man has reached 12 months ADTd and is tolerating it
0.2 0.4 0.6 0.8 1.0
0.2
0.4
0.6
0.8
1.0
5 Year FFbF predicted by Nomogram
Obs
erve
d 5
Year
FFb
F
Fig. 4. Calibration curve for the nomogram. The X axis portrays thenomogram predicted freedom from bF and the Y axis the observedvalues and 95% CI ranges from bootstrap resampling.
poorly, then he can be counseled that if his baseline risk
was <63%, he will not be losing more than 5% in absolute
biochemical benefit by not undertaking a further 6 to 24
months of therapy.
On the other hand, accurate predictions of ADT toxicity
are difficult to make. Following ADT cessation, functional
androgen recovery is variable, with approximately 90% of
men recovering within 3 years. Testosterone recovery ap-
pears to depend more on initial testosterone and age, rather
than the prescribed duration of ADT per se (34, 35), and
the duration of suppression likely exceeds that prescribed
by several months (34). Although testosterone levels were
not available in the present data, the prescribed ADT duration
rather than the physiological castration duration is the only
variable open to the physician, and hence the study data
may be more indicative of the clinical situation. Toxicity of
ADT includes not only those side effects that may be catego-
rized as a bothersome (such as hot flashes and erectile dys-
function) but also potentially serious complications such as
osteoporotic fracture or metabolic syndrome with attendant
risks of diabetes and weight gain (9, 36). Premature cardiac
death has also been identified (33), although this may be con-
fined to those with preexisting cardiac dysfunction (37).
Many patients are willing to trade quantity for improved
quality of life (38, 39), which becomes pertinent if ADTd be-
yond 18 months are predominately contributing to toxicity
rather than tumor control.
While the conclusions of our analysis may be weakened by
their generation from observational rather than randomized
data, this can also be a strength in terms of our specific
aims. Although ADT has unequivocal benefit based on
randomized controlled trial data, the fixed inclusion criteria
these studies utilize can limit the extrapolation of findings

730 I. J. Radiation Oncology d Biology d Physics Volume 79, Number 3, 2011
to the individual. To extend known ADT efficacy to either
subgroups of patients or individuals with prognostic features
outside those of the randomized studies (the establishment of
ADT ‘‘effectiveness’’ in these patients [40]), a range of data
and patient selection methods outside of those of the original
study criteria need to be to be examined. By employing mul-
ticenter data, interactive covariates, and a nonparametric
bootstrap method, we have developed model estimates which
are likely robust yet conservative (18, 19), suggesting appli-
cability across a broad range of cohorts, as reinforced by in-
ternal validation. Comparisons to published randomized trial
trials of ADTd also suggests that external validity is also sat-
isfactory. An Australian study (4) comparing 3 or 6 months of
ADT to none shows a Phoenix definition FFbF hazard ratio
(HR) of 0.70 (range, 0.56-0.88) and 0.58 (range, 0.46-
0.74), respectively, corresponding well to our predictions
of 0.79 (range, 0.74-0.84) and 0.62 (range, 0.54-0.71). In lon-
ger-term ADT studies, the Radiation Therapy Oncology
Group (RTOG) 9202 study (2) comparing 4 to 24 months
of ADT showed the 5-year risk of bF (ASTRO definition)
to be reduced from 55% to 28%, closely consistent with
that predicted (44% relative improvement for 3 to 24
months). Similarly, longer-term ADT data from Europe (1),
using a different bF definition, observed a HR of 0.42
(95% CI, 0.28–0.64). That value well approximates our find-
ing of an HR range at 36 months of 0.24 to 0.47 despite that
study’s use of 70 Gy of radiation. Those investigators’ recent
randomized follow-up study (41) finding that 6 months of
ADT was inferior to 36 months of ADT in locally advanced
disease may have been anticipated, although actuarial bF data
are not available for direct comparison.
CONCLUSIONS
In conclusion, we have shown that the bulk of the benefit of
AADT occurs in the first year of treatment (approximately
85% of that obtainable from a full 3 years, on average), with
relatively little additional benefit from the second (a further
5%). Due to the modeled minimal additional benefit, recom-
mendations for 3 years of ADT over 2 years cannot be
substantiated. When faced with these figures, many oncolo-
gists and their patients will choose a balance between ongoing
symptoms of castration and chance of cancer control. ADTd
can be specifically tailored to risk. Those patients with locally
advanced tumors may have greater benefit from ADT, as may
those treated with lower radiation doses. To what extent dose
escalation obviates this benefit requires prospective analysis
and evaluation on more advanced endpoints.
REFERENCES
1. Bolla M, Collette L, Blank L, et al. Long-term results withimmediate androgen suppression and external irradiation inpatients with locally advanced prostate cancer (an EORTCstudy): A phase III randomised trial. Lancet 2002;360:103–106.
2. Hanks GE, Pajak TF, Porter A, et al. Phase III trial of long-termadjuvant androgen deprivation after neoadjuvant hormonal cy-toreduction and radiotherapy in locally advanced carcinoma ofthe prostate: The Radiation Therapy Oncology Group Protocol92-02. J Clin Oncol 2003;21:3972–3978.
3. Pilepich MV, Caplan R, Byhardt RW, et al. Phase III trial of an-drogen suppression using goserelin in unfavorable-prognosiscarcinoma of the prostate treated with definitive radiotherapy:Report of Radiation Therapy Oncology Group Protocol 85-31.J Clin Oncol 1997;15:1013–1021.
4. Denham JW, Steigler A, Lamb DS, et al. Short-term androgendeprivation and radiotherapy for locally advanced prostate can-cer: Results from the Trans-Tasman Radiation Oncology Group96.01 randomised controlled trial. Lancet Oncol 2005;6:841–850.
5. Cooperberg MR, Grossfeld GD, Lubeck DP, et al. Nationalpractice patterns and time trends in androgen ablation for local-ized prostate cancer. J Natl Cancer Inst 2003;95:981–989.
6. Roach M 3rd, Lu J, Pilepich MV, et al. Predicting long-term sur-vival, and the need for hormonal therapy: A meta-analysis ofRTOG prostate cancer trials. Int J Radiat Oncol Biol Phys2000;47:617–627.
7. Beasley M, Williams SG, Pickles T. Expanded risk groups helpdetermine which prostate radiotherapy sub-group may benefitfrom adjuvant androgen deprivation therapy. Radiat Oncol2008;3:8.
8. Loblaw DA, Mendelson DS, Talcott JA, et al. AmericanSociety of Clinical Oncology recommendations for the initialhormonal management of androgen-sensitive metastatic, recur-rent, or progressive prostate cancer. J Clin Oncol 2004;22:2927–2941.
9. Keating NL, O’Malley AJ, Smith MR. Diabetes and cardiovas-cular disease during androgen deprivation therapy for prostatecancer. J Clin Oncol 2006;24:4448–4456.
10. Smith MR, Lee WC, Brandman J, et al. Gonadotropin-releasinghormone agonists and fracture risk: A claims-based cohortstudy of men with nonmetastatic prostate cancer. J Clin Oncol2005;23:7897–7903.
11. Green HJ, Pakenham KI, Headley BC, et al. Quality of life com-pared during pharmacological treatments and clinical monitor-ing for non-localized prostate cancer: A randomizedcontrolled trial. BJU Int 2004;93:975–979.
12. Bahnson RR, Hanks GE, Huben RP, et al. NCCN practiceguidelines for prostate cancer. Oncology (Williston Park)2000;14:111–119.
13. Pickles T, Kim-Sing C, Morris WJ, et al. Evaluation of theHouston biochemical relapse definition in men treated with pro-longed neoadjuvant and adjuvant androgen ablation and assess-ment of follow-up lead-time bias. Int J Radiat Oncol Biol Phys2003;57:11–18.
14. Buyyounouski MK, Hanlon AL, Eisenberg DF, et al. Definingbiochemical failure after radiotherapy with and without andro-gen deprivation for prostate cancer. Int J Radiat Oncol BiolPhys 2005;63:1455–1462.
15. Kestin LL, Vicini FA, Martinez AA. Practical application ofbiochemical failure definitions: What to do and when to do it.Int J Radiat Oncol Biol Phys 2002;53:304–315.
16. Williams SG, Buyyounouski MK, Pickles T, et al. Percentageof biopsy cores positive for malignancy and biochemical failurefollowing prostate cancer radiotherapy in 3,264 men: Statisticalsignificance without predictive performance. Int J Radiat OncolBiol Phys 2008;70:1169–1175.
17. Roach M 3rd, Hanks G, Thames H Jr., et al. Defining biochem-ical failure following radiotherapy with or without hormonaltherapy in men with clinically localized prostate cancer: Recom-mendations of the RTOG-ASTRO Phoenix consensus confer-ence. Int J Radiat Oncol Biol Phys 2006;65:965–974.

Androgen deprivation duration effect d S. WILLIAMS et al. 731
18. Harrell FE Jr., Lee KL, Mark DB. Multivariable prognosticmodels: Issues in developing models, evaluating assumptionsand adequacy, and measuring and reducing errors. Stat Med1996;15:361–387.
19. Assmann SF, Pocock SJ, Enos LE, et al. Subgroup analysis andother (mis)uses of baseline data in clinical trials. Lancet 2000;355:1064–1069.
20. Bolla M, Gonzalez D, Warde P, et al. Improved survival in pa-tients with locally advanced prostate cancer treated with radio-therapy and goserelin. N Engl J Med 1997;337:295–300.
21. Pilepich MV, Winter K, John MJ, et al. Phase III radiation ther-apy oncology group (RTOG) trial 86-10 of androgen depriva-tion adjuvant to definitive radiotherapy in locally advancedcarcinoma of the prostate. Int J Radiat Oncol Biol Phys 2001;50:1243–1252.
22. Park S, Meng MV, Elkin EP, et al. Androgen deprivation usewith external beam radiation for prostate cancer: Results fromCaPSURE. J Urol 2005;174:1802–1807.
23. Shahinian VB, Kuo YF, Freeman JL, et al. Increasing use ofgonadotropin-releasing hormone agonists for the treatment oflocalized prostate carcinoma. Cancer 2005;103:1615–1624.
24. Weight CJ, Klein EA, Jones JS. Androgen deprivation falls asorchiectomy rates rise after changes in reimbursement in theU.S. Medicare population. Cancer 2008;112:2195–2201.
25. Mohler J, Babaian RJ, Bahnson RR, et al. Prostate cancer. Clin-ical practice guidelines in oncology. J Natl Compr Cancer Net-work 2007;5:650–683.
26. Kuban DA, Tucker SL, Dong L, et al. Long-term results of theM.D. Anderson randomized dose-escalation trial for prostatecancer. Int J Radiat Oncol Biol Phys 2008;70:67–74.
27. Zietman AL, DeSilvio ML, Slater JD, et al. Comparison of con-ventional-dose vs high-dose conformal radiation therapy inclinically localized adenocarcinoma of the prostate: a random-ized controlled trial. JAMA 2005;294:1233–1239.
28. Lu-Yao GL, Albertsen PC, Moore DF, et al. Survival followingprimary androgen deprivation therapy among men with local-ized prostate cancer. JAMA 2008;300:173–181.
29. Zietman AL. Correction: Inaccurate analysis and results ina study of radiation therapy in adenocarcinoma of the prostate.JAMA 2008;299:898–899.
30. Dearnaley DP, Sydes MR, Graham JD, et al. Escalated-doseversus standard-dose conformal radiotherapy in prostate cancer:
First results from the MRC RT01 randomised controlled trial.Lancet Oncol 2007;8:475–487.
31. Peeters STH, Heemsbergen WD, Koper PCM, van Putten WLJ,Slot A, Dielwart MFH, Bonfrer JMG, IncrocCi, L, Lebesque JV.Dose-response in radiotherapy for localized prostate cancer: Re-sults of the Dutch Multicenter Randomised Phase III Trial com-paring 68 Gy of radiotherapy with 78 Gy. J Clin Oncol 2006;24:1990–1996.
32. D’Amico AV, Manola J, Loffredo M, et al. 6-month androgensuppression plus radiation therapy vs radiation therapy alone forpatients with clinically localized prostate cancer: A randomizedcontrolled trial. JAMA 2004;292:821–827.
33. D’Amico AV, Denham JW, Crook J, et al. Influence of andro-gen suppression therapy for prostate cancer on the frequencyand timing of fatal myocardial infarctions. J Clin Oncol 2007;25:2420–2425.
34. Pickles T, Agranovich A, Berthelet E, et al. Testosterone recov-ery following prolonged adjuvant androgen ablation for prostatecarcinoma. Cancer 2002;94:362–367.
35. Spry NA, Kristjanson L, Hooton B, et al. Adverse effects toquality of life arising from treatment can recover with intermit-tent androgen suppression in men with prostate cancer. Eur JCancer 2006;42:1083–1092.
36. Tsai HK, D’Amico AV, Sadetsky N, et al. Androgen depriva-tion therapy for localized prostate cancer and the risk of cardio-vascular mortality. J Natl Cancer Inst 2007;99:1516–1524.
37. Nanda A, Chen MH, Braccioforte MH, et al. Hormonal therapyuse for prostate cancer and mortality in men with coronary ar-tery disease-induced congestive heart failure or myocardial in-farction. JAMA 2009;302:866–873.
38. Crawford ED, Bennett CL, Stone NN, et al. Comparison of per-spectives on prostate cancer: analyses of survey data. Urology1997;50:366–372.
39. van Tol-Geerdink JJ, Stalmeier PF, van Lin EN, et al. Dopatients with localized prostate cancer treatment really wantmore aggressive treatment? J Clin Oncol 2006;24:4581–4586.
40. Antman K, Amato D, Wood W, et al. Selection bias in clinicaltrials. J Clin Oncol 1985;3:1142–1147.
41. Bolla M, de Reijke TM, Van Tienhoven G, et al. Duration ofandrogen suppression in the treatment of prostate cancer.N Engl J Med 2009;360:2516–2527.