Embed Size (px)
Citation preview

Kidney International, Vol. 36 (1989), pp. 891—896
Predictive value of renal pathology in diffuse proliferativelupus glomerulonephritis
MELVIN M. SCHWARTZ, JAY BERNSTEIN, GARY S. HILL, KEITH HOLLEY,ELIZABETH A. PHILLIPS, and THE Luus NEPHRITIS COLLABORATIVE STUDY GROUP
The Lupus Nephritis Collaborative Study Group: Clinical Coordinating Center: Edmund J. Lewis, Principal Investigator, B.S. Kasinath, Co-principal Investigator, Anil K. Bidani, Director, Central Immunology Laboratory, Rush-Presbyterian-St. Luke's Medical Center, Chicago,
Illinois. Biostatistics Coordinating Center: John Lachin, Shu-ping Lan, Elizabeth A. Phillips, George Washington University, Bethesda,Maryland. Pathology Reading Committee: Melvin M. Schwartz, Chairman and Director of the Central Pathology Laboratory, Rush-
Presbyterian-St. Luke's Medical Center, Chicago, Illinois; Jay Bernstein, William Beaumont Hospital, Royal Oak, Michigan; Gary S. Hill,Francis Scott Key Medical Center, Baltimore, Maryland; Keith Holley, Mayo Clinic, Rochester, Minnesota. Clinics: Marc A. PohI, John
Clough, Gordon Gephardt, Cleveland Clinic, Cleveland, Ohio; Tomas Berl, University of Colorado, Denver, Colorado; Nathan Levin, HenryFord Hospital, Detroit, Michigan; Lawrence G. Hunsicker, Stephen Bonsib, University of Iowa, Iowa City, Iowa; Norman Simon, Hartmann
Friederici, Evanston Hospital, Evanston, Illinois; Francesco del Greco, Frank A. Carone, Northwestern University, Chicago, Illinois; LeeHebert, Han M. Sharma, Ohio State University, Columbus, Ohio; Eric Neilson, John Tomazewski, University of Pennsylvania, Philadelphia,
Pennsylvania; Howard L. Corwin, Melvin M. Schwartz, Rush-Presbyterian-St. Luke's Medical Center, Chicago, Illinois; Andrew Levey,Angelo Ucci, Tufts-New England Medical Center, Boston, Massachusetts; Howard Shapiro, Barbara F. Rosenberg, William Beaumont
Hospital, Royal Oak, Michigan; Jacob Lemann, John Garancis, Medical College of Wisconsin, Milwaukee, Wisconsin; Kenneth Shapiro,Praveen Chander, New York Medical College, Valhalla, New York; Fred Whittier, John W. Graves, Joan Bathon, Roger Riley, West Virginia
University, Morgantown, West Virginia, USA
Predictive value of renal pathology in diffuse proliferative lupus gb-merulonephritis. We tested the value of the activity (A!) and chronicity(CI) indices devised by Austin et alE!, 21 as predictors of outcome inlupus patients with diffuse proliferative glomerulonephntis (DPGN).Four renal pathologists independently scored the Al and CI on 84 renalbiopsy specimens from patients with lupus DPGN followed for 109 74weeks (mean SD), and the mean score was compared to thedevelopment of renal failure and to adverse outcome (combined data forrenal failure, death and predefined clinical stop points). Receiveroperator characteristic curves were derived from a series of 2 x 2 tablesin which one variable was renal failure or adverse outcome and theother variable was Al or Cl dichotomized by a cut-off point. Over theentire range (0 to 10) of the CI there was no value that separatedpatients who developed renal failure from those who did not. The ROCcurve analysis indicated that the sensitivity and specificity of the CIwere too low to allow it to function as a good test. Once patientsentering renal failure were identified, the mean CI approached but didnot reach a significant difference when compared to the mean CI ofthose who did not go into renal failure (4,38 0.42, mean SE vs. 3.19
0.23, P = 0.0620). The Cl did not predict the adverse clinicaloutcomes, There was no cut-off value of the CI which separatedpatients who had an adverse outcome from those who did not, and thisresult was confirmed by ROC analysis. As a group, the patients whoreached an adverse outcome had a higher CI (4.12 0.37, mean SE)than those who did not (3.2 0.24), but this difference was notsignificant (P = 0.3944). In this population of patients with the his-tologic diagnosis of DPGN, there was no value for the Al over its entirerange (4 to 22) that predicted either renal failure or adverse outcome.The mean Al was not different either for those who developed renalfailure and those who did not (11.24 0.48, mean SE vs. 11.35 0.47,P = 0.7257) or for those with and without an adverse outcome (11.410.44, mean SE vs. 11.27 0.50, P = 0.7061). This finding indicates
Received for publication August 19, 1988and in revised form May 30, 1989Accepted for publication June 18, 1989
© 1989 by the International Society of Nephrology
that the degree of inflammation required for the diagnosis of DPON isalone predictive of outcome. Since the histological indices did notimprove the predictive value of the standard histological classification(ISKDC/WHO) in this group of patients with DPGN, we recommendholding in abeyance therapeutic decisions based upon the CI until itspredictive value is independently confirmed.
Glomerular pathology has been demonstrated to be an indi-cator of prognosis in the patient with systemic lupus erythema-tosus (SLE) [2—7]. Although patients falling within the categoryof diffuse proliferative glomerulonephritis (DPGN) have theworst prognosis among those with lupus nephritis, there ismarked variability in the clinical course. Because of this, effortshave been made to define the histological features associatedwith a poor renal prognosis. Austin et al [1, 2] have reportedthat a semiquantitative index of glomerular sclerosis, fibrousglomerular crescents, tubular atrophy, and interstitial fibrosis(Chronicity Index, CI) is a better indicator of renal failure thanis either a conventional histological classification system basedupon the extent and nature of the glomerular abnormality or anindex based upon the quantitation of active histological signs ofacute inflammation (Activity Index, Al). Because of the broadprognostic and therapeutic implications of these studies, others[8, 9] have attempted to duplicate their findings with conflictingresults.
As part of a multicenter, prospective, randomized trial of theeffect of plasmapheresis on outcome in severe SLE glomerulo-nephntis (GN), we have biopsied and studied a large number ofpatients with histologic diagnosis of DPGN as defined by theInternational Study of Kidney Disease in Children/WorldHealth Organization (ISKDC/WHO) Classification [10]. To testthe efficacy of the Al/Cl as predictors of outcome in patients
891

892 Schwartz et a!: Pathology of lupus glomerulonephritis
Number of patientsAgeMale/femaleCaucasianBlackHispanicOtherRenal involvement to biopsyDiastolic blood pressureSerum creatinineSerum C3Urine protein excretionAzathioprine within
3 months of biopsyAlkylating agent within
3 months of biopsyPrednisone therapy at time
of biopsya Mean SD
with SLE and DPGN, we scored each biopsy for activity andchronicity indices, and the histological indices were related tooutcome.
Methods
PatientsThe present analysis is based upon the 84 patients from whom
prerandornization renal biopsy specimens were available in theStudy of Plasmapheresis In Severe Lupus Nephritis undertakenby the Lupus Nephritis Collaborative Study Group (LNCSG).The detailed pathologic description of the biopsies [11] has beenreported elsewhere, The patients' clinical and laboratory valuesare given in Table 1. Admission criteria included: (a) a diagnosisof SLE conforming to the criteria of the American RheumatismAssociation [14]; (b) clinical evidence of' renal disease; (c) theabsence of defined exclusion criteria (Table 2); and (d) biopsydiagnosis of DPGN obtained within three weeks of randomiza-tion. The 85 patients who met the admission criteria wererandomized to either standard treatment or standard treatmentplus plasmapheresis to assess the clinical effect of plasmapher-esis in severe lupus GN. All patients received 60 mg/dayprednisone if they weighed less than 80 kg and 80 mg/day if theyweighed more than 80 kg. They received this dose for fourweeks, after which they were reevaluated and either continuedor entered into a regimen with tapering dosage. They alsoreceived cyclophosphamide, 2 mg/kg/day, for five weeks, fol-lowed by 1 mg/kg/day for 2 weeks. Cyclophosphamide was thendiscontinued [12]. The validity of the therapeutic trial dependedupon the homogeneity of the patients in the different treatmentgroups. A total of 45 demographic features, historical andtherapeutic details, physical findings, and laboratory data werecompared for the standard and the standard plus plasmaphere-sis groups, and they were similar in all respects [11]. The ARAcriteria gave us a standard for the diagnosis of systemic lupuserythematosus; the exclusion criteria assured us that the pa-tients were able to tolerate either therapeutic regimen and thatthey did not have end-stage kidney disease; the renal biopsydocumented the presence of "active" inflammation and/ornecrosis in fifty percent or more of the glomeruli. Thus, thepatients were homogeneous with respect to the severity of their
Table 2. Exclusion critera
A. Less than 16 years old.B. Currently pregnant.C. Serum creatinine greater than 6 mg/dl.D. Ever received plasmapheresis.E. Has a history of primary myocardial disease.F. Has a history of neoplasia within past 5 years.G. Has a history of prednisone associated psychosis.H. Has a history of peptic ulceration documental by radiology or
endoscopy within the past 3 years.I. Has evidence of primary active liver disease.J. Physician does not agree to patient participating in the study.
renal lesions, the type and severity of systemic symptoms, andthe therapy they received. The two treatment groups did notdiffer with respect to the prognosis of severe SLE GN, survival,development of renal failure, or the appearance or outcome ofsevere life-threatening complications [13]. Study entry andanalysis began at the time of randomization, and the length offollow-up ranged from 3 to 258 weeks with a mean of 109 74weeks (mean SD).
Renal pathologyPathology material. The Central Pathology Laboratory re-
ceived the following materials from the individual clinic pathol-ogists: (1) the set of histologic slides stained with hematoxylinand eosin, Masson's trichrome, periodic acid-Schiff (PAS), andPAS-silver methenamine that had been used in the clinic toestablish the histologic diagnosis and to determine eligibility; (2)photomicrographs documenting immunofluorescence stainingwith anti-IgG and anti-fibrin; and (3) copies of the electronmicrographs. Methodological details have been previously re-ported [13]. The morphological material was coded in theCentral Pathology Laboratory so the pathologists scoring thebiopsies would not have direct knowledge of the clinic labora-tories or of their pathologic diagnosis.
Definition of DPGN as an entry criterion. The biopsies wereclassified according to a modification of the ISKDC/WHOclassification of SLE ON [10]. DPGN, as described in theliterature [3—7], includes a heterogenous group of lesions thatare separated from less severe forms of lupus ON by signs of"severe" inflammation in the majority of the glomeruli. For thepurpose of this report the diagnosis of DPGN was establishedeither by: (1) involvement of all or nearly all (more than 80%) ofglomeruli by severe cellular proliferation and infiltration in aglobal endocapillary, mesangiocapillary or crescentic pattern orby prominent subendothelial deposits; or (2) severe segmentalUN with active histological evidence of inflammation in morethan 50% of the glomeruli [7, 15]. Patients with extensiveepimembranous immune deposits who also had severe prolifer-ative changes in more than 50% of glomeruli qualified to enterthis study. These forms of lupus GN are the most severe end ofthe morphologic spectrum of the ISKDC/WHO categories. Aminimum of ten glomeruli were required for classification, andthe 84 biopsies contained 19.4 10 glomeruli (mean SD).One-third of the biopsies had no hyalinized glomeruli, and thosewith obscolescent glomeruli had 2.9 0.6 glomeruli (meanSD) involved.
Activity and chronicity indices (Al/Cl). The published criteriafor scoring the Al/Cl were followed [1, 2]. The following
Table 1. Patient characteristics at baseline
8432.1 12.5 yearsa14/7060%22%7%
11%13.40 27.22 monthsa88 13 mm Hga2 1.30 mg/dla
57 29 mgldla5.5 4.2 g/24 hoursa
13%
7%
75%

Schwartz et a!: Pathology of lupus glomerulonephritis 893
features were scored on the basis of the percentage of totalglomeruli involved (less than 25 percent—i +, 25 to 50 per-cent—2+, and >50 percent—3 +): glomerular cell proliferation,karyorrhexis and fibrinoid necrosis, cellular crescents, hyalinedeposits (wire loops and hyaline thrombi), glomerular sclerosis,and fibrous crescents. Leukocyte exudation was scored on thenumber of neutrophils/glomerulus, (2/glomerulus—i +, 3/gb-merulus—2 +, 3 or more/glornerulus—3 +). Interstitial inflam-mation, tubular atrophy, and interstitial fibrosis were scored asmild (<20 percent—l+), moderate (20 to 40%) or severe(>40%) based on the proportion of cortical tissue involved. TheAl/Cl were the sum of the scores of the individual pathologicalfeatLres except for karyorrhexis/fibrinoid necrosis and cellularcrescents which were weighted (score x 2). The Al was thusdefined as the sum of the scores for glomerular proliferation,leukocyte exudation, karyorrhexis and fibrinoid necrosis (x2),cellular crescents (x2), hyaline deposits and interstitial inflam-mation. The maximum score for the AT was 24 points. The CIwas the sum of glomerular sclerosis, fibrous crescents, tubularatrophy, and interstitial fibrosis. The maximum score for the CIwas 12 points.
Pathology Reading Committee (PRC)The eligibility of the patient for entry into the study, based on
the renal pathology, was determined by the individual clinicpathologists, but histologic stratification and scoring of the A!and CI were accomplished by the PRC. As cases accrued, thePRC met at six month intervals and reached a consensus onhistologic diagnosis and patient eligibility in each case afterexamining all the pathology materials and filling out a detailedworksheet. The worksheet was sent to the LNCSG Biostatisti-cal Coordinating Center (BCC) in Bethesda, Maryland foranalysis. At the end of the Clinical Trial, the Chairman of thePRC (MMS) abstracted the criteria for the Al and CI, and, afterconsultation with the other members, a second worksheet wasconstructed. Each member independently scored each biopsyfor Al and CI. The worksheets containing each member's scorefor the Al and C! were sent to the BCC for analysis. Evaluationof Al/Cl in relation to outcome and pathologic diagnosis arebased upon the mean score of the four observers.
OutcomesThree endpoints were organized in the clinical trial: death
(due to renal and non-renal causes), chronic renal failure (serumcreatinine 6.0 mgldl or a rise in serum creatinine of >3.0mg/dl), or defined clinical stop points that indicated seriouscomplications due to SLE, the therapeutic program or anintercurrent disease process [12]. For this presentation onlyrenal failure and adverse outcome, the latter comprising allthree study endpoints, will be analyzed in relationship to the CIand the A!.
StatisticsSensitivity and specificity were determined from a series of 2
x 2 tables in which the binary outcome variable (renal failure/no renal failure; adverse outcome/no adverse outcome) is oneclassification and activity or chronicity dichotomized by acutoff point is the second classification. In this type of analysisthe 2 x 2 tables for each value of the test (CI or Al) allows thecalculation of a chi-square statistic [16]. When the specificity
Table 3. Chronicity index (CI) summarized by outcomes (Austin etal [2] definition of chronicity cut offs)
PresentN
Not presentN
TotalsN
Renal failureaCI�l 2a 11 13CI=2,3 5 24 29CI�4 16 26
T424
= 4.86
Adverse outcomeCI�1 2 11 13
CI=2,3 8 21 29CI�4 18- 24 424x2 = 403b
a Defined in textb None of the above statistics reach the 5% significance level, the
critical values for the chi-square distribution being 5.99 for 2 degrees offreedom (chronicity).
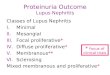
and sensitivity of each test value are plotted (ordinate =sensitivity and abscissa = 1— specificity), the resulting receiveroperator characteristics (ROC) curve describes the diagnosticefficacy of the test [17, 181. For example, in a test that has bothhigh sensitivity and specificity the ROC curve will be shifted upand to the left. The point where the rapidly rising curve shifts toa plateau will be the value separating the true positives from thetrue negatives. In contrast a curve with low sensitivity andspecificity will be a straight line midway between the axes. Foreach outcome, a Wilcoxon Rank Sum Test was carried out forboth Activity and Chronicity, within each Pathology Category.The tests, appropriately weighted, were combined over thesestrata and (applying the normal approximation) yielded P-values quoted in the text [19].
Results
Relationship of the CI to the specific outcome of renal failureThe CI did not predict renal failure as a specific outcome. The
entire range (range = 0 to 10) of CI scores was evaluated forpredictive efficacy, and there was no value of the CI thatseparated patients who developed renal failure from those whodid not develop renal failure (data not shown). For example,when the cutoff points, previously reported to have gradedpredictive values, were tested [2] (Table 3), they failed toseparate patients with and without renal failure. The same datawere used in the ROC analysis (Fig. 1), and the data revealed astraight line relationship. That is, for any value of the CI thepatient had a 50% chance of reaching the renal failure endpoint,and as a test, the C! did not predict the occurrence of renalfailure for individuals. While not prospectively predictive, themean CI of patients who developed renal failure was higherthan those who did not reach renal failure, but this analysis ofretrospective difference did not reach statistical significance(4.38 0.42, mean SE vs. 3.19 0.23, P = 0.0620).
Relationship of the CI to the combined study outcomesThe CI was tested against the combined study outcomes
(death, renal failure, and clinical stop points), and it did notpredict an adverse result. There was no value of the CI which

894 Schwartz a al: Pathology of lupus glomerulonephritis
0.6>Cl,C(0 0.4
separated patients who reached an adverse outcome from thosewho did not (data not shown), and the selected values of the CI[2] illustrated in Table 3 did not reach significance. The ROCanalysis based upon these data (Fig. 2) graphically demon-strates the predictive failure of the CI. As a group, the patientswho reached an adverse outcome had a higher CI (4.12 0.37,mean SE) than those who did not reach an adverse outcome(3.2 0.24), but the difference was not significant (P = 0.14).
Relationship of the Al to the spec j/ic outcome of renal failureand to the combined study endpoints (adverse outcome)
There was no predictive value for the Al over its entire range(range 4 to 22). When the patients were arbitrarily divided at ascore of 12 (12 < Al � 12) [2], there was no predictive value foreither renal failure or adverse outcome (Table 4). When the datain the 2 X 2 tables was used to determine specificity andsensitivity, ROC curves for renal failure (not shown) andadverse outcome (Fig. 3) were straight lines. Thus, the Al did
not predict renal failure or adverse outcome in our individualpatients with DPGN. When the mean AT for the group ofpatients who developed renal failure (11.24 0.48) was com-pared with the mean AT for the group of patients who did notdevelop renal failure (11.35 0.47), there was no difference (P= 0.7257). The mean Al was also tested for all the studyendpoints, and there was no difference between the group withadverse outcome (11.41 0.44, mean SE) and withoutadverse outcome (11.27 0.50, P = 0.385).
Discussion
The glomerular lesion of DPGN has been considered to carrya poor prognosis in lupus patients [2—7, 15], and it appears toreflect a degree of systemic disease activity that places thepatient at increased risk of both renal and non-renal complica-tions of SLE [2—7, 15]. In this study of a clinically well-definedgroup of patients with lupus DPGN who had been treatedaccording to defined therapeutic protocols, neither the Al nor
*
a
1.0
0.8
0.6>1C
0.4
0.2
0.0
a
Table 4. Activity index[21
(Al) summarized by outcomesdefinition of activity cut offs)
(Austin et al
Present Not present TotalsN N N
Renal failureaAI<12 iia 30 41AI�12 12 31
T43
= 0.0I2Adverse outcomea
AI<12 13 28 41AI�12 15 28 43
=
1.0
0.8
*
*
0.8
*
0.0 0.2 0.4 0.6 0.8 1.0 a Defined in textb None of the above statistics reach the 5% significance level, the
1 - Specificity critical values for the chi-square distribution being 3.84 for 1 degree ofFig. 1. ROC curve using CI as a test for renal failure. The curve freedom (activity).indicates that CI does not differentiate patients who develop renalfailure from those who do not.
1.0*
*
0.6 **
a,C0.4 *
0.2
—' 0.01.0 0.0 0.2 0.4 0.6 0.8 1.0
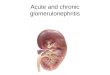
Fig. 3. ROC curve using Al as a test for the study endpoints (renalfailure, death and clinical stop points). The curve indicates that the Aldoes not distinguish patients who reach a study endpoint (adverseoutcome) from those who do not.
0.2 *
0.00.0 0.2 0.4 0.6 0.8
1 - SoecificityFig. 2. ROC curve using CI as a test for the study endpoints (renalfailure, death and clinical stop points). The curve indicates that CI doesnot distinguish patients who reach a study endpoint (adverse outcome)from those who do not.
*
*
1 - Specificity

Schwartz et a!: Pathology of lupus glomerulonephrizis 895
the CI identified the individuals who would develop adverseoutcomes or renal failure over a mean follow-up of 109 74(mean SD) weeks. There were no significant differences in theCI between groups of patients who did well and those who didpoorly, and the lack of a discriminating value for either the Alor the CI markedly reduces their prognostic value in individualpatients. Thus, the histological indices of glomerular injuryproposed by Austin et all 1, 2] failed to augment informationavailable from standard histopathologic evaluation.
Patients with an elevated CI, analyzed as a group, may be atgreater risk of developing renal failure than individuals withcomparable "active" glomerular lesions and no morphologicalevidence of chronicity. Austin et al reported that an elevated CIidentifies a group of patients at risk of developing renal failurewhen they are followed for four [1] and five [2] years. Rush etal [8] studied 20 children with diffuse proliferative lupus GN.Using an index of clinical outcome based on urinalysis, serumcreatinine, need for dialysis/transplantation, and death fromend-stage renal failure, they found that CI was predictive ofrenal outcome but the A! was not. However, the significance ofthese observations may be questioned. The presence of both anelevated CI and DPGN in a renal biopsy implies not onlyirreversible damage but the potential of further glomerulardestruction and loss of renal function. It is logical to reason thata patient with lupus nephritis who has travelled a portion of theroad to renal failure will develop renal insufficiency morequickly than a patient with comparable glomerular inflammationwho has not yet suffered irreversible nephron loss. The problemwith this tautological approach is that most patients with anelevated CI do not develop renal failure (Table 3). In fact, anelevated CI did not help us to identify the individual patient whodeveloped renal failure after a mean follow-up of 109 weeks.The reason that some patients with an elevated CI eventuallydevelop renal failure may be related to non-immunologicalfactors in the progression of chronic renal disease. A lessspeculative interpretation of the data, based upon our currentunderstanding of the pathogenesis of glomerular scarring andnephron loss in lupus nephritis, is that patients with an elevatedCI exhibit the sequelae of a protracted course and have a moreadvanced renal lesion at the time of biopsy.
The pathology seen on renal biopsy is frequently used as atherapeutic guide in addition to its role as a prognostic indicator[2, 7, 15]. The effectiveness of standard treatment and the lackof correlation between the activity index and outcome isattributed, at least in part, to the response to therapy of the"active" signs of inflammation that form the basis for theISKDC/WHO classification [20]. In contrast, Magil et al [9]found that the AT but not the CI predicted renal insufficiency(established Se,. = 2.0 mg/dl). General experience with lupusnephritis dating from the first renal biopsy study [3] indicatesthat patients with DPGN should be treated whether or not theglomerular lesion is accompanied by chronic parenchymaldamage. The CI indicates a level of chronic renal damage, andthe glomerular scars, tubular atrophy and interstitial fibrosisthat constitute the CI are thought to be irreversible and thera-peutically unresponsive. In drawing a distinction betweenchronic parenchymal damage and glomerular "activity," the CIhas focused attention on untreatable abnormalities. The rationaltherapy of lupus nephritis is directed at reducing the destructiveeffect of the active inflammatory lesion, and any implication
that the CI is an independent therapeutic guide should bediscouraged.
Technical issues regarding accurate quantitation and repro-ducibility of a histologic index must be taken into considerationif we are to evaluate the potential benefit of this parameter.Histopathologic grading systems, such as the activity andchronicity indices, are based upon a series of subjective inter-pretations. Differences among pathologists or between tempo-rally separate observations by a single pathologist are fre-quently a function of observer variation rather than realdifferences in pathology [21—23]. Even assuming that the his-tologic indices are reproducible, a minor amount of chronicdisease may significantly elevate the CI. Glomerular sclerosisinvolving less than 25% of the glomeruli and concomitanttubular atrophy and interstitial fibrosis can result in the calcu-lation of a CI of 2 or higher, and Austin et al report that patientswith even this level of chronicity had a significantly worsecourse than those with a CI of I or 0. However, analysis of theirpublished reports [1, 2] reveals 30 patients who did not developrenal failure who had glomerular lesions other than DPGN anda chronicity index of two or higher [24]. If the chronicity indexonly predicts renal failure in patients with DPGN, its usefulnessis considerably diminished in lupus, a disease with notoriousvariability in its rate of progression and a significant proportionof initially benign forms of glomerulonephritis that transform tomore aggressive lesions. The issues raised by Austin et al [1, 2,25, 26] in the histologic assessment of the renal biopsy in lupusare important. However, the lack of predictive value of the CIin our large group of patients with DPGN and in lupus patientswith glomerular lesions other than DPGN raises doubt regard-ing the clinical value of this measurement. We recommendholding in abeyance therapeutic decisions based upon the CIuntil its value is independently confirmed.
Acknowledgments
This work was supported by United States Public Health Serviceresearch award AM 27770. We thank Christine Spano for assistance inpreparing the manuscript.
Reprint requests to Melvin M. Schwartz, M.D., Department ofPathology, Rush-Presbyterian-St. Luke's Medical Center, 1653 W.Congress Parkway, Chicago, Illinois 60612, USA.
References
I. AUSTIN HA III, MUENZ LR, JOYCE KM, ANTONOVYCH T, KUL-LICK ME, KLIPPEL JH, DECKER JL, BALOW JE: Prognostic factorsin Lupus Nephritis. Contribution of renal histologic data. Am JMed 75:382—391, 1983
2. AUSTIN HA III, MUENZ LR, JOYCE KM, ANTONOVYCH T, BALOWJE: Diffuse proliferative lupus nephritis: Identification of specificpathologic features affecting renal outcome. Kidney liii 25:689—695,1984
3. MUEHRCKE RC, KARK RM, PI1NI CL, POLLAK VE: LupusNephritis. A clinical and pathologic study based on renal biopsies.Medicine 36: 1—146, 1957
4. POLLAK yE, PI1LANI CL, SCHWARTZ FD: The natural history of therenal manifestations of systemic lupus erythematosus. J Lab ClinMed 63:537—550, 1964
5. BALDWIN DS, LOWENSTEIN J, ROTHFIELD NF, GALLO U, MC-CLUSKEY RT: The clinical course of the proliferative and membra-nous forms of lupus nephritis. An mt Med 73:929—942, 1970

896 Schwartz et a!: Pathology of lupus glomerulonephritis
6. BALDWIN DS, GLUCK MC, LOWENSTEIN J, GALLO GR: Lupusnephritis. Clinical course as related to morphologic forms and theirtransitions. Am J Med 62:12—30, 1977
7. APPEL GB, SILVA FG, PIRANI CL, MELTZER JI, ESTES D: Renalinvolvement in systemic lupus erythematosus (SLE): A study of 56patients emphasizing histologic classification. Medicine (Baltimore)57:371—410, 1978
8. RUSH PJ, BAUMAL R, SHORE A, BALFE JW, SCHREIBER M:Correlation of renal histology with outcome in children with lupusnephritis. Kidney In! 29:1066—1071, 1986
9. MAGIL AB, PUTERMAN ML, BALLON HS, CHAN V, LIRENMANDS, RAE A, SUTTON RAL: Prognostic factors in diffuse prolifera-tive lupus glomerulonephritis. Kidney mt 34:511—517, 1988
10. CHURO J, SOBIN LH: Renal disease. Classification and Atlas ofGlomerular Disease. New York, Igaku-Shoin, 1982, pp. 127—149
Ii. SCHWARTZ MM, LAN S-P, THE Lueus NEPHRITIS COLLABORA-TIVE STUDY GROUP: Clinical outcome of 3 discrete glomerularlesions in severe lupus glomerulonephritis (LGN). Am J Kid Dis13:273—283, 1989
12. HEBERT L, NEILSON E, POHL M, LACHIN J, HUNSICKER L, LEWISEJ, THE LuPus NEPHRITIS COLLABORATIVE STUDY GROUP: Clin-ical course of severe lupus nephritis during the controlled clinicaltrial of plasmapheresis therapy. (abstract) Kidney In! 31:201, 1987
13. LEWIS EJ, LACHIN J, THE LuPus NEPHRITIS COLLABORATIVESTUDY GROUP: Primary outcomes in the controlled trial of plasma-pheresis therapy. (abstract) Kidney mt 31:208, 1987
14. TAN EM, COHEN AS, FRIES JF, MASt AT, MCSHANE DJ, ROTH-FIELD NF, SCHALLER JG, TALAL N, WINCHESTER RJ: The 1982revised criteria for the classification of systemic lupus erythemato-sus. Arthr Rheurn 25:1271—1277, 1982
15. SCHWARTZ MM, KAWALA KS, CORWIN HL, LEWIS EJ: Theprognosis of segmental glomerulonephritis in systemic lupuserythematosus. Kidney mt 32:274—279, 1987
16. FLEIS JL: Statistical Methods. New York, John Wiley and Sons,1981
17. SWETS JA, PICKETT RM, WHITEHEAD SF, GErrY DJ, SCHNUR JA,SWETS JB, FREEMAN BA: Assessment of diagnostic technologies.Advanced measurement methods are illustrated in a study ofcomputed tomography of the brain. Science 205:753—759, 1979
18. LANGLEY FA, BUCKLEY CH, TASKER M: The use of ROC curves inhistopathologic decision making. Anal Quant Cytol Histol 7:167—173, 1985
19. LEHMANN EL: Nonparametrics: Statistical Method Based onRanks. New York, Holden-Day, 1975
20. CAMERON JS, TURNER DR, Ooo CS, WILLIAMS DG, LESSOF MH,CHANTLER C, LEIBOWITZ S: Systemic lupus with nephritis: Along-term study. Q J Med 48:1—24, 1979
21. SissoNs HA: Agreement and disagreement between pathologists inhistological diagnosis. Postgrad Med J 51:685—689, 1975
22. SILCOCKS PBS: Measuring repeatability and validity of histologicaldiagnosis—A brief review with some practical examples. J ClinPathol 36:1269—1275, 1983
23. REID B, HAGGITT RC, RUBIN EE, ROTH G, SUROWICZ CM, VANBELLE G, LEWIN K, WEINSTEIN WM, ANTONIOLI DA, GOLDMANH, MACDONALD W, OWEN D: Observer variation in the diagnosisof dysplasia in Barrett's esophagus. Hum Pathol 19:166—178, 1988
24. LEWIS EJ, KAWALA K, SCHWARTZ MM: Histologic features thatcorrelate with the prognosis of patients with lupus nephritis. Am JKidney Dis 10:192—197, 1987
25. BALOW JE, AUSTIN HA III, MUENZ LR, JOYCE KM, AN-TONOVYCH TT, KLIPPEL JH, STEINBERG AD, PLATZ PH, DECKERJL: Effect of treatment on the evolution of renal abnormalities inlupus nephritis. N EnglJ Med 311:491—495, 1984
26. AUSTIN HA III, KLIPPEL JH, BALOW JE, LERICHE NGH, STEIN-BERG AD, PLATZ PH, DECKER JL: Therapy of lupus nephritis:Controlled trial of prednisone and cytotoxic drugs. N Engi J Med314:614—619, 1986