Embed Size (px)
Citation preview

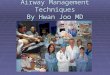
Prediction of difficult airway in school-aged patients with microtia (Uezono et al, Paediatr Anaesth 2001)
0
5
10
15
20
25
30
35
40
45
controls
unilateral microtia
bilateral microtia
difficult airway %
93 children scheduled for first-stage reconstruction of the auricleAge-matched controlled children
2%0%
42%

Stratégie d’épargne sanguine
• En fonction de la perte sanguine prévisible, discuter l’indication d’une autotransfusion et de l’administration d’EPO (chirurgie orthopédique)
• Commande de sang prévisionnelle et information du patient sur les risques

Allergie au latex: un problème de santé publique ?
groupes % risque d’allergie au latex
1980 1996
population générale 1 8
personnel de santé 3 20
profession dentaire 7 40
spina bifida 18 72

Prévention primaire
• Éviction de tout produit en latex (gants, sondes, tétines…)
• chez les nouveau-nés ayant un spina bifida
• chez les nouveau-nés qui vont être soumis à des chirurgies itératives (exstrophie vésicale, malformations uro-génitales…)

Quels examens complémentaires ?
• Aucune justification médico-légale d’un bilan systématique
• RMO : pas d’ECG, radio pulmonaire, ionogramme, fibrinémie chez l’enfant > 3 ans
• Importance de l’interrogatoire, de l’examen clinique, de l’existence d’un bilan antérieur
• Tout examen demandé doit être analysé !

Le dilemme du bilan d’hémostase
• Indispensable si ATCD hémorragiques personnels ou familiaux, chirurgie induisant des perturbations (CEC), chirurgie à risque hémorragique (amygdalectomie)….
• Un interrogatoire fiable est difficile chez les étrangers, et chez les jeunes enfants d’âge préscolaire

Des anomalies du bilan d’hémostase sont retrouvées dans 2% des cas…..
… mais la moitié des anomalies ne seront pas confirmées lors du contrôle
Burk et al 1992, Kang et al 1994
Il faut donc d’abord répéter les examens en cas d’anomalie, idéalement dans un délai d’une semaine

Allongement du TCA
• Anticoagulants circulants pas de risque hémorragique
• Déficit en facteur XII pas de risque hémorragique
• Maladie de Willebrand (1:100) discuter la desmopressine
• Hémophilie (1/10,000)

A la fin de la consultation
• Durée du jeûne préopératoire
• Choix de la prémédication ?
• Choix du mode d’hospitalisation

La durée du jeûne doit être limitée
• Autoriser les liquides clairs jusqu’à 2h avant l’anesthésie
• Autoriser le lait jusqu’à 4h chez les nourrissons < 6 mois
• Respecter un jeûne de 6h pour les solides au delà de 6 mois
• Intérêt : diminue l’inconfort lié à la soif, évite une déshydratation relative, facilite la tâche des parents

Recommandations pour réduire le risque d’inhalation (chirurgie réglée)
Apports durée minimale de jeûne (h)
Liquides clairs 2
Lait de femme 4Lait maternisé 6 (# des experts)
Lait d’autre origine 6
Repas léger 6
ASA Task force on preoperative fasting. Anesthesiology 1999;90:896

Présence des parents ou prémédication?
• Parents > contrôles non prémédiqués (Cameron 1996,Kain 1996)
• Mais des parents anxieux majorent les réactions négatives des enfants (Bevan 1990)
• Prémédication (midazolam PO 0.5 mg/kg) > présence des parents (Kain 1998) pour contrôler l’anxiété des enfants à l’induction

Parents vs prémédication
0
10
20
30
40
50
60
70
salle d'attente entrée salle op masque
prémédication
parents
contrôle
Yale preoperative Anxiety Scale
Kain et al. Anesthesiology 1998

Il faut prémédiquer les enfants…
• Diminution des scores de détresse à l’induction (Kain, Anesthesiology 1998)
• Diminution des troubles du comportement négatifs dans la 1ere semaine postopératoire versus contrôle chez des enfants d’âge moyen ~ 5ans (Kain, Anesthesiology 1999)

Effet de la prémédication (mdz 0.5 mg/kg PO) sur les troubles du comportement postopératoires après chirurgie ambulatoire
(Kain et al. Anesthesiology 1999;90:758-65)
0
10
20
30
40
50
60
70
80
90
J1 J2 J3 Semaine 1 Semaine 2
placebo
traités
%

Choix du mode d’hospitalisation
• Éviter le traumatisme de la séparation quel que soit le mode d’hospitalisation
« Mes parents viendront me voir tous les jours très longtemps : peut-être même, maman pourradormir avec moi. »

Les limites de l’ambulatoire
• Âge limite ? Non défini sauf prématurité
• Problèmes postopératoires attendus : douleur importante, risque de saignement, risque de vomissements ….
• Distance et/ou durée de transfert : à fixer avec l’équipe chirurgicale
• Conditions socio-économiques
• Le contrat peut toujours être réévalué….


Tait et al. Anesthesiology 2001
The URI dilemma

Risk factors for perioperative adverse respiratory events in children with upper
respiratory tract infections (Tait et al Anesthesiology 2001)
« children with active and recent URIs (within 4 weeks) are at increased risk for adverse respiratory events » ……
but ….« with careful management, most of these children can undergo elective procedures safely without increased morbidity »

La mortalité anesthésique des enfants ayant une cardiopathie congénitale opérés d’une chirurgie non cardiaque est augmentée par
rapport aux enfants sans cardiopathie (Baum VC et al. Pediatrics 2000;105:302)
OR (IC 95)
Mortalité globale (30 j) 3,5 (3,1-3,9)
Mortalité (1 j) 2,8 (2,4-3,4)
Effet de l’âge (30 j)< 31 j 2,2 (1,9-2,5)
31 j - 1 an 2,2 (1,6 – 3,1)
> 1 an 1,2 (0,9 – 1,6)

Cardiopathie congénitale (CC+) et chirurgie mineure
Chirurgie mortalité à 30 j/1000 AG
CC+ vs. CC-
Appendicectomie 22 2
Amygdalectomie 31 1
ATT 16 2
Hernie bilatérale 9 3
Hernie unilatérale 49 3