Embed Size (px)
Citation preview
Preconceptional Health Promotion in Low- Income Rural Communities: Randomized
Trial Results From The Central Pennsylvania Women’s Health Study
(CePAWHS)
Marianne M. Hillemeier, Carol S. Weisman, John J. Botti, Danielle Symons Downs, Mark Feinberg, Gary A. Chase,
Sara A. Baker, Anne-Marie Dyer, and Diana Velott
The Pennsylvania State University
To conduct a randomized trial of a new behavior change intervention – Strong Healthy Women – designed to improve the health and health behaviors of pre- and interconceptional women in low-income rural communities
Research Objectives
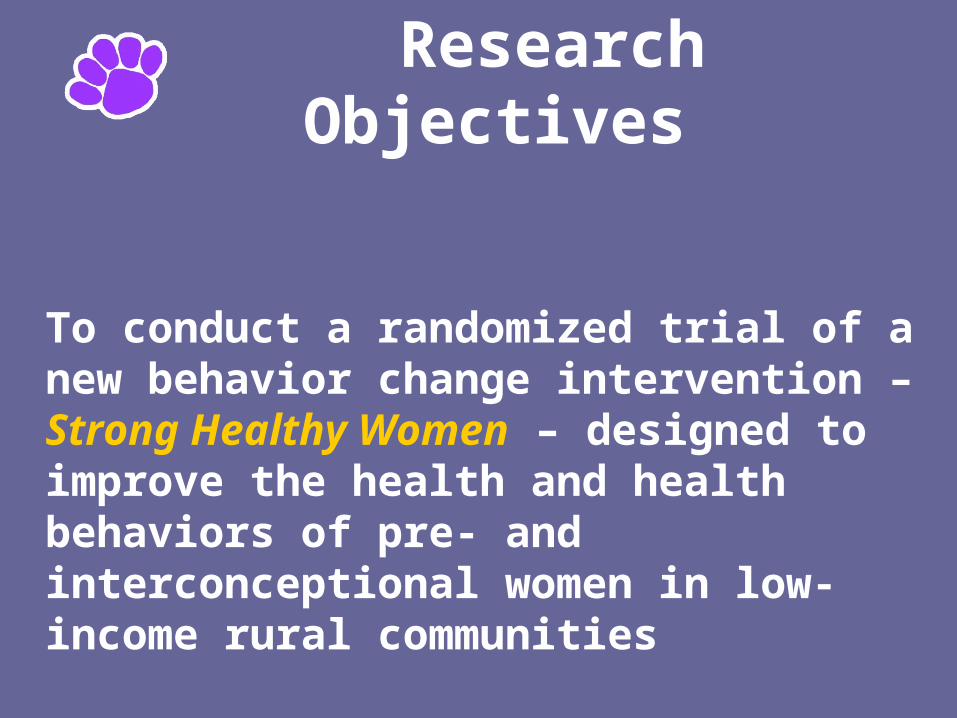
Prevalent Risk Factors in CePAWHS
Population-based Survey, Compared with PA and U.S.*(Women ages 18-45, weighted data)
CePAWHS PA U.S.
Obesity (BMI = 30+) 23% 18% 19%Depression/anxiety dx 29% -- 16%Nutritional deficits: Fruit < daily 68% 57% 60% Vegetables < daily 56% 31% 34%Alcohol use (ever) 48% -- 32%Binge drinking (among drinkers) 34% 29% 23%
Smoking 28% 32% 23%Folic acid supplementation 38% 53% 50%
* Comparison data sets include BRFSS 2003, Commonwealth Fund Survey of Women’s Health 1998, National Health Interview Survey 2003
Curriculumdeveloped by teamled by Drs.Mark Feinberg, Prevention ResearchCenterand Danielle Symons Downs,Department of Kinesiology,Pennsylvania StateUniversity
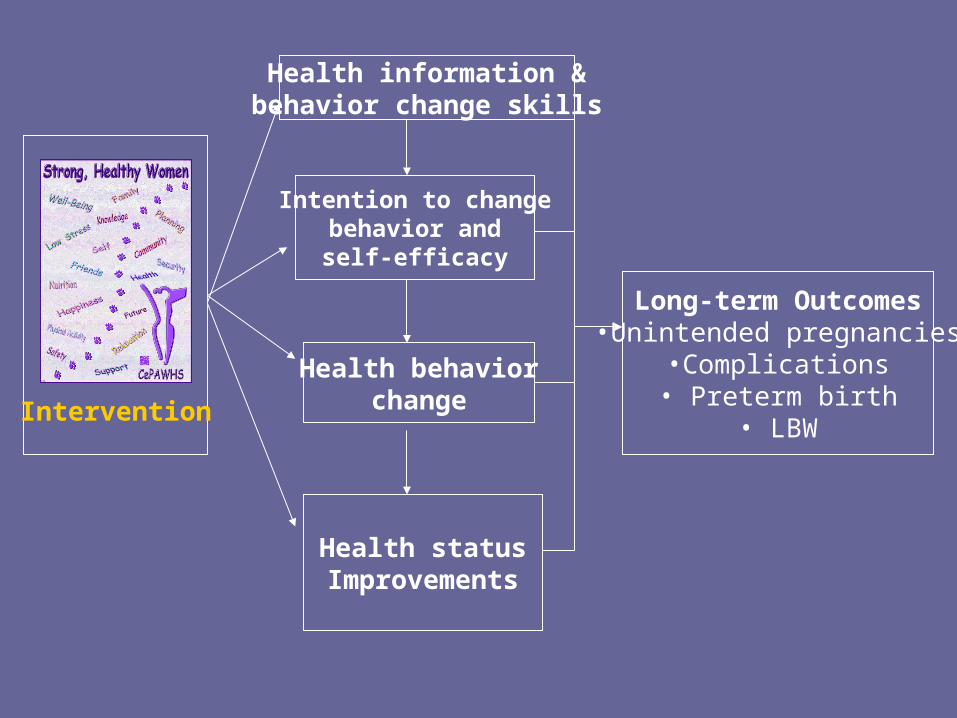
Intervention
Health information &behavior change skills
Intention to changebehavior andself-efficacy
Health behaviorchange
Health statusImprovements
Long-term Outcomes•Unintended pregnancies
•Complications• Preterm birth
• LBW
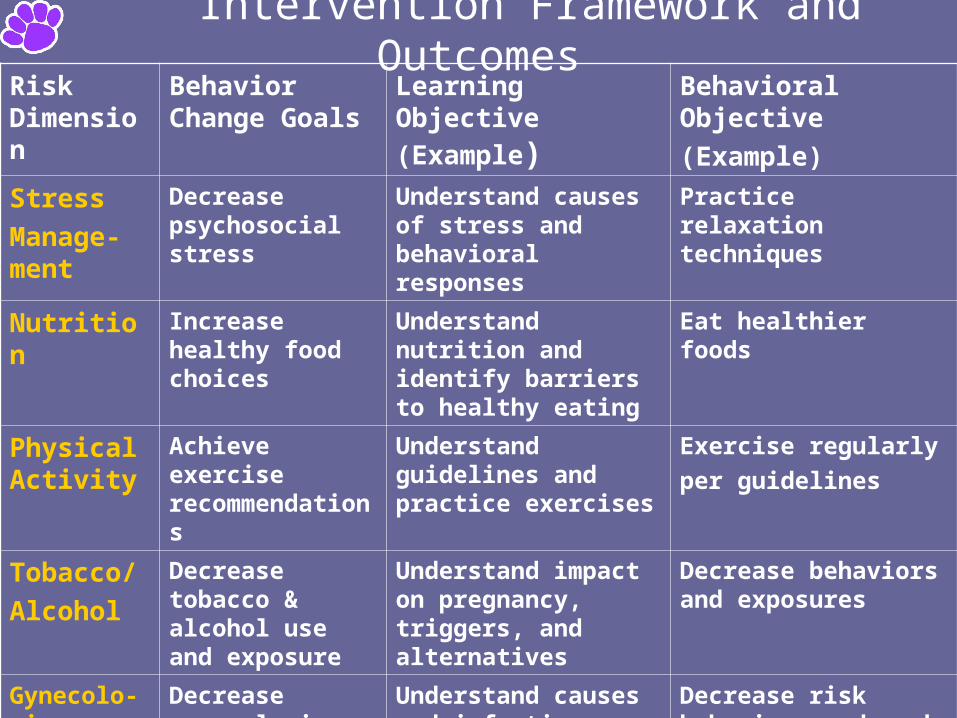
Intervention Framework and OutcomesRisk Dimension
Behavior Change Goals
Learning Objective
(Example)Behavioral Objective
(Example)
Stress
Manage-ment
Decrease psychosocial stress
Understand causes of stress and behavioral responses
Practice relaxation techniques
Nutrition Increase healthy food choices
Understand nutrition and identify barriers to healthy eating
Eat healthier foods
Physical Activity
Achieve exercise recommendations
Understand guidelines and practice exercises
Exercise regularly
per guidelines
Tobacco/
Alcohol
Decrease tobacco & alcohol use and exposure
Understand impact on pregnancy, triggers, and alternatives
Decrease behaviors and exposures
Gynecolo-gic
Infections
Decrease gynecologic infx
Understand causes and infection
Decrease risk behaviors and seek care
Pregnancy planning
Strategize for pregnancy planning
Understand maternal health and contraception
Discuss plan with provider; use folic acid
Intervention Process
• Six 2-hour sessions over 12-weeks
• Groups facilitated by 2 trained personnel
• Mix of topics at each session• Active learning (discussions, physical activity
sessions, cooking, handouts)
• Goal-setting (“baby steps”)
• Social support (buddy system;
facilitator phone calls)
• Incentives (gift cards, supplies)
A group using core balls
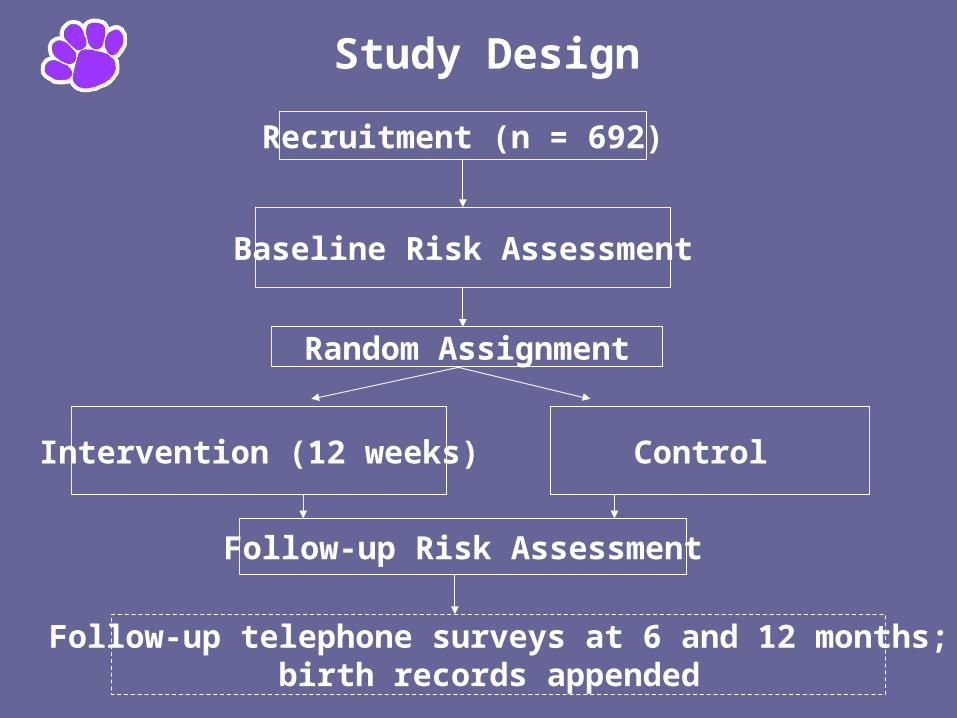
Study Design
Recruitment (n = 692)
Baseline Risk Assessment
Random Assignment
Intervention (12 weeks) Control
Follow-up Risk Assessment
Follow-up telephone surveys at 6 and 12 months;birth records appended
Risk Assessment Content (Behavioral and Biological Markers)
• Questionnaire (health status, health behaviors, psychosocial stress, access to health care, behavioral intent, self-efficacy, etc.)
• Anthropometric measurements (height, weight, BMI, waist circumference)
• Blood pressure
• Non-fasting blood glucose and lipid panel using fingerstick blood
and CardioChek analyzer
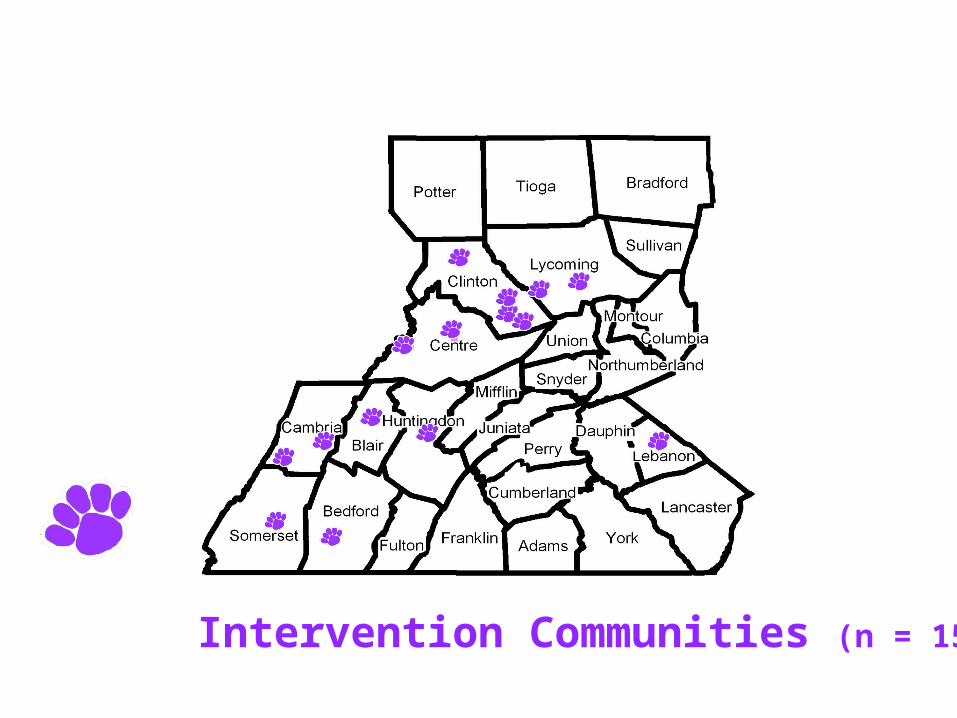
Intervention Communities (n = 15)
Eligibility
• Age 18-35 years at enrollment*• Resides in Central PA target area• Not pregnant at enrollment• Capable of becoming pregnant
(no hysterectomy or tubal ligation)• Exclusions: non-English speaking______________________* This age group accounts for > 85% of pregnancies in Central PA
Recruitment MethodsTailored to communities with help of local
Steering Committee members
Active • One-on-one recruitment at social service agencies
(e.g., WIC programs, childcare), schools, and retail settings
Passive• Presentations in social service agencies, schools• Posters and tear-off flyers in businesses, churches,
community centers• Kiosks at local health fairs, farm shows• Inserts in utility bills• Postcards to parents of subsidized child care
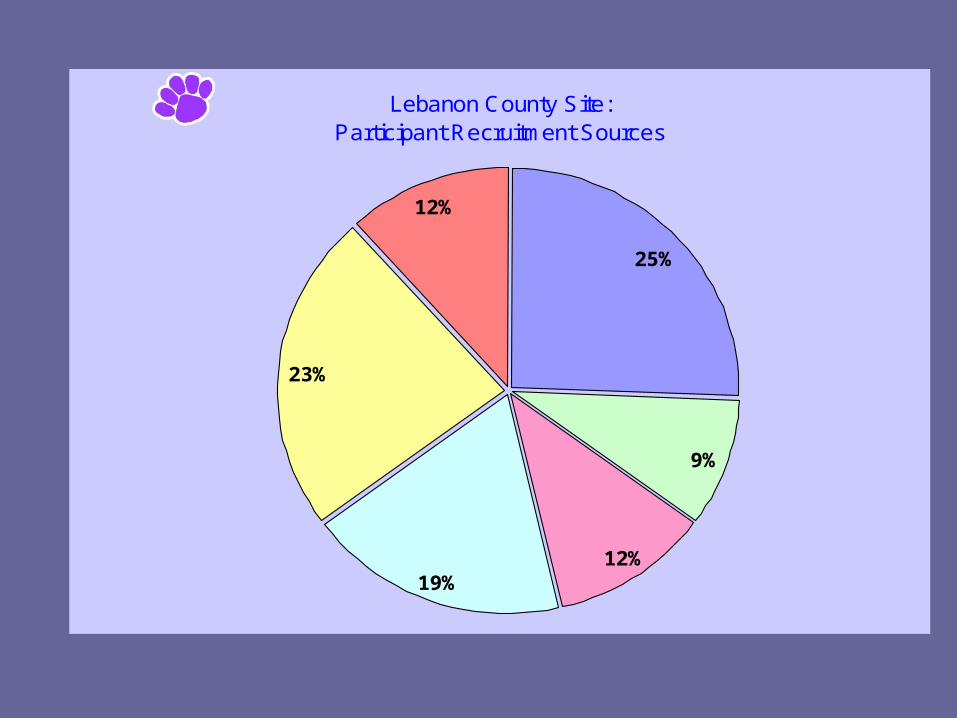
Lebanon County Site:Participant Recruitment Sources
25%
9%
12%19%
23%
12%
Utility bill Mailing Insert
Word of Mouth, Other
Social Service Agencies
Subsidized Child Care
Educational Institutions
Retail Establishments
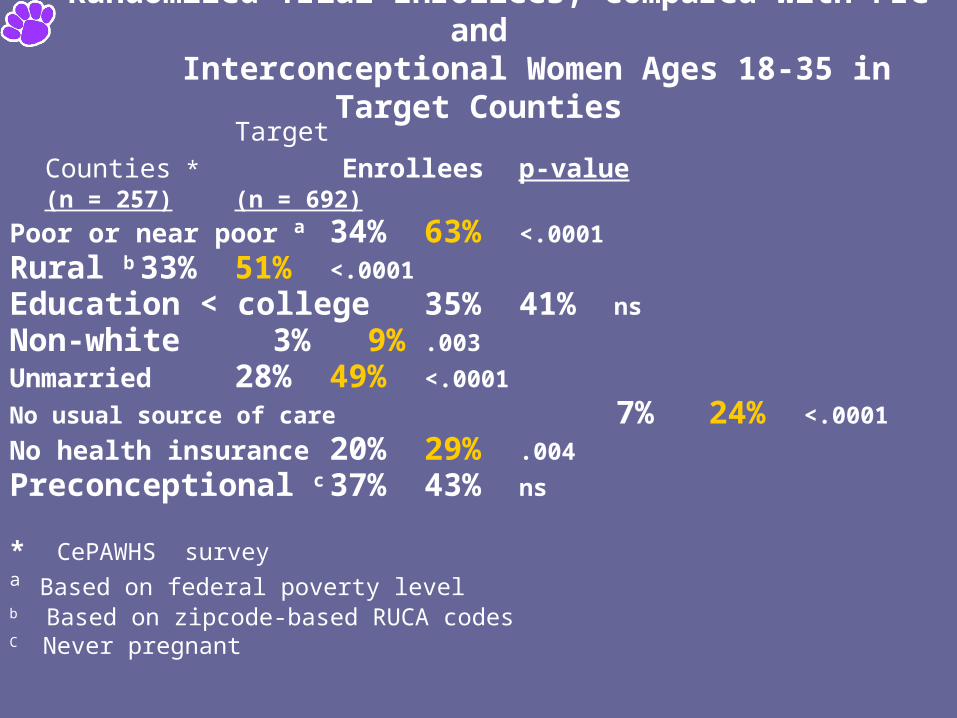
Randomized Trial Enrollees, Compared with Pre- and Interconceptional Women Ages 18-35 in Target Counties
Target
Counties * Enrollees p-value(n = 257) (n = 692)
Poor or near poor a 34% 63% <.0001
Rural b 33% 51% <.0001
Education < college 35% 41% ns
Non-white 3% 9% .003
Unmarried 28% 49% <.0001
No usual source of care 7% 24% <.0001
No health insurance 20% 29% .004
Preconceptional c 37% 43% ns
* CePAWHS surveya Based on federal poverty levelb Based on zipcode-based RUCA codesC Never pregnant
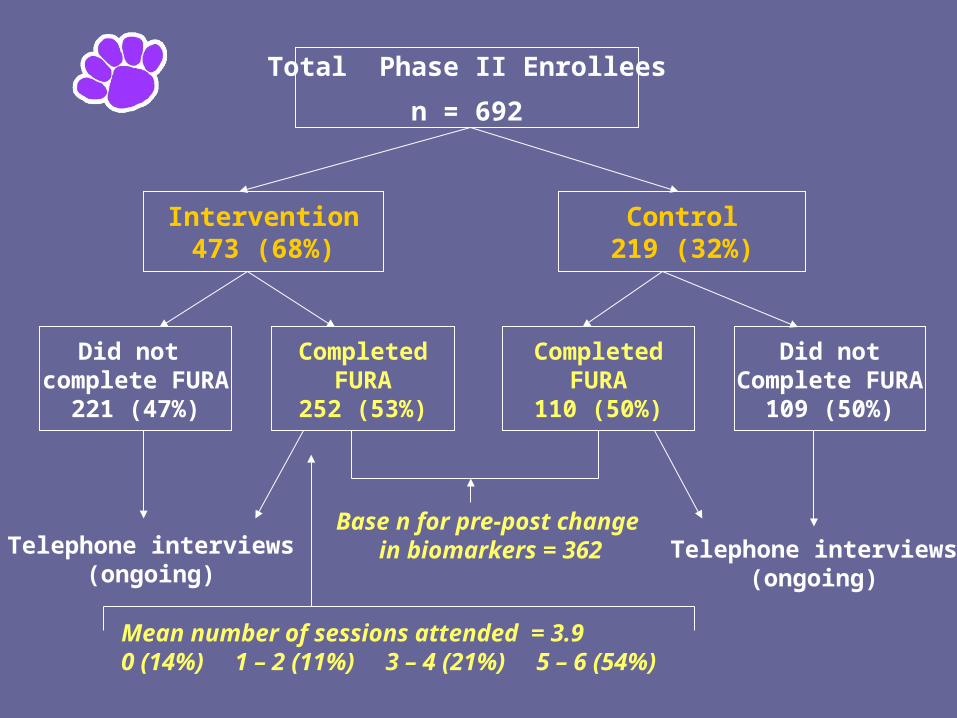
Total Phase II Enrollees
n = 692
Intervention473 (68%)
Control219 (32%)
Did not complete FURA
221 (47%)
CompletedFURA
252 (53%)
CompletedFURA
110 (50%)
Did notComplete FURA
109 (50%)
Base n for pre-post change in biomarkers = 362Telephone interviews
(ongoing)Telephone interviews
(ongoing)
Mean number of sessions attended = 3.90 (14%) 1 – 2 (11%) 3 – 4 (21%) 5 – 6 (54%)
Key Retention IssuesThose who dropped out of the study tended to be younger and to have lower educational levels than those who were retained.
Problem SolutionInadequate inter-session Improve trainingreminder contacts by and supervision ofgroup facilitators group facilitators; use
email and telephone contacts
Lack of reliable childcare Provide on-sitechildcare
Fidelity
Videotaped group sessions were rated for:
– Percent of content delivered in each domain (77% overall; worst for smoking reduction)– Group facilitator performance (e.g., engaging
and involved; confident; provides positive feedback to participants)
– Variation across sites (found only for facilitator performance)
Statistical Analyses
• Intent-to-treat pre-post analyses conducted with analysis of variance
• Baseline measure (pre-test) included as covariate to adjust for differences in baseline measures; follow-up (post-test) measure is the dependent variable
• Used GLM, ordinal logistic regression, or ordinary logistic regression (depending on dependent variable)
• Age and educational attainment controlled to account for potential confounding
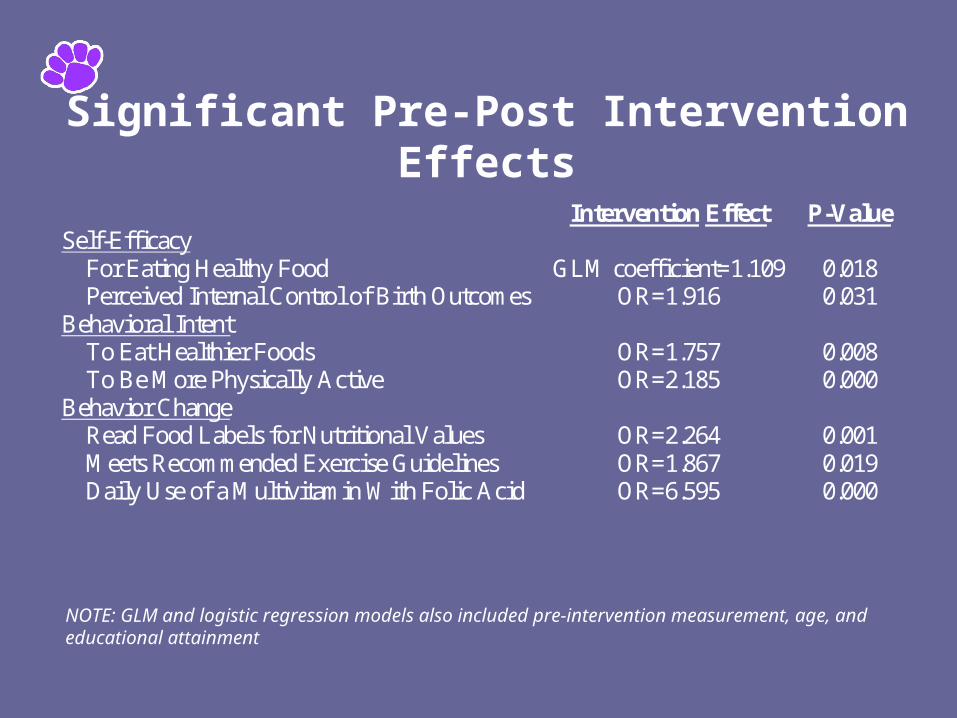
Significant Pre-Post Intervention Effects
Intervention Effect P-Value Self-Efficacy For Eating Healthy Food GLM coefficient=1.109 0.018 Perceived Internal Control of Birth Outcomes OR=1.916 0.031 Behavioral Intent To Eat Healthier Foods OR=1.757 0.008 To Be More Physically Active OR=2.185 0.000 Behavior Change Read Food Labels for Nutritional Values OR=2.264 0.001 Meets Recommended Exercise Guidelines OR=1.867 0.019 Daily Use of a Multivitamin With Folic Acid OR=6.595 0.000
NOTE: GLM and logistic regression models also included pre-intervention measurement, age, and educational attainment
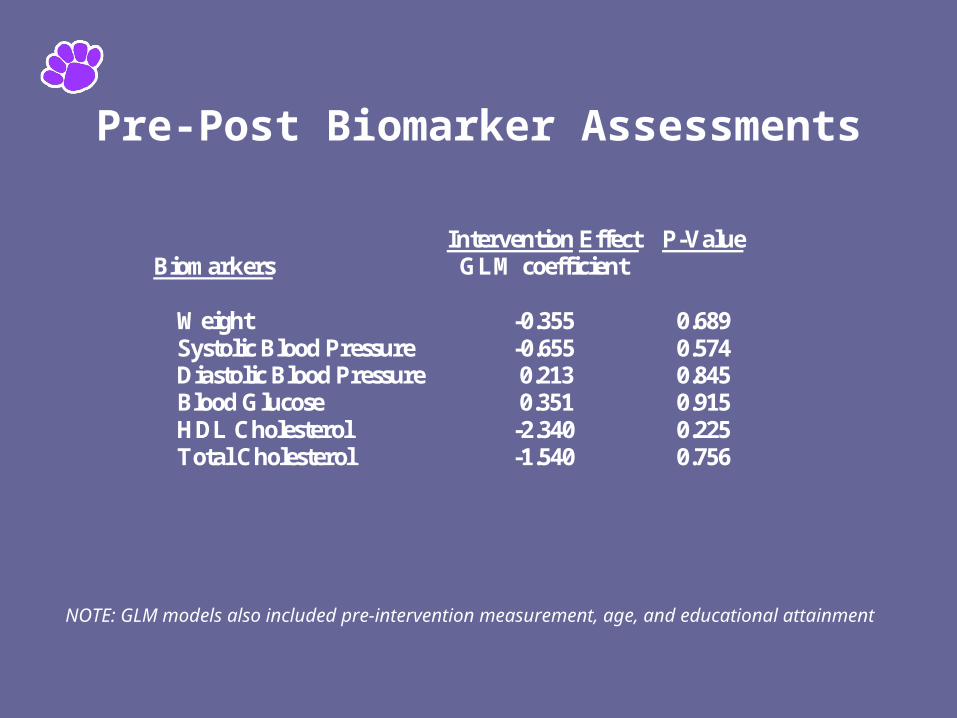
Pre-Post Biomarker Assessments
Intervention Effect P-Value Biomarkers GLM coefficient Weight -0.355 0.689 Systolic Blood Pressure -0.655 0.574 Diastolic Blood Pressure 0.213 0.845 Blood Glucose 0.351 0.915 HDL Cholesterol -2.340 0.225 Total Cholesterol -1.540 0.756
NOTE: GLM models also included pre-intervention measurement, age, and educational attainment
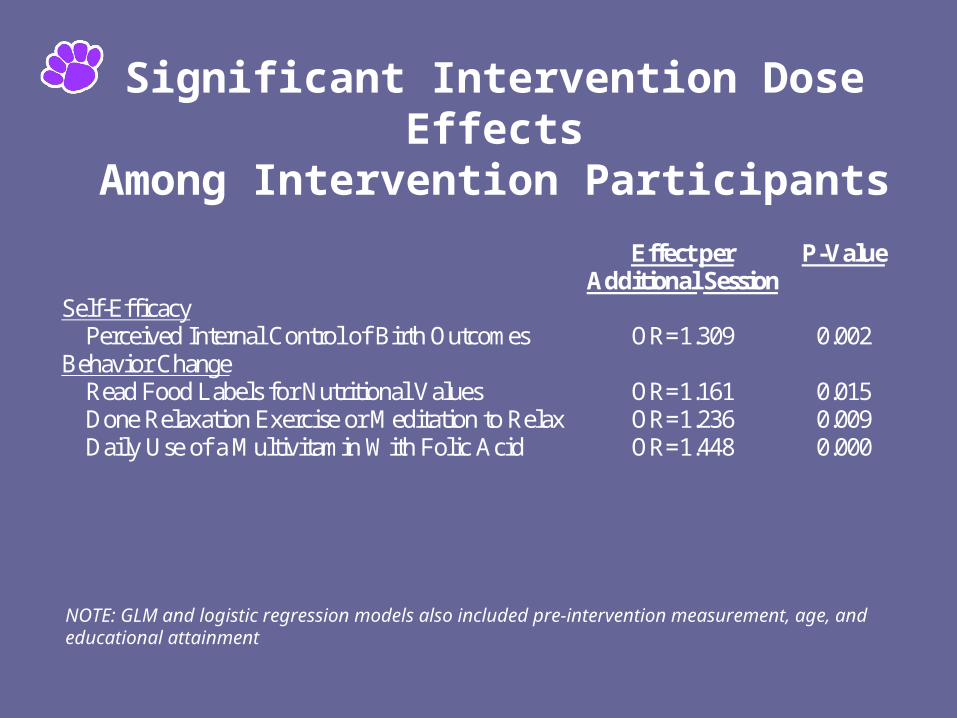
Significant Intervention Dose EffectsAmong Intervention Participants
Effect per Additional Session
P-Value
Self-Efficacy Perceived Internal Control of Birth Outcomes OR=1.309 0.002 Behavior Change Read Food Labels for Nutritional Values OR=1.161 0.015 Done Relaxation Exercise or Meditation to Relax OR=1.236 0.009 Daily Use of a Multivitamin With Folic Acid OR=1.448 0.000
NOTE: GLM and logistic regression models also included pre-intervention measurement, age, and educational attainment
Next Steps in Analyses
• Moderation effects (e.g., Did the intervention work better for certain subgroups of women? Did degree of fidelity affect impact?)
• Maintenance of attitudinal and behavior change over the 12-month follow-up period
• Any impact on pregnancy complications or outcomes during follow-up period (~ 115 live births occurred)
Future Research Plans
• Modify the Strong Healthy Women intervention based on Phase II data
• Test the modified intervention in a randomized trial of alternative modes of delivery in a more diverse target population
Acknowledgements
• Funded, in part, by a grant from the Pennsylvania Department of Health
• Collaborating organizations:Pennsylvania State UniversityFamily Health Council of Central PennsylvaniaFranklin & Marshall CollegeLock Haven University of Pennsylvania
• Steering Committee of community representatives