Embed Size (px)
Citation preview

17/11/2017
1
Therapy-Related Toxicities:
Unique Challenges and the Importance of Communication
Communication on Toxicity Management: How Do We Get the Message Across
Karis Cheng
National University of Singapore
Disclosure
Nothing to disclose
How Do We Get the Message Across Meaningfully
…who are hearing our messages …who are hearing our messages
Make sense in contextMake sense in context
Demographic Values and perspectives
Relevancy and meaningRelevancy and meaning
Two-third patients
indicate ‘maintaining my
QoL is more important to me than living longer’
Two-third patients
indicate ‘maintaining my
QoL is more important to me than living longer’
Dr. SIOG
Optimal Optimal dose
My
QoL
My
QoL
Your clinical benefits
…survival
Acute/ late/
chronic toxicity
Acute/ late/
chronic toxicity
Supportive care
Supportive care
GA -
Risk
GA -
Risk
Mohile S. 2017Mohile S. 2017
Key finding: Older patients want chemotherapy as long as side effects do not reduce quality of life or ability to function independently
Overarching questions
Does it mean that QoL would be a determinant and have a
role to play in cancer treatment decision making?
Why toxicity and supportive care matter?
Effective communication – what is the bottom line?

17/11/2017
2
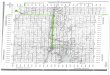
Cheng, Lim & Kanesvaran. Quality of life of elderly patients with solid tumours undergoing adjuvant cancer therapy: a systematic review (in 2nd review)
• To summarise the evidence of QoL during and after adjuvant therapy in elderly cancer patients
• A systematic search in CINAHL plus, CENTRAL, PubMed, PsycINFO and Web of Science from the inception of these
databases to December 2016 (43,433 of
records)
• 4 RCTs (low or unclear RoB for most items) and 14 non-RCTs (low or moderate ROB for all domains – 5 studies; had a serious risk of bias in at least one domain –9 studies) on 1,633 participants
• The geriatric domains of functional status and/or co-morbidities at
baseline were examined and reported in 14 studies
• 12 out of 18 studies measured toxicity during adjuvant therapy
– Hematological toxicity• 2 studies reported grade 3 or 4 toxicity in <10% of participants, 5 reported in ≥25% of
participants
– Non-hematological toxicity• 1 study reported grade 3 or 4 toxicity in <10% of participants, 4 reported in ≥25% of participants
Breast
AdjuvantBaseline global or overall QoL
scores (score range)
From baseline to the middle of
adjuvant
From baseline to the time of completion of
adjuvant
From baseline to post adjuvant follow up
period (1-24 months) Toxicity reported
RCTs
Kornblith 2011
n=48
CMF or FEC75.4 (0-100)
Capecitabine76.5 (0-100)
↓NS
↓NS
↓NS
↓NS
↑NS
↑NS
Participants treated with capecitabine has sign fewer
toxicity
Perrone 2015n=252
CMF
Docetaxel(mean was not reported)
↓NS
↓NS
Grade 2 hemato 70% of participants with CMF, 9% with
docetaxel; non-hemato 19% with CMF, 28% with docetaxcel
Crivellari2000
n=58
Tamoxifen aloneTamoxifen & CMF
Median 59 (0-100)↑NS ↑NS
Grade 3 hemato 9.2%, non-hemato 6.6%
Non-RCTs
Arraras 2008n=48
RT59.6 (0-100)
↓NS ↑*(p<0.05; ES 0.52)
Level 2 non-hemato 2.1% to 8.4%
Browall 2008n=39
FEC or CMF76 (0-100)
↓*(p<0.05; ES 0.74)
↓*(p<0.05; ES 0.71)
↓NS
(an improving trend)
NR
Dees 2000n=11
AC7.65 (0-10)
↓NS No cl sign age related trends in toxicity
Hurria 2006n=49
CMF or AC or ACT or ACT-H116 (0-148)
0 ↑NS Grade 3 or 4 hemato 27%, non-hemato 31%
Watters 2003n=16
FEC78 (0-100)
↓NS ↓*(p<0.05; ES 0.66)
↓NS
(an improving trend)
NR
Glioblastoma
Adjuvant
Baseline global or overall QoL scores (score range)
From baseline to
the middle of adjuvant
From baseline to the
time of completion of adjuvant
From baseline to post
adjuvant follow up period (1-24 months) Toxicity reported
RCTs
Keime-Guibert
2007n=35
Supportive care & RT
62.9 (0-100)
↓NS ↓NS
(an improving trend)
No adverse effects related to
RT
Non-RCTs
Gallego 2011
n=59
Temozolomide
mean was not reported
↑*(narrative)
Grade 3-4 hemato 25%
Minniti 2009
n=36
RT & Temozolomide
58.3 (0-100)
↓NS Grade 2-3 confusion during/
after RT 14%; grade 3-4 hemato during CT 28%, non-
hemato 9-35%
Minniti 2013
n=65
RT & Temozolomide
61.5 (0-100)
↑* NR
Adjuvant
Baseline global or overall QoL scores (score range)
From baseline to
the middle of adjuvant
From baseline to the
time of completion of adjuvant
From baseline to post
adjuvant follow up period (1-24 months) Toxicity reported
Mixed
Mohile 2011
n=368
RT
2.07 (0-10)
↑NS NR
Prostate
Arraras 2008
n=137
RT
66.8 (0-100)
0 ↑*
(p<0.05; ES 0.25)
NR
Colon
Bouvier 2008
n=11
Flurouracil or Oxaliplatin
& Flurouracil or Capecitabine
60 (0-100)
↑NS ↑NS NR
Chang 2012
n=57
Capecitabine
59 (0-100)
↓NS ↑NS Grade 3 or 4 hemato <1%
Cervical
Caffo 2003 RT
2.11 (1-4)
↑NS ↑NS NR
Lung
Park 2013
n=66
Cisplatin or Carboplatin &
Paclitaxel53 (0-100)
↓NS ↓NS Grade 3 or 4 hemato 1.5-39.4%
• Heterogeneity and RoBs, caution is warranted in the interpretation of the results.
• A negative change in QoL was short-lived during adjuvant CT for some elderly patients with breast cancer.
• Adjuvant CT/ RT may not have detrimental effects on QoL in most elderly patients with solid tumours
• No pattern of the relationship between treatment toxicity and QoL score
– stable or improved QoL is unlikely to be attributable to relatively low treatment toxicity
• Possible explanation and impact on our treatment/ care
– Positive perception of the adjuvant therapy and may adjust better to the treatment
– Response shift phenomenon
– Poor sensitivity of the generic QoL measures
– Selection bias – under-representation of less healthy older patients and those with limited expectations of treatment benefits

17/11/2017
3
• QoL could be a language to communicate with patients/ families regarding the toxicity
• Help older adults patients better understand the impact of adjuvant therapy on their QoL, and could help make better treatment decisions
QoL is considered a useful outcome
measure to enhance patient-clinician communication and patient compliance in elderly patients with breast cancer during cancer treatment (Reimer & Gerber 2010)
• Supportive care is integral to anti-cancer treatment regardless of age or treatment intent
• Older adults with cancer benefit from GA-guided supportive care interventions
• Treatment-related issues of particular importance in older adults
include hemato toxicity, nausea/vomiting, and neurotoxicity
A qualitative study to understand elderly cancer patients’ perception and experiences in toxicity and supportive care
• 8 participants with stage 0 to III
breast cancer and aged ≥65
years
• Content analysis
• Themes (insights)
– Positive emotions
– Trust in oncologist
– Sense of fear
– Information need for diet and daily
living
– Financial toxicity
• Clinical toxicity
• Symptomatic adverse effects
(AEs)
• NCI-CTCAE
– 124 individual items represent the 78 symptomatic AEs in the PRO-CTCAE item library
– English, Spanish, Danish, Chinese…versions
Effective patient-clinician communication –what is the bottom line?
• Patient-centred communication
– Respect and respond to patients’ preferences, needs and values
– Shared understanding and shared power
– Rapport among older adult patients, families and HC professionals
– Understandable, comprehensible and retentable information
• Elderly might have little in their educational background to help them understand their treatment
and toxicity
– Cross-cultural differences
• Tools for the assessment of communication in clinical practice and clinical trials
• Guidelines for communication
Tools to evaluate communication in cancer settings
• Patient Assessment of Cancer Communication Experiences (Mazor et al 2016)
• EORTC-COMU 26 (communication-specific) module (Arraras et al 2014; Arraras et al
2017)
– Evaluate the different domains of communication between patients and HC professionals
Treatment Decision Making Item Set
I got clear, understandable information about treatments we were considering.
I understood the risks of my different treatment choices.
I was encouraged to give my opinion about what treatment choices I would prefer.
Scale
1.Patient’s active role behaviors 4.Professional’s skills
2.Aspects of the clinician-patient relationship 5.Professional’s management of patient’s emotions
3.Professional’s qualities creating a relationship 6.Professional’s skills related to information

17/11/2017
4
Evidence/ consensus
- based guidelines on
communication
Evidence/ consensus
- based guidelines on
communication
Key recommendation
• Discussing treatment options and clinical trials
– Clarify the goals of treatment so that the patient understands likely outcomes
– Provide information about the potential benefits and burdens of any treatment and check the patient’s understanding of these benefits and burdens
– Discuss treatment options in a way that preserves patient hope, promotes autonomy and facilitate understanding
– Make patients aware of all treatment options including clinical trials; start with standard treatments available, then move to a discussion of applicable clinical trials if the patient is interested
A milestone moment to take action
Embracing best practice in communication on toxicity management/
treatment decision making and bringing older cancer patients’
perspectives and concerns to the forefront

























![[Kornblith Hilary] the Laws of Thought(BookFi.org)](https://img.pdfslide.us/doc/110x75/563db780550346aa9a8ba332/kornblith-hilary-the-laws-of-thoughtbookfiorg.jpg)

