Embed Size (px)
DESCRIPTION
PRE-TERM LABOR. Insert Presenter’s Name. Dr Uma.T Department of Obstetrics and Gynecology SAT Hospital,Government Medical College Trivandrum. PRETERM LABOUR. Def : Regular painful uterine contractions after 20 wks and before 37 wks Associated with effacement and dilatation of cervix - PowerPoint PPT Presentation
Citation preview

Insert Presenter’s NameDr Uma.TDepartment of Obstetrics and Gynecology SAT Hospital,Government Medical College Trivandrum

Def : Regular painful uterine contractions after 20 wks and before 37 wks
Associated with effacement and dilatation of cervix
Incidence – 20 – 30%Impact – Regarding chance of survival
of preterm neonate- Quality of life achieved.

AETIOLOGYMaternal CharacteristicsAge – Low & HighSocioeconomic status– PoorPhysical Activity Maternal habits & – Cigarette,
addictions Alcohol, Cocaine
Psychological Stress

MATERNAL SYSTEMIC DISEASESRenal Diseases – Acute infection
& asymptomatic bacteruria
Hypertensive disordersMaternal diabetes – HydramniosImmunological
disorder – SLE, APLA syndrome

MATERNAL INFECTIONS
Febrile illnesses – MalariaInfective diseases – Syphilis,
toxoplasmosisChorioamnionitisBacterial vaginosis - PPROM

UTERINE FACTORSUterine MalformationsCervical incompetencePrevious history of abortion &
Preterm birthsPREGNANCY COMPLICATIONSMultiple pregnancyHydramniosPlacenta Praevia or abruptionGENETIC FACTORS

PATHOGENESISExact mechansim not knownFetus plays synergestic role ↑ PG synthesis – stimulated by
intrauterine infection, haemorrhage, overdistension etc.
From decidua & fetal membranes ↑ Cytokines, IL – 6, IL - 1, TNF, PAF
– produced by fetal lungs, kidney

PREDICTION OF PRETERM LABOUR1. Measuring cervical length using TVS
– At 24 wks – Mean cervical length is
35 mm . Shortened cervix had ↑ rate of
preterm labour Requires special expertise2. History of preterm birth3. Fetal fibronectin – in cervicovaginal
secretions4. Ambulatory uterine contraction
testing 5. Maternal Salivary estriol – not used

DIAGNOSISContractions at a frequency of 4 in
20 mts. or 8 in 60 mts.Cervical dilatation more than 1 cm.Cervical effacement of 80% or
greater.

MANAGEMENTDepends on gestational age and neonatal
care facilitiesGestational age between 24 and 34 wks –
administer corticosteroids2 doses of 12 mg betamethasone given
intramuscularly 24 hour apart.If delivery occurs 24 hrs after completion
of betamethasone and within 7 days, chance of respiratory distress less.

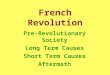
MECHANISM OF ACTIONInduces proteins that regulate
biochemical systems in type 2 cells.Increases alveolar surfactant,
compliance and lung volume.Adverse effects – Short termMaternal – Pulmonary edema,
infections, poor diabetic controlFetal – Nil.

Epithelial cell
Structural Developme
nt
Type II
PneumocytesApoprotei
ns
Steroids
Steroids
surfactant

Repeated Doses of Steroids?Not recommended
Adverse effects
1.Chorioamnionitis.2.Cause early onset neonatal sepsis.3.NND.4.Low birth weight.5.Abnormal psychomotor development.

Tocolysis in preterm labourDoes tocolysis prevent preterm labour?No clear evidence improve outcome; only to
complete course of corticosteroids or inuterotransfer
(Evidence A)
Does tocolysis prevent NND and morbidity ?No clear reduction (Evidence
A)

INDICATION FOR TOCOLYSISGestational age less than 37 wks Cervical dilatation less than 3 cmNo history of unclean examination
or evidence of chorio amnionitis.No pregnancy complication like
APH, PE Fetus normal, alive, no signs of
distress.

COMMONLY USED…
16

17

TOCOLYTICSBetadrenergic drugsIsoxuprine, Riltodrine, salbutamol,
terbutalineInhibit uterine contraction by
stimulating myometrial β-2 receptors.Adverse effects due to stimulation of
receptors elsewhere.Maternal hypotension, Tachycardia,
palpitation, fetal Tachycardia.

MAGNESIUM SULPHATEHigh concentration decreases contractilityNot used for this purpose.
PROSTAGLANDIN INHIBITORSAspirin, IndomethacinUse avoided – Premature closure of neonatal
ductus arteriosus and neonatal pulmonary hypertension

CALCIUM CHANNEL BLOCKERSAll smooth muscle activity related to
free calcium in cytoplasmReduction in Calcium inhibits
uterine contraction.Nifedipine – Efficacy not been
adequately studied.

Pre-term Labor in Women with a Past History of PTL
Am J Obstet Gynecol. 1998;178(5):1035–1040.
Fetal fibronectin positive women with a prior history of preterm birth
Estimated recurrence riskof preterm birth <35 weeks’
gestation
Cervical Length ≤25 mm 65%
Cervical Length 26 to 35 mm 45%
Cervical Length > 35 mm 25%Fetal fibronectin negative women with a prior history of preterm birth
Estimated recurrence riskof preterm birth <35 weeks’
gestation
Cervical Length ≤25 mm 25%
Cervical Length 26 to 35 mm 14%
Cervical Length > 35 mm 07%
21

Oral Micronized Progesterone Improves Maternal and Fetal Outcomes in Women with a History of PTL
Oral micronized progesterone was associated with
Improved birth weight (2400 g vs. 1890 g, p<0.001)
Lower stay in the neonatal ICU (p<0.001)
More favorable Apgar scores (p<0.001)
J Obstet Gynaecol. 2009;29(6):493–498.Int J Gynaecol Obstet. 2009;104(1):40–43.22
22
Reference and study type
Intervention (N)
Mean GA SD
(weeks)
PTB<37 weeks
(%)
PTB≤36 weeks
(%)
PTB≤34 weeks
(%)
PTB≤33 weeks
(%)
PTB≤28 weeks
(%)
Majhi et al.2 (2009), RCT
Vaginal (50)
NR 12.0* NR 4.0 NR NR
None (50) NR 38.0 NR 6.0 NR NR
Rai et al.2 (2009), RCT
Oral (74)36.12.
6*39.2* NR 27.0 2.7* 0
Placebo (74)
34.03.25
59.5 NR 25.7 20.3 4.0
NR=Not reported. *Statistically significant.

Pre-term Labor and Uterine Abnormalities
Women with uterine anomalies have poorer reproductive
outcomes when compared to that of the general population.
Unicornuate uterus is associated with the poorest fetal
survival.
The incidence of preterm deliveries among women with
bicornuate uterus and didelphic uterus has been reported in
as high as one-fourth of the pregnancies
J Womens Health (Larchmt). 2004;13(1):33–39.
Number of pregnancies (n)
Preterm deliveries (n)
Unicornuate uterus
393 43.3% (170)
Didelphic uterus 86 24.4% (21)
Bicornuate uterus
56 25.0% (14)
23

Vaginal Micronized Progesterone for Prophylaxis of PTL
– Results from Cetingoz et al.
Arch Gynecol Obstet 2011;283:423–429.
Vaginal progesterone (100 mg) administered between 24 and 34 weeks has the following outcomes in women with
prior pre-term birth, twin pregnancy and uterine malformations
24
Placebo (%) Progesterone (%)
Total population
Delivery <37 weeks 40/70 (57.2) 32 of 80 (40)
Delivery <34 weeks 17/70 (24.3) 7 of 80 (8.8)
Preterm labor admission 32/70 (45.7) 20 of 80 (25)
History of PTB
Delivery <37 weeks 17/34 (50) 9 of 37 (24.3)
Delivery <34 weeks 9/34 (26.5) 2 of 37 (5.4)
Preterm labor admission 19/34 (55.9) 11 of 37 (29.7)

Pre-term Labor and Cervical Length – Results from Iams et al.
Even a small decrease in cervical length between the 24th
and 28th weeks of gestation was associated with an
increased risk of preterm birth (relative risk, 2.03; 95% CI,
1.28–3.22)
N Engl J Med. 1996;334(9):567–572.
Measures (at 24 weeks) Relative risk
Cervical length ≤ 25th percentile (30 mm) as compared to > 75th percentile
3.79 (95% CI, 2.32–6.19)
Cervical length ≤ 10th percentile (26 mm) as compared to > 75th percentile
6.19 (95% CI, 3.84–9.97)7
25

Progesterone Preserves Cervical Length – Results from O’Brien et al.
Ultrasound Obstet Gynecol 2009;34:653–659.
Intravaginal progesterone preserves cervical length
26

NEONATAL CARE
Preterm infants require neonatal intensive care.
If facilities not available, give corticosteroids and refer patient to appropriate higher centre
INTRAPARTUM MANAGEMENT
Proper fetal heart rate monitoringDelivery – RMLE put If poor voluntary efforts in second stage –
Outlet forceps.