Embed Size (px)
Citation preview

www.wjpps.com │ Vol 10, Issue 2, 2020. │ ISO 9001:2015 Certified Journal │
232
Hawraa et al. World Journal of Pharmacy and Pharmaceutical Sciences
PRE-ECLAMPSIA, PATHOPHYSIOLOGY AND MANAGEMENT
*Dr. Hawraa Saadi Ismael Albuslman and Dr. Israa Abdulameer Kadhim
1,2
M.B.Ch.B, DGO.
INTRODUCTION
Pathophysiological Foundations
Some evidence supports the hypothesis of maternal immune system
involvement in the disease. In case there are problems of
immunological adaptation to the trophoblast, there will be problems in
trophoblast perfusion, with consequent hypoxia. These primary
alterations would trigger a series of local hypoxia phenomena, and
reoxygenation could amplify the local effects, such as the formation of
oxygen-reactive species, activation of the maternal inflammatory
system, and acceleration of cellular apoptosis processes that would limit the establishment of
normal placentation and imbalance between pro-angiogenic factors, such as the vascular
endothelial growth factor (VEGF) and the placental growth factor (PlGF), and soluble
antiangiogenic factors such as the soluble fms-like tyrosine kinase-1 (sFLT-1), with
predominance of the latter, resulting in generalized activation of the maternal inflammatory
system, universal endothelial dysfunction, and limited placental vascularization. Universal
arteriolar spasm due to endothelial activation results in an insidious and progressive process,
culminating in multiple organ insufficiency. Preeclampsia should be interpreted as a chronic
disease with potential for progressive multiple organ failure. This evolutionary character must
be taken into account, as well as its unpredictability and clinical instability in decisions.
Endothelial activation basically determines: vasoconstriction and consequent increase in
peripheral resistance; changes in capillary permeability, which are responsible for edema; and
activation of the coagulation system. The kidneys suffer from anatomo pathological patterns
(glomerular endotheliosis and focal sclerosis), with consequent proteinuria and impairment of
the glomerular filtration. In the liver, ischemia occurs with varying intensity, leading to
dysfunction with elevated levels of transaminases. Focal or confluent edema and/or
hemorrhage distend the capsule, and may result in hepatic rupture with massive bleeding.
Vasospasm hinders the uteroplacental blood flow with varying intensity, depending on the
WORLD JOURNAL OF PHARMACY AND PHARMACEUTICAL SCIENCES
SJIF Impact Factor 7.632
Volume 10, Issue 2, 232-251 Research Article ISSN 2278 – 4357
*Corresponding Author
Dr. Hawraa Saadi Ismael
Albuslman
M.B.Ch.B, DGO.
Article Received on
10 Dec. 2020,
Revised on 30 Dec 2020,
Accepted on 19 Jan. 2021
DOI: https://doi.org/10.17605/OSF.IO/8ZW75
www.wjpps.com │ Vol 10, Issue 2, 2020. │ ISO 9001:2015 Certified Journal │
233
Hawraa et al. World Journal of Pharmacy and Pharmaceutical Sciences
moment of the process and on the existence of a chronic pre-existing injury. Regarding
coagulation, there is activation and consumption of platelets with progressive consumption
and disseminated coagulation. The brain can be affected by ischemia aggravated by diffuse
edema, resulting in seizure (eclampsia) or stroke. Patients presenting severe conditions,
particularly eclampsia, should receive differentiated care, given the progressive functional
limitation of multiple organs.
METHOD
This systematic review was conducted following the Preferred Reporting Items for
Systematic Reviews and Meta-analysis (PRISMA) guidelines. A search of peer-reviewed
literature was originally undertaken during 23 January and 31 March 2019, using the
following search criteria for study selection exp Education, Continuing/’ OR ‘Inservice
Training/’ OR ‘insertion training.mp.’ ‘training�.mp.’) AND (‘clinician�.mp.’ OR
‘physician�.mp.’ OR ‘Family Nurse Practitioners/’ OR ‘nurse�.mp.’ OR ‘exp General
Practitioners/’ OR ‘Gynaecologist.mp.’ OR ‘Obstetrician. mp.’ OR ‘exp Physicians/’ OR
‘exp Medical Staff/’) All articles identified in the search were screened by the first author
(MO) based on title and abstract for potential inclusion. Authors 1 (MO) and 2 (KP) then
independently screened the full-text articles to determine their eligibility for inclusion.
Disagreements were resolved by discussion or with a third review (KM). Inclusion criteria
were 1) evaluated the PREECLAMCIA training or clinical education programs for health
care providers permitted to insert PREECLAMCIAs; and 2) study participants included
physicians, nurses, midwives, medical officers, general practitioners, gynaecologists and/or
obstetricians. There was no limitation on the study designs except general discussions
without presentation of data and results. We excluded studies that were conducted in low- or
middle- income countries according to the World Bank definition [11] or which did not
measure the outcomes of insertion/removal practices of clinicians after PREECLAMCIA
training. A flowchart for the selection of eligible research articles is presented in Fig 1. After
confirming eligibility for inclusion, the following data were extracted—authors, geographical
location, study design, study setting, study type and size of participants, year of publication,
type/s of PREECLAMCIA training and outcome details—by the first author and then
independently checked by the second author. The GRADE system and risk of bias approach,
as recommended by the Cochrane Collaboration, were used to evaluate the quality of
evidence of each selected study [12]. As there was heterogeneity among the studies with
respect to study design (RCT, cohort or cross-sectional study), study participants and
www.wjpps.com │ Vol 10, Issue 2, 2020. │ ISO 9001:2015 Certified Journal │
234
Hawraa et al. World Journal of Pharmacy and Pharmaceutical Sciences
outcomes measured (incidence, frequency or association), summary measures of the effect of
PREECLAMCIA training were not calculated.
RESULTS
The combined database searches yielded results. Of these, were included to conduct full-text
screening, following review of the title and abstract. In reviewing the full text, 30 studies
were identified as eligible to include. The quality of evidence of most ranged from very low
to moderate, primarily because the majority of studies were observational studies with small
sample sizes (Table 1). Included studies were conducted in Australia, the UK, the USA,
Canada and New Zealand. The PREECLAMCIA training was provided to family planning
physicians (such as obstetricians and gynaecologists), general practitioners, nurses and
midwives (Table 2). Canada and the USA have family planning residency programs for
healthcare providers; and PREECLAMCIA training is compulsory for family planning and
obstetrics-gynaecology residents.[13,14]
Physician interns, nurse practitioner students and
physician assistants in the USA may also receive PREECLAMCIA insertion training.[15]
Family physicians were more likely to receive training in placement of PREECLAMCIAs
compared to medicine physicians (70.4% vs. 9.9%).[16]
Compared to nurse practitioners
working in primary care, those working in women’s health were more likely to receive
PREECLAMCIA insertion practicum training (12% vs. 66%).[17]
Most of the
PREECLAMCIA training for nurses was conducted in family planning services and
clinics.[18–21]
www.wjpps.com │ Vol 10, Issue 2, 2020. │ ISO 9001:2015 Certified Journal │
235
Hawraa et al. World Journal of Pharmacy and Pharmaceutical Sciences
www.wjpps.com │ Vol 10, Issue 2, 2020. │ ISO 9001:2015 Certified Journal │
236
Hawraa et al. World Journal of Pharmacy and Pharmaceutical Sciences
www.wjpps.com │ Vol 10, Issue 2, 2020. │ ISO 9001:2015 Certified Journal │
237
Hawraa et al. World Journal of Pharmacy and Pharmaceutical Sciences
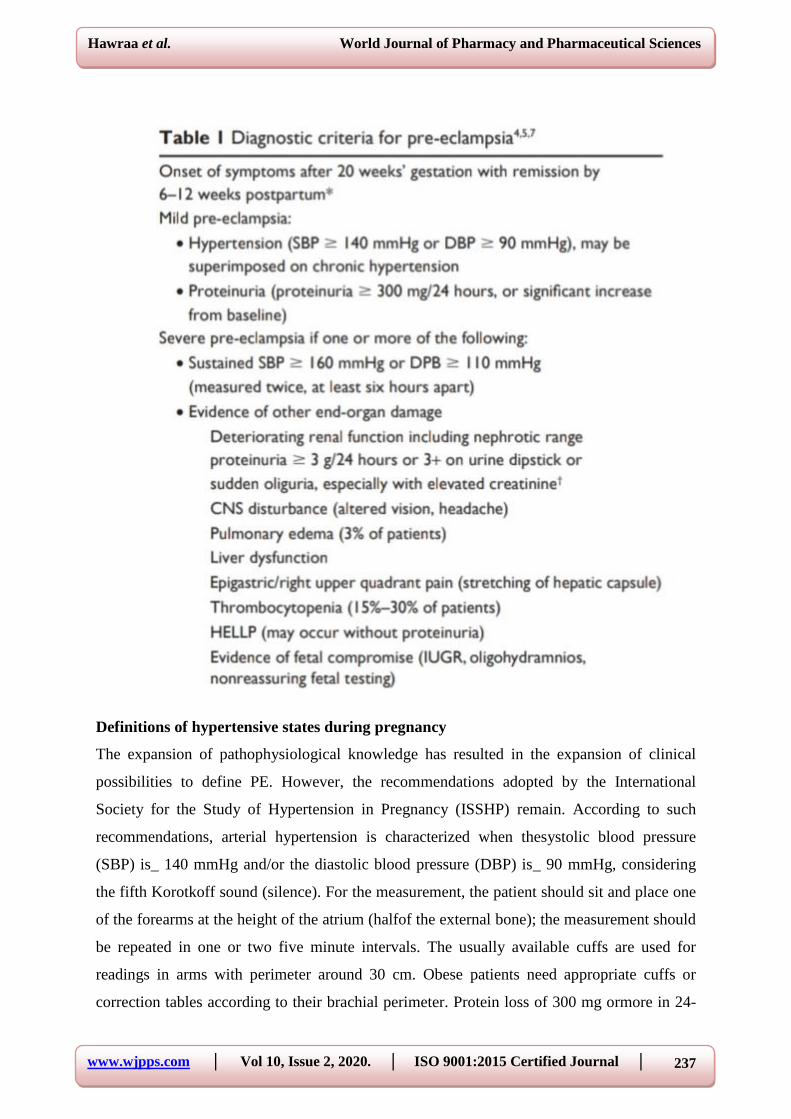
Definitions of hypertensive states during pregnancy
The expansion of pathophysiological knowledge has resulted in the expansion of clinical
possibilities to define PE. However, the recommendations adopted by the International
Society for the Study of Hypertension in Pregnancy (ISSHP) remain. According to such
recommendations, arterial hypertension is characterized when thesystolic blood pressure
(SBP) is_ 140 mmHg and/or the diastolic blood pressure (DBP) is_ 90 mmHg, considering
the fifth Korotkoff sound (silence). For the measurement, the patient should sit and place one
of the forearms at the height of the atrium (halfof the external bone); the measurement should
be repeated in one or two five minute intervals. The usually available cuffs are used for
readings in arms with perimeter around 30 cm. Obese patients need appropriate cuffs or
correction tables according to their brachial perimeter. Protein loss of 300 mg ormore in 24-
www.wjpps.com │ Vol 10, Issue 2, 2020. │ ISO 9001:2015 Certified Journal │
238
Hawraa et al. World Journal of Pharmacy and Pharmaceutical Sciences
hour urine specimen collection should be considered for the definition of proteinuria. For
more agility in the diagnosis, evaluations in an isolated sample of urine with
proteinuria/creatininuria (P/C) ratio (both in mg/dL) _ 0.3 are considered adequate. In the
absence of such diagnostic possibilities, proteinuria with at least 1þ reagent tape may be
considered as long as the quality of the method is assured. Differently from previous
recommendations, the intensity of the proteinuria should no longer be associated with
thematernal prognosis, nor be the only aspect to guide decisions.
Preeclampsia is defined as arterial hypertension identified for the first time after the 20th
week associated with proteinuria, and it may overlap with another hypertensive state. Taking
into account the current concept of PE syndrome, rigid concepts have been abandoned.6
Thus, in the absence of proteinuria, the diagnosis of PE may be based on the presence of
headache, visual turbidity, abdominal pain or altered laboratory tests, such as
thrombocytopenia (less than 100,000/mm3), hepatic enzyme elevation (double the basal),
renal impairment (>1.1 mg/dL or double the baseline), or pulmonary edema and visual or
brain disorders such as headache, scotomas, or convulsions. These criteria should be adopted
for patients with preexisting hypertension (arterial hypertension preceding pregnancy or
identified before 20 weeks), with worsening of baseline blood pressure (BP), and the onset of
proteinuria, suggesting PE overlap. Hence, concerning the diagnosis, preeclampsia is
considered hypertension after the twentieth week and one of the following criteria.
1. Significant proteinuria (P/C ratio > 0.3; > 1.0 g/L on reagent tape).
2. Maternal organic dysfunctions
• Loss of renal function (creatinine > 1.02 mg/dL);
• Hepatic dysfunction (increase of transaminases by > 2 times the normal upper limit;
epigastralgia);
• Neurologic complications (altered mental state; blindness; hyperreflexia with clonus,
scotomas, visual blurring, diplopia, Doppler of maternal ophthalmic artery with peak ratio
> 0.78);
• Hematologic complications (thrombocytopenia, disseminated intravascular coagulation
[DIC] < hemolysis);
• Antiangiogenesis status (PlGF < 36 pg/mL or sFlt-1/ PlGF ratio > 85).
3. Uteroplacental dysfunction (asymmetric intrauterine growth restriction [IUGR]; altered
umbilical Doppler, especially if the Doppler is altered in both maternal uterine arteries).
www.wjpps.com │ Vol 10, Issue 2, 2020. │ ISO 9001:2015 Certified Journal │
239
Hawraa et al. World Journal of Pharmacy and Pharmaceutical Sciences
When PE occurs in pregnant women with chronic hypertension, it is considered over lapping
preeclampsia. Severe preeclampsia is defined as PE associated with severe enough maternal
fetal complications to pose imminent risk of maternal-fetal impairment. Persistent SBP _ 160
mm Hg or DBP _ 110 mm Hg or presence of any of the criteria listed in ►Table 1
characterize a pregnant woman as having severe PE. In general, pregnant women with signs
or symptoms of severe PE have a decompensated disease that may rapidly progress to
maternal and perinatal morbidity and mortality. Proteinuria levels should not be considered
criteria of severity in PE. The presence of PE, regardless of its severity, entails increased fetal
and maternal risk. Eclampsia is the occurrence of generalized motor seizures (grand mal
seizures) in pregnant women with PE that are not caused by coincident neurological disease
and may occur in the prepartum period (50%), during delivery (20%), and in the postpartum
period (between 11 and 44%).
Classification
There are several classifications described for hypertensive disorders in pregnancy. In 2014,
the ISSHP reviewed the classification of hypertensive disorders during pregnancy ►Table2).
Significant Proteinuria It is the excretion of 300 mg ormore of proteins in a 24-hour urine
collection. The 24-hour collection is subject to many collection and storage errors, and should
not be used for clinical purposes unless 24-hour creatinine clearance is also.
Table 2: Classification of hypertensive disorders of pregnancy classification.
1. Chronic hypertension.
2. Gestational hypertension.
3. Preeclampsia with or without over lapping chronichyper tension.
4. White coat hypertension.
Adapted from: Tranquilli et al (2014). measured to assess the adequacy of the collection.5
The measurement of the P/C ratio in the urine sample has been of clinical utility, and values _
0.3 demonstrate a good correlation with significant proteinuria. A P/C ratio in an isolated
sample of urine _ 0.3 corresponds to significant proteinuria 92% of times, and a ratio _ 0.5
corresponds to significant proteinuria 100% of times.9 The presence of 1.0 g/l or more of
proteins on the reagent tape strongly suggests significant proteinuria.
www.wjpps.com │ Vol 10, Issue 2, 2020. │ ISO 9001:2015 Certified Journal │
240
Hawraa et al. World Journal of Pharmacy and Pharmaceutical Sciences
Chronic Arterial Hypertension
Chronic arterial hypertension in pregnancy is the occurrence of systemic arterial hypertension
(SAH) preceding pregnancy. As there often are no records of BP measurements before
gestation, SAHis considered chronicwhen observe din the first trimester of gestation or,
atmost, up to the 20th
week. In most cases, chronic hypertension refers to essential
hypertension, usually associated with family history of hypertension, and often accompanied
by over weightness or obesity. More rarely, secondary hypertension may occur. Given the
age range of the pregnant women, the presence of secondary hypertension is usually due to
underlying parenchymal renal diseases, such as glomerulonephritis and reflux nephropathy.
Gestational hypertension
Gestational hypertension is defined as arterial hypertension arising for the first time after the
20th week of gestation without being accompanied by any signs, symptoms or laboratory
abnormalities that characterize preeclampsia.
White coat hypertension (syndrome)
About 25% of people with increased BP measurements in medical consultations have white
coat hypertension. The diagnosis can be confirmed by serial measurements (preferably taken
by nurses) or ambulatory BP monitoring (ABPM). There are few studies on the repercussion
of this type of disorder in pregnancy, some suggesting that up to 50% of these cases evolve to
gestational hypertension or PE.5 Preeclampsia diagnosis should be presumed in pregnant
women with arterial hypertension and significant proteinuria occurring after the 20th week of
gestation (except in cases of hydatidiform mole, when PE can occur before the 20th week). If
the increase in BP and proteinuria occurs after the 20th week in a primigravida with family
history (mainlysister ormother) of PE or eclampsia, the probability of correct PE diagnosis
will be greater than 90%. Even in the abs ence of significant proteinuria, the occurrence of
hypertension after the 20th week should translate into a PE diagnosis if there are signs of
maternal or placental dysfunction (sFLT-1/PlGF ratio > 85, PlGF < 36 pg/mL, creatinine >
1.02 mg/dL; increased transaminase levels by > 2 times the upper limit of normal;
epigastralgia; altered mental status; blindness; hyperreflexia with clonus, scotomas, visual
disturbance, diplopia, maternal ophthalmic artery Doppler with peak ratio > 0.78;
thrombocytopenia < 150,000/dL, DIC, hemolysis; asymmetric IUGR, umbilical Doppler with
decrease or absence of diastolic flow, reverse diastolic flow in umbilical, especially if it is a
Doppler with a protodiastolic notch in both maternal uterine arteries). Serum uric acid
www.wjpps.com │ Vol 10, Issue 2, 2020. │ ISO 9001:2015 Certified Journal │
241
Hawraa et al. World Journal of Pharmacy and Pharmaceutical Sciences
increases early in PE, and has a positive correlation with placental bed atheromatosis injuries,
lower birth weight infants, degree of hemoconcentration and severity of glomerular
endotheliosis. Uric acid levels > 4.5 mg/dL are abnormal in gestation. The decreased activity
of antithrombin III (AT III, < 70%) correlates with renal glomerular endotheliosis, and its
measurement may be important in the differential diagnosis with chronic hypertension.
Calciuria is decreased in PE, and may also be useful in the differential diagnosis with chronic
hypertension. A 24-hour calciuria below 100 mg suggests PE. In patients at high risk for PE
(►Table 1), it is prudent to perform baseline tests at the beginning of pregnancy for further
comparison. This evaluation should be restricted to the measurement of platelets, creatinine,
uric acid, and a search for basal proteinuria (that is, a P/C ratio in the urine sample). In these
patients, a precise dating of the gestational age (GA) through ultrasonographic examination in
the first trimester is fundamental. A Doppler evaluation of the uterine arteries after the
23rdweek of GA is useful to evaluate the presence of an adequate placental implantation or
not. Uterine arteries with normal resistance indices indicate low probability of occurrence of
PE during pregnancy (high negative predictive value). However, pulsatility indices above the
95th percentile for GA and presence of bilateral protodiastolic notch beyond 27 weeks are
signs of deficient trophoblastic invasion and consequent increased risk of PE and/or IUGR.
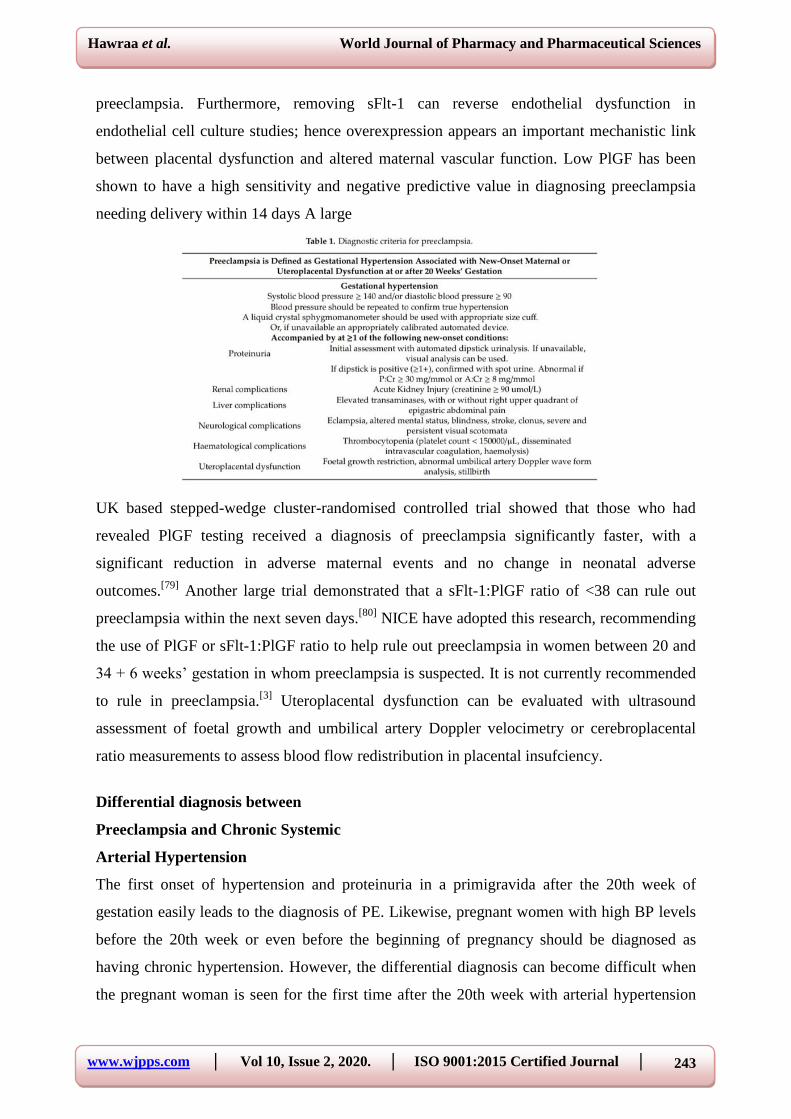
Diagnosis
Internationally, preeclampsia is defined as new-onset gestational hypertension (systolic blood
pressure _140 mmHg and/or diastolic blood pressure _90 mmHg) associated with new-onset
of at least one of proteinuria, maternal organ dysfunction (liver, neurological, haematological,
or renal involvement), or uteroplacental dysfunction at or after 20 weeks’ gestation. It is
important to note that preeclampsia may develop for the first time intrapartum or postpartum.
Super-imposed preeclampsia can also be diagnosed in women with chronic hypertension who
develop new onset proteinuria, maternal organ, or uteroplacental dysfunction consistent with
preeclampsia. Eclampsia occurs when there are convulsions in the setting of preeclampsia.
Blood Pressure
In order to confirm the presence of hypertension, blood pressure should be measured on at
least two occasions four hours apart using an appropriately sized cu_ and validated device for
use in women with preeclampsia. For women at high risk, guidelines recommend monitoring
blood pressure at increased frequency in antenatal clinics, however no exact frequency is
recommended. Recent studies have addressed the potential for women to self-monitor their
www.wjpps.com │ Vol 10, Issue 2, 2020. │ ISO 9001:2015 Certified Journal │
242
Hawraa et al. World Journal of Pharmacy and Pharmaceutical Sciences
blood pressure at home to improve the detection of hypertension in pregnancy, particularly in
women with elevated risk. It appears that self-monitoring is feasible, acceptable to pregnant
women, may reduce clinic visits], and be e_ective for detecting hypertension in pregnancy
and distinguishing white coat hypertension. A current RCT (BUMP) hopes to provide a larger
evidence base to determine the impact of self-monitoring on maternal and neonatal outcomes
and advise how self-monitoring can be implemented into clinical practice.
Proteinuria
The presence of proteinuria has traditionally been screened for by dipstick testing and
confirmedby additional laboratory tests using 24 h urine, or more recently spot samples of
urine. Screening assessment with dipstick testing is best done with an automated reagent-strip
reading device rather than visual analysis. Previously, 24 h urine collection was considered
the gold standard for confirmation of proteinuria but it has several problems: it is time
consuming, requires refrigeration, samples are often incomplete, and is infrequently used in
hospitals. Therefore, after a positive dipstick test (one protein or more), the use of either spot
urine albumin to creatinine (A:Cr) or protein to creatinine (P:Cr) ratios are now
recommended to quantify proteinuria . Both P:Cr and A:Cr testing are shown to significantly
correlate with proteinuria as detected by 24 h urine . Diagnostic thresholds of 30 mg/mmol
and 8 mg/mmol have been determined to provide high sensitivity and specificity,
respectively.
3.3. Laboratory and imaging tests
The ISSHP recommends that pregnant women with de novo hypertension are investigated
with laboratory tests measuring haemoglobin, platelet count, serum creatinine, liver enzymes,
and serum uric acid to determine the presence of maternal organ dysfunction and the
diagnosis of preeclampsia. New guidelines have also implemented PlGF or sFlt-1:PlGF ratio
testing for preeclampsia diagnosis in specific circumstances. There is a large body of work
indicating a role of circulating angiogenic factors, such as sFlt-1 and PlGF, in the
pathogenesis of preeclampsia. Women with preeclampsia have higher circulating levels of
sFlt-1 and lower levels of PlGF, noticeable before the onset of the disease. SFlt-1 is an anti-
angiogenic protein that acts as an antagonist to the angiogenic proteins PlGF and vascular
endothelial growth factor (VEGF). By inhibiting VEGF and PlGF, sFlt-1 alters downstream
signalling pathways, which results in vasoconstriction and endothelial dysfunction.
Increasing sFlt-1 levels in mouse models have been shown to produce a syndrome resembling
www.wjpps.com │ Vol 10, Issue 2, 2020. │ ISO 9001:2015 Certified Journal │
243
Hawraa et al. World Journal of Pharmacy and Pharmaceutical Sciences
preeclampsia. Furthermore, removing sFlt-1 can reverse endothelial dysfunction in
endothelial cell culture studies; hence overexpression appears an important mechanistic link
between placental dysfunction and altered maternal vascular function. Low PlGF has been
shown to have a high sensitivity and negative predictive value in diagnosing preeclampsia
needing delivery within 14 days A large
UK based stepped-wedge cluster-randomised controlled trial showed that those who had
revealed PlGF testing received a diagnosis of preeclampsia significantly faster, with a
significant reduction in adverse maternal events and no change in neonatal adverse
outcomes.[79]
Another large trial demonstrated that a sFlt-1:PlGF ratio of <38 can rule out
preeclampsia within the next seven days.[80]
NICE have adopted this research, recommending
the use of PlGF or sFlt-1:PlGF ratio to help rule out preeclampsia in women between 20 and
34 + 6 weeks’ gestation in whom preeclampsia is suspected. It is not currently recommended
to rule in preeclampsia.[3]
Uteroplacental dysfunction can be evaluated with ultrasound
assessment of foetal growth and umbilical artery Doppler velocimetry or cerebroplacental
ratio measurements to assess blood flow redistribution in placental insufciency.
Differential diagnosis between
Preeclampsia and Chronic Systemic
Arterial Hypertension
The first onset of hypertension and proteinuria in a primigravida after the 20th week of
gestation easily leads to the diagnosis of PE. Likewise, pregnant women with high BP levels
before the 20th week or even before the beginning of pregnancy should be diagnosed as
having chronic hypertension. However, the differential diagnosis can become difficult when
the pregnant woman is seen for the first time after the 20th week with arterial hypertension

www.wjpps.com │ Vol 10, Issue 2, 2020. │ ISO 9001:2015 Certified Journal │
244
Hawraa et al. World Journal of Pharmacy and Pharmaceutical Sciences
and cannot inform her previous blood pressure levels accurately. If the pregnant woman is
not a primigravida, her serum uric acid level is < 4.5 mg/dL, and the 24-hour calciuria > 100
mg, the diagnosis of chronic hypertension is more likely.
Prediction of preeclampsia
Advances in the knowledge of the pathophysiology of PE have resulted in the adoption of
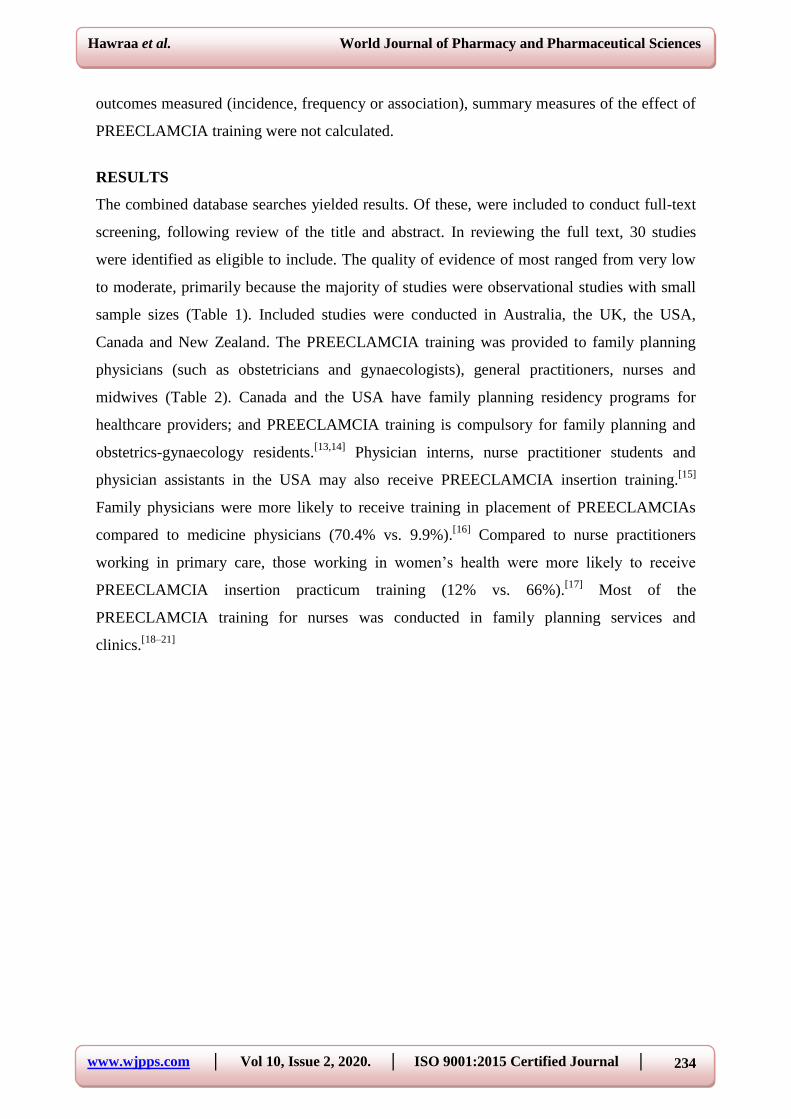
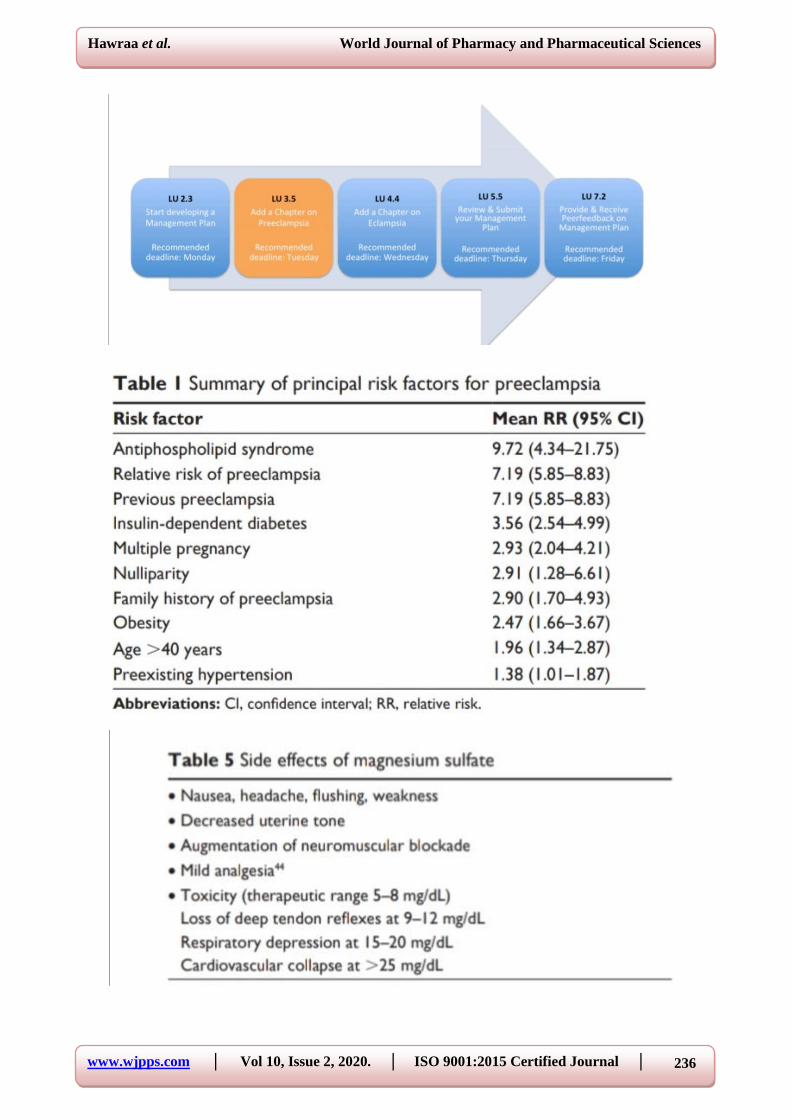
prediction methods. Through epidemiological data, it is possible to recognize women more
likely to develop the disease18 (►Table 1), and develop a differentiated prenatal follow-up
strategy. In addition to the clinical features, the literature is rich in publications suggesting
prediction methods. Among the several alternatives, the use of Doppler of the uterine arteries
and detection of plasmatic substances, such as proteins of placental origin or resulting from
angiogenic imbalance, stand out. The uterine artery Doppler performed in the first or second
trimesters has limited accuracy, presents difficulties in assuring the standardization and
qualifications in its measurement, and the equipment is costly. The various alternatives of
plasma markers also lack the accuracy that justifies their adoption in the clinical practice. The
use of plasma markers related to angiogenesis/antiangiogenesis imbalance has been described
in the literature as a promising tool for the early detection of PE. However, additional studies
are needed to define uniform methods of quantification and evaluate their accuracy before
recommending the use in the clinical practice. Despite the large number of ‘predictive
factors,’ there is no consistent evidence identifying the impact of these methods on maternal
and perinatal prognosis. Thus, there is no consistent evidence to adopt universal screening in
the clinical practice besides the identification of clinical risk. Due to the high incidence and
severity of PE, several attempts have been made to identify the patients at greatest risk of
developing it. Preeclampsia in a previous pregnancy poses an average risk of around 15% for
PE recurrence, and of 22% for gestational hypertension. Recurrence ismore likely if the
previous PE had early onset, was severe, or complicated by eclampsia or HELLP syndrome.
A high BMI during the previous PE increases the risk of recurrence. Among the several tests
proposed to predict the occurrence of PE, the most used currently is the Doppler flowmetry of
the uterine arteries. The Doppler study of the uterine arteries in patients at risk for PE
showing persistent protodiastolic incisions beyond the 23rd week of gestation identifies high-
resistance placental circulation that usually results fromthis deficiency of vascular invasion
by the trophoblast and consequent increased risk of PE and/or IUGR in the current
pregnancy. In a systematic review including 74 studies with 79,547 patients, it was concluded
that the 24-week uterine artery Doppler study is the best predictor of PE. The Doppler should
www.wjpps.com │ Vol 10, Issue 2, 2020. │ ISO 9001:2015 Certified Journal │
245
Hawraa et al. World Journal of Pharmacy and Pharmaceutical Sciences
be considered positive in the presence of an altered pulsatility index (above the 95th
percentile for GA) in combination or not with the persistence of a bilateral protodiastolic
notch in the uterine arteries. The presence of these alterations in the velocimetry test is not a
diagnosis of PE, but in patients with clinical risk, it shows a greater chance of having
pregnancy-specific hypertensive disease and/or IUGR in the current gestation. The greatest
usefulness of this Doppler evaluation is its high negative predictive value. Thus, if a patient at
high clinical risk for PE (that is, mother and sister with positive history of PE) has a Doppler
flowmetry test indicating good diastolic flow in the uterine arteries after the 25th week, her
risk of developing PE decreases. In pregnant women at low clinical risk for PE and IUGR,
there is no use for a Doppler evaluation of the uterine arteries, since this test cannot identify
an increased risk in this population of pregnant women.
www.wjpps.com │ Vol 10, Issue 2, 2020. │ ISO 9001:2015 Certified Journal │
246
Hawraa et al. World Journal of Pharmacy and Pharmaceutical Sciences
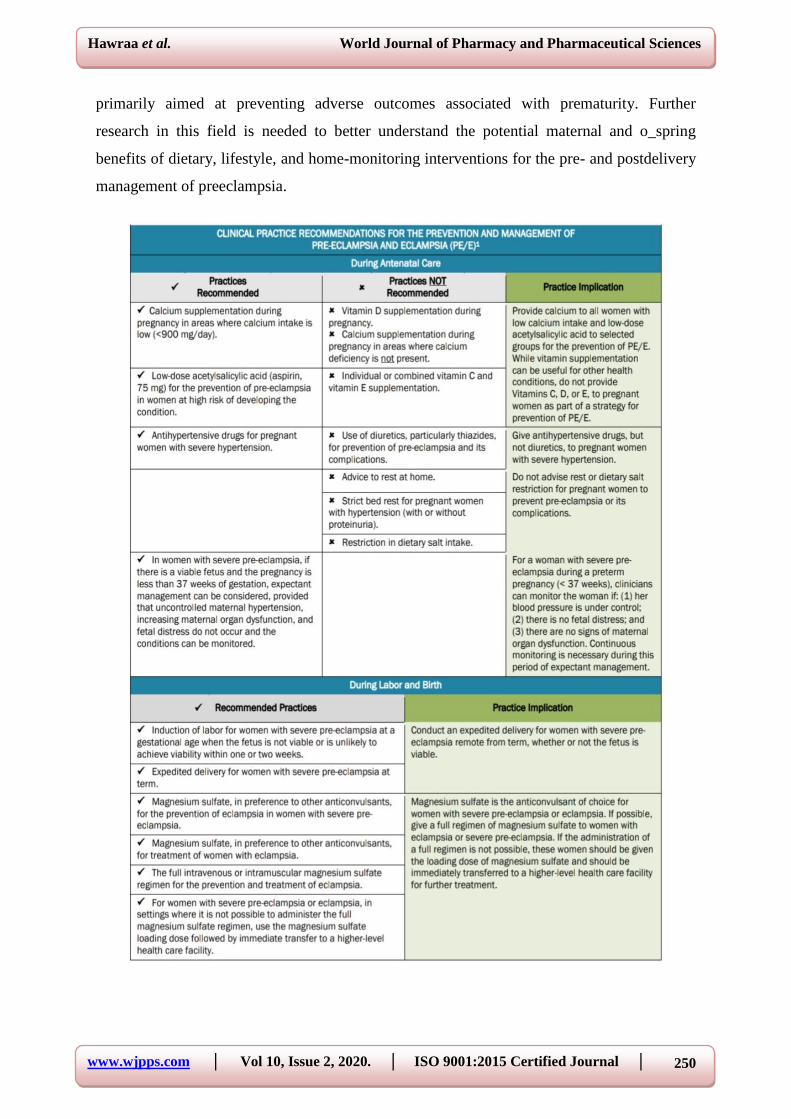
Prevention
Only theuse ofcalciumandlow-dose aspirin are recommended and considered effective in the
clinical practice. Calcium supplementation (calcium carbonate, 1,000–2,000 mg/day) and the
use of small daily doses (50–170 mg) of aspirin for at-risk groups are the only alternatives
that have shown some degree of effectiveness in randomized clinical trials (Grade A of
recommendation).
Immediate emergency management
Delivery is the only curative treatment for pre-eclampsia. Management is multidisciplinary,
involving an obstetrician, an anesthetist, and a pediatrician. In some cases consultation of
maternal fetal medicine and hypertension or nephrology subspecialists may be required.
Management decisions must balance the maternal risks of continued pregnancy against the
fetal risks associated with induced preterm delivery. The criteria for delivery are based on
two often interrelated factors, ie, gestational age at diagnosis (estimated fetal weight) and
severity of pre-eclampsia. Severe pre-eclampsia requires treatment with a dual aim, ie,
preventing the harmful effects of elevated maternal blood pressure and preventing eclampsia.
Management of severe pre-eclampsia begins with transfer of the mother in a fully equipped
ambulance or helicopter to a maternity ward providing an appropriate level of care for both
mother and child. At admission and daily thereafter, clinical, cardiotocographic, laboratory,
and ultrasound testing are required to detect the severity of pre-eclampsia and tailor
management accordingly. Regardless of the severity of pre-eclampsia, there is no advantage
in continuing the pregnancy when pre-eclampsia is discovered after 36–37 weeks. Nor is
expectant management justified for severe pre-eclampsia before 24 weeks, in view of the
high risk of maternal complications and the poor neonatal prognosis. The obstetric team must
then discuss with the parents the possibility of a medical interruption of pregnancy.
Prolongation of pregnancy in the event of mild pre-eclampsia can be discussed and
reevaluated on a regular basis. At 34 –37 weeks, management depends on the severity of the
pre-eclampsia. Expectant management is possible for mild pre-eclampsia to limit the risk of
induced preterm delivery, but for severe pre-eclampsia, delivery remains the rule due to the
increased risk of maternal and fetal complications. Similarly, at 24–34 weeks, management
depends on the severity of pre-eclampsia. The presence of one or more of the following signs
indicates the need for immediate delivery uncontrolled severe hypertension (not responsive to
dual therapy), eclampsia, acute pulmonary edema, abruptio placentae, subcapsular hepatic
hematoma, or thrombocytopenia ,50,000/mm3. Delivery after corticosteroid therapy for
www.wjpps.com │ Vol 10, Issue 2, 2020. │ ISO 9001:2015 Certified Journal │
247
Hawraa et al. World Journal of Pharmacy and Pharmaceutical Sciences
pulmonary maturation is necessary if any of the following criteria is present: persistent
epigastric pain, signs of imminent eclampsia (headaches or persistent visual disorders), de
novo creatinine.120 mol/L, oliguria below 20 mL/hour, progressive HELLP syndrome,
prolonged or severe variable decelerations with short-term variability less than 3
milliseconds. When emergency delivery is not required, labor can be induced by cervical
ripening. Antihypertensive treatment is useful only in severe pre- eclampsia because the sole
proven benefit of such management is to diminish the risk of maternal complications
(cerebral hemorrhage, eclampsia, or acute pulmonary edema). 29 There is no international
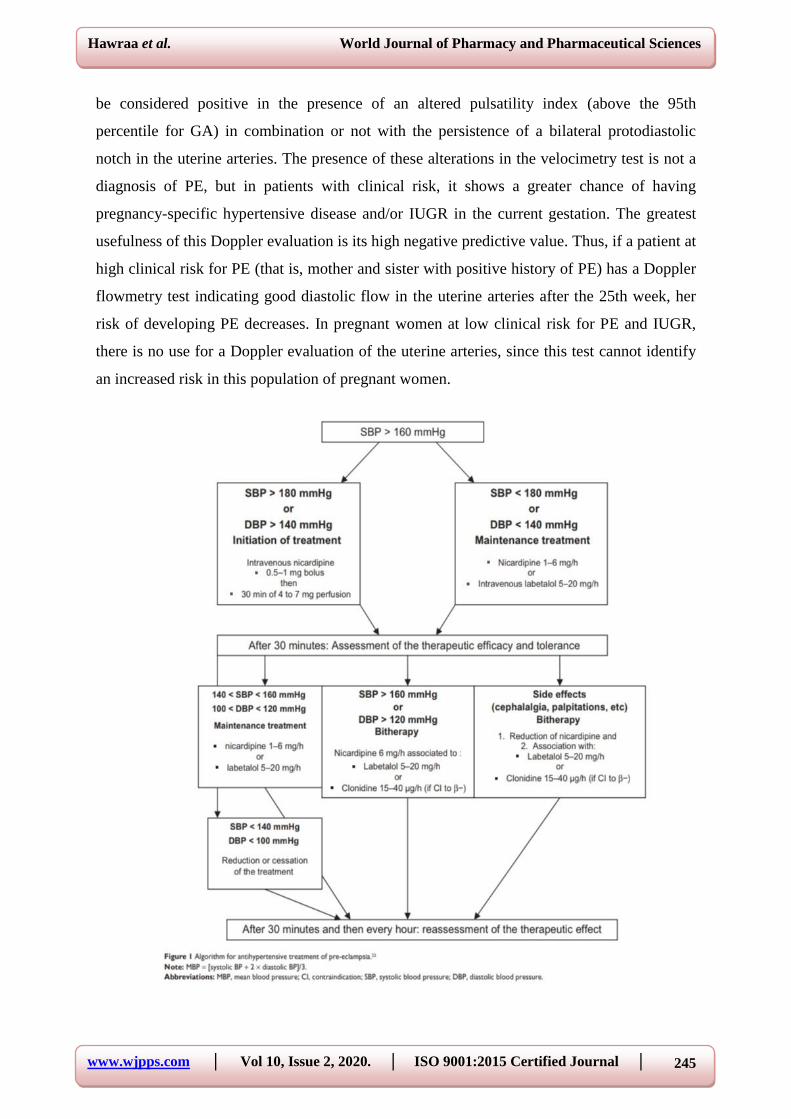
consensus concerning antihypertensive treatment in pre-eclampsia. The four drugs authorized
for the treatment of hypertension in severe pre- eclampsia in France are nicardipine, labetalol,
clonidine, and dihydralazine. There is no ideal target blood pressure value, and too
aggressivea reduction in blood pressure is harmful to the fetus.30 Therapy with a single agent
is advised as first-line treatment, followed by combination treatment when appropriate. The
algorithm for antihypertensive treatment Pulmonary maturation using corticosteroids must be
considered, taking gestational age into account. Betamethasone remains the gold standard at a
dosage of two injections of 12 mg 24 hours apart; this treatment reduces the risk of hyaline
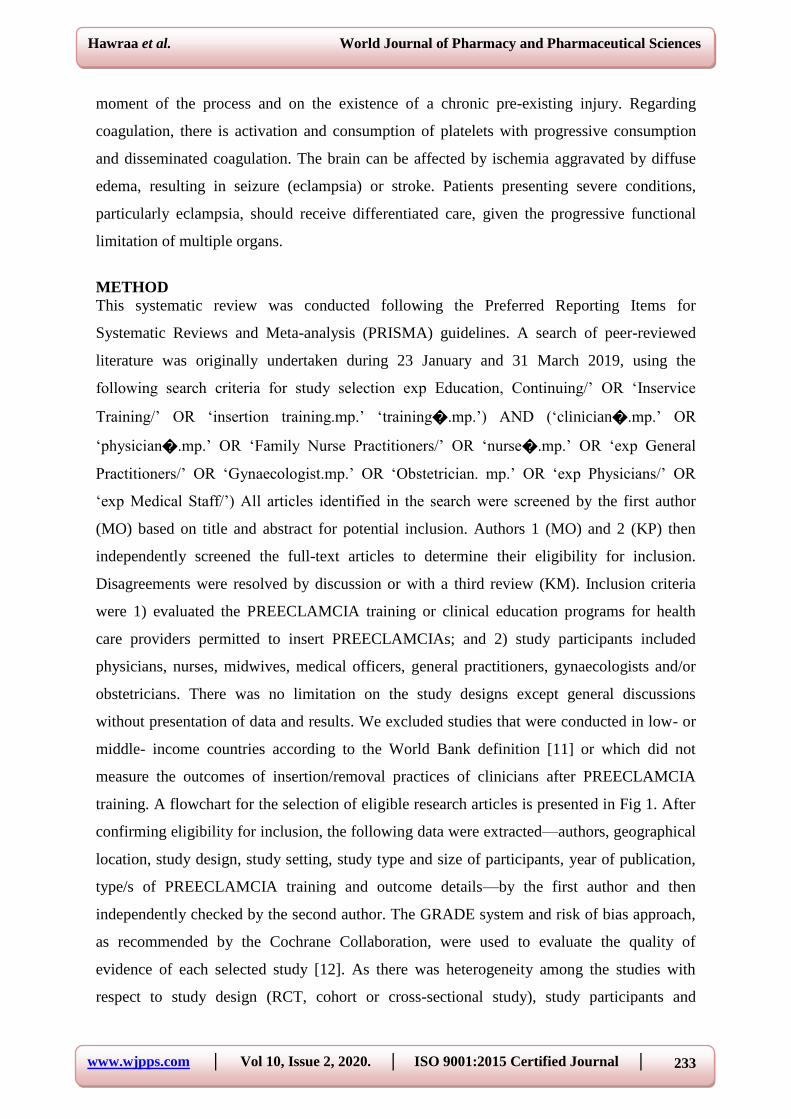
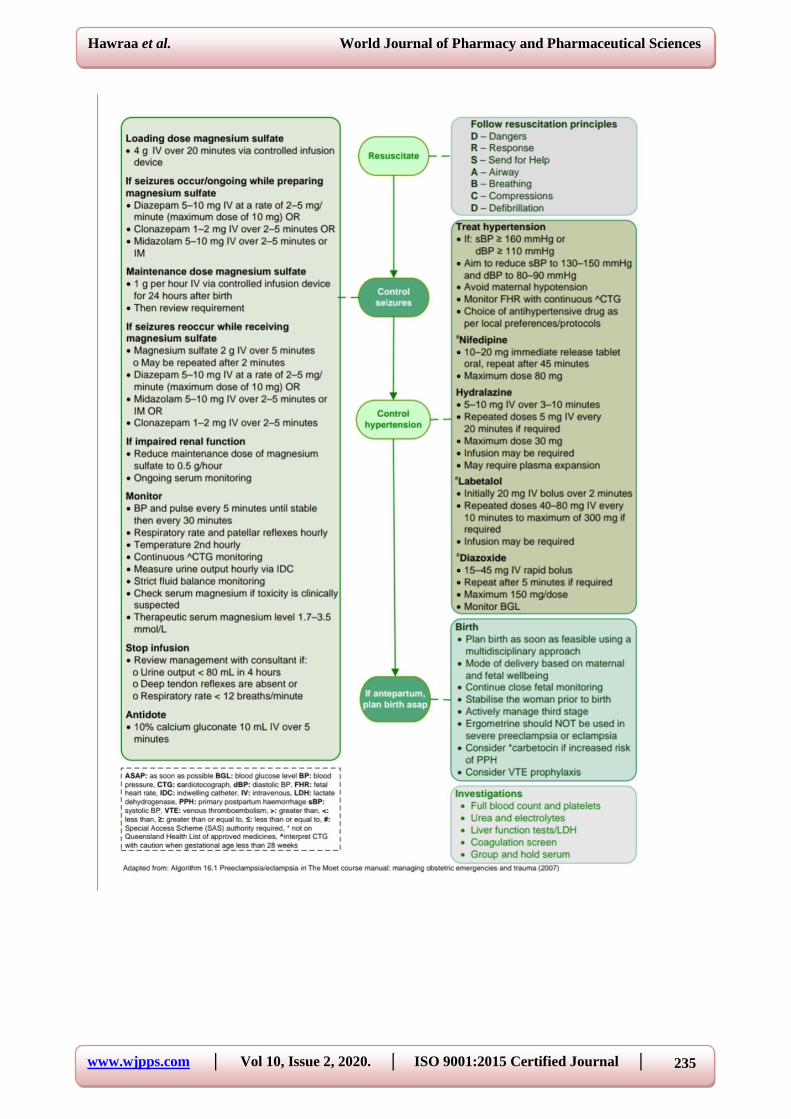
membrane disease, intraventricular hemorrhage, and neonatal mortality. Magnesium sulfate
(MgSO4) may be part of the therapeutic armamentarium for severe pre-eclampsia. It is
indicated in the treatment of eclamptic convulsions as well as for secondary prevention of
eclampsia, thus replacing treatment by diazepam, phenytoin, or the combination of
chlorpromazine, promethazine, and pethidine. The efficacy of MgSO4 in the reduction of
maternal and neonatal complications of eclampsia is well established. It is administered
intravenously, first at a loading dose of 4 g over 15–20 minutes, which can be repeated at a
half dose (2 g) if convulsion recurs, and then at a maintenance dose of 1 g/hour for 24 hours.
22,32 MgSO4 treatment must be monitored in the intensive care unit because organ failure
may occur. This monitoring is based on repeated checking for a Glasgow score of 15, tendon
reflexes, respiratory frequency. 12 per minute, and diuresis. 30 mL/hour. Any manifestation
of overdose requires stopping the infusion, considering injection of calcium gluconate, and
measuring blood magnesium levels. Eclampsia is generally considered an indication for
emergency cesarean section. Nonetheless, a decision to delay a cesarean, albeit rare, may be
based on fetal status and justified if the mother’s condition is stable and reassuring after
treatment.

www.wjpps.com │ Vol 10, Issue 2, 2020. │ ISO 9001:2015 Certified Journal │
248
Hawraa et al. World Journal of Pharmacy and Pharmaceutical Sciences
Management following delivery
Although delivery is the only effective treatment forpre-eclampsia, and despite the fact that
clinical symptoms and laboratory abnormalities usually regress in the hours afterwards, the
risk of complications persists for some time following delivery. Pre-eclampsia is associated
with longterm morbidity and mortality. Approximately 20% of women with pre-eclampsia
develop hypertension or microalbuminuria during long-term follow-up, and the risk of
subsequent cardiovascular and cerebrovascular disease is doubled in women with pre
eclampsia and gestational hypertension compared with age-matched controls. A recent
prospective epidemiological study with a median follow-up duration of 30 years provides
evidence that pre-eclampsia is a marker of increased mortality from cardiovascular disease.
Hemodynamic, neurological, and laboratory monitoring is necessary following delivery for
patients with severe preeclampsia Hemodynamic monitoring includes frequent blood pressure
measurements to enable adjustment of antihypertensive treatment and frequent monitoring of
diuresis and weight according to intake (oliguria should prompt progressive fluid
resuscitation and sometimes diuretic use). Neurological monitoring consists of checking for
signs of imminent eclampsia, including headaches, phosphene signals, tinnitus, and brisk
tendon reflexes. Clinical monitoring must be done several times daily during the week after
delivery, a period considered at high risk for complications. If necessary, monitoring can be
performed in an intensive care unit. Laboratory monitoring should be done several times
daily in the first 72 hours after delivery and thereafter adapted according to progress of the
indices. It must include a complete blood count, liver function tests, and measurement of
lactate dehydrogenase. Discharge from hospital cannot be considered until all clinical and
laboratory indices have returned to normal, and regular monitoring by the patient’s general
practitioner as necessary if treatment for hypertension is to be continued after discharge The
risk of recurrence of pre-eclampsia during a subsequent pregnancy has to be considered. This
risk is estimated to be less than 10% for all cases of pre-eclampsia, but is greater when pre
eclampsia is discovered before 28 weeks. The relative risk is 15 if pre-eclampsia occurs at
20–33 weeks, 10 at 33–36 weeks, and 8 after 37 weeks. Three months after delivery,
screening for underlying renal or hypertensive disease may be requested by the patient’s
primary physician. Such screening is intended to check for normalization of blood pressure
values and disappearance of proteinuria, and if abnormalities persist, a referral should be
made to a nephrologist or a hypertension expert to determine the cause. This examination is
important because pre-eclampsia may unmask previously undiagnosed systemic or kidney
disease or thrombophilia. It should include a specific set of questions, blood pressure
www.wjpps.com │ Vol 10, Issue 2, 2020. │ ISO 9001:2015 Certified Journal │
249
Hawraa et al. World Journal of Pharmacy and Pharmaceutical Sciences
measurement, a clinical examination looking for signs of autoimmune conditions, and a
urinary dipstick test. Testing for antiphospholipid antibodies is recommended after severe
pre-eclampsia. The search for hereditary thrombophilia by assays for protein C and S,
antithrombin III, and a test for resistance to activated protein C is recommended in the case of
a personal or family history of venous thromboembolic disease, early pre-eclampsia, or pre-
eclampsia with any intrauterine growth retardation, abruptio placentae, or in utero death.
Percutaneous needle biopsy of the kidney should be performed only if kidney failure persists
at three months postpartum or if signs of a systemic underlying condition or proteinuria
persist at 6 months. Patients who have had severe pre-eclampsia may share predispositions
with nonpregnant patients who have cardiovascular risk factors. Accordingly, long-term
monitoring of cardiovascular, renal, and metabolic risk factors is recommended after severe
pre-eclampsia.
CONCLUSIONS
Hypertensive disorders of pregnancy now a_ect around one in 10 pregnancies world wide.
This incidence is continuing to increase worldwide and will continue to do so not only in
westernized countries as mothers conceive increasingly later in life, but also in continents
where the vast majority of our population now resides. This includes India, Asia, Africa, and
South America, where changes in socioeconomic status are resulting in a shift towards
conception at an older age, coupled to increasing obesity rates worldwide. In the face of this,
advances in screening, detection, and diagnosis as well as the antenatal, perinatal, and
postnatal management of preeclampsia are required for the mother and their o_spring.
Forwomen at high risk, home blood pressure self-monitoring to improve the detection of
hypertension in pregnancy may be warranted. This could be particularly effective in areas of
the world where access to regular antenatal clinics and midwives remains is limited.
Telemonitored blood pressure o_ers further potential for earlier diagnosis in remote areas,
which is currently being trialled as part of the CRADLE programs. At present, aspirin is the
only therapy with robust evidence to reduce the risk of preeclampsia in high-risk women.
Current recommendations advise low dose (75–150 mg) aspirin as prophylaxis from 12
weeks’ gestation until delivery. Other interventions including nutritional supplements,
pharmacological agents, and dietary and lifestyle interventions have been investigated for
protective e_ects against preeclampsia with varying e_cacy. At present, interventions to
reduce the risk of early foetal complications of preeclampsia remain limited and include
administration of antenatal corticosteroids and magnesium sulphate infusions, which are
www.wjpps.com │ Vol 10, Issue 2, 2020. │ ISO 9001:2015 Certified Journal │
250
Hawraa et al. World Journal of Pharmacy and Pharmaceutical Sciences
primarily aimed at preventing adverse outcomes associated with prematurity. Further
research in this field is needed to better understand the potential maternal and o_spring
benefits of dietary, lifestyle, and home-monitoring interventions for the pre- and postdelivery
management of preeclampsia.
www.wjpps.com │ Vol 10, Issue 2, 2020. │ ISO 9001:2015 Certified Journal │
251
Hawraa et al. World Journal of Pharmacy and Pharmaceutical Sciences
REFERENCES
1. Sibai B, Dekker G, Kupferminc M. Pre-eclampsia. Lancet, 2005; 365: 785–799.
2. Pottecher T, Luton D. Prise en Charge Multidisciplinaire de la Prééclampsie. Issy Les
Moulineaux, France: Elsevier Masson SAS; 2009; French.
3. Carty DM, Delles C, Dominiczak AF. Preeclampsia and future maternal health. J
Hypertens, 2010; 28: 1349–1355.
4. Duley L. The global impact of pre-eclampsia and eclampsia. Semin Perinatol, 2009; 33:
130–137.
5. Zhang J, Zeisler J, Hatch MC, Berkowitz G. Epidemiology of pregnancy-induced
hypertension. Epidemiol Rev, 1997; 19: 218–232.
6. Barton JR, Sibai BM. Prediction and prevention of preeclampsia. Obstet Gynecol, 2008;
112(2 Pt 1): 359–372.
7. Rijhsinghani A, Yankowitz J, Strauss AR, et al. Risk of preeclampsia in second-trimester
triploid pregnancies. Obstet Gynecol, 1997; 90: 884–888.
8. Pre-eclampsia: pathophysiology, diagnosis, and management, Jennifer Uzan1Marie
Carbonnel1Olivier Piconne1, 3Roland Asmar2 Jean-Marc Ayoubi11Department of
Gynecology andObstetrics, Hôpital Foch, Suresnes, France; 2Foundation Medical
ResearchInstitutes, Geneva, Switzerland; 3Department of Gynecology and Obstetrics,
Hôpital Antoine Béclère, Clamart, France.
9. Preeclampsia_José Geraldo Lopes Ramos1 Nelson Sass2 Sérgio Hofmeister Martins
Costa1.
10. Review Preeclampsia: Risk Factors, Diagnosis, Management, and the Cardiovascular
Impact on the O_spring Rachael Fox 1,2, Jamie Kitt 1, Paul Leeson 1, Christina Y.L. Aye
1,3 and Adam J. Lewandowski.





























