Embed Size (px)
Citation preview

PRAXIS LATERALIZATION: ERRORS IN RIGHT AND LEFTHEMISPHERE STROKE
Brenda Hanna-Pladdy1,2* , Stephanie K. Daniels1,3, Melanie A. Fieselman1, KennethThompson1, Jennifer J. Vasterling1,4, Kenneth M. Heilman2 and Anne L. Foundas1,5
(1Department of Psychiatry and Neurology, Tulane University School of Medicine, NewOrleans; 2Department of Neurology, University of Florida, Gainesville; 3Speech PathologyService, Veterans Affairs Medical Center, New Orleans; 4Mental Health Service, Veterans
Affairs Medical Center, New Orleans, and Department of Psychiatry, Louisiana StateUniversity School of Medicine, New Orleans; 5Neurology Service, Veterans Affairs
Medical Center, New Orleans)
ABSTRACT
Whereas the representations of skilled movements in most right handers are stored inthe left hemisphere, the right hemisphere’s contribution to action planning remains unclear.We investigated error patterns in left (LHD) and right hemisphere damaged (RHD) subjectsas well as normal control subjects (C) to determine if specific components of actionprograms may be processed by the right hemisphere or bilaterally represented. We hadthese subjects perform gestures to verbal command with the ipsilesional limb. Although theLHD group made significantly more qualitative errors than the C and RHD groups, theRHD subjects produced a number of apraxic errors. Specifically, the LHD group produceda wide range of spatiotemporal and conceptual errors for both transitive and intransitivegestures, while the RHD group made specific spatial and temporal errors primarily whenperforming transitive gestures. These findings support the postulate that the left hemispherestores the spatiotemporal and conceptual representations of learned skilled movements,while several specific components of action programs, such as external configuration (limborientation) and timing, may have bihemispheric representations.
Key words: apraxia, right hemisphere, error types
INTRODUCTION
Liepmann (1905) studied right handed patients with left or right hemispherelesions for the failure to perform skilled movements. All of Liepmann’s patientswith ideomotor apraxia had left hemisphere lesions. Liepmann suggested thatapraxia was a disorder involving the control of purposeful movements caused bythe destruction of movement representations stored in the left hemisphere of righthanders (Liepmann, 1908). Nonetheless, Liepmann did not completely exclude thepotential contribution of the right hemisphere for action planning (Rothi andHeilman, 1996). The hypothesis that the left hemisphere is dominant forprogramming motor skills in right handers has received a great deal of supportfrom a number of investigators (Ajuriaguerra, Hécaen and Angelergues, 1960; DeRenzi, Faglioni and Sorgato, 1982; Goodglass and Kaplan, 1963; Haaland andHarrington, 1996; Kimura and Archibald, 1974). However there are few cases in
Cortex, (2001) 37, 219-230
* Is currently at the University of Florida.
the literature of right handed patients who developed apraxia with righthemisphere damage (Assal, Perentes and Deruaz, 1981; De Renzi et al., 1982;Mozaz, Marti, Carrera et al., 1990; Rapcsak, Rothi and Heilman, 1987). Patientswith ideomotor apraxia make spatial, timing, and sequencing errors (Poizner,Mack, Verfaellie et al., 1990; Rothi, Ochipa and Heilman, 1991). However, thereremains considerable controversy regarding which error types are pathognomonicof ideomotor apraxia and whether the error types reflect specific deficits incognitive-motor operations (Goodglass and Kaplan, 1963; Haaland and Flaherty,1984; Harrington and Haaland, 1997; Rothi, Mack, Verfaellie et al., 1988; Roy,1985; McDonald, Tate and Rigby, 1994). Although there is a consensus that therepresentations of learned skilled movements are stored in the left hemisphere inmost right handers, it is unclear whether some specific components of thesemovements may be preferentially processed in the right hemisphere or may bebilaterally represented. The contribution of the right hemisphere to action planninghas been addressed in a few studies, but the nature of this contribution remainsunclear (Haaland and Flaherty, 1984; Maher, Rothi and Heilman, 1997).
Although, in most right handed patients, impairment in the performance ofskilled purposeful movements is more commonly associated with left than righthemisphere damage, there is some evidence that praxis functions might be morebilaterally distributed than are language functions (Foundas, Henchey, Gilmoreet al., 1995). Several investigators have found that the incidence of aphasia withleft hemisphere damage is greater than the incidence of apraxia. Thisdissociation between language functions and praxis functions (Alexander, Baker,Naeser et al., 1992; Foundas et al., 1995; Kertesz, Ferro and Shewan, 1984;Papagno, Della Sala and Basso, 1993) may be related to the role of the righthemisphere in praxis function. Furthermore, there is some controversy as towhether the qualitative aspects of praxis are significantly different in righthemisphere versus left hemisphere damage, with few studies directly comparingleft and right hemisphere qualitative praxis error types (De Renzi, Motti andNichelli, 1980; Duffy and Duffy, 1989; Foundas et al., 1995; Haaland andFlaherty, 1984; Maher et al., 1997; Rapcsak et al., 1987).
The aim of this study was to compare transitive and intransitive gestures inpatients with left and right brain damage to controls, and to explore theexistence of qualitative differences between these groups. Furthermore, thisanalysis will help determine which error types are most predictive of limbapraxia, and whether the scoring system utilized is successful in discriminatingbetween these groups. The differential error patterns within left and righthemisphere damaged patients may reflect the relative contribution of eachhemisphere to praxis functions.
MATERIALS AND METHODS
Subjects
The subjects of this study were right handed men who were recruited and tested at theNew Orleans Veterans Administration Medical Center (VAMC). The subject groupsincluded 12 normal subjects who were without a history of neurological or psychiatricdiseases (mean age = 59; mean education = 12.36), 14 patients with unilateral ischemic
220 Brenda Hanna-Pladdy and Others
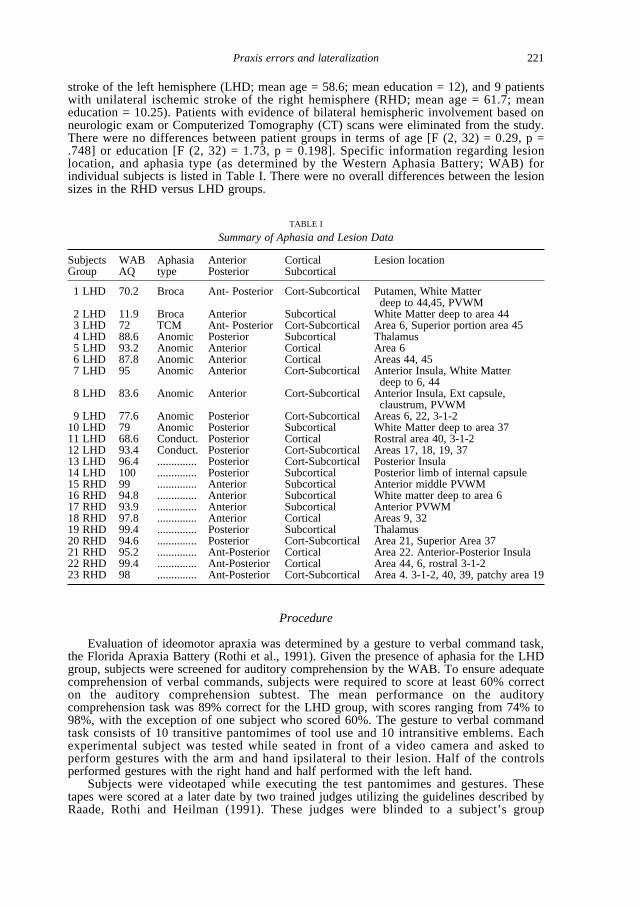
stroke of the left hemisphere (LHD; mean age = 58.6; mean education = 12), and 9 patientswith unilateral ischemic stroke of the right hemisphere (RHD; mean age = 61.7; meaneducation = 10.25). Patients with evidence of bilateral hemispheric involvement based onneurologic exam or Computerized Tomography (CT) scans were eliminated from the study.There were no differences between patient groups in terms of age [F (2, 32) = 0.29, p =.748] or education [F (2, 32) = 1.73, p = 0.198]. Specific information regarding lesionlocation, and aphasia type (as determined by the Western Aphasia Battery; WAB) forindividual subjects is listed in Table I. There were no overall differences between the lesionsizes in the RHD versus LHD groups.
Procedure
Evaluation of ideomotor apraxia was determined by a gesture to verbal command task,the Florida Apraxia Battery (Rothi et al., 1991). Given the presence of aphasia for the LHDgroup, subjects were screened for auditory comprehension by the WAB. To ensure adequatecomprehension of verbal commands, subjects were required to score at least 60% correcton the auditory comprehension subtest. The mean performance on the auditorycomprehension task was 89% correct for the LHD group, with scores ranging from 74% to98%, with the exception of one subject who scored 60%. The gesture to verbal commandtask consists of 10 transitive pantomimes of tool use and 10 intransitive emblems. Eachexperimental subject was tested while seated in front of a video camera and asked toperform gestures with the arm and hand ipsilateral to their lesion. Half of the controlsperformed gestures with the right hand and half performed with the left hand.
Subjects were videotaped while executing the test pantomimes and gestures. Thesetapes were scored at a later date by two trained judges utilizing the guidelines described byRaade, Rothi and Heilman (1991). These judges were blinded to a subject’s group
Praxis errors and lateralization 221
TABLE I
Summary of Aphasia and Lesion Data
Subjects WAB Aphasia Anterior Cortical Lesion locationGroup AQ type Posterior Subcortical
1 LHD 70.2 Broca Ant- Posterior Cort-Subcortical Putamen, White Matter deep to 44,45, PVWM
2 LHD 11.9 Broca Anterior Subcortical White Matter deep to area 443 LHD 72 TCM Ant- Posterior Cort-Subcortical Area 6, Superior portion area 454 LHD 88.6 Anomic Posterior Subcortical Thalamus5 LHD 93.2 Anomic Anterior Cortical Area 66 LHD 87.8 Anomic Anterior Cortical Areas 44, 457 LHD 95 Anomic Anterior Cort-Subcortical Anterior Insula, White Matter
deep to 6, 448 LHD 83.6 Anomic Anterior Cort-Subcortical Anterior Insula, Ext capsule,
claustrum, PVWM9 LHD 77.6 Anomic Posterior Cort-Subcortical Areas 6, 22, 3-1-2
10 LHD 79 Anomic Posterior Subcortical White Matter deep to area 3711 LHD 68.6 Conduct. Posterior Cortical Rostral area 40, 3-1-212 LHD 93.4 Conduct. Posterior Cort-Subcortical Areas 17, 18, 19, 3713 LHD 96.4 .............. Posterior Cort-Subcortical Posterior Insula14 LHD 100 .............. Posterior Subcortical Posterior limb of internal capsule15 RHD 99 .............. Anterior Subcortical Anterior middle PVWM16 RHD 94.8 .............. Anterior Subcortical White matter deep to area 617 RHD 93.9 .............. Anterior Subcortical Anterior PVWM18 RHD 97.8 .............. Anterior Cortical Areas 9, 3219 RHD 99.4 .............. Posterior Subcortical Thalamus20 RHD 94.6 .............. Posterior Cort-Subcortical Area 21, Superior Area 3721 RHD 95.2 .............. Ant-Posterior Cortical Area 22. Anterior-Posterior Insula22 RHD 99.4 .............. Ant-Posterior Cortical Area 44, 6, rostral 3-1-223 RHD 98 .............. Ant-Posterior Cort-Subcortical Area 4. 3-1-2, 40, 39, patchy area 19
membership when scoring the responses. The use of the ipsilesional limb by the strokepatients may have provided a clue to the judges about which hemipshere may have beeninjured. Control subjects, however, also used either the left or right limb, making itdifficult for the judges to fully ascertain group membership. Gestures were scoredquantitatively for accuracy using a severity scale similar to that used by Kaplan (1968): 0(no response, unrecognizable), 1 (degraded, recognizable), 2 (imperfect but not apraxic), 3(perfect), maximum correct = 60. Error types were scored for each apraxic gesture (a scoreof 0 or 1) using Rothi et al.’s (1988) criteria as described in the Appendix. Errors werecategorized as spatial, temporal, content, or other errors. Each gesture/pantomime couldhave multiple error types.
RESULTS
Transitive/Intransitive Gestures
A MANOVA was performed with group (controls, LHD, RHD) as theindependent variable (IV) and the quantitative scores reflecting the degree ofaccuracy (0, 1, 2, 3) of transitive (pantomimes involving the use of an object ortool) and intransitive gestures by group as the dependent variables (DVs). TheMANOVA was significant, F (4, 64) = 10.752, p < .0001, and was followed byunivariate analyses set at an α of .01 to reduce the risk of Type I errors. Therewas a significant difference in transitive [F (2, 32) = 21.64, p < .0001] andintransitive [F (2, 32) = 9.26, p < .001] scores between groups. Bonferronicorrected t-tests to control for multiple comparisons (4 total tests), revealed thatboth the LHD (mean transitive= 40.95% correct; mean intransitive= 63.3%correct) and the RHD groups (mean transitive= 56.67% correct; meanintransitive= 81.1% correct) produced significantly lower transitive scores (tLHD = – 6.94, p < .0001; tRHD = – 3.83, p < .001) than controls (mean transitive= 84.72% correct; mean intransitive= 93% correct), while the LHD group wasalso impaired for intranstive gestures (tLHD = – 4.83, p < .0001; tRHD = – 1.77, p = .056).
Specific Errors
Four separate MANOVAs were conducted on the major error types: (1)spatial errors (amplitude, movement, body part as tool, internal and externalconfiguration), (2) temporal errors(time, sequence, occurrence), (3) contenterrors (perseveration, related content, unrelated content), and (4) other errors(unrecognizable, no-response).
Spatial Errors
The multivariate test revealed a significant effect of group on the number ofqualitative spatial errors, F (10, 58) = 2.374, p < .02. Univariate F-tests(utilizing α = .01 to reduce Type I errors) revealed a significant difference forthe number of internal configurationerrors [F (2, 32) = 10.19, p < .0001],movementerrors [F (2, 32) = 9.51, p < .001], external configurationerrors
222 Brenda Hanna-Pladdy and Others
[F (2, 32) = 9.08, p < .001], body part as tool errors [F (2, 32) = 6.59, p <.004], but not amplitude errors [F (2, 32) = 1.637, p = .211] between groups.
Temporal Errors
The multivariate test revealed a significant effect of group on the number ofqualitative temporal errors, F (4, 64) = 5.723, p < .001. Univariate F-tests(utilizing α = .01 to reduce Type I errors) revealed a significant differencebetween groups for the number of timing errors [F (2, 32) = 7.839, p < .002],but insignificance for occurrenceerrors [F (2, 32) = 2.393, p = .108] andsequence errorswhich were not produced by any of the groups.
Content Errors
The multivariate test revealed a significant effect of group on the number ofqualitative content errors, F (6, 62) = 3.267, p < .007. Univariate F-tests with anα at .01 revealed a significant difference for the number of unrelated contenterrors [F (2, 32) = 4.624, p < .01], while related content errors [F (2, 32) =3.84, p < .032] and perseverative errors[F (2, 32) = 1.29, p = .287] were notsignificant between groups.
Other Errors
The multivariate test did not reveal a significant effect of group on thenumber of other errors (unrecognizable, no response), F (4, 64) = 1.089, p =.369.
Follow-up Comparisons
Follow-up contrasts were performed to determine whether stroke groupsproduced significantly more errors than control subjects for the 6 specific errors(internal configuration, external configuration, movement, body part as tool,timing, and unrelated content) that were significant at the univariate level acrossthe 4 MANOVAs. A Bonferroni-Holm correction procedure was utilized tocontrol for the 12 comparisons.
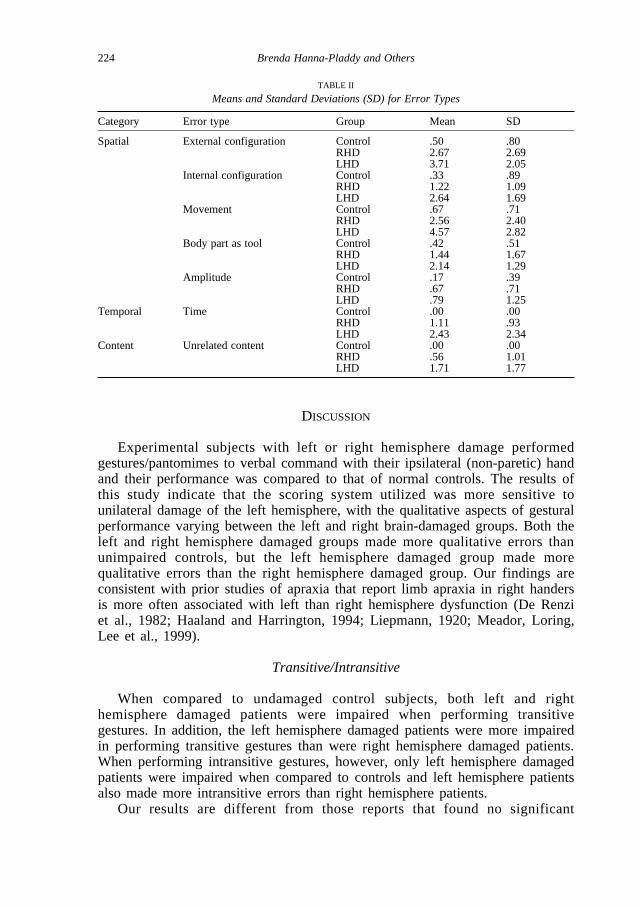
The LHD group made significantly more external configuration (t = 5.399, p < .0001), movement (t = 4.685, p < .0001), body part as tool (t = 4.59, p < .0001), internal configuration (t = 4.44, p < .0001), timing (t = 3.877, p < .008), and unrelated content (t = 2.89, p < .030) errors than controls (seeTable II for means and standard deviations). The RHD group made significantlymore timing (t = 3.592, p < .0245) and external configuration (t = 2.338, p < .04) errors relative to controls, but did not produce a significantly greaternumber of movement (t = 2.155, p = .108), internal configuration (t = 2.058, p = .081), body part as tool (t = 2.026, p = .057), or unrelated content errors (t = .855, p = .403) when compared to the control subjects (Table II).
Praxis errors and lateralization 223
DISCUSSION
Experimental subjects with left or right hemisphere damage performedgestures/pantomimes to verbal command with their ipsilateral (non-paretic) handand their performance was compared to that of normal controls. The results ofthis study indicate that the scoring system utilized was more sensitive tounilateral damage of the left hemisphere, with the qualitative aspects of gesturalperformance varying between the left and right brain-damaged groups. Both theleft and right hemisphere damaged groups made more qualitative errors thanunimpaired controls, but the left hemisphere damaged group made morequalitative errors than the right hemisphere damaged group. Our findings areconsistent with prior studies of apraxia that report limb apraxia in right handersis more often associated with left than right hemisphere dysfunction (De Renziet al., 1982; Haaland and Harrington, 1994; Liepmann, 1920; Meador, Loring,Lee et al., 1999).
Transitive/Intransitive
When compared to undamaged control subjects, both left and righthemisphere damaged patients were impaired when performing transitivegestures. In addition, the left hemisphere damaged patients were more impairedin performing transitive gestures than were right hemisphere damaged patients.When performing intransitive gestures, however, only left hemisphere damagedpatients were impaired when compared to controls and left hemisphere patientsalso made more intransitive errors than right hemisphere patients.
Our results are different from those reports that found no significant
224 Brenda Hanna-Pladdy and Others
TABLE II
Means and Standard Deviations (SD) for Error Types
Category Error type Group Mean SD
Spatial External configuration Control .50 .80RHD 2.67 2.69LHD 3.71 2.05
Internal configuration Control .33 .89RHD 1.22 1.09LHD 2.64 1.69
Movement Control .67 .71RHD 2.56 2.40LHD 4.57 2.82
Body part as tool Control .42 .51RHD 1.44 1.67LHD 2.14 1.29
Amplitude Control .17 .39RHD .67 .71LHD .79 1.25
Temporal Time Control .00 .00RHD 1.11 .93LHD 2.43 2.34
Content Unrelated content Control .00 .00RHD .56 1.01LHD 1.71 1.77
difference between left hemisphere damaged patients and controls whenperforming intransitive movements (Haaland and Flaherty, 1984). Our results arealso different from those reports indicating no significant differences betweenleft and right hemisphere patients’ error types when performing transitivegestures (Duffy and Duffy, 1989). Furthermore, these findings do not supportthe work of those who attribute the association of left hemisphere damage andapraxia to the heavy reliance on transitive gestures (Duffy and Duffy, 1989;Haaland and Flaherty, 1984), but are more in line with researchers who havesuggested that there is a greater impairment of transitive than intransitivegestures (Foundas et al., 1999; Goldstein, 1948; Goodglass and Kaplan, 1963;Haaland and Flaherty, 1984; Kertesz and Hooper, 1982; Rapcsak, Ochipa,Beeson et al., 1993; Roy, Square-Storer, Hogg et al., 1991). Given thecomplexity in movement components associated with transitive movements andthe number of possible errors, it is unclear if the differences we found betweentransitive and intransitive gestures are related to conceptual-semantic features,the use of different praxis representations, or the different degrees of movementcomplexity. Further investigation exploring intrahemispheric processing ofskilled movements that control for the number of movement componentsbetween transitive and intransitive gestures might aid in determination of therelative role of each hemisphere in performing transitive and intransitivegestures.
Types of Errors
The results of this study are consistent with the prior reports that ideomotorapraxia is often associated with spatial and temporal errors (Foundas et al.,1995; Goodglass and Kaplan, 1963; Rothi et al., 1988; Poizner et al., 1990).Although spatial and temporal errors were the most frequently made errors (withboth left and right hemisphere damaged groups making more spatial andtemporal errors than controls), it was the left hemisphere damaged group thatmade the most spatial and temporal errors, supporting prior studies whichsuggest that spatiotemporal movement representations are primarily stored in thishemisphere (Heilman, Rothi and Valenstein, 1982; Rothi et al., 1988). The lefthemisphere damaged group also made more content errors than did the othergroups, suggesting the left hemisphere also mediates action semantics (Heilman,Maher, Greenwald et al., 1995).
Spatiotemporal errors are thought to result from injury to the “visuokinestheticengrams” or ”praxicons” in the left hemisphere that contain the spatiotemporalmovement representations, disconnection of these engrams from motor associationareas, or damage to the motor association (premotor) cortex that translates theserepresentations to motor programs (Heilman, 1979; Liepmann, 1905, 1920).Without access to the information in the “visuokinesthetic engrams”, the motorsystem is unable to position the body parts correctly in space (Heilman and Rothi,1985). The specific error types (internal configuration, movement, externalconfiguration, BPT, timing, unrelated content) successfully discriminated lefthemisphere damaged patients from controls. Our findings are in agreement withRothi et al. (1988) who identified similar error types with left hemisphere
Praxis errors and lateralization 225
impairment, and with Haaland and Flaherty (1984), who suggested that the lefthemisphere patient has problems in the integration and differentiation of theintrapersonal and extrapersonal representation of space. Although externalconfiguration errors discriminated between left hemisphere damage and controls,right hemisphere damaged patients also evidenced poor extrapersonal movements.It has been shown using regional cerebral blood flow that extrapersonalmovements require activation of the parietal areas of both hemispheres (Roland,Skinhoj and Lassen, 1981). In contrast, internal configuration errors were impairedwith left hemisphere damaged subjects but unimpaired in right hemispheredamaged subjects, suggesting that the representations that guide a limb to a real orimagined object in the environment are different than those that guide the limb’sposture (e.g., extrapersonal versus intrapersonal).
Heilman and Rothi (1985) posited that when an apraxic patient is asked topantomime transitive movements, they may use a body part as a tool becausewith a loss of internal configuration or postural representations but relativelyintact emblems (intransitive representations), the emblems may be used as analternative strategy. While transitive movements appear to be mediated, to someextent, by both hemispheres (although greater impairment was evident for theLHD group), the finding that BPT and internal configuration errors wereassociated with left hemisphere damage is consistent with the postulate thatpostural representations are stored in the left hemisphere. However, perseverativeand sequencing errors, which have been emphasized in prior studies, were notimportant errors for either the left or right hemisphere groups.
Alterations from the typical timing or speed of a pantomime or irregular ratesof movement production (i.e., time errors), were the best predictors of righthemisphere damage. The prospect of right hemisphere control of timingmovements, is compatible with Harrington, Haaland, and Knight’s (1998)findings of time perception deficits with focal right, but not left, hemispherelesions. Similarly, Rao, Harrington, Haaland and colleagues (1997) reportedfunctional magnetic resonance imaging (fMRI) activation of the right inferiorfrontal gyrus in a motor timing task. Based on these findings and theiridentification of 100% impaired timing for RHD patients with either anterior orposterior damage, Harrington and colleagues (1998) proposed a role for anteriorand posterior regions of the right hemisphere in temporal computationscompatible with the reciprocal connections between the inferior parietal cortexand corresponding frontal cortical areas in monkeys (Selemon and Goldman-Rakic, 1988). They posited that the right inferior parietal cortex and its role intime-dependent processes may represent an analog of left hemisphere dominancefor spatiotemporal patterning of movements (Haaland and Harrington, 1996;Harrington et al., 1998). Although a number of other studies have implicated theright hemisphere to have a time-dependent component (Maquet, Lejeune,Pouthas et al., 1996; Rao et al., 1997; Roland et al., 1981), studies ofhemispheric asymmetries of timing have been somewhat inconsistent, with onepositron emission tomography (PET) study failing to reveal hemispheric bias forinterval discriminations (Jueptner, Rijntes, Weiller et al., 1995).
An analysis of errors types made during praxis testing in patients undergoingselective hemispheric anesthesia (Wada testing), also suggested differential roles
226 Brenda Hanna-Pladdy and Others
of the left and right hemispheres in praxis functions (Foundas et al., 1995).Whereas the left hemisphere appeared to be more important for the spatialaspects of the praxis program, the right hemisphere appeared to be moreimportant for the temporal aspects.Overall, the pattern of error types in thiscurrent study, support the dominance of the left hemisphere for therepresentation of action semantics and spatiotemporal movement representations,but also highlight the role of the right hemisphere in timing as it relates to thebinding of the spatial properties of produced movements.
These findings support the dominant role of the left hemisphere for skilledmovements, but also reveal the potential for more bilateral representation ofpraxis, which was evident in the significant number of timing and externalconfiguration errors made by right hemisphere damaged patients. A recent studyof tool-use pantomimes with fMRI revealed bilateral intraparietal cortexactivation in addition to significant left hemisphere activation (Moll, DeOliveira-Souza, Passman et al., 2000). There is some evidence that a relationshipexists between atypical language dominance and greater bilateral distribution ofspatiotemporal movement representations (Meador et al., 1999). Futureinvestigations of associated bihemispheric representation of the praxis systemsuch as strength of handedness and/or atypical language representation, as wellas identification and development of a qualitative system which bettercharacterizes right hemispheric errors, might further enhance our knowledge andunderstanding of praxis lateralization.
In summary, the results of this study support a dominant role of the lefthemisphere in programming skilled movements or praxis, and indicate that theapraxia scoring system was successful in capturing the nature of the errorsinduced by left hemisphere dysfunction (Rothi et al., 1988). Additionally, thequalitative analysis between left and right hemisphere damage revealed a patternof errors which implicates bihemispheric representation of specific spatial andtemporal aspects of skilled movements. Our data supports the notion that learnedskilled movements are mediated by a distributed modular network in the lefthemisphere, although some aspects, such as timing and extrapersonalrepresentations of learned skilled movements may also be processed in the righthemisphere (Haaland and Harrington, 1996; Heilman and Rothi, 1993; Foundaset al., 1995; Maher et al., 1997).
Acknowledgements. This work was presented, in part, at the Twenty-fifth Annualmeeting of the International Neuropsychological Society (INS), Orlando, FL, February1997. This project was supported by NIH grant DC00135 (ALF) and the Department ofVeterans Affairs VISN 16 MIRECC.
REFERENCES
AJURIAGUERRA, DE F., HÉCAEN, H., and ANGELERGUES, R. Les apraxies. Varietes cliniques etlateralization lesionelle. Revue Neurologique, 102: 566-594, 1960.
ALEXANDER, M.P., BAKER, E., NAESER, A., KAPLAN, E., and PALUMBO, C. Neuropsychological andneuroanatomical dimensions of ideomotor apraxia. Brain, 115: 87-107, 1992.
ASSAL, G., PERENTES, E., and DERUAZ, J.P. Crossed aphasia in a right handed patient. Postmortemfindings. Archives of Neurology, 38: 455-458, 1981.
Praxis errors and lateralization 227
DE RENZI, E., FAGLIONI, P., and SORGATO, P. Modality-specific and supramodal mechanisms of apraxia.Brain, 105: 301-312, 1982.
DE RENZI, E., MOTTI, F., and NICHELLI , P. Imitating gestures: A quantitative approach to ideomotorapraxia. Archives of Neurology, 37: 1-10, 1980.
DUFFY, R.J., and DUFFY, J.F. An investigation of body part as object (BPO) responses in normal andbrain-damaged adults. Brain and Cognition, 10: 220-236, 1989.
FOUNDAS, A.L., HENCHEY, R., GILMORE, R.L., FENNELL, E.B., and HEILMAN , K.M. Apraxia during Wadatesting. Neurology, 45: 1379-1383, 1995.
GESCHWIND, N. Disconnexion syndromes in animals and man, Part II. Brain, 88: 585-644, 1965.GESCHWIND, N. The apraxias: Neural mechanisms of disorders of learned movement. American Scientist,
63: 188-95, 1975.GOLDSTEIN, K. Language and Language Disturbances. New York: Grune and Stratton, 1948.GOODGLASS, H., and KAPLAN, E. Disturbances of gesture and pantomime in aphasia. Brain, 86: 703-720,
1963.HAALAND , K.Y., and HARRINGTON, D.L. Hemispheric asymmetry of movement. Current Opinions in
Neurobiology, 6: 796-800, 1996.HAALAND , K.Y., and FLAHERTY, D. The different types of limb apraxia errors made by patients with left
vs. right hemisphere damage. Brain and Cognition, 3: 370-384, 1984.HARRINGTON, D.L., and HAALAND , K.Y. Representations of actions in ideomotor limb apraxia: Clues
from motor programming and control. In L.G. Rothi and K.M. Heilman (Eds.), Apraxia: TheNeuropsychology of Action. East Sussex, UK: Psychology Press, 1997, Ch. 9, pp. 111-147.
HARRINGTON, D.L., HAALAND , K.Y., and KNIGHT, R.T. Cortical networks underlying mechanisms of timeperception. The Journal of Neuroscience, 18: 1085-1095, 1998.
HEILMAN , K.M. Apraxia. In K.M. Heilman and E. Valenstein (Eds.), Clinical Neuropsychology. NewYork: North Holland, 1979.
HEILMAN , K.M., MAHER, L.H., GREENWALD, L., and ROTHI, L.J.G. Conceptual apraxia from lateralizedlesions. Neurology, 32, A: 266, 1995.
HEILMAN , K.M., and ROTHI, L.J. Apraxia. In K.M. Heilman and E. Valenstein (Eds.), ClinicalNeuropsychology. New York: Oxford University Press, 1985, pp. 131-150.
HEILMAN , K.M., and ROTHI, L.J.G. In K.M. Heilman and E. Valenstein (Eds.), Clinical Neuropsychology(3rd edition). New York: North Holland, 1993, Ch. 7, pp. 141-163.
HEILMAN , K.M., ROTHI, L.J.G., and VALENSTEIN, E. Two forms of ideomotor apraxia. Neurology, 32:342-346, 1982.
JUEPTNER, I.H., RIJNTES, M., WEILLER, C., FAISS, J.H., TIMMANN , D., MUELLER, S.P., and DIENER, H.C.Localization of a cerebellar timing process using PET. Neurology, 45: 1540-1545, 1995.
KAPLAN, E. Gestural representation of implement usage: An organismic-development study. Doctoraldissertation. Ann Arbor, MI: University Microfilms International, 1968.
KERTESZ, A., FERRO, J.U., and SHEWAN, C.M. Apraxia and aphasia: The functional anatomical basis fortheir dissociation. Neurology, 34: 40-47, 1984.
KERTESZ, A., and HOOPER, P. Praxis and language: The extent and variety of apraxia in aphasia.Neuropsychologia, 20: 275-286, 1982.
KIMURA, D., and ARCHIBALD, Y. Motor functions of the left hemisphere. Brain, 97: 337-350, 1974.LIEPMANN, H. Die linke Hemisphare und das Handeln. Muenchner Medizinische Wochenschrift, 49:
2322-2326, 2375-2378, 1905.LIEPMANN, H. Drei Aufsatze aus dem Apraxiegebiet. Berlin: Karger, 1908.LIEPMANN, H. Apraxie. Ergebnisse der Gesamten Medizin, 1: 516-543, 1920.MAHER, L.M., ROTHI, L.J.G., and HEILMAN , K.M. Praxis performance with left versus right hemisphere
lesions. Neurorehabilitation, 9: 45-47, 1997.MAQUET, P., LEJEUNE, H., POUTHAS, V., BONNET, M., CASINI, L., MACAR, F., TIMSIT-BERTHIER, M.,
VIDAL , F., FERRARA, A., DEGUELDRE, C., QUAGLIA , L., DELFIORE, G., LUXEN, A., WOODS, R.,MAZZIOTTA, J.C., and COMAR, D. Brain activation induced by estimation of duration: A PET study.Neuroimage, 3: 119-126, 1996.
MEADOR, K.J., LORING, D.W., LEE, K., HUGHES, M., LEE, G., NICHOLS, M., and HEILMAN , K.M. Cerebrallateralization: Relationship of language and ideomotor praxis. Neurology, 53: 2028-2031, 1999.
MCDONALD, S., TATE, R.L., and RIGBY, J. Error types in ideomotor apraxia: A qualitative analysis. Brainand Cognition, 25: 250-270, 1994.
MOLL, J., DE OLIVEIRA -SOUZA, R., PASSMAN, L.J., CIMINI CUNHA, SOUZA-LIMA , F., and ANDREIUOLO,P.A. Functional MRI correlates of real and imagined tool-use pantomimes. Neurology, 54: 1331-1336, 2000.
MOZAZ, M., MARTI, J.F., CARRERA, E., and PUENTE, E.D. Apraxia in a patient with lesion located in rightsub-cortical area. Analysis of errors. Cortex, 26: 651-655, 1990.
PAPAGNO, C., DELLA SALA , S., and BASSO, A. Ideomotor apraxia without aphasia and aphasia withoutapraxia: The anatomical support for a double dissociation. Journal of Neurology, Neurosurgery, andPsychiatry, 56: 286-289, 1993.
228 Brenda Hanna-Pladdy and Others
POIZNER, H., MACK, L., VERFAELLIE, M., ROTHI, L.J.G., and HEILMAN , K.M. Three dimensional computergraphic analysis of apraxia. Brain, 113: 85-101, 1990.
RAADE, A.S., ROTHI, L.J.G., and HEILMAN , K.M. The relationship between buccofacial and limb apraxia.Brain and Cognition, 16: 130-146, 1991.
RAO, S.M., HARRINGTON, D.L., HAALAND , K.Y., BOBHOLZ, J.A., COX, R.W., and BINDER, J.R. Distributedneural systems underlying the timing of movements. Journal of Neuroscience, 17: 5528-5535, 1997.
RAPCSAK, S.Z., OCHIPA, C., BEESON, P.M., and RUBENS, A.B. Praxis and the right hemisphere. Brain andCognition, 23: 181-202, 1993.
RAPCSAK, S.Z., ROTHI, L.J.G., and HEILMAN , K. Apraxia in a patient with atypical cerebral dominance.Brain and Cognition, 6: 450-463, 1987.
ROLAND, P.E., SKINHOJ, E., and LASSEN, A. Focal activations of human cerebral cortex during auditorydiscrimination. Journal of Neurophysiology, 45: 1139-1151, 1981.
ROTHI, L.J.G., and HEILMAN , K.M. Liepmann: A definition of apraxia and a model of praxis, 1900 and1905. In C. Code, C-W. Wallesch, A.R. Lecours and Y. Joanette (Eds.), Classic Cases inNeuropsychology. Hove, East Sussex: Psychology Press, 1996, pp. 111-122.
ROTHI, L.J.G., MACK, L., VERFAELLIE, M., BROWN, P., and HEILMAN , K.M. Ideomotor apraxia: Errorpattern analysis. Aphasiology, 2 (3/4): 381-388, 1988.
ROTHI, L.J.G., OCHIPA, C., and HEILMAN , K.M. A cognitive neuropsychological model of limb praxis.Cognitive Neuropsychology, 8: 443-458, 1991.
ROY, E. (Ed.). Neuropsychological Studies of Apraxia and Related Disorders. New York: ElsevierScience, 1985.
ROY, E.A., SQUARE-STORER, P., HOGG, S., and ADAMS, S. Analysis of task demands in apraxia.International Journal of Neuroscience,56: 177-186, 1991.
SELEMON, L.D., and GOLDMAN-RAKIC, P.S. Common cortical and subcortical targets of the dorsolateralprefrontal and posterior parietal cortices in the rhesus monkey: Evidence for a distributed neuralnetwork subserving spatially guided behavior. Journal of Neuroscience, 8: 4049-4068, 1988.
Brenda Hanna-Pladdy, Ph.D., Department of Neurology, University of Florida Health Science Center, 100 South Newell Drive RoomL3-100 Box 100236 UFBI, Gainesville, Florida, 32610-0236. E-mail: [email protected]
(Received 25 July 2000, reviewed 11 September 2000, revised 3 October 2000; accepted 8November 2000)
APPENDIX
Types of Errors (Rothi et al., 1988)
I. Content
P = perseverative – the subject produces a response that includes all or part of apreviously produced pantomime.
RC = related content – the pantomime is an accurately produced pantomime associatedin content to the target. For example, the subject might pantomime playing a trombone fora target of a bugle.
NC = non-related content – the pantomime is an accurately produced pantomime notassociated in content to the target. For example, the subject might pantomime playing atrombone for a target of shaving.
II. Temporal
S = sequence – some pantomimes require multiple positioning that are performed in acharacteristic sequence. Sequencing errors involve any perturbation of this sequenceincluding addition, deletion, or transposition of movement elements as long as the overallmovement structure remains recognizable.
T = time – this error reflects any alterations from the typical timing or speed of apantomime and may include abnormally increased, decreased, or irregular rate ofproduction.
O = occurrence – pantomimes may involve either single (i.e. unlocking a door with a
Praxis errors and lateralization 229
key) or repetitive (i.e. screwing in a screw with a screwdriver) movement cycles. This errortype reflects any multiplication of single cycles or reduction of a repetitive cycle to singleevent.
III. Spatial
A = amplitude – any amplification, reduction, or irregularity of the characteristicamplitude of a target pantomime.
IC = internal configuration – when pantomiming, the fingers and hand must be in aspecific spatial relation to one another to reflect recognition and respect for the imaginedtool. This error type reflects any abnormality of the required finger/hand posture and itsrelationship to the target tool. For example, when asked to pretend to brush teeth, thesubject’s hand may close tightly into a fist with no space allowed for the imaginedtoothbrush handle.
BPT = body-part-as tool – the subject uses his/her finger, hand, or arm as the imaginedtool of the pantomime. For example, when asked to smoke a cigarette, the subject mightpuff on his index finger.
ECO = external configuration orientation – when pantomiming, the fingers/hand/armand the imagined tool must be in a specific relationship the ‘object’ receiving the action.Errors of this type involve difficulties orienting to the ‘object’ or in placing the ‘object’ inspace. For example, the subject might pantomime brushing teeth by holding his hand nextto his mouth without reflecting the distance necessary to accommodate an imaginedtoothbrush. Another example would be when asked to hammer a nail, the subject mighthammer in differing location in space reflecting difficulty placing the imagined nail in astable orientation.
M = movement – when acting on an object with a tool, a movement characteristic ofthe action and necessary to accomplishing the goal is required. Any disturbance of thecharacteristic movement reflects a movement error. For example, a subject, when asked topantomime using a screwdriver, may orient the imagined screwdriver correctly to theimagined screw but instead of stabilizing the shoulder and wrist and twisting at the elbow,the subject stabilizes the elbow and twists at the wrist or shoulder.
IV. Other
NR = no responseUR = unrecognizable response – a response that is not recognizable and shares no
temporal or spatial features of the target.
230 Brenda Hanna-Pladdy and Others