Embed Size (px)
Citation preview

Pragmatism in a Time of Polarization?:
Implementing Health Insurance Marketplaces in the States
Simon F. Haeder
Doctoral Student
Department of Political Science
University of Wisconsin-Madison
Abstract
The Affordable Care Act (ACA) has been one of the centerpieces of the Obama Administration’s
domestic policy agenda. Yet Republicans opposition has shown little subsiding even three years
after its enactment. Do standard accounts of Republican opposition actually square with reality?
Looking beyond the rhetoric and taking a more nuanced approach to analyzing the
implementation of insurance marketplaces, this paper shows that while Republicans in the states
are less eager than their Democratic counterparts to implement the ACA, they have nonetheless
made considerable headway in pragmatically participating in the shared governance of insurance
marketplaces. It appears as if even the staunchest opponents of the ACA remain eager to defend
long-time state prerogatives when it comes to the regulation of insurance.

Page 1 of 40
Introduction
The Affordable Care Act (ACA) has been one of the centerpieces of the Obama
Administration’s domestic policy agenda (see for example, Altman and Shactman 2011; Haeder
2012; Jacobs and Skocpol 2010, 2011; McDonough 2011; Starr 2011; The Staff of the
Washington Post 2010; Brennan and Studdert 2010). Implementation is a key component of
every policy initiative but the design of the ACA relies extensively on state and private partners
to cooperate with the national government over extensive periods of time (see Greer 2011; Kersh
2011; Miller 2010; Miller 2011; Skocpol 2010; Nichols 2010; Weil and Scheppach 2010;
Brennan and Studdert 2010). However, few pieces of legislation have proven as controversial
even after legislative passage, and doubts linger if the ACA could go the way of the ill-fated
Medicare Catastrophic Coverage Act of 1988 (Himelfarb 1995). Despite a Supreme Court
verdict and a presidential election, Republicans in Congress and across the states have, by and
large, shown few signs of accommodation even three years after the president’s signature,
particular with regard to the establishment of insurance marketplaces (Haeder and Weimer
2013b; Rigby and Haselswerdt 2013a). 1 Newspaper accounts are filled with stories of
grandstanding opposition to the various components of the ACA. Just recently, the U.S. House of
Representatives voted for the 46th
time to repeal or dismantle the ACA (Kapur 2013). Clearly,
the implementation of the ACA has confirmed that “the fight over policies does not end with the
presidential signature on a bill” (Haeder 2012, 66).
This essay seeks to answer two important sets of questions about the implementation of
insurance marketplaces. First, who is participating in the implementation of insurance
marketplaces? Specifically, are Republicans merely sitting on the sidelines, or worse, doing
1 The original terminology used by the Affordable Care Act is “health insurance exchanges.” However, in January
2013, citing concerns for non-English speakers, the Obama administration officially decided to rebrand the
exchanges as “health insurance marketplaces.” I use the new terminology in this paper.

Page 2 of 40
everything they can to impede implementation? Is implementation solely left to Democrats as a
result? Second, if Republicans are actively attempting to participate in the implementation of
marketplaces, how do they contribute and to what extent? And perhaps even more importantly,
how successful are they in influencing the implementation of marketplaces?
To answer these questions, I proceed as follows. First, I provide a brief review of the
implementation of shared governance programs like the ACA, with a particular focus on partial
pre-emption, and the conflicts during the process. Second, I illustrate the role states were
envisioned to play in the shared governance of insurance marketplaces. Third, I answer the
question, whether Republicans are participating in the implementation of insurance
marketplaces, and if so, how successful they are utilizing a variety of hierarchical models.
Finally, I conclude and provide a brief outlook for the future of the insurance marketplaces.
Looking beyond the rhetoric, this paper shows that while Republicans in the states are less eager
than their Democratic counterparts to implement the ACA, they have nonetheless made
considerable headway in pragmatically participating in the shared governance of insurance
marketplaces, particularly when it comes to lower profile issues. It appears as if even the
staunchest opponents remain eager to defend long-time state prerogatives when it comes to the
regulation of insurance.
Shared Governance Programs
Shared Governance and American Federalism
The debate about shared governance has long roots in the American and English
constitutional history (Beer 1993). This normative debate pits two opposing views of the
American federal system against each other. One the one side a strict dualists like David Walker
(1995) and Edward Corwin (1950) who are strongly opposed to federal interferences into states’

Page 3 of 40
affairs. They are supported, for instance, by those who worry about reduced competition
(Tiebout 1956), distortion of voter preferences (Tullock et al. 2002), government failure
(McKinnon and Nechyba 1997), the flypaper effect (Romer and Rosenthal 1980; Courant et al.
1979), a lack of accountability (Rivlin 1992, 2012), and potential fiscal defaults (Rodden 2006).
The opposing side is best exemplified by Morton Grodzins (1966) and Daniel Elazar (1962,
1984) and their partnership model, as well as scholars of fiscal federalism (Musgrave 1959,
1971; Oates 1972) and those worried about effects on equity and equality (Derthick 1970), a race
to the bottom (Cary 1974; Bailey and Rom 2004), and implications for democracy and
citizenship (Mettler 1998). Yet despite the vivid normative debate, the federal government and
the states have long shared in the governance for a wide variety of purposes (Clark 1938;
Bittermann 1938) including the state militia (Riker 1957) and a long list of healthcare programs
(Haeder and Weimer 2013a). However, a general increase in the polarization of American
politics (McCarty et al. 2006; McCarty 2007; Theriault 2008) has certainly revitalized the
debate.
Partial Preemption under Shared Governance Healthcare Program
A common form of shared governance between the federal government and the states can
be found in partial pre-emption (Crotty 1987; Hedge and Scicchitano 1994; Scicchitano and
Hedge 1993; Zimmerman 2007). Partial pre-emption is defined as “federal laws establishing
minimum national regulatory standards under which administrative responsibilities may be
delegated to states or localities provided they meet certain federal criteria” (Conlan 1991, 51).
Partial pre-emption, as utilized by the Obama Administration, can be considered as a form of
one-tail devolution, i.e. grants states significant opportunities for innovation and choice to
advance a more progressive agenda exceeding the national floor (Conlan and Posner 2011).

Page 4 of 40
While not without its problems, partial pre-emption is often considered a less controversial and
coercive approach compared to, for example outright mandates, restraints or total preemption
(Zimmerman 2001). At least in theory, “ partial preemption seemed to satisfy everybody; it
would achieve national regulatory goals and assuage those concerned about the intrusion of the
federal government into state affairs” (Scicchitano and Hedge 1993, 108).
Partial pre-emption is not a new development with regard to healthcare. One of the
earliest examples is the Federal Emergency Relief Administration (FERA) (Greenfield 1958).
Services covered under FERA were extensive, including physician care, emergency dental
services, bedside nursing, prescription drugs, and emergency appliances and the program “set a
precedent for increased participation of state and federal governments in financing medical care
for the needy” (Greenfield 1958, 25). FERA (and subsequent programs like the Civil Works
Administration (CWA) and the Works Progress Administration (WPA)) appear as a significant
break from past grant programs due to the relatively vast powers assigned to the federal
government in the form of “federal assumption” (Macmahon et al. 1941/1971; Williams and
Williams 1940). Whereas prior to FERA federal administrators had to rely solely on the
withdrawing of grant funding, the federal government now could choose to take over
administration of a program in case states were in non-compliance with grant requirements
(Maxwell 1946).2
More recently, partial pre-emption has occurred under the Health Insurance Portability
and Accountability Act of 1996 (HIPAA) and the Health Coverage Tax Credit (HCTC)
established under the Trade Act of 2002. While HIPAA is most widely known for its regulation
of medical record privacy and the partial pre-emption of state medical privacy laws (Ko 2005), it
2 Assumption occurred in Illinois, Kentucky, Oklahoma, North Dakota, Maine, Massachusetts, Ohio, Louisiana, and
Georgia (Clark 1938, 250-3). Moreover, several other states entered into a partnership with the federal government
(Clark 1938, 258).
Page 5 of 40
also established certain insurance portability requirements with regard to transitions from group
to individual coverage (Ladenheim 1997; Chaikind et al. 2005). HIPAA offered states a variety
of compliance options including the creation of qualified high-risk pools. At the same time,
HIPAA created a federal fallback option in case of non-compliance (Atchinson and Fox 1997;
Ladenheim 1997; Pollitz et al. 2000b). While many states chose to implement their preferred
program, various states failed to do so, forcing the federal government to administer programs in
nine states in 1998 and ten stats in 2005 (Chaikind et al. 2005; Fuchs et al. 1998).
Similarly, the HCTC provides tax credits to certain individuals that amount to 65 percent
of premium costs (Dorn and Kutyla 2004). The Trade Act, in addition to establishing fast-track
authority for trade agreements, established ten tax-credit eligible types of insurance plans, three
of which did not require any state action (Stone-Axelrad and Lyke 2005). State implementation
has been uneven and as a result solely federal options were available in 24 states in 2003 and 21
stats in 2005 (Stone-Axelrad and Lyke 2005). Arguably the increasing use of the 1915c and 1115
Medicaid State Waiver Program (Thompson 2012; Thompson and Burke 2009) could also be
considered a form of partial pre-emption with the traditional Medicaid program as the fallback
options.
Conflict in Recent Shared Governance Programs
Before moving on to a discussion of the implementation of insurance marketplaces, it is
worthwhile emphasizing that state opposition to federal programs has not been confined to the
Obama Administration or healthcare programs. Instead, research has described such opposition
with regard to the REAL ID Act (Regan and Deering 2009), No Child Left Behind (Loveless
2007; Shelly 2008), abstinence only programs (Doan and McFarlane 2012), various
environmental programs since the 1990s (Scheberle 2004), and OSHA (Thompson 1983). This is
Page 6 of 40
in addition to high-speed rail, the American Recovery and Reinvestment Act of 2009 and the
Race to the Top program under the Obama Administration (Nicholson-Crotty 2012).
The Role of States under the ACA in Setting up Health Insurance Marketplaces
Intended to provide coverage to millions of individuals, marketplaces are in many
respects the linchpin of ACA implementation. States have been tasked with a significant role in
this process and the ACA relies extensively on their cooperation for their shared governance. It is
not surprising that the ACA followed this precedent given the long tradition of shared
governance and partial pre-emption, particularly in the healthcare field, described above.
However, the establishment of health insurance marketplaces has been challenging as, with the
exception of Massachusetts and, to a very limited degree, Utah, marketplaces are new and hence
largely untested. As a result, many organizational questions remain to be answered and states
have little experience to rely upon in this process (Weil and Scheppach 2010).
Haeder and Weimer (2013b) provide an extensive treatment of the role of states in the
implementation of insurance marketplaces as they emphasize the extent of shared governance
envisioned under the ACA. Specifically, states are granted significant leeway in the
establishment of marketplaces with regard to governance and administrative structure, regulatory
power over the insurance market, financing mechanisms, and benefit structure. Most
importantly, the ACA offers states the opportunity to choose between a purely state-based
marketplace without any federal involvement at one end of the continuum, and a fully federal
marketplace without any state involvement at the other hand. Although not originally contained
in the ACA, federal regulations have also created an implicit compromise between these two
extremes in the form of Partnership Exchanges in which states and the federal government
essentially share in the regulation and administration of the various components of the

Page 7 of 40
marketplaces (Haeder and Weimer 2013b). While “HHS, by law, retains authority over each
FFE” (Center for Consumer Information and Insurance Oversight 2012, 6), the notion of a
partnership offers a variety of avenues for cooperation between the different levels of
government.
Overall, the relationship envisioned under the ACA in general, and the creation of
insurance marketplaces in particular, is thus one of shared governance in which the federal
government serves as a partner, providing funding and expertise while establishing a federal
floor. While the degree of state leeway can be debated, the ACA certainly grants states
significant opportunities for innovation and (Conlan and Posner 2011).
A Tale of Two Reponses: Creating vs. Regulating Marketplaces
Opposition to marketplaces has become a key issue for Republicans eager to verify their
anti-Obama credentials (Erickson 2012; Knickerbocker 2012). Sean Nicholson-Crotty has
described similar behavior for a variety of grant programs and differentiates between high-profile
issues, which are inherently partisan, and lower profile issues, which illicit much more pragmatic
responses (Nicholson-Crotty 2012). Nicholson-Crotty’s differentiation between high- and low-
profile responses provides the theoretical foundation for this research. Specifically, I expect state
responses to differ significantly in their response to the implementation of insurance
marketplaces with regard to (1) the establishment of marketplaces and (2) the regulation of
marketplaces. Given the strong opposition to the ACA, particularly by conservative voters,3 open
opposition the creation of insurance marketplaces seems a prudent political calculation for
Republican legislators. However, I argue that states, while being openly hostile with regard to
high-profile issues such as the actual creation of marketplaces, may very well be much more
3 The Kaiser Health Tracking Poll by the The Henry J. Kaiser Family Foundation provides more detailed insights. It
is available at http://kff.org/interactive/health-tracking-poll-exploring-the-publics-views-on-the-affordable-care-act-
aca/.

Page 8 of 40
cooperative on lower profile issues such as the regulation of marketplaces, i.e. the technical
implementation of their various components. As a result, and in direct opposition to assertions of
wide-spread state defiance, states may be much more cooperative and involved in the
establishment of marketplaces than commonly believed for a variety of reasons.
Traditionally, state legislators of all parties have been eager to retain regulatory control of
their insurance markets. While the insurance industry, particularly in the healthcare field, is one
of the most heavily regulated industries in the United States, the regulation of insurance has
traditionally been the domain of the states (see Klein 2009; Field 2007; McCray 1993; Teske
2004; Gerber and Teske 2002; Gormley 1983; Berry 1984; Meier 1988, 1991). State primacy
was confirmed by the Supreme Court decision in Paul v. Virginia in 1869 which directly limited
federal regulatory efforts until its reversal in U.S. v. South-Eastern Underwriters Association in
1944 (McCray 1993). However, states were able to limit federal intrusion by lobbying Congress
to pass the McCarran-Ferguson Act of 1945 (Pub.L. 79−15) which reestablished state primacy
by statute. Nonetheless, recent increases in state regulation have been accompanied by extensive
federal regulations (see Pollitz et al. 2000a; Meier 1988) most prominently in the form of the
Employee Retirement Income Security Act (ERISA) of 1974 (Pub.L. 93–406), the Consolidated
Omnibus Budget Reconciliation Act (COBRA) of 1985 (Pub.L. 99–272), and the Health
Insurance Portability and Accountability Act (HIPAA) of 1996 (Pub.L. 104–191). The federal
government also indirectly regulates insurance through several benefits programs including the
Federal Employee Health Benefits Program (FEHBP), as well as Medicare, Medicaid, and
TRICARE. Despite this interference states, often against the preferences of insurers, have
eagerly guarded their regulatory powers (see Klein 2009; Field 2007; McCray 1993).
Page 9 of 40
In addition, democratic legislators throughout the country have a particular incentive to
assure that the implementation of insurance marketplaces progresses safely. Perhaps no other
piece of the legislation is as strongly identified with the Democratic Party as the ACA.
Democrats, whether they like it or not, own the ACA and will be held accountable for its
implementation, especially for its potential shortcomings. As a result, we would expect
significant implementation activities by Democratic legislatures. At the same time, Republican
legislators also have an incentive to participate in the regulation of insurance marketplaces, albeit
not equally as strong, given the alternative policy outcome: direct regulation by the federal
Department of Health and Human Services, i.e. the decidedly more liberal Obama
Administration (Haeder and Weimer 2013b). While it may be political expedient to openly
oppose the creation of the marketplaces, it appears futile to surrender all regulatory power as
well, given the inevitability of the establishment of marketplaces. As a result, Republican
legislators may very well participate in the regulation of insurance marketplaces, albeit in the
less visible manner hypothesized above.
Additionally, Republican legislators have an additional incentive to participate in the
regulation of insurance marketplaces in states with Democratic governors. Here Republican
legislators may seek to limit the independent implementation activities undertaken by the
executive. Without statutory guidance, Democratic governors are relatively free to cooperate
with the Obama Administration in the implementation of the marketplaces, again leading to
much more liberal outcomes than preferred to be Republican legislators. Only statutory guidance
offers the possibility of exerting any kinds of influence. Again, Republican participation appears
rather plausible on lower profile issues. Finally, states with unified Republican control may seek
to distinctively shape implementation and create the most conservative marketplace possible.

Page 10 of 40
Establishing Insurance Marketplaces: A High-Profile Issue
Very little empirical research has been conducted evaluating the implementation of health
insurance marketplaces.4 Nonetheless, two recent articles provide an initial analysis of the
developments (Rigby and Haselswerdt 2013b; Haeder and Weimer 2013b).5 However, both
analyses are very much focused on the relatively blunt question of whether states established
insurance marketplaces, i.e. the high-profile component of establishing insurance marketplaces.
Nonetheless, the articles show that, mostly driven by partisanship, state responses to the ACA
have varied significantly, ranging from enthusiastic support to outright hostility (Figure 1): given
a few outliers, strongly Democratic states have created insurance marketplaces while strongly
Republican states have failed to do so (Haeder and Weimer 2013b; Haeder 2013; Rigby and
Haselswerdt 2013a). Paradoxically, the implementation of insurance marketplaces appears to
have turned into a particularly maligned component of the ACA. This is surprising because
conservative reform plans have long advocated the establishment of such marketplaces in order
to improve the provision of private insurance products by alleviating information asymmetries
and facilitating consumer choice. (Haislmaier 2006; Haislmaier and Owcharenko 2006).
Moreover, the individual mandate is clearly based on the concept of personal responsibility.
Nonetheless, opposition to the creation of marketplaces has become a key issue for Republicans
4 However, there is no dearth of material released by various foundations, legal scholars, and think tanks offering a
wide variety of suggestions and advice for implementers yet providing no empirical assessment (Bachrach and
Boozang 2011; Blumberg 2011; Carey 2010; Corlette and Volk 2011; Gardiner and Perera 2011; Health Access
2010; Jost 2010; Lischko 2007; Wicks 2009). 5 Rigby and Haselswerdt (2013b) use elapsed-time conditional risk set models to assess the states’ progress in
establishing marketplaces. The authors find that public support, a Democratic governor, and Democratic seat share
in the legislature are positively related to progress whereas elected Republican insurance commissioners, resident
age and income are negatively related.5 They also provide a qualitative evaluation of 5 outlier states. Haeder and
Weimer (2013b) provide a very detailed and more nuanced overview of state activities with regard to the
implementation of insurance marketplace summarized under five distinct themes. They also illustrate the vast
differences in state responses. Further, they find empirical evidence that the probability of establishing a
marketplace is positively related to capacity of the insurance department as well as unified Democratic control of
state government

Page 11 of 40
thus making any outright cooperation, or mere appearance thereof, by Republicans a political
liability.
Regulating Insurance Marketplaces: A Low-Profile Issue
Analyzing the creation of insurance marketplaces, however, does not fully capture the
extent of states responses. Similarly to Haeder and Weimer (2013b) who also emphasize the less
visible activities states have undertaken, including upgrades to Medicaid eligibility systems, the
role of insurance commissioners, and foundation grants, states have been very active in
regulating the various components of the newly-created insurance exchanges. Descriptive
statistics do much to dispel the notion that insurance marketplaces have been exclusively the
domain of Democrats. Overall, 551 distinct bills were introduced from January 2011 through
May 2013: 215 in 2011 (39 percent), 128 in 2012 (23 percent), and 217 in the first 5 months of
2013 (38 percent). Bills were introduced in all states except Delaware. The number of bills
introduced is slightly skewed toward Democratic authors who introduced 292 bills (107/79/106)
compared to 238 bills (101/44/93) introduced by Republicans (Figure 1). The remainder was
introduced by non-partisan (Nebraska), independent, or bipartisan sponsors. Introductions are not
stable across time and there appears to be a significant dip in the presidential election year and
acceleration in 2013.6 About 55 percent of the bills were introduced in the lower chamber. This
pattern holds across all three years.
[Figure 1 about here]
Moreover, the 431 bills implementing the ACA (506 if counting abortion-related bills)
vastly outnumber those in opposition (51). Bills implementing the ACA numbered 152 in 2011,
6 Note that only bills up to May of 2013 are included here.

Page 12 of 40
105 in 2012, and 174 in 2013. Not surprisingly virtually all Democratic bills were supportive of
the ACA. All of the independent and bipartisan bills were in support as was a majority of the
non-partisan bills. Strikingly, also a majority (56 percent or 83 percent if counting abortion-
related bills) of Republican bills moved to implement the ACA. However, of the 51 bills that
clearly opposed implementation of the ACA, 47 were sponsored by Republican members.
Finally, the incredibly small number of bipartisan bills deserves to be noted (0.9 percent).
Clearly, the ACA is a highly partisan issue and the parties have found little room for
compromise.
The most active states were California (36 bills), Illinois (25), Minnesota (25), Oregon
(23), Michigan (23), and New Mexico (23). Interestingly, neither Illinois not Michigan actually
established a marketplace and New Mexico only did so very recently. Thus even in states with
federal marketplaces, states are seeking to continue their regulatory role.7 However, 8 of the bills
in Michigan can be classified as seeking to prevent the implementation of the ACA.
Interestingly, Michigan is a significant outlier as the next highest number of opposition bills is 5
in Minnesota. All 36 bills in California moved to implement the ACA followed by Oregon (21),
Minnesota (20), Vermont (19) and Connecticut (19). The least active states are Delaware (0),
Alaska (1), Massachusetts (2), Oklahoma (3), and South Dakota (3). However, in all four of the
latter states at least one bill was introduced that was in support of the ACA. Finally, I note that
various states strongly opposing marketplaces like Texas (20 total, 13 implementing), Florida (9,
5), and Louisiana (5, 5) were nonetheless not completely inactive.
Looking at outcomes, I note that 288 bills (215 in support) did not move beyond the
introduction stage whereas another 90 (73) gained at least support from one committee and
7 For example, Ohio and South Dakota retained control over health plan management and Virginia will continue to
license and certify health plans in the marketplace (Haeder and Weimer 2013b)

Page 13 of 40
another 33 (25) were passed in one chamber. An additional 22 bills (19) then gained additional
support from at least one legislative committee in the non-originating chamber, and another 18
(15) passed both chambers but were not enacted either due to a veto or failure to agree on a
conference report. Finally, 100 bills (83) were enacted into law. Looking at party success we find
that about 18 percent of both Democratic and Republican bills were enacted while a majority
failed to move beyond the introduction stage.
Two specific bill topics stand out. Of the 551 bills, 76 bills deal with abortion and another
33 bills deal with marketplace navigators. The vast majority of abortion-related bills were
introduced by Republicans (64) and only 9 were introduced by Democrats. However, in a
majority of states no bills addressing the coverage of abortion were introduced. Again, Michigan
is an outlier with 11 abortion-related bills introduced. However, navigator bills are slightly more
likely to be introduced by Democrats than Republicans. Only 14 of the abortion bills and 6 of the
navigator bills have been enacted. In both cases, the vast majority of bills did not even gain
committee support. As most of the abortion bills were introduced by Republican sponsors, it
appears as if Republican tried to make a statement during the implementation process that could
gain the support of their constituencies, particularly Tea Party activists and social conservatives.
Later in the process, as the implementation of the ACA became more and more inevitable, both
Republicans and Democrats sought to be more pragmatic by participating in the implementation
generally, and to accommodate interest group pressure by addressing the issue navigators in
particular.
Finally, it is worth examining the role of the Supreme Court decision as well as the 2012
presidential election. Interestingly, between the Supreme Court affirmation of the ACA and the

Page 14 of 40
election, only a single bill was introduced in the entire country.8 It appears as if the decision was
made to hold out for the outcome of the presidential election before moving forward. Overall,
346 of the bills were introduced in the time prior to the election compared to 205 bills in the 7
months after the election. The ratio between Democratic and Republican bills has stayed largely
the same. However, 84 percent of abortion-related bills and only one third of navigator bills were
introduced prior to the election. Clearly, with increasing institutionalization, the persistence of
the ACA has become more and more settled. It appears as if Republicans in the states have
settled on the dual strategy of rhetorical opposition while pragmatically sharing in the
governance of the program.
Taking a Closer Look at State Regulation of Insurance Marketplaces
The preceding section established that both Republican and Democratic state legislatures
have been active on the lower profile issue of regulating insurance marketplaces. At the same
time, Republicans have been much more reserved in terms of the higher profile issue of creating
insurance exchanges. A more nuanced treatment offers an opportunity to more adequately
evaluate state responses. Data for the following section were obtained from a variety of sources.
First, information regarding the bills and their outcomes was obtained from the Federal Health
Reform State Legislative Tracking Database, which is maintained by the National Conference of
State Legislatures and covers the period from January 2011 through May 2013. This website
provides information about key variables including the author, the topic, the legislative history,
and a summary of the bill. The summary of the bill was used to code whether a bill was in
support9 or in opposition
10 to the implementation of the ACA. The coding decision was
8 The bill was introduced in New Jersey as NJ A 3186.
9 For example CO H 1245 is summarized as “Concerns funding mechanisms for the Colorado health benefit
exchange. On and after January 1, 2014, in order to fund the Colorado health benefit exchange, the bill allows: The
health benefit exchange board of directors to assess against small group and individual health insurers in an amount

Page 15 of 40
straightforward except in a handful of cases. For these, reading the bill in question made the
coding decision obvious.11
Moreover, I coded whether a bill dealt with abortions12
and whether a
bill dealt with the role of navigators and brokers13
in the marketplace. Additionally, I obtained
information about the partisan balances of the various chambers as well as the party of the
governor from The Book of States published by The Council of State Governments. Nebraska has
a non-partisan, unicameral legislature and is thus only included in the section on descriptive
statistics and omitted from all other estimations. Finally, information about the establishment of
insurance marketplaces was obtained from two recent articles published on the subject (Rigby
and Haselswerdt 2013b; Haeder and Weimer 2013b).
Hierarchical Poisson Models: Introduction of Bills
In order to assess the introduction of bills empirically and to decipher differences based
on party affiliation, I resort to multi-level analysis.14
“Multilevel analysis is a methodology for
the analysis of data with complex patterns of variability, with a focus on nested sources of
variability” (Snijders and Bosker 1999). These models are generalizations of various linear and
non-linear models that take account of the clustering or nesting of observations and treat the
underlying dependence not as a nuisance but rather as “an interesting phenomenon” (Snijders
necessary to provide for the sustainability of the exchange, and a credit against the tax imposed against insurance
companies.” 10
For example, TN S 666 is summarized as “Would prohibit, by state statute, health insurers doing business in the
state under insurance law from participating, selling or offering coverage in any American Health Benefit Exchange
or other exchange operated under the PPACA.” 11
In this sections, bills dealing with abortion issues were treated as neutral with regard to implementation. However,
it appears plausible to code the neutral bills as supportive because they move forward with implementation. As this
coding scheme is only used for descriptive statistics, I resorted to the more nuanced solution here and combine the
abortion-related bills and other bills in support in the following sections for estimation. 12
For example, IN S 116 is summarized as “Relates to abortion coverage by qualified health plans, prohibits
qualified health plans under the federal health care reform law from providing coverage for abortion.” 13
Navigators are individuals who support consumers in navigating through the insurance marketplace. Traditional
insurance brokers have actively sought to gain access to these marketplaces and to obtain compensation for their
activities. For example, 14
Other terms used include, for example, hierarchical linear models, nested models, mixed models, random
coefficient, random-effects models, random parameter models, or split-plot designs.

Page 16 of 40
and Bosker 1999, 7). The nesting structure in this case appears straightforward: bills are nested
within chambers, chambers within states, and states within years. Ignoring this multi-level
structure may have significant detrimental effect on estimates and inference (Snijders and Bosker
1999). In this case chambers are nested within states.15
Quite reasonably, bills introduced merely
to oppose the implementation of the ACA come from a different population than those
introduced to implement it. Hence, I only use the subsample of my data that contains bills that
implement the ACA.16
Given the nature of hierarchical models, a data-driven approach is often
recommended that begins with a simple model and then expands the model while accounting for
data constraints.17
Hence, I estimate a two-level hierarchical variance component model first
(Model 1).18
I also tested adding a third level for Years but the estimations were compromised as
they were asking too much of the data. Instead, I resorted to time fixed effects (Model 2). Next I
added various level-one covariates (Model 3) as well as a random slope for the Governor
variable (Model 4). The covariates include indicators for the Chamber (coded 1 for the
assembly), the Proportion of Republicans in the Chamber, and whether the Governor was a
15
Again, there were no bills introduced in Delaware; Nebraska is excluded for reasons stated above. The total
number of cases, i.e. chambers by year, in this case is 205. 16
Bills coded in opposition and excluded in the following include such summaries as “Would amend the Executive
Reorganization Implementation Act, by prohibiting an executive order of the governor from establishing or
providing for the administration or operation of a State-based health benefit exchange.” or “Would prohibit the state
and other entities from establishing, operating, or purchasing insurance from an American health benefit exchange
and would make such health insurance contracts void. Also would give an individual a tax credit if taxed under the
individual responsibility or coverage mandate of the PPACA, allows the Attorney General to bring an action against
a person or entity causing harm when implementing the PPACA.” 17
In all of the following models the multi-level structure was tested and compared to a single level structure. In
every case, the multi-level structure was strongly preferred. All models here were estimated with Stata/MP 12.1
(StataCorp 2011b). The command used was xtmepoisson. This is Stata’s command for mixed-effects models for
count responses containing both fixed and random effects. Fixed effects are interpreted similar to standard
regression coefficients but random effects are not directly estimated and variances are presented. As no closed form
of the log likelihood exists the model is estimated with adaptive Gaussian quadrature. The default number of
quadrature points is 7. For a detailed overview of the command see StataCorp (2011a).
18 In order to account for the potential non-normality of the random intercept √
the model is also estimated with
nonparametric maximum likelihood estimation (Model 1a). The results are largely similar. Nonparametric maximum
likelihood estimation assumes that the random intercept is distributed with discrete locations and probabilities. The
process is iterative as locations are added and assessed whether the likelihood is as large as possible. The process
stops when the maximum Gâteaux derivative is less than 0.00001.

Page 17 of 40
Republican. Next, I added a cross-level interaction between the Party of the Governor and the
Proportion of Republicans in the Chamber; first I estimated the model with a random intercept
only (Model 5) and then I added a random slope as well (Model 6).19
Finally, in order to account
for potential level-one over-dispersion and other model misspecifications I followed Rabe-
Hesketh and Skrondal (2012a,b) and estimated a robust model for the random intercept and the
random coefficient model (Models 5a and 6a).20
In both cases, the results are essentially similar.
Finally, I re-estimated Model 5 using nonparametric maximum likelihood estimation as
described earlier (Model 5b). A comparison of the predicted counts between the two versions
largely overlaps pointing to a good fit of the original model.21
All models were also estimated
with a larger number of integration points22
than the program default, in order to obtain more
precise estimates, and tested for various covariance structures. Likelihood ratio tests showed that
an unstructured variance was appropriate, i.e. all variances were distinctly estimated. Ultimately,
Model 5a was selected as the preferred model because it is parsimonious and coefficients are
essentially similar and relatively small.23
The fixed part of the model is rather consistent across specifications. The time fixed
effects (with 2011 as the base excluded) are negatively signed and statistically significant for
2012. The Chamber variable never reaches statistical significance. In the models without the
interactions, the proportion of Republicans is negatively signed and highly significant. However,
19
Other interactions were tested with likelihood ratio tests, as standard Wald tests are inappropriate, but did not
achieve significance. 20
For the robust models the gllamm command (Generalized Linear Latent and Mixed Models) was used as it is the
only command capable of estimating robust standard errors. For an overview of gllamm and its framework 21
The difference between the two has a mean of 2.53e-08 and a standard deviation of .397. More than 95 percent of
the difference in predicted counts is between -0.5 and 0.5. 22
This process is iterative. I began with a relatively low number of integration points to obtain a base set of
estimates and then used these as starting values in the next iteration with a higher number of integration point. The
process was repeated until estimates did not change further. 23
In addition to the most appropriate fit to theoretical considerations, I also conducted various tests to assess the
appropriateness of the model including residual analysis (deviance and Anscombe residuals). In addition, model
interpretation as described below was essentially similar.
Page 18 of 40
the models with the interactions appear most appropriate from a theoretical perspective. We
would expect the behavior of legislators to vary depending on the partisan balance in the
legislature as well as the party of the governor. Both strongly influence the probability of a bill
becoming law; the effect is conditional. Moreover, it seems plausible that legislators may be
particularly interested in curbing the power of governors by imposing statutory restrictions. The
case of New Mexico comes to mind where the Democratic legislature actively sought to rein in
the independent actions of a Republican governor. The opposite situation occurred in Kentucky.
Interactions in hierarchical count models pose challenges for interpretation. Hence, I only briefly
note that the party of the governor as well as its interaction with the proportion of the chamber
that is Republican are positively signed and significant in some of the specifications. Turning to
the random parts of the model, I note the relative stability across specifications.
[Table 1 about here]
A better illustration of the statistical results may be gained from a comparison of
predicted counts at various interesting values. 24
I used the predicted counts to extrapolate the
expected number of bills introduced nationwide including a 90 percent confidence interval and
present results for both chambers as there appear to be slight differences (Table 2). The
predictions are stratified by year.25
Several interesting patterns emerge. First, although not
24
i.e. the predicted mean of the Poisson distribution. The predicted mean is based both on the fixed and random
effects and is conditional on the random effects. For more details see StataCorp (2011a). For comparative purposes,
the observed data had a mean of 2.48, a median of 2.00, a standard deviation of 1.60, and included a total of 497
bills for all three years. 25
An illustrative example. The total for a Republican Governor and a Strongly Democratic Legislature in 2011 is
831 (599-1430) for the Senate and 895 (659-1544) for the assembly. This number is the total number of bills across
all states that we would expect to be introduced, given that there is a Republican governor with a strongly
Democratic legislature and the indicators for 2012 and 2013 switched off, i.e. the entire period of observation is
treated as if it were 2011 for all 29 months.

Page 19 of 40
statistically significant, in all predictions the number of bills dips in 2012 and bounces back in
2013. Second, by far the most bills are introduced in Democratic legislatures with both
Democratic and Republican governors. Obviously, Democrats are seeking to move their states
into compliance with the ACA. Often this occurs despite the opposition of Republican
governors. The cases of New Jersey and, again, New Mexico come to mind. However, given the
limitation of the data we cannot find statistically significant differences across governors. Third,
states with strong Republican legislatures introduce the lowest number of bills, particularly if the
Governor is a Democrat. We could imagine that little compromise between the two is possible
and Democrats may try to use executive tools to move implementation forward given Republican
opposition in the legislature. Results for Republican legislatures are clearly statistically different
from those for Democratic legislature and, at times, even from split legislatures. Fifth, split
assemblies frequently produce statistically fewer bills than Democratic ones. Finally, despite the
lower numbers, it should be noted that Republican-controlled legislatures are nonetheless
expected to produce a significant number of bills ranging from annual point estimates of 157 to
218 nationwide if all legislatures were Republican. This is the more remarkable given the strong
rhetorical opposition presented in newspaper accounts and the Internet. Apparently, pragmatism
and accommodation prevails in the long run, at least to a certain degree.
[Table 2 about here]
Hierarchical Ordered Probit Models: Progress of Bills
Bill introductions are certainly an interesting part of the story of insurance marketplaces.
So far we have shown that while Democrats generally are more likely to introduce bills to

Page 20 of 40
implement the ACA, Republicans nonetheless are actively participating. However, if
Republicans or Democrats are introducing bills merely as symbolic actions, the effect on the
implementation of the ACA will remain negligible. We need to learn something about the
progress of the bills and under what conditions they become law. To do so I coded the progress
of a bill as follows. If it was introduced in either chamber, it was coded as 1. If it then was voted
upon by at least one committee of the same chamber it received a 2; if it passed the chamber of
origin it received a 3. Once the bill moved to the other chamber, it received a 4 if it gained the
support of at least one committee, if it passed that chamber it received a 5. Finally, if it was
enacted into law, it received a 6. In order to take advantage of the ordering and to account for the
nested structure, a hierarchical ordered probit model is appropriate. In the OLS environment,
ordered probit models usually show very similar results to standard OLS regressions. The same
holds for hierarchical models. With multi-level models, this can help with obtaining adequate
starting values as well as with model building, diagnosis, and interpretation.
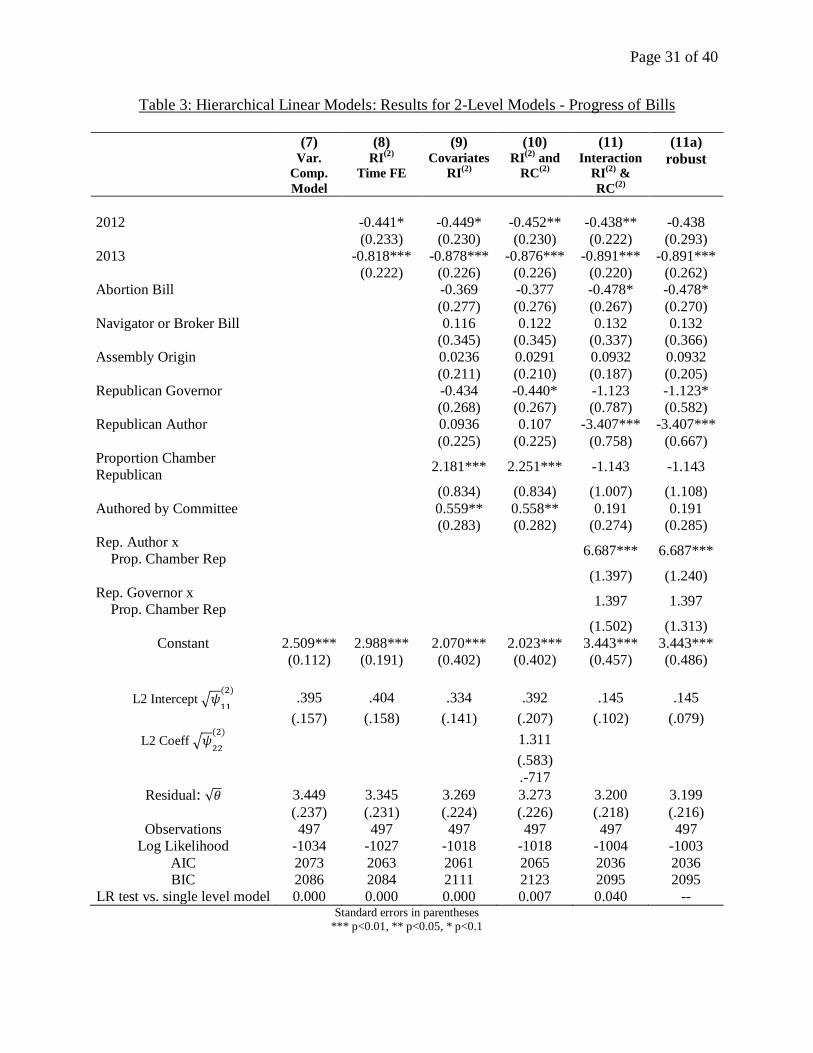
[Table 3 about here]
Again, I began by estimating two-level standard hierarchical variance component models
with either state chamber or states as the higher level for all bills implementing the ACA. From a
theoretical and modeling perspective, the inclusion of the state-chamber level seemed most
appropriate (Model 7, other results omitted).26
Variance components can be interpreted in several
26
I also estimated various three-level (bills are nested in chambers are nested in states) and four-level (bills are
nested in chambers are nested in states are nested in years) variance components models. While these may seem
most appropriate from a theoretical perspective, hierarchical models are very data intensive. The estimations either
showed miniscule results for the intercept or failed to show reasonable results. Various estimation procedures and
algorithms were used. In both cases, the state level soaked up virtually all of the variance from the state chamber
level. Hence, it seems most appropriate in this case to resort to a lower level model with time fixed effects.
Page 21 of 40
ways but variance partition coefficients (VPC) and intraclass correlation coefficients (ICC) are
the most common. The former accounts for the proportion of the observed response variation at a
given level and hence point to the relative importance of the different levels. The ICC accounts
for the correlation within clusters. In the two-level model the ICC is .103, the chamber-level
VPC is .103 and the bill-level VPC is .897.27
Apparently, most of the variation occurs at the bill
level, emphasizing the need for a well-specified bill level model.
I subsequently added year fixed effects (Model 8) and other level-one covariates (Model
9). I also added a random slope for the Proportion of Republicans in the Chamber (Model 10).
The fixed part of the model included indicators for abortion-related bills, navigator-related bills,
committee-authored bills, and whether the bill originated in the assembly, whether the author
was a Republican, and whether the governor of the state was a Republican. In addition,
interactions between Republican governor and the proportion of the chamber that is Republican
and between Republican authors and the proportion of the chamber that is Republican were
added. This accounts again for conditional effects.28
I also estimated the model with restricted
maximum likelihood estimation with essentially similar results (omitted). Hence, for all other
models I resorted to standard maximum likelihood estimation in order to test various level-one
variables with likelihood ratio tests. For comparative purposes I also estimated several three-
level (Models 12-14a) and four-level models (omitted).29
The estimation results for the random
27
In the three level model, the ICC is 0.025 at the year level and .272 at the chamber level. The VPCs, from top to
bottom level, are .024, .266, and .684, respectively. The year fixed effects essentially eliminate the year-level VPC
and ICC and are left with .276 at the chamber-level for the ICC and .269 for the chamber-level VPC and .704 for the
bill-level VPC. In all cases, most of the variation occurs at the bill level. 28
Other interactions were tested, e.g. between abortion-related bills and the proportion of the chamber that is
Republican and navigator-related bills and the proportion of the chamber that is Republican, but likelihood ratio
tests did not warrant an inclusion. 29
Again, likelihood ratio tests showed that an unstructured variance was appropriate, i.e. all variances were
distinctly estimated. ICC and VPC results were presented in footnote 21.

Page 22 of 40
parts in these models are often compromised and imprecise and hence favor a more parsimonious
specification. However, the results are essentially similar.
[Table 4 about here]
Next, I utilized the estimates from linear hierarchical models as starting values for the
estimation of hierarchical ordered probit models. Specifications were again tested for multiple
levels but the most parsimonious structure, a two-level structure with a random intercept,
provided the most appropriate fit (Model 15). 30
A robust version of the model to account for
potential misspecifications (Model 15a) showed essentially similar results.31
The preferred model
used for illustration here is Model 15a.32
[Table 5 about here]
As ordered probit models are non-linear, little is gained by interpreting the coefficients
directly. Hence I merely note that estimates were consistent across specifications and several of
the coefficients in the fixed part of the model achieved or nearly achieved statistical significance
at conventional levels. In the random part of the model, I note that with added complexity the
random parameters became significantly more imprecise and hence it is advisable to utilize a
parsimonious structure if possible (models omitted).
30
For all order probit models I utilized adaptive quadrature instead of the default ordinary Gauss-Hermite
quadrature. I followed (Rabe-Hesketh and Skrondal (2012a), 2012b)) and iteratively increased the number of
quadrature points until estimates did not change anymore. All models converge relatively quickly. 31
Subsequently, I added a random intercept for the Proportion of Republicans in the Chamber (omitted). For
comparative purposes I also estimated several three-level models (omitted). Again, when illustrating the results, a
largely similar picture emerges. 32
In addition to the most appropriate fit to theoretical considerations, I also conducted various tests to assess the
appropriateness of the model including residual analysis.

Page 23 of 40
One simple way to interpret ordered probit models are marginal probabilities.33
The best
way to interpret these generally are graphical displays. Figure 2 presents the predicted
probabilities for various interesting scenarios. The figure presents information about abortion-
related bills, bills that originate in the Senate and the Assembly, bills authored by Democrats and
Republicans, and Republican and Democratic governors. In all cases, results are presented for a
strongly Democratic, an evenly split, and a strongly Republican legislature. For abortion-related
bills, I note the unsurprising difference between Republican legislatures on the one hand and
Democratic and split legislatures on the other hand. The biggest difference here is between bills
that do not move beyond the introduction stage and those that are enacted, respectively.
Moreover, there appears to be little difference between the two chambers with regard to all levels
of outcomes. As expected, Democratic authors do well in Democratic legislatures and
significantly worse in Republican legislatures. The reverse holds true for Republican authors
who seem to be doing even worse when the opposing party controls the legislature. However,
Republicans do much better than Democrats when they control the legislature with a probability
almost twice as large. Finally, Democrats do slightly better under Democratic governors than
Republicans under Republican governors. Overall, the fewest bills get enacted under divided
government. Finally, I note that bills related to navigators were not assessed because of the
limited number available for predicting probabilities. As with the earlier count models we find
results that are inherently plausible: Democrats are more active than Republicans in
implementing the ACA. However, as in the earlier models, Republicans are far from inactive and
participate in the shared governance of the program.
[Figure 2 about here]
33
These are also referred to as population-averaged probabilities.

Page 24 of 40
Conclusion
The future of the ACA appears largely settled although funding concerns for federal
marketplaces as well as several ongoing court challenges have yet to be resolved (Haeder and
Weimer 2013b). Recent problems with the commencement of the enrollment period and the
significant problems with the IT infrastructure are also likely to be overcome eventually.
However, Republican opposition remains as staunch as ever and may even have increased as
potential contenders for the 2016 Republican presidential nomination, many of whom are
governors, are eager to verify their conservative credentials. However, looking beyond the
rhetoric, this paper shows that while Republicans in the states are less eager than their
Democratic counterparts to implement the ACA, they have nonetheless made considerable
headway in pragmatically participating in the shared governance of insurance marketplaces.
Even the staunchest opponents remain eager to defend the long-time state prerogatives when it
comes to the regulation of insurance. Hence while a significant number of states have failed to
create a completely state-based marketplace, virtually all of them appear to be sharing in its
governance in some way. Moreover, participation seems to have increased over time and we
have reason to suspect that this trend will continue. After all, in the first five months of 2013 we
have already seen a significant number of bills introduced. As with other joint programs, it is not
surprising that some states will hold out longer than others for political, financial, or some other
reasons. However, usually states will take up the invitation of the national government and take
advantage of its resources. The ACA appears to follow in these footsteps.

Page 25 of 40
Figures

Page 26 of 40
Figure 1: Implementation of Insurance Marketplaces: Creation of Marketplaces and Number of Bills Introduced
Number of Bills Introduced

Page 27 of 40
Figure 2: Predicted Probabilities for Ordered Probit Model - Progress of Bills
Note: If a bill was introduced in either chamber, it was coded as 1. If it then was voted upon by at least one committee of the same chamber it received a 2; if it
passed the chamber of origin it received a 3. Once the bill moved to the other chamber, it received a 4 if it gained the support of at least one committee, if it
passed that chamber it received a 5. Finally, if it was enacted into law, it received a 6. The figure presents the predicted probabilities for various interesting
scenarios: abortion-related bills, bills that originate in the Senate and the Assembly, bills authored by Democrats and Republicans, and Republican and
Democratic governors. In all cases, results are presented for a strongly Democratic, an evenly split, and a strongly Republican legislature. Confidence Intervals
are omitted to facilitate display.
0 .2 .4 .6 .8 1
Senate
Republican Governor
Republican Author
Democratic Governor
Democratic Author
Assembly
Abortion
Split
Republican
Democratic
Split
Republican
Democratic
Split
Republican
Democratic
Split
Republican
Democratic
Split
Republican
Democratic
Split
Republican
Democratic
Split
Republican
Democratic
1 2 3 4 5 6

Page 28 of 40
Tables

Page 29 of 40
Table 1: Results: Hierarchical Poisson Models – Number of Bills Introduced
(1) (1a) (2) (3) (4) (5) (5a) (5b) (6) (6a)
Support1 Var. Comp.
Model
Non-
parametric
MLE
RI(2)
Time FE
Covariates
RI(2)
RI(2)
and
RC(2)
Interaction
RI(2)
Robust RI(2)
Non-
parametric
MLE
Interaction
RI(2)
& RC(2)
Robust
Fix
ed P
art
2012 -0.271** -0.286** -0.288** -0.278** -0.263** -0.245** -0.280** -0.263***
(0.122) (0.121) (0.121) (0.121) (0.121) (0.120) (0.121) (0.0842)
2013 -0.0270 -0.0352 -0.0402 -0.0290 -0.0252 -0.0167 -0.0331 -0.0252
(0.102) (0.102) (0.103) (0.102) (0.102) (0.101) (0.103) (0.0708)
Chamber 0.123 0.121 0.126 0.105 0.0382 0.122 0.105
(0.0910) (0.0909) (0.0910) (0.103) (0.102) (0.0909) (0.101)
Republican
Governor -0.00489 0.0511 0.503 0.635* 0.882** 0.571 0.635*
(0.152) (0.169) (0.447) (0.380) (0.384) (0.437) (0.358)
Proportion
Chamber
Republican
-1.088*** -1.196*** -0.667 -0.673 -0.458 -0.693 -0.673
(0.414) (0.437) (0.534) (0.504) (0.409) (0.572) (0.422)
Rep. Governor x
Prop. Chamber
Rep.
-0.989 -1.155 -1.715** -1.034 -1.155*
(0.822) (0.721) (0.737) (0.815) (0.658)
Constant 0.817*** .856 0.887*** 1.407*** 1.438*** 1.241*** 1.259*** 1.232*** 1.238*** 1.259***
(0.0703) (.0587) (0.0891) (0.202) (0.210) (0.244) (0.231) (0.192) (0.261) (0.184)
Ran
dom
Par
t
Intercept √
.105 0.060 .109 .077 .104 .070 .055 .032 .095 .081
(.041) (.042) (.034) (.059) (.032) (0.030) (.055) (.060)
Slope √
.295 .256 .023
(.140) (.136) (0.060)
Covariance -.175 -.156 -.043
Observations 203 203 203 203 203 203 203 203 203 203
LR test vs. single
level model 0.000 0.000 0.000 0.003 0.001 0.009
Log likelihood -350 -347 -342 -341 -341 -343 -340 -341 -343
AIC 704 703 697 700 698 704 698 701 707
BIC 711 716 721 730 725 730 728 734 740
Integration Points 20 20 20 20 20 20 20 13 Standard errors in parentheses *** p<0.01, ** p<0.05, * p<0.1

Page 30 of 40
Table 2: Predicted Number of Bills Introduced Nationwide with 90 Percent Confidence Interval
2011
2012
2013
Chamber Low Point
Estimate High
Low Point
Estimate High
Low Point
Estimate High
Republican Governor and Strongly
Democratic Legislature
Senate 599 831 1430
479 699 1213
589 820 1413
Assembly 659 895 1544
531 756 1310
647 883 1524
Democratic Governor and Strongly
Democratic Legislature
Senate 342 550 951
255 453 796
336 542 935
Assembly 388 598 1023
292 495 863
380 590 1013
Republican Governor and Split
Legislature
Senate 330 536 925
243 441 776
322 528 915
Assembly 371 583 1000
281 481 838
366 574 987
Democratic Governor and Split
Legislature
Senate 154 337 585
102 272 474
153 331 573
Assembly 184 370 647
124 300 521
177 364 637
Republican Governor and Strongly
Republican Legislature
Senate 147 327 566
97 264 458
143 322 556
Assembly 173 359 627
117 291 506
170 354 615
Democratic Governor and Strongly
Republican Legislature
Senate 44 197 350
19 157 275
46 194 341
Assembly 63 218 385
29 174 306
59 215 379
Actual
152
105
174
Page 31 of 40
Table 3: Hierarchical Linear Models: Results for 2-Level Models - Progress of Bills
(7) (8) (9) (10) (11) (11a)
Var.
Comp.
Model
RI(2)
Time FE Covariates
RI(2)
RI(2)
and
RC(2)
Interaction
RI(2)
&
RC(2)
robust
2012 -0.441* -0.449* -0.452** -0.438** -0.438
(0.233) (0.230) (0.230) (0.222) (0.293)
2013 -0.818*** -0.878*** -0.876*** -0.891*** -0.891***
(0.222) (0.226) (0.226) (0.220) (0.262)
Abortion Bill -0.369 -0.377 -0.478* -0.478*
(0.277) (0.276) (0.267) (0.270)
Navigator or Broker Bill 0.116 0.122 0.132 0.132
(0.345) (0.345) (0.337) (0.366)
Assembly Origin 0.0236 0.0291 0.0932 0.0932
(0.211) (0.210) (0.187) (0.205)
Republican Governor -0.434 -0.440* -1.123 -1.123*
(0.268) (0.267) (0.787) (0.582)
Republican Author 0.0936 0.107 -3.407*** -3.407***
(0.225) (0.225) (0.758) (0.667)
Proportion Chamber
Republican 2.181*** 2.251*** -1.143 -1.143
(0.834) (0.834) (1.007) (1.108)
Authored by Committee 0.559** 0.558** 0.191 0.191
(0.283) (0.282) (0.274) (0.285)
Rep. Author x
Prop. Chamber Rep 6.687*** 6.687***
(1.397) (1.240)
Rep. Governor x
Prop. Chamber Rep 1.397 1.397
(1.502) (1.313)
Constant 2.509*** 2.988*** 2.070*** 2.023*** 3.443*** 3.443***
(0.112) (0.191) (0.402) (0.402) (0.457) (0.486)
L2 Intercept √
.395 .404 .334 .392 .145 .145
(.157) (.158) (.141) (.207) (.102) (.079)
L2 Coeff √
1.311
(.583)
.-717
Residual: √ 3.449 3.345 3.269 3.273 3.200 3.199
(.237) (.231) (.224) (.226) (.218) (.216)
Observations 497 497 497 497 497 497
Log Likelihood -1034 -1027 -1018 -1018 -1004 -1003
AIC 2073 2063 2061 2065 2036 2036
BIC 2086 2084 2111 2123 2095 2095
LR test vs. single level model 0.000 0.000 0.000 0.007 0.040 -- Standard errors in parentheses
*** p<0.01, ** p<0.05, * p<0.1

Page 32 of 40
Table 4: Hierarchical Linear Models: Results for 3-Level Models - Progress of Bills
(12) (13) (14) (14a)
Var. Comp.
Model
Covariates
RI(2) &
RI(3)
Interaction
RI(2) &
RI(3)
Robust
Abortion Bill -0.340 -0.397 -0.259
(0.270) (0.263) (0.262)
Navigator or Broker Bill 0.0300 0.0976 -0.00566
(0.329) (0.323) (0.346)
Assembly Origin 0.0252 0.0883 0.0852
(0.214) (0.201) (0.196)
Republican Governor -0.516* -1.163 -1.136*
(0.272) (0.842) (0.657)
Republican Author 0.248 -3.109*** -3.118***
(0.218) (0.759) (0.740)
Proportion Chamber Republican 1.863** -1.291 -1.149
(0.841) (1.076) (1.120)
Authored by Committee 0.539* 0.245 0.252
(0.275) (0.272) (0.290)
Rep. Author x
Prop. Chamber Rep
6.361*** 6.336***
(1.399) (1.347)
Rep. Governor x
Prop. Chamber Rep
1.374 1.243
(1.592) (1.408)
Constant 2.630*** 1.824*** 3.081*** 2.983***
(0.212) (0.416) (0.496) (0.427)
L3 Intercept √
.097 .112 .119 --
(.114) (.125) (.127) --
L2 Intercept √
1.063 .958 .726 .790
(.251) (.234) (.205) (.227)
Residual: √ 2.735 2.687 2.650 2.675
(.217) (.212) (.209) (.258)
Observations 497 497 497 497
Log Likelihood -1019 -1011 -998 -998
AIC 2046 2044 2021 2021
BIC 2063 2090 2076 2076
LR test vs. single level model 0.000 0.000 0.000 0.000
Integration Points -- -- -- 13 Standard errors in parentheses
*** p<0.01, ** p<0.05, * p<0.1

Page 33 of 40
Table 5: Hierarchical Order Probit Models: Results - Progress of Bills
(15) (15a)
Outcome Robust
Fix
ed P
art
2012 -0.403* -0.403
(0.243) (0.314)
2013 -0.684*** -0.684**
(0.243) (0.298)
Abortion -0.462 -0.462
(0.301) (0.312)
Navigator or Broker Bill -0.0690 -0.0690
(0.383) (0.420)
Assembly Origin 0.0510 0.0510
(0.202) (0.219)
Republican Governor -0.878 -0.878
(0.869) (0.764)
Republican Bill Author -3.931*** -3.931***
(0.917) (1.102)
Proportion Chamber Republican -1.680 -1.680
(1.079) (1.223)
Authored by Committee 0.196 0.196
(0.300) (0.317)
Rep. Governor x
Prop. Chamber Rep
0.993 0.993
(1.657) (1.616)
Rep. Author x
Prop. Chamber Rep.
7.747*** 7.747***
(1.664) (1.814)
Fix
ed P
art:
Thre
shold
s
κ 1 -1.100** -1.100**
(0.495) (0.531)
κ 2 -0.286 -0.286
(0.494) (0.537)
κ 3 0.0398 0.0398
(0.495) (0.535)
κ 4 0.289 0.289
(0.496) (0.533)
κ 5 0.511 0.511
(0.497) (0.539)
Ran -
dom
Par
t Intercept √
.158 .158
(.122) (.111)
Observations 497 497
Log Likelihood -649.6 -649.6
AIC 1333 1333
BIC 1405 1405
Integration Points 15 15
Standard errors in parentheses
*** p<0.01, ** p<0.05, * p<0.1

Page 34 of 40
Works Cited
Altman, Stuart, and David Shactman. 2011. Power, Politics, and Universal Health Care: The
Inside Story of a Century-Long Battle. Amherst, NY: Prometheus Books.
Atchinson, B.K., and D.M. Fox. 1997. "The politics of the Health Insurance Portability and
Accountability Act." Health Affairs 16 (3):146-50.
Bachrach, Deborah, and Patricia Boozang. 2011. "Federally-Facilitated Exchanges and the
Continuum of State Options: Report from the Study Panel on Health Insurance
Exchanges created under the Patient Protection and Affordable Care Act." Washington,
D.C.: National Academy of Social Insurance.
Bailey, Michael A., and Mark Carl Rom. 2004. "A Wider Race? Interstate Competition across
Health and Welfare Programs." The Journal of Politics 66 (2):326-47.
Beer, Samuel H. 1993. To Make a Nation: The Rediscovery of American Federalism. Cambridge,
MA: The Belknao Press of Harvard University Press.
Berry, William D. 1984. "An Alternative to the Capture Theory of Regulation: The Case of State
Public Utility Commissions." American Journal of Political Science 28 (3):524-58.
Bittermann, Henry J. 1938. State and Federal Grants-in-Aid. New York: Mentzer, Bush &
Company.
Blumberg, Linda J. 2011. "Multi-state Health Insurance Exchanges." In Timely Analysis of
Immediate Health Policy Issues. Washington, D.C.: Urban Institute.
Brennan, Troyen A., and David M. Studdert. 2010. "How Will Health Insurers Respond To New
Rules Under Health Reform?" Health Affairs 29 (6):1147-51.
Carey, Robert. 2010. "Health Insurance Exchanges: Key Issues for State Implementation." In
State Coverage Initiatives. Washington, D.C.: Robert Wood Johnson Foundation.
Cary, William L. 1974. "Federalism and Corporate Law: Reflections upon Delaware." The Yale
Law Journal 83 (4):663-705.
Center for Consumer Information and Insurance Oversight. 2012. "General Guidance on
Federally-facilitated Exchanges." Washington, D.C.: Centers for Medicare & Medicaid
Services.
Chaikind, Hinda R., Jean Hearne, Bob Lyke, and Stephen Redhead. 2005. "The Health Insurance
Portability and Accountability Act (HIPAA) of 1996: Overview and Guidance on
Frequently Asked Questions." Washington, D.C.: Congressional Research Service.
Clark, Jane Perry. 1938. The Rise of a New Federalism: Federal-State Cooperation in the United
States. New York: Columbia University Press.
Conlan, Timothy J. 1991. "And the Beat Goes On: Intergovernmental Mandates and Preemption
in an Era of Deregulation." Publius: The Journal of Federalism 21 (3):43-57.
Conlan, Timothy J., and Paul L. Posner. 2011. "Inflection Point? Federalism and the Obama
Administration." Publius 41 (3):421-46.
Corlette, Sabrina, and JoAnn Volk. 2011. "Active Purchasing for Health Insurance Exchanges:
An Analysis of Options." Georgetown University Health Policy Institute & the National
Academy of Social Insurance.
Corwin, Edward S. 1950. "The Passing of Dual Federalism." Virginia Law Review 36 (1):1-24.
Courant, Paul N., Edward M. Gramlich, and Daniel L. Rubinfeld. 1979. "The Stimulative Effects
of Intergovernmental Grants: Or Why Money Sticks Where It Hits." In Fiscal Federalism
and Grants-in-Aid, ed. P. Mieszkowski and W. H. Oakland. Washington, D.C.: The
Urban Institute.

Page 35 of 40
Crotty, Patricia McGee. 1987. "The New Federalism Game: Primacy Implementation of
Environmental Policy." Publius 17 (2):53-67.
Derthick, Martha. 1970. The Influence of Federal Grants: Public Assistance in Massachusetts.
Cambridge, MA: Harvard University Press.
Doan, Alesha E., and Deborah R. McFarlane. 2012. "Saying No to Abstinence-Only Education:
An Analysis of State Decision-Making." Publius: The Journal of Federalism 42 (4):613-
35.
Dorn, Stan, and Todd Kutyla. 2004. "Health Coverage Tax Credits Under the Trade Act of 2002:
A Preliminary Analysis of Program Operation." New York: The Commonwealth Fund.
Elazar, Daniel J. 1962. The American Partnership: Intergovernmental Co-Operation in the
Nineteenth-Century United States. Chicago: University of Chicago Press.
———. 1984. American Federalism: A View From the States. 3rd ed. New York: Harper &
Row, Publishers.
Erickson, Erick. 2012. "Dear Conservative Organizations." Redstate.com, November 11.
Field, Robert I. 2007. Health Care Regulation in America: Complexity, Confrontation, and
Compromise. Oxford: Oxford University Press.
Fuchs, Beth C., Bob Lyke, Richard Price, and Madeleine Smith. 1998. "The Health Insurance
Portability and Accountability Act (HIPAA) of 1996: Guidance on Frequently Asked
Questions." Washington, D.C.: Congressional Research Service.
Gardiner, Terry, and Isabel Perera. 2011. "SHOPping Around: Setting up State Health Care
Exchanges for Small Businesses: A Roadmap." Washington, D.C.: Center for American
Progress.
Gerber, Brian J., and Paul Eric Teske. 2002. "Regulatory Policymaking in the American States:
A Review of Theories and Evidence." Political Research Quarterly 53 (4):849-86.
Gormley, William T. 1983. "Policy, Politics, and Public Utility Regulation." American Journal
of Political Science 27 (1):86-105.
Greenfield, Margaret. 1958. Medical care for welfare recipients: Basic problems. Berkeley, CA:
University of California, Berkeley.
Greer, Scott L. 2011. "The States’ Role under the Patient Protection and Affordable Care Act."
Journal of Health Politics, Policy and Law 36 (3):469-73.
Grodzins, Morton. 1966. The American System: A New View of Government in the United States.
Chicago: Rand McNally & Company.
Haeder, Simon F. 2012. "Beyond Path Dependence: Explaining Healthcare Reform and Its
Consequences." Policy Studies Journal 40 (S1):65-86.
———. 2013. "Making the Affordable Care Act Work: High-Risk Pools and Health Insurance
Marketplaces." The Forum 11 (3):499-511.
Haeder, Simon F., and David L. Weimer. 2013a. "You Can't Make Me Do It, but I Could Be
Persuaded: Implementation of Health Reforms by the States." In Annual Conference of
the Association for Public Policy Analysis & Management (APPAM). Washington, DC.
———. 2013b. "You Can't Make Me Do It: State Implementation of Insurance Exchanges under
the Affordable Care Act." Public Administration Review 73 (s1):S34-S47.
Haislmaier, Edmund F. 2006. "Massachusetts Health Reform: What the Doctor Ordered."
Washington Times.
Haislmaier, Edmund F., and Nina Owcharenko. 2006. "The Massachusetts Approach: A New
Way To Restructure State Health Insurance Markets And Public Programs." Health
Affairs 25 (6):1580-90.

Page 36 of 40
Health Access. 2010. "Fulfilling the Promise of Health Reform: Creating a Fair & Transparent
Exchange." Sacramento, CA: Health Access.
Hedge, David M., and Michael J. Scicchitano. 1994. "Regulating in Space and Time: The Case
of Regulatory Federalism." The Journal of Politics 56 (1):134-53.
Himelfarb, Richard. 1995. Catastrophic Politics: The Rise and Fall of the Medicare
Catastrophic Coverage Act of 1988. University Park, PA: Pennsylvania State University
Press.
Jacobs, Lawrence R., and Theda Skocpol. 2010. Health Care Reform and American Politics:
What Everyone Needs to Know. New York: Oxford University Press.
———. 2011. "Hard Fought Legacy: Obama, Congressional Democrats, and the Struggle for
Comprehensive Health Care Reform." In Reaching for a New Deal: Ambitious
Governance, Economic Meltdown, and Polarized Politics in Obama's First Two Years,
ed. T. Skocpol and L. R. Jacobs. New York: Russell Sage Foundation.
Jost, Timothy Stoltzfus. 2010. "Health Insurance Exchanges and the Affordable Care Act: Eight
Difficult Issues." Washington, D.C.: The Commonwealt Fund.
Kapur, Sahil. 2013. "House Has Now Voted 46 Times To Repeal Or Dismantle Obamacare."
Talking Points Memo, October 1.
Kersh, Rogan. 2011. "Health Reform: The Politics of Implementation." Journal of Health
Politics, Policy and Law 36 (3):613-23.
Klein, Robert W. 2009. "The Insurance Industry and Its Regulation: An Overview." In The
Future of Insurance Regulation in the United States, ed. M. F. Grace and R. W. Klein.
Washington, D.C.: Brookings Institutions Press.
Knickerbocker, Brad. 2012. "Obamacare Won't Be Repealed. States Now Must Act." Christina
Science Monitor, November 10.
Ko, Grace. 2005. "Partial Preemption Under the Health Insurance Portability and Accountability
Act." Southern California Law Review 79:497-535.
Ladenheim, Kala. 1997. "Health Insurance in Transition: The Health Insurance Portability and
Accountability Act of 1996." Publius 27 (2):33-51.
Lischko, Amy. 2007. "Health Insurance Connectors & Exchanges: A Primer for State Officials."
Princeton, NJ: Robert Wood Johnson Foundation.
Loveless, Tom. 2007. "The Peculiar Politics of No Child Left Behind." In Standards-Based
Reform and the Poverty Gap: Lessons for No Child Left Behind, ed. A. Gamoran.
Washington, D.C.: Brookings Institution Press.
Macmahon, Arthur W., John D. Millett, and Gladys Ogden. 1941/1971. The Administration Of
Federal Work Relief. New York: Da Capo Press.
Maxwell, James A. 1946. The Fiscal Impact of Federalism in the United States. Cambridge,
MA: Harvard University Press.
McCarty, Nolan. 2007. "The Policy Consequences of Partisan Polarization in the United States."
In The Transformation of American Politics: Activist Government and the Rise of
Conservatism, ed. P. Pierson and T. Skocpol. Princeton, NJ: Princeton University Press.
McCarty, Nolan, Keith T. Poole, and Howard Rosenthal. 2006. Polarized America: The Dance
of Ideology and Unequal Riches. Cambridge, MA: The MIT Press.
McCray, Sandra B. 1993. "Federal Preemption of State Regulation of Insurance: End of a 200-
Year Era?" Publius: The Journal of Federalism 23 (4):33-48.
McDonough, John E. 2011. Inside National Health Reform. Berkeley, CA: University of
California Press.

Page 37 of 40
McKinnon, Ronald, and Thomas Nechyba. 1997. "Competition in Federal Systems: The Role of
Political and Financial Constraints." In The New Federalism: Can the States Be Trusted?,
ed. J. Ferejohn and B. R. Weingast. Stanford, CA: Hover Institution Press.
Meier, Kenneth J. 1988. The Political Economy of Regulation: The Case of Insurance. Albany,
NY: State University of New York Press.
———. 1991. "The Politics of Insurance Regulation." The Journal of Risk and Insurance 58
(4):700-13.
Mettler, Suzanne. 1998. Dividing Citizens: Gender and Federalism in New Deal Policy. Ithaca,
NY: Cornell University Press.
Miller, Edward Alan. 2011. "Affordability of Health Insurance to Small Business: Implications
of the Patient Protection and Affordable Care Act." Journal of Health Politics, Policy and
Law 36 (3):539-46.
Miller, Thomas P. 2010. "Health Reform: Only A Cease-Fire In A Political Hundred Years’
War." Health Affairs 29 (6):1101-5.
Musgrave, Richard A. 1959. The Theory of Public Finance: A Study in Public Economy. New
York: McGraw-Hill.
———. 1971. "Economics of Fiscal Federalism." Nebraska Journal of Economics & Business
10 (4):3.
Nichols, Len M. 2010. "Implementing Insurance Market Reforms Under The Federal Health
Reform Law." Health Affairs 29 (6):1152-7.
Nicholson-Crotty, Sean. 2012. "Leaving Money on the Table: Learning from Recent Refusals of
Federal Grants in the American States." Publius: The Journal of Federalism 42 (3):449-
66.
Oates, Wallace E. 1972. Fiscal Federalism. New York: Harcourt Brace Jovanovich, Inc.
Pollitz, K, N Tapay, E Hadley, and J Specht. 2000a. "Early Experience with 'New Federalism' in
Health Iinsurance Regulation." Health Affairs 19 (4):7-22.
Pollitz, Karen, Nicole Tapay, Elizabeth Hadley, and Jalena Specht. 2000b. "Early Experience
With ‘New Federalism’ in Health Insurance Regulation." Health Affairs 19 (4):7-22.
Rabe-Hesketh, Sophia, and Anders Skrondal. 2012a. Multilevel and Longitudinal Modelingt
Using Stata: Categorical Responses, Counts, and Survival. 3rd ed. College Station, TX:
Stata Press.
———. 2012b. Multilevel and Longitudinal Modelingt Using Stata: Continuous Variables. 3rd
ed. College Station, TX: Stata Press.
Rabe-Hesketh, Sophia, Anders Skrondal, and Andrew Pickles. 2004. "Generalized Multilevel
Structural Equation Modeling." Psychometrika 69 (2):167-90.
———. 2005. "Maximum Likelihood Estimation of Limited and Discrete Dependent Variable
Models with Nested Random Effects." Journal of Econometrics 128 (2):301-23.
Regan, Priscilla M., and Christopher J. Deering. 2009. "State Opposition to REAL ID." Publius:
The Journal of Federalism 39 (3):476-505.
Rigby, Elizabeth, and Jake Haselswerdt. 2013a. "Hybrid Federalism, Partisan Politics, and Early
Implementation of State Health Insurance Exchanges." Publius: The Journal of
Federalism 43 (3):368-91.
———. 2013b. "Hybrid Federalism, Partisan Politics, and Early Implementation of State Health
Insurance Exchanges." Publius: The Journal of Federalism.
Riker, William H. 1957. Soldiers of the States. Washington, D.C.: Public Affairs Press.

Page 38 of 40
Rivlin, Alice M. 1992. Reviving the American Dream: The Economy, the State, and the Federal
Government. Washington, D.C.: The Brookings Institution.
———. 2012. "Rethinking Federalism for More Effective Governance." Publius 42 (3):387-400.
Rodden, Jonathan A. 2006. Hamilton's Paradox: The Promise and Peril of Fiscal Federalism.
New York: Cambridge University Press.
Romer, Thomas, and Howard Rosenthal. 1980. "An Institutional Theory of the Effect of
Intergovernmental Grants." National Tax Journal 33 (4):451-8.
Scheberle, Denise. 2004. Federalism and Environmental Policy: Trust and The Politics of
Implementation. Washington, D.C.: Georgetown University Press.
Scicchitano, Michael J., and David M. Hedge. 1993. "From Coercion to Partnership in Federal
Partial Preemption: SMCRA, RCRA, and OSH Act." Publius 23 (4):107-21.
Shelly, Bryan. 2008. "Rebels and Their Causes: State Resistance to No Child Left Behind."
Publius: The Journal of Federalism 38 (3):444-68.
Skocpol, Theda. 2010. "The Political Challenges That May Undermine Health Reform." Health
Affairs 29 (7):1288-92.
Snijders, Tom A.B., and Roel J. Bosker. 1999. Multilevel Analysis: An introduction to basic and
advanced multilevel modeling. London: Sage Publications.
Starr, Paul. 2011. Remedy and Reaction: The Peculiar American Struggle over Health Care
Reform. New Haven, CT: Yale University Press.
StataCorp. 2011a. Stata Longitudinal-Data/Panel-Data Reference Manual Version 12. College
Station, TX: Stata Press.
———. 2011b. Stata Statistical Software: Release 12. College Station, TX: StataCorp LP.
Stone-Axelrad, Julie, and Bob Lyke. 2005. "Health Coverage Tax Credit Authorized by the
Trade Act." Washington, D.C.: Congressional Research Service.
Teske, Paul Eric. 2004. Regulation in the States. Washington, D.C.: Brookings Institution Press.
The Staff of the Washington Post. 2010. Landmark: The Inside Story of America's New Health-
Care Law and What It Means for Us All. New York: Public Affairs.
Theriault, Sean M. 2008. Party Polarization in Congress. New York: Cambridge University
Press.
Thompson, Frank J. 1983. "The Substitution Approach to Intergovernmental Relations: The Case
of OSHA." Publius 13 (4):59-78.
———. 2012. Medicaid Politics: Federalism, Policy Durability, and Health Reform.
Washington, D.C.: Georgetown University Press.
Thompson, Frank J., and Courtney Burke. 2009. "Federalism by Waiver: MEDICAID and the
Transformation of Long-term Care." Publius: The Journal of Federalism 39 (1):22-46.
Tiebout, Charles M. 1956. "A Pure Theory of Local Expenditures." The Journal of Political
Economy 64 (5):416-24.
Tullock, Gordon, Arthur Seldon, and Gordon L. Brady. 2002. Government Failure: A Primer in
Public Choice. Wahington, D.C.: Cato Institute.
Walker, David B. 1995. The Rebirth of Federalism: Slouching toward Washington. Chatham,
NJ: Chatham House Publishers, Inc.
Weil, Alan, and Raymond Scheppach. 2010. "New Roles For States In Health Reform
Implementation." Health Affairs 29 (6):1178-82.
Wicks, Elliot K. 2009. "Building a National Insurance Exchange: Lessons from California."
Oakland, CA: California HealthCare Foundation.

Page 39 of 40
Williams, J. Kerwin, and Edward A. Williams. 1940. "New Techniques in Federal Aid." The
American Political Science Review 34 (5):947-54.
Zimmerman, Joseph F. 2001. "National-State Relations: Cooperative Federalism in the
Twentieth Century." Publius 31 (2):15-30.
———. 2007. "Congressional Preemption During the George W. Bush Administration."
Publius: The Journal of Federalism 37 (3):432-52.