Embed Size (px)
Citation preview



Practice Transformation: A Roadmap for FQHCs

Deena Pourshaban, MPH, PMCH CCEChief Operating Officer
Elevation Health [email protected]
About DeenaDeena’s expertise is in Practice Transformation, Large‐scale Program Design and Management, Business Process Management, Patient Centered Medical Home (PCMH), Social Determinants of Health (SDoH), and Primary Care Workforce Strengthening .
Welcome
Slide 4

Lauren Philp, MSHIProject Manager/Coach
Community Clinic Association of Los Angeles [email protected]
About LaurenLauren is a Six Sigma Black Belt with many years of experience in FQHC quality improvement and risk management. Her expertise is preparing health centers for value‐based payment, work measurement and process improvement, and promoting integrated care.
Welcome
Slide 5

Objectives
By the end of today’s presentation, attendees will:• Increase their understanding of a successful approach to implement practice transformation and PCMH methodologies
• Learn current efforts of 23 Los Angeles FQHC organizations that applied practice transformation to their organization
• Gain access to a practice transformation toolkit in order to implement operational strategies within their own agency.

LA Practice Transformation Network
• Funding to support this work at Los Angeles‐based FQHCs was provided through CMMI’s Transforming Clinical Practice Initiative (TCPi)
• L.A. Care is one of 29 organizations awarded TCPI funding, Los Angeles Practice Transformation Network (LAPTN) helps 3,200 clinicians
• CCALAC provides project management and coaching for the community clinic providers enrolled in LAPTN
• Elevation Health is the lead firm providing an onsite, dedicated masters coaching team to lead the practice transformation effort among 23 FQHCs in Los Angeles County (over 800 providers)
• Four year program through November 2019• Health centers are required to address 27 metrics in order to be ready for Value Based Reimbursement

Practice Transformation Approach
Set aims and enroll practices (align aims
with Federal, State and organizational goals)
Pull baseline data on quality measures
Assign practice coach
Monthly data reporting on
measures. Follow‐up PAT assessment every
6 months
DO THE WORK (implement intervention, empanelment, care teams, QI, ER/hospitalization, pop health, care coordination,
high risk…)
Conduct baseline practice assessment
Assess progress, revise approach if not
meeting target goals
Celebrate success!!!
Implement a sustainability plan to maintain progress

Practice Assessment Tool (PAT)
• A 27 question tool created by CMS to lead progression of practice transformation across 5 phases of maturity ‐ or readiness for value based payment participation
• Based off of Prochaska’s Theory of Change• Engage in PAT every 6 months• Use PAT results to drive improvement • Practice gives a score of 0‐3 on each metric. Each metric has a scoring criteria description

PAT Main Drivers
1. Patient and Family Engagement: Setting self‐management goals, patient feedback into QI clinic system2. Team Relationships: Continuity of care, roles/responsibilities for staff 3. Population Health Management: Empanelment, care management/risk stratification 4. Community Partner: Community referrals 5. Coordinated Care Delivery: Following up on ER visits, care coordination6. Organized and Evidence‐based Care: Address gaps in care, whole person7. Enhanced Care Access: Call patients within 24/78. QI Strategy: PDSA and lean approach, empowering staff9. Transparent Data Monitoring: Produce report and share results 10. Strategic use of Practice Revenue: ROI calculations 11. Joy in work: Workforce and staff satisfaction 12. Analyze and document value: Share financial data, migrate to APM13. Efficient in Operation: Eliminating waste

Practice Transformation
• Our coaching team has assisted the health centers in implementing:
Care teams and huddles
Screening for Social Determinants of
Health
Optimizing EHR use and data reporting
Searching and implementing evidence‐based interventions
Conducting outreach initiatives
Building practice quality
improvement capacity
Team building and communication
Empathy, bias, and motivational skill
building
Risk stratification Empanelment methodologies

PAT

Practice Transformation Toolkits
• CQMs: Workflow redesign, coding, addressing data integrity issues, mapping, EMR templates, training and PDSAs • PAT: Created a “Phase Approach” document, that outlines examples for meeting a score of 2 or 3 for each PAT item• Empanelment: Implementing empanelment in an FQHC• PDSA: Database of tailored interventions to improve CQMs (Diabetes, Depression screening and BMI screening)• Business process management: Protocol on using Lean and time and motion studies• SDOH: Workflow implementation for addressing SDOH• Trainings: Motivational interviewing, empathy, SDOH• BH integration into primary care: Assessment tools, policies• Care coordination (diabetes): Job descriptions workflows, manuals • Utilization: Piloting ER/hospitalization program with FQHCs • Data visualization: Templates to trend CQM data (provider level data)• Workforce: Toolkit to implement strategic HR interventions

Onsite Practice Coaching
0
500
1000
1500
2000
2500
3000
1.3.1 Assign topanels
Diabetes CQM 3.2.3 CultivateJoy
3.3.4 Documentvalue
2.2.2 Build QIcapability
Total H
ours
Top 5 PAT Tasks: 2018‐August 2019
2018 2019 Grand Total

Practice Coaching
0100200300400500600700800900
1000
Total H
ours
Other PAT Tasks: 2018‐August 2019
2018 2019 Grand Total

Onsite Assistance
0 100 200 300 400 500 600 700 800 900 1000
All for HealthAll‐Inclusive Community Health Center
Asian Pacific Health Care VentureBAART
Bartz‐Altadonna (BACHC)East Valley Community Health Center
Eisner Pediatric & Family Medical CenterFamily Health Care Centers of Greater LA
Harbor Community ClinicHCHC
JWCH InstituteNortheast Valley Health Corp
Pomona Community Health CenterSouth Bay Family Health Care
St. John's Well Child and Family CenterT.H.E. Clinic Inc
Tarzana Treatment Centers, Inc.The Children's Clinic
Valley Community HealthcareVenice Family ClinicWatts Healthcare
Westside Family Health CenterWilmington Community Clinic
Hours
Onsite vs. Offsite‐2018
Offsite Onsite
0 100 200 300 400 500 600 700 800
All for HealthAll‐Inclusive Community Health Center
Asian Pacific Health Care VentureBAART
Bartz‐Altadonna (BACHC)East Valley Community Health Center
Eisner Pediatric & Family Medical CenterFamily Health Care Centers of Greater LA
Harbor Community ClinicHCHC
JWCH InstituteNortheast Valley Health Corp
Pomona Community Health CenterSouth Bay Family Health Care
St. John's Well Child and Family CenterT.H.E. Clinic Inc
Tarzana Treatment Centers, Inc.The Children's Clinic
Valley Community HealthcareVenice Family ClinicWatts Healthcare
Westside Family Health CenterWilmington Community Clinic
Hours
Onsite vs. Offsite: Jan‐Aug 2019
Offsite Onsite

Practice Coaching
• Coaching model: 2+ check‐ins per month solidified engagement and accountability
• Phase approach based on change package
• 6 month practice assessments

Savings to Health Plan
• L.A. Care Health Plan has reported that the LAPTN program has realized more than $150,00,000 in cost savings as of August 2019 toward a goal of $60 million by 2019*
• Saved in hospital related claims for diabetes and depression
*Presented at the California Transformation Summit August 21 2019

CCALAC Network Progress (9/2019)
Phase Current % Achieved Goal Achieve
By
# Completed Phase 3 23 96% 24 5/31/18
# Completed Phase 2 24 100% 24 12/31/17
# Completed Phase 5 21 87% 20 9/30/19
# Completed Phase 1 24 100% 24 12/31/16
# Completed Phase 4 21 87% 24 3/31/19

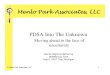
CQM Improvement: 2015‐2019
20
Measure 2015 Baseline
LAPTN Threshold
August 2019
Hemoglobin A1c Poor
Control >9%38.91% 29% 32.39%
Medical Attention for Nephropathy
71.92% 80% 86.32%
Screening for Clinical
Depression & Follow‐Up
40.57% 58% 71.27%
BMI Screening & Follow‐Up 50.49% 51% 86.72%

A1c CQM Improvement

Nephropathy Screening CQM Improvement

Depression Screening CQM Improvement

BMI Screening CQM Improvement

Practice Transformation Toolkits

Empanelment Toolkit & Approach
Panel Calculation Tool & Four Cut Access Database
Training Content
PCP Change Process
Team‐based care
Policies & Job Descriptions
EMR Coordination

Empanelment Toolkit & Approach

Empanelment Toolkit & Approach

Diabetes: Demonstrating A1c Improvement
Data Integrity
• Ensure report mapping is accurate
• Verify lookback period is independent from reporting period
• Working lab interface OR coding is accurate
Gap Outreach
• Check unmatched lab results in interface holding tank
• Implement standing orders for A1c
• Outreach campaigns
• Point of Care testing
Care Management
• Health education classes or videos
• Group visits• Care management program for new diabetics
• Clinical Pharmacist for titration and adherence

Diabetes: Demonstrating A1c Improvement

Diabetes: Demonstrating A1c Improvement
• Pair and Share Activity!• Review A1c checklist for 2 minutes on your own• Notice:
• Where your organization may be skipping a step• Opportunities for further improvement• Steps that seem insurmountable
• Share your thoughts with a partner or two for 3‐4 minutes• Volunteer to share a‐ha moments with group?

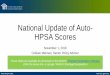
Work Measurement Toolkit
Value47%
Necessary15%
Defects2%
Over‐production12%
Not utilizing Talent14%
Extra‐Processing10%
• Gemba = the real place• Going from guessing what the problem is to knowing what the problem is
• Set a goal and observe the current state
• Empower front‐line staff to participate in improvement
• Apply DOWNTIME to evaluate activities
• Choose intervention, work it, and remeasure!

Work Measurement Toolkit
Type of Waste Examples
Defects Incorrect entry of ICD/CPT code, incorrect EMR mapping with external software, computers freezing, mediation of interpersonal issues
Overproduction Send info automatically when not required, printing and filing unnecessary documents, long set‐up times
Waiting Patient waiting to be seen by provider, patient waiting to get vitals complete
Non‐utilized or underutilized talent
Having Care Managers work the front desk
Transportation Moving files from one location to another, scanning documents
Inventory Running out of flu vaccines, unused or rarely used equipment
Motion People searching for materials, tools or equipment, looking for support staff, too many clicks in the EMR to complete a task
Excess Processing Too many approvals to get a task completed, double documenting

Work Measurement Toolkit
Clinic Testimony:This time and motion study has been exceedingly helpful in identifying inefficient workflows with our clinics. As a result, we have a comprehensive list of changes that we can implement to improve efficient, high value work at our clinics. Our hope is this will make patients more satisfied and thus more compliant with clinical goals and staff happier with their employment experience. One center director told me this study was “ the most important information he’s ever gotten in running this clinic.”

Poll!
• Poll Everywhere• Text ELEVATIONHEA964 in body of text to 22333 to sign up for access

Workforce Pilot and Tools
Measure and EvaluateImplement HR ApproachData Report-Out
Phas
es Trend and Analyze Data
Tim
ing
Key
Act
iviti
es
Schedule working session to collect turnover data
Complete workforce assessment data collection tool
Data will be collected by staff and by department
Collect turnover data as far back as possible
Workforce project team to trend and analyze data using Tableau
Analysis will stratify turnover rates by position, determine turnover rates by clinic site
Needs assessment with clinic stakeholders
Schedule meeting with clinic executive team to share data summary and findings
Workforce project team will prepare a list of HR recommendations to implement
Selection of HR strategic approach to implement
Implementation of strategic HR approach
• Manager Trainings• Exit Interviews• Data Collection &
Analysis• Onboarding• Performance
Evaluation• Staff Engagement• Stay Interviews
Jan 2018-Feb-2019 March-June 2019 July-Present 2019Oct-Dec 2018
Remeasure turnover data
Present findings
Conduct post-intervention surveys & intervention
Focus-group interviews
Draft scale up and spread plan (if HR strategic approach worked)
Nov-Dec 2019
Baseline Data Collection

Workforce Tools
FQHC Workforce Maturity Model• Talent Acquisition• Employee Recognition• Performance Management
• Leadership Development
Turnover Data Collection• Exit Interview Policy• Exit Interview Questionnaire
• Data collection template (Excel)
• Turnover rate calculator
Manager Training• Coaching Model of Management
• Trust and Grow the Model
• Feedback and Time Management
Policies and Procedures (Gaps)• Staff Onboarding• Data Collection• Performance Evaluation• Staff Engagement

Workforce Interventions•3‐ series training on how to effectively manage your staff, use of empathy, how to coach and support staff, implementation of the GROW Model, and time prioritization
• 4 clinics implemented
Manager Trainings
• Levering HRIS system to accurately capture and report data to develop retention strategies
• 4 clinics implemented
Data Collection and Analysis
•Employee pulsing; stay interviews, 360‐degree feedback; exit interviews•2 clinics implementedEmployee Engagement
• Protocol to onboard and train employees, cost of onboarding template• 1 clinic implementedOnboarding
•Protocol for conducting performance evaluations. Provider‐specific and MA‐specific performance
• 3 clinics implemented
Performance Management

Workforce Tools

Workforce Maturity Model

Social Determinants of Health
• Support Health Centers to understand the screening tools available, tailor services and solutions to the resources of the organization, develop optimal workflow, collect patient level data, better understand the resources in their community, and build the necessary partnerships to address the Social Determinants of Health (SDoH) affecting their patients
• Toolkits and workflows were created to address food insecurity, housing and transportation referrals
• Our “Training Through Empathy: SDoH Screening in Primary Care” incorporates the latest evidence base in team care, medical home, social linkages, and empathy to empower care teams to address SDoH in the primary care setting

Hunger Vital Sign• Implemented 2 question food insecurity
screening questionnaire • Within the past 12 months you worried
whether your food would run out before you got money to buy more?
• Within the past 12 months the food you bought just didn’t last and you didn’t have money to get more.
• Would you like a referral to services that can help you?

Practice In ActionJWCH Food Insecurity Approach Agency Overview • 15 main clinic sites (31 health center sites)
• Services 36,472 patients • Secured $75,000 in funding to address food insecurity from LA Care Health Plan
Food Insecurity Intervention
• Implement Hunger Vital Sign Questionnaire for all patients. • Patients screened at every visit• Patients who screen positive have 3 opportunities for follow‐up: Rx Food Guide, direct referral to nutritionist and referral to CalFresh Application Assistor
• Ensured all Diabetes Care Coordinators and enrollment specialists were certified as application assistors
• Developed internal referral• Provided incentives to staff to meet target enrollment goals• Timeline for implementation 6 months • Conducted site specific trainings • Public Charge Talking points
Outcomes • Timeline: Jan‐August 2019• Need total number of certified application assistors: 26 • Total number of submitted CalFresh applications : 339• Total CalFresh approved: 151• Total CalFresh pending: 22• Total CalFresh denied: 166

Competencies and Tools for SDoH
Validated Tools and Technology
Empathy, Bias and Humility
Training
Data Collection and Reporting
Motivational Skill Building
Community Partnerships
Training slide decks*
Food Rx Guide*
Workflow Models*
Scripts and talking points*
Sample Reports*
Evidence Based Screening Tools*

Food Rx Guide

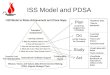
Food Insecurity Reports Application Assistor Approved Pending Grand Total
Timeline: Jan‐August 2019Fernando 2 0 2Aileen 11 3 14Andrea 26 9 35Carlos 27 4 31Denise 21 2 23Felicia 6 2 8Iridian 15 4 19Maria 11 1 12Maribel 18 2 20Grand Total 137 27 164
1 1 1 13 2 2
1
25 1
24
6
5
41 2 51
6
63
3 1
34
6
104
4
33
32
2 5
5
2
21
2
1
21
12
0
5
10
15
20
25
30
? Aileen Andrea Carlos Denise Felicia Iridian Maria MaribelTotal n
umbe
r of C
alFresh Ap
ps
Approved CalFresh Applications: Jan‐August 2019
1‐Jan 1‐Feb 1‐Mar 1‐Apr 1‐May 1‐Jun 1‐Jul 1‐Aug

Talking Points: MA and Provider
MA Talking Points
• We have a food resource guide that you and your family can use to access resources to keep you healthy
• If you need food immediately. There are places in the community that offer free groceries. Here is list (Give patient list)
• I will let the provider know, so you and him/her can discuss the best options for you and your family
Provider Talking Points
• Food is important to our health. I want to make sure you have access to enough food and the right types of food. This guide has a lot of great resources for you. I am also referring you to Cal Fresh (Insert info about Cal Fresh).
• If you need more community resources please speak with the Diabetes Care Coordinator and she/he will make sure you get the resources you need.
Provider Talking Points
• Many of the other patients use food assistance programs and it is really helpful.
• This guide has many resources that are available to you. I am also referring you to nutrition services.
• A nutritionist will contact you to help answer any of your nutrition questions and connect you to additional resources.

Questions

Thank You!
Deena Pourshaban, MPH, PCMH CCEElevation Health Partners, [email protected]‐313‐3321
Lauren Philp, MSHI Community Clinic Association of Los Angeles County, [email protected]‐201‐6520