Embed Size (px)
Citation preview

Copyright © American Burn Association. Unauthorized reproduction of this article is prohibited.e539
RECOMMENDATIONS
StandardsThere are 20 reports in the literature evaluating exercise program prescription for burn survivors; 14 were randomized controlled trials (RCTs), 11 included pediatric burn survivors, and three included adult burn survivors. All of these studies found the prescription of exercise programs to be advanta-geous. The clinical outcomes that showed significant improvement in the RCTs included aerobic capacity, functional outcomes, lean body mass (LBM), mobil-ity evaluations, occupational performance, pulmo-nary function, resting energy expenditure, strength, total work volume, treadmill times, and weight. All exercise training programs took place at burn cen-ters; however, most included additional in-hospital standard of care (SOC) treatment components provided by burn team members. Many of these outcomes may have improved, in part, due to the quality and quantity of in-hospital SOC treatments compared with the outpatient community or home-based programs that were not quantified. It is our
Copyright © 2015 by the American Burn Association 1559-047X/2015
DOI: 10.1097/BCR.0000000000000282
J Burn Care Res
The objective of this review was to systematically evaluate the available clinical evidence for the prescription of strength training and cardiovascular endurance exercise programs for pediatric and adult burn survivors so that practice guidelines could be proposed. This review provides evidence-based recommendations specifically for rehabilitation professionals who are responsible for burn survivor rehabilitation. Summary recommendations were made after the literature was retrieved by systematic review, was critically appraised by multiple authors and the level of evidence determined in accordance with the Oxford Centre for Evidence-based Medicine criteria.1 Although gaps in the literature persist and should be addressed in future research projects, currently, strong research evidence supports the prescription of strength training and aerobic conditioning exercise programs for both adult and pediatric burn survivors when in the presence of strength limitations and/or decreased cardiovascular endurance after evaluation. (J Burn Care Res 2016;37:e539–e558)
From the *School of Physical and Occupational Therapy, McGill University, Montreal, Quebec, Canada; †Centre de recherche, Centre hospitalier de l’Université de Montréal (CRCHUM), Quebec, Canada; ‡Hôpital de réadaptation Villa Medica, Montreal, Quebec, Canada; §Shriners Hospitals for Children, Northern California, Sacramento; ║Division of Physical Medicine and Rehabilitation, Department of Medicine, University of Alberta, Glenrose Rehabilita-tion Hospital, Edmonton, Alberta, Canada; ¶Rhode Island Hospital, Rehabilitation Medicine, Providence; #University of Nebraska Medi-cal Center, Omaha, Nebraska; **University of Washington, Seattle, Washington; ††Alberta Health Services, Foothills Medical Centre, Calgary, Canada; ‡‡Parkland Health & Hospital System, Dallas, Texas; §§Westchester Medical Center, Valhalla, New York; ║║Medi-cal Director of Inpatient Rehabilitation, University of Colorado Hospital, Aurora, Colorado; ¶¶Children’s Hospital Colorardo, Aurora, Colorado; ##Connecticut Burn Center, Bridgeport Hospital, Bridgeport, Connecticut; ***Arizona Burn Center, Phoenix, Arizona; †††University of Utah Burn Center, Salt Lake City, Utah; ‡‡‡Shriners Hospitals for Children, Galveston, Texas; §§§University of Texas Medical Branch, Galveston, Texas; ║║║Arkansas Children’s Hospital Burn Center, Little Rock, Arkansas; and ¶¶¶Library, McGill University, Montreal, Quebec, Canada.
This study was supported by the Edith and Richard Strauss Foundation.
Address correspondence to Bernadette Nedelec, PhD, McGill University, Faculty of Medicine, 3654 Promenade Sir William Osler, Montreal, Quebec, Canada H3G 1Y5. E-mail:[email protected].
Practice Guidelines for Cardiovascular Fitness and Strengthening Exercise Prescription After Burn Injury
Bernadette Nedelec, BSc OT(c), PhD,*†‡ Ingrid Parry, MS, PT,§ Hernish Acharya, BSc, MD, FRCPC,║ Lynne Benavides, OT/CHT,¶ Sara Bills, PT,# Janelle L. Bucher, OTR/L,** Joanne Cheal, BMR, OT,†† Annick Chouinard, BSc, PT,‡ Donna Crump, PT,‡‡ Sarah Duch, PT,§§ Matthew Godleski, MD,║║ Jennifer Guenther, MSPT,¶¶ Catherine Knox, OTR/L,§§ Eric LaBonte, PT,## David Lorello, DPT,*** J. Xavier Lucio, MS OTR/L,††† Lori E. Macdonald, MSc PT,†† Jennifer Kemp-Offenberg, OTR/L,‡‡‡ Candice Osborne, OT,‡‡‡§§§ Kara Pontius, PT,¶¶ Miranda Yelvington, MS,OTR/L, BCPR,║║║ Ana de Oliveira, BSc,† Lorie A. Kloda BA, MLIS, PhD¶¶¶
ORIGINAL ARTICLE

Copyright © American Burn Association. Unauthorized reproduction of this article is prohibited.
Journal of Burn Care & Researche540 Nedelec et al November/December 2016
recommendation that further RCTs be conducted that are entirely in-hospital or community-based.
Recommended Practice Guidelines
• Burn survivors’ strength and cardiovascular endurance should be evaluated in individuals 7 years of age and older. Those who test below normal levels should be prescribed a supervised resistance and/or aerobic exercise program.
• Exercise programs may begin as early as imme-diately postdischarge from acute care and as late as 14 years after burn.
• Exercise programs should last 6 to 12 weeks for adults and up to 12 weeks for children. Studies have not extended beyond 12 weeks therefore it is not known whether longer exercise pro-grams would be more beneficial.
OVERVIEW
PurposeThe purpose of this review was to formulate guide-lines for practice, based on the strength of the pub-lished evidence evaluating the benefit of exercise programs designed to increase the cardiovascular fit-ness or muscular strength of adult and/or pediatric burn survivors.
UsersThese guidelines are designed to aid burn care team members (exercise physiologists, kinesiologists, occupational therapists [OT], physicians, physio-therapists [PT], etc.), who are responsible for the prescription of exercise programs as a component of burn survivor rehabilitation programs. In addition, the recommended guidelines can be implemented by health professionals who do not routinely treat burn patients at their facilities, such as community-based fitness centers, schools, rural facilities, etc.
Clinical ProblemImprovements in acute care and surgical manage-ment of burn survivors have resulted in increased survival rates.2–5 As more individuals recover from major burn injuries there has been an increased focus on rehabilitation to ensure that optimal func-tion and quality of life is achieved.6,7 The need and potential value of cardiovascular endurance and strengthening exercise programs for burn survi-vors is particularly pertinent after prolonged peri-ods of immobilization during acute care and the
characteristic physiological responses to burn injury, such as marked hypermetabolism and skeletal muscle catabolism.8–11 When comparisons have been made between nonburned children relative to pediatric burn survivors, it has been shown that their aero-bic capacity, LBM,12 strength,12–14 quadriceps size, gait parameters,14 pulmonary function, and treadmill times15,16 are significantly reduced in pediatric burn survivors. Comparisons of nonburned adults with adult burn survivors have additionally shown that aerobic capacity,17,18 ambulation speed,19 physical activity participation,17 pulmonary function,17,20 and strength19,21,22 are significantly reduced and oxygen consumption elevated22 in adult burn survivors.
Currently, the resources required, such as testing and training equipment and rehabilitation person-nel, to offer rehabilitation programs that continue for weeks or months after discharge from acute care are lacking at most burn centers. Thus, the objective of this review was to systematically evaluate the avail-able evidence examining the effectiveness of exercise programs to increase cardiovascular fitness or mus-cular strength in adult and/or pediatric burn sur-vivors so that practice guidelines can be developed that specifically describe the required rehabilitation interventions and resources.
PROCESS
The steps taken to develop the practice guidelines reported here are those outlined by Bowker et al.23 These steps included setting up a guideline develop-ment group, forging links with stakeholder groups, agreeing on the scope of the guidelines, formulat-ing a clinically relevant PICO (population, interven-tion, condition, outcome) question, searching the literature for evidence, systematically appraising the evidence found, and making recommendations. The guideline development group consisted of an inter-national assembly of OTs, physicians, and PTs who were members of the American Burn Association Rehabilitation Committee, and clinicians recruited from the American Burn Association. This group met at the American Burn Association meeting in March 2014 for a practice guidelines development workshop where the steps associated with the devel-opment of practice guidelines were reviewed and several practice sessions, focused on critiquing the evidence, were performed until participants were comfortable with the critique form and process. The scope of the guideline is limited to the PICO question: “Does exercise increase the cardiovascular fitness and/or muscular strength of adult and/or pediatric burn survivors?”
Copyright © American Burn Association. Unauthorized reproduction of this article is prohibited.
Journal of Burn Care & Research Volume 37, Number 6 Nedelec et al e541
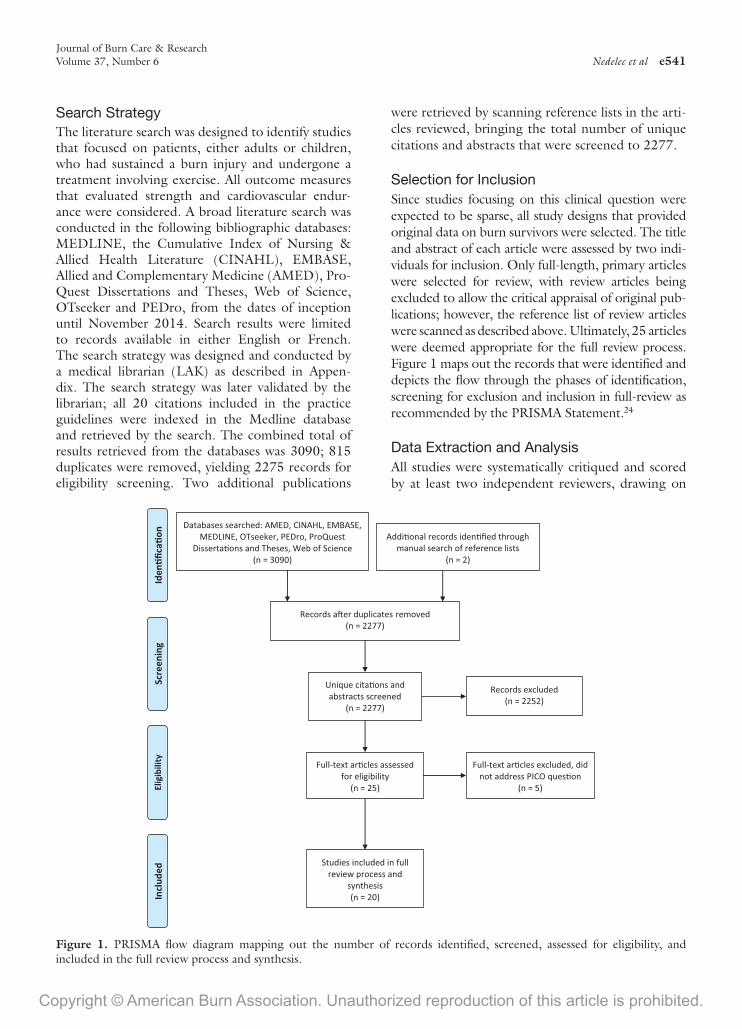
Search StrategyThe literature search was designed to identify studies that focused on patients, either adults or children, who had sustained a burn injury and undergone a treatment involving exercise. All outcome measures that evaluated strength and cardiovascular endur-ance were considered. A broad literature search was conducted in the following bibliographic databases: MEDLINE, the Cumulative Index of Nursing & Allied Health Literature (CINAHL), EMBASE, Allied and Complementary Medicine (AMED), Pro-Quest Dissertations and Theses, Web of Science, OTseeker and PEDro, from the dates of inception until November 2014. Search results were limited to records available in either English or French. The search strategy was designed and conducted by a medical librarian (LAK) as described in Appen-dix. The search strategy was later validated by the librarian; all 20 citations included in the practice guidelines were indexed in the Medline database and retrieved by the search. The combined total of results retrieved from the databases was 3090; 815 duplicates were removed, yielding 2275 records for eligibility screening. Two additional publications
were retrieved by scanning reference lists in the arti-cles reviewed, bringing the total number of unique citations and abstracts that were screened to 2277.
Selection for InclusionSince studies focusing on this clinical question were expected to be sparse, all study designs that provided original data on burn survivors were selected. The title and abstract of each article were assessed by two indi-viduals for inclusion. Only full-length, primary articles were selected for review, with review articles being excluded to allow the critical appraisal of original pub-lications; however, the reference list of review articles were scanned as described above. Ultimately, 25 articles were deemed appropriate for the full review process. Figure 1 maps out the records that were identified and depicts the flow through the phases of identification, screening for exclusion and inclusion in full-review as recommended by the PRISMA Statement.24
Data Extraction and AnalysisAll studies were systematically critiqued and scored by at least two independent reviewers, drawing on
Figure 1. PRISMA flow diagram mapping out the number of records identified, screened, assessed for eligibility, and included in the full review process and synthesis.

Copyright © American Burn Association. Unauthorized reproduction of this article is prohibited.
Journal of Burn Care & Researche542 Nedelec et al November/December 2016
the critical appraisal form designed by Law et al.25 Fourteen items comprised in the scoring of this form relate to study purpose, literature review, study sam-ple, outcomes, interventions, results, conclusions, and clinical implications. The two to three review-ers independently extracted details required to com-plete the critical appraisal form. Each item was rated numerically as (1) for Yes and (0) for No or Not Applicable. A total score was then calculated and compared with the other reviewers’ results. If there were minor differences (±2 points), the discrepancies were discussed until a consensus was reached. When larger differences occurred, an additional reviewer was called upon to critique the article and consen-sus was achieved among all reviewers. After this pro-cess, five articles were removed22,26–29 because the authors’ clinical question was not addressed.
SCIENTIFIC FOUNDATION
Study CharacteristicsTable 1 summarizes the critique results for the 20 retained citations. Citations are categorized based on the population of patients included: (1) pediatric burn survivors only (denoted by single asterisk) and
(2) adult burn survivors. As shown on the last column of this table, 2/20 citations (10%) received a score of <5 out of a possible total score of 14 but were included for completeness sake. Of the remaining citations 18 (90%) received a score ≥10 therefore are considered high quality studies.
Table 2 summarizes the study characteristics, results, and level of evidence for each of the 20 cita-tions. Fourteen were RCTs,12,14,16,19,31,32,34–36,38,41–44 one was a follow-up study,39 four were case–control studies,20,30,33,37 and one a historically controlled study.40 The sample sizes of all studies ranged from 16 to 222. Those including only pediatric partici-pants ranged from 20 to 222 while those with only adult participants ranged from 16 to 40. Sample size of the RCTs ranged from 21 to 222 for those that included only pediatric participants and 31 to 40 for those that included only adult participants. The level of evidence was assigned according to the updated Oxford Centre for Evidence-based Medicine Levels of Evidence.1
Pediatric Burn Survivor StudiesEleven of the 20 publications included in this review specifically addressed exercise prescription
Table 1. Evidentiary Table: Evaluation of the Quality of Intervention Studies
Citation
Sample Outcomes Intervention Results
Study Purpose
Literature Review Design Size Details Justified Reliable Valid
Detailed Description Contamination Co-intervention
Statistical Significance
Analysis Appropriate
Clinical Importance
Drop Outs Reported
Conclusions Appropriate
Total Score
Ahmed et al (2011) 1 1 CC 30 1 0 1 1 1 0 0 1 1 1 1 1 11Al-Mousawi et al (2010) 1 1 RCT 21* 1 0 1 1 1 1 1 1 1 1 1 1 13Cronan et al (1990) 0 1 CC 16 0 0 0 0 0 0 0 0 0 1 0 0 2Cucuzzo et al (2001) 1 1 RCT 21* 1 0 1 1 1 1 0 1 1 1 1 1 12de Lateur et al (2007) 1 1 RCT 35 1 0 1 1 1 0 0 1 1 1 1 1 11Ebid et al (2012) 1 1 RCT 31 1 0 1 1 1 1 1 1 1 1 1 1 13Ebid et al (2014) 1 1 RCT 33* 1 1 1 1 1 1 1 1 1 1 1 1 14Ebid et al (2012) 1 1 RCT 40 1 1 1 1 1 1 1 1 1 1 1 1 14Grisbrook et al (2012) 1 1 CC 18 1 0 1 1 1 0 0 1 1 1 1 1 11Grisbrook et al (2013) 1 1 CC 18 1 0 1 1 1 0 0 1 1 1 1 1 11Hardee et al (2014) 1 1 RCT 47* 1 0 1 1 1 1 1 1 1 1 0 1 12Paratz et al (2012) 1 1 Non-RCT 30 1 0 1 1 1 0 0 1 1 1 1 1 11Parrot et al (1988) 1 1 HC 40 0 0 0 0 0 1 0 0 0 1 0 0 4Porro et al (2012) 1 1 RCT 222* 1 1 1 1 1 1 1 1 1 1 1 1 14Porro et al (2013) 1 1 RCT 58* 1 0 1 1 1 1 1 1 1 1 1 1 13Prkzora et al (2007) 1 1 RCT 51* 1 0 1 1 1 1 1 1 1 1 0 1 12Suman et al (2002) 1 1 RCT 51* 1 0 1 1 1 1 1 1 1 1 1 1 13Suman et al (2001) 1 1 RCT 35* 1 1 1 1 1 0 1 1 1 1 1 1 13Suman et al (2003) 1 1 RCT 44* 1 1 1 1 1 0 0 1 1 1 1 1 12Suman et al (2007) 1 1 RCT 20* 1 0 1 1 1 0 0 1 1 1 0 1 10
Design: CC, case-controlled study; HC, historically controlled studies; non-RC, nonrandomized controlled cohort/follow-up study; RCT, randomized, controlled, trial.YES = 1; NO = 0; N/A = 0.*Pediatric burn survivors.

Copyright © American Burn Association. Unauthorized reproduction of this article is prohibited.
Journal of Burn Care & Research Volume 37, Number 6 Nedelec et al e543
for pediatric burn survivors. Of these 11, 10 were carried out at the Shriners Hospital for Children, Galveston. All of the pediatric studies were RCTs and all received a rating of between 10 and 14 of 14 on the critique form. The prescribed resistance and/or aerobic exercise program had positive ben-efits, that are outlined in detail in Table 2, for a num-ber of outcome measures including bone mineral content,41 gait measures,14,34 LBM,12,31,32,38,41,43,44 pulmonary function,16 quad size,14 resting heart rate,34 strength,12,14,31,32,34,41–44 total work volume,32,34 treadmill time,16,32 and VO2peak.
12,16,32,38,42,43 Two pediatric studies26,29 were excluded from full review and incorporation into the final recommendation as they did not respond directly to the PICO question but did nonetheless demonstrate benefits from exer-cise for the outcomes that they examined. No adverse events were reported in any of these studies.
Adult Burn SurvivorsThere were several case series published in 1988 and 1990 that reported on the benefits of exer-cises or exercise programs specifically prescribed for burn survivors33,40 but had many methodological limitations that were identified during the critique
(Table 1). Since 2007, there have been seven addi-tional reports that were rated between 11 and 14 of 14. Three were case–control studies, one was a fol-low-up study and three were RCTs. The prescribed resistance and/or aerobic exercise program had posi-tive benefits, that are outlined in detail in Table 2, for a number of outcome measures including func-tion,20,39 gait measures,19,39 LBM,37 quality of life,39 strength,19,30,36,37,39 total work volume,19 and VO2max or peak.
20,39 One case–control study, which was published in two different manuscripts with two dif-ferent sets of outcomes reported in each,20,37 reported an improvement with exercise but the improvement in the burn survivor group did not significantly differ from the improvement reported in their healthy con-trols. This group also reported on the impact of the exercise program on the participants’ self-reported quality of life28 but this article was excluded from full review as it did not include any muscle strength or cardiovascular fitness measure, therefore did not respond to the PICO question.
Outcome MeasuresThe outcome measures that were used in these reports varied across studies. Those outcomes that
Table 1. Evidentiary Table: Evaluation of the Quality of Intervention Studies
Citation
Sample Outcomes Intervention Results
Study Purpose
Literature Review Design Size Details Justified Reliable Valid
Detailed Description Contamination Co-intervention
Statistical Significance
Analysis Appropriate
Clinical Importance
Drop Outs Reported
Conclusions Appropriate
Total Score
Ahmed et al (2011) 1 1 CC 30 1 0 1 1 1 0 0 1 1 1 1 1 11Al-Mousawi et al (2010) 1 1 RCT 21* 1 0 1 1 1 1 1 1 1 1 1 1 13Cronan et al (1990) 0 1 CC 16 0 0 0 0 0 0 0 0 0 1 0 0 2Cucuzzo et al (2001) 1 1 RCT 21* 1 0 1 1 1 1 0 1 1 1 1 1 12de Lateur et al (2007) 1 1 RCT 35 1 0 1 1 1 0 0 1 1 1 1 1 11Ebid et al (2012) 1 1 RCT 31 1 0 1 1 1 1 1 1 1 1 1 1 13Ebid et al (2014) 1 1 RCT 33* 1 1 1 1 1 1 1 1 1 1 1 1 14Ebid et al (2012) 1 1 RCT 40 1 1 1 1 1 1 1 1 1 1 1 1 14Grisbrook et al (2012) 1 1 CC 18 1 0 1 1 1 0 0 1 1 1 1 1 11Grisbrook et al (2013) 1 1 CC 18 1 0 1 1 1 0 0 1 1 1 1 1 11Hardee et al (2014) 1 1 RCT 47* 1 0 1 1 1 1 1 1 1 1 0 1 12Paratz et al (2012) 1 1 Non-RCT 30 1 0 1 1 1 0 0 1 1 1 1 1 11Parrot et al (1988) 1 1 HC 40 0 0 0 0 0 1 0 0 0 1 0 0 4Porro et al (2012) 1 1 RCT 222* 1 1 1 1 1 1 1 1 1 1 1 1 14Porro et al (2013) 1 1 RCT 58* 1 0 1 1 1 1 1 1 1 1 1 1 13Prkzora et al (2007) 1 1 RCT 51* 1 0 1 1 1 1 1 1 1 1 0 1 12Suman et al (2002) 1 1 RCT 51* 1 0 1 1 1 1 1 1 1 1 1 1 13Suman et al (2001) 1 1 RCT 35* 1 1 1 1 1 0 1 1 1 1 1 1 13Suman et al (2003) 1 1 RCT 44* 1 1 1 1 1 0 0 1 1 1 1 1 12Suman et al (2007) 1 1 RCT 20* 1 0 1 1 1 0 0 1 1 1 0 1 10
Design: CC, case-controlled study; HC, historically controlled studies; non-RC, nonrandomized controlled cohort/follow-up study; RCT, randomized, controlled, trial.YES = 1; NO = 0; N/A = 0.*Pediatric burn survivors.

Copyright © American Burn Association. Unauthorized reproduction of this article is prohibited.
Journal of Burn Care & Researche544 Nedelec et al November/December 2016
Tab
le 2
. Cha
ract
eris
tics
of I
nclu
ded
Stud
ies
Aut
hors
Des
ign
Sam
ple
Out
com
e M
easu
res
Inte
rven
tion
Res
ults
Lev
el o
f E
vide
nce
Ahm
ed e
t al
(2
011)
30
Cas
e–co
ntro
l st
udy
• n
= 30
mal
es (
burn
su
rviv
ors
= 15
; hea
lthy
= 15
)•
Mea
n ag
e (y
rs):
bur
n s
urvi
vors
= 2
4.4;
hea
lthy
= 24
.8•
%T
BSA
B: r
ange
30–
40•
Dee
p pa
rtia
l thi
ckne
ss a
nter
ior
thig
h bu
rn•
Bas
elin
e:
21–2
5 da
ys p
ost-
burn
• St
reng
th (
Bio
dex
Syst
em-3
dy
nam
omet
er)
• E
valu
ated
at
base
line
and
6 w
eeks
pos
t-tr
aini
ng
• 6-
wee
k tr
eatm
ent
peri
od (
2×/
52)
• E
x: is
okin
etic
st
reng
then
ing
• B
urn
surv
ivor
s an
d he
alth
y su
bjec
ts e
ccen
tric
and
con
cent
ric
peak
tor
que
30°
and
90°/
sec
sign
ifica
ntly
impr
oved
• %
pea
k to
rque
impr
ovem
ent
was
si
gnifi
cant
ly g
reat
er fo
r bu
rn
surv
ivor
s th
an h
ealth
y su
bjec
ts fo
r ec
cent
ric
90ᵒ
/se
c an
d 30ᵒ
/se
c as
w
ell a
s co
ncen
tric
30ᵒ
/se
c•
Peak
tor
ques
wer
e si
gnifi
cant
ly
grea
ter
for
heal
thy
subj
ects
dur
ing
conc
entr
ic p
eak
torq
ues
at 3
0° a
nd
ecce
ntri
c to
rque
s at
30°
and
90°
4
In 2
011,
Ahm
ed e
t al
30 p
erfo
rmed
a c
ase-
cont
rolle
d fo
llow
-up
stud
y w
here
a g
roup
of b
urn
surv
ivor
s an
d he
alth
y pa
rtic
ipan
ts w
ere
eval
uate
d an
d th
en t
rain
ed w
ith e
xerc
ises
on
an
isok
inet
ic d
ynam
omet
er. A
fter
6 w
eeks
, of t
wic
e-pe
r-w
eek
trai
ning
, the
ecc
entr
ic a
nd c
once
ntri
c m
uscl
e pe
ak t
orqu
e im
prov
ed in
bot
h gr
oups
. The
aut
hors
rep
orte
d a
sign
ifica
ntly
gr
eate
r pe
rcen
tage
of i
mpr
ovem
ent
for
the
burn
sur
vivo
rs a
s co
mpa
red
with
the
hea
lthy
part
icip
ants
for
ecce
ntri
c co
ntra
ctio
ns a
t bo
th 3
0° a
nd 9
0° p
er s
econ
d an
d co
ncen
tric
co
ntra
ctio
ns a
t 30
° pe
r se
cond
aft
er t
rain
ing.
Al-
Mou
saw
i et
al
(201
0)31
RC
T•
n =
21 (
Ex
= 11
, SO
C =
10)
• M
ean
age
(yrs
): E
x =
12.2
; SO
C =
13.
7•
Mea
n %
TB
SAB
: Ex
= 61
; SO
C =
56
• B
asel
ine:
6 m
os p
ost-
burn
• R
EE
• L
BM
(D
EX
A)
• St
reng
th (
Bio
dex
Syst
em-3
dy
nam
omet
er: i
soki
netic
)•
Hei
ght,
wei
ght
• 12
-wee
k tr
eatm
ent
peri
od•
SOC
: sam
e as
Sum
an
et a
l (20
01)
• E
x: (
Figu
re 2
)
• M
ean
wei
ght
gain
was
sig
nific
ant
for
the
Ex
grou
p, b
ut n
o di
ffer
ence
be
twee
n gr
oups
• N
o si
gnifi
cant
diff
eren
ce in
the
m
ean
chan
ge in
RE
E o
r pe
rcen
t pr
edic
ted
RE
E•
Subj
ects
in t
he E
x gr
oup
gain
ed
sign
ifica
ntly
gre
ater
LB
M, e
ven
whe
n no
rmal
ized
to
heig
ht•
Ex
grou
p de
mon
stra
ted
sign
ifica
ntly
gre
ater
str
engt
h im
prov
emen
ts, w
hich
per
sist
ed
whe
n no
rmal
ized
to
LB
M in
dex
2
In 2
010,
Al-
Mou
saw
i et
al31
rep
orte
d on
a s
tudy
usi
ng t
he e
xerc
ise
prog
ram
des
crib
ed in
Fig
ure
2 pl
us S
OC
com
pare
d w
ith S
OC
onl
y. T
he a
utho
rs c
onfir
med
pre
viou
s fin
ding
s th
at
LB
M a
nd s
tren
gth
impr
oved
but
con
trar
y to
the
ir p
revi
ous
findi
ngs32
the
y re
port
ed t
hat
RE
E d
id n
ot s
igni
fican
tly in
crea
se w
ith t
ime
in e
ither
gro
up a
nd t
hat
ther
e w
as n
o si
gnifi
cant
di
ffer
ence
bet
wee
n gr
oups
. Unl
ike
thei
r pr
evio
us p
ublic
atio
n th
ey n
orm
aliz
ed t
he R
EE
mea
sure
s to
the
cor
resp
ondi
ng c
hang
es in
LB
M, w
hich
res
ulte
d in
the
diff
eren
ces
in R
EE
be
com
ing
negl
igib
le, t
hus,
exe
rcis
e tr
aini
ng d
id n
ot e
xace
rbat
e po
stbu
rn h
yper
met
abol
ism
.(C
onti
nued
)

Copyright © American Burn Association. Unauthorized reproduction of this article is prohibited.
Journal of Burn Care & Research Volume 37, Number 6 Nedelec et al e545
Cro
nan
et a
l (1
990)
33
Cas
e–co
ntro
l st
udy
• n
= 16
(8
isok
inet
ic; 8
isom
etri
c/is
oton
ic)
patie
nt-m
atch
ed jo
ints
w
ith fu
ll A
RO
M•
Age
ran
ge: 2
0–40
yrs
• %
TB
SAB
: ran
ge 9
–64
• B
asel
ine:
5–9
mos
pos
t-bu
rn
• St
reng
th (
Cyb
ex I
I du
al
isok
inet
ic d
ynam
omet
er)
• SO
C: s
plin
ting,
st
retc
hing
, iso
met
ric, a
nd
isoto
nic
wor
k lo
ads
• E
x: c
ardi
ovas
cula
r tr
aini
ng a
nd is
okin
etic
pr
otoc
ol
• %
defi
cit
of p
eak
torq
ue w
as le
ss
in E
x gr
oup
com
pare
d w
ith S
OC
gr
oup
for
all j
oint
s te
sted
• N
o st
atis
tical
ana
lysi
s
4
Cro
nan
et a
l33 c
ompa
red
burn
sur
vivo
rs w
ho h
ad r
ecei
ved
SOC
to
burn
sur
vivo
rs w
ho h
ad r
ecei
ved
SOC
plu
s ca
rdio
vasc
ular
and
str
engt
h tr
aini
ng u
tiliz
ing
the
isok
inet
ic d
ynam
omet
er.
The
pat
ient
s se
rved
as
thei
r ow
n co
ntro
ls b
y co
mpa
ring
an
invo
lved
ext
rem
ity t
o an
uni
nvol
ved
extr
emity
. Tho
se w
ho r
ecei
ved
exer
cise
tra
inin
g an
d SO
C p
erfo
rmed
bet
ter
whe
n te
sted
on
an is
okin
etic
dyn
amom
eter
tha
n th
e co
mpa
riso
n jo
int.
The
aut
hors
rep
ort
sign
ifica
nt p
eak
torq
ue d
efici
t in
the
non
isok
inet
ic t
reat
men
t gr
oup,
alth
ough
no
stat
istic
al
anal
yses
wer
e re
port
ed. I
n ad
ditio
n, d
etai
ls o
f the
stu
dy p
opul
atio
n an
d in
terv
entio
n pr
ogra
m w
ere
extr
emel
y lim
ited.
Cuc
uzzo
et
al
(200
1)34
RC
T•
n =
21 (
Ex
= 11
; SO
C =
10)
• M
ean
age
(yrs
): 1
0.6;
(ra
nge
5.9–
19.9
)•
%T
BSA
B: m
ean
59.7
; ran
ge
40–8
7•
Bas
elin
e: 6
mos
pos
t-bu
rn
• W
eigh
t, h
eigh
t, r
estin
g he
art
rate
, 6 M
WT
• St
reng
th (
3RM
)•
Eva
luat
ed a
t ba
selin
e &
12
wee
ks la
ter
(6 a
nd 9
mos
po
st-b
urn)
• 12
-wee
k tr
eatm
ent
peri
od•
SOC
: OP
OT
and
PT
tw
ice
daily
× 1
hr
• E
x: F
igur
e 2
exce
pt
aero
bic
exer
cise
3×/
wee
k pl
us O
T a
nd P
T
daily
× 1
hr,
scho
ol
2–3
hrs/
d, p
lay
ther
apy
and
psyc
holo
gica
l co
unse
lling
as
nece
ssar
y
• Si
gnifi
cant
cha
nge
for
the
follo
win
g ou
tcom
es: w
eigh
t E
x gr
oup
and
SOC
gro
up, r
estin
g he
art
rate
for
the
Ex
grou
p, 3
RM
fo
r th
e E
x gr
oup
(bic
eps,
tri
ceps
, fo
rear
ms,
qua
dric
eps,
ham
stri
ngs)
an
d SO
C g
roup
(fo
rear
ms,
qu
adri
ceps
, ham
stri
ngs)
, tot
al
volu
me
wor
k fo
r th
e E
x an
d SO
C
grou
p, 6
MW
T fo
r th
e E
x an
d SO
C g
roup
• Im
prov
emen
ts w
ere
sign
ifica
ntly
gr
eate
r fo
r th
e E
x th
an S
OC
gro
up
for:
3R
M (
ham
stri
ngs)
, tot
al
volu
me
wor
k, 6
MW
T
2
Cuc
uzzo
et
al34
rep
orte
d on
21
part
icip
ants
tha
t w
ere
rand
omiz
ed t
o ei
ther
an
exer
cise
gro
up o
r a
SOC
gro
up. T
he b
asel
ine
age,
per
cent
bur
n, h
eigh
t, w
eigh
t, a
nd r
estin
g he
art
rate
did
no
t si
gnifi
cant
ly d
iffer
bet
wee
n gr
oups
. The
pos
t-tr
eatm
ent
eval
uatio
n re
veal
ed t
hat
wei
ght,
tot
al v
olum
e of
wor
k, a
nd t
he 6
-min
ute
wal
k te
st in
crea
sed
sign
ifica
ntly
in b
oth
grou
ps.
The
res
ting
hear
t ra
te im
prov
ed in
the
exe
rcis
e gr
oup
but
not
the
SOC
gro
up. A
ll fiv
e of
the
3R
M in
crea
sed
for
the
exer
cise
gro
up a
nd t
hree
of t
he fi
ve fo
r th
e SO
C g
roup
. The
gr
oup
com
pari
sons
rev
eale
d si
gnifi
cant
diff
eren
ces
betw
een
grou
ps fo
r ha
mst
ring
3R
M, t
otal
vol
ume
of w
ork
and
the
6-m
inut
e w
alk
test
. The
re w
ere
no a
dver
se e
vent
s or
dro
pout
s.de
Lat
eur
et a
l (2
007)
35
RC
T•
n =
35 (
WT
Q =
13;
WT
T =
11;
SO
C =
11)
• M
ean
age
(yrs
): W
TQ
= 3
5.4;
W
TT
= 4
3.5;
SO
C =
34.
9•
Mea
n %
TB
SAB
: WT
Q =
19.
5;
WT
T =
16.
8; S
OC
= 2
1.6
• M
ax a
erob
ic c
apac
ity
(VO
2 m
ax)
• E
valu
ated
at
base
line
an
d 12
wee
ks
• 12
-wee
k tr
eatm
ent
peri
od•
SOC
: OT
and
PT
(R
OM
, mas
sage
, sp
lintin
g, s
tret
chin
g,
stre
ngth
enin
g, m
obili
ty
trai
ning
, AD
L t
rain
ing)
• SO
C +
WT
Q S
OC
+
WT
T
• W
TT
and
WT
Q g
roup
: sig
nific
ant
impr
ovem
ents
in a
erob
ic c
apac
ity
(VO
2 m
ax)
from
bas
elin
e to
12/
52
and
com
pare
d w
ith S
OC
but
not
be
twee
n gr
oups
• SO
C g
roup
: no
sign
ifica
nt
impr
ovem
ent
in a
erob
ic c
apac
ity•
No
adve
rse
effe
cts
repo
rted
2
Tab
le 2
. (C
onti
nued
)
Aut
hors
Des
ign
Sam
ple
Out
com
e M
easu
res
Inte
rven
tion
Res
ults
Lev
el o
f E
vide
nce
(Con
tinu
ed )

Copyright © American Burn Association. Unauthorized reproduction of this article is prohibited.
Journal of Burn Care & Researche546 Nedelec et al November/December 2016
In 2
007,
de
Lat
eur
et a
l35 p
ublis
hed
the
first
RC
T in
volv
ing
adul
t bu
rn s
urvi
vors
. Par
ticip
ants
wer
e ra
ndom
ly a
ssig
ned
to o
ne o
f thr
ee g
roup
s: (
1) “
func
tiona
l res
tora
tion”
(SO
C);
(2)
w
ork-
to-t
oler
ance
gro
up (
WT
T);
and
(3)
wor
k-to
-quo
ta (
WT
Q).
The
WT
T g
roup
per
form
ed a
erob
ic e
xerc
ise
at t
heir
tar
get
hear
t ra
te fo
r as
long
as
tole
rate
d to
a m
axim
um o
f 30
min
utes
. The
WT
Q g
roup
exe
rcis
ed t
o pr
eset
quo
tas
that
gra
dual
ly in
crea
sed
the
exer
cise
inte
nsity
. The
max
imal
oxy
gen
cons
umpt
ion
of t
he W
TT
and
WT
Q g
roup
s si
gnifi
cant
ly
incr
ease
d m
ore
than
the
SO
C g
roup
. The
re w
as, h
owev
er, n
o di
ffer
ence
bet
wee
n th
e tw
o ex
erci
se g
roup
s.E
bid
et a
l (2
012)
36
RC
T•
n =
31 a
dults
(E
x =
15;
SOC
= 1
6)•
Mea
n ag
e (y
rs):
Ex
= 35
.86;
SO
C =
36.
06•
%T
BSA
B r
ange
: 36–
45•
Bas
elin
e: ~
50 d
pos
t-bu
rn
• St
reng
th (
Bio
dex
isok
inet
ic d
ynam
omet
er)
• E
valu
ated
at
base
line
and
8 w
eeks
late
r•
Mat
ched
hea
lthy
cont
rols
co
mpa
red
with
bas
elin
e m
easu
res
• 8-
wee
k tr
eatm
ent
peri
od•
SOC
: hom
e pr
ogra
m
(RO
M, s
plin
ting,
st
retc
hing
of L
E, d
aily
w
alki
ng, f
unct
iona
l am
bula
tion,
res
ista
nce
exer
cise
s, A
DL
tr
aini
ng)
• E
x: w
hole
bod
y vi
brat
ion
3×/
52
• K
nee
and
ankl
e st
reng
th w
as
signi
fican
tly g
reat
er in
hea
lthy
subj
ects
co
mpa
red
with
bur
n su
rviv
ors
• K
nee
and
ankl
e st
reng
th s
igni
fican
tly
incr
ease
d in
bot
h tr
eatm
ent
grou
ps
acro
ss t
ime
• M
ean
% c
hang
e in
str
engt
h w
as
sign
ifica
ntly
gre
ater
for
Ex
grou
p co
mpa
red
with
SO
C
2
In 2
012,
Ebi
d et
al36
con
duct
ed a
RC
T s
tudy
ing
two
grou
ps o
f bur
n su
rviv
ors
who
rec
eive
d ei
ther
who
le b
ody
vibr
atio
n (W
BV
) pl
us S
OC
or
SOC
onl
y. W
hole
bod
y vi
brat
ion
invo
lved
th
e su
bjec
t st
andi
ng in
a 9
0° s
quat
pos
ition
on
a vi
brat
ing
plat
form
. The
aut
hors
mea
sure
d st
reng
th o
utco
me
and
com
pare
d it
to h
ealth
y, m
atch
ed c
ontr
ols
at b
asel
ine.
Bot
h gr
oups
de
mon
stra
ted
an in
crea
se in
str
engt
h af
ter
8 w
eeks
of t
reat
men
t, a
lthou
gh t
he W
BV
gro
up’s
str
engt
h ga
ins
wer
e si
gnifi
cant
ly g
reat
er t
han
the
SOC
gro
up. T
he b
urn
surv
ivor
s’
stre
ngth
was
sig
nific
antly
red
uced
rel
ativ
e to
the
hea
lthy
cont
rols
at
base
line
but
near
ly r
etur
ned
to t
he h
ealth
y, m
atch
ed, c
ontr
ols
afte
r th
e 8
wee
ks.
Ebi
d et
al
(201
4)14
RC
T•
n =
33 (
Ex
= 16
; SO
C =
17;
he
alth
y =
20)
• M
ean
age
(yrs
): E
x =
13.4
6;
SOC
= 1
3.6;
hea
lthy
= 14
.2•
Mea
n %
TB
SAB
: Ex
= 48
.86;
SO
C =
42.
4•
LE
bur
ns
• St
reng
th (
Bio
dex
Syst
em-3
dy
nam
omet
er)
• Q
uadr
icep
s si
ze (
tape
m
easu
re)
• G
ait
para
met
ers
(GA
ITR
ite s
yste
m)
• E
valu
ated
at
base
line
and
12 w
eeks
late
r•
Mat
ched
hea
lthy
cont
rols
co
mpa
red
with
bas
elin
e m
easu
res
• 12
-wee
k tr
eatm
ent
peri
od•
SOC
: hom
e pr
ogra
m•
Ex:
SO
C +
3×/
52,
trea
dmill
war
m-u
p,
hotp
acks
, str
etch
ing,
is
okin
etic
exe
rcis
es
• Q
uad
stre
ngth
: sig
nific
antly
less
for
burn
sur
vivo
rs c
ompa
red
with
hea
lthy
subj
ects
at b
asel
ine;
sig
nific
antly
in
crea
sed
for
Ex
and
SOC
gro
up b
ut
signi
fican
tly m
ore
for
Ex
• Q
uad
size
: sig
nific
antly
gre
ater
for
heal
thy
subj
ects
com
pare
d w
ith b
urn
surv
ivor
s at
bas
elin
e; s
igni
fican
t in
crea
se in
Ex
grou
p•
All
gait
para
met
ers:
signi
fican
tly
diffe
rent
for b
urn
surv
ivor
s com
pare
d w
ith h
ealth
y su
bjec
ts a
t bas
elin
e;
signi
fican
tly in
crea
sed
for E
x an
d SO
C
but s
igni
fican
tly m
ore
for E
x gr
oup
2
The
one
ped
iatr
ic s
tudy
not
con
duct
ed b
y th
e G
alve
ston
gro
up w
as a
RC
T in
201
4, b
y E
bid
et a
l.14 C
hild
ren
with
low
er e
xtre
mity
bur
ns w
ere
rand
omiz
ed t
o ei
ther
a 1
2 w
eek
isok
inet
ic
quad
str
engt
heni
ng p
rogr
am in
add
ition
to
SOC
or
just
SO
C. T
hey
eval
uate
d th
e ef
fect
of a
n is
okin
etic
qua
d st
reng
then
ing
prog
ram
on
the
size
and
str
engt
h of
the
qua
dric
eps
and
on
gait
para
met
ers.
All
mea
sure
s si
gnifi
cant
ly im
prov
ed fo
r bo
th g
roup
s du
ring
the
12-
wee
k tr
eatm
ent
peri
od e
xcep
t qu
ad s
ize
for
the
SOC
gro
up. T
he im
prov
emen
ts w
ere
sign
ifica
ntly
gr
eate
r fo
r th
e ex
erci
se g
roup
com
pare
d w
ith t
he S
OC
gro
up fo
r al
l mea
sure
s. T
hey
also
com
pare
d ba
selin
e m
easu
res
of q
uad
size
and
str
engt
h an
d ga
it pa
ram
eter
s to
age
-mat
ched
he
alth
y ch
ildre
n. A
ll ba
selin
e m
easu
res
diff
ered
sig
nific
antly
from
tho
se o
f hea
lthy
child
ren.
It
shou
ld b
e no
ted
that
the
res
ista
nce
trai
ning
pro
gram
pre
scri
bed
used
the
sam
e eq
uipm
ent
that
was
use
d fo
r te
stin
g th
eref
ore
som
e of
the
str
engt
h be
nefit
s m
ay b
e at
trib
uted
to
incr
ease
d fa
mili
arity
with
the
tes
ting
equi
pmen
t.
Tab
le 2
. (C
onti
nued
)
Aut
hors
Des
ign
Sam
ple
Out
com
e M
easu
res
Inte
rven
tion
Res
ults
Lev
el o
f E
vide
nce
(Con
tinu
ed )
Copyright © American Burn Association. Unauthorized reproduction of this article is prohibited.
Journal of Burn Care & Research Volume 37, Number 6 Nedelec et al e547
Ebi
d et
al
(201
2)19
RC
T•
n =
40 (
Ex
= 20
; SO
C =
20;
he
alth
y =
23)
• M
ean
age
(yrs
): E
x =
24.6
; SO
C =
27.
3; h
ealth
y =
24.6
• M
ean
%T
BSA
B: 4
5.5
(ran
ge
35–5
5%)
• B
asel
ine:
6 m
os p
ost-
burn
• St
reng
th (
Bio
dex
Syst
em-3
dy
nam
omet
er)
• A
mbu
latio
n sp
eed
• B
asel
ine
com
pari
son
to
heal
thy
subj
ects
• E
valu
ated
at
base
line
and
12 w
eeks
late
r (6
and
9
mos
pos
t-bu
rn)
• 12
-wee
k tr
eatm
ent
peri
od•
SOC
: OT
& P
T•
Ex:
3×/
wk,
tre
adm
ill
war
m u
p, q
uadr
icep
s an
d ha
mst
ring
s st
retc
hing
, con
cent
ric
stre
ngth
enin
g
• Pe
ak k
nee
exte
nsor
and
flex
or
torq
ue si
gnifi
cant
ly in
crea
sed
for E
x gr
oup
from
bas
elin
e to
pos
t-tr
aini
ng•
Ex
grou
p’s
peak
tor
que
and
tota
l w
ork
sign
ifica
ntly
impr
oved
mor
e th
an S
OC
• Pe
ak t
orqu
e an
d to
tal w
ork
of
heal
thy
subj
ects
was
sig
nific
antly
gr
eate
r th
an b
oth
burn
sur
vivo
rs
grou
ps p
ost-
trai
ning
• E
x gr
oup
ambu
latio
n sp
eed
sign
ifica
ntly
incr
ease
d fr
om
base
line
and
com
pare
d w
ith S
OC
• A
mbu
latio
n sp
eed
was
sig
nific
antly
gr
eate
r fo
r he
alth
y su
bjec
ts
com
pare
d w
ith b
oth
burn
sur
vivo
r gr
oups
at
base
line
2
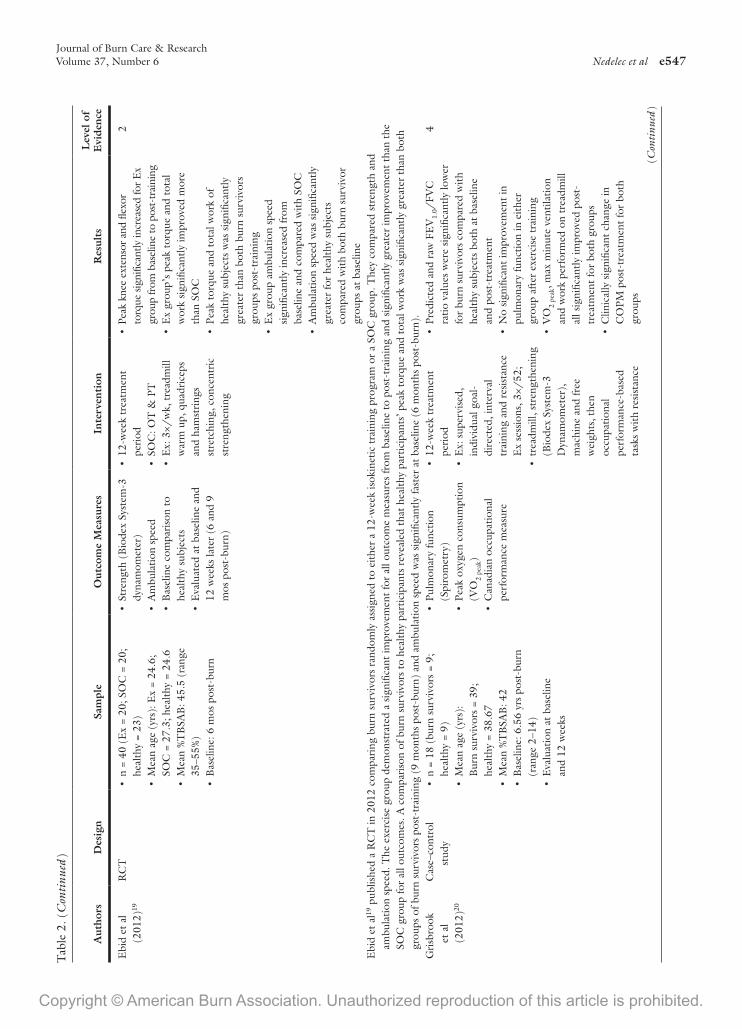
Ebi
d et
al19
pub
lishe
d a
RC
T in
201
2 co
mpa
ring
bur
n su
rviv
ors
rand
omly
ass
igne
d to
eith
er a
12-
wee
k is
okin
etic
tra
inin
g pr
ogra
m o
r a
SOC
gro
up. T
hey
com
pare
d st
reng
th a
nd
ambu
latio
n sp
eed.
The
exe
rcis
e gr
oup
dem
onst
rate
d a
sign
ifica
nt im
prov
emen
t fo
r al
l out
com
e m
easu
res
from
bas
elin
e to
pos
t-tr
aini
ng a
nd s
igni
fican
tly g
reat
er im
prov
emen
t th
an t
he
SOC
gro
up fo
r al
l out
com
es. A
com
pari
son
of b
urn
surv
ivor
s to
hea
lthy
part
icip
ants
rev
eale
d th
at h
ealth
y pa
rtic
ipan
ts’ p
eak
torq
ue a
nd t
otal
wor
k w
as s
igni
fican
tly g
reat
er t
han
both
gr
oups
of b
urn
surv
ivor
s po
st-t
rain
ing
(9 m
onth
s po
st-b
urn)
and
am
bula
tion
spee
d w
as s
igni
fican
tly fa
ster
at
base
line
(6 m
onth
s po
st-b
urn)
.G
risb
rook
et
al
(201
2)20
Cas
e–co
ntro
l st
udy
• n
= 18
(bu
rn s
urvi
vors
= 9
; he
alth
y =
9)•
Mea
n ag
e (y
rs):
B
urn
surv
ivor
s =
39;
heal
thy
= 38
.67
• M
ean
%T
BSA
B: 4
2•
Bas
elin
e: 6
.56
yrs
post
-bur
n (r
ange
2–1
4)•
Eva
luat
ion
at b
asel
ine
an
d 12
wee
ks
• Pu
lmon
ary
func
tion
(Spi
rom
etry
)•
Peak
oxy
gen
cons
umpt
ion
(VO
2 pe
ak)
• C
anad
ian
occu
patio
nal
perf
orm
ance
mea
sure
• 12
-wee
k tr
eatm
ent
peri
od•
Ex:
sup
ervi
sed,
in
divi
dual
goa
l-di
rect
ed, i
nter
val
trai
ning
and
res
ista
nce
Ex
sess
ions
, 3×/
52;
• tr
eadm
ill, s
tren
gthe
ning
(B
iode
x Sy
stem
-3
Dyn
amom
eter
),
mac
hine
and
free
w
eigh
ts, t
hen
occu
patio
nal
perf
orm
ance
-bas
ed
task
s w
ith r
esis
tanc
e
• Pr
edic
ted
and
raw
FE
V1.
0/FV
C
ratio
val
ues
wer
e si
gnifi
cant
ly lo
wer
fo
r bu
rn s
urvi
vors
com
pare
d w
ith
heal
thy
subj
ects
bot
h at
bas
elin
e an
d po
st-t
reat
men
t•
No
sign
ifica
nt im
prov
emen
t in
pu
lmon
ary
func
tion
in e
ither
gr
oup
afte
r ex
erci
se t
rain
ing
• V
O2
peak
, max
min
ute
vent
ilatio
n an
d w
ork
perf
orm
ed o
n tr
eadm
ill
all s
igni
fican
tly im
prov
ed p
ost-
trea
tmen
t fo
r bo
th g
roup
s•
Clin
ical
ly s
igni
fican
t ch
ange
in
CO
PM p
ost-
trea
tmen
t fo
r bo
th
grou
ps
4
Tab
le 2
. (C
onti
nued
)
Aut
hors
Des
ign
Sam
ple
Out
com
e M
easu
res
Inte
rven
tion
Res
ults
Lev
el o
f E
vide
nce
(Con
tinu
ed )

Copyright © American Burn Association. Unauthorized reproduction of this article is prohibited.
Journal of Burn Care & Researche548 Nedelec et al November/December 2016
In 2
012,
Gri
sbro
ok e
t al
20 c
ondu
cted
a c
ase–
cont
rol s
tudy
exa
min
ing
the
effe
cts
of a
12-
wee
k ex
erci
se t
rain
ing
prog
ram
on
pulm
onar
y fu
nctio
n an
d ae
robi
c ca
paci
ty o
f bur
n su
rviv
ors
com
pare
d w
ith h
ealth
y co
ntro
ls. N
ine
burn
sur
vivo
rs a
nd n
ine
heal
thy
cont
rol p
artic
ipan
ts w
ere
recr
uite
d in
to a
sup
ervi
sed,
indi
vidu
aliz
ed, o
ccup
atio
nal p
erfo
rman
ce, a
nd g
oal-
dire
cted
tra
inin
g pr
ogra
m. A
ll bu
rn s
urvi
vors
wer
e at
leas
t 2
year
s po
st-b
urn
with
at
leas
t a
20%
sur
face
are
a bu
rn. T
here
was
a s
tatis
tical
ly s
igni
fican
t di
ffer
ence
in t
he fo
rce
expi
rato
ry
volu
me/
forc
ed v
ital c
apac
ity r
atio
s of
bur
n su
rviv
ors
com
pare
d w
ith h
ealth
y co
ntro
ls, b
oth
at b
asel
ine
and
post
-exe
rcis
e pr
ogra
m. A
fter
the
exe
rcis
e pr
ogra
m, a
erob
ic c
apac
ity a
s m
easu
red
by V
O2p
eak,
max
imal
min
ute
vent
ilatio
n an
d w
ork
perf
orm
ance
on
the
trea
dmill
sig
nific
antly
impr
oved
rel
ativ
e to
bas
elin
e fo
r bo
th g
roup
s, b
ut t
here
was
no
impr
ovem
ent
in
pulm
onar
y fu
nctio
n fo
r ei
ther
gro
up w
ith t
ime.
The
re w
as a
lso
a cl
inic
ally
sig
nific
ant
incr
ease
in o
ccup
atio
nal p
erfo
rman
ce fo
r bo
th g
roup
s, t
hus
thei
r ab
ility
to
part
icip
ate
in a
ctiv
ities
th
at w
ere
impo
rtan
t to
the
m a
nd t
heir
sat
isfa
ctio
n w
ith t
heir
per
form
ance
sig
nific
antly
impr
oved
.G
risb
rook
et
al
(201
3)37
Cas
e–co
ntro
l st
udy
• Sa
me
as G
risb
rook
et
al (
2012
)•
Stre
ngth
(B
iode
x Sy
stem
-3
dyna
mom
eter
)•
LB
M (
DE
XA
)
• Sa
me
as G
risb
rook
et
al
(201
2)•
Peak
torq
ue, w
ork,
and
pow
er:
repo
rted
on
a su
bgro
up o
f bur
n su
rviv
ors a
nd a
ll ni
ne h
ealth
y su
bjec
ts:
signi
fican
t im
prov
emen
t acr
oss a
ll m
uscl
e gr
oups
with
trea
tmen
t•
Sign
ifica
nt in
crea
se in
LB
M w
ith
exer
cise
for
both
gro
ups
4
Furt
her
anal
ysis
of t
he c
ase–
cont
rol s
tudy
pub
lishe
d in
201
220 w
as p
ublis
hed
in 2
01337
and
rep
orte
d on
the
eff
ect
of t
he e
xerc
ise
trai
ning
pro
gram
on
mus
cle
stre
ngth
and
LB
M. F
or
the
anal
ysis
, the
aut
hors
com
bine
d th
e da
ta o
f the
bur
n su
rviv
ors
and
nonb
urne
d he
alth
y co
ntro
ls t
o de
term
ine
the
with
in g
roup
eff
ect,
whi
ch d
emon
stra
ted
an in
crea
se fo
r al
l of t
he
stre
ngth
out
com
es. T
here
was
no
betw
een
grou
p ef
fect
for
any
of t
he s
tren
gth
outc
omes
. The
y al
so r
epor
ted
that
the
re w
as a
n in
crea
se in
LB
M p
oste
xerc
ise
for
the
grou
p w
hen
they
co
mbi
ned
the
burn
sur
vivo
rs a
nd h
ealth
y pa
rtic
ipan
ts.
Har
dee
et a
l (2
014)
38
RC
T•
n =
47 (
Ex
= 24
; SO
C =
23)
• M
ean
age
(yrs
):
Ex
= 13
; SO
C =
13
• M
ean
%T
BSA
B:
Ex
= 60
; SO
C =
59
• H
eigh
t, w
eigh
t•
Stre
ngth
(B
iode
x Sy
stem
-3
dyna
mom
eter
)•
LB
M (
DE
XA
)•
Peak
oxy
gen
cons
umpt
ion
(VO
2pea
k)•
Mix
ed m
uscl
e fr
actio
nal
synt
hetic
rat
e (s
tabl
e is
otop
e in
fusi
on s
tudy
)
• 12
-wee
k tr
eatm
ent
peri
od b
egin
ning
im
med
iate
ly p
ost-
disc
harg
e•
SOC
gro
up: O
T/
PT
hom
e pr
ogra
m•
Ex:
Fig
ure
2
• Si
gnifi
cant
diff
eren
ce b
etw
een
grou
ps fo
r pe
ak to
rque
whe
n co
rrec
ted
for
body
wei
ght,
VO
2pea
k, %
cha
nge
in L
BM
disc
harg
e to
po
st tr
eatm
ent a
nd w
hole
-bod
y,
leg,
arm
, and
% c
hang
e in
LB
M
disc
harg
e to
12
mon
ths
post
-bur
n fo
r w
hole
-bod
y an
d le
g•
Sign
ifica
nt c
hang
e w
ith t
reat
men
t:
both
Ex
and
SOC
gro
up’s
m
uscl
e fr
actio
nal s
ynth
etic
rat
e re
duce
d be
twee
n di
scha
rge
and
post
-tre
atm
ent
but
ther
e w
as n
o di
ffer
ence
bet
wee
n gr
oups
2
In 2
014,
Har
dee
et a
l38 c
ondu
cted
a R
CT
stu
dyin
g th
e ef
fect
of a
12-
wee
k ex
erci
se p
rogr
am in
itiat
ed im
med
iate
ly a
fter
disc
harg
e fr
om th
e ac
ute
care
cen
ter
com
pare
d w
ith S
OC
, as
oppo
sed
to 6
mon
ths
post
-bur
n, w
hich
was
the
case
with
all
of th
eir
prev
ious
rep
orts
from
this
grou
p. T
here
was
no
diff
eren
ce b
etw
een
the
exer
cise
gro
up a
nd th
e SO
C g
roup
at b
asel
ine
for
age,
hei
ght,
wei
ght,
TB
SA b
urne
d, le
ngth
of s
tay,
or
fem
ale
to m
ale
ratio
. Aft
er c
ompl
etio
n of
the
exer
cise
pro
gram
com
paris
on b
etw
een
grou
ps r
evea
led
that
the
exer
cise
gro
up h
ad
signi
fican
tly g
reat
er r
elat
ive
peak
torq
ue, V
O2p
eak,
perc
ent c
hang
e in
who
le-b
ody,
leg
and
arm
LB
M b
etw
een
disc
harg
e an
d po
st-t
reat
men
t, an
d pe
rcen
t cha
nge
in w
hole
-bod
y an
d le
g L
BM
bet
wee
n di
scha
rge
and
12 m
onth
s po
st-b
urn.
Bot
h gr
oups
dem
onst
rate
d a
redu
ctio
n in
mus
cle
frac
tiona
l syn
thet
ic r
ate
betw
een
disc
harg
e an
d po
st-t
reat
men
t, w
hich
is c
onsis
tent
w
ith a
dec
reas
e in
hyp
erm
etab
olism
, but
ther
e w
as n
o di
ffer
ence
bet
wee
n gr
oups
, dem
onst
ratin
g th
at e
xerc
ise tr
aini
ng d
id n
ot n
egat
ivel
y af
fect
hyp
erm
etab
olism
in b
urn
surv
ivor
s.
Tab
le 2
. (C
onti
nued
)
Aut
hors
Des
ign
Sam
ple
Out
com
e M
easu
res
Inte
rven
tion
Res
ults
Lev
el o
f E
vide
nce
(Con
tinu
ed )

Copyright © American Burn Association. Unauthorized reproduction of this article is prohibited.
Journal of Burn Care & Research Volume 37, Number 6 Nedelec et al e549
Para
tz e
t al
(2
012)
39
Non
rand
omiz
ed
cont
rolle
d fo
llow
-up
stud
y
• n
= 30
(E
x =1
6; S
OC
= 1
4)•
Mea
n ag
e (y
rs):
Ex
= 30
.4;
SOC
= 4
2.64
• M
ean
%T
BSA
B: E
x =
47;
SOC
29.
9•
Ex
grou
p: s
igni
fican
tly y
oung
er,
larg
er s
urfa
ce a
rea
burn
, lon
ger
hosp
ital a
nd I
CU
sta
y, in
crea
se
% h
and
burn
s an
d #
of s
eptic
ep
isod
es
• M
SWT
• Pe
ak o
xyge
n
cons
umpt
ion
(VO
2pea
k)•
Stre
ngth
, gri
p•
Func
tion
and
qual
ity o
f lif
e (Q
uick
DA
SH, L
EFS
, B
SHS-
A)
• 12
-wee
k tr
eatm
ent
peri
od•
SOC
: sel
f-m
anag
emen
t pr
ogra
m o
f exe
rcise
s and
re
ferr
al to
loca
l the
rapi
st•
Ex:
sup
ervi
sed
aero
bic
and
resi
stan
ce t
rain
ing
• Si
gnifi
cant
cha
nge
with
tre
atm
ent:
qu
ad, l
atis
sim
us d
orsi
, R &
L g
rip
stre
ngth
, LE
FS, Q
uick
DA
SH•
Sign
ifica
nt d
iffer
ence
bet
wee
n gr
oups
: at b
asel
ine
R &
L g
rip
stre
ngth
; at 6
wee
ks q
uad,
latis
simus
do
rsi,
VO
2pea
k, Q
uick
DA
SH; a
t 3
mos
qua
ds, l
atiss
imus
dor
si, V
O2p
eak,
MSW
T, Q
uick
DA
SH•
No
adve
rse
effe
cts
repo
rted
3
A n
onra
ndom
ized
, fol
low
-up
stud
y co
nduc
ted
in A
ustr
alia
was
als
o re
port
ed in
201
2.39
Bur
n su
rviv
ors
recr
uite
d in
to t
his
stud
y w
ere
assi
gned
to
the
exer
cise
plu
s SO
C g
roup
if t
hey
lived
in
clo
se p
roxi
mity
to
the
burn
cen
ter
to a
tten
d th
erap
y se
ssio
ns o
n a
regu
lar
basi
s fo
r a
6-w
eek
peri
od o
f tim
e or
wer
e as
sign
ed t
o SO
C if
the
y liv
ed fa
r en
ough
from
the
bur
n ce
nter
th
at t
hey
coul
d on
ly a
tten
d in
term
itten
t fo
llow
up
appo
intm
ents
. Stu
dy o
utco
mes
incl
uded
the
mod
ified
shu
ttle
wal
k te
st, V
O2p
eak,
mus
cle
and
grip
str
engt
h, Q
uick
DA
SH, l
ower
ex
trem
ity fu
nctio
nal s
cale
and
bur
n-sp
ecifi
c he
alth
sca
le (
BSH
S)—
abbr
evia
ted
vers
ion.
At
base
line,
the
exe
rcis
e gr
oup
was
sig
nific
antly
you
nger
, had
larg
er s
urfa
ce a
rea
burn
s, s
taye
d lo
nger
in t
he in
tens
ive
care
uni
t an
d ho
spita
l, le
ss g
rip
stre
ngth
, and
was
tw
ice
as li
kely
to
have
han
d bu
rns
and
sept
ic e
piso
des
duri
ng t
he a
cute
sta
y. F
or t
he B
SHS,
the
mot
or a
nd
skill
s su
bdom
ain
was
sig
nific
antly
hig
her
for
the
exer
cise
gro
up a
t ba
selin
e. A
ll ou
tcom
e m
easu
res
sign
ifica
ntly
impr
oved
ove
r tim
e fo
r th
e ex
erci
se g
roup
and
all
exce
pt V
O2p
eak,
rest
ing
hear
t ra
te, s
hutt
le d
ista
nce,
low
er e
xtre
mity
func
tiona
l sca
le a
nd Q
uick
DA
SH fo
r th
e SO
C g
roup
. In
addi
tion,
the
re w
as n
o si
gnifi
cant
impr
ovem
ent
in a
ny o
f the
dom
ains
or
the
tota
l sco
re fo
r th
e SO
C g
roup
with
tim
e, in
fact
the
psy
chol
ogic
al d
omai
n si
gnifi
cant
ly w
orse
ned
with
tim
e fo
r th
is g
roup
. Han
d fu
nctio
n im
prov
ed fo
r bo
th g
roup
s w
ith t
ime.
The
gr
oup
allo
catio
n pr
oced
ure
empl
oyed
in t
his
stud
y m
akes
it v
ery
diffi
cult
to c
oncl
ude
that
the
aer
obic
and
res
istiv
e ex
erci
se t
rain
ing
com
pone
nts
wer
e re
spon
sibl
e fo
r th
e di
ffer
ence
in
outc
omes
sin
ce t
here
are
so
man
y di
ffer
ence
s be
twee
n th
eir
base
line
char
acte
rist
ics
and
the
afte
r di
scha
rge
care
tha
t th
ese
patie
nts
rece
ived
. How
ever
, des
pite
the
fact
tha
t th
e ex
erci
se
grou
p ha
d la
rger
bur
ns t
hat
requ
ired
long
er in
patie
nt c
are
and
wer
e m
ore
likel
y to
invo
lve
thei
r ha
nds,
the
ir im
prov
emen
t ac
ross
tim
e fo
r im
pair
men
t, fu
nctio
nal a
nd q
ualit
y of
life
ou
tcom
es w
ere
mor
e su
bsta
ntia
l tha
n th
e SO
C g
roup
tha
t w
as n
ot t
reat
ed a
t th
e bu
rn c
ente
r. T
hus,
the
ove
rall
reha
bilit
atio
n pr
ogra
m t
hat
was
rec
eive
d by
the
gro
up t
reat
ed a
t th
e bu
rn c
ente
r ha
d su
bsta
ntia
l ben
efits
rel
ativ
e to
the
“se
lf-m
anag
emen
t” S
OC
pro
gram
.Pa
rrot
t et
al
(198
8)40
His
tori
cally
co
ntro
lled
stud
y
• n=
40
(Ex
= 20
; his
tori
cal
cont
rols
= 2
0)•
Age
ran
ge: 1
8–65
yrs
• %
TB
SAB
: ran
ge 1
5–50
• L
OS
• N
umbe
r of
OT
/PT
vis
its•
Tim
e re
turn
ing
to w
ork
• Su
bjec
tive
ques
tionn
aire
• C
ontr
ol: 1
–2 h
rs/
d O
T/
PT (
unst
ruct
ured
in
divi
dual
ized
pro
gram
)•
Ex:
2 h
rs/
d of
IP
OT
/PT
(s
truc
ture
d ci
rcui
t of p
ulle
y w
ork,
bic
ycle
wor
k, U
E
ergo
met
er, L
E m
at w
ork,
ch
in-u
ps, s
tair
step
wor
k,
writ
ing
on a
nd c
lean
ing
a m
irror
, mac
ram
é or
bel
t w
ork,
UE
wan
d ex
erci
se, a
pi
pe p
roje
ct)
• Si
mila
r L
OS
• E
x co
mpa
red
with
con
trol
: de
crea
sed
num
ber
of O
P vi
sits
an
d ea
rlie
r re
turn
to
wor
k•
Posi
tive
part
icip
ant
feed
back
on
ques
tionn
aire
• N
o st
atis
tical
ana
lysi
s
4
Parr
ott
et a
l40 r
epor
ted
on a
str
uctu
red
inpa
tient
exe
rcis
e pr
ogra
m t
hat
was
impl
emen
ted
for
20 a
dult
burn
sur
vivo
rs. T
his
grou
p’s
outc
omes
wer
e th
en c
ompa
red
with
a h
isto
rica
l con
trol
gr
oup.
The
y sh
owed
tha
t al
thou
gh t
he le
ngth
of s
tay
for
the
two
grou
ps w
ere
com
para
ble,
the
gro
up w
ho p
artic
ipat
ed in
the
str
uctu
red
exer
cise
pro
gram
req
uire
d le
ss o
utpa
tient
O
T/
PT v
isits
and
ret
urne
d to
wor
k so
oner
, alth
ough
no
stat
istic
al a
naly
ses
wer
e re
port
ed.
Tab
le 2
. (C
onti
nued
)
Aut
hors
Des
ign
Sam
ple
Out
com
e M
easu
res
Inte
rven
tion
Res
ults
Lev
el o
f E
vide
nce
(Con
tinu
ed )

Copyright © American Burn Association. Unauthorized reproduction of this article is prohibited.
Journal of Burn Care & Researche550 Nedelec et al November/December 2016
Porr
o et
al
(201
2)41
RC
T•
n =
222
(4 g
roup
s: O
x +
E
x =
14; O
x +
SOC
= 5
6;
P +
Ex
= 21
; P +
SO
C =
131
)•
Mea
n ag
e (y
rs):
Ox
+ E
x an
d
Ox
+ SO
C =
8; P
+ E
x an
d
P +
SOC
= 8
(ra
nge
0–18
)•
Mea
n %
TB
SAB
: Ox
+ E
x an
d O
x +
SOC
= 5
7; P
+ E
x an
d
P +
SOC
= 5
4
• R
EE
(Se
nsor
-Med
ics
Vm
ax
29 m
etab
olic
car
t)•
Hei
ght,
wei
ght
• W
hole
bod
y fa
t, L
BM
, bo
ne m
iner
al c
onte
nt,
bone
min
eral
den
sity
(D
EX
A)
• C
ardi
ac fu
nctio
n•
Sexu
al m
atur
atio
n•
Con
cent
ratio
n of
ser
um
infla
mm
ator
y cy
toki
nes,
ho
rmon
es, a
nd li
ver
enzy
mes
• St
reng
th (
Bio
dex
Syst
em-3
dy
nam
omet
er)
• E
valu
ated
at
adm
issi
on,
disc
harg
e, 6
, 9, 1
2, 1
8,
24, 3
6, 4
8, 6
0, a
nd 7
2 m
onth
s po
st-b
urn
• Sa
me
as P
rkzo
ra
et a
l (20
07)
NO
TE
: onl
y re
sults
rel
ated
to
exer
cise
rep
orte
d he
re•
Bon
e m
iner
al c
onte
nt s
igni
fican
tly
diff
ered
bet
wee
n O
x +
Ex
com
pare
d w
ith P
+ E
x gr
oup
• L
BM
sig
nific
antly
incr
ease
d in
Ox
+ E
x co
mpa
red
with
P +
Ex
grou
p at
24
to 7
2 m
os fo
llow
-up
• St
reng
th s
igni
fican
tly g
reat
er in
O
x +
Ex
grou
p co
mpa
red
with
al
l oth
er g
roup
s at
9, 1
2, 1
8,
and
24 m
os
2
In 2
012,
Por
ro e
t al
42 p
ublis
hed
a lo
ng-t
erm
follo
w u
p pa
per
to P
rzko
ra e
t al
’s12
200
7 ar
ticle
. Alth
ough
thi
s m
anus
crip
t di
d no
t di
rect
ly r
espo
nd t
o ou
r PI
CO
que
stio
n, s
ince
the
ir fo
cus
was
on
the
safe
ty a
nd e
ffica
cy o
f oxa
ndro
lone
, it
was
ret
aine
d si
nce
they
rep
orte
d on
the
long
-ter
m e
ffec
ts o
f oxa
ndro
lone
and
exe
rcis
e on
bon
e m
iner
al c
onte
nt, l
ean
body
mas
s, a
nd
stre
ngth
. The
ir lo
ng-t
erm
follo
w u
p re
sults
dem
onst
rate
d th
at t
he m
uscl
e st
reng
th o
f the
gro
up t
hat
rece
ived
oxa
ndro
lone
and
par
ticip
ated
in t
he e
xerc
ise
prog
ram
(Fi
gure
2)
was
si
gnifi
cant
ly g
reat
er t
han
the
othe
r th
ree
grou
ps a
t 9,
12,
18,
and
24
mon
th p
ost-
burn
. For
chi
ldre
n ag
ed 7
–18
year
s ol
d th
ere
was
a s
igni
fican
t di
ffer
ence
in b
one
min
eral
con
tent
and
L
BM
com
pare
d w
ith t
he e
xerc
ise
cont
rol g
roup
at
2 ye
ars
post
-bur
n an
d at
the
end
of t
he s
tudy
or
at 5
yea
rs p
ost-
burn
.Po
rro
et a
l (2
013)
42
RC
T•
n =
58 (
prop
rano
lol +
E
x =
27; E
x =
31)
• M
ean
age
(yrs
): P
ropr
anol
ol +
E
x =
13.7
; Ex
= 13
.1 (
rang
e 7–
18)
• M
ean
%T
BSA
B: P
ropr
anol
ol +
E
x =
60; E
x =
60•
Bas
elin
e: 6
mos
pos
t-bu
rn
• St
reng
th (
Bio
dex
Syst
em-3
dy
nam
omet
er)
• L
BM
(D
EX
A)
• Pe
ak o
xyge
n co
nsum
ptio
n (V
O2p
eak)
• Pr
opra
nolo
l: do
sage
tit
rate
d to
dec
reas
e re
stin
g he
art
rate
by
15–2
0% fr
om a
dmis
sion
va
lue
• E
x: (
Figu
re 2
)
• St
reng
th, L
BM
, VO
2pea
k all
sign
ifica
ntly
incr
ease
d w
ith
trea
tmen
t fo
r bo
th g
roup
s•
Sign
ifica
nt c
hang
e in
VO
2pea
k fo
r pr
opra
nolo
l + E
x co
mpa
red
with
Ex
• St
reng
th, L
BM
, VO
2pea
k per
cent
ch
ange
was
sig
nific
antly
hig
her
than
SO
C h
isto
ric
cont
rols
• N
o ad
vers
e ef
fect
s re
port
ed
2
(Con
tinu
ed )
Tab
le 2
. (C
onti
nued
)
Aut
hors
Des
ign
Sam
ple
Out
com
e M
easu
res
Inte
rven
tion
Res
ults
Lev
el o
f E
vide
nce

Copyright © American Burn Association. Unauthorized reproduction of this article is prohibited.
Journal of Burn Care & Research Volume 37, Number 6 Nedelec et al e551
In 2
013,
Por
ro e
t al
41 p
ublis
hed
a re
port
exa
min
ing
the
effe
cts
of p
ropr
anol
ol a
nd e
xerc
ise.
The
tw
o gr
oups
rec
eive
d pr
opra
nolo
l and
exe
rcis
e or
exe
rcis
e al
one
with
the
exe
rcis
e pr
ogra
m
desc
ribe
d in
Fig
ure
2. T
here
was
a s
igni
fican
t in
crea
se in
mus
cle
stre
ngth
, lea
n bo
dy m
ass,
and
VO
2pea
k aft
er t
he 1
2-w
eek
exer
cise
pro
gram
for
both
gro
ups
with
the
VO
2pea
k bei
ng
sign
ifica
ntly
hig
her
in t
he g
roup
rec
eivi
ng p
ropr
anol
ol c
ompa
red
with
exe
rcis
e al
one.
The
aut
hors
als
o co
mpa
red
both
gro
ups
to h
isto
ric
cont
rols
who
rec
eive
d SO
C b
ut d
id n
ot
part
icip
ate
in t
he e
xerc
ise
prog
ram
and
did
not
rec
eive
pro
pran
olol
and
foun
d th
e ex
erci
se g
roup
s ha
d si
gnifi
cant
ly g
reat
er p
erce
nt c
hang
e in
str
engt
h, le
an b
ody
mas
s an
d V
O2p
eak.
Pkzo
ra e
t al
(2
007)
12
RC
T•
n =
51 (
4 gr
oups
: Ox
+ E
x =
14;
Ox
+ SO
C =
9; P
+ E
x =
17; P
+
SOC
= 1
1),
• M
ean
age
(yrs
): O
x +
Ex
= 12
.1;
Ox
+ SO
C =
11.
8; P
+
Ex
= 10
.9; P
+ S
OC
= 1
1.8
(ran
ge 7
–18)
• M
ean
%T
BSA
B: O
x +
Ex
= 52
.1;
Ox
+ SO
C =
54.
7; P
+
Ex
= 55
.6; P
+ S
OC
= 5
1.6
• B
asel
ine:
6 m
os p
ost-
burn
• St
reng
th (
Bio
dex
Syst
em-3
dy
nam
omet
er•
Peak
oxy
gen
cons
umpt
ion
(VO
2pea
k)•
LB
M (
DE
XA
)•
Hor
mon
e pa
nel
• O
x or
P a
dmin
iste
red
disc
harg
e to
9
mos
pos
t-bu
rn•
SOC
: sam
e as
Sum
an
et a
l (20
03)
• E
x (F
igur
e 2)
NO
TE
: onl
y re
sults
rel
ated
to
exer
cise
rep
orte
d he
re.
• N
o ba
selin
e di
ffer
ence
s in
hei
ght,
w
eigh
t, L
BM
, str
engt
h, o
r V
O2p
eak
• W
eigh
t si
gnifi
cant
ly in
crea
sed
in
Ox
+ E
x gr
oup
com
pare
d w
ith a
ll ot
her
grou
ps a
nd fo
r O
x +
SOC
co
mpa
red
with
P +
SO
C•
LB
M s
how
ed a
sig
nific
ant
mea
n %
ch
ange
in E
x co
mpa
red
with
SO
C
grou
ps a
nd O
x +
SOC
and
P +
Ex
com
pare
d w
ith P
+ S
OC
• E
x gr
oups
sho
wed
sig
nific
antly
gr
eate
r in
crea
ses
in m
ean
%
stre
ngth
cha
nge
than
P +
SO
C•
VO
2pea
k mea
n %
cha
nge
sign
ifica
ntly
incr
ease
in E
x gr
oups
co
mpa
red
with
SO
C
2
Usi
ng t
he s
ame
desi
gn a
nd s
tudy
gro
ups
as S
uman
et
al,43
Prz
kora
et
al12
exa
min
ed t
he e
ffec
ts o
f oxa
ndro
lone
(in
stea
d of
rhG
H)
and
exer
cise
on
mus
cle
stre
ngth
and
car
diop
ulm
onar
y fit
ness
wer
e. T
here
was
a s
igni
fican
t in
crea
se in
bod
y w
eigh
t as
soci
ated
with
oxa
ndro
lone
and
exe
rcis
e co
mpa
red
with
the
oth
er t
hree
gro
ups
and
with
oxa
ndro
lone
alo
ne c
ompa
red
with
pla
cebo
. Lea
n bo
dy m
ass
show
ed a
sig
nific
ant
mea
n pe
rcen
t in
crea
se a
ssoc
iate
d w
ith o
xand
rolo
ne a
nd e
xerc
ise
com
pare
d w
ith t
he o
ther
thr
ee g
roup
s an
d w
ith o
xand
rolo
ne a
lone
co
mpa
red
with
pla
cebo
with
exe
rcis
e an
d pl
aceb
o w
ith S
OC
. Mus
cle
stre
ngth
sig
nific
antly
incr
ease
d in
all
grou
ps c
ompa
red
with
the
pla
cebo
and
SO
C. A
erob
ic c
apac
ity (
VO
2pea
k)
sign
ifica
ntly
incr
ease
d in
bot
h ex
erci
se g
roup
s co
mpa
red
with
the
SO
C g
roup
s su
gges
ting
that
oxa
ndro
lone
alo
ne h
as n
o de
mon
stra
ble
impa
ct o
n th
is v
aria
ble.
Sum
an e
t al
(2
002)
16
RC
T•
n =
51 (
Ex
= 17
; SO
C =
14,
he
alth
y =
20)
• M
ean
age
(yrs
): h
ealth
y =
12.6
; E
x =
10.6
; SO
C =
10.
7 (r
ange
7–
18)
• M
ean
%T
BSA
B: E
x =
59.8
; SO
C =
57.
2•
Bas
elin
e: 6
mos
pos
t-bu
rn
• Pu
lmon
ary
func
tion
(FE
V1.
0, F
VC
, max
vo
lunt
ary
vent
ilatio
n)•
Peak
oxy
gen
cons
umpt
ion
(VO
2pea
k)•
Tre
adm
ill t
ime
(mod
ified
B
ruce
pro
toco
l)
• 12
-wee
k tr
eatm
ent
peri
od•
SOC
: as
Sum
an e
t al
(2
001)
• E
x: F
igur
e 2
• A
ll ba
selin
e m
easu
res
of p
ulm
onar
y fu
nctio
n w
ere
sign
ifica
ntly
de
crea
sed
in b
urn
com
pare
d w
ith
heal
thy
child
ren
• Si
gnifi
cant
incr
ease
s in
pul
mon
ary
func
tion
and
VO
2pea
k in
Ex
grou
p af
ter
12/
52•
Sign
ifica
nt b
etw
een
grou
ps
diff
eren
ce fo
r m
ean
% c
hang
e in
max
vol
unta
ry v
entil
atio
n,
trea
dmill
tim
e, a
nd V
O2p
eak
2
(Con
tinu
ed )
Tab
le 2
. (C
onti
nued
)
Aut
hors
Des
ign
Sam
ple
Out
com
e M
easu
res
Inte
rven
tion
Res
ults
Lev
el o
f E
vide
nce

Copyright © American Burn Association. Unauthorized reproduction of this article is prohibited.
Journal of Burn Care & Researche552 Nedelec et al November/December 2016
In 2
002,
Sum
an e
t al
16 p
ublis
hed
a st
udy
exam
inin
g th
e ef
fect
of e
xerc
ise
trai
ning
(Fi
gure
2)
com
pare
d w
ith S
OC
on
pulm
onar
y fu
nctio
n. T
he p
edia
tric
bur
n su
rviv
ors
wer
e ra
ndom
ly
assi
gned
to
the
exer
cise
gro
up o
r th
e SO
C g
roup
and
a g
roup
of n
onbu
rn c
hild
ren
wer
e in
clud
ed a
s a
com
pari
son
grou
p. A
t ba
selin
e, t
he e
xerc
ise
and
SOC
gro
up d
id n
ot d
iffer
w
ith r
espe
ct t
o ag
e, p
erce
nt b
urn
surf
ace
area
, hei
ght,
wei
ght,
and
bod
y su
rfac
e ar
ea b
ut t
he n
on-b
urn
grou
ps w
ere
sign
ifica
ntly
hea
vier
. Bas
elin
e pu
lmon
ary
func
tion
was
nor
mal
for
the
nonb
urn
grou
p an
d th
ere
was
no
diff
eren
ce in
pul
mon
ary
func
tion
betw
een
the
exer
cise
and
SO
C g
roup
. How
ever
, all
pulm
onar
y fu
nctio
n te
sts
wer
e si
gnifi
cant
ly lo
wer
in t
he
exer
cise
and
SO
C g
roup
s co
mpa
red
with
the
non
burn
chi
ldre
n. A
fter
12
wee
ks o
f exe
rcis
e th
ere
was
a s
igni
fican
t in
crea
se in
FE
V1,
FV
C a
nd M
VV
with
a s
igni
fican
t be
twee
n gr
oup
diff
eren
ce (
exer
cise
vs
SOC
) fo
r M
VV,
tre
adm
ill t
ime,
and
VO
2pea
k.Su
man
et
al
(200
1)32
RC
T•
n =
35 (
Ex
= 19
; SO
C =
16)
• M
ean
age
(yrs
): E
x =
10.5
; SO
C =
11
• M
ean
%T
BSA
B: E
x =
59.4
; SO
C =
58.
0•
Bas
elin
e: 6
mos
pos
t-bu
rn
• H
eigh
t, w
eigh
t•
Stre
ngth
(C
ybex
dy
nam
omet
er)
• L
BM
(D
EX
A)
• Pe
ak o
xyge
n co
nsum
ptio
n (V
O2p
eak)
• R
EE
(m
etab
olic
car
t)•
Eva
luat
ed a
t ba
selin
e an
d 12
wee
ks la
ter
(6 a
nd 9
m
os p
ost-
burn
)
• 12
-wee
k tr
eatm
ent
peri
od•
SOC
: OP
OT
&
PT 2
x/d
x 1
hr•
Ex:
(Fi
gure
2)
• Si
gnifi
cant
cha
nge
with
trea
tmen
t: E
x gr
oup
– m
ean
incr
ease
d ch
ange
pe
ak to
rque
, tot
al w
ork,
ave
rage
po
wer
, LB
M, V
O2p
eak,
peak
tr
eadm
ill ti
me;
SO
C g
roup
– R
EE
sig
nific
antly
incr
ease
d fr
om b
asel
ine
• Si
gnifi
cant
bet
wee
n gr
oup
diff
eren
ces:
mea
n ch
ange
pea
k to
rque
, tot
al w
ork,
ave
rage
wor
k,
LB
M, c
hang
e in
tre
adm
ill t
ime,
V
O2p
eak
2
Sum
an e
t al
32 s
tudi
ed t
he e
ffec
t of
a 1
2-w
eek
exer
cise
pro
gram
(Fi
gure
2)
com
pare
d w
ith S
OC
on
pedi
atri
c bu
rn s
urvi
vors
str
engt
h, t
otal
wor
k av
erag
e po
wer
, LB
M, p
eak
trea
dmill
tim
e, a
nd p
eak
oxyg
en c
onsu
mpt
ion
(VO
2pea
k). S
ubje
cts
wer
e ra
ndom
ly a
ssig
ned
eith
er t
o th
e ex
erci
se g
roup
or
the
SOC
gro
up. T
hey
foun
d a
sign
ifica
nt im
prov
emen
t in
all
of t
hese
pa
ram
eter
s, in
the
exe
rcis
e gr
oup
and
a si
gnifi
cant
impr
ovem
ent
in t
ime
whe
n co
mpa
ring
bet
wee
n th
e ex
erci
se a
nd t
he S
OC
gro
up.
Sum
an e
t al
(2
003)
43
RC
T•
n =
44 (
GH
+ E
x =
10;
P +
Ex
= 13
; GH
+
SOC
= 1
0; P
+ S
OC
= 1
1)•
Mea
n ag
e (y
rs):
GH
+ E
x =
11.0
; P
+ E
x =
10.5
; GH
+
SOC
= 1
1.5;
P +
SO
C =
10.
8 (r
ange
: 7–1
7)•
Mea
n %
TB
SAB
: GH
+
Ex
= 60
.3; P
+ E
x =
58.5
; GH
+
SOC
= 5
5.9;
P +
SO
C =
53.
4•
Bas
elin
e: 6
mos
pos
t-bu
rn
• H
eigh
t, w
eigh
t•
Stre
ngth
(B
iode
x Sy
stem
-3
dyna
mom
eter
)•
LB
M (
DE
XA
)•
Fat-
free
mas
s (w
hole
bo
dy p
otas
sium
)•
Peak
oxy
gen
cons
umpt
ion
(VO
2pea
k)•
Hor
mon
e pa
nel
• E
valu
ated
at
base
line
and
12 w
eeks
late
r (6
and
9
mos
pos
t-bu
rn)
• rh
GH
or
P ad
min
iste
red
post
-di
scha
rge
• SO
C: s
ame
as
Sum
an e
t al
(20
01)
• E
x: F
igur
e 2
NO
TE
: onl
y re
sults
rel
ated
to
exer
cise
rep
orte
d he
re•
No
diff
eren
ces
heig
ht &
wei
ght
betw
een
6 an
d 9
mos
pos
t-bu
rn•
LB
M in
crea
sed
sign
ifica
ntly
aft
er
12/
52 in
all
grou
ps e
xcep
t
P +
SOC
• N
o si
gnifi
cant
diff
eren
ce in
fat-
free
m
ass
at b
asel
ine
or a
fter
12/
52•
Stre
ngth
(pe
ak t
orqu
e) in
crea
sed
sign
ifica
ntly
for
GH
+ E
x, P
+ E
x,
GH
+ S
OC
, and
P +
SO
C•
VO
2pea
k inc
reas
ed s
igni
fican
tly fo
r G
H +
Ex
and
P +
Ex
but
not
for
GH
+ S
OC
or
P +
SOC
• N
o si
de e
ffec
ts n
oted
with
ad
min
istr
atio
n of
GH
2
(Con
tinu
ed )
Tab
le 2
. (C
onti
nued
)
Aut
hors
Des
ign
Sam
ple
Out
com
e M
easu
res
Inte
rven
tion
Res
ults
Lev
el o
f E
vide
nce

Copyright © American Burn Association. Unauthorized reproduction of this article is prohibited.
Journal of Burn Care & Research Volume 37, Number 6 Nedelec et al e553
In 2
003,
Sum
an e
t al
43 p
ublis
hed
a re
port
exa
min
ing
the
effe
ct o
f exo
geno
us g
row
th h
orm
one
and
exer
cise
on
LB
M a
nd m
uscl
e st
reng
th. B
urne
d ch
ildre
n w
ere
rand
omly
ass
igne
d to
fo
ur g
roup
s 1
day
befo
re b
eing
dis
char
ged
from
hos
pita
l: (1
) th
ose
who
rec
eive
d re
com
bina
nt h
uman
gro
wth
hor
mon
e (r
hGH
) an
d pa
rtic
ipat
ed in
the
exe
rcis
e pr
ogra
m (
Figu
re 2
) th
at w
as in
itiat
ed 6
mon
ths
post
-dis
char
ge, (
2) t
hose
who
rec
eive
d rh
GH
and
SO
C, (
3) t
hose
who
rec
eive
d sa
line
plac
ebo
and
part
icip
ated
in t
he e
xerc
ise
prog
ram
tha
t w
as in
itiat
ed
6 m
onth
s po
st-d
isch
arge
, and
(4)
tho
se w
ho r
ecei
ved
salin
e pl
aceb
o an
d SO
C. D
urin
g th
e 12
-wee
k pe
riod
, the
re w
as a
sig
nific
ant
incr
ease
in L
BM
for
all g
roup
s, w
ith t
he e
xcep
tion
of t
he g
roup
tha
t re
ceiv
ed t
he p
lace
bo a
nd S
OC
, but
the
re w
as n
o be
twee
n gr
oup
diff
eren
ces.
Str
engt
h an
d V
O2p
eak s
igni
fican
tly in
crea
sed
in t
he t
wo
exer
cise
gro
ups
but
was
not
si
gnifi
cant
ly im
pact
ed b
y gr
owth
hor
mon
e ad
min
istr
atio
n.Su
man
et
al
(200
7)44
RC
T•
n =
20 (
Ex
= 9;
SO
C =
11;
he
alth
y =
26)
• M
ean
age
(yrs
): E
x =
11.8
; SO
C =
13.
4; h
ealth
y =
13.5
(r
ange
7–1
7)•
Mea
n %
TB
SAB
: Ex
= 61
; SO
C =
56
• B
asel
ine:
6 m
os p
ost-
burn
• H
eigh
t, w
eigh
t•
LB
M (
DE
XA
)•
Stre
ngth
(B
iode
x Sy
stem
-3
dyna
mom
eter
) E
valu
ated
at
bas
elin
e an
d 12
wee
ks
late
r an
d 3
mos
aft
er
exer
cise
ces
satio
n (6
, 9,
and
12 m
os p
ost-
burn
)
• 12
-wee
k tr
eatm
ent
peri
od (
6 to
9 m
os
post
-bur
n) t
hen
3 m
onth
follo
w-u
p (1
2 m
os p
ost-
burn
)•
SOC
: sam
e as
Sum
an
et a
l (20
03)
• E
x: F
igur
e 2
• Si
gnifi
cant
wei
ght
gain
in t
he E
x gr
oup
only
bet
wee
n 6
and
9 m
os•
LB
M m
ean
% c
hang
e: s
igni
fican
tly
incr
ease
d be
twee
n 6
and
9 m
onth
s in
the
Ex
grou
p bu
t no
t th
e SO
C
grou
p; c
ontin
ued
to s
igni
fican
tly
incr
ease
at
the
12 m
onth
s fo
llow
up
in t
he E
x gr
oup
com
pare
d w
ith
the
SOC
gro
up•
Stre
ngth
mea
n %
cha
nge:
si
gnifi
cant
ly in
crea
sed
in t
he
Ex
grou
p co
mpa
red
with
SO
C;
cont
inue
d to
incr
ease
at
the
12
mon
ths
follo
w-u
p in
the
Ex
grou
p co
mpa
red
with
SO
C b
ut t
his
was
no
t st
atis
tical
ly s
igni
fican
t no
r w
ere
ther
e an
y gr
oup
diff
eren
ces
2
In 2
007,
Sum
an e
t al
44 e
xam
ined
the
long
-ter
m e
ffec
t af
ter
stop
ping
the
12-
wee
k ex
erci
se p
rogr
am. T
he s
tudy
des
ign
was
sim
ilar
to t
heir
200
1 st
udy32
with
the
add
ition
of a
follo
w-u
p ev
alua
tion
3 m
onth
s af
ter
exer
cise
ces
satio
n (1
2 m
onth
s po
st-b
urn)
. The
aut
hors
rep
orte
d th
at L
BM
and
str
engt
h in
crea
sed
duri
ng t
he 1
2 w
eek
exer
cise
pro
gram
for
the
exer
cise
gr
oup
com
pare
d w
ith t
he S
OC
and
con
tinue
d to
impr
ove
afte
r th
e pr
ogra
m s
topp
ed b
ut t
his
late
r im
prov
emen
t w
as n
ot s
igni
fican
t.
AD
L, a
ctiv
ities
of
daily
livi
ng;
AR
OM
, ac
tive
rang
e of
mot
ion;
BM
I, b
ody
mas
s in
dex;
BSH
S-A
, bu
rn-s
peci
fic h
ealth
sca
le –
abb
revi
ated
; B
SHS-
B,
burn
-spe
cific
hea
lth s
cale
– b
rief
; C
, co
ntro
l; C
OPM
, C
anad
ian
Occ
upat
iona
l Per
form
ance
Mea
sure
; d, d
ay; D
EX
A, d
ual-
ener
gy X
-ray
abs
orpt
iom
etry
; Ex,
exe
rcis
e; ex
t, e
xten
sion
; FE
V1.
0, fo
rced
exp
irat
ory
volu
me;
flex
, flex
ion;
FV
C, f
orce
d vi
tal c
apac
ity; G
H, g
row
th h
orm
one;
hr,
ho
ur; I
GF-
1, in
sulin
-lik
e gr
owth
fact
or-1
; IG
FBP-
3, in
sulin
-lik
e gr
owth
fact
or b
indi
ng p
rote
in-3
; IP,
inpa
tient
; LB
M, l
ean
body
mas
s; L
E, l
ower
ext
rem
ity; L
EFS
, low
er e
xtre
mity
func
tiona
l sca
le; L
OS,
leng
th o
f sta
y;
mos
, mon
ths;
max
, max
imum
; MW
T, m
inut
e w
alk
test
; MSW
T, m
odifi
ed s
hutt
le w
alk
test
; n, s
ampl
e si
ze n
umbe
r; O
P, o
utpa
tient
; OT
, occ
upat
iona
l the
rapy
; Ox,
oxa
ndro
lone
; P, p
lace
bo; P
T, p
hysi
othe
rapy
; RC
T,
rand
omiz
ed c
ontr
olle
d tr
ials
; RE
E, r
estin
g en
ergy
exp
endi
ture
; rep
s, re
petit
ions
; RO
M, r
ange
of m
otio
n; S
F-36
, Med
ical
Out
com
es S
tudy
36-
Item
Sho
rt F
orm
; SO
C, s
tand
ard
of c
are;
TB
SAB
, tot
al b
ody
surf
ace
area
bu
rned
; UE
, upp
er e
xtre
mity
, VO
2pea
k, pe
ak O
2 co
nsum
ptio
n; v
s, ve
rsus
; ×, t
imes
; W&
E, W
elln
ess
and
Exe
rcis
e; W
BV
, who
le b
ody
vibr
atio
n; W
TQ
, wor
k-to
-quo
ta; W
TT
, wor
k-to
-tol
eran
ce; y
rs, y
ears
; ×/5
2, n
umbe
r of
wee
ks; #
, num
ber;
3R
M, t
hree
rep
etiti
on m
axim
um; °
/s, d
egre
es p
er s
econ
d.In
all
case
s si
gnifi
cant
cha
nges
ref
ers
to a
rep
orte
d P
valu
e of
<0.
05.
Tab
le 2
. (C
onti
nued
)
Aut
hors
Des
ign
Sam
ple
Out
com
e M
easu
res
Inte
rven
tion
Res
ults
Lev
el o
f E
vide
nce

Copyright © American Burn Association. Unauthorized reproduction of this article is prohibited.
Journal of Burn Care & Researche554 Nedelec et al November/December 2016
are more commonly accessible to clinicians will be thoroughly reviewed to facilitate rehabilitation pro-fessionals’ ability to document baseline values and outcomes postintervention.
For studies that measured aerobic capacity the vast majority used a modified Bruce Protocol.45 As out-lined in Figure 2, this is a standard procedure for ambulatory stress testing that begins at 2.7 kilome-ter/hr (1.7 mph) at 0% grade. The workload was then increased every 3 min by increasing the speed and/or grade. The maximum35 or peak oxygen con-sumption12,16,20,32,38,39,41,43 was then calculated. Since the Bruce protocol requires expensive equipment, a validated equation has been generated for children to predict maximal aerobic capacity using treadmill time46 offering a clinically accessible option. Pre-dictive equations for estimating VO2max have been developed for adults and can be used with the origi-nal or modified tests.47 Bruce et al45 developed the first predictive equations, which are population spe-cific for active and sedentary adults with and without cardiac conditions, but to the best of our knowledge these have not specifically been tested with adult burn survivors. For the adult burn survivor popula-tion, the modified shuttle walk test has been recom-mended to evaluate cardiovascular fitness48 and has been validated as a clinically accessible, safe evalua-tion for monitoring aerobic capacity during the early postacute discharge rehabilitation phase.49
For studies that measured strength the vast major-ity used an isokinetic, computerized dynamometer.
The testing was most commonly performed on the dominant leg extensors at an angular velocity of 30°/sec,30 60°/sec,20,33 90°/sec,30,32 120°/sec,39 or 150°/sec.12,14,19,31,35,36,38,41,43,44 The only study that used two different angular velocities and reported specific outcome showed improvements with time for both measures, but the between group differ-ences were significant for both eccentric and con-centric measures at 30°/sec but only the eccentric measures at 90°/sec.30 However, the impact of performing the prescribed exercise program on the same equipment used for testing is unknown. To the best of our knowledge, there are no studies exam-ining the clinimetric advantages or disadvantages of using a particular angular velocity or concentric vs eccentric contractions when evaluating burn survi-vors. However, isokinetic computerized dynamome-ters are not always clinically feasible but some studies used more commonly accessible equipment, such as 3RM using free weights34,39 or grip strength dyna-mometer39 to evaluate strength outcomes.
Other related clinical outcomes that benefited from exercise programs included the Burn Specific Health Scale (BSHS)-abbreviated,39 the Canadian Occupa-tional Performance Measure,20 gait parameters,14,19 lower extremity functional scale,39 quad size,14 the QuickDASH,39 resting heart rate,34 6-minute walk test,34 and weight,12,31,34 all of which are clinically acces-sible. The BSHS-brief, the SF-36,28 the Child Health Questionnaire,29 and the need for surgical release26 were also used in studies that were excluded from full review.
Progressive Resistive Training Aerobic Conditioning Program
Baseline evaluation Baseline evaluation
Instruct in correct weight lifting techniqueWarm up with lever arm and bar or wooden dowel
Attempt to lift a weight 4 timesIf successful, with correct technique, 1 min rest
Lift progressively increased amountContinue until unable to perform 4th repetition
Final weight/load=3RM
Standardized treadmill exercise test (modified Bruce Protocol)
Oxygen consumption and heart rate measuredBegin to walk on treadmill 1.7 mph 0% grade
3-minute intervals - increase speed and inclineVO2peak=respiratory exchange ratio≥1.10 and peak
volitional effort achieved
Resistance Exercises Aerobic Exercises
Eight exercises: bench press, leg squats, shoulder press, leg press, biceps curl, leg curl, triceps curl,
toe raises
1st week: 50-60% 3RM 4-10 reps x 3 sets2nd-6th week: 70-75% 3RM 4-10 reps x 3 sets7th-12th week: 80-85% 3RM 8-12 reps x 3 sets
1 minute rest between sets
5 minutes warm up (<50% treadmill or cycle ergometer VO2peak)
30 minutes(70-85% treadmill or cycle ergometer VO2peak)
5 minutes cool down (<50% treadmill or cycle ergometer VO2peak)
30 minutes/3 non-consecutive days/week x 12 weeks
30 minutes/5 days/week x 12 weeks
Figure 2. Progressive resistive training and aerobic conditioning program evaluation and training program details in Galves-ton studies.

Copyright © American Burn Association. Unauthorized reproduction of this article is prohibited.
Journal of Burn Care & Research Volume 37, Number 6 Nedelec et al e555
Exercise Program PrescriptionWhen reported, the exercise training programs were either 6,30 8,36 or 12 weeks12,14,16,19,20,31,32,34,35,37–39,41–44 in length and all but one were initiated after dis-charge from the acute care center.40 Since the later report was published in 1988 and considering the accelerated rate at which patients are discharged from hospital since then the feasibility and applicability of prescribing a similar conditioning and strengthening program during the acute care stay at the present moment would be questionable. Thus, at this point, the evidence supporting the prescription of exercise programs to increase muscle strength or cardiovas-cular fitness is applied after the burn survivor has been discharged from the acute care center.
The specifics of the training programs for the stud-ies performed in Galveston12,16,31,32,34,38,41–44 were similar across the studies and have been described in Figure 2. Some exercise resistance training programs used the isokinetic dynamometer as the basis of the training program.14,19,20,30,37,38 Whole body vibration was also used for lower extremity strengthening.36 Several studies also incorporated functional activi-ties into their strengthening or cardiovascular fitness programs.20,37,40
All studies that included an aerobic condition-ing program included treadmill or cycle ergometer training12,16,20,31,32,34,35,37–44 although one study did not provide any details.33 One study examined an aero-bic conditioning or cardiovascular retraining program that had participants work to quota or to tolerance on a treadmill. Although they reported an improvement across time for both groups compared with the SOC group there was no difference between those assigned to work to quota vs work to tolerance.35
Standard of Care RegimensFor those studies that compared with a SOC treat-ment regime there was enormous variation in the details reported. Some provided no details at all, others provided a list of different types of interven-tions but no details with respect to treatment param-eters (intensity, frequency, or duration) and others provided hours/day. None of the studies appear to monitor the SOC that was delivered using monitor-ing tools, such as treatment diaries. Future studies would benefit from more thorough documentation and monitoring of the SOC received by both groups.
DISCUSSION
The objective of this review was to systematically appraise the available evidence with regards to the
use of exercise programs to increase the cardiovas-cular fitness or muscle strength of pediatric or adult burn survivors so that rehabilitation-specific clinical practice guidelines could be generated. Twenty stud-ies were included in this review of which 11 were RCTs that included pediatric burn survivors and three were RCTs that included adult burn survivors. There has been one systematic review50 that com-bined the pediatric and adult evidence. This review was excluded from the analysis to allow for a system-atic critique of the original articles. All of the evi-dence incorporated in this review reported improved cardiovascular fitness and/or muscle strength with no identified adverse effects. However, it should be noted that a thorough review of the literature evaluating heat intolerance was not incorporated into this review so caution should be exercised when performing exercise programs in hot and/or humid environments. In addition, the literature evaluat-ing the potential overall benefit of propranolol, growth hormone, and oxandrolone was not thor-oughly reviewed as prescription of these medications is not the responsibility of rehabilitation thera-pists. Although improvements in aerobic capacity with propranolol administration41 and significantly greater increases in strength with growth hormone43 or oxandrolone administration combined with exer-cise12 have been noted in the literature; no conclu-sions were made with respect to their overall benefit in this review. Overall, there is strong evidence to support the prescription of resistance and aerobic exercise training programs for burn survivors. None-theless there are some methodological issues that should be considered and gaps in the literature that need to be addressed in future studies.
With respect to the pediatric literature 10 of the 11, RCTs were performed at the Shriners Hospital for Children in Galveston. The strength of this lit-erature is the fact that a wide variety of outcomes were evaluated using a consistent exercise regimen (Table 2). The results of all of these investigations have been positive demonstrating that exercise pro-grams enhance cardiovascular fitness and muscle strength when they are initiated immediately post-discharge or if initiated 6 months postdischarge and that there continues to be measurable exercise ben-efits for at least 3 months after the exercise program has been discontinued.42,44 The limitation associated with the majority of literature coming from one cen-ter is that there is a potential lack of generalizabil-ity to other populations. In addition, many of the studies of Galveston are part of a larger project with “rolling” enrollment (personal communication O.E. Suman September 2014); therefore, the participants

Copyright © American Burn Association. Unauthorized reproduction of this article is prohibited.
Journal of Burn Care & Researche556 Nedelec et al November/December 2016
included in the publications may or may not include distinct populations of participants.
It must also be kept in mind that all of the pediatric exercise programs reported in the literature were 12 week in-hospital programs that in addition included SOC treatment provided by other burn team mem-bers including OTs, PTs, and psychologists, which were then compared with outpatient or home-based programs. Community therapists who provided the outpatient treatment may not have specific expertise in treating burn survivors, their dedicated time for face-to-face treatment may have been limited, there may have been limited access to a variety of health professionals and the adherence rates of these com-munity or home-based programs were not reported, all of which may bring into question whether the SOC component was equivalent between groups. Thus, the benefits attributed to the exercise pro-grams may partially reflect the added value of an in-hospital, highly specialized inter-professional burn care team. All of the burn survivors recruited also had very large surface area burns (greater than 40% TBSA in all except one report which was greater than 30%) that are significantly larger burns than the average burn injury.50 Studies from a variety of burn rehabilitation settings that investigate whether the same benefits are seen with smaller burn injuries are also needed.
In addition, all of the evidence in the literature has employed an in-hospital exercise program and the majority of these regimens have been 30 minutes per day, 3 days per week for 12 weeks. It would be valu-able to determine if the total dosage of exercise could be concentrated in shorter time period (ie, 5 days per week for 45 minutes for 2 weeks) or whether spread-ing it across time (ie, 3 days per week for 15 minutes for 10 weeks) is equally as beneficial. It would also be valuable to determine if the benefits of a community-based program would have comparable benefits to the in-hospital programs. Finally, evaluation of the long-term benefits of these programs and the extent to which the participants chose to, or are required to, continue these exercise regimes to maintain the benefits gained would provide additional guidance.
AREAS FOR FUTURE INVESTIGATION
There are a number of research questions that would be important to address in future investigations.
It would be extremely valuable to determine whether community-based exercise facilities would be able to provide exercise training programs for burn survivors that have the same reported benefits
as the in-hospital programs described in the litera-ture or whether the expertise and environment asso-ciated with a burn center is a critical component of the success of these exercise programs.
There have been a number of studies initiated at different time points after burn that confirm that there are benefits to exercise programs initiated immediately postdischarge from acute care as well as 6 months or later post-discharge. It would be beneficial to further investigate whether there is an ideal time point to initi-ate these programs and whether the exercise program cessation results in a loss of the gained benefits at an equal rate to healthy control subject. Several stud-ies of adult subjects36,37 demonstrated that the burn survivors were able to increase their strength to levels comparable with the gains demonstrated by healthy controls performing the same exercise program, but long-term follow-up was not performed therefore it is unknown whether they were able to maintain the strength gains after exercise cessation to the same extent as healthy controls. It would also be beneficial to further investigate the effect of isokinetic training at various speeds in both adults and children.
Most of the studies recruited participants with moderate to large surface area burns (40% TBSA or greater). It would be important to determine the extent of the problem with smaller burn injuries as well as the benefits of these exercise programs with this population.
Further investigations of the impact of cardio-vascular endurance and strengthening programs on other outcomes, such as return to work, quality of life, community reintegration, and the need for reconstructive surgery would be particularly benefi-cial in the adult population.
ACKNOWLEDGMENTSThe editorial assistance of Suzana Anjos, Research Support Office, Research Centre, CHUM is gratefully acknowl-edged. Additional librarian support from Diane Monheit, Shriners Hospitals for Children, Northern California is gratefully acknowledged.
REFERENCES
1. Howick J, Chalmers I, Glasziou P, et al; Oxford Centre for Evidence-Based Medicine Working Group. The Oxford 2011 Levels of Evidence. 2011. http://www.cebm.net/in-dex.aspx?o=5653. Accessed September 12, 2013.
2. Bloemsma GC, Dokter J, Boxma H, Oen IM. Mortality and causes of death in a burn centre. Burns 2008;34:1103–7.
3. Muller MJ, Pegg SP, Rule MR. Determinants of death fol-lowing burn injury. Br J Surg 2001;88:583–7.
4. Saffle JR, Davis B, Williams P. Recent outcomes in the treat-ment of burn injury in the United States: a report from the

Copyright © American Burn Association. Unauthorized reproduction of this article is prohibited.
Journal of Burn Care & Research Volume 37, Number 6 Nedelec et al e557
American Burn Association Patient Registry. J Burn Care Rehabil 1995;16(3 Pt 1):219–32; discussion 288–9.
5. Pruitt BA Wolf SE Mason AD. Epidemiological, demograph-ic, and outcome characterisitcs of burn injury. Chapter 3. In: Herndon DN, editors. Total burn care. 3rd ed. Philadelphia, PA: Saunders Elsevier; 2007.
6. Esselman PC, Thombs BD, Magyar-Russell G, Fauerbach JA. Burn rehabilitation: state of the science. Am J Phys Med Rehabil 2006;85:383–413.
7. Richard R, Baryza MJ, Carr JA, et al. Burn rehabilitation and research: proceedings of a consensus summit. J Burn Care Res 2009;30:543–73.
8. Hasselgren PO. Burns and metabolism. J Am Coll Surg 1999;188:98–103.
9. Pereira C, Murphy K, Jeschke M, Herndon DN. Post burn muscle wasting and the effects of treatments. Int J Biochem Cell Biol 2005;37:1948–61.
10. Hart DW, Wolf SE, Mlcak R, et al. Persistence of muscle catabolism after severe burn. Surgery 2000;128:312–9.
11. Jeschke MG, Chinkes DL, Finnerty CC, et al. Pathophysiologic response to severe burn injury. Ann Surg 2008;248:387–401.
12. Przkora R, Herndon DN, Suman OE. The effects of oxan-drolone and exercise on muscle mass and function in chil-dren with severe burns. Pediatrics 2007;119:e109–16.
13. Alloju SM, Herndon DN, McEntire SJ, Suman OE. Assessment of muscle function in severely burned children. Burns 2008;34:452–9.
14. Ebid AA, El-Shamy SM, Draz AH. Effect of isokinetic training on muscle strength, size and gait after healed pediatric burn: a randomized controlled study. Burns 2014;40:97–105.
15. Desai MH, Mlcak RP, Robinson E, et al. Does inhalation injury limit exercise endurance in children convalescing from thermal injury? J Burn Care Rehabil 1993;14:16–20.
16. Suman OE, Mlcak RP, Herndon DN. Effect of exercise training on pulmonary function in children with thermal in-jury. J Burn Care Rehabil 2002;23:288–93; discussion 287.
17. Willis CE, Grisbrook TL, Elliott CM, Wood FM, Wallman KE, Reid SL. Pulmonary function, exercise capacity and physical activity participation in adults following burn. Burns 2011;37:1326–33.
18. Ganio MS, Pearson J, Schlader ZJ, et al. Aerobic fitness is disproportionately low in adult burn survivors years after in-jury. J Burn Care Res 2014 [Epub ahead of print].
19. Ebid AA, Omar MT, Abd El Baky AM. Effect of 12-week isokinetic training on muscle strength in adult with healed thermal burn. Burns 2012;38:61–8.
20. Grisbrook TL, Wallman KE, Elliott CM, Wood FM, Edgar DW, Reid SL. The effect of exercise training on pulmonary function and aerobic capacity in adults with burn. Burns 2012;38:607–13.
21. St-Pierre DM, Choinière M, Forget R, Garrel DR. Muscle strength in individuals with healed burns. Arch Phys Med Rehabil 1998;79:155–61.
22. Black S, Carter GM, Nitz AJ, Worthington JA. Oxygen con-sumption for lower extremity exercises in normal subjects and burned patients. Phys Ther 1980;60:1255–8.
23. Bowker R, Lakhanpaul M, Atkinson M, Armon K, MacFaul R, Stephenson T. How to write a guideline from start to finish: a handbook for healthcare professionals. Toronto, Canada: Elsevier; 2008.
24. Moher D, Liberati A, Tetzlaff J, Altman DG; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med 2009;6:e1000097.
25. Law M, Stewart D, Pollock N, Letts L, Bosch J, Westmorland M. McMaster University 1998. Available at: http://www.srs-mcmaster.ca/ResearchResourcesnbsp/ResearchGroups/CentreforEvidenceBasedRehabilitation/EvidenceBasedPracticeResearchGroup/tabid/630/Default.asp. Accessed November 14, 2013.
26. Celis MM, Suman OE, Huang TT, Yen P, Herndon DN. Effect of a supervised exercise and physiotherapy program on surgical interventions in children with thermal injury. J Burn Care Rehabil 2003;24:57–61; discussion 56.
27. Demling RH, DeSanti L. Oxandrolone induced lean mass gain during recovery from severe burns is main-tained after discontinuation of the anabolic steroid. Burns 2003;29:793–7.
28. Grisbrook TL, Reid SL, Edgar DW, Wallman KE, Wood FM, Elliott CM. Exercise training to improve health related quality of life in long term survivors of major burn injury: a matched controlled study. Burns 2012;38:1165–73.
29. Rosenberg M, Celis MM, Meyer W 3rd, et al. Effects of a hospital based wellness and exercise program on quality of life of children with severe burns. Burns 2013;39:599–609.
30. Ahmed ET, Abdel-aziem AA, Ebid AA. Effect of isokinetic training on quadriceps peak torgue in healthy subjects and patients with burn injury. J Rehabil Med 2011;43:930–4.
31. Al-Mousawi AM, Williams FN, Mlcak RP, Jeschke MG, Herndon DN, Suman OE. Effects of exercise training on resting energy expenditure and lean mass during pediatric burn rehabilitation. J Burn Care Res 2010;31:400–8.
32. Suman OE, Spies RJ, Celis MM, Mlcak RP, Herndon DN. Effects of a 12-wk resistance exercise program on skel-etal muscle strength in children with burn injuries. J Appl Physiol (1985) 2001;91:1168–75.
33. Cronan T, Hammond J, Ward CG. The value of isokinetic exercise and testing in burn rehabilitation and determination of back-to-work status. J Burn Care Rehabil 1990;11:224–7.
34. Cucuzzo NA, Ferrando A, Herndon DN. The effects of exercise programming vs traditional outpatient therapy in the rehabilitation of severely burned children. J Burn Care Rehabil 2001;22:214–20.
35. de Lateur BJ, Magyar-Russell G, Bresnick MG, et al. Augmented exercise in the treatment of deconditioning from major burn injury. Arch Phys Med Rehabil 2007;88(12 Suppl 2):S18–23.
36. Ebid AA, Ahmed MT, Mahmoud Eid M, Mohamed MS. Effect of whole body vibration on leg muscle strength af-ter healed burns: a randomized controlled trial. Burns 2012;38:1019–26.
37. Grisbrook TL, Elliott CM, Edgar DW, Wallman KE, Wood FM, Reid SL. Burn-injured adults with long term functional impairments demonstrate the same response to resistance training as uninjured controls. Burns 2013;39:680–6.
38. Hardee JP, Porter C, Sidossis LS, et al. Early rehabilitative exercise training in the recovery from pediatric burn. Med Sci Sports Exerc 2014;46:1710–6.
39. Paratz JD, Stockton K, Plaza A, Muller M, Boots RJ. Intensive exercise after thermal injury improves physical, functional, and psychological outcomes. J Trauma Acute Care Surg 2012;73:186–94.
40. Parrott M, Ryan R, Parks DH, Wainwright DJ. Structured exercise circuit program for burn patients. J Burn Care Rehabil 1988;9:666–8.
41. Porro LJ, Herndon DN, Rodriguez NA, et al. Five-year outcomes after oxandrolone administration in severely burned children: a randomized clinical trial of safety and efficacy. J Am Coll Surg 2012;214:489–502; discussion 502–4.
42. Porro LJ, Al-Mousawi AM, Williams F, Herndon DN, Mlcak RP, Suman OE. Effects of propranolol and exercise training in children with severe burns. J Pediatr 2013;162:799–803.e1.
43. Suman OE, Thomas SJ, Wilkins JP, Mlcak RP, Herndon DN. Effect of exogenous growth hormone and exercise on lean mass and muscle function in children with burns. J Appl Physiol (1985) 2003;94:2273–81.
44. Suman OE, Herndon DN. Effects of cessation of a struc-tured and supervised exercise conditioning program on lean mass and muscle strength in severely burned children. Arch Phys Med Rehabil 2007;88(12 Suppl 2):S24–9.
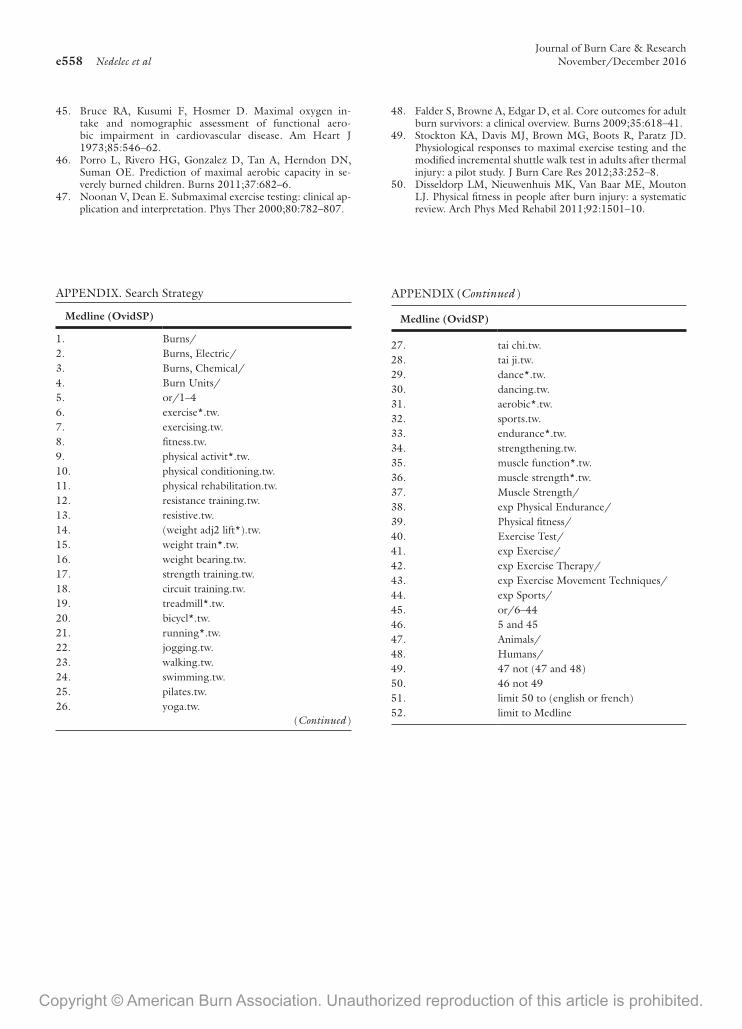
Copyright © American Burn Association. Unauthorized reproduction of this article is prohibited.
Journal of Burn Care & Researche558 Nedelec et al November/December 2016
45. Bruce RA, Kusumi F, Hosmer D. Maximal oxygen in-take and nomographic assessment of functional aero-bic impairment in cardiovascular disease. Am Heart J 1973;85:546–62.
46. Porro L, Rivero HG, Gonzalez D, Tan A, Herndon DN, Suman OE. Prediction of maximal aerobic capacity in se-verely burned children. Burns 2011;37:682–6.
47. Noonan V, Dean E. Submaximal exercise testing: clinical ap-plication and interpretation. Phys Ther 2000;80:782–807.
48. Falder S, Browne A, Edgar D, et al. Core outcomes for adult burn survivors: a clinical overview. Burns 2009;35:618–41.
49. Stockton KA, Davis MJ, Brown MG, Boots R, Paratz JD. Physiological responses to maximal exercise testing and the modified incremental shuttle walk test in adults after thermal injury: a pilot study. J Burn Care Res 2012;33:252–8.
50. Disseldorp LM, Nieuwenhuis MK, Van Baar ME, Mouton LJ. Physical fitness in people after burn injury: a systematic review. Arch Phys Med Rehabil 2011;92:1501–10.
APPENDIX. Search Strategy
Medline (OvidSP)
1. Burns/2. Burns, Electric/3. Burns, Chemical/4. Burn Units/5. or/1–46. exercise*.tw.7. exercising.tw.8. fitness.tw.9. physical activit*.tw.10. physical conditioning.tw.11. physical rehabilitation.tw.12. resistance training.tw.13. resistive.tw.14. (weight adj2 lift*).tw.15. weight train*.tw.16. weight bearing.tw.17. strength training.tw.18. circuit training.tw.19. treadmill*.tw.20. bicycl*.tw.21. running*.tw.22. jogging.tw.23. walking.tw.24. swimming.tw.25. pilates.tw.26. yoga.tw.
27. tai chi.tw.28. tai ji.tw.29. dance*.tw.30. dancing.tw.31. aerobic*.tw.32. sports.tw.33. endurance*.tw.34. strengthening.tw.35. muscle function*.tw.36. muscle strength*.tw.37. Muscle Strength/38. exp Physical Endurance/39. Physical fitness/40. Exercise Test/41. exp Exercise/42. exp Exercise Therapy/43. exp Exercise Movement Techniques/44. exp Sports/45. or/6–4446. 5 and 4547. Animals/48. Humans/49. 47 not (47 and 48)50. 46 not 4951. limit 50 to (english or french)52. limit to Medline
Medline (OvidSP)
APPENDIX (Continued )
(Continued )





























