Embed Size (px)
Citation preview
7/25/2019 Practice Essentials of pulmonary thromboembolism.docx
http://slidepdf.com/reader/full/practice-essentials-of-pulmonary-thromboembolismdocx 1/39
• Practice Essentials
• Background
• Anatomy
• Pathophysiology
• Etiology
• Epidemiology
• Prognosis
• Patient Education
• Show All
Multimedia LibraryReferences
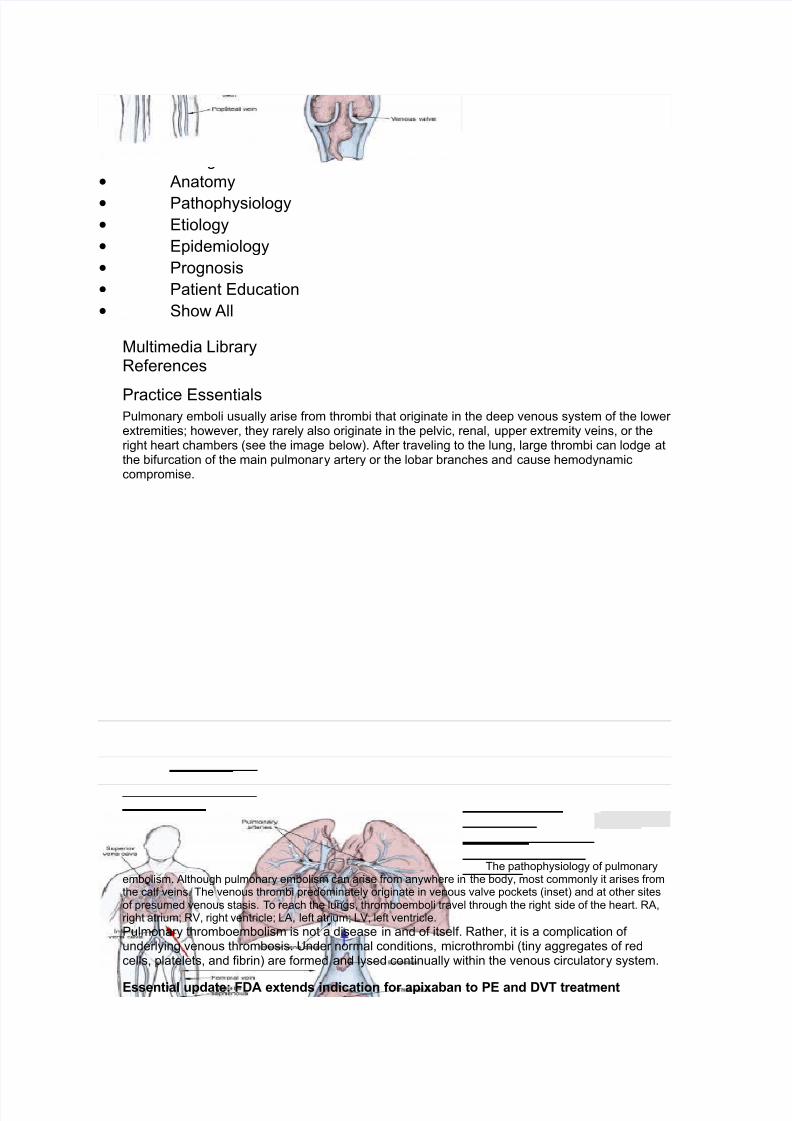
Practice EssentialsPulmonary emboli usually arise from thrombi that originate in the deep venous system of the loweretremities! however" they rarely also originate in the pelvic" renal" upper etremity veins" or theright heart chambers #see the image below$% After traveling to the lung" large thrombi can lodge atthe bifurcation of the main pulmonary artery or the lobar branches and cause hemodynamiccompromise%
&he pathophysiology of pulmonaryembolism% Although pulmonary embolism can arise from anywhere in the body" most commonly it arises fromthe calf veins% &he venous thrombi predominately originate in venous valve pockets #inset$ and at other sitesof presumed venous stasis% &o reach the lungs" thromboemboli travel through the right side of the heart% RA"right atrium! R'" right ventricle! LA" left atrium! L'" left ventricle%
Pulmonary thromboembolism is not a disease in and of itself% Rather" it is a complication ofunderlying venous thrombosis% (nder normal conditions" microthrombi #tiny aggregates of redcells" platelets" and fibrin$ are formed and lysed continually within the venous circulatory system%
Essential update: FDA extends indication for apixaban to PE and DVT treatment
7/25/2019 Practice Essentials of pulmonary thromboembolism.docx
http://slidepdf.com/reader/full/practice-essentials-of-pulmonary-thromboembolismdocx 2/39
&he (S )ood and *rug Administration #)*A$ has etended the indications for the oralanticoagulant apiaban" a selective factor +a inhibitor" to include the treatment of pulmonaryembolism #PE$ and deep venous thrombosis #*'&$" as well as the reduction of PE and *'&recurrence risk% &he drug was previously approved for stroke and systemic embolism riskreduction in nonvalvular atrial fibrillation and for PE and *'& prophylais following hip, or knee,replacement surgery%-./
&he )*A based its approval for the etended indication primarily on the outcome of the Apiabanfor the 0nitial Management of Pulmonary Embolism and *eep,'ein &hrombosis as )irst,Line&herapy #AMPL0)1$ and AMPL0)1,E+& studies" in which apiaban therapy was compared withenoaparin and warfarin treatment% &he AMPL0)1 study showed that" in comparison with thestandard anticoagulant regimen" apiaban therapy resulted in a .23 reduction in the risk of acomposite endpoint that included recurrent symptomatic venous thromboembolism #'&E$ or '&E,associated death%-4" 5/
Signs and symptoms
&he classic presentation of pulmonary embolism is the abrupt onset of pleuritic chest pain"shortness of breath" and hypoia% 6owever" most patients with pulmonary embolism have noobvious symptoms at presentation% Rather" symptoms may vary from sudden catastrophichemodynamic collapse to gradually progressive dyspnea% &he diagnosis of pulmonary embolism
should be suspected in patients with respiratory symptoms uneplained by an alternativediagnosis%
Patients with pulmonary embolism may present with atypical symptoms" such as the following7
• Sei8ures
• Syncope
• Abdominal pain
• )ever
• Productive cough
• 9hee8ing
• *ecreasing level of consciousness
• :ew onset of atrial fibrillation
• 6emoptysis
• )lank pain -;/
• *elirium #in elderly patients$ -</
See =linical Presentation for more detail%
Diagnosis
Evidence,based literature supports the practice of using clinical scoring systems to determine theclinical probability of pulmonary embolism before proceeding with testing% -2/ 'alidated clinicalprediction rules should be used to estimate pretest probability of pulmonary embolism and tointerpret test results%->" ?/
Physical signs of pulmonary embolism include the following7
• &achypnea #respiratory rate @.2min$7 23
• Rales7 <?3
• Accentuated second heart sound7 <53
• &achycardia #heart rate @.CCmin$7 ;;3
• )ever #temperature @5>%?D=$7 ;53
• *iaphoresis7 523
• S 5 or S ; gallop7 5;3
• =linical signs and symptoms suggesting thrombophlebitis7 543
• Lower etremity edema7 4;3
• =ardiac murmur7 453
• =yanosis7 .3
Testing
7/25/2019 Practice Essentials of pulmonary thromboembolism.docx
http://slidepdf.com/reader/full/practice-essentials-of-pulmonary-thromboembolismdocx 3/39
Perform diagnostic testing on symptomatic patients with suspected pulmonary embolism to confirmor eclude the diagnosis or until an alternative diagnosis is found% Routine laboratory findings arenonspecific and are not helpful in pulmonary embolism" although they may suggest anotherdiagnosis%
A hypercoagulation workup should be performed if no obvious cause for embolic disease isapparent" including screening for conditions such as the following7
• Antithrombin 000 deficiency
• Protein = or protein S deficiency
• Lupus anticoagulant
• 6omocystinuria
• ccult neoplasm
• =onnective tissue disorders
Potentially useful laboratory tests in patients with suspected pulmonary embolism include thefollowing7
• *,dimer testing
• 0schemia,modified albumin level
•
9hite blood cell count• Arterial blood gases7
• Serum troponin levels
• Brain natriuretic peptide
Imaging studies
0maging studies that aid in the diagnosis of pulmonary embolism include the following7
• =omputed tomography angiography #=&A$7 Multidetector,row =&A #M*=&A$ is the
criterion standard for diagnosing pulmonary embolism
• Pulmonary angiography7 =riterion standard for diagnosing pulmonary embolism when
M*=&A is not available
• =hest radiography7 Abnormal in most cases of pulmonary embolism" but nonspecific
•
'F scanning7 9hen =& scanning is not available or is contraindicated• E=G7 Most common abnormalities are tachycardia and nonspecific S&,& wave
abnormalities
• MR07 (sing standard or gated spin,echo techniHues" pulmonary emboli demonstrate
increased signal intensity within the pulmonary artery
• Echocardiography7 &ransesophageal echocardiography may identify central pulmonary
embolism
• 'enography7 =riterion standard for diagnosing *'&
• *uple ultrasonography7 :oninvasive diagnosis of pulmonary embolism by demonstrating
the presence of a *'& at any siteSee 9orkup for more detail%
Management
Anticoagulation and thrombolysis
0mmediate full anticoagulation is mandatory for all patients suspected of having *'& or pulmonaryembolism%-/ *iagnostic investigations should not delay empirical anticoagulant therapy%
&hrombolytic therapy should be used in patients with acute pulmonary embolism who havehypotension #systolic blood pressureI C mm 6g$ who do not have a high bleeding risk and inselected patients with acute pulmonary embolism not associated with hypotension who have a lowbleeding risk and whose initial clinical presentation or clinical course suggests a high risk ofdeveloping hypotension%-/
Long,term anticoagulation is critical to the prevention of recurrence of *'& or pulmonaryembolism" because even in patients who are fully anticoagulated" *'& and pulmonary embolismcan and often do recur%
Anticoagulation medications include the following7

7/25/2019 Practice Essentials of pulmonary thromboembolism.docx
http://slidepdf.com/reader/full/practice-essentials-of-pulmonary-thromboembolismdocx 4/39
• (nfractionated heparin
• Low,molecular,weight heparin
• )actor +a 0nhibitors
• )ondaparinu
• 9arfarin
&hrombolytic agents used in managing pulmonary embolism include the following7
• Alteplase
• Reteplase
• (rokinase
• Streptokinase
Surgical options
Surgical management options include the following7
• =atheter embolectomy and fragmentation or surgical embolectomy
• Placement of vena cava filters
See &reatment and Medication for more detail%
BackgroundPulmonary embolism is a common and potentially lethal condition% Most patients who succumb topulmonary embolism do so within the first few hours of the event% *espite diagnostic advances"delays in pulmonary embolism diagnosis are common and represent an important issue% -.C/ As acause of sudden death" massive pulmonary embolism is second only to sudden cardiac death%
0n patients who survive a pulmonary embolism" recurrent embolism and death can be preventedwith prompt diagnosis and therapy% (nfortunately" the diagnosis is often missed because patientswith pulmonary embolism present with nonspecific signs and symptoms% 0f left untreated"approimately one third of patients who survive an initial pulmonary embolism die from asubseHuent embolic episode% #See Prognosis%$
9hen a pulmonary embolism is identif ied" it is characteri8ed as acute or chronic% 0n terms of
pathologic diagnosis" an embolus is acute if it is situated centrally within the vascular lumen or if itoccludes a vessel #vessel cutoff sign$ #see the first image below$% Acute pulmonary embolismcommonly causes distention of the involved vessel% An embolus is chronic if it is eccentric andcontiguous with the vessel wall #see the second image below$" it reduces the arterial diameter bymore than <C3" evidence of recanali8ation within the thrombus is present" and an arterial web ispresent%

7/25/2019 Practice Essentials of pulmonary thromboembolism.docx
http://slidepdf.com/reader/full/practice-essentials-of-pulmonary-thromboembolismdocx 5/39
=omputed tomography angiogramin a <5,year,old man with acute pulmonary embolism% &his image shows an intraluminal filling defect thatoccludes the anterior basal segmental artery of the right lower lobe% Also present is an infarction of thecorresponding lung" which is indicated by a triangular" pleura,based consolidation #6ampton hump$%
=omputed tomographyangiography in a young man who eperienced acute chest pain and shortness of breath after atranscontinental flight% &his image demonstrates a clot in the anterior segmental artery in the left upper lung#LA4$ and a clot in the anterior segmental artery in the right upper lung #RA4$%
A pulmonary embolism is also characteri8ed as central or peripheral" depending on the location orthe arterial branch involved% =entral vascular 8ones include the main pulmonary artery" the left andright main pulmonary arteries" the anterior trunk" the right and left interlobar arteries" the left upper
lobe trunk" the right middle lobe artery" and the right and left lower lobe arteries% A pulmonaryembolus is characteri8ed as massive when it involves both pulmonary arteries or when it results inhemodynamic compromise% Peripheral vascular 8ones include the segmental and subsegmental

7/25/2019 Practice Essentials of pulmonary thromboembolism.docx
http://slidepdf.com/reader/full/practice-essentials-of-pulmonary-thromboembolismdocx 6/39
arteries of the right upper lobe" the right middle lobe" the right lower lobe" the left upper lobe" thelingula" and the left lower lobe% #See Physical Eamination%$
&he variability of presentation sets the patient and clinician up for potentially missing the diagnosis%&he challenge is that the JclassicJ presentation with abrupt onset of pleuritic chest pain" shortnessof breath" and hypoia is rarely seen% Studies of patients who died unepectedly of pulmonaryembolism revealed that the patients had complained of nagging symptoms" often for weeks" beforedying% )orty percent of these patients had been seen by a physician in the weeks prior to theirdeath%-../ #See the images below%$
A large pulmonary arterythrombus in a hospitali8ed patient who died suddenly%
Pulmonary embolism wasidentified as the cause of death in a patient who developed shortness of breath while hospitali8ed for hip Kointsurgery% &his is a close,up view%
&he most important conceptual advance regarding pulmonary embolism over the last severaldecades has been the reali8ation that pulmonary embolism is not a disease! rather" pulmonaryembolism is a complication of venous thromboembolism" most commonly deep venousthrombosis #*'&! shown in the image below$% 'irtually every physician who is involved in patientcare encounters patients who are at risk for venous thromboembolism" and therefore at risk forpulmonary embolism% #See Etiology%$

7/25/2019 Practice Essentials of pulmonary thromboembolism.docx
http://slidepdf.com/reader/full/practice-essentials-of-pulmonary-thromboembolismdocx 7/39
=omputed tomographyvenograms in a 2<,year,old man with possible pulmonary embolism% &his image shows acute deep venousthrombosis with intraluminal filling defects in the bilateral superficial femoral veins%
=linical signs and symptoms for pulmonary embolism are nonspecific! therefore" patientssuspected of having pulmonary embolismbecause of uneplained dyspnea" tachypnea" or chestpain or the presence of risk factors for pulmonary embolismmust undergo diagnostic tests untilthe diagnosis is ascertained or eliminated or an alternative diagnosis is confirmed% )urther" routinelaboratory findings are nonspecific and are not helpful in pulmonary embolism" although they maysuggest another diagnosis% Pulmonary angiography historically was the criterion standard for the
diagnosis of pulmonary embolism" but with the improved sensitivity and specificity of =&angiography" it is now rarely performed% #See 9orkup%$
0mmediate full anticoagulation is mandatory for all patients suspected to have *'& or pulmonaryembolism% *iagnostic investigations should not delay empirical anticoagulant therapy% #See&reatment and Management%$
Long,term anticoagulation is critical to the prevention of recurrence of *'& or pulmonaryembolism% &he general consensus is that a significant reduction in
Anatomy
nowledge of bronchovascular anatomy #seen in the image below$ is the key to the accurateinterpretation of =& scans obtained for the evaluation of pulmonary embolism% A systematicapproach in identifying all vessels is important% &he bronchovascular anatomy has been described
on the basis of the segmental anatomy of lungs% &he segmental arteries are seen near theaccompanying branches of the bronchial tree and are situated either medially #in the upper lobes$or laterally #in the lower lobes" lingula" and right middle lobe$%

7/25/2019 Practice Essentials of pulmonary thromboembolism.docx
http://slidepdf.com/reader/full/practice-essentials-of-pulmonary-thromboembolismdocx 8/39
&he pathophysiology of pulmonaryembolism% Although pulmonary embolism can arise from anywhere in the body" most commonly it arises fromthe calf veins% &he venous thrombi predominately originate in venous valve pockets #inset$ and at other sitesof presumed venous stasis% &o reach the lungs" thromboemboli travel through the right side of the heart% RA"right atrium! R'" right ventricle! LA" left atrium! L'" left ventricle%
Pulmonary thromboembolism is not a disease in and of itself% Rather" it is a complication ofunderlying venous thrombosis% (nder normal conditions" microthrombi #tiny aggregates of redcells" platelets" and fibrin$ are formed and lysed continually within the venous circulatory system%&his dynamic eHuilibrium ensures local hemostasis in response to inKury without permitting
uncontrolled propagation of clot% #See Etiology%$
Previous:et Section7 Pathophysiology
Pathophysiology
&here are both respiratory and hemodynamic conseHuences associated with pulmonary embolism%
Respiratory conseuences
Acute respiratory conseHuences of pulmonary embolism include the following7
• 0ncreased alveolar dead space
• 6ypoemia
•
6yperventilation Additional conseHuences that may occur include regional loss of surfactant and pulmonaryinfarction #see the image below$% Arterial hypoemia is a freHuent" but not universal" finding inpatients with acute embolism% &he mechanisms of hypoemia include ventilation,perfusionmismatch" intrapulmonary shunts" reduced cardiac output" and intracardiac shunt via a patentforamen ovale% Pulmonary infarction is an uncommon conseHuence because of the bronchialarterial collateral circulation%

7/25/2019 Practice Essentials of pulmonary thromboembolism.docx
http://slidepdf.com/reader/full/practice-essentials-of-pulmonary-thromboembolismdocx 9/39
Lung infarction secondary topulmonary embolism occurs rarely%
A segmental ventilation perfusionmismatch is evident in a left anterior obliHue proKection%
!emodynamic conseuences
Pulmonary embolism reduces the cross,sectional area of the pulmonary vascular bed" resulting inan increment in pulmonary vascular resistance" which" in turn" increases the right ventricularafterload% 0f the afterload is increased severely" right ventricular failure may ensue% 0n addition" thehumoral and refle mechanisms contribute to the pulmonary arterial constriction% )ollowing the
initiation of anticoagulant therapy" the resolution of emboli usually occurs rapidly during the first 4weeks of therapy! however" it can persist on chest imaging studies for months to years% =hronicpulmonary hypertension may occur with failure of the initial embolus to undergo lyses or in thesetting of recurrent thromboemboli%
Previous:et Section7 Etiology
Etiology
&hree primary influences predispose a patient to thrombus formation! these form the so,called'irchow triad" which consists of the following -.4" .5" .;/ 7
• Endothelial inKury
• Stasis or turbulence of blood flow
• Blood hypercoagulability

7/25/2019 Practice Essentials of pulmonary thromboembolism.docx
http://slidepdf.com/reader/full/practice-essentials-of-pulmonary-thromboembolismdocx 10/39
&hrombosis usually originates as a platelet nidus on valves in the veins of the lower etremities%)urther growth occurs by accretion of platelets and fibrin and progression to red fibrin thrombus"which may either break off and emboli8e or result in total occlusion of the vein% &he endogenousthrombolytic system leads to partial dissolution! then" the thrombus becomes organi8ed and isincorporated into the venous wall%
Pulmonary emboli usually arise from thrombi originating in the deep venous system of the loweretremities! however" they may rarely originate in the pelvic" renal" or upper etremity veins or theright heart chambers% After traveling to the lung" large thrombi can lodge at the bifurcation of themain pulmonary artery or the lobar branches and cause hemodynamic compromise% Smallerthrombi typically travel more distally" occluding smaller vessels in the lung periphery% &hese aremore likely to produce pleuritic chest pain by initiating an inflammatory response adKacent to theparietal pleura% Most pulmonary emboli are multiple" and the lower lobes are involved morecommonly than the upper lobes%
&he causes for pulmonary embolism are multifactorial and are not readily apparent in many cases%&he causes described in the literature include the following7
• 'enous stasis
• 6ypercoagulable states
•0mmobili8ation
• Surgery and trauma
• Pregnancy
• ral contraceptives and estrogen replacement
• Malignancy
• 6ereditary factors
• Acute medical illness
A study by Malek et al confirmed the hypothesis that individuals with 60' infection are more likelyto have clinically detected thromboembolic disease%-.</ &he risk of developing a pulmonaryembolism or *'& is increased ;C3 in these individuals%
Venous stasis
'enous stasis leads to accumulation of platelets and thrombin in veins% 0ncreased viscosity mayoccur due to polycythemia and dehydration" immobility" raised venous pressure in cardiac failure"or compression of a vein by a tumor%
!ypercoagulable states
&he comple and delicate balance between coagulation and anticoagulation is altered by manydiseases" by obesity" or by trauma% 0t can also occur after surgery%
=oncomitant hypercoagulability may be present in disease states where prolonged venous stasisor inKury to veins occurs%
6ypercoagulable states may be acHuired or congenital% )actor ' Leiden mutation causingresistance to activated protein = is the most common risk factor% )actor ' Leiden mutation ispresent in up to <3 of the normal population and is the most common cause of familial
thromboembolism%
Primary or acHuired deficiencies in protein =" protein S" and antithrombin 000 are other risk factors%&he deficiency of these natural anticoagulants is responsible for .C3 of venous thrombosis inyounger people%
"mmobili#ation
0mmobili8ation leads to local venous stasis by accumulation of clotting factors and fibrin" resultingin thrombus formation% &he risk of pulmonary embolism increases with prolonged bed rest orimmobili8ation of a limb in a cast%
0n the Prospective 0nvestigation of Pulmonary Embolism *iagnosis 00 #P0PE* 00$ study"immobili8ation #usually because of surgery$ was the risk factor most commonly found in patients
with pulmonary embolism%
Surgery and trauma

7/25/2019 Practice Essentials of pulmonary thromboembolism.docx
http://slidepdf.com/reader/full/practice-essentials-of-pulmonary-thromboembolismdocx 11/39
A prospective study by Geerts and colleagues indicated that maKor trauma was associated with a<?3 incidence of *'& in the lower etremities and an .?3 incidence in proimal veins% -.2/
Surgical and accidental traumas predispose patients to venous thromboembolism by activatingclotting factors and causing immobility% Pulmonary embolism may account for .<3 of allpostoperative deaths% Leg amputations and hip" pelvic" and spinal surgery are associated with thehighest risk%
)ractures of the femur and tibia are associated with the highest risk of fracture,related pulmonaryembolism" followed by pelvic" spinal" and other fractures% Severe burns also carry a high risk of*'& or pulmonary embolism%
Pregnancy
&he incidence of thromboembolic disease in pregnancy has been reported to range from . case in4CC deliveries to . case in .;CC deliveries #see Epidemiology$% )atal events are rare" with .,4cases occurring per .CC"CCC pregnancies%
$ral contracepti%es and estrogen replacement
Estrogen,containing birth control pills have increased the occurrence of venous thromboembolism
in healthy women% &he risk is proportional to the estrogen content and is increased inpostmenopausal women on hormonal replacement therapy% &he relative risk is 5,fold" but theabsolute risk is 4C,5C cases per .CC"CCC persons per year%
Malignancy
Malignancy has been identified in .>3 of patients with venous thromboembolism% Pulmonaryemboli have been reported to occur in association with solid tumors" leukemias" and lymphomas%&his is probably independent of the indwelling catheters often used in such patients% -.>/ &heneoplasms most commonly associated with pulmonary embolism" in descending order offreHuency" are pancreatic carcinoma! bronchogenic carcinoma! and carcinomas of thegenitourinary tract" colon" stomach" and breast%
!ereditary factors
6ereditary factors associated with the development of pulmonary embolism include the following7
• Antithrombin 000 deficiency
• Protein = deficiency
• Protein S deficiency
• )actor ' Leiden #most common genetic risk factor for thrombophilia$
• Plasminogen abnormality
• Plasminogen activator abnormality
• )ibrinogen abnormality
• Resistance to activated protein =
Acute medical illness
Acute medical illnesses associated with the development of pulmonary embolism include the
following7
• A0*S #lupus anticoagulant$
• BehNet disease
• =ongestive heart failure #=6)$
• Myocardial infarction
• Polycythemia
• Systemic lupus erythematosus
• (lcerative colitis
Additional ris& factors
Risk factors for pulmonary embolism also include the following7
•
*rug abuse #intravenous -0'/ drugs$• *rug,induced lupus anticoagulant
• 6emolytic anemias

7/25/2019 Practice Essentials of pulmonary thromboembolism.docx
http://slidepdf.com/reader/full/practice-essentials-of-pulmonary-thromboembolismdocx 12/39
• 6eparin,associated thrombocytopenia
• 6omocystinemia
• 6omocystinuria
• 6yperlipidemias
• Phenothia8ines
• &hrombocytosis
• 'aricose veins
• 'enography
• 'enous pacemakers
• 'enous stasis
• 9arfarin #first few days of therapy$
• 0nflammatory bowel disease
• Sleep,disordered breathing -.?/
0n the P0PE* 00 study" ;3 of patients with pulmonary embolism had . or more of the followingrisk factors-./ 7
• 0mmobili8ation
• &ravel of ; hours or more in the past month
•Surgery within the last 5 months
• Malignancy" especially lung cancer
• =urrent or past history of thrombophlebitis
• &rauma to the lower etremities and pelvis during the past 5 months
• Smoking
• =entral venous instrumentation within the past 5 months
• Stroke" paresis" or paralysis
• Prior pulmonary embolism
• 6eart failure
• =hronic obstructive pulmonary disease
Pulmonary embolism in c'ildren
0n contrast to adults" most children #?3$ diagnosed with pulmonary emboli have an identifiable
risk factor or a serious underlying disorder #see Epidemiology$%
0n .5" *avid et al reported that 4.3 of children with *'& andor pulmonary emboli had anindwelling central venous catheter %-4C/ Additional series have reported the presence of central linesin as many as 523 of patients%-4./ A clot may form as a fibrin sleeve that encases the catheter%9hen the catheter is removed" the fibrin sleeve is often dislodged" releasing a nidus for embolusformation% 0n another scenario" a thrombus may adhere to the vessel wall adKacent to the catheter%
*avid and colleagues also reported that <,.C3 of children with venous thromboembolic diseasehave inherited disorders of coagulation" such as antithrombin 000" protein =" or protein S deficiency%-4C/ 0n .>" :uss et al reported that >C3 of children with a diagnosis of pulmonary embolism haveantiphospholipid antibodies or coagulation,regulatory protein abnormalities% -44/6owever" this was asmall study in a population with clinically recogni8ed pulmonary emboli! hence" its applicability tothe broader pediatric population is uncertain%
A study reported that maKor thrombosis or pulmonary embolism was present in more than 553 ofchildren treated with long,term hyperalimentation and that pulmonary embolism was the maKorcause of death in 5C3 of these children% )at emboli8ation may eacerbate this clinical picture% -45/
*ehydration" especially hyperosmolar dehydration" is typically observed in younger infants withpulmonary emboli%
Previous:et Section7 Epidemiology
Epidemiology
(nited States statistics
&he incidence of pulmonary embolism in the (nited States is estimated to be . case per .CCCpersons per year %-4;/ Studies from 4CC? suggest that the increasing use of computed tomography

7/25/2019 Practice Essentials of pulmonary thromboembolism.docx
http://slidepdf.com/reader/full/practice-essentials-of-pulmonary-thromboembolismdocx 13/39
#=&$ scanning for assessing patients with possible pulmonary embolism has led to an increase inthe reported incidence of pulmonary embolism%-4<" 42/
)rom .>,.?" the age,adKusted death rate for pulmonary embolism in the (nited Statesdecreased from .. deaths per million population to ; deaths per million population% -4;/ Regionalstudies covering the years after .? found either a slight decrease in the incidence of mortality orno change in the freHuency%-4<" 42/
Pulmonary embolism is present in 2C,?C3 of patients with *'&" even though more than half thesepatients are asymptomatic% Pulmonary embolism is the third most common cause of death inhospitali8ed patients" with at least 2<C"CCC cases occurring annually% Autopsy studies have shownthat approimately 2C3 of patients who have died in the hospital had pulmonary embolism" withthe diagnosis having been missed in up to >C3 of the cases% Prospective studies havedemonstrated *'& in .C,.53 of all medical patients placed on bed rest for . week" 4,553 of allpatients in medical intensive care units" 4C,423 of patients with pulmonary diseases who aregiven bed rest for 5 or more days" 4>,553 of patients admitted to a critical care unit after amyocardial infarction" and ;?3 of patients who are asymptomatic after a coronary artery bypassgraft%
'enous thromboembolism is a maKor health problem% &he average annual incidence of venousthromboembolism in the (nited States is . person per .CCC population" -2" 4>" 4?/ with about 4<C"CCCincident cases occurring annually%
A challenge in understanding the real disease has been that autopsy studies have found an eHualnumber of patients diagnosed with pulmonary embolism at autopsy was were initially diagnosed byclinicians%-4>" 4/ &his has led to estimates of between 2<C"CCC to CC"CCC fatal and nonfatal venousthromboembolic events occurring in the (S annually% &he incidence of venous thromboembolismhas not changed significantly over the last 4< years%-4>/ =apturing the true incidence going forwardwill be challenging because of the decreasing rate of autopsy% 0n a longitudinal" 4<,yearprospective study from .22,.C" autopsy rates dropped from <<3 to 5C3 over the study period%-4>/ =urrent trends would suggest a continued decline in autopsy rate%
"nternational statistics
&he incidence of pulmonary embolism may differ substantially from country to country! observed
variation is likely due to differences in the accuracy of diagnosis rather than in the actual incidence%
=anadian data derived from .< tertiary care centers showed a freHuency of C%?2 events per .C"CCCpediatric hospital admissions for patients aged . month to . year %-5C/ )reHuency of pulmonaryembolism in developed countries has been increasing when compared with historical data% &hisincrease in freHuency is linked with the increased use of central venous lines in the pediatricpopulation%-5./&he overall freHuency in children is still considerably less than that in adults%
Association bet)een sex and pulmonary embolism
*ata are conflicting as to whether male se is a risk factor for pulmonary embolism! however" ananalysis of national mortality data found that death rates from pulmonary embolism were 4C,5C3higher among men than among women%-4;/ &he incidence of venous thromboembolic events in theolder population is greater among men than women% 0n patients younger than << years" the
incidence of pulmonary is higher in females% &he overall age, and se,adKusted annual incidenceof venous thromboembolism is reported to be ..> cases per .CC"CCC people #*'&" ;? cases per.CC"CCC! pulmonary embolism" 2 cases per .CC"CCC$%-4>/
A prospective cohort study of female nurses found an association between idiopathic pulmonaryembolism and hours spent sitting each week% 9omen who reported in both .?? and .C thatthey sat more than ;C hours per week had more than twice the risk of pulmonary embolismcompared with women who reported both years that they sat less than .Chours per week% -54/
Association bet)een race and pulmonary embolism
&he incidence of pulmonary embolism appears to be significantly higher in blacks than in whites%-55/ Mortality rates from pulmonary embolism for blacks have been <C3 higher than those for whites"and those for whites have been <C3 higher than those for people of other races #eg" Asians"
:ative Americans$%
-4;/
AsianPacific 0slandersAmerican 0ndian patients have a markedly lower riskof thromboembolism%-4;" 5;/

7/25/2019 Practice Essentials of pulmonary thromboembolism.docx
http://slidepdf.com/reader/full/practice-essentials-of-pulmonary-thromboembolismdocx 14/39
Pulmonary embolism in elderly persons
Pulmonary embolism is increasingly prevalent among elderly patients" yet the diagnosis is missedmore often in these patients than in younger ones because respiratory symptoms often aredismissed as being chronic% Even when the diagnosis is made" appropriate therapy freHuently isinappropriately withheld because of bleeding concerns% An appropriate diagnostic workup andtherapeutic anticoagulation with a careful risk,to,benefit assessment is recommended in this
patient population%
Pulmonary embolism in pediatric patients
*'& and pulmonary embolism are rare in pediatric practice% 0n .5" *avid et al identified 5C?children reported in the medical literature from .><,.5 with *'& of an etremity andorpulmonary embolism%-4C/ 0n .?2" Bernstein reported >? episodes of pulmonary embolism per.CC"CCC hospitali8ed adolescents%-5</(nselected autopsy studies in children estimate the incidenceof pulmonary embolism from C%C<,5%>3%
6owever" among pediatric patients in whom *'& or pulmonary emboli do occur" these conditionsare associated with significant morbidity and mortality% 'arious authors suggest that pulmonaryembolism contributes to the death of affected children in approimately 5C3 of cases% -52/ #thers"however" have reported pulmonary embolism as a cause of death in fewer than <3 of affected
children%-5>/
$
T'romboembolic disease in pregnancy
A population,based study covering the years .22,.< collated the cases of *'& or pulmonaryembolism in women during pregnancy or postpartum% &he relative risk was ;%4" and the overallincidence of venous thromboembolism #absolute risk$ was .%> incidents per .CC"CCC woman,years% Among postpartum women" the annual incidence was < times higher than in pregnantwomen #<..%4 vs <%? incidents per .CC"CCC women" respectively$%
&he incidence of *'& was 5 times higher than that of pulmonary embolism #.<.%? vs ;>%incidents" respectively" per .CC"CCC women$% Pulmonary embolism was relatively less commonduring pregnancy than in the postpartum period #.C%2 vs .<%> incidents" respectively" per .CC"CCCwomen" respectively$%-4?/ A national review of severe obstetric complications from .?,4CC< found
a significant increase in the rate of pulmonary embolism associated with the increasing rate ofcesarean delivery%-5?/
Pulmonary embolism and postoperati%e mortality
Pulmonary embolism may account for .<3 of all postoperative deaths% Leg amputations and hip"pelvic" and spinal surgery are associated with the highest risk%
Previous:et Section7 Prognosis
Prognosis
&he prognosis of patients with pulmonary embolism depends on 4 factors7 the underlying diseasestate and appropriate diagnosis and treatment% Approimately .C3 of patients who developpulmonary embolism die within the first hour" and 5C3 die subseHuently from recurrent embolism%
Mortality for acute pulmonary embolism can be broken down into 4 categories7 massive pulmonaryembolism and nonmassive pulmonary embolism%
Anticoagulant treatment decreases mortality to less than <3% At < days of anticoagulant therapy"523 of lung scan defects are resolved! at 4 weeks" <43 are resolved! and at 5 months" >53 areresolved% Most patients treated with anticoagulants do not develop long,term seHuelae uponfollow,up evaluation% &he mortality in patients with undiagnosed pulmonary embolism is 5C3%
0n the P0PE* study" the .,year mortality rate was 4;3% -5/ &he deaths occurred due to cardiacdisease" recurrent pulmonary embolism" infection" and cancer%
&he risk of recurrent pulmonary embolism is due to the recurrence of proimal venous thrombosis!approimately .>3 of patients with recurrent pulmonary embolism were found to have proimal*'&% 0n a small proportion of patients" pulmonary embolism does not resolve! hence" chronic
thromboembolic pulmonary arterial hypertension results%

7/25/2019 Practice Essentials of pulmonary thromboembolism.docx
http://slidepdf.com/reader/full/practice-essentials-of-pulmonary-thromboembolismdocx 15/39
Elevated plasma levels of natriuretic peptides #brain natriuretic peptide and N ,terminal pro,brainnatriuretic peptide$ have been associated with higher mortality in patients with pulmonaryembolism%-;C/ 0n one study" levels of N ,terminal pro,brain natriuretic peptide greater than <CC ngLwere independently associated with central pulmonary embolism and were a possible predictor ofdeath from pulmonary embolism%-;./
0n a study of 4>C adult patients with symptomatic pulmonary embolism that was obKectivelyconfirmed" researchers found that elevated plasma lactate levels #O4 mmolL$ were associatedwith an increased risk of mortality and other adverse outcomes" independent of shock"hypotension" right,sided ventricular dysfunction" or inKury markers%-;4/
Massi%e pulmonary embolism
As a cause of sudden death" massive pulmonary embolism is second only tosudden cardiac death%Massive pulmonary embolism is defined as presenting with a systolic arterial pressure less than Cmm 6g% &he mortality for patients with massive pulmonary embolism is between 5C3 and 2C3"depending on the study cited%-4" ;5" ;;/ Autopsy studies of patients who died unepectedly in a hospitalsetting have shown approimately ?C3 of these patients died from massive pulmonary embolism%
&he maKority of deaths from massive pulmonary embolism occur in the first .,4 hours of care" so itis important for the initial treating physician to have a systemi8ed" aggressive evaluation and
treatment plan for patients presenting with pulmonary embolism%
*onmassi%e pulmonary embolism
:onmassive pulmonary embolism is defined as having a systolic arterial pressure greater than oreHual to C mm 6g% &his is the more common presentation for pulmonary embolism and accountsfor <%<,23 of the patients%-;5" ;</
6emodynamically stabile pulmonary embolism has a much lower mortality rate because oftreatment with anticoagulant therapy% 0n nonmassive pulmonary embolism" the death rate is lessthan <3 in the first 5,2 months of anticoagulant treatment% &he rate of recurrent thromboembolismis less than <3 during this time% 6owever" recurrent thromboembolism reaches 5C3 after .Cyears%-5;/
Previous :et Section7 Patient Education
•
Approach =onsiderations
• &hrombolysis
• Anticoagulation
• Embolectomy
• 'ena =ava )ilters
• Supportive =are
• Pulmonary Embolism in Pregnancy
• =omplications
• *eterrence and Prevention of Pulmonary Embolism
• Medicolegal =oncerns
• )uture Research
• =onsultations
• Long &erm Monitoring
• Show All
Multimedia LibraryReferences

7/25/2019 Practice Essentials of pulmonary thromboembolism.docx
http://slidepdf.com/reader/full/practice-essentials-of-pulmonary-thromboembolismdocx 16/39
Approach =onsiderations
According to American =ollege of =hest Physicians #A==P$ guidelines" immediate therapeuticanticoagulation should be initiated for patients in whom *'& or pulmonary embolism #PE$ #grade.B$ is suspected%-/ Anticoagulation therapy reduces mortality rates from 5C3 to less than .C3%*iagnostic investigations should not delay empirical anticoagulant therapy in patients with high orintermediate risk of PE #grade 4=$%
)or acute PE" the A==P guidelines recommend starting lowmolecular weight heparin #LM96$ orfondaparinu" preferred over unfractionated heparin #()6$ #grade 4= for LM96! grade 4B forfondaparinu$ or subcutaneous heparin #grade 4B for LM96! grade 4= for fondaparinu$% -/ 0fpatients are to be treated with LM96" once daily treatment is preferred to twice daily treatment#grade 4=$%
Patients who are considered to be low risk should be discharged early from hospital #grade 4B$%
Patients should have an oral anticoagulant #warfarin$ initiated at the time of diagnosis" and theyshould have ()6" LM96" or fondaparinu discontinued only after the international normali8edratio #0:R$ is 4%C for at least 4; hours but no sooner than < days after warfarin therapy has beenstarted #grade .B$% &he recommended duration of ()6" LM96" and fondaparinu is based onevidence suggesting that the relatively long half,life of factor 00" along with the short half,lives of
protein = and protein S" may provoke a paradoical hypercoagulable state if these agents arediscontinued prematurely%
&he ninth edition of the A==P guidelines for antithrombotic and thrombolytic therapy aresummari8ed as follows7-/
• &hrombolytic therapy should be used in patients with acute PE associated with
hypotension #systolic BP I C mm 6G$" who do not have a high bleeding risk #grade 4=$%
• &hrombolytic therapy is suggested in select patients with acute PE not associated with
hypotension and with a low bleeding risk whose initial clinical presentation or clinical course after starting anticoagulation suggests a high risk of developing hypotension #grade 4=$ +
• Assessment of PE severity" prognosis" and risk of bleeding dictate whether thrombolytic
therapy should be started% &hrombolytic therapy is not recommended for most patients with
acute PE not associated with hypotension #grade .=$%Even in patients who are fully anticoagulated" however" *'& and PE can and often do recur% :ewPE in the hospital can occur in the following patients despite therapeutic anticoagulation7
• Patients who have nonfloating *'& without PE at presentation #53$
• Patients who present with a floating thrombus but have no PE #.53$
• Patients who present with PE but have no floating thrombus #..3$
• Patients who present with PE who have a floating thrombus visible at venography #53$
*eciding how to treat a venous thrombosis that may lead to a PE is difficult% A survey of =anadianpediatric intensivists reported ; patient factors commonly used to determine if a venousthrombosis is clinically important7-5C/
• =linical suspicion of a PE
• Symptoms
• *etection of thrombosis on clinical eamination
• Presence of an acute or chronic cardiopulmonary comorbidity that affects the patientQs
ability to tolerate a PE Anticoagulants are the treatment of choice in most children with pulmonary emboli% &hrombolyticsare rarely used% &o date" little data are available regarding the use of LM96 in children withthromboembolic disease%
&hrombolysis
All patients with PE reHuire rapid risk stratification% &he A==P guidelines recommend thatthrombolytic therapy should be used in patients with acute PE associated with hypotension#systolic BPI C mm 6G$ who do not have a high bleeding risk #grade 4=$% -/ *o not delaythrombolysis in this population because irreversible cardiogenic shock can develop% &hrombolytic
therapy is suggested in select patients with acute PE not associated with hypotension and with alow bleeding risk whose initial clinical presentation or clinical course after starting anticoagulationsuggests a high risk of developing hypotension #grade 4=$ + Assessment of pulmonary embolism

7/25/2019 Practice Essentials of pulmonary thromboembolism.docx
http://slidepdf.com/reader/full/practice-essentials-of-pulmonary-thromboembolismdocx 17/39
severity" prognosis" and risk of bleeding dictate whether thrombolytic therapy should be started%&hrombolytic therapy is not recommended for most patients with acute PE not associated withhypotension #grade .=$%
Although most studies demonstrate the superiority of thrombolytic therapy with respect to theresolution of radiographic and hemodynamic abnormalities within the first 4; hours" this advantagedisappears > days after treatment% =ontrolled clinical trials have not demonstrated benefits interms of reduced mortality rates or earlier resolution of symptoms when currently compared withheparin% A large retrospective review suggests that the use of thrombolytic therapy in unstablepatients with PE may lead to reduced mortality when compared to anticoagulation therapy alone%=oncurrent use of thrombolytic therapy and vena cava filters in such patients may reduce mortalityeven further%-?<" ?2/
0n a meta,analysis of .2 randomi8ed studies comparing thrombolytic therapy with anticoagulationtherapy in patients with pulmonary embolism" including intermediate,risk" hemodynamically stablepatients with right ventricular dysfunction" =hatterKee et al found that thrombolytic therapy" ascompared with standard anticoagulant therapy" reduced mortality by ;>3 but was associated witha 4%>,fold increase in maKor bleeding%-?>/
&he investigators also found" however" that the rate of maKor bleeding was not significantlyincreased with thrombolysis among patients younger than 2< years" whereas it more than tripled inthe subgroup of patients older than 2< years%-?>/&hrombolytic therapy was associated with a greater risk of intracranial hemorrhage and a lower risk of recurrent pulmonary embolism% -?>/
(ntil randomi8ed clinical trials demonstrate a clear morbidity or mortality benefit" the role ofthrombolytic therapy in the management of acute pulmonary embolism will remain controversial#especially in the management of intermediate,risk patients$%-??" ?" C/ &he currently acceptedindications for thrombolytic therapy include hemodynamic instability #systolic BP I C mm 6g$ or aclinical risk factor assessment that suggests that hypotension is likely to develop%
Anticoagulation
(nfractionated 'eparin t'erapy
0n patients with acute PE" anticoagulation with 0' ()6" LM96" or fondaparinu is preferred over
no anticoagulation #grade .B$%-/
Most patients with acute PE should receive LM96 or fondaparinuinstead of 0' ()6 #grade 4= for LM96" grade 4B for fondaparinu$% 0n patients with PE" ifconcerns regarding subcutaneous absorption arise" severe renal failure eists" or if thrombolytictherapy is being considered" 0' ()6 is the recommended form of initial anticoagulation% -/=liniciansoften choose to use 0' ()6 in preference to LM96 and fondaparinu in specific clinicalcircumstances where medical or surgical procedures are likely to be performed and the short half,life of 0' ()6 allows for temporary cessation of anticoagulation and presumed reduction ofbleeding risk during the procedure% &hough this strategy has limited supporting evidence" itappears to represent a reasonable practice%
&he efficacy of heparin therapy depends on achieving a critical therapeutic level of heparin withinthe first 4; hours of treatment% &he critical therapeutic level of heparin is .%< times the baselinecontrol value or the upper limit of normal range of the activated partial thromboplastin time #aP&&$%
&his level of anticoagulation is epected to correspond to a heparin blood level of C%4,C%; (mL bythe protamine sulfate titration assay and C%5,C%2 by the anti,factor + assay%
Each laboratory should establish the minimal therapeutic level for heparin" as measured by theaP&&" to coincide with a heparin blood level of at least C%4 (mL for each batch of thromboplastinreagent being used%
0f 0' ()6 is chosen" an initial bolus of ?C (kg or <CCC ( followed by an infusion of .? (kgh or.5CC (h should be given" with the goal of rapidly achieving and maintaining the aP&& at levelsthat correspond to therapeutic heparin levels% )ied,dose and monitored regimens ofsubcutaneous ()6 are available and are acceptable alternatives%
,o)-molecular-)eig't 'eparin t'erapy
=urrent guidelines for patients with acute PE recommend LM96 over 0' ()6 #grade 4=$ and over S= ()6 #grade 4B$%-/ 0n patients being treated with LM96" once,daily regimens are preferred over

7/25/2019 Practice Essentials of pulmonary thromboembolism.docx
http://slidepdf.com/reader/full/practice-essentials-of-pulmonary-thromboembolismdocx 18/39
twice,daily regimens #grade 4=$% &he choice between fondaparinu and LM96 should be basedon local considerations to include cost" availability" and familiarity of use%
LM96s have many advantages over ()6% &hese agents have a greater bioavailability" can beadministered by subcutaneous inKections" and have a longer duration of anticoagulant effect% Afied dose of LM96 can be used" and laboratory monitoring of aP&& is not necessary%
&rials comparing LM96 with ()6 have shown that LM96 is at least as effective and as safe as()6% &he studies have not pointed to any significant differences in recurrent thromboembolicevents" maKor bleeding" or mortality between the 4 types of heparin%
LM96 can be administered safely in an outpatient setting% &his has led to the development ofprograms in which clinically stable patients with PE are treated at home" at substantial costsavings% &he A==P guidelines suggest that patients with low,risk PE and who have acceptablehome circumstances be discharged early from hospital #ie" before the first five days of treatment$#grade 4B$%
An international" open,label" randomi8ed trial compared outpatient and inpatient treatment #bothusing the LM96 enoaparin as initial therapy$ of low,risk patients with acute PE and concludedthat outpatient treatment was noninferior to inpatient treatment%-./
Direct t'rombin in'ibitors and factor .a in'ibitors
Apiaban" dabigatran" rivaroaban" and edoaban are alternatives to warfarin for prophylais andtreatment of PE% Apiaban" edoaban" and rivaroaban inhibit factor +a" whereas dabigatran is adirect thrombin inhibitor%
Rivaroxaban
Rivaroaban #+arelto$ is an oral factor +a inhibitor approved by the )*A in :ovember 4C.4 for thetreatment of *'& or PE" and to reduce risk of recurrent *'& and PE following initial treatment%
Approval for this indication was based on studies totaling ;>? patients with *'& or PE%Participants were randomly assigned to receive rivaroaban" a combination of enoaparin and avitamin antagonist #'A$ #eg" warfarin$" or a placebo% Study endpoints were designed to
measure the number of patients who eperienced recurrent symptoms of *'&" PE" or death afterreceiving treatment%-4" 5/ Additionally" results from etended treatment demonstrated a reduced riskof recurrent *'& and PE% Approimately .%53 in the rivaroaban group eperienced recurrent *'&or PE compared with >%.3 in the placebo group%-;" </
&he results of the Einstein,PE study provide an important advance in the treatment of symptomaticPE% 0n a prospective" open,label study" ;?54 patients were randomi8ed to receive eitherrivaroaban or enoaparin followed by an adKusted,dose vitamin antagonist for 5" 2" or .4months% &reatment with a fied,dose regimen of rivaroaban was noninferior to standard therapyand had a satisfactory safety profile%-4/
*ata from a pooled analysis of the E0:S&E0:,PE and E0:S&E0:,*'& studies in the treatment of*'& or pulmonary embolism suggest that rivaroaban is as effective in preventing '&E recurrenceas administration of enoaparin followed by a vitamin, antagonist% -2" >/ Rivaroaban may also be
associated with less bleeding" particularly in elderly patients and those with moderate renalimpairment%-2" >/
Apixaban
Apiaban was approved for treatment of PE in August 4C.;% &he approval for treatment of PE andprevention of recurrence was based on the outcome of the AMPL0)1 #Apiaban for the 0nitialManagement of Pulmonary Embolism and *eep,'ein &hrombosis as )irst,Line &herapy$ and AMPL0)1,E+& studies" in which apiaban therapy was compared with enoaparin and warfarintreatment% &he AMPL0)1 study showed that" in comparison with the standard anticoagulantregimen apiaban therapy resulted in a .23 reduction in the risk of a composite endpoint thatincluded recurrent symptomatic venous thromboembolism #'&E$ or '&E,associated death% -4" 5/
&his advance thus offers the prospect of a safe and effective regimen of anticoagulation for
patients with the advantages of simplicity and cost,effectiveness in comparison to currentmanagement strategies%

7/25/2019 Practice Essentials of pulmonary thromboembolism.docx
http://slidepdf.com/reader/full/practice-essentials-of-pulmonary-thromboembolismdocx 19/39
Dabigatran
*abigatran #Pradaa$ was approved by the )*A in 4C.; for the treatment of *'& and PE andreducing venous thromboembolic recurrence% 0n the RE,='ER and RE,='ER 4 studies"patients with *'& and PE who had received initial parenteral anticoagulation #eg" 0' heparin" S=LM96$ for <,.C days were randomi8ed to warfarin or dabigatran% &hese two trials showeddabigatran was noninferior to warfarin in reducing *'& and PE and was associated with lowerbleeding rates%-?" /
Edoxaban
Edoaban #Savaysa$ was approved by the )*A in anuary 4C.< for the treatment of *'& and PEin patients who have been initially treated with a parenteral anticoagulant for <,.C days% Approvalwas based on the 6okusai,'&E study" which included 5"5. patients with PE% f these patients"5? had right ventricular dysfunction" as assessed by measurement of :,terminal pro,brainnatriuretic peptide levels% &he rate of recurrent '&E in this subgroup was 5%53 in the edoabangroup and 2%43 in the warfarin group% Edoaban was noninferior to high,Huality standard warfarintherapy and caused significantly less bleeding in a broad spectrum of patients with '&E" includingthose with severe pulmonary embolism%-.CC/
Fondaparinux
0n patients with acute PE" fondaparinu as initial treatment is favored over 0' ()6 #grade 4B$ andover S= ()6 #grade 4=$%-/ &he choice between fondaparinu and LM96 should be based on localconsiderations to include cost" availability" and familiarity of use% )ondaparinu is a syntheticpolysaccharide derived from the antithrombin binding region of heparin% )ondaparinu cataly8esfactor +a inactivation by antithrombin without inhibiting thrombin%
nce,daily fondaparinu was found to have similar rates of recurrent PE" bleeding" and death as0' ()6" according to one randomi8ed open,label study of 44.5 patients with symptomaticpulmonary embolism%-.C./
0n general" the use of LM96 or fondaparinu is recommended over 0' ()6 and S= ()6% &his isbecause of a more predictable bioavailability" more rapid onset of full anticoagulant effect" and thebenefit of not typically needing to monitor anticoagulant effect% 6owever" if uncertainty arises
regarding the accuracy of dosing" factor +a levels can be monitored to determine efficacy%
/arfarin t'erapy
&he A==P guidelines recommend that a vitamin antagonist such as warfarin be started on thesame day as anticoagulant therapy in patients with acute PE #grade .B$%-/ Parenteralanticoagulation and warfarin should be continued together for a minimum of at least five days anduntil the 0:R is 4%C%
&he anticoagulant effect of warfarin is mediated by the inhibition of vitamin dependent factors"which are 00" '00" 0+" and +% &he peak effect does not occur until 52,>4 hours after drugadministration" and the dosage is difficult to titrate%
A prothrombin time ratio is epressed as an 0:R and is monitored to assess the adeHuacy ofwarfarin therapy% &he recommended therapeutic range for venous thromboembolism is an 0:R of4,5% &his level of anticoagulation markedly reduces the risk of bleeding without the loss ofeffectiveness% 0nitially" 0:R measurements are performed on a daily basis! once the patient isstabili8ed on a specific dose of warfarin" the 0:R determinations may be performed every .,4weeks or at longer intervals%
Duration of anticoagulation t'erapy
A patient with a first thromboembolic event occurring in the setting of reversible risk factors" suchas immobili8ation" surgery" or trauma" should receive warfarin therapy for at least 5 months% :odifference in the rate of recurrence was observed in either of 4 studies comparing 5 versus 2months of anticoagulant therapy in patients with idiopathic #or unprovoked$ first events% -.C4" .C5/ &hecurrent recommendation is anticoagulation for at least 5 months in these patients! the need foretending the duration of anticoagulation should be reevaluated at that time%
&he current A==P guidelines recommend that all patients with unprovoked PE receive threemonths of treatment with anticoagulation over a shorter duration of treatment and have an

7/25/2019 Practice Essentials of pulmonary thromboembolism.docx
http://slidepdf.com/reader/full/practice-essentials-of-pulmonary-thromboembolismdocx 20/39
assessment of the risk,benefit ratio of etended therapy at the end of three months #grade .B$%-/ Patients with a first episode of venous thromboembolism and with a low or moderate risk ofbleeding should have etended anticoagulant therapy #grade 4B$% Patients with a first episode ofvenous thromboembolism who have a high bleeding risk should have therapy limited to threemonths #grade .B$%
0n patients with a second unprovoked episode of venous thromboembolism and low or moderaterisk of bleeding" etended anticoagulant therapy is recommended #grades .B and 4B"respectively$% 0n patients with a second episode of venous thromboembolism and a high risk ofbleeding" three months of anticoagulation is preferred over etended anticoagulation #grade 4B$%
Patients who have pulmonary embolism and preeisting irreversible risk factors" such asdeficiency of antithrombin 000" protein S and =" factor ' Leiden mutation" or the presence ofantiphospholipid antibodies" should be placed on long,term anticoagulation%
0ancer patients
Patients who have PE in association with an active neoplasm provide challenges for long,termmanagement because of their increased continuing risk for recurrent '&E and PE% &he ninthedition of the A==P guidelines recommends that such patients receive etended anticoagulationas opposed to three month therapy if they are at low or moderate risk of bleeding
complications#grade .B$%-/ 0f patients with active neoplasm are at high risk of bleeding" it is stillsuggested that they receive etended therapy" though the supporting evidence is less conclusive#grade 4B$% )or the treatment of PE in cancer patients" LM96 is recommended in preference to avitamin antagonist such as warfarin #grade 4B$% 6owever" some cancer patients choose not tohave long,term treatment with LM96 because of the need for daily inKections and treatment costs%0f cancer patients with PE choose not to have treatment with LM96" a vitamin antagonist suchas warfarin is preferred over dabigatran or rivaroaban #grade 4=$%
!eparin-induced t'rombocytopenia
6eparin,induced thrombocytopenia #60&$ is a transient prothrombotic disorder initiated by heparin%&he main features of 60& are #.$ thrombocytopenia resulting from immunoglobulin Gmediatedplatelet activation and #4$ in vivo thrombin generation and increased risk of venous and arterialthrombosis%
&he highest freHuency of 60&" <3" has been reported in postorthopedic surgery patients receivingup to 4 weeks of unfractionated heparin% 60& occurred in approimately C%<3 of postorthopedicsurgery patients receiving LM96 for up to 4 weeks%
60& may manifest clinically as etension of the thrombus or formation of new arterial thrombosis%60& should be suspected whenever the patientQs platelet count falls to less than .CC"CCCL or lessthan <C3 of the baseline value" generally after <,.< days of heparin therapy% )or patients receivingheparin where the risk of 60& is thought to be greater than .3" guidelines suggest that plateletcounts be obtained every two or three days from day ; to day .; of therapy" or until the heparin isstopped #grade 4=$%-/ &he definitive diagnosis is made by performing a platelet activation factorassay%
&he treatment of patients who develop 60& is to stop all heparin products" including catheter
flushes and heparin,coated catheters" and to initiate an alternative" nonheparin anticoagulant"even when thrombosis is not clinically apparent% 0n patients with 60& with or without thrombosis"the use of lepirudin" argatroban" or danaparoid is preferred over continued use of heparin" LM96"or either initiation or continuation of a vitamin antagonist #grade .=$%-/
0f a vitamin antagonist has already been started when 60& is diagnosed" guidelines recommendthat it be discontinued and that vitamin should be administered #grade 4=$%-/ 9hen 60& has beenconfirmed" vitamin antagonists should not be started until the platelet count has recovered to atleast .<C .CL #grade .=$" it should be started at low doses #ie" < mg of warfarin$" and it shouldbe given concomitantly with a nonheparin anticoagulant for a minimum of five days and until the0:R is within the target range #grade .=$%-/ 0n patients with renal failure who have 60& andthrombosis" argatroban is preferred over other nonheparin anticoagulants #grade 4=$% -/
Resistance to 'eparin
)ew patients with venous thromboembolism reHuire large doses of heparin for achieving anoptimal activated partial thromboplastin time #aP&&$% &hose patients who do reHuire them have

7/25/2019 Practice Essentials of pulmonary thromboembolism.docx
http://slidepdf.com/reader/full/practice-essentials-of-pulmonary-thromboembolismdocx 21/39
increased plasma concentrations of factor '000 and heparin,binding proteins% 0ncreased factor '000concentration causes dissociation between aP&& and plasma heparin values% &he aP&& issuboptimal" but patients have adeHuate heparin levels upon protamine titration% &his commonlyoccurs in patients with a concomitant inflammatory disease%
Monitoring the antifactor +a assay results in this situation is safe and effective and results in lessescalation of the heparin dose when compared with monitoring with aP&&% 9henever a therapeuticlevel of aP&& cannot be achieved with large doses of ()6" either determination of plasma heparinconcentration or therapy with LM96 should be instituted%
Embolectomy
Guidelines from the American 6eart Association #A6A$ advise that either catheter embolectomyand fragmentation or surgical embolectomy is reasonable for patients with massive pulmonaryembolism who have contraindications to fibrinolysis or who remain unstable after receivingfibrinolysis%-.C;/ 0f these procedures are not available locally" it is reasonable to consider transferringthe patient to an institution with eperience in one of these procedures" providing the transfer canbe accomplished safely%
0n patients with submassive acute PE" either catheter embolectomy or surgical embolectomy maybe considered if they have clinical evidence of an adverse prognosis #ie" new hemodynamic
instability" worsening respiratory failure" severe right ventricular dysfunction" or maKor myocardialnecrosis$% &hese interventions are not recommended for patients with low,risk or submassiveacute pulmonary embolism who have minor right ventricular dysfunction" minor myocardialnecrosis" and no clinical worsening%-.C;/
'ena =ava )ilters
&he current grade .B recommendation is that patients with acute PE should not routinely receivevena cava filters in addition to anticoagulants%-/ An ideal 0'= filter should be easily and safelyplaced using a percutaneous techniHue" biocompatible and mechanically stable" and able to trapemboli without causing occlusion of the vena cava%-.C</
0'= interruption by the insertion of an 0'= filter #Greenfield filter$ is only indicated in the followingsettings7
• Patients with acute venous thromboembolism who have an absolute contraindication to
anticoagulant therapy #eg" recent surgery" hemorrhagic stroke" significant active or recentbleeding$
• Patients with massive PE who survived but in whom recurrent embolism invariably will be
fatal
• Patients who have obKectively documented recurrent venous thromboembolism" adeHuate
anticoagulant therapy notwithstanding0n patients with a time,limited indication for 0'= filter placement #eg" a short,term contraindicationto anticoagulation$" it is reasonable to select a retrievable 0'= filter and evaluate the patientperiodically for filter retrieval% After placement of an 0'= filter" A6A guidelines recommend thatanticoagulation be resumed once contraindications to anticoagulation or active bleedingcomplications have resolved%-.C;/
Supportive =are
0ompression stoc&ings
)or patients who have had a proimal *'&" the use of elastic compression stockings provides asafe and effective adKunctive treatment that can limit postphlebitic syndrome% Stockings with apressure of 5C,;C mm 6g at the ankle" worn for 4 years following diagnosis" are recommended#grade 4B$ to reduce the risk of postphlebitic syndrome%
&rue gradient compression stockings are highly elastic" providing a gradient of compression that ishighest at the toes and gradually decreases to the level of the thigh% &his reduces capacitivevenous volume by approimately >C3 and increases the measured velocity of blood flow in thedeep veins by a factor of < or more% =ompression stockings of this type have been proveneffective in the prophylais of thromboembolism and are also effective in preventing progression of
thrombus in patients who already have *'& and pulmonary embolism%

7/25/2019 Practice Essentials of pulmonary thromboembolism.docx
http://slidepdf.com/reader/full/practice-essentials-of-pulmonary-thromboembolismdocx 22/39
A .; meta,analysis calculated a *'& risk odds ratio of C%4? for gradient compression stockings#as compared to no prophylais$ in patients undergoing abdominal surgery" gynecologic surgery" or neurosurgery%
ther studies found that gradient compression stockings and LM96 were the most effectivemodalities in reducing the incidence of *'& after hip surgery! they were more effective thansubcutaneous ()6" oral warfarin" detran" or aspirin%
&he ubiHuitous white stockings known as anti,embolic stockings or J&ed hoseJ produce amaimum compression of .? mm 6g% &ed hose rarely are fitted in such a way as to provide eventhat inadeHuate gradient compression% Because they provide such limited compression" they haveno efficacy in the treatment of *'& and pulmonary embolism" nor have they been proven effectiveas prophylais against a recurrence%
&rue 5C,;C mm 6g gradient compression pantyhose are available in si8es for pregnant women%&hey are recommended by many specialists for all pregnant women because they not only prevent*'&" but they also reduce or prevent the development of varicose veins during pregnancy%
Additional support t'erapies
Activity is recommended as tolerated% Early ambulation is recommended over bed rest when
feasible #grade 4= recommendation$%
Pharmacologic support of the cardiovascular system may be necessary% *opamine anddobutamine are the usual inotropic agents% Mechanical ventilation may be necessary to providerespiratory support and as adKunctive therapy for a failing circulatory system%
=hildren with sickle cell disease who present with pulmonary symptoms reHuire treatment with amacrolide and cephalosporin antibiotic% &heir clinical status should be closely monitored in order toanticipate those children who may develop acute chest syndrome% -;/ &ransfusion with packed redblood cells #either simple or echange$ improves oygenation immediately" helping to break thevicious cycle outlined above%
0' fluids may help or may hurt the patient who is hypotensive from pulmonary embolism"depending on which point on the Starling curve describes the patientQs condition% A cautious trial of
a small fluid bolus may be attempted" with careful surveillance of the systolic and diastolic bloodpressures and immediate cessation if the situation worsens after the fluid bolus% 0mprovement ornormali8ation of blood pressure after fluid loading does not mean the patient has becomehemodynamically stable%
0ndividuals with acute" submassive pulmonary embolisms have low levels of endogenous activatedprotein =% A study by *empfle et al determined that administering drotrecogin alfa #activated$ alongwith therapeutic doses of enoaparin enhanced the inhibition of fibrin formation in these patients%-.C2/
*rotrecogin alfa was withdrawn from the worldwide market ctober 4<" 4C.. after analysis of theRecombinant 6uman Activated Protein = 9orldwide Evaluation in Severe Sepsis #PR9ESS$,S6= clinical trial% *rotrecogin alfa failed to demonstrate a statistically significant reduction in4?,day all,cause mortality in patients with severe sepsis and septic shock% &rial results observed a
4?,day all,cause mortality rate of 42%;3 in patients treated with activated drotrecogin alfacompared with 4;%43 in the placebo group of the study%
Pulmonary Embolism in Pregnancy
&he risk of venous thromboembolism is increased during pregnancy and the postpartum period%Pulmonary embolism is the leading cause of death in pregnancy% *'& and pulmonary embolismare common during all trimesters of pregnancy and for 2,.4 weeks after delivery%
Diagnosis
&he diagnostic approach to patients with pulmonary embolism should be eactly the same in apregnant patient as in a nonpregnant one% A nuclear perfusion lung scan is safe in pregnancy" as isa chest =& scan%
Guidelines by the professional societies on the diagnosis of pulmonary embolism make this difficultassessment easier and reduce the risks of radiation to the fetus% 0f the patient has a low pretestprobability for pulmonary embolism and a normal *,dimer test result" clinical eclusion from further

7/25/2019 Practice Essentials of pulmonary thromboembolism.docx
http://slidepdf.com/reader/full/practice-essentials-of-pulmonary-thromboembolismdocx 23/39
investigations is recommended% 9hen the suspicion is high" the patients should have bilateral leg*oppler assessment% 0f the results are positive" the patient should be treated for pulmonaryembolism% 0f the results are negative" =& pulmonary angiography is the net step% &o rule outcontrast,induced hypothyroidism" all neonates eposed to the iodinated contrast in utero shouldhave their serum thyrotropin level checked in the first week of life%
Treatment
6eparin and fibrinolysis are safe in pregnancy% )ailure to treat the mother properly is the mostcommon cause of fetal demise%
Pregnant patients diagnosed with *'& or pulmonary embolism may be treated with LM96throughout their pregnancy% 9arfarin is contraindicated" because it crosses the placental barrierand can cause fetal malformations% (nfractionated heparin is category =% &herefore" LM96 at fullanticoagulation doses should be continued until delivery% 9omen eperiencing a thromboembolicevent during pregnancy should receive therapeutic treatment with unfractionated heparin or LM96during pregnancy" with anticoagulation continuing for ;,2 weeks postpartum and for a total of atleast 2 months%
0n addition to the thrombotic risks in pregnancy" women of childbearing age who are prescribedwarfarin should be advised of the teratogenic effects of this drug% Alteplase is a category = drug"
and should only be given following a Kudicious assessment of the risk,to,benefit ratio%
Pregnant women who are in a hypercoagulable state or who have had previous venousthromboembolism should receive prophylactic anticoagulation during pregnancy%
=omplications
=omplications of pulmonary embolism include the following7
• Sudden cardiac death
• bstructive shock
• Pulseless electrical activity
• Atrial or ventricular arrhythmias
• Secondary pulmonary arterial hypertension
• =or pulmonale
• Severe hypoemia
• Right,to,left intracardiac shunt
• Lung infarction
• Pleural effusion
• Paradoical embolism
• 6eparin,induced thrombocytopenia
• &hrombophlebitis
*eterrence and Prevention of Pulmonary Embolism
Preventing idiopathic outpatient pulmonary embolism is difficult" if not impossible% &hat said" themaKority of pulmonary embolisms occur in hospitali8ed patients% &he incidence in these cases canbe reduced through appropriate prophylais" achieved mechanically or via the administration ofheparin" LM96" or warfarin%-.C>/
&he incidence of venous thrombosis" pulmonary embolism" and death can be significantly reducedby embracing a prophylactic strategy in high,risk patients% Prevention of *'& in the loweretremities inevitably reduces the freHuency of pulmonary embolism! therefore" populations at riskmust be identified" and safe and efficacious prophylactic modalities should be used%
&he F&hrombosis algorithm is intended to identify currently asymptomatic adults at greatest futurerisk of venous thrombosis based on established risk factors% According to the study in which it wasdeveloped and validated" F&hrombosis estimates the absolute risk of venous thrombosis at . year and < years into the future" information that can be used to guide prophylais and medicationdecisions%-.C?/
Medicolegal =oncerns

7/25/2019 Practice Essentials of pulmonary thromboembolism.docx
http://slidepdf.com/reader/full/practice-essentials-of-pulmonary-thromboembolismdocx 24/39
Pulmonary embolism is an etremely common disorder% 0t presents with nonspecific clinicalfeatures and reHuires speciali8ed investigations for confirmation of diagnosis% &herefore" manypatients die from unrecogni8ed pulmonary embolism% &he other common pitfalls are as follows7
• *isregarding patientQs complaints of uneplained dyspnea as aniety or hyperventilation
• Blaming complaints of uneplained chest pain on musculoskeletal pain
•
)ailing to recogni8e" diagnose" and treat *'&• )ailing to initiate an appropriate diagnostic workup in patients with symptoms consistent
with pulmonary embolism
• )ailing to initiate therapeutic anticoagulant therapy with heparin in patients suspected to
have pulmonary embolism" before the 'F scan or other investigations
• )ailure to advise of risk factors" such as smoking" pregnancy" and use of the oral
contraceptive pill
• )ailure to diagnose predisposing or associated conditions
)uture Research
Advances over the past several decades have significantly improved physiciansT ability todiagnosis pulmonary embolism and have refined the treatment of this disorder% 6owever" severalareas need further research and properly conducted therapeutic trials% &he role of LM96 and theoptimal duration of anticoagulant therapy in different subgroups of patients with venousthromboembolism reHuire further study%
Because warfarin therapy results in bleeding" future studies should determine whether less intensewarfarin therapy is effective in preventing recurrences of pulmonary embolism%
9hether drugs that inhibit the action of thrombin #eg" hirudin$ are useful in treating patients withvenous thromboembolic disease also needs to be determined by future trials%
=onsultations
)ibrinolytic therapy should not be delayed while consultation is sought% &he decision to treatpulmonary embolism by fibrinolysis is properly made by the responsible emergency physicianalone" and fibrinolytic therapy is properly administered in the E*%
A pulmonologist is often consulted before the true diagnosis is made because of the nonspecificnature of the symptoms" and consultation with a cardiologist is warranted to rule out a cardiacetiology for the presenting symptoms and signs and to perform E=6 and pulmonaryangiography%
0f embolectomy is considered" consultation with a cardiac surgeon is mandatory% )ew data areavailable regarding the use of surgical embolectomy in children% =onsider embolectomy in thesetting of massive cardiac failure when time is insufficient for natural or pharmacologicthrombolysis or if thrombolysis is contraindicated% &hrombotic endarterectomy is another surgicaltreatment option for patients with hemodynamic compromise from large pulmonary emboli%&hrombotic endarterectomy is only performed at certain centers and has a high mortality rate" butit can be successful in certain populations%
A hematologist can suggest an appropriate workup for a procoagulant defect and can recommend
an anticoagulation regimen% =onsultation with a hematologist is essential in children with sickle celldisease% A free clinical consultation service for comple cases of thromboembolism in children isavailable for clinicians by calling .,?CC,:,=L&S #.,?CC,224,<2?>$%
An interventional radiology consultation may be helpful for catheter,directed fibrinolysis in selectedpatients% 0n rare cases" arranging for placement of a venous filter may be appropriate if the patientis not a candidate for thrombolytic therapy%
Long &erm Monitoring
P& should be measured on a regular basis! the goal is an 0:R of 4,5%
&he length of treatment depends on the presence of risk factors% 0f no underlying risk factors arepresent" therapy can be stopped within .,4 months% 0f risk factors are present" especiallyanticardiolipin antibodies" therapy should continue for at least ;,2 months%

7/25/2019 Practice Essentials of pulmonary thromboembolism.docx
http://slidepdf.com/reader/full/practice-essentials-of-pulmonary-thromboembolismdocx 25/39
Long,term anticoagulation is essential for patients who survive an initial *'& or pulmonaryembolism% &he optimum total duration of anticoagulation is controversial" but general consensusholds that at least 2 months of anticoagulation is associated with significant reduction inrecurrences and a net positive benefit%-.C/
Patients may have treatment initiated using concomitant warfarin and unfractionated heparin for <days in the hospital" with discharge on warfarin alone when the international normali8ed ratio #0:R$is 4% Alternatively" patients may be discharged on concomitant therapy with a LM96 and warfarinfor at least < days% &he LM96 is then discontinued in the outpatient setting when the 0:R reaches4%
• Medication Summary
• Anticoagulants
• &hrombolytics
• *irect &hrombin 0nhibitors and )actor +a 0nhibitors
• Show All
Multimedia LibraryReferences
Medication Summary
0mmediate therapeutic anticoagulation is initiated for patients with suspected deep venousthrombosis #*'&$ or pulmonary embolism #PE$% Anticoagulation therapy with heparin reducesmortality rates from 5C3 to less than .C3% Anticoagulation is essential" but anticoagulation alonedoes not guarantee a successful outcome% *'& and PE may recur or etend despite full andeffective heparin anticoagulation%
=hronic anticoagulation is critical to prevent relapse of *'& or PE following initial heparini8ation%6eparin works by activating antithrombin 000 to slow or prevent the progression of *'& and toreduce the si8e and freHuency of PE% 6eparin does not dissolve eisting clot%
&he ninth edition of the American =ollege of =hest Physicians #A==P$ guidelines forantithrombotic and thrombolytic therapy are summari8ed as follows7-/
• &hrombolytic therapy should be used in patients with acute PE associated with
hypotension #systolic BPI C mm 6G$" who do not have a high bleeding risk #grade 4=$%
• &hrombolytic therapy is suggested in select patients with acute PE not associated with
hypotension and with a low bleeding risk whose initial clinical presentation or clinical course after starting anticoagulation suggests a high risk of developing hypotension #grade 4=$ +
• Assessment of pulmonary embolism severity" prognosis" and risk of bleeding dictate
whether thrombolytic therapy should be started% &hrombolytic therapy is not recommended formost patients with acute PE not associated with hypotension #grade .=$%
&he current A==P guidelines recommend that all patients with unprovoked PE receive threemonths of treatment with anticoagulation rather than a shorter duration of treatment" and have anassessment of the risk,to,benefit ratio of etended therapy at the end of three months #grade .B$%
Patients with a first episode of venous thromboembolism and with a low or moderate risk ofbleeding should have etended anticoagulant therapy #grade 4B$% Patients with a first episode ofvenous thromboembolism who have a high bleeding risk should have therapy limited to threemonths #grade .B$% 0n patients with a second unprovoked episode of venous thromboembolismand low or moderate risk of bleeding" etended anticoagulant therapy is recommended #grades .Band 4B" respectively$% 0n patients with a second episode of venous thromboembolism and a highrisk of bleeding" three months of anticoagulation is preferred rather than etended anticoagulation#grade 4B$%
Patients who have PE and preeisting irreversible risk factors" such as deficiency of antithrombin
000" protein S and =" factor ' Leiden mutation" or the presence of antiphospholipid antibodies"should be placed on long,term anticoagulation%

7/25/2019 Practice Essentials of pulmonary thromboembolism.docx
http://slidepdf.com/reader/full/practice-essentials-of-pulmonary-thromboembolismdocx 26/39
Anticoagulants
0lass Summary
6eparin augments the activity of antithrombin 000 and prevents the conversion of fibrinogen to fibrin%)ull,dose LM96 or full,dose unfractionated 0' heparin should be initiated at the first suspicion of*'& or PE%
9ith proper dosing" several LM96 products have been found safer and more effective thanunfractionated heparin both for prophylais and for treatment of *'& and PE% Monitoring the aP&&is neither necessary nor useful when giving LM96" because the drug is most active in a tissuephase and does not eert most of its effects on coagulation factor 00a%
Many different LM96 products are available around the world% Because of pharmacokineticdifferences" dosing is highly product specific% Several LM96 products are approved for use in the(nited States7 enoaparin #Loveno$" dalteparin #)ragmin$" and tin8aparin #0nnohep$% Enoaparinand tin8aparin are currently approved by the )*A for treatment of *'&% *alteparin is )*Aapproved for prophylais and has approval for cancer patients% Each of the other agents has beenapproved by the )*A at a lower dose for prophylais" but all appear to be safe and effective atsome therapeutic dose in patients with active *'& or PE%
)ractionated LM96 administered subcutaneously is now the preferred choice for initialanticoagulation therapy% (nfractionated 0' heparin can be nearly as effective but is more difficult totitrate for therapeutic effect% 9arfarin maintenance therapy may be initiated after .,5 days ofeffective heparini8ation%
&he weight,adKusted heparin dosing regimens that are appropriate for prophylais and treatment of coronary artery thrombosis are too low to be used unmodified in the treatment of active *'& andPE% =oronary artery thrombosis does not result from hypercoagulability but rather from plateletadhesion to ruptured plaHue% 0n contrast" patients with *'& and PE are in the midst of ahypercoagulable crisis" and aggressive countermeasures are essential to reduce mortality andmorbidity rates%
'iew full drug information
Enoxaparin 1,o%enox2
Eonaparin was the first low,molecular,weight heparin #LM96$ released in the (nited States% 0twas approved by the )*A for both treatment and prophylais of *'& and PE% Enoaparinenhances the inhibition of factor +a and thrombin by increasing antithrombin 000 activity% 0n addition"it preferentially increases the inhibition of factor +a% LM96 has been used widely in pregnancy"although clinical trials are not yet available to demonstrate that it is as safe as unfractionatedheparin% Ecept in overdoses" checking P& or aP&& has no utility" as aP&& does not correlate withanticoagulant effect of fractionated LM96% )actor +a levels can be monitored if concern arisesabout whether the dose is adeHuate%
'iew full drug information
Dalteparin 1Fragmin2
*alteparin is an LM96 with many similarities to enoaparin but with a different dosing schedule% 0tis approved for *'& prophylais in patients undergoing abdominal surgery% Ecept in overdoses"checking P& or aP&& has no utility" as aP&& does not correlate with anticoagulant effect offractionated LM96% LM96% )actor +a levels can be monitored if concern arises about whetherthe dose is adeHuate%
'iew full drug information
Tin#aparin 1"nno'ep2
&in8aparin is approved for treatment of *'& in hospitali8ed patients% Enhances inhibition of factor+a and thrombin by increasing antithrombin 000 activity% 0n addition" preferentially increasesinhibition of factor +a%
'iew full drug information
!eparin 1!ep-,oc& (3P4 !ep-,oc&4 !ep-Flus'-562
6eparin augments the activity of antithrombin 000 and prevents conversion of fibrinogen to fibrin% 0tdoes not actively lyse but is able to inhibit further thrombogenesis% 6eparin prevents thereaccumulation of a clot after spontaneous fibrinolysis% 9hen ()6 is used" the aP&& should not be

7/25/2019 Practice Essentials of pulmonary thromboembolism.docx
http://slidepdf.com/reader/full/practice-essentials-of-pulmonary-thromboembolismdocx 27/39
checked until 2 hours after the initial heparin bolus" because an etremely high or low value duringthis time should not provoke any action
'iew full drug information
/arfarin 10oumadin4 7anto%en2
9arfarin #=oumadin$ interferes with the hepatic synthesis of vitamin dependent coagulation
factors% 0t is used for the prophylais and treatment of venous thrombosis" pulmonary embolism"and thromboembolic disorders% :ever administer warfarin to patients with thrombosis until afterthey have been fully anticoagulated with heparin #the first few days of warfarin therapy produce ahypercoagulable state$% )ailing to anticoagulate with heparin before starting warfarin causes clotetension and recurrent thromboembolism in approimately ;C3 of patients" compared with ?3 ofthose who receive full,dose heparin before starting warfarin% 6eparin should be continued for thefirst <,> days of oral warfarin therapy" regardless of the P& time" to allow time for depletion ofprocoagulant vitamin dependent proteins%
&ailor the warfarin dose to maintain an 0:R in the range of 4%<,5%<% &he risk of serious bleeding#including hemorrhagic stroke$ is approimately constant when the 0:R is 4%<,;%< but risesdramatically when the 0:R is over <% 0n the (nited ingdom" a higher 0:R target of 5,; often isrecommended%
Evidence suggests that 2 months of anticoagulation reduces the rate of recurrence to half of therecurrence rate observed when only 2 weeks of anticoagulation is given% Long,termanticoagulation is indicated for patients with an irreversible underlying risk factor and recurrent*'& or recurrent pulmonary embolism%
Procoagulant vitamin dependent proteins are responsible for a transient hypercoagulable statewhen warfarin is first started and stopped% &his is the phenomenon that occasionally causeswarfarin,induced necrosis of large areas of skin or of distal appendages% 6eparin is always used toprotect against this hypercoagulability when warfarin is started! when warfarin is stopped" however"the problem resurfaces" causing an abrupt" temporary rise in the rate of recurrent venousthromboembolism%
At least .?2 different foods and drugs reportedly interact with warfarin% =linically significantinteractions have been verified for a total of 42 common drugs and foods" including 2 antibiotics
and < cardiac drugs% Every effort should be made to keep the patient adeHuately anticoagulated atall times" because procoagulant factors recover first when warfarin therapy is inadeHuate%
Patients who have difficulty maintaining adeHuate anticoagulation while taking warfarin may beasked to limit their intake of foods that contain vitamin %
)oods that have moderate to high amounts of vitamin include Brussels sprouts" kale" green tea"asparagus" avocado" broccoli" cabbage" cauliflower" collard greens" liver" soybean oil" soybeans"certain beans" mustard greens" peas #black,eyed peas" split peas" chick peas$" turnip greens"parsley" green onions" spinach" and lettuce%
'iew full drug information
Fondaparinux sodium 1Arixtra2
)ondaparinu sodium is a synthetic anticoagulant that works by inhibiting factor +a" a keycomponent involved in blood clotting% 0t provides a highly predictable response and has abioavailability of .CC3% &he drug has a rapid onset of action and a half,life of .;,.2 hours" allowingfor sustained antithrombotic activity over a 4;,hour period% )ondaparinu sodium does not affectprothrombin time or activated partial thromboplastin time" nor does it affect platelet function oraggregation%
&hrombolytics
0lass Summary
&hrombolysis is indicated for hemodynamically unstable patients with pulmonary embolism%&hrombolysis dramatically improves acute cor pulmonale% &hrombolytic therapy has replacedsurgical embolectomy as the treatment for hemodynamically unstable patients with massivepulmonary embolism%

7/25/2019 Practice Essentials of pulmonary thromboembolism.docx
http://slidepdf.com/reader/full/practice-essentials-of-pulmonary-thromboembolismdocx 28/39
)ibrinolytic regimens currently in common use for pulmonary embolism include 4 forms ofrecombinant tPA" alteplase and reteplase" along with urokinase and streptokinase% Alteplaseusually is given as a front,loaded infusion over C or .4C minutes% (rokinase and streptokinaseusually are given as infusions over 4; hours or more% Reteplase is a new,generation thrombolyticwith a longer half,life! it is given as a single bolus or as 4 boluses administered 5C minutes apart%
f the ; drugs" the faster,acting agents reteplase and alteplase are preferred for patients withpulmonary embolism" because the condition of patients with pulmonary embolism can deteriorateetremely rapidly%
Many comparative clinical studies have shown that administration of a 4,hour infusion of alteplaseis more effective #and more rapidly effective$ than urokinase or streptokinase over a .4,hourperiod% ne prospective" randomi8ed study comparing reteplase and alteplase found that totalpulmonary resistance #along with pulmonary artery pressure and cardiac inde$ improvedsignificantly after Kust one half hour in the reteplase group as compared with 4 hours in thealteplase group% )ibrinolytic agents do not seem to differ significantly with respect to safety oroverall efficacy%
Streptokinase is least desirable of all the fibrinolytic agents because antigenic problems and otheradverse reactions force the cessation of therapy in a large number of cases%
Empiric thrombolysis may be indicated in selected hemodynamically unstable patients" particularlywhen the clinical likelihood of pulmonary embolism is overwhelming and the patientQs condition isdeteriorating% &he overall risk of severe complications from thrombolysis is low and the potentialbenefit in a deteriorating patient with pulmonary embolism is high% Empiric therapy especially isindicated when a patient is compromised so severely that he or she wil l not survive long enough toobtain a confirmatory study% Empiric thrombolysis should be reserved" however" for cases that trulymeet these definitions" as many other clinical entities #including aortic dissection$ may masHueradeas pulmonary embolism" yet may not benefit from thrombolysis in any way%
:ewborns may be relatively resistant to thrombolytics because of their lack of fibrinogen activity%
'iew full drug information
Reteplase 1Reta%ase2
Reteplase is a second,generation recombinant tissue plasminogen activator #recombinant tPA$that forms plasmin after facilitating cleavage of endogenous plasminogen% 0n clinical trials"reteplase has been shown to be comparable to the recombinant tPA alteplase in achieving &0M0" 4or 5 patency" at C minutes% Reteplase is given as a single bolus or as 4 boluses administered 5Cminutes apart%
As a fibrinolytic agent" reteplase seems to work faster than its forerunner" alteplase" and may bemore effective in patients with larger clot burdens% 0t has also been reported to be more effectivethan other agents in lysis of older clots% &wo maKor differences help to eplain these improvements%Because reteplase does not bind fibrin as tightly as does alteplase" this allows reteplase drug todiffuse more freely through the clot% Another advantage seems to be that reteplase does notcompete with plasminogen for fibrin,binding sites" allowing plasminogen at the site of the clot to betransformed into clot,dissolving plasmin%
&he )*A has not approved reteplase for administration to patients with pulmonary embolism%Studies of the drugQs use for pulmonary embolism have employed the same dose approved by the)*A for coronary artery fibrinolysis%
'iew full drug information
Alteplase 1Acti%ase4 0at'flo Acti%ase2
Alteplase" a recombinant tPA" is used in the management of acute myocardial infarction #AM0$"acute ischemic stroke" and pulmonary embolism% Alteplase is most often used to treat patients withpulmonary embolism in the E*% 0t is usually given as a front,loaded infusion over C,.4C minutes%0t is )*A approved for this indication% Most E* personnel are familiar with alteplaseQs use" becauseit is widely employed in the treatment of patients with AM0% An accelerated C,minute regimen iswidely used" and most believe it is safer and more effective than the approved 4,hour infusion% Anaccelerated,regimen dose is based on patient weight%
6eparin therapy should be instituted or reinstituted near the end of or immediately followinginfusion" when the aP&& or thrombin time returns to twice normal or less%

7/25/2019 Practice Essentials of pulmonary thromboembolism.docx
http://slidepdf.com/reader/full/practice-essentials-of-pulmonary-thromboembolismdocx 29/39
(ro&inase 1Abbo&inase4 8inlytic2
(rokinase is a direct plasminogen activator produced by human fetal kidney cells grown in culture%0t acts on the endogenous fibrinolytic system and converts plasminogen to the en8yme plasmin"which" in turn" degrades fibrin clots" fibrinogen" and other plasma proteins% An advantage ofurokinase is that it is nonantigenic! however" it is more epensive than streptokinase" which limitsits use% 9hen urokinase is used for locali8ed fibrinolysis" it is given as a local" catheter,directed"
continuous infusion directly into area of the thrombus with no loading dose% 9hen it is used forpulmonary embolism" a loading dose is necessary%
Strepto&inase 1Streptase2
Streptokinase acts with plasminogen to convert plasminogen to plasmin% Plasmin degrades fibrinclots" fibrinogen" and other plasma proteins% An increase in fibrinolytic activity that degradesfibrinogen levels for 4;,52 hours takes place with 0' infusion of streptokinase% &he agent is highlyantigenic" and it is highly likely that treatment will be interrupted due to allergic drug reactions%
=hills" fever" nausea" and skin rashes are freHuent #up to 4C3$% Blood pressure and heart ratedrop in approimately .C3 of cases during or shortly after treatment%
Late complications may include purpura" respiratory distress syndrome" serum sickness" Guillain,
BarrU syndrome" vasculitis" and renal or hepatic dysfunction%
*irect &hrombin 0nhibitors and )actor +a 0nhibitors
0lass Summary
)actor +a inhibitors inhibit platelet activation by selectively blocking the active site of factor +awithout reHuiring a cofactor #eg" antithrombin 000$ for activity% *irect thrombin inhibitors preventsthrombus development through direct" competitive inhibition of thrombin" thus blocking theconversion of fibrinogen to fibrin during the coagulation cascade%
'iew full drug information
Ri%aroxaban 1.arelto2
0ndicated for treatment of PE and for prevention of recurrence #following initial 2 months of
treatment$%
'iew full drug information
Apixaban 1Eliuis2
0ndicated for treatment of PE and for prevention of recurrence #following initial 2 months oftreatment$%
'iew full drug information
Dabigatran 1Pradaxa2
*abigatran is indicated for treatment of *'& and PE in patients who have been treated with aparenteral anticoagulant for <,.C days% 0t is also indicated to reduce the risk of recurrence of *'&and PE in patients who have been previously treated%
'iew full drug information
Edoxaban 1Sa%aysa2
Edoaban is a factor +a inhibitor indicated for treatment of *'& and PE in patients who have beeninitially treated with a parenteral anticoagulant for <,.C days%
Definition
By Mayo Clinic Staff

7/25/2019 Practice Essentials of pulmonary thromboembolism.docx
http://slidepdf.com/reader/full/practice-essentials-of-pulmonary-thromboembolismdocx 30/39
Appointments & care
At Mayo Clinic, we take the time to listen, to find answers and to
provide you the best care.
Learn more. Request an appointment.
Multimedia
•
Pulmonary embolism
Pulmonary embolism is a blockage in one of the pulmonary arteries in your
lungs. In most cases, pulmonary embolism is caused by blood clots that travelto the lungs from the legs or, rarely, other parts of the body (deep vein
thrombosis).
Because pulmonary embolism almost always occurs in conjunction with deep
vein thrombosis, most doctors refer to the two conditions together as venous
thromboembolism.
Although anyone can develop deep vein thrombosis (DVT) and pulmonary
embolism, factors such as immobility, cancer and surgery increase your risk.
Pulmonary embolism can be life-threatening, but prompt treatment can greatly
reduce the risk of death. Taking measures to prevent blood clots in your legs
will help protect you against pulmonary embolism.
Symptoms
By Mayo Clinic Staff

7/25/2019 Practice Essentials of pulmonary thromboembolism.docx
http://slidepdf.com/reader/full/practice-essentials-of-pulmonary-thromboembolismdocx 31/39
Pulmonary embolism symptoms can vary greatly, depending on how much of
your lung is involved, the size of the clots and your overall health — especially
the presence or absence of underlying lung disease or heart disease.
Common signs and symptoms include:
• Shortness of breath. This symptom typically appears suddenly and
always gets worse with exertion.
• Chest pain. You may feel like you're having a heart attack. The pain
may become worse when you breathe deeply (pleurisy), cough, eat, bend
or stoop. The pain will get worse with exertion but won't go away when you
rest.
• Cough. The cough may produce bloody or blood-streaked sputum.
Other signs and symptoms that can occur with pulmonary embolism include:
• Leg pain or swelling, or both, usually in the calf
• Clammy or discolored skin (cyanosis)
• Fever
• Excessive sweating
• Rapid or irregular heartbeat
• Lightheadedness or dizziness
When to see a doctor
Pulmonary embolism can be life-threatening. Seek immediate medical
attention if you experience unexplained shortness of breath, chest pain or a
cough that produces bloody sputum.
Causes
By Mayo Clinic Staff
Multimedia

7/25/2019 Practice Essentials of pulmonary thromboembolism.docx
http://slidepdf.com/reader/full/practice-essentials-of-pulmonary-thromboembolismdocx 32/39
•
Pulmonary embolism
Pulmonary embolism occurs when a clump of material, most often a blood
clot, gets wedged into an artery in your lungs. These blood clots most
commonly originate in the deep veins of your legs, but they can also come
from other parts of your body. This condition is known as deep vein
thrombosis (DVT).
Occasionally, substances other than blood clots can form blockages within the
blood vessels inside your lungs. Examples include:
• Fat from within the marrow of a broken long bone
• Part of a tumor
• Air bubbles
It's rare to have a single pulmonary embolism. In most cases, multiple clots
are involved but not necessarily all at once. The portions of lung tissue served
by each blocked artery are robbed of blood and may die. This is known aspulmonary infarction. This makes it more difficult for your lungs to provide
oxygen to the rest of your body.
Risk factors
By Mayo Clinic Staff
Multimedia
•
Blood clot in leg
Although anyone can develop blood clots and subsequent pulmonary
embolism, certain factors can increase your risk.
Medical history

7/25/2019 Practice Essentials of pulmonary thromboembolism.docx
http://slidepdf.com/reader/full/practice-essentials-of-pulmonary-thromboembolismdocx 33/39
You're at higher risk if you or any of your family members have had venous
blood clots or pulmonary embolism in the past. This may be due to inherited
disorders that affect blood, making it more prone to clot.
In addition, certain medical conditions put you at risk, such as:
• Heart disease. Cardiovascular disease, specifically heart failure,
makes clot formation more likely.
• Cancer. Certain cancers — especially pancreatic, ovarian and lung
cancers, and many cancers with metastasis — can increase levels of
substances that help blood clot, and chemotherapy further increases the
risk. Women with a personal or family history of breast cancer who are
taking tamoxifen or raloxifene also are at higher risk of blood clots.Prolonged immobility
Blood clots are more likely to form in your legs during periods of inactivity,
such as:
• Bed rest. Being confined to bed for an extended period after surgery, a
heart attack, leg fracture, trauma or any serious illness makes you far
more vulnerable to blood clots. When the lower extremities are horizontal
for long periods of time, the flow of venous blood slows and blood pools inthe legs.
• Long journeys. Sitting in a cramped position during lengthy plane or
car trips slows blood flow, which contributes to the formation of clots in
your legs.
Surgery
Surgery is one of the leading causes of problem blood clots, especially seen
after joint replacements of the hip and knee. During the preparation of thebones for the artificial joints, tissue debris may enter the bloodstream and
contribute to causing a clot. Simply being immobile during any type of surgery
can lead to the formation of clots. The risk increases with the length of time
you're under general anesthesia. For this reason, most people undergoing a
type of surgery predisposing them to DVT will receive medication before and
after surgery to prevent clot formation.
Other risk factors

7/25/2019 Practice Essentials of pulmonary thromboembolism.docx
http://slidepdf.com/reader/full/practice-essentials-of-pulmonary-thromboembolismdocx 34/39
• Smoking. For reasons that aren't well-understood, tobacco use
predisposes some people to blood clot formation, especially when
combined with other risk factors.
• Being overweight. Excess weight increases the risk of blood clots —particularly in women who smoke or have high blood pressure.
• Supplemental estrogen. The estrogen in birth control pills and in
hormone replacement therapy can increase clotting factors in your blood,
especially if you smoke or are overweight.
• Pregnancy. The weight of the baby pressing on veins in the pelvis can
slow blood return from the legs. Clots are more likely to form when blood
slows or pools.
Complications• By Mayo Clinic Staff
• Pulmonary embolism can be life-threatening. About one-third of people
with undiagnosed and untreated pulmonary embolism don't survive.
When the condition is diagnosed and treated promptly, however, that
number drops dramatically.
• Pulmonary embolism can also lead to pulmonary hypertension, a
condition in which the blood pressure in your lungs and in the right sideof the heart is too high. When you have obstructions in the arteries
inside your lungs, your heart must work harder to push blood through
those vessels. This increases the blood pressure within these vessels
and the right side of the heart, which can weaken your heart.
• In rare cases, small emboli occur frequently and develop over time,
resulting in chronic pulmonary hypertension, also known as chronic
thromboembolic pulmonary hypertension.
Tests and diagnosis• By Mayo Clinic Staff
•
Appointments & care

7/25/2019 Practice Essentials of pulmonary thromboembolism.docx
http://slidepdf.com/reader/full/practice-essentials-of-pulmonary-thromboembolismdocx 35/39
• At Mayo Clinic, we take the time to listen, to find answers
and to provide you the best care.
• Learn more. Request an appointment.
• Pulmonary embolism can be difficult to diagnose, especially in people
who have underlying heart or lung disease. For that reason, your doctor
may order a series of tests to help find the cause of your symptoms.
Your doctor may order one or more of the following tests.
Blood tests• Your doctor may order a blood test for the clot-dissolving substance D
dimer in your blood. High levels may suggest an increased likelihood of
blood clots, although D dimer levels may be elevated by many other
factors, including recent surgery. In addition, blood tests may be done
to determine whether you have an inherited clotting disorder.
Chest X-ray• This noninvasive test shows images of your heart and lungs on film.
Although X-rays can't diagnose pulmonary embolism and may even
appear normal when pulmonary embolism exists, they can rule outconditions that mimic the disease.
Ultrasound• A noninvasive "sonar" test known as duplex ultrasonography
(sometimes called duplex scan, or compression ultrasonography) uses
high-frequency sound waves to check for blood clots in your thigh
veins. In this test, your doctor uses a wand-shaped device called a
transducer to direct the sound waves to the veins being tested. These
waves are then reflected back to the transducer and translated into amoving image by a computer. The absence of the presence of clots
reduces the likelihood of DVT. If the upper thigh vessels are clear, the
ultrasonography will also scan the veins behind the knee looking for
residual clots. If clots are present, treatment likely will be started
immediately.
CT scan• Regular CT scans take X-rays from many different angles and then
combine them to form images showing 2-D "slices" of your internal
structures. In a spiral (helical) CT scan, the scanner rotates around

7/25/2019 Practice Essentials of pulmonary thromboembolism.docx
http://slidepdf.com/reader/full/practice-essentials-of-pulmonary-thromboembolismdocx 36/39
your body in a spiral — like the stripe on a candy cane — to create 3-D
images. This type of CT can detect abnormalities within the arteries in
your lungs with much greater precision, and it's also much faster than
are conventional CT scans. In some cases, contrast material is given
intravenously during the CT scan to outline the pulmonary arteries.
Pulmonary angiogram• This test provides a clear picture of the blood flow in the arteries of your
lungs. It's the most accurate way to diagnose pulmonary embolism, but
because it requires a high degree of skill to administer and has
potentially serious risks, it's usually performed when other tests fail to
provide a definitive diagnosis.
• In a pulmonary angiogram, a flexible tube (catheter) is inserted into a
large vein — usually in your groin — and threaded through into yourheart and on into the pulmonary arteries. A special dye is then injected
into the catheter, and X-rays are taken as the dye travels along the
arteries in your lungs.
• One risk of this procedure is a temporary change in your heart rhythm.
In addition, the dye may cause kidney damage in people with
decreased kidney function.
MRI• MRI scans use radio waves and a powerful magnetic field to produce
detailed images of internal structures. Because MRI is expensive, it's
usually reserved for pregnant women (to avoid radiation to the fetus)
and people whose kidneys may be harmed by dyes used in other tests.
Treatments and drugs
By Mayo Clinic Staff
Appointments & care

7/25/2019 Practice Essentials of pulmonary thromboembolism.docx
http://slidepdf.com/reader/full/practice-essentials-of-pulmonary-thromboembolismdocx 37/39
At Mayo Clinic, we take the time to listen, to find answers and to
provide you the best care.
Learn more. Request an appointment.
Treatment is aimed at keeping the blood clot from getting bigger and
preventing new clots from forming. Prompt treatment is essential to prevent
serious complications or death.
Medications
• Blood thinners (anticoagulants). These drugs prevent new clots from
forming while your body works to break up the clots. Heparin is a
frequently used anticoagulant that can be given through the vein or
injected under the skin. It acts quickly and is often overlapped for several
days with an oral anticoagulant, such as warfarin, until it becomes
effective, which can take days. A newer class of anticoagulants has been
tested and approved for treatment of venous thromboembolism, including
pulmonary embolism. These medications have the advantage of being
given by mouth, without the need for overlap with heparin. Also, they work
quickly and have fewer interactions with other medications. All blood
thinners have side effects, with bleeding being the most common.
• Clot dissolvers (thrombolytics). While clots usually dissolve on their
own, there are medications given through the vein that can dissolve clots
quickly. Because these clot-busting drugs can cause sudden and severe
bleeding, they usually are reserved for life-threatening situations.
Surgical and other procedures
• Clot removal. If you have a very large, life-threatening clot in your lung,
your doctor may suggest removing it via a thin, flexible tube (catheter)
threaded through your blood vessels.
Vein filter. A catheter can also be used to position a filter into the body's main
vein — called the inferior vena cava — that leads from your legs to the right
side of your heart. This filter can help keep clots from being carried into your

7/25/2019 Practice Essentials of pulmonary thromboembolism.docx
http://slidepdf.com/reader/full/practice-essentials-of-pulmonary-thromboembolismdocx 38/39
lungs. This procedure is typically reserved for people who can't take
anticoagulant drugs or when anticoagulant drugs don't work well enough or
fast enough. The catheter with the filter in the tip is usually inserted in a vein in
your neck, and then into the vena cava. Some filters can be removed when
they are no longer needed. Prevention
By Mayo Clinic Staff
Preventing clots in the deep veins in your legs (deep vein thrombosis) will help
prevent pulmonary embolism. For this reason, most hospitals are aggressive
about taking measures to prevent blood clots, including:
• Anticoagulants. Anticoagulants are often given to people at risk of
clots before and after an operation — as well as to people admitted to the
hospital with a heart attack, stroke or complications of cancer.
• Compression stockings. Compression stockings steadily squeeze
your legs, helping your veins and leg muscles move blood more efficiently.
They offer a safe, simple and inexpensive way to keep blood from
stagnating during and after general surgery.
• Pneumatic compression. This treatment uses thigh-high or calf-high
cuffs that automatically inflate with air and deflate every few minutes to
massage and squeeze the veins in your legs and improve blood flow.
• Physical activity. Moving as soon as possible after surgery can help
prevent pulmonary embolism and hasten recovery overall. This is one of
the main reasons your nurse may push you to get up, even on your day of
surgery, and walk despite pain at the site of your surgical incision.
• Leg elevation. Elevating your legs when possible and during the night
also can be very effective. Raise the bottom of your bed 4 to 6 inches with
blocks or books.
Prevention while traveling
The risk of blood clots developing while traveling is low, but increases as travel
increases. If you have risk factors for blood clots and you're concerned about
traveling, talk with your doctor. He or she might suggest the following steps to
help prevent blood clots from forming:

7/25/2019 Practice Essentials of pulmonary thromboembolism.docx
http://slidepdf.com/reader/full/practice-essentials-of-pulmonary-thromboembolismdocx 39/39
• Take a break from sitting. Move around the airplane cabin once an
hour or so. If you're driving, stop every hour and walk around the car a
couple of times. Do a few deep knee bends.
• Fidget in your seat. Flex your ankles every 15 to 30 minutes, or tryrising up and down on your toes while standing. Don't sit with your legs
crossed at the knees for long periods of time.
• Drink plenty of fluids. Water is the best liquid for preventing
dehydration, which can contribute to the development of blood clots. Avoid
alcohol, which contributes to fluid loss.
• Wear support stockings. Your doctor may recommend these to help
promote circulation and fluid movement in your legs. Compressionstockings no longer look like something only a grandmother would wear —
they're available in a range of stylish colors and textures. There are even
devices, called stocking butlers, to help you put on the stockings.
•
















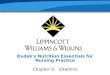



![[Www.englishcourses.edu.Vn]Thomson - IELTS Practice Tests Exam Essentials](https://img.pdfslide.us/doc/110x75/54964344ac7959a4178b4574/wwwenglishcourseseduvnthomson-ielts-practice-tests-exam-essentials.jpg)