Embed Size (px)
Citation preview

Practice AlertPractice AlertDysrhythmia MonitoringDysrhythmia Monitoring
Issued April 2008Issued April 2008
Authors & Reviewers:Authors & Reviewers:Nancy M. Richards, RN, CNS, MSN, CCRN, CCNSNancy M. Richards, RN, CNS, MSN, CCRN, CCNS

Practice Alert - Dysrhythmia Monitoring2
Lecture Content
Skin Preparation Lead Placement Ventricular Dysrhythmias QT Intervals

Practice Alert - Dysrhythmia Monitoring3
Skin Preparation
Skin oil and debris can cause noisy signals Clip excessive hair before placing
electrodesClean skin with alcohol or washcloth
to remove skin oils and/or debris

Practice Alert - Dysrhythmia Monitoring4
Electrode PlacementLimb leads (I,II,III)
Place to decrease muscle artifact during limb movement
PlacementRight Arm (RA) infra-clavicular fossa close to right
shoulderLeft Arm (LA) infra-clavicular fossa close to left
shoulderLeft Leg (LL) below rib cage on left side of
abdomenGround (RL) anywhere on torso

Practice Alert - Dysrhythmia Monitoring5
Electrode Placement
Precordial LeadsDependent on patient’s needs and goals of
monitoringConsider marking electrode location with
indelible ink Ensures electrodes will be placed in same
position.
Precordial leads misplaced by 1 ICS can change the QRS morphology

Practice Alert - Dysrhythmia Monitoring6
Dysrhythmia Monitoring
Lead V1 to distinguish Ventricular Tachycardia (VT) from Supraventricular Tachycardia (SVT) with aberrant conduction
V1 lead of choice for dysrhythmia monitoringLead II or III if patient condition indicates
need to monitor for atrial dysrhythmias

Practice Alert - Dysrhythmia Monitoring7
Dysrhythmia Monitoring Lead Placement
V1 (5 lead system)
4th intercostal space (ICS) to the right of the sternum
MCL1 (3 lead system)
4th intercostal space (ICS) to the right of the sternum

Practice Alert - Dysrhythmia Monitoring8
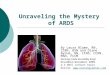
3 Lead Electrode Placement
Simple 3-electrode lead system
Electrode placement for MCL1
Only 1 lead can be monitored with a 3 lead system
From Philips Cardiac Monitoring Pocket Card 2002

Practice Alert - Dysrhythmia Monitoring9
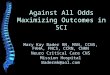
5 Lead Electrode Placement
5 lead systems allow for the recording of any of the six limb leads plus one precordial (V) lead.
Shown lead placement for recording V1 or V6.
5 Lead monitoring systems are recommended over 3 lead systems for monitoring QRS morphology
From Philips Cardiac Monitoring Pocket Card 2002
V1V1
V
6
V
6
Angle of Louis
Angle of Louis

Practice Alert - Dysrhythmia Monitoring10
QRS Morphology Ventricular Tachycardia
V 1 or MCL1 Monophasic R wave Notched R wave with
taller left peak Biphasic RS Biphasic qR Any of the following in V1
or V2
R > 30ms Slurred or notched S
descent QRS onset to S nadir
>60 ms
V6 or MCL6 Biphasic rS with R:S
ratio <1.0 Monophasic Q Notched QS Biphasic qR Intrinsicoid deflection >
70ms

Practice Alert - Dysrhythmia Monitoring11
QRS Morphology
From Philips Cardiac Monitoring Pocket Card 2002

Practice Alert - Dysrhythmia Monitoring12
QRS MorphologySVT with Aberration
V1 or MCL1
Bimodal rR’ or triphasic rsR’
All of the following in V1 or V2 R < 30 ms or no R Straight S descent QRS onset to S nadir
< 60 ms and no Q in V6
V6 or MCL6
Triphasic qRs with R:s ratio > 1.0
Intrinsicoid deflection < 50 ms

Practice Alert - Dysrhythmia Monitoring13
QRS Morphology
From Philips Cardiac Monitoring Pocket Card 2002

Practice Alert - Dysrhythmia Monitoring14
QRS MorphologyNot Helpful
V1 or MCL1
R slurred or notched with taller right peak
V6 or MCL6
Monophasic RNotched R with taller
left or right peakBiphasic Rs with R:S
ratio > 1.0
Applies only to tachycardias with a positive waveform in V1

Practice Alert - Dysrhythmia Monitoring15
QRS Morphology
From Philips Cardiac Monitoring Pocket Card 2002

Practice Alert - Dysrhythmia Monitoring16
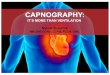
Accurate Lead Placement
V1
II
V1
II
(A) Onset of wide QRS complex tachycardia shows a “taller right peak” pattern in lead V1, which is unhelpful in distinguishing between ventricular tachycardia and supraventricular tachycardia with aberrant conduction. Examination of the patient revealed that the V1 electrode was misplaced to the 5th, rather than the 4th intercostal space
(B) After lead placement was corrected, another episode of wide QRS complex tachycardia showed the “taller left peak” pattern in lead V1 which is strongly suggestive of ventricular tachycardia (Wellens, et al 1978). Subsequent invasive cardiac electrophysiologic study confirmed the patient had ventricular tachycardia.
Used with permission of Barbara J. Drew RN, PhD

Practice Alert - Dysrhythmia Monitoring17
QT Interval
Approximate measure of the duration of ventricular repolarization.
Measured from the beginning of the Q wave to the end of the T wave
Varies with heart rateLengthens with bradycardiaShortens with tachycardia

Practice Alert - Dysrhythmia Monitoring18
QT Interval
Measure from beginning of the QRS complex to the end of the T wave
From Philips Cardiac Monitoring Pocket Card 2002

Practice Alert - Dysrhythmia Monitoring19
QTc Interval
QT interval corrected for heart rate (QTc)Formula for calculating QTc (Bazett’s formula)
QTc > 0.50 seconds considered dangerously prolonged and is associated with a higher risk of Torsades de Pointes.

Practice Alert - Dysrhythmia Monitoring20
Measuring the QTc
• Measure the QT of the second complex used in R – R measurement.
• Using Bazett’s formula: QTc = 0.36 / √0.72 = 0.36 / 0.85 = 0.42
QTc = 0.42
QT = 0.36
R – R = 0.72

Practice Alert - Dysrhythmia Monitoring21
Torsades de Pointes
Polymorphic Ventricular TachycardiaPrecipitated by prolonged QT intervalNot responsive to and may be
exacerbated by class Ia and some Ic medications

Practice Alert - Dysrhythmia Monitoring22
Arrhythmias associated with prolonged QT interval that place the patient at immediate risk for developing torsades de pointes. ECG characteristics include underlying prolonged QT interval, T wave alternans, polymorphic ventricular premature beats that fall near the T-U portion of repolarization, pause-dependent enhancement of the QT interval (arrow), and non-sustained polymorphic ventricular tachycardia.
Pause
Used with permission of Barbara J. Drew RN, PhD

Practice Alert - Dysrhythmia Monitoring23
Torsades de PointesMonitor QT interval for patients identified at
high risk:Patients on medications known to prolong QT
intervalQuinidine, procainaminde,
disopyraminde, sotalol, dofetilide, ibutilideFor more information see:
http://www.arizonacert.org/medical-pros/drug-lists/printable-drug-list.cfm
Patients who overdose on potentially pro- dysrhythmic medications
New onset bradycardiaSevere hypokalemia or hypomagnesemia

Practice Alert - Dysrhythmia Monitoring24
Treatment
Emergency•IV Magnesium•Defibrillation•Overdrive pacing
Long Term•Monitor QTc interval•Discontinue or modify drug dose if QTc interval increases > 0.50 secs

Practice Alert - Dysrhythmia Monitoring25
For more information or further assistance, please contact a clinical practice specialist with the AACN Practice Resource Network.
Email:[email protected]
Phone:
(800) 394-5995
Need Further Assistance?