Embed Size (px)
Citation preview
Dr. S.L. Asa Pituitary and Parathyroid Pathology
1
Practical Procedures Practical Procedures for Problematic for Problematic
Parathyroids and Pituitaries Parathyroids and Pituitaries Sylvia L. Asa, M.D., Ph.D.
Pathologist-in-Chief and Medical Director, Laboratory Medicine ProgramUniversity Health Network
Senior Scientist, Ontario Cancer Institute
Professor, Department of Laboratory Medicine and Pathobiology University of Toronto
Pituitary ProblemsPituitary Problems
The autopsy pituitary: Grossing and handling
The surgical specimen: Pituitary or not?If pituitary, hyperplasia or adenoma?If adenoma, what kind?What is this inflammation all about?
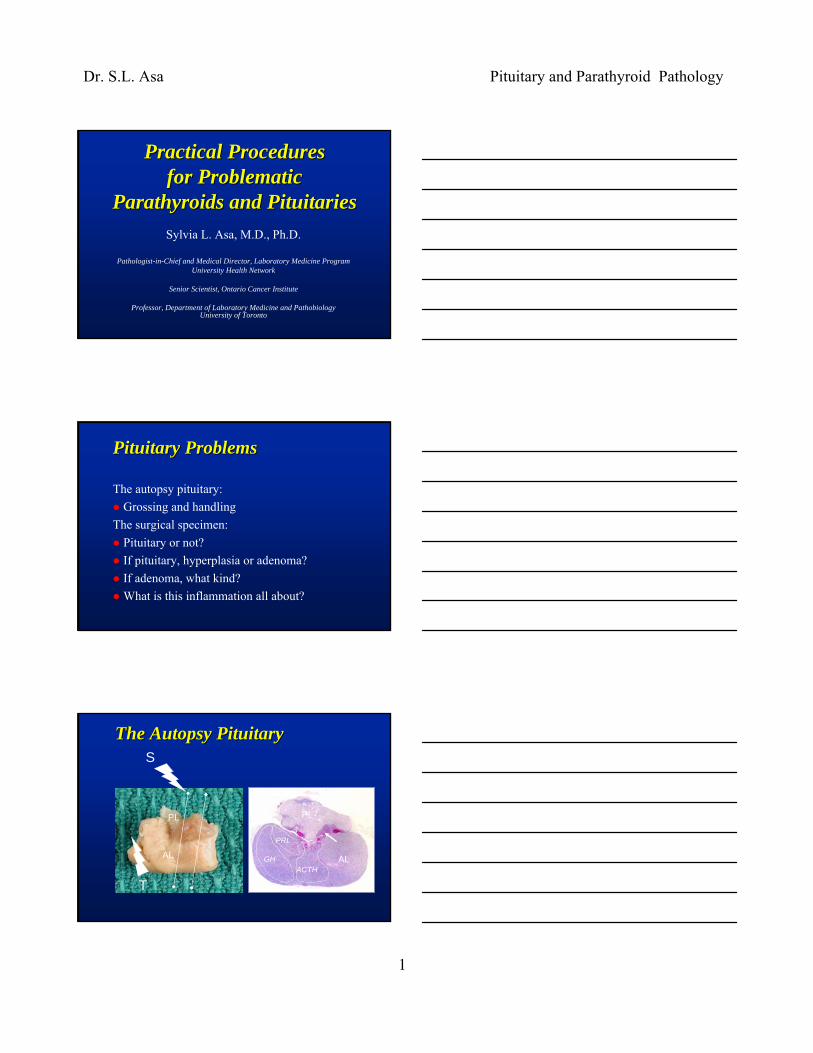
S
T
TPL
ALACTH
GH
PRL
PL
AL
The Autopsy PituitaryThe Autopsy Pituitary
Dr. S.L. Asa Pituitary and Parathyroid Pathology
2
Pitfalls in Autopsy PituitariesPitfalls in Autopsy Pituitaries
Infarcts and fibrosisBasophil invasion of the posterior lobeCrooke’s hyaline changeHypophysitisTumorsTumorsTumors
The Surgical Biopsy:The Surgical Biopsy:Is This PituitaryIs This Pituitary??
Pituitary adenomas (or very rare carcinoma)Craniopharyngiomas, cystsOther CNS lesions» neuronal tumors, paraganglioma, pituicytoma, glioma,
meningioma, schwannomaVascular and mesenchymal tumors» spindle cell oncocytoma, granular cell tumors, chordomas
Lymphomas, leukemias, histiocytoses, germ cell tumorsMetastatic
What Is This CystWhat Is This Cyst??
Rathke cleft cyst vs CraniopharyngiomaArachnoid Cyst Dermoid vs Epidermoid
Dr. S.L. Asa Pituitary and Parathyroid Pathology
3
This is Pituitary; Now WhatThis is Pituitary; Now What??
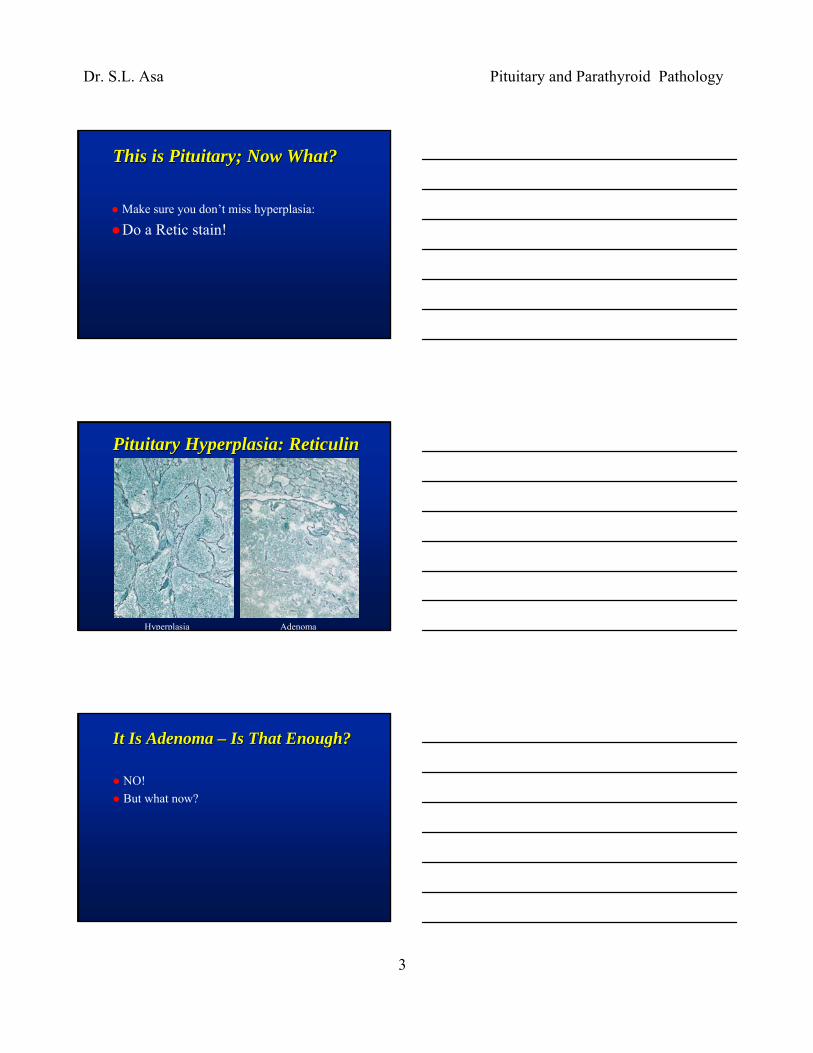
Make sure you don’t miss hyperplasia:
Do a Retic stain!
Pituitary Hyperplasia: ReticulinPituitary Hyperplasia: Reticulin
Hyperplasia Adenoma
It Is Adenoma It Is Adenoma –– Is That EnoughIs That Enough??
NO!But what now?
Dr. S.L. Asa Pituitary and Parathyroid Pathology
4
Prognostic Markers in Prognostic Markers in Pituitary TumorsPituitary Tumors
Best is still tumor typeBest is still tumor typeClinicopathologic features – size, invasionOthers suggested:» MIB-1 (<5%, 5-15%, >15%)» PTTG (same idea as MIB-1)» p27 (lost in corticotroph adenomas)» p53 (no proven value)
Pituitary Tumor ClassificationPituitary Tumor Classification
Silent subtype 3Null cell, oncocytoma
PlurihormonalUnclassified
Silent gonadotrophGonadotropin Excess
Gonadotroph
Silent thyrotrophTSH excess
Thyrotroph
Silent lactotrophPRL excess
LactotrophAcidophil stem cell
Silent somatotroph
GH excessDG/SG somatotrophMammosomatotroph
Silent corticotrophACTH excess
Corticotroph adenoma
SilentFunctioning
Immunohistochemical ClassificationImmunohistochemical Classificationof Pituitary Adenomasof Pituitary Adenomas
Major ComponentGH-PRL-TSH» GH
» SG, DG
» GH/PRL» PRL» TSH
ACTHGonadotropinUnclassified
Other ReactivityPit-1» α-subunit
» Keratins
» α-subunit, ER» ER» α-subunit
TpitSF-1???

Dr. S.L. Asa Pituitary and Parathyroid Pathology
5
Pitfalls in CushingPitfalls in Cushing’’s Diseases Disease
Usual finding: basophil microadenomaProblem 1: Large chromophobe adenomaProblem 2: No adenomaProblem 3: Crooke’s cell adenoma
Sparsely Granulated Corticotroph AdenomaSparsely Granulated Corticotroph AdenomaPAS
ACTH
CushingCushing’’s Diseases Disease::The Case of the Missing AdenomaThe Case of the Missing Adenoma
Cushing’s vs Pseudo-Cushing’s» Crooke’s hyaline change
Dr. S.L. Asa Pituitary and Parathyroid Pathology
6
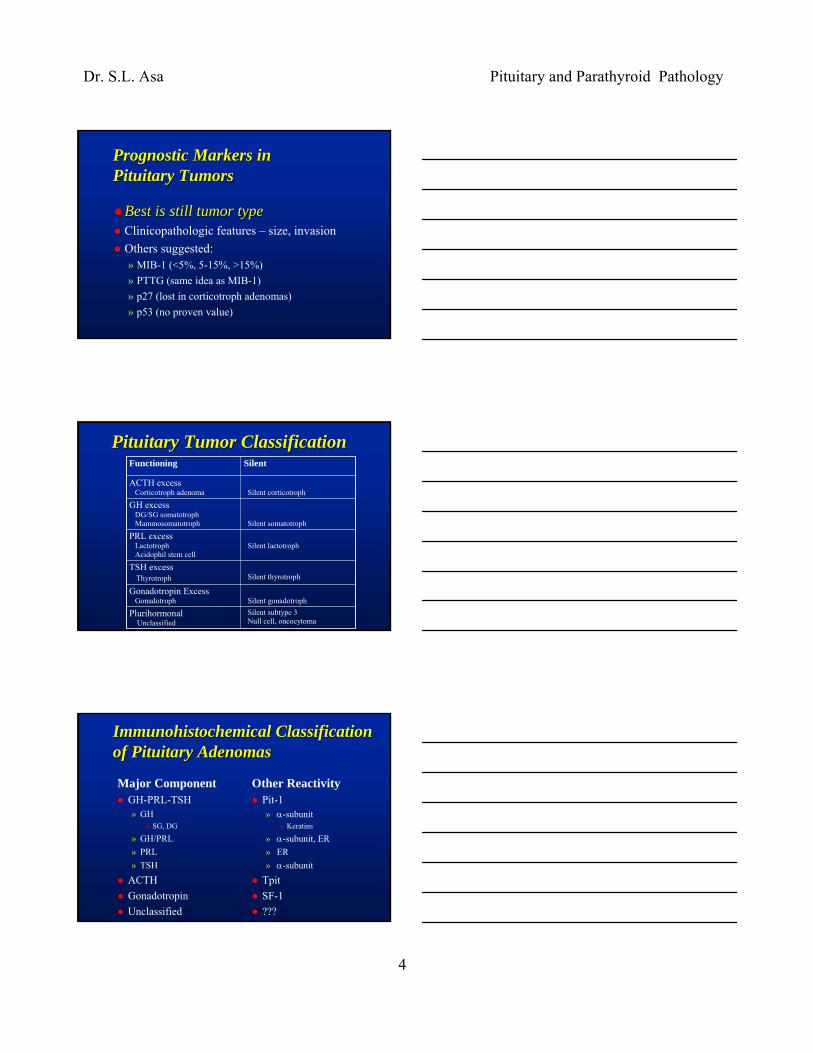
Cytology of Cytology of ““NormalNormal”” GlandGlandPAS
ACTH and Cam 5.2ACTH and Cam 5.2ACTH
Cam 5.2
CrookesCrookes’’ Cell AdenomaCell Adenoma
Keratin accumulation in cytoplasm
Dr. S.L. Asa Pituitary and Parathyroid Pathology
7
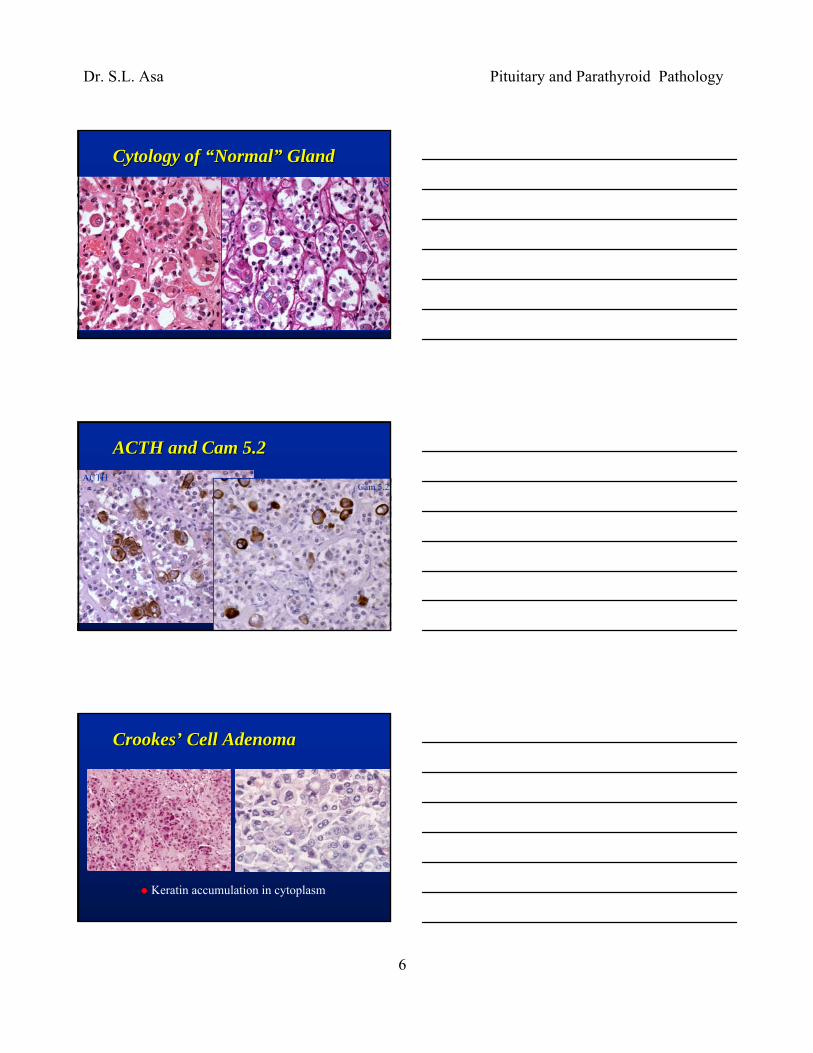
AcromegalyAcromegaly--Gigantism (Gigantism (↑↑ GH):GH):Differential DiagnosisDifferential Diagnosis
Adenoma vs hyperplasiaSomatotroph vs Mammosomatotroph adenomaDensely vs Sparsely granulated adenomaGangliocytoma
Somatotroph HyperplasiaSomatotroph Hyperplasia
H&E Reticulin GH
Ectopic GRH in Endocrine TumorsEctopic GRH in Endocrine Tumors
H&E GRH
Dr. S.L. Asa Pituitary and Parathyroid Pathology
8
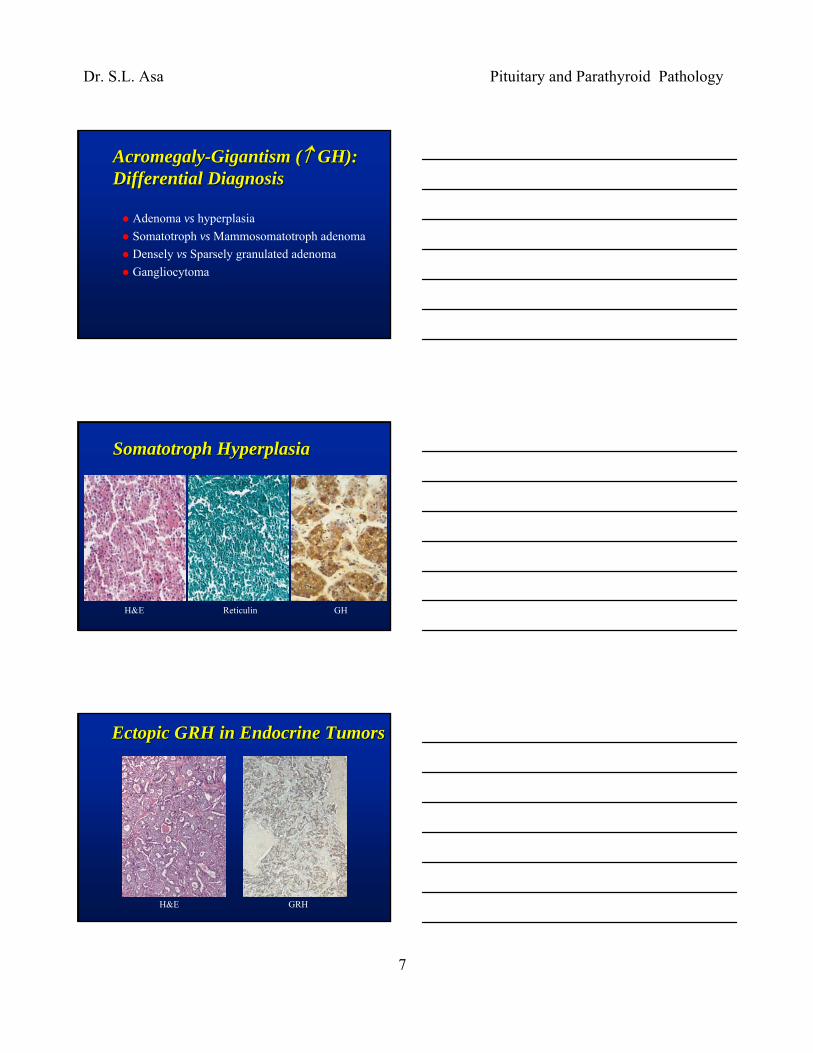
AcromegalyAcromegaly--Gigantism (Gigantism (↑↑ GH);GH);Pituitary AdenomasPituitary Adenomas
Somatotroph vs MammosomatotrophDensely vs Sparsely granulated (keratin)
H&E Cam 5.2 H&E Cam 5.2
Sellar Gangliocytoma with Sellar Gangliocytoma with Pituitary AdenomaPituitary Adenoma
H&E GHRH GH
Prognostic and Therapeutic Prognostic and Therapeutic Considerations in AcromegalyConsiderations in Acromegaly
Hyperplasia» look for source of GHRH excess
Densely granulated somatotroph adenoma» likely responsive to somatostatin analogue therapy
Sparsely granulated somatotroph adenoma» may be due to altered GH autoregulation» may be candidates for GH antagonist therpay
Mammosomatotroph adenoma» possible response to dopaminergic agents
Dr. S.L. Asa Pituitary and Parathyroid Pathology
9
Pitfalls in HyperprolactinemiaPitfalls in Hyperprolactinemia
Adenoma vs Other TumorAdenoma vs HyperplasiaAdenoma vs Lymphocytic HypophysitisSparsely Granulated vs Densely GranulatedAcidophil Stem Cell Adenoma
Inflammatory Lesions of the Inflammatory Lesions of the Pituitary: HypophysitisPituitary: Hypophysitis
Lymphocytic hypophysitisGranulomatous hypophysitisXanthomatous hypophysitisInfundibulo-neurohypophysitisSecondary hypophysitis
Lymphocytic Hypophysitis: HistologyLymphocytic Hypophysitis: Histology

Dr. S.L. Asa Pituitary and Parathyroid Pathology
10
Granulomatous HypophysitisGranulomatous Hypophysitis
Xanthomatous HypophysitisXanthomatous HypophysitisThe least common form of primary hypophysitisResembles xanthomatous inflammatory processes elsewhere, such as xanthomatous cholecystitis, endometritis or pyelonephritisCystic on radiologic or surgical evaluationMay be a response to ruptured cyst???
InfundibuloInfundibulo--NeurohypophysitisNeurohypophysitis
RarePresent with isolated diabetes insipidusLocalized enlargement of posterior lobe/stalkLymphoplasmacytic infiltrate resembling LH? Autoimmune disorder
Dr. S.L. Asa Pituitary and Parathyroid Pathology
11
Pitfalls in TSH HypersecretionPitfalls in TSH Hypersecretion
Thyrotroph hyperplasia
Pituitary TSH ExcessPituitary TSH Excess
HyperplasiaH&E» large chromophobic
“thyroidectomy cells”» interspersed acidophils
and basophilsPAS» positive globules
Reticulin stain» acini intact, enlarged
AdenomaH&E » monotonous population of
elongated chromophobes» marked nuclear atypia» nil else
PAS» positive globules
Reticulin stain» acini disrupted
Histology: Thyrotroph HyperplasiaHistology: Thyrotroph Hyperplasia
H&E PAS Reticulin
Dr. S.L. Asa Pituitary and Parathyroid Pathology
12
The Role of the PathologistThe Role of the Pathologistin the Management of Patients in the Management of Patients with Pituitary Pathologywith Pituitary Pathology
To ensure correct diagnosisTo guide correct managementTo be responsible for ongoing investigations to determine pathogenesis and future therapies
ReferencesReferencesAsa SL: Tumors of the Pituitary Gland. Fascicle 22, Third Series, in The Atlas of Tumor Pathology, Armed Forces Institute of Pathology, Washington DC, 1998.(Fourth series in press)ASA SL: Practical Pituitary Pathology: What Does the Pathologist Need to Know? Arch Pathol Lab Med 2008;132:1231-1240 ASA SL, EZZAT S: The pathogenesis of pituitary adenomas. Nature Reviews Cancer 2002; 2:836-49.ASA SL, EZZAT S: The pathogenesis of pituitary tumors. Annu Rev Pathol 2009;4:97-126..
Dr. S.L. Asa Pituitary and Parathyroid Pathology
13
Parathyroid ProblemsParathyroid Problems
Parathyroid or not?If parathyroid, hyperplasia or adenoma?What about carcinoma?
The The ““OldOld”” Approach to Approach to Parathyroid SurgeryParathyroid Surgery
Identify all parathyroid glandsRemove dominant pathologyBiopsy all other glands
→Put the onus on the Pathologist to make the diagnosis of hyperplasia vs adenoma» often wrong or impossible!
The The ““NewNew”” Approach to Approach to Parathyroid SurgeryParathyroid Surgery
Radioguided surgery identifies the dominant glandLimited approach traumatizes only that glandIntraoperative PTH measurement confirms resection of culprit lesion
→ Pathologist only needs to confirm that abnormal (cellular) parathyroid tissue was resected
Dr. S.L. Asa Pituitary and Parathyroid Pathology
14
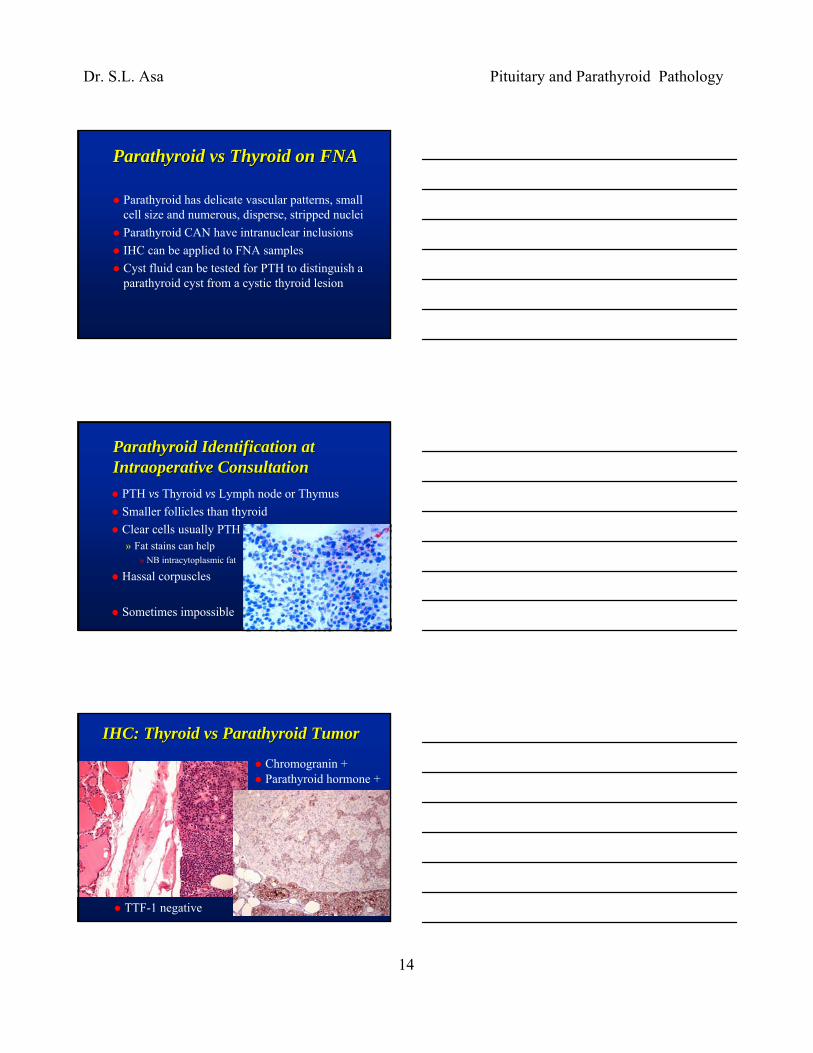
Parathyroid Parathyroid vsvs Thyroid on FNAThyroid on FNA
Parathyroid has delicate vascular patterns, small cell size and numerous, disperse, stripped nucleiParathyroid CAN have intranuclear inclusionsIHC can be applied to FNA samplesCyst fluid can be tested for PTH to distinguish a parathyroid cyst from a cystic thyroid lesion
Parathyroid Identification at Parathyroid Identification at Intraoperative ConsultationIntraoperative Consultation
PTH vs Thyroid vs Lymph node or ThymusSmaller follicles than thyroidClear cells usually PTH» Fat stains can help
» NB intracytoplasmic fat
Hassal corpuscles
Sometimes impossible
IHC: Thyroid vs Parathyroid TumorIHC: Thyroid vs Parathyroid Tumor
Chromogranin +Parathyroid hormone +
TTF-1 negative
Dr. S.L. Asa Pituitary and Parathyroid Pathology
15
Hyperplasia Hyperplasia vsvs AdenomaAdenomaHyperplasia» multiple (>1) glands» poorly encapsulated» diffuse or nodular» comparable areas in
adjacent glands» all 3 cell types» mitoses but little
pleomorphism
Neoplasia» solitary» encapsulated» nodule » adjacent normal gland
no hypercellularity» chief cells predominate» nuclear pleomorphism
WrongDoesn’t matter
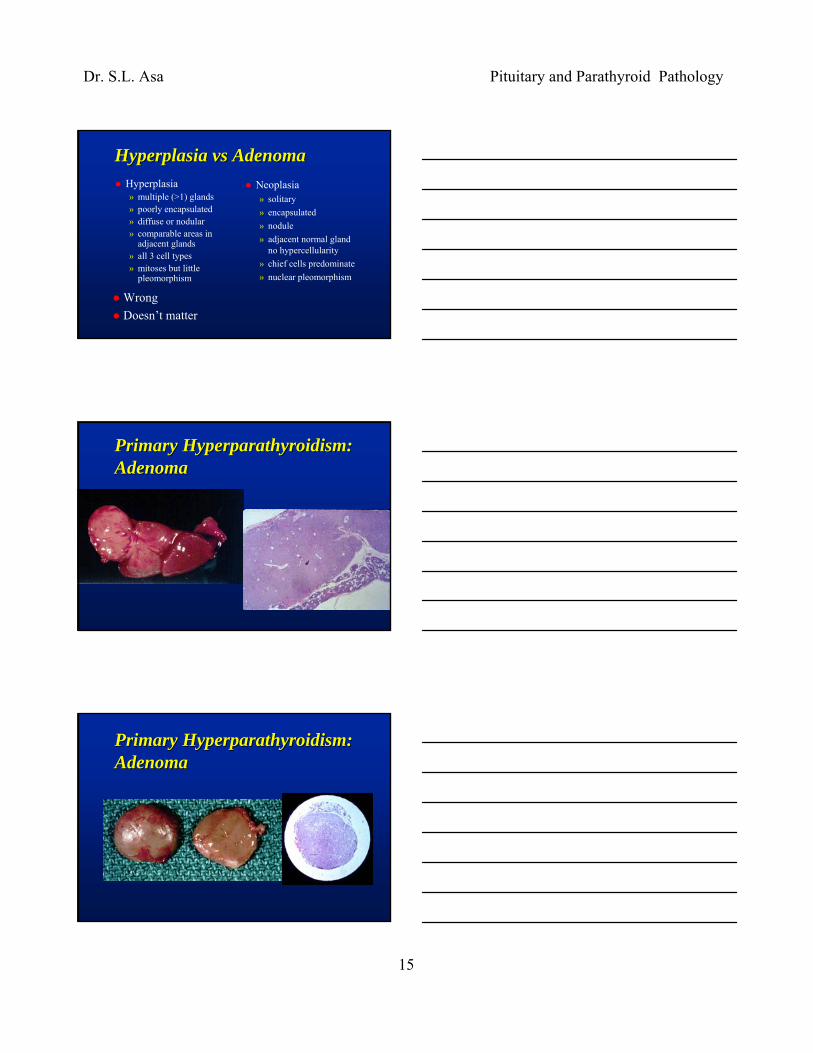
Primary Hyperparathyroidism:Primary Hyperparathyroidism:AdenomaAdenoma
Primary Hyperparathyroidism:Primary Hyperparathyroidism:AdenomaAdenoma
Dr. S.L. Asa Pituitary and Parathyroid Pathology
16
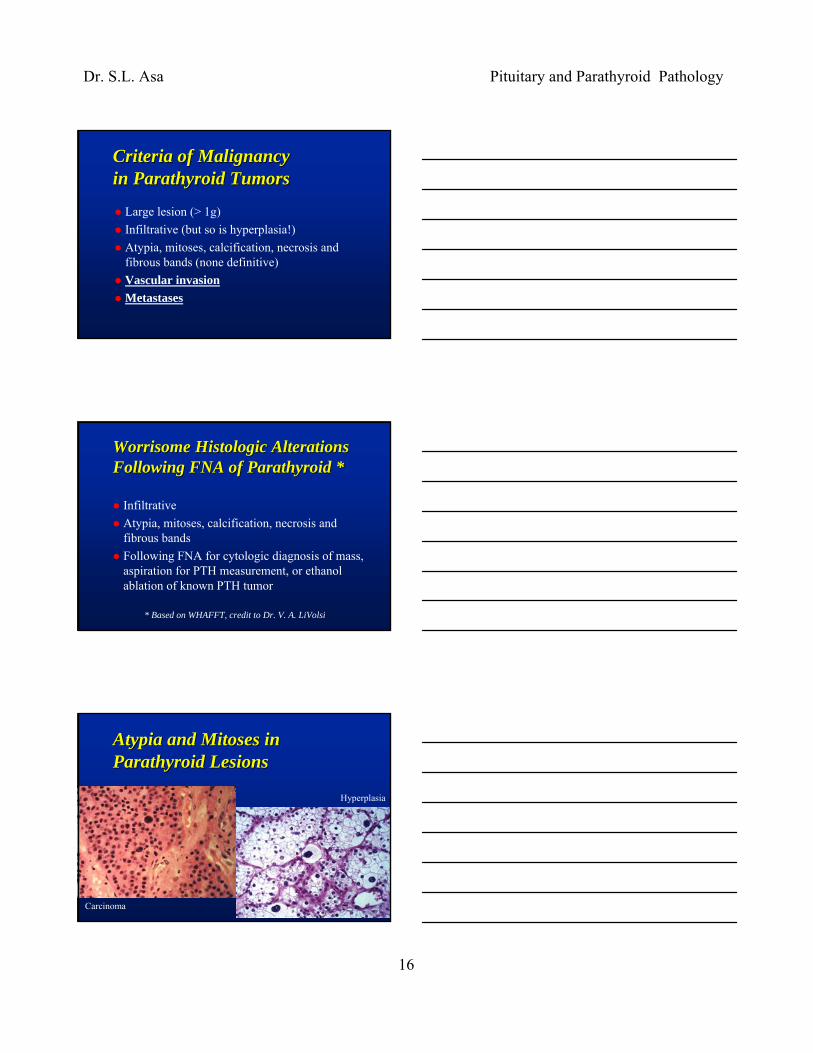
Criteria of MalignancyCriteria of Malignancyin Parathyroid Tumorsin Parathyroid Tumors
Large lesion (> 1g)Infiltrative (but so is hyperplasia!)Atypia, mitoses, calcification, necrosis and fibrous bands (none definitive)Vascular invasionMetastases
Worrisome Histologic Alterations Worrisome Histologic Alterations Following FNA of Parathyroid *Following FNA of Parathyroid *
InfiltrativeAtypia, mitoses, calcification, necrosis and fibrous bands Following FNA for cytologic diagnosis of mass, aspiration for PTH measurement, or ethanol ablation of known PTH tumor
* Based on WHAFFT, credit to Dr. V. A. LiVolsi
Atypia and Mitoses in Atypia and Mitoses in Parathyroid LesionsParathyroid Lesions
Carcinoma
Hyperplasia

Dr. S.L. Asa Pituitary and Parathyroid Pathology
17
Necrosis and CalcificationNecrosis and Calcification
WorrisomeMore common in carcinoma
Not diagnostic alone
Fibrosis:Fibrosis:HyperplasiaHyperplasiavs Carcinomavs Carcinomavsvs PostPost--FNAFNA
Criteria of Malignancy:Criteria of Malignancy:InfiltrationInfiltration
Infiltration through capsule in a proven neoplasmAlso seen in hyperplasia →

Dr. S.L. Asa Pituitary and Parathyroid Pathology
18
Local Invasion vs Local Invasion vs Intrathyroidal ParathyroidIntrathyroidal Parathyroid
Intrathyroidal parathyroids are common
Can mimic thyroid invasion by carcinoma
Vascular Invasion: Unequivocal Vascular Invasion: Unequivocal Evidence of MalignancyEvidence of Malignancy
Parathyroid Carcinoma:Parathyroid Carcinoma:Metastases Metastases
Lymph nodesBoneLungsAdrenals

Dr. S.L. Asa Pituitary and Parathyroid Pathology
19
Ancillary Tests for Borderline CasesAncillary Tests for Borderline Cases
Parafibromin loss
ImmunostainsImmunostains
Negative Rb ↓
High MIB-1 ↑p53 positivity
ReferencesReferences
DeLellis RA: Tumors of the Parathyroid Gland. Fascicle 6, Third Series, in The Atlas of Tumor Pathology, Armed Forces Institute of Pathology, Washington DC, 1993 Apel RL and Asa SL: The parathyroid glands. In Endocrine Pathology, LiVolsi VA and Asa SL (eds), Philadelphia, Churchill Livingstone, 2002, pp. 103-147DeLellis RA, Lloyd RV, Heitz PU, and Eng C: Pathology and Genetics of Tumours of Endocrine Organs. Lyons, France IARC Press, 2004