Embed Size (px)
Citation preview

Practical Guide to Selecting Tissue for Molecular Diagnostics:
A Case-based Approach and Live Microscope Tutorial
Dara L. Aisner, M.D., Ph.D.
Co-Director, Colorado Molecular Correlates Laboratory
University of Colorado
Sinchita Roy-Chowdhuri, M.D., Ph.D. MD Anderson Cancer Center
Disclosures
• DLA: Honoraria from Clovis Oncology and AstraZeneca
Molecular Profiling: The Next Wave in Cancer Care • Molecular status for key analytes is now standard of care for several
disease types • Lung cancer: EGFR, ALK, ROS1 (KRAS, RET, MET, BRAF,
ERBB2) • Colon Cancer: KRAS, NRAS (BRAF, PIK3CA) • Melanoma: BRAF (NRAS, KIT) • GIST: KIT, PDGFRA
• Evolving targets • PIK3CA, PTEN, AKT1: potential implications for use of mTOR
inhibitors (Everolimus, Temsirolimus) • MAP2K1/2 (and family members): Trametinib, MEK inhibitors • FGFR family (Regorafanib, Ponatanib etc) • NOTCH1: gamma-secretase inhibitors
Important Details of a Molecular Test to Know • No such thing as a perfect test – ALL tests have
limitations • Clinical and Analytical Sensitivity
• What does the test look for? • Not all tests detect all possible alterations
• How sensitively does the test look for these changes? • All tumor samples are a mixture of tumor and non-tumor cells • Some tests require a much higher proportion of tumor cells to
work – this requirement can be hard to fulfill
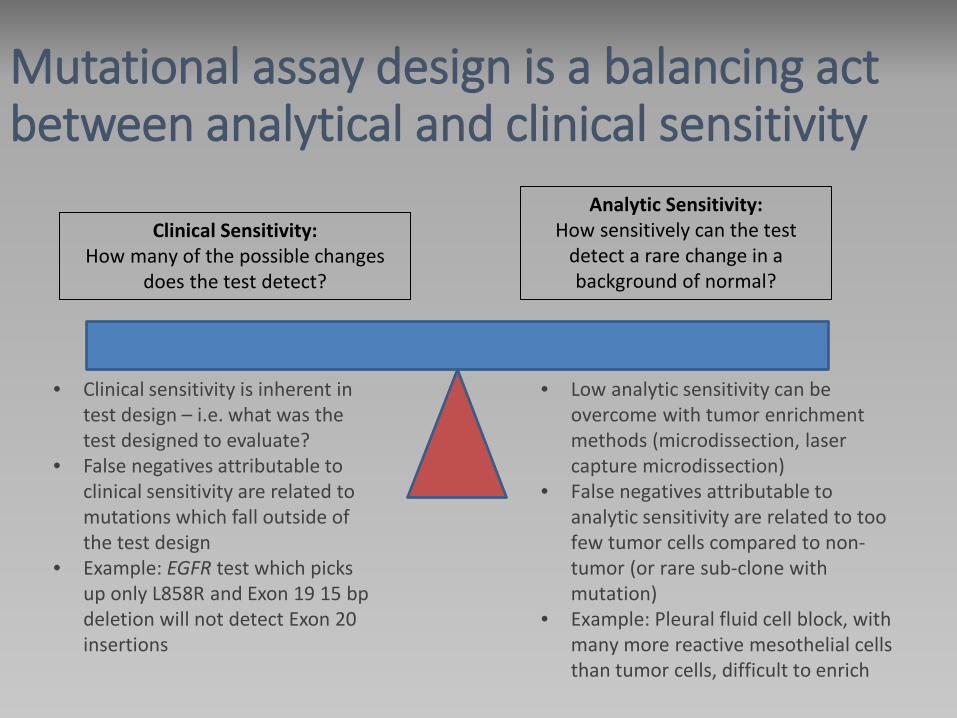
Mutational assay design is a balancing act between analytical and clinical sensitivity
Analytic Sensitivity: How sensitively can the test
detect a rare change in a background of normal?
Clinical Sensitivity: How many of the possible changes
does the test detect?
• Low analytic sensitivity can be overcome with tumor enrichment methods (microdissection, laser capture microdissection)
• False negatives attributable to analytic sensitivity are related to too few tumor cells compared to non-tumor (or rare sub-clone with mutation)
• Example: Pleural fluid cell block, with many more reactive mesothelial cells than tumor cells, difficult to enrich
• Clinical sensitivity is inherent in test design – i.e. what was the test designed to evaluate?
• False negatives attributable to clinical sensitivity are related to mutations which fall outside of the test design
• Example: EGFR test which picks up only L858R and Exon 19 15 bp deletion will not detect Exon 20 insertions

Looking for a needle in a haystack - The test can identify needles of many
different colors, but need to exist at a relatively high level
Looking for a needle in a haystack - The test can identify only a couple of
colors of needles, but can pick them out even when they are very rare
Analytic Sensitivity: How sensitively can the test
detect a rare change in a background of normal?
Clinical Sensitivity: How many of the possible changes
does the test detect?
Mutational assay design is a balancing act between analytical and clinical sensitivity
Analytical Sensitivity
Analytical sensitivity:
ability of a test to reliably detect a mutation (lowest limit of detection) in a sample
e.g. 20% analytical sensitivity means reliably detects a mutation when present in at least 20% of ALL ALLELES (normal + mutant)
Assuming most tumors are heterozygous, a given sample would need to have at least 40% tumor cells to give the required 20% mutant alleles to be detected.
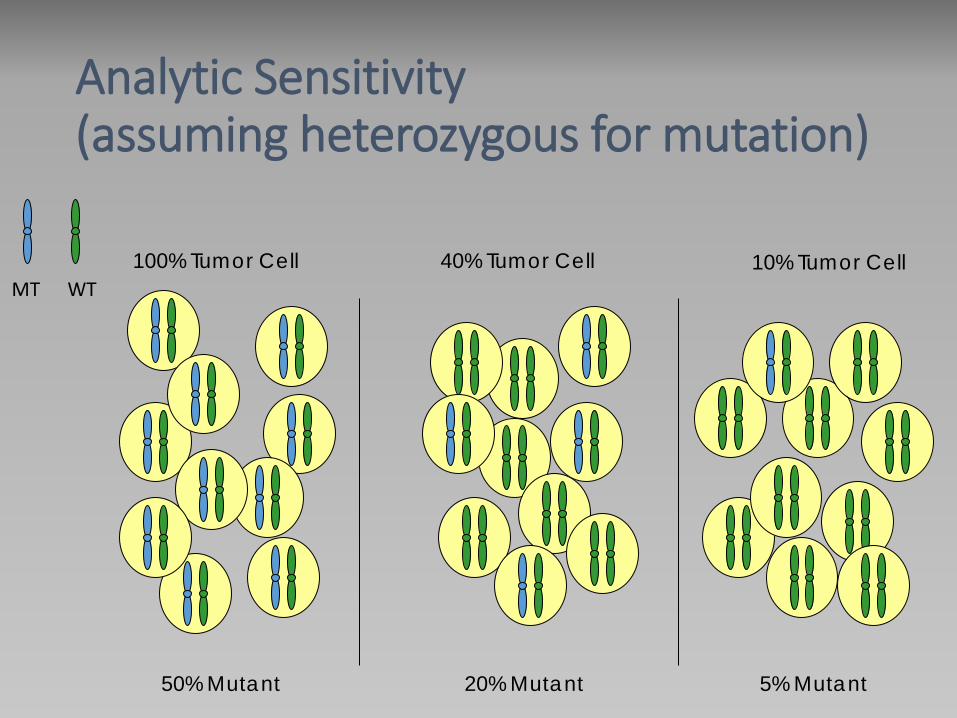
Analytic Sensitivity (assuming heterozygous for mutation)
MT
50% Mutant
100% Tumor Cell WT
40% Tumor Cell
20% Mutant
10% Tumor Cell
5% Mutant

Generally speaking, as clinical sensitivity improves, the analytical sensitivity decreases and vice versa.
Targeted assays usually have a high analytical sensitivity but are limited in the number of changes that can be detected (i.e. low clinical sensitivity).
Assays with high clinical sensitivity can detect a wide range of changes, but require a higher allelic proportion
Mutational assay design is a balancing act between analytical and clinical sensitivity
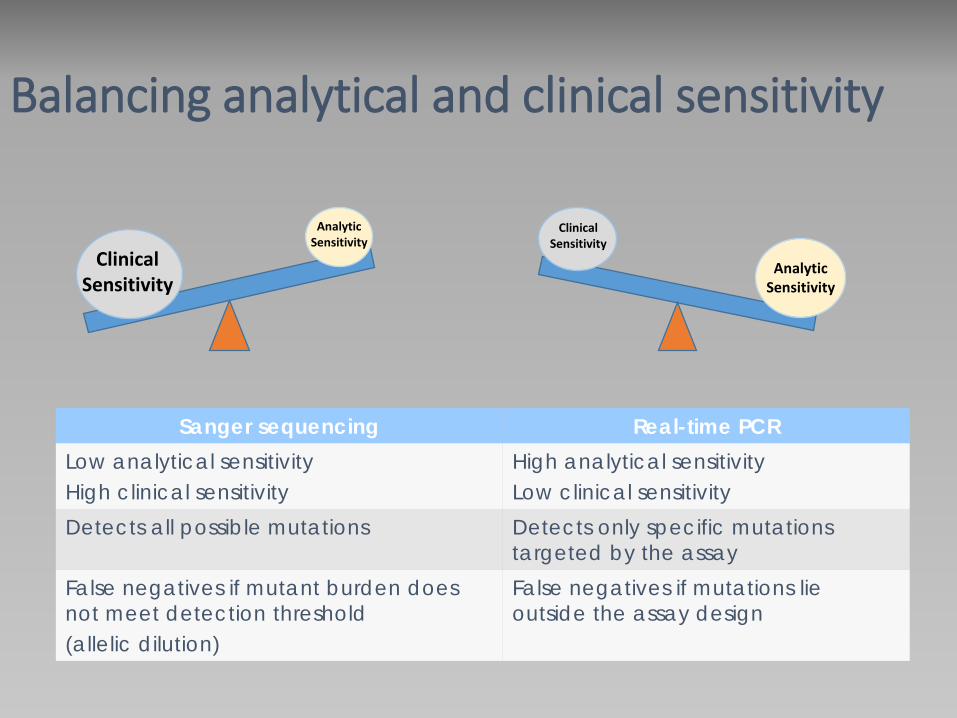
Balancing analytical and clinical sensitivity
Sanger sequencing Real-time PCR Low analytical sensitivity High clinical sensitivity
High analytical sensitivity Low clinical sensitivity
Detects all possible mutations Detects only specific mutations targeted by the assay
False negatives if mutant burden does not meet detection threshold (allelic dilution)
False negatives if mutations lie outside the assay design
Clinical Sensitivity
Analytic Sensitivity
Clinical Sensitivity
Analytic Sensitivity
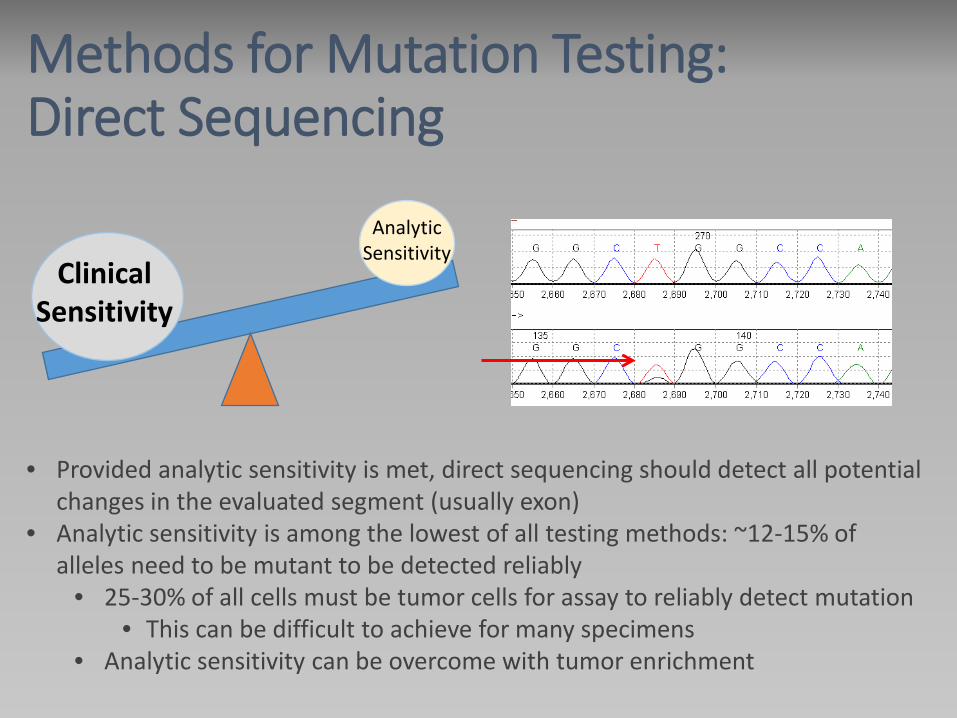
Methods for Mutation Testing: Direct Sequencing
Clinical Sensitivity
Analytic Sensitivity
• Provided analytic sensitivity is met, direct sequencing should detect all potential changes in the evaluated segment (usually exon)
• Analytic sensitivity is among the lowest of all testing methods: ~12-15% of alleles need to be mutant to be detected reliably
• 25-30% of all cells must be tumor cells for assay to reliably detect mutation • This can be difficult to achieve for many specimens
• Analytic sensitivity can be overcome with tumor enrichment
Example: Sanger sequencing Issue
• Pleural effusion with NSCLC • Testing for EGFR performed by Sanger sequencing is negative
• Possibility of false negative is high if the specimen had a low proportion of tumor cells

Methods for Mutation Testing: Real-Time PCR (and variations)
• FDA Approved tests predominantly use this approach • Can have a very high analytic sensitivity (~1-5% allelic)
• The mutations identified are strictly those which are part of the assay design • Individual probes for individual mutations • Thus, there is ultimately a limit on the number of mutations which can be
evaluated • Can require a large amount of nucleic acid
Clinical Sensitivity
Analytic Sensitivity
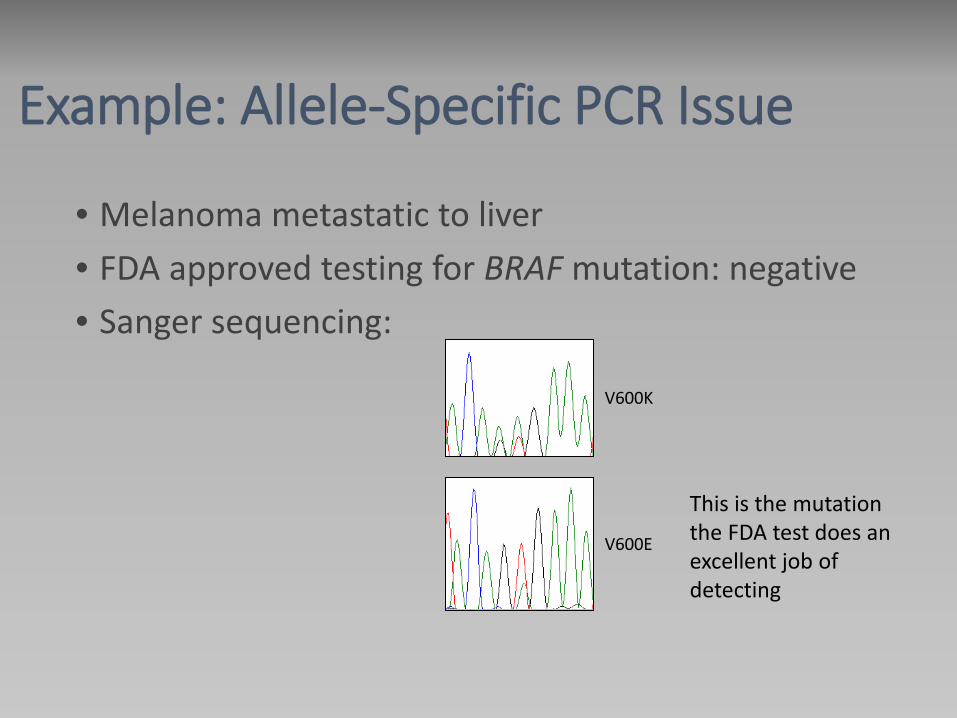
Example: Allele-Specific PCR Issue
• Melanoma metastatic to liver • FDA approved testing for BRAF mutation: negative • Sanger sequencing:
V600K
V600E
This is the mutation the FDA test does an excellent job of detecting
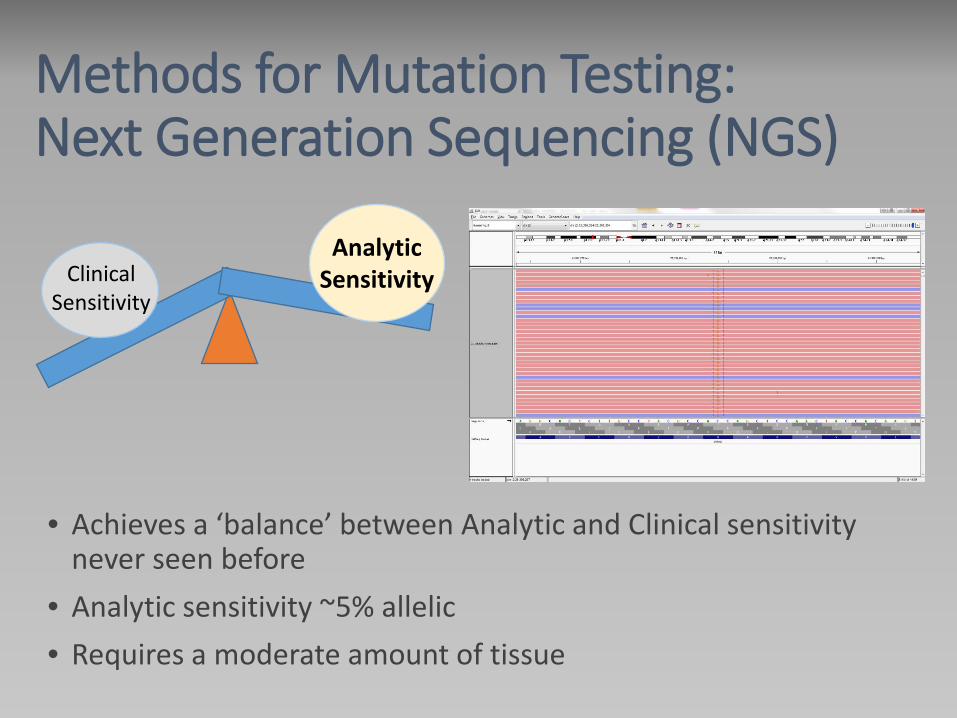
Methods for Mutation Testing: Next Generation Sequencing (NGS)
• Achieves a ‘balance’ between Analytic and Clinical sensitivity never seen before
• Analytic sensitivity ~5% allelic • Requires a moderate amount of tissue
Clinical Sensitivity
Analytic Sensitivity

Aisner DL and Sams SB. Diagn Cytopathol. 2012 Jun;40(6):511-24.
Common PCR-based methods for Molecular Testing
Key concepts in Molecular Diagnostics
•Extremely small specimens are not necessarily an obstacle. • The absolute number of tumor cells can be less important than the proportion of tumor in the sample. •The key element in a mutation assay hinges on being able to pick up a mutant allele present only in tumor cells from a background of wild type alleles present in all the non-tumor cells
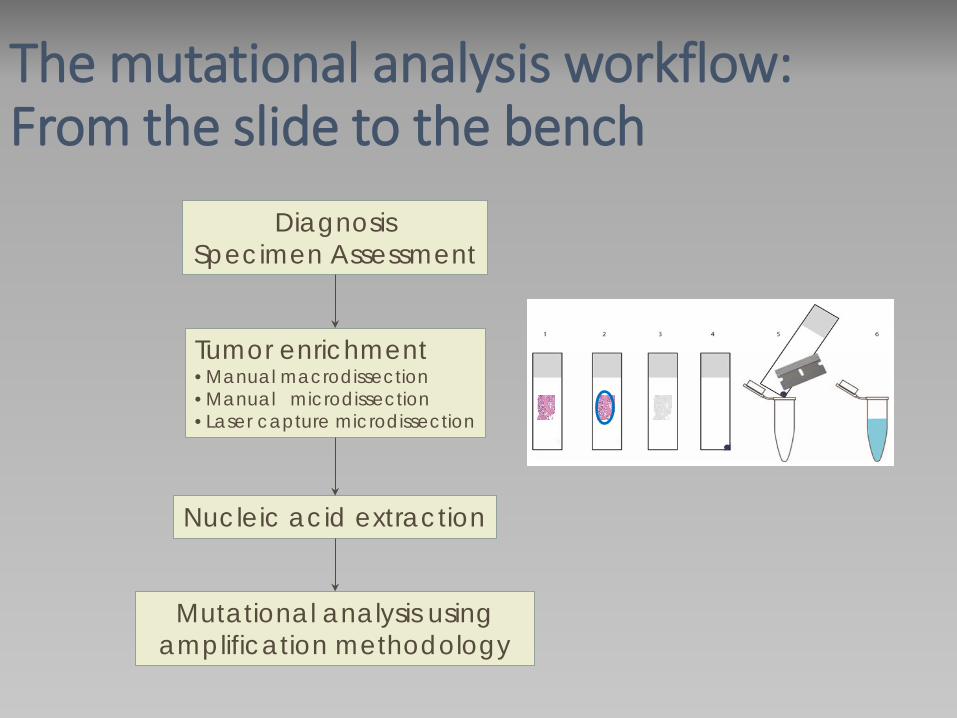
The mutational analysis workflow: From the slide to the bench
Diagnosis Specimen Assessment
Tumor enrichment •Manual macrodissection •Manual microdissection •Laser capture microdissection
Nucleic acid extraction
Mutational analysis using amplification methodology
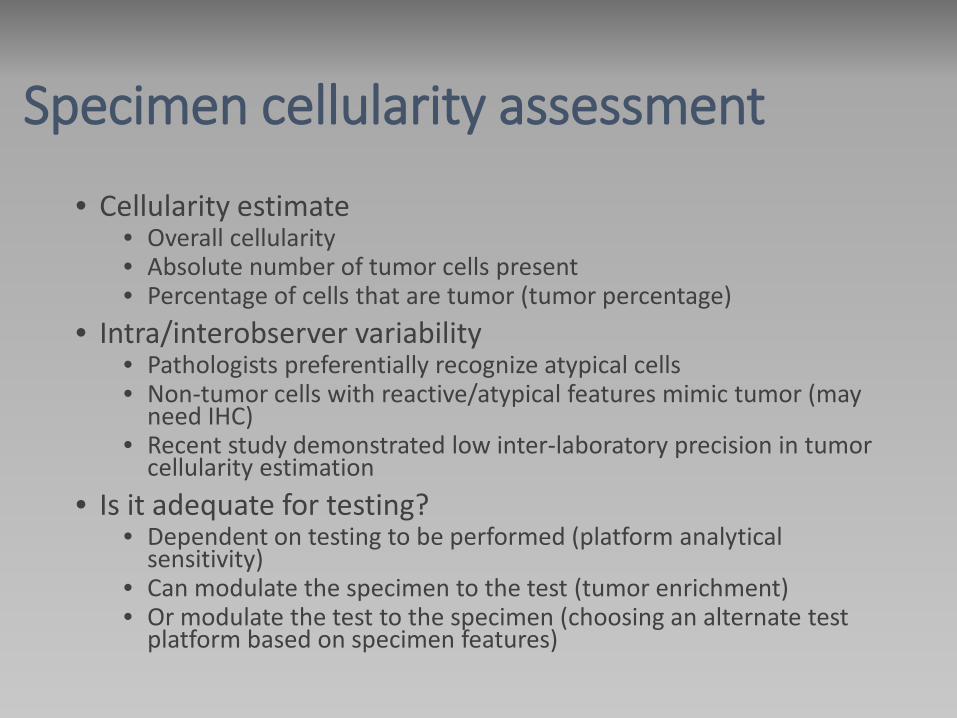
Specimen cellularity assessment
• Cellularity estimate • Overall cellularity • Absolute number of tumor cells present • Percentage of cells that are tumor (tumor percentage)
• Intra/interobserver variability • Pathologists preferentially recognize atypical cells • Non-tumor cells with reactive/atypical features mimic tumor (may
need IHC) • Recent study demonstrated low inter-laboratory precision in tumor
cellularity estimation • Is it adequate for testing?
• Dependent on testing to be performed (platform analytical sensitivity)
• Can modulate the specimen to the test (tumor enrichment) • Or modulate the test to the specimen (choosing an alternate test
platform based on specimen features)

Specimen cellularity assessment
Intra/interobserver variability
• Visual estimation of percentage of tumor cells by
the pathologist is a critical variable in testing
accuracy
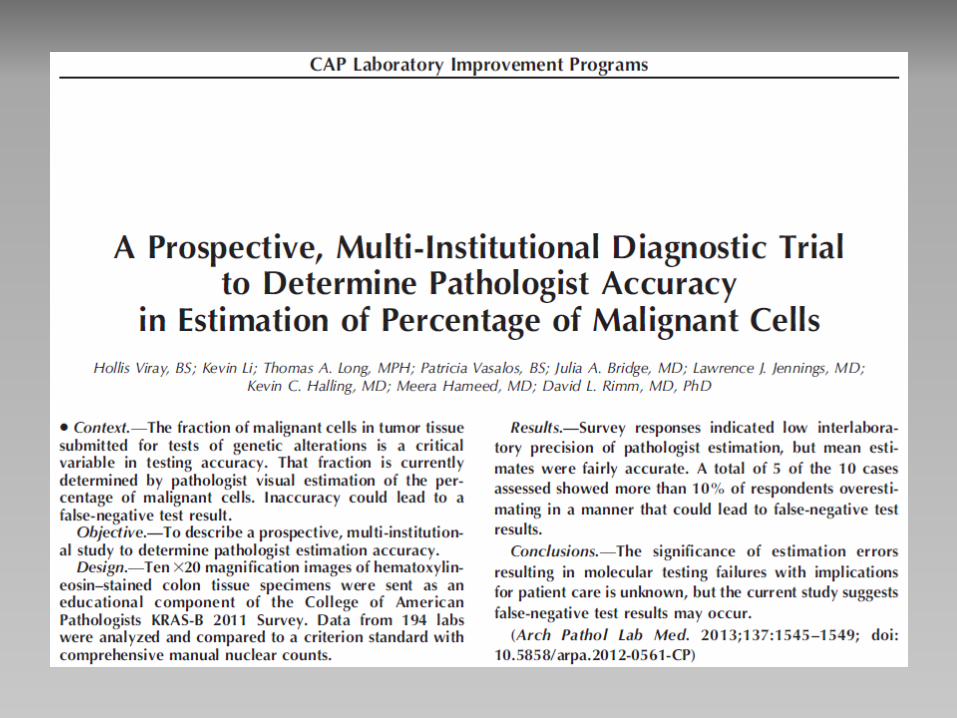

Viray H et al. Arch Pathol Lab Med. 2013 Nov;137(11):1545-9. doi: 10.5858/arpa.2012-0561-CP
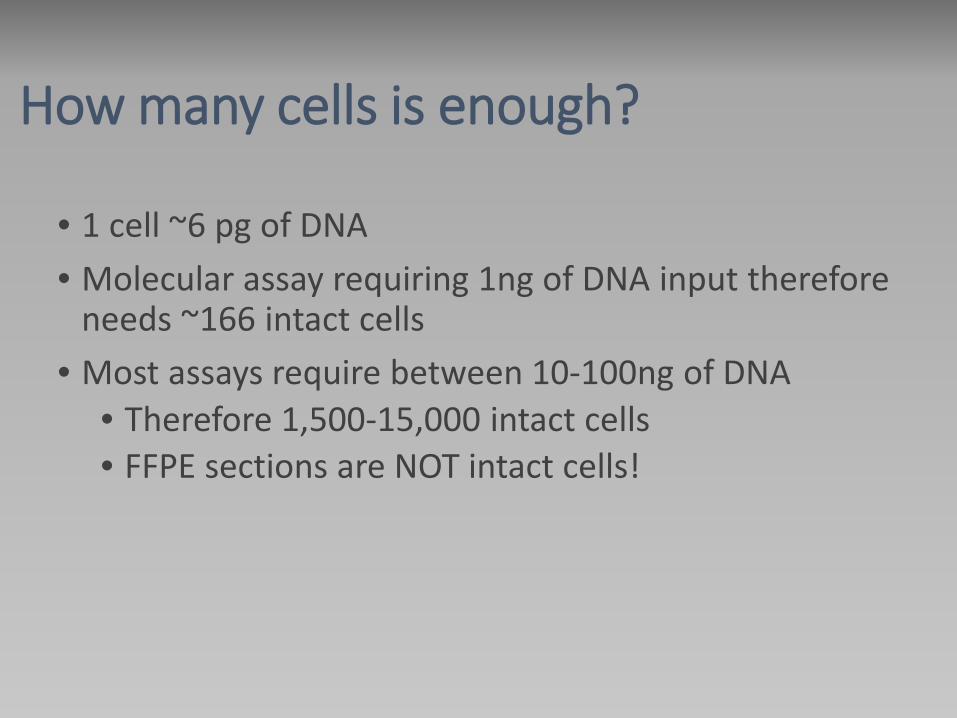
How many cells is enough?
• 1 cell ~6 pg of DNA • Molecular assay requiring 1ng of DNA input therefore
needs ~166 intact cells • Most assays require between 10-100ng of DNA
• Therefore 1,500-15,000 intact cells • FFPE sections are NOT intact cells!
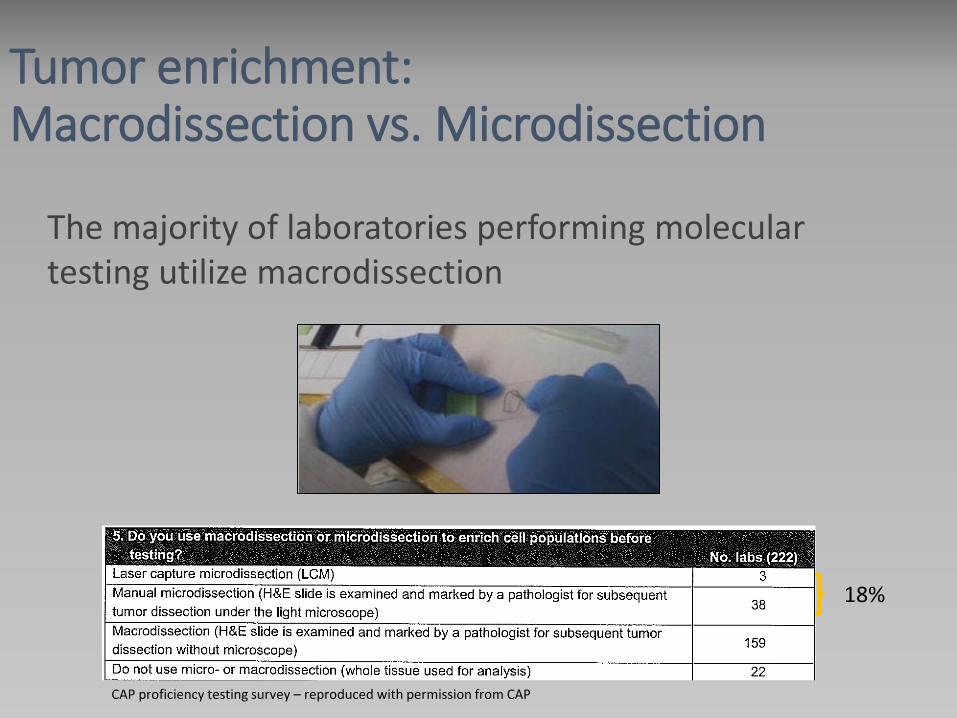
Tumor enrichment: Macrodissection vs. Microdissection
The majority of laboratories performing molecular testing utilize macrodissection
18%
CAP proficiency testing survey – reproduced with permission from CAP

Tumor enrichment: Microdissection
Tumor enrichment can be performed by manual/laser capture microdissection
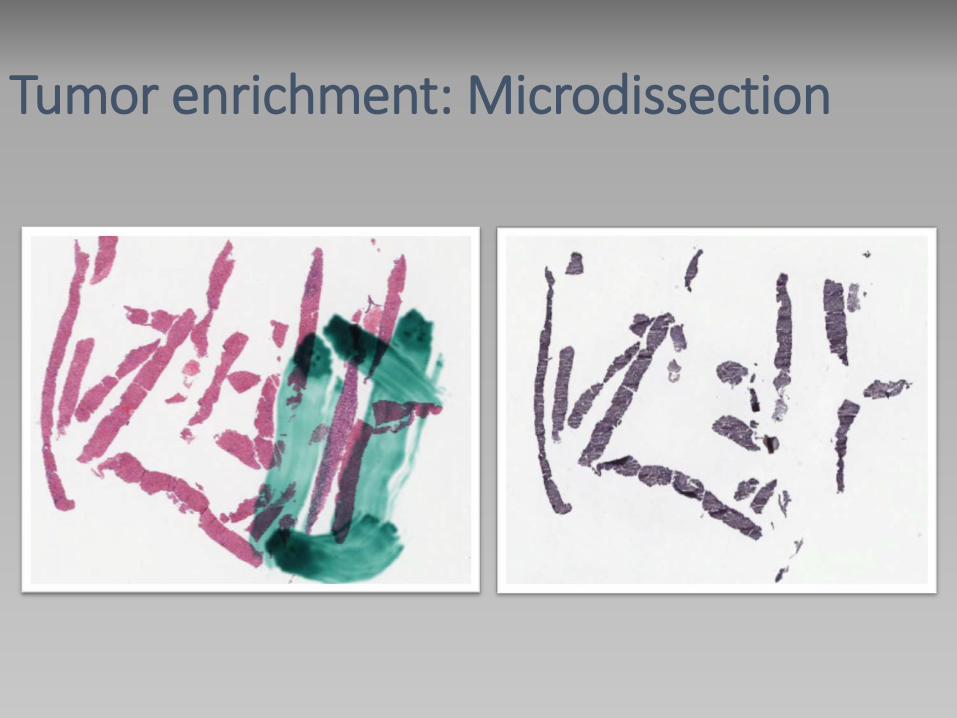
Tumor enrichment: Microdissection

Tumor enrichment: Microdissection

Microdissected x 30 levels
Tumor enrichment: Microdissection
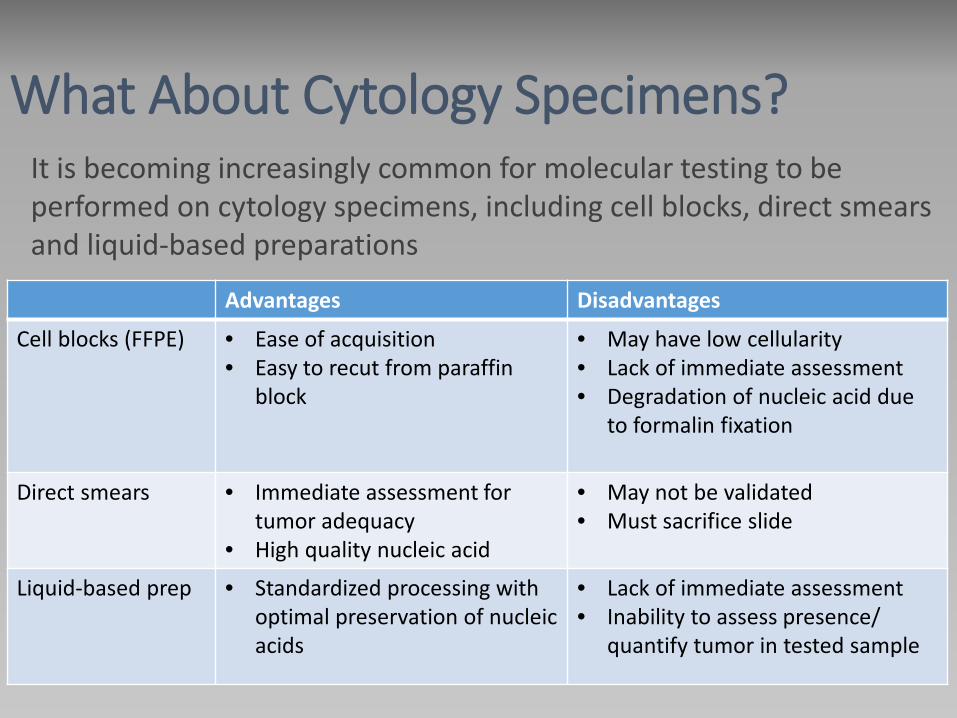
What About Cytology Specimens? It is becoming increasingly common for molecular testing to be performed on cytology specimens, including cell blocks, direct smears and liquid-based preparations
Advantages Disadvantages
Cell blocks (FFPE) • Ease of acquisition • Easy to recut from paraffin
block
• May have low cellularity • Lack of immediate assessment • Degradation of nucleic acid due
to formalin fixation
Direct smears • Immediate assessment for tumor adequacy
• High quality nucleic acid
• May not be validated • Must sacrifice slide
Liquid-based prep • Standardized processing with optimal preservation of nucleic acids
• Lack of immediate assessment • Inability to assess presence/
quantify tumor in tested sample
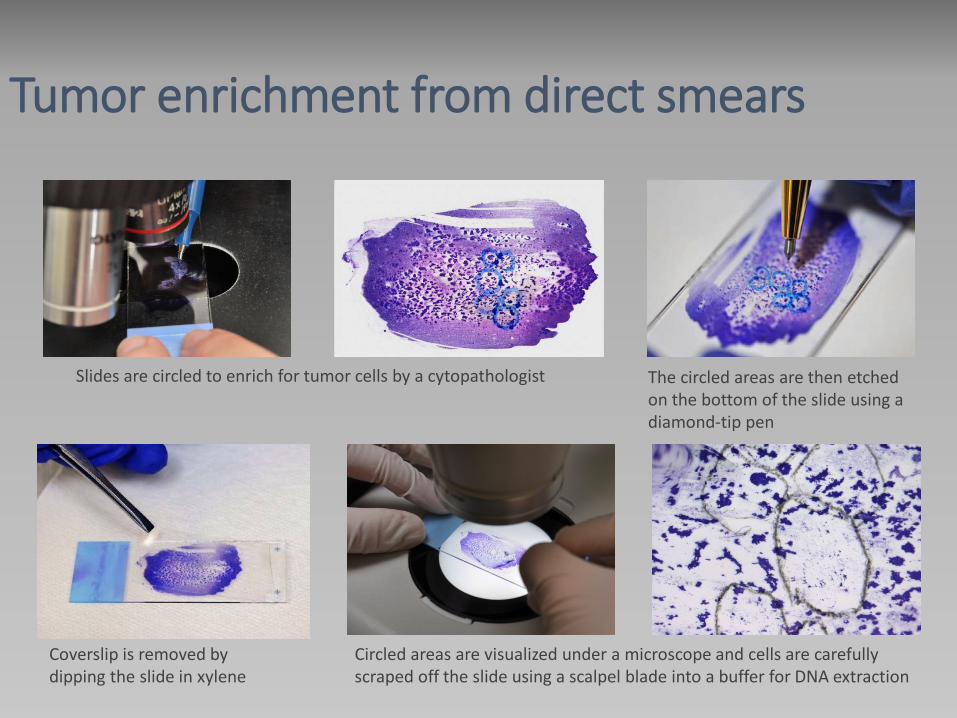
Tumor enrichment from direct smears
Slides are circled to enrich for tumor cells by a cytopathologist The circled areas are then etched on the bottom of the slide using a diamond-tip pen
Coverslip is removed by dipping the slide in xylene
Circled areas are visualized under a microscope and cells are carefully scraped off the slide using a scalpel blade into a buffer for DNA extraction

RLL US guided FNA Cell block with IHC performed Virtually no tumor cells remaining in cell block If no smear testing possible, patient will need re-biopsy, or no testing
Tumor enrichment from direct smears
Cancer Cytopathology 2013
Cancer Cytopathology 2013
2012
J Thorac Oncol 2014

Molecular testing: Preanalytic Aspects
Preanalytic aspects to consider include:
• specimen requirements
• specimen collection and handling
• criteria for rejection
Molecular testing: Key questions that pathologists need to consider
1. Know the test. Know the limitations.
- Understanding the key features of the molecular assay:
Analytical and clinical sensitivity
Whether microdissection is routinely utilized
Specimen types accepted by the lab for that specific test
2. Know your specimen.
- Which specimen do you pick: resection vs. biopsy vs. FNA?
- For cytology specimens: can you test from smears/ liquid based
preparations or do you need a cell block?
- For cytology on-site evaluations: do you need an extra pass for
a cell block or material for molecular? Do you need additional
sections for immunostains?
- During initial workup: do you request recuts up-front to avoid
having to reface the cell block?
Molecular testing: Key questions that pathologists need to consider
3. Know your clinical team.
- What tests are being requested? What does the oncologist
want? - Consider the specimen in the context of this – do they want testing on any
specimen for the patient or a specimen at a particular point in time?
- Reflex testing vs. clinician directed testing
- Choosing between send-outs vs. in-house tests, lab developed
tests vs. FDA approved tests.
Molecular testing: Key questions that pathologists need to consider
• Be the bridge between the clinical team and
the molecular lab
Molecular testing: Key role of the pathologist
Complications/constraints
• Pathology department is “custodian” of tissue • Legal requirements for minimal storage of slides and
block (differs by governing body)
• Small tissue size and risk of exhausting the block and/or sacrificing a smeared slide
• Prioritization for testing required • When using smears, may result in loss of slides from
archive • Must meet legal requirements (differs by state)
Summary • Targeted therapy has transformed the practice of oncology and pathology
• Mutational assay design is a balancing act between analytical and clinical sensitivity.
• The key element in a molecular assay hinges on being able to pick up a mutant allele present only in tumor cells from a background of wild type alleles present in all the non-tumor cells.
• Tumor enrichment techniques help improve tumor DNA content in a sample.
• Cytology specimens can be effectively utilized for molecular diagnostics.
• Understanding the specific specimen requirement criteria of your molecular lab may help triage cases for molecular testing more effectively.





























