Embed Size (px)
Citation preview

Practical Aspects of MRImaging Safety Test
Methods for MR ConditionalActive Implantable MedicalDevices Louai Al-Dayeh, MD, PhD*, Mizan Rahman, PhD, Ross Venook, PhDKEYWORDS
� AIMD � Implants � Medical devices � MR imaging safety � ISO/TS 10974
KEY POINTS
� MR Conditional implants undergo a wide range of well-developed test methods before receivingFDA approval under the specified conditions of use.
� MR imaging safety test methods for implants are empirical, measurement-based, or numericalmodeling-based.
� Conditions of use for MR Conditional devices include a combination of factors that are not easilyextrapolated.
INTRODUCTION
Because MR imaging, the unique nonionizing im-aging modality, uses three different types of elec-tromagnetic (EM) fields (static, gradient, andradiofrequency [RF]), a patient inside theMR scan-ner is prone to these fields’ interaction with thebody. Hence, MR safety standards, such asIEC60601-2-33,1 dictate limits on field exposurelevels and characteristics to reduce patient risksfrom hazards including RF burns, local andwhole-body heating, peripheral nerve stimulation,and cardiac stimulation, among others. Althoughthese risks are well-established, and MR imagingsystems have a strong history of safe use, thereare many reports of different types of adverseevents, including in the Food and Drug Administra-tion (FDA) Manufacturer and User Facility DeviceExperience database.2
All authors are employees of Boston Scientific NeuromoBoston Scientific Neuromodulation, 25155 Rye Canyon L* Corresponding author.E-mail address: [email protected]
Magn Reson Imaging Clin N Am 28 (2020) 559–571https://doi.org/10.1016/j.mric.2020.07.0081064-9689/20/� 2020 Elsevier Inc. All rights reserved. Downloaded for Anonymous User (n/a) at Washington University in Saint
November 18, 2020. For personal use only. No other uses witho
If the patient has an implantable medical device,there are added safety concerns for the patientbecause of the interactions of these fields withthe implant. These potential hazards, along withseveral unfortunate patient injuries related to inter-actions between MR scanners and implanted de-vices,3–8 historically led to appropriatelyconservative default consideration of implantabledevices as being contraindicated for MR imaging.In the mid-1990s, passive medical devices(without any internal power source), such asstents, began to get MR Conditional labelingfollowing guidelines and published safety stan-dards of ASTM International (formerly known asAmerican Society for Testing and Materials)9,10
and recommended MR imaging safety guidelinesper early publications on the subject.11,12 Becauseof the many different types of interactions, and po-tential patient harms, active implantable medical
dulation Corp.oop, Valencia, CA 91355, USA
mri.th
eclinics.com
Louis Bernard Becker Medical Library from ClinicalKey.com by Elsevier onut permission. Copyright ©2020. Elsevier Inc. All rights reserved.

Al-Dayeh et al560
Dow
devices (AIMDs; those relying for its functioning ona source of electrical energy or any source of po-wer other than that directly generated by the hu-man body or gravity13) continued to becontraindicated at most sites.Since the first successful MR imaging safety la-
beling of an implanted Deep Brain Stimulation(DBS) system by Medtronic (Minneapolis, MN)approximately 20 years ago, with significant limita-tions on applied fields, AIMD manufacturers havecome a long way in designing their implants withMR safety in mind and in assessing what condi-tions of MR scanning (eg, limits of RF and/orgradient) can allow MR imaging without compro-mising patient safety. The first successful FDA la-beling of an MR Conditional pacemaker byMedtronic in 201114 marked the beginning of therecent era in which many more patients withimplanted devices from manufacturers acrossthe industry now have access to MR imagingthrough MR Conditional labeling.What facilitated getting to the current state of
MR Conditional devices today is a joint effort thatstarted in 2006 across the MR imaging safetycommunity, including representatives fromimplanted device manufacturers, scanner manu-facturers, and regulatory bodies. Experts in eacharea formed a joint working group that participatedin various technical venues helping to shape andupdate multiple standards. A major outcome ofthis effort was publication of an international tech-nical specification (TS), ISO/TS 10974, document-ing guidelines on the assessment of MR imagingsafety for patients with an AIMD. The first versionof this TS published in 2012,15 and the secondupdated version published in 2018.16 The work isongoing, and the group is updating and transition-ing the TS into an international standard, with ex-pected publication in 2021 or 2022.To have a specific focus, this article mainly ad-
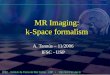
dresses AIMDs with extended leads (eg, cardiacleads or neuromodulation leads), that is, animplanted pulse generator (IPG) plus one or moreleads (see Fig. 1 for a representative spinal cordstimulator).
RELEVANT FACTS TO COUNTERMISCONCEPTIONS ABOUT MR IMAGINGSAFETY TESTING OF ACTIVE IMPLANTABLEMEDICAL DEVICES
� There are many types of potential patient haz-ards, which require comprehensive testing. Itis not simply about magnetic materials or RFburns.
� Most implants that allow MR imaging scan-ning are MR Conditional; there is practically
nloaded for Anonymous User (n/a) at Washington University in Saint Louis Ber November 18, 2020. For personal use only. No other uses without permis
no “MR Safe” active implant. In general, ifthe implant has metallic components, it iseither MR Conditional or MR Unsafe.
� What is MR Conditional is a specific device/system (specific pulse generator 1 specificlead) per the device’s formal MR imagingsafety label conditions listed in its instructionsfor use/manual.� No generalizations of MR safety can bemade about any other device/system fromthe same manufacturer or other manufac-turers (eg, lead extensions that are notincluded in the MR label, and not MRConditional).
� Mixing and matching a pulse generator froman MR Conditional device/system with leadsfrom another MR Conditional device/systemdoes not make the new combination MR Con-ditional. There is typically no testing or dataavailable to assess such combinations.
� Fractured leads, abandoned leads, and otherdamaged or nonfunctional implants are typi-cally not assessed for safety, and their levelof risk is unknown.
� There are no strong guidelines on how tosafely scan a patient with multiple AIMDs(eg, a pacemaker and a spinal cord stimu-lator). Even if each system is MR Conditionalby itself, the multisystem combination is notin general labeled for MR Conditional safety,because of the lack of testing on suchcombinations.
� Almost all present safety testing and MR Con-ditional labeling of implants is for either 1.5-Tor 3-T cylindrical bore MR imaging scanners(or both). Open-bore systems, and higher- orlower-field scanners, typically are notincluded in testing standards or in MR Condi-tional labels.
� If an MR Conditional device/system is deemedsafe in a specific MR field strength (eg, 1.5 T),this has no implication on MR safety of the de-vice within other field strengths (eg, lower B0,such as 1 T, or higher B0, such as 3 T or 7 T).No presumption of safety can be made at anyfield strength other than the one at which thesafety assessment was done, because theRF-dependent propertiesof the systemchangesignificantly (eg, RF wavelength, current depo-sition on leads, exposure fields in the patientcaused by scanner design differences) andcould be either more safe or less safe.
� In general, accessories of devices/systems(eg, remote control, charger) are not MR Con-ditional, and many are MR Unsafe and cannotbe brought into Zone 4 (the MR imaging scan-ner room) of the imaging facility.
nard Becker Medical Library from ClinicalKey.com by Elsevier onsion. Copyright ©2020. Elsevier Inc. All rights reserved.

Fig. 1. Illustration of a generic spinalcord stimulator system as an exampleof AIMD with extended leads. Variouspotential MR imaging hazards arelisted (with reference in parenthesesto the causing fields). B0, static field;GRD, time-varying gradient field.Note that understanding the inducedfields for an AIMD for RF and time-varying gradients includes surgicalimplantation variables, such as leadsubcutaneous routing and coiling ofthe lead in the IPG pocket.
Practical Aspects of MR Imaging Safety Test Methods 561
MR IMAGING AND ACTIVE IMPLANTABLEMEDICAL DEVICES INTERACTIONS:POTENTIAL SAFETY HAZARDS (PER ISO/TS10974)
Demonstration of MR Conditional status byimplantable device manufacturers (eg, to achieveFDA labeling) involves testing hundreds or thou-sands of different exposure conditions andmodeling many thousands or millions of such po-tential exposure conditions. This includes expo-sure in realistic MR imaging scanningenvironments, benchtop injection testing, anddevelopment of appropriate risk assessmentsthough physical experiments and modeling. Thequick methods used by some researchers of tryingto assess device safety through testing of a hand-ful of configurations of a device within a box of tis-sue simulating medium (which was common inpast decades, and still finds its way into the litera-ture) is simply insufficient. Although it is a helpfulfirst step, or potentially useful in demonstratinghazards, it unfortunately does not meaningfullyevaluate safety. This section of the article de-scribes the full range of proper test methods, perestablished standards, that collectively form thetesting package regulatory bodies review for agiven MR Conditional device label.
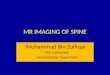
Per ISO/TS 10974:201816 the potential safetyhazards caused by the MR imaging scanner andAIMD interaction physics are listed in Table 1.Fig. 2 also illustrates these hazards. Each of thethree different types of EM fields in a scanner(B0, time-varying gradient, and RF) generate spe-cific interactions and potential safety hazards forpatients, as do the different combinations of fields(eg, device vibration is a result of the combinationof B0 1 time-varying gradient fields).
Most test methods described in various stan-dards do not include explicit acceptance criteria
Downloaded for Anonymous User (n/a) at Washington University in Saint November 18, 2020. For personal use only. No other uses witho
(eg, how many degrees centigrade of temperaturerise is acceptable for electrode heating) becausethe standards must work for many different typesof implants. Because the risk level depends onthe nature and location of the implant, and tissuessurrounding it, each implant manufacturer mustset and justify acceptance criteria for each poten-tial hazard according to their internal risk manage-ment procedures, subject to review by regulatoryauthorities. Typically, this includes using internalcompany data from a combination of relevant his-tory of safe use, human trials, or animal studies,and accepted literature references. Implant manu-facturers are also working on creating verticalstandards for a specific type of implants with rele-vant acceptance criteria for these hazards.
Table 2 includes a more detailed view on oneway an AIMD manufacturer might consider andaddress the wide variety of potential safety haz-ards and acceptance criteria.
TEST METHODS ADDRESSING POTENTIALSAFETY HAZARDS CAUSED BY MR IMAGINGAND ACTIVE IMPLANTABLE MEDICALDEVICES INTERACTION: PULSE GENERATORD LEADS
Evaluation of the AIMD for MR imaging hazards in-volves benchtop testing, modeling, MR scanners,or a combination of these approaches. One wayto categorize these evaluations is whethermodeling is a part of the assessment or not(Table 3).
B0-Induced Force
A displacement force produced by the static mag-netic field (B0) on a device containing magneticmaterials has the potential to cause unwantedmovement of the implanted device.
Louis Bernard Becker Medical Library from ClinicalKey.com by Elsevier onut permission. Copyright ©2020. Elsevier Inc. All rights reserved.

Table 1Potential patient hazards and corresponding test methods
Hazard Test Method Clause
Heat RF field-induced heating of the AIMD 8Gradient field-induced device heating 9
Vibration Gradient field-induced vibration 10
Force B0-induced force 11
Torque B0-induced torque 12
Unintended stimulation Gradient field-induced lead voltage (extrinsic electric potential) 13RF field-induced rectified lead voltage
Malfunction B0 field-induced device malfunction 14RF field-induced device malfunction 15Gradient field-induced device malfunction 16Combined fields test 17
Each clause of the test method document defines the specific conditions for the testing to ensure proper coverage in theMR imaging environment.
From ISO/TS 10974:2018. Assessment of the safety of magnetic resonance imaging for patients with an active implant-able medical device; with permission.
Al-Dayeh et al562
Dow
Force exerted on the device is a function of thespatial gradient of B0 (or the product of B0 and thespatial gradient of B0, depending on whether thematerials are greater or less than magnetic satura-tion) and the mass of magnetic material. Thisestablished test method is described in ASTMF2052,17 is measurement-based, and is typicallyconducted in a scanner.The concept of testing is to measure the
magnetically induced displacement force of theimplant where the spatial gradient is greatest(near the opening of the bore) and compareagainst the gravitational force acting on the device(because all implanted devices are subjected tothe force caused by gravity without patientharm). One version of this test is to suspend the
nloaded for Anonymous User (n/a) at Washington University in Saint Louis B November 18, 2020. For personal use only. No other uses without perm
device by a thin string at that location andmeasurethe deflection angle; if it deflects less than 45�, itsmagnetic force is less than that of gravity.Implants with a displacement force less than the
force of gravity are automatically deemed accept-able. If that force is greater, it still could be accept-able with appropriate justification of anappropriate acceptance criterion to maintain pa-tient safety.For most AIMDs with extended leads, with the
main magnetic components implanted subcutane-ously and far from vulnerable structures, B0-induced force is not considered a high-risk hazard.There is real potential for concern if the device is ina sensitive physiologic location (eg, brain aneu-rysm clip).
Fig. 2. Relationship between MR im-aging scanner output fields RF,gradient (G), static (B0), and hazards(ISO/TS 10974 test method clausenumbers in parentheses). (From ISO/TS 10974:2018. Assessment of thesafety of magnetic resonance imag-ing for patients with an activeimplantable medical device; withpermission.)
ernard Becker Medical Library from ClinicalKey.com by Elsevier onission. Copyright ©2020. Elsevier Inc. All rights reserved.

Table 2Example list of MR imaging–AIMD safety hazards, each of which generates requirements that an AIMD manufacturer must assess with appropriate testmethods and rationale
Requirement10,974Clause Details of Meeting Requirement Rationale/Source
RF-induced lead heating patient harm limit 8 When exposed to RF fields, heating of thelead shall not exceed XX CEM 43�C21
ISO/TS 10974Tissues around lead heating acceptance
criteriaMR imaging environment exposure durations,
levels
Device (IPG) heating patient harm limit:Gradient-inducedRF-induced
89
When exposed to combined RF and gradientfields, the thermal exposure of tissuesurrounding the pocket shall not exceed XXCEM 43�C
ISO/TS 10974Tissues around stimulator heating acceptance
criteriaMR imaging environment exposure durations,
levelsMR imaging EMC acceptance criterion
Gradient-induced vibration patient harm limit 10 When exposed to combined static andgradient fields, the pressure exerted byimplanted IPG or leads on the tissue shallnot exceed XX psi
ISO/TS 10974MR imaging vibration tissue damage
acceptance criteriaMR imaging environment exposure durations,
levels
B0-induced force patient harm limit 11 When exposed to static field:Translational force on the IPG shall notexceed XX N
Translational force on any implantablesystem components shall not exceed theweight of the component
ASTM F2052MR imaging force torque acceptance criterionMR imaging environment exposure durations,
levels
B0-induced torque patient harm limit 12 When exposed to static field:Torque on the IPG shall not exceed XX NmTorque on all implanted systemcomponents shall not exceed the weighttimes the length of the longest side of thecomponent
ASTM F2213MR imaging force torque acceptance criterionMR imaging environment exposure durations,
levels
(continued on next page)
Practica
lAspects
ofMRIm
agingSa
fety
Test
Methods
563
Dow
nloaded for Anonym
ous User (n/a) at W
ashington University in Saint L
ouis Bernard B
ecker Medical L
ibrary from C
linicalKey.com
by Elsevier on
Novem
ber 18, 2020. For personal use only. No other uses w
ithout permission. C
opyright ©2020. E
lsevier Inc. All rights reserved.

Table 2(continued )
Requirement10,974Clause Details of Meeting Requirement Rationale/Source
Electric potential patient harm limitGradient-induced, extrinsicRF-induced and RF rectification
1315
When exposed to combined RF and gradientfields:The current conducted by the IPG shall notexceed a pulse charge limit of XX mC ineach electrode
Amplitude of the current pulse shall notexceed XX mA in IPG stimulation-offcondition
Amplitude of the current pulse shall bewithin specified tolerances in IPGstimulation-on condition
ISO/TS 10974MR imaging environment exposure durations,levels
RF-induced device malfunction limit 15 When exposed to RF field, the IPG shall passEMC criteria during and following exposure
ISO/TS 10974MR imaging environment exposure durations,levels
MR imaging EMC acceptance criterion
B0-induced device malfunction limit 14 When exposed to static field, the IPG shallpass EMC criteria during and followingexposure
ISO/TS 10974MR imaging environment exposure durations,levels
MR imaging EMC acceptance criterion
Gradient-induced device malfunction limit 16 When exposed to gradient field, the IPG shallpass EMC criteria during and followingexposure
ISO/TS 10974MR imaging environment exposure durations,levels
MR imaging EMC acceptance criterion
Combined fields, induced device malfunctionlimit
17 When exposed to combined static, RF andgradient fields, the IPG shall:Pass EMC criteria during and followingexposure
Retain its complete functionality duringand following exposure
ISO/TS 10974MR imaging environment exposure durations,levels
MR imaging EMC acceptance criterion
Combined fields, image artifacts or distortion Image artifacts caused by the presence ofIPG 1 leads shall be evaluated per ASTMF2219
ASTM F211922
Abbreviations: CEM 43�C, cumulative number of equivalent minutes at 43�C temperature; EMC, electromagnetic compatibility; N, Newton (force unit); Nm, N m (torque unit); mC,micro Coulomb (charge unit).
Al-D
aye
hetal
564
Dow
nloaded for Anonym
ous User (n/a) at W
ashington University in Saint L
ouis Bernard B
ecker Medical L
ibrary from C
linicalKey.com
by Elsevier on
Novem
ber 18, 2020. For personal use only. No other uses w
ithout permission. C
opyright ©2020. E
lsevier Inc. All rights reserved.

Table 3Categorization of MR imaging safety assessments, based onwhether or not electromagnetic modelingis involved
Six MR Imaging Safety Assessments Rely onBenchtop Testing and/or MR Imaging ScannersWithout Modeling
Three MR Imaging Safety Assessments RelyHeavily on Modeling (in Addition toMeasurement-Based Testing)
1. B0-induced force2. B0-induced torque3. Gradient field-induced vibration4. Gradient field-induced device (IPG) heating5. Device (IPG) malfunction (B0 field and/or RF
field and/or gradient field-induced)6. Combined fields test
7. RF field-induced heating of the AIMD8. Unintended stimulation from RF field-induced
lead voltage9. Unintended stimulation from gradient field-
induced lead voltage (extrinsic electricpotential)
Practical Aspects of MR Imaging Safety Test Methods 565
B0-Induced Torque
Magnetically induced torque, produced by thestatic magnetic field (B0), has the potential tocause unwanted movement of a device containingmagnetic materials (rotating the implant to align itwith the B0 field).
Torque is sensitive to B0 and should bemeasured at a location where the static magneticfield is homogeneous (eg, the isocenter of an MRscanner). This established test method isdescribed in ASTM F2213,18 is measurement-based, and is typically conducted in a scanner.
Experimental approaches to conducting torquetesting vary in complexity and applicability.Some methodologies are only applicable to de-vices that experience little to no torque, whereasothers are appropriate for devices that experiencesignificant torque and must be more rigorouslyquantified to assess safety.
Most implantable devices, including AIMDs withextended leads, experience measurable torquebut have no trouble passing a reasonable accep-tance criterion. There is real potential for concernif the device is in a sensitive physiologic location(eg, brain aneurysm clip).
Gradient Field-Induced Vibration
Time-varying gradient magnetic fields from an MRscanner induce eddy currents on the conductivesurfaces of an AIMD. These eddy currents pro-duce a time-varying magnetic moment that inter-acts with the static magnetic field (B0) causingvibration of the conductive surfaces and, subse-quently, the device. The primary potential for pa-tient harm, because the vibration of the device istypically very low-amplitude because of the highfrequency of oscillation, arises from possiblebreakage of internal components that lead to mal-function of the device, which could result in
Downloaded for Anonymous User (n/a) at Washington University in Saint November 18, 2020. For personal use only. No other uses witho
compromised functionality or lack of therapyfrom the device.
Vibration is sensitive to B0 and gradient dB/dt.This test is described in ISO/TS 10974:2018,16 ismeasurement-based, and is conducted in a scan-ner or using a shaker table.
There are two methods for testing. One methodrequires the use of an MR scanner and provideshigher accuracy with an increase in test burden,whereas the other method uses a shaker tableand uses conservative approximations to reducetest burden after initial calibration testing in anMR scanner. Because most conceived failuresare caused by fatigue fractures of internal compo-nents, the concept of testing is to expose theimplant to extended periods of vibration andconfirm full device functionality afterward.
Test duration represents the cumulative patientscan time over the lifetime of a typical AIMD.Guidelines in the standard establish, based onprior clinical experience, that conservative totalMR imaging scan time exposure ranges from2.5 hours to 7.5 hours, if looking at the top 0.8%of the population to the top 0.01% of the popula-tion, respectively.
For medium- or small-sized IPGs, and non-life-sustaining devices, vibration is not considered ahigh-risk hazard. Larger devices typically vibratemore, with potentially greater likelihood of devicedamage.
Gradient Field-Induced Device (ImplantedPulse Generator) Heating
The time-varying gradient dB/dt fields during MRimaging sequences induce eddy currents onconductive AIMD enclosures and other conductiveinternal surfaces, such as battery components andcircuit ground planes, and can result in deviceheating.
IPG heating is sensitive to average or root-meansquare (RMS) gradient field amplitude jdB/dtj, with
Louis Bernard Becker Medical Library from ClinicalKey.com by Elsevier onut permission. Copyright ©2020. Elsevier Inc. All rights reserved.

Al-Dayeh et al566
Dow
secondary dependence on the gradient waveformcharacteristics (shape and frequency). It is great-est when the device is located where the gradientfield jdB/dtj RMS is maximum and when the de-vice is oriented so that the gradient field vector isorthogonal to the AIMD surfaces with the largestconductive area. This heating also scales stronglywith device radius (larger devices heat more).This test is described in ISO/TS 10974:2018.16 It
is measurement-based, with preferential use of alaboratory gradient coil, amplifier, and functiongenerator that can simulate clinical gradient fieldexposure. Alternatively, testing may be conductedusing a clinical MR scanner.Testing may be conducted using one of two tiers
for the gradient waveform shape. Tier 1 uses aconservative waveform shape, and tier 2 allowsthe characterization and use of a clinically relevantwaveform. Tier 2 is most useful for AIMDs withlarger conductive surfaces.The standard calls for a test duration that is the
maximum allowed scan duration as specified bythe AIMD MR Conditional labeling, or 30 minutes.All other testing parameters are determined bythe AIMD manufacturer to reflect conservativeclinical use conditions for their device.The key concern is local tissue heating because
of radiant heat from the IPG. For most AIMDs withextended leads, this is not considered a high-riskhazard, although some MR Conditional labelshave suggested using an ice pack near a subcu-taneous device if the patient reports local heatingsensations near the device (IPG).
Device (Implanted Pulse Generator)Malfunction (B0 Field and/or RadiofrequencyField and/or Gradient Field-Induced)
Exposure to the scanner’s B0 field and/or RF fieldand/or gradient field could have certain effects onan AIMD, such as but not limited to:
� B0: Device reset, reprogramming, magneticremanence, battery drain, and permanentdamage.
� B1: Failure to deliver the intended therapy, re-programming, device reset, permanent dam-age, and tissue stimulation caused by RFrectification.
� Gradient: Failure to deliver intended therapy,memory corruption, or temporary or perma-nent loss of device programmed settings.
These effects are transient or permanent andmight create a safety hazard that impacts theAIMD patient. Malfunction also has different impli-cations per the patient’s dependence on the
nloaded for Anonymous User (n/a) at Washington University in Saint Louis B November 18, 2020. For personal use only. No other uses without perm
device (eg, whether it is a life-sustaining therapy,such as a pacemaker, or not).The assessment is sensitive to a function of B0,
peak B1, and peak dB/dt.Three tests (one per MR field) are described in
ISO/TS 10974:201816 in elaborate details,including specifying a mixture of radiated andbenchtop tests.
� For B0: Implants are divided into three classeswith various testing complexities. For manyAIMDs with IPG 1 lead, it is sufficient for theirclass to meet the test requirement with nospecific B0 susceptibility orientationsrequired, and for those, monitoring is done inaccordance with a combined field testrequirement (eg, the test is done in scanner,with all three fields active).
� For B1 and gradient: The field level andinduced voltages are found via a combinationof computational modeling (see the later sec-tion on modeling) and exposure testing. Chal-lenge testing of the device circuitry formalfunction includes benchtop injectedvoltage tests using sources of waveformswith appropriate shapes and magnitudesthat reflect MR-relevant sequences.
The IPG should pass the acceptance criterionestablished by the device manufacturer based onthe intended functionality (ie, confirm expecteddevice functionality) after the implant is exposedto each one of the three fields as describedpreviously.
Combined Fields Test
The combined fields test provides field exposurestypically encountered in clinical MR imaging ex-aminations. It establishes an in vitro evaluation ofthe AIMD functioning under simultaneous expo-sure to the static, gradient, and RF magnetic fieldconditions. Unlike the maximal exposures requiredin the rest of measurement-based tests, this testexposes the AIMD to representative levels andtemporal patterns of all three MR magnetic fieldssimultaneously.This measurement-based assessment is con-
ducted in a scanner and is sensitive to (a functionof) B0, RF peak, and dB/dt Peak. The test isdescribed in ISO/TS 10974:2018.16
The combined fields test is performed using anAIMD (the IPG and the connected leads) posi-tioned in a tissue-simulating media phantom andplaced inside an MR scanner. The AIMD isexposed to a series of MR imaging sequences(representing various common and clinically rele-vant protocols) performed at different landmarks
ernard Becker Medical Library from ClinicalKey.com by Elsevier onission. Copyright ©2020. Elsevier Inc. All rights reserved.

Practical Aspects of MR Imaging Safety Test Methods 567
or simulated patient positions within the bore. Theconcept of testing is to expose the implant to theclinical combined fields and confirm expected de-vice functionality during and after the exposure.
This test is viewed as redundant to device (IPG)malfunction testing. However, it is required tomake sure the device is actually tested in radiatedenvironment under clinical conditions. In addition,benchtop exposure tests are typically more strin-gent, because they can apply higher-than-expected injection levels.
MR IMAGING SAFETY ASSESSMENTS WITHELECTROMAGNETIC MODELING
ISO/TS 10974:201816 has tiered approaches tomodeling where the low tier is easily implement-able but overestimates the needed assessment,and modeling in higher tiers is more complex butmore accurate (with less overestimation). Practi-cally, for AIMDs with extended leads, tier 3 is thehighest tier that is attainable with acceptableaccuracy.
Tier 3 includes modeling the EM environmentsurrounding the AIMD to obtain the incident elec-tric fields potentially picked up by the AIMD,together with measurements of how the AIMDhandles such incident fields.
The process includes running a computer simu-lation: using a hardware model of the scanner coilitself, whether an RF birdcage coil or a gradientcoil, and anatomic models of humans as represen-tative samples per the device’s patient character-istics. EM simulations (RF or gradient) are runusing these models in all relevant clinical land-marks or patient positions to mimic the EM envi-ronment of the scanner. Modern simulations,across a range of human body models, and witha range of MR imaging scanner coil models, cangive the EM field distribution everywhere insidethe anatomic models across a range of potentialMR examination circumstances.
Downloaded for Anonymous User (n/a) at Washington University in Saint November 18, 2020. For personal use only. No other uses witho
The First Element Needed for Modeling,Tangential Electric Fields
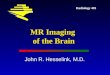
For the three assessments that rely heavily onmodeling (see Table 3), tier 3 modeling requiresthat, along the lead path in every anatomic model,the tangential vector of the electrical component(E-tan) of the incident fields be extracted fromthe EM simulation. Fig. 3 shows the E-tan magni-tude of example DBS and Spinal Cord Stimulation(SCS) routings, for a specific landmark in an MRscanner with an RF body coil.
The Second Element Needed for Modeling,the Transfer Function
For RF (the first two of the three assessments inTable 3) the transfer function19 is needed, whichis really a characterization of how a particularAIMD (ie, a specific IPG 1 lead combination) be-haves as an RF Antenna in the scannerenvironment.
For safety purposes benefiting the patient, wewant the AIMD to be a bad antenna in the EM envi-ronment of the MR imaging scanner. The transferfunction of an AIMD (when exposed to a uniformE-tan excitation) is measured in benchtop RFinjected setup (Fig. 4) or simulated. The transferfunction is a 1D vector (having the length of thelead under test) of complex values (term S in Equa-tions 1 and 2) whose magnitude shows the reso-nance lengths of the AIMD (see Fig. 5), which isthe frequencies at which the AIMD is a goodantenna.
Discussed next are the three MR safety assess-ments that rely on modeling.
Radiofrequency Field-Induced Heating of theActive Implantable Medical Device (LeadElectrode Heating)
Patient harm caused by RF-induced lead elec-trode heating is a function of absolute tempera-ture, duration of the temperature, and individual
Fig. 3. (Left) Human model with twoDBS and two SCS lead routings (path-ways). (Upper Right) RF E-tan magni-tude of one DBS routing. (LowerRight) RF E-tan magnitude of oneSCS routing.
Louis Bernard Becker Medical Library from ClinicalKey.com by Elsevier onut permission. Copyright ©2020. Elsevier Inc. All rights reserved.

Fig. 4. The transfer function bench-top RF injected setup: Vector NetworkAnalyzer (1), RF source (2), senseinput (3), transmitting antenna (4),localized E-tan (z) (5), coaxial antenna(6), tip electrode (7), the AIMD(lead 1 IPG) (8), and tissue simulatingphantom (9). (From ISO TIR21900:2018. Guidance for uncertaintyanalysis regarding the application ofISO/TS 10974; with permission.)
Al-Dayeh et al568
Dow
implant considerations. The assessment is sensi-tive to (a function of) B1 RMS, and the test methodis described in ISO/TS 10974:2018.16
The concept of this assessment is:
� Benchtop/scanner: The AIMD (the IPG andthe connected leads) is positioned in atissue-simulating media phantom and placedinside an RF birdcage (designed for testingor of a scanner) and lead electrode heatingis measured under various incident field con-ditions (multiple lead pathways and/or RFexposures).
� Simulation: Using simulation of this benchtopsetup (in vitro), the E-tans are extracted for allclinical lead pathways.
� Benchtop or simulation: The transfer functionof the AIMD is measured in benchtop injectedsetup or simulated.
� A predictive model of heating (and/or power)is established using the dot product of
nloaded for Anonymous User (n/a) at Washington University in Saint Louis B November 18, 2020. For personal use only. No other uses without perm
E-tans and transfer function per the followingformula19:
P 5 A
����Z l
0
ShotspotðzÞEtanðzÞdz����2
Equation 1
Where P is power (or heating), A is scaler imbe-dding the linear fit of the AIMD model and the inci-dent field levels, S is the transfer function, E-tansare the in vitro tangential electrical incident fields,and dz is the spatial distance increment alonglead length.
� The previous formula, which describes howthe AIMD model is derived, is also applied tothe extracted E-tans of the human (in vivo)simulations. This often results in thousandsto millions of heating predictions, accounting
Fig. 5. When the AIMD is exposed toa uniform E-tan excitation, the trans-fer function is obtained via measure-ments in benchtop RF injected setupor simulation. The peaks in its magni-tude represent resonance lengths.The example here shows two reso-nance lengths. (From ISO/TS10974:2018. Assessment of the safetyof magnetic resonance imaging forpatients with an active implantablemedical device; with permission.)
ernard Becker Medical Library from ClinicalKey.com by Elsevier onission. Copyright ©2020. Elsevier Inc. All rights reserved.

Practical Aspects of MR Imaging Safety Test Methods 569
for all clinical lead pathway scenarios and im-aging conditions (human models, RF coils,and landmarks).
� Experimental exposure tests yield normaliza-tion factors that tie the heating results to spe-cific B1 1 RMS levels, allowing prediction ofheating under any desired B1 1 RMS, andMR imaging normal mode or first level modeSpecific Absorption Rate (SAR) conditions.
� The heating acceptance criterion for the tissuesurrounding the electrodes dictates what RFlimit is appropriate for this specific AIMD.� If the results of this assessment determinethat this particular AIMD lead electrodesheat up tissue surrounding the electrodesup to X degrees Celsius under MR imagingnormal mode SAR, and if the acceptancecriterion threshold for these tissues heatingis greater than this X level, then scanningunder normal mode is safe for this AIMD.
� However, if the acceptance criterion forthese tissues heating is lower than this Xlevel, then safe scanning requires dialingdown the RF level in the scanner environ-ment to lower than the MR imaging normalmode limit, all the way to the level at whichheating is lower than the acceptance crite-rion threshold. That RF exposure level willbe deemed acceptable and will be ex-pressed in B1 1 RMS (and its correspond-ing SAR) as the RF limit in the MRConditional list of the device label.
Unintended Stimulation from RadiofrequencyField-Induced Rectified Lead Voltage
This assessment is similar to the lead electrodeheating. However, it is sensitive to (a function of)B1 peak. The test is described in ISO/TS10974:2018.16
The concept of this assessment is as follows:
� Benchtop/scanner: The AIMD (the IPG andthe connected leads) is positioned in atissue-simulating media phantom and placedinside an RF birdcage (designed for testingor of a scanner) and lead injection voltage to-ward the IPG is measured under various inci-dent field conditions (multiple lead pathwaysand/or RF exposures).
� Simulation: Using simulation of this benchtopsetup (in vitro), the E-tans are extracted for allclinical lead pathways.
� Benchtop or simulation: The transfer functionof the AIMD is measured in benchtop injectedsetup or simulated.
� A predictive model of injection voltage is es-tablished using the dot product of E-tans
Downloaded for Anonymous User (n/a) at Washington University in Saint November 18, 2020. For personal use only. No other uses witho
and transfer function per the followingformula:
V 5 A
Z l
0
SðzÞEtanðzÞdz Equation 2
Where V is the voltage level, A is scaler imbeddingthe linear fit of the AIMD model and the incidentfield levels, S is the transfer function, E-tans arethe in vitro tangential electrical incident fields,and dz is the spatial distance increment alonglead length.
� The previous formula, which describes howthe AIMD model is derived, is also applied tothe extracted E-tans of the human (in vivo)simulations. That results in thousands to mil-lions of RF level predictions accounting forall clinical lead pathway scenarios and imag-ing conditions (human models, RF coils, andlandmarks).
� The proper B1 peak values reflecting variousRF coil types in clinical scanners are used inthis assessment.
� The IPG should pass the acceptance criterionestablished by the device manufacturerbased on the intended functionality whenthis voltage level is injected into the IPG.
Unintended Stimulation from Gradient Field-Induced Lead Voltage (Extrinsic ElectricPotential)
Various scenarios of intralead, interlead, or be-tween electrodes and a conductive IPG enclosurecan result in current flow through the IPG andcould cause unintended stimulation to tissue incontact with the electrodes. This assessment issimilar to the RF field-induced rectified leadvoltage. However, per the nature of gradient fields,it does not rely on a transfer function. The assess-ment is sensitive to (a function of) dB/dt peak. Thetest is described in ISO/TS 10974:2018.16
The concept of this assessment is as follows:
� The injection voltage assessment is estab-lished using the extracted E-tans of the hu-man (in vivo) gradient simulations:
V 5
ZE,dl Equation 3
Where V is the voltage level, E are the in vitrotangential electrical incident fields, and dl is thespatial distance increment along lead length.
Louis Bernard Becker Medical Library from ClinicalKey.com by Elsevier onut permission. Copyright ©2020. Elsevier Inc. All rights reserved.

Al-Dayeh et al570
Dow
� That results in thousands to millions of voltagepredictions accounting for all clinical leadpathway scenarios and imaging conditions(human models, gradient coils, andlandmarks).
� The IPG should pass the acceptance criterionestablished by the device manufacturerbased on the intended functionality whenthis voltage is injected into the IPG.
Learning points for radiologists on scanning pa-tients safely per implant MR labels:
� For an MR Conditional AIMD, the labelingconditions take care of the safety issues aslong as clinical conditions stay within themper the device MR imaging instructions foruse. That is, the clinical team does not needto deal with specific AIMD-MR risk-benefit de-cisions, if the conditions are be met as per theMR Conditional labels.
� Some implants allow scanning under the MRimaging scanner normal mode, which doesnot usually pose a challenge to MR technolo-gists in performing safe and effectiveexaminations.
� Other implants may have limits on time-varying gradients (not likely) and/or RF, whichis the most common limit (typically expressedas B1 1 RMS and/or SAR limits).
� Implants with a zonal (landmark) restrictiontypically have a restriction based on sensitivityto B1 1 RMS.
� Implants with coil-type restriction (eg, a headcoil–only MR label) are also related to RF re-striction based on sensitivity to B1 1 RMS(although B1 peak is different for variouscoils). Head-only Tx coils expose the patientsto RF fields only within the head coil. In de-vices only cleared for head coil transmission,if the RF body coil activates, or if the RF coilis a receive-only head coil, it could present asignificant patient hazard.
� For those implants with RF limit of B1 1 RMS(and its corresponding SAR limit), using theB1 1 RMS based limit is better (less restric-tive), provided the scanner shows B1 1RMS. This is because the SAR limit is the min-imum value for the range of SAR values corre-sponding to this one B1 1 RMS limit (ie, foreach B1 1 RMS value, the correspondingSAR is a range because SAR is a function ofbody weight and landmark).
� Not obeying the RF limits of MR Conditionallabel can lead to exceeding the acceptablelimit for patient harms that are sensitive toB1 1 RMS/SAR and/or RF coil type
nloaded for Anonymous User (n/a) at Washington University in Saint Louis Ber November 18, 2020. For personal use only. No other uses without permis
restrictions and/or zone landmark restrictions,most importantly electrode heating. The mostprominent example, documented in 2005, is aDBS patient who was scanned in violation ofmultiple labeling conditions, leading to a per-manent neurologic deficit.8
� Device malfunctions are related to B0 fieldstrength, or B1 peak or dB/dt peak levels, pa-rameters that cannot readily be altered pres-ently by an MR technologist in the clinic.Thus, it is important to abide by the MR imag-ing conditions defined in the label for safescanning.
� For AIMDs requiring setting up the device inMR imaging mode before scanning, it isimportant to do so to avoid potential devicemalfunctions that can occur either during orfollowing MR imaging exposure.
� For AIMDs requiring RF lower than normalmode when the pulse sequence to be usedexceeds the implant B1 1 RMS/SAR limit,� If the scanner is implant friendly, use therecommended option/software. A goodexample of that is Philips Healthcare (Am-sterdam, the Netherlands) ScanWiseImplant system.20 Otherwise, any param-eter that affects RF can be adjusted toreduce RF.
� Use the “Low SAR” option. It is available onmost scanners and helps to reduce B1 1RMS/SAR, typically without impacting im-age quality significantly. Always use this op-tion in combination with one or moreoptions from the following:
� Increase TR (not to the extent of changingcontrast, as in T1-SE sequences), and/or,
� Reduce the number of slices (slicegrouping), and/or,
� Reduce flip-angle (alpha), reduce refocus-ing flip angle, or using fewer RF saturationbands.
� Reduce the number of echoes (echo trainlength/turbo factor/shot factor).
SUMMARY
MR Conditional labels for AIMDs are developedthrough rigorous testing by implantable devicemanufacturers, using methods and guidelinesthat were developed with contributions from ex-perts in various fields including MR scanner man-ufacturers, implant manufacturers, and regulatoryagencies. Formal instructions for use of MRCondi-tional implants are the proper source for MR scan-ning conditions and parameters that can ensurepatient safety. The MR imaging safety communityis gaining expertise from the use of more MR
nard Becker Medical Library from ClinicalKey.com by Elsevier onsion. Copyright ©2020. Elsevier Inc. All rights reserved.

Practical Aspects of MR Imaging Safety Test Methods 571
Conditional AIMDs and reflecting these learningswith collaborations from experts in the field forthe benefit and safety of scanning patients with im-plants. Patients and clinicians have also benefittedfrom efforts by MR manufacturers to design moreadvanced MR imaging scanners and software,including those with options for limiting exposurefields. These have already helped clinicians to pro-vide access to MR imaging for patients withimplanted devices, and there are exciting opportu-nities for improving patient safe access in thefuture through advancing technologies andcontinued collaboration in the development ofsafety testing methods and standards.
REFERENCES
1. IEC 60601-2-33:20101AMD1:20131AMD2:2015
CSV, Consolidated version. Medical electrical equip-
ment - Part 2-33: Particular requirements for the
basic safety and essential performance of magnetic
resonance equipment for medical diagnosis.
2. Delfino JG, Krainak DM, Flesher SA, et al. MRI-
related FDA adverse event reports: a 10-yr review.
Med Phys 2019;46(12):5562–71.
3. Erlebacher JA, Cahill PT, Pannizzo F, et al. Effect of
magnetic resonance imaging on DDD pacemakers.
Am J Cardiol 1986;57(6):437–40.
4. Becker RL, Norfray JF, Teitelbaum GP, et al. MR im-
aging in patients with intracranial aneurysm clips.
AJNR Am J Neuroradiol 1988;9(5):885–9.
5. Klucznik RP, Carrier DA, Pyka R, et al. Placement of
a ferromagnetic intracerebral aneurysm clip in a
magnetic field with a fatal outcome. Radiology
1993;187(3):855–6.
6. Fagan LL, Shellock FG, Brenner RJ, et al. Ex vivo
evaluation of ferromagnetism, heating, and artifacts
of breast tissue expanders exposed to a 1.5-T MR
system. J Magn Reson Imaging 1995;5(5):614–6.
7. Hess T, Stepanow B, Knopp MV. Safety of intrauter-
ine contraceptive devices during MR imaging. Eur
Radiol 1996;6(1):66–8.
8. Henderson JM, Tkach J, Phillips M, et al. Permanent
neurological deficit related to magnetic resonance
imaging in a patient with implanted deep brain stim-
ulation electrodes for Parkinson’s disease: case
report. Neurosurgery 2005;57(5):E1063.
Downloaded for Anonymous User (n/a) at Washington University in Saint November 18, 2020. For personal use only. No other uses witho
9. ASTM F2182 - 19e2. Standard test method for mea-
surement of radio frequency induced heating on or
near passive implants during magnetic resonance
imaging.
10. ASTM F2503-20. Standard practice for marking
medical devices and other items for safety in the
magnetic resonance environment.
11. Shellock FG, Kanal E. Magnetic resonance: bio-
effects, safety, and patient management. New
York: Raven Press; 1994.
12. Shellock FG. Pocket guide to MR procedures and
metallic objects: update 1994. New York: Raven
Press; 1994.
13. ISO 14708-1:2014. Implants for surgery — Active
implantable medical devices — Part 1: General re-
quirements for safety, marking and for information
to be provided by the manufacturer.
14. Mitka M. First MRI-safe pacemaker receives condi-
tional approval from FDA. JAMA 2011;305(10):
985–6.
15. ISO/TS 10974:2012. Assessment of the safety of
magnetic resonance imaging for patients with an
active implantable medical device.
16. ISO/TS 10974:2018. Assessment of the safety of
magnetic resonance imaging for patients with an
active implantable medical device.
17. ASTM F2052-15. Standard test method for measure-
ment of magnetically induced displacement force on
medical devices in the magnetic resonance
environment.
18. ASTM F2213-17. Standard test method for measure-
ment of magnetically induced torque on medical de-
vices in the magnetic resonance environment.
19. Park SM, Kamondetdacha R, Nyenhuis JA. Calcula-
tion of MRI-induced heating of an implanted medical
lead wire with an electric field transfer function.
J Magn Reson Imaging 2007;26(5):1278–85.
20. Available at: https://www.usa.philips.com/
healthcare/education-resources/technologies/mri/
scanwise-implant. Accessed July 18, 2020.
21. Kainz W. MR heating tests of MR critical implants.
J Magn Reson Imaging 2007;26(3):450–1.
22. ASTM F2119 - 07(2013). Standard test method for
evaluation of MR image artifacts from passive
implants.
Louis Bernard Becker Medical Library from ClinicalKey.com by Elsevier onut permission. Copyright ©2020. Elsevier Inc. All rights reserved.