Embed Size (px)
Citation preview
Practical approach to the pediatric chest Xray
IX Congress of the Latin American Society of Pediatric Radiology
Buenos Aires on September 7-9, 2005
Mutsuhisa Fujioka, M.D.Chairman, The Asian and Oceanic Society for Pediatric Radiology
Professor and Chairman, Department of Radiology, Dokkyo University School of Medicine
Valoraction practica de la RX de torax
http://www.aospr.org/
Journal
Editorial board members
Managing Editors
(Africa, Asia, Australasia, Europe, and elsewhere outside the Americas)Dr. S. ChapmanThe Birmingham Children’s Hospital NHS TrustSteelhouse LaneBirmingham B4 6NHUnited Kingdom [email protected]
(The Americas)Dr. T. L. SlovisChildren’s Hospital c/o: CRCM3901 Beaubien BoulevardDetroit, MI 48201, [email protected]
Assistant Editors
Dr. D. FrushDuke University Medical Center Div of Pediatric Radiology (Box 3808)1905 McGovern Davison Children’s Hlth. Ctr.Durham, NC 27710, [email protected]
Dr. G. SebagDepartment of Paediatric RadiologyHồpital Robert Debré48, boulevard Sérurier75935 Paris Cedex, [email protected]
Honorary Editor
Dr. W. E. BerdonColumbia Presbyterian Medical Center, Babies HospitalDept of Radiology (3-318)3959 BroadwayNew York, NY 10032-1590, [email protected]
Editorial Board
CardiovascularT. Chung, HoustonJ. A. Culham, VancouverM. Oddone, GenoaS. Laurin, LundC. Holmqvist, Lund
ChestV. Donoghue, DublinE. Effmann, SeattleM. Fujioka, UtsunomiyaJ. Lucaya, BarcelonaB. Newman, Pittsburgh
EducationJ. Reid, ClevelandJ-N. Dacher, Rouen
Experimental DesignK. Applegate, Indianapolis
Genetics – Molecular ImagingR. Lachman, Santa MonicaW. McAlister – St. Louis
General Paediatric RadiologyS. Andronikou, Cape TownM. Argyropoulou, IoanninaP. Babyn, TorontoA. Daneman, TorontoH. Ducou Le Pointe, ParisF. Gudinchet, LausanneI-O, Kim, SeoulH. Lederman, San PauloP. Strouse, Ann ArborG. Taylor, BostonR. Teele, Auckland
GastrointestinalG. Benz-Bohm, CologneD. Bloom, DetroitD. Eggli, HersheyM. Hernanz-Schulman, NashvilleK. McHugh, LondonD. Pariente, BicetreC. Sivit, Cleveland
InterventionalP. Chait, TorontoP. Clapuyt, BrusselsJ. Donaldson, ChicagoD. Roebuck, LondonR. Towbin, Philadelphia
MusculoskeletalM. Azouz, MiamiH. Carty, LiverpoolC. Hall, LondonD. Jaramillo, BostonG. Kalifa, ParisM. Keller, WilmingtonT. Laor, Cincinnati
NeuroradiologyC. Adamsbaum, ParisN. Boddaert, ParisF. Brunelle, ParisB. Koch, CincinnatiM. Nelson, Los AngelesC. Robson, BostonY. Sato, Iowa City
OncologyH. Brisse, ParisS. Kaste, MemphisJ. Meyer, WilmingtonC. Owens. London
PerinatalC. Garel, ParisL. Garel, MontrealL. Guibaud, LyonE. Simon, Philadelphia
TechnologyM. Claudon, NancyW. Huda, SyracuseT. Metens, BrusselsW.K. Rorhschneider, HeidelbergK. White, Salt Lake CityC. Willis, HoustonP. Winkler, Stuttgart
UroradiologyF. Avni, BrusselsB. Coley, ColumbusK. Darge, WuerzburgR. Fotter, GrazU. Willi, ZurichM. Zerin, Detroit
Book ReviewsJ. Haller, TeaneckM. Hassan, Paris
Statistics, Information, Technology and EditingH. Fischer, DetroitW. Grever, DetroitR. Thomas, Detroit
Manuscripts must be sent to the appropriate Managing editor only. Please ensure that the manuscript complies with the “Instructions to authors: at http://link.springer.de/link/service/journals/00247/instr.htm
A practical approach to the pediatric chest radiograph
Steps for reading
1. Detection
2. Differentiation
Change in size and shape of normal anatomical structures.
Soft tissue, bones, heart, aorta, trachea, main bronchi, thymus, hili, esophagus, pleura, diaphragms, pulmonary arteries, veins, bronchial walls, gastric air bubble, liver, spleen
What are we looking for?
Abnormality(increased or decreased opacity) which should not be present in normal individual
What are we looking for?
ground-glass opacity(haziness)
consolidation
nodule or mass
linear, reticular or band like shadow
calcification
Increased lung opacity
hyperlucency(air trapping or pneumothorax)
lung cyst or bulla
honeycomb
cavitary nodule or mass
cystic bronchiectasis
Decreased lung opacity and cystic abnormalities
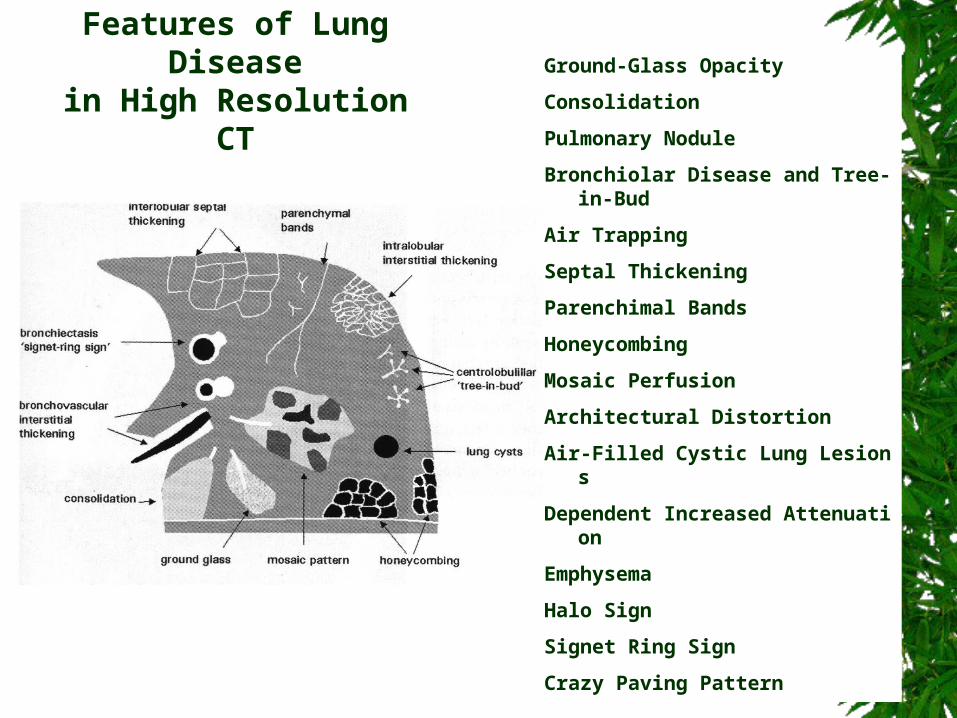
Features of Lung Diseasein High Resolution CT
Ground-Glass Opacity
Consolidation
Pulmonary Nodule
Bronchiolar Disease and Tree-in-Bud
Air Trapping
Septal Thickening
Parenchimal Bands
Honeycombing
Mosaic Perfusion
Architectural Distortion
Air-Filled Cystic Lung Lesions
Dependent Increased Attenuation
Emphysema
Halo Sign
Signet Ring Sign
Crazy Paving Pattern
The main role of HRCT is to differentiate fine pathological abnormality.
Change in size and shape of normal anatomical structures can rather be easier to be detected by the findings of chest radiograph rather than those of CT.
Therefore for adequate interpretation of pediatric chest radiographs, we should be aware of gross abnormal findings which might be overlooked by particular reasons.
However it is very important to know what kind of abnormality is not demonstrable on usual chest radiograph but well demonstrated on CT or HRCT.
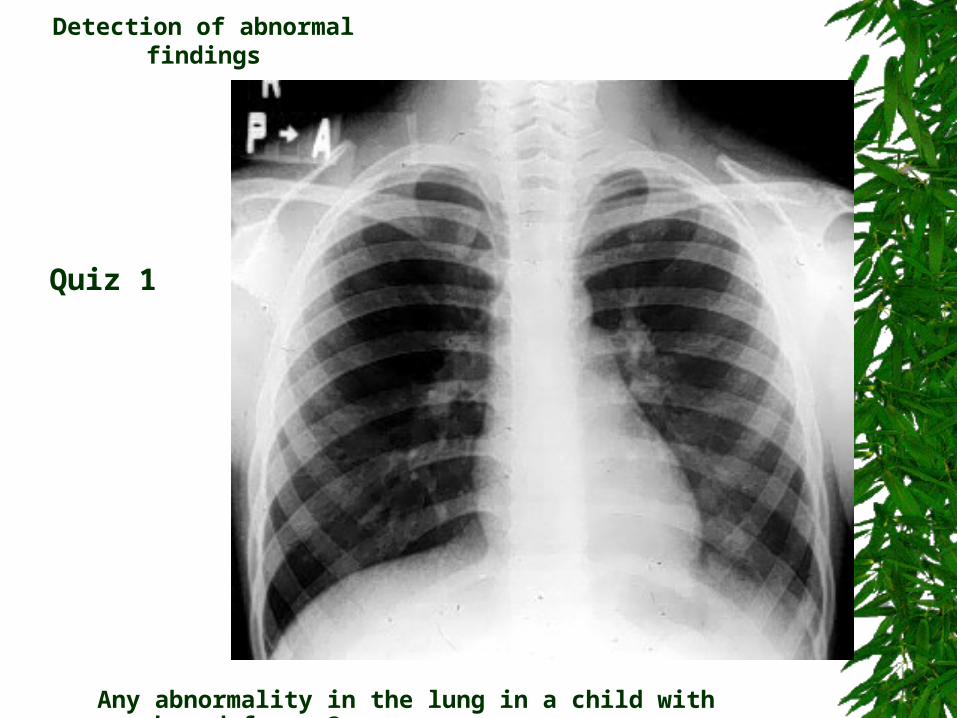
Detection of abnormal findings
Quiz 1
Any abnormality in the lung in a child with cough and fever ?
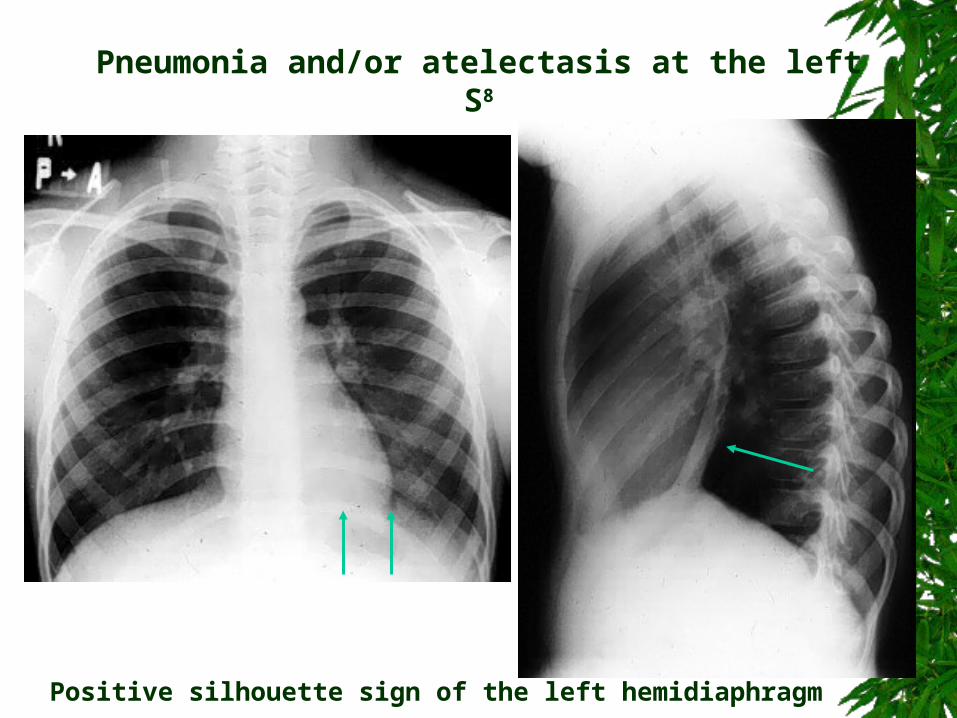
Pneumonia and/or atelectasis at the left S8
Positive silhouette sign of the left hemidiaphragm
2yo Bilateral pneumonia: Lingula of the left upper lobe, right lower lobe
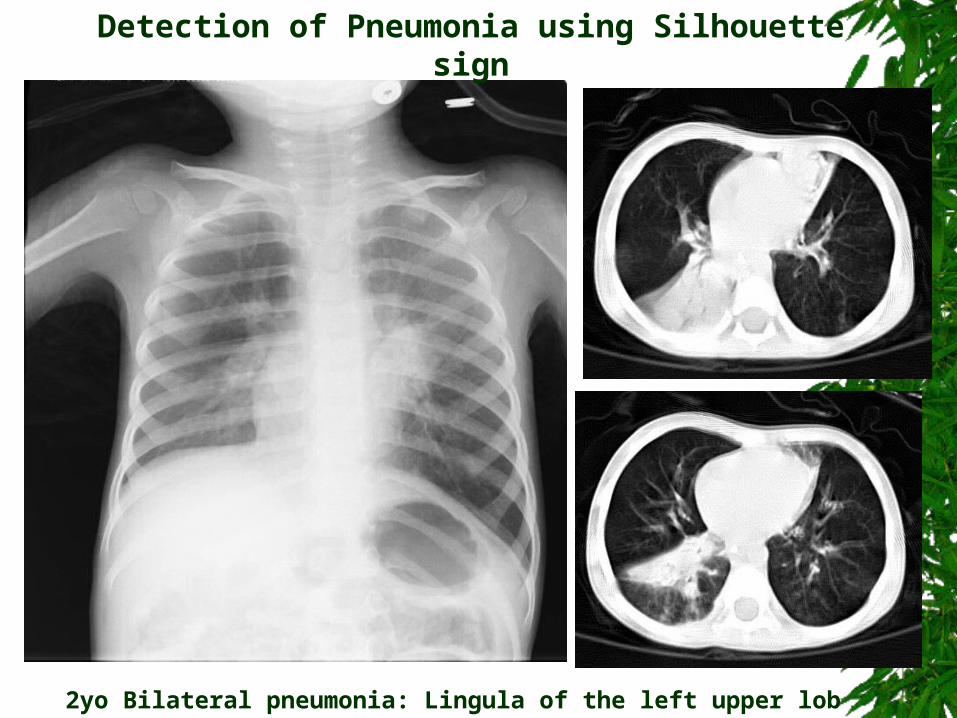
Detection of Pneumonia using Silhouette sign
2yo Bilateral pneumonia: Lingula of the left upper lobe, right lower lobe
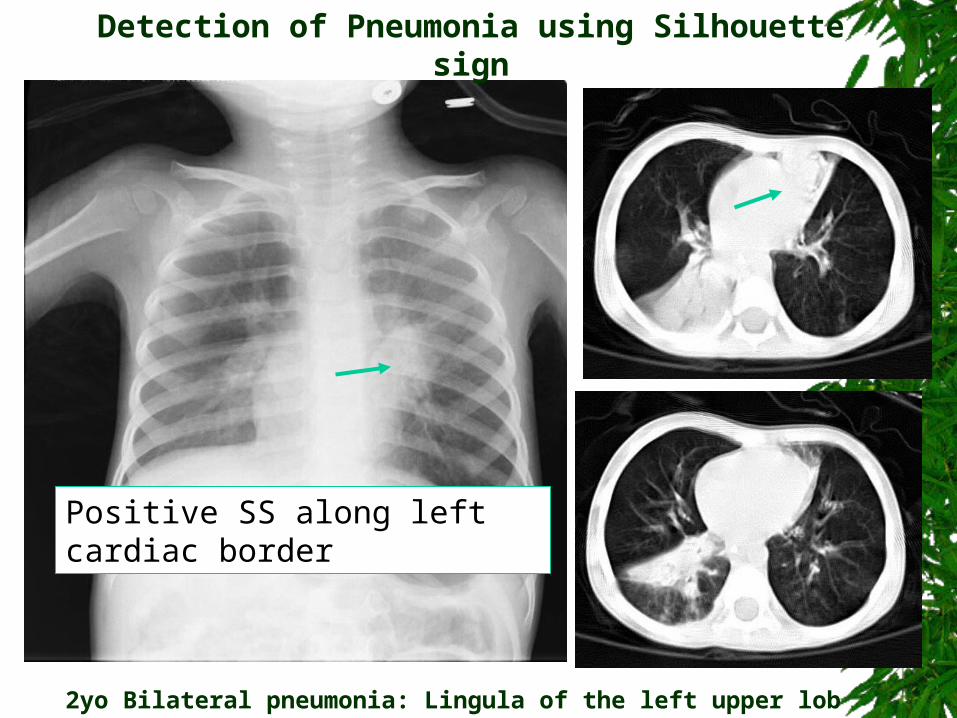
Positive SS along left cardiac border
Detection of Pneumonia using Silhouette sign
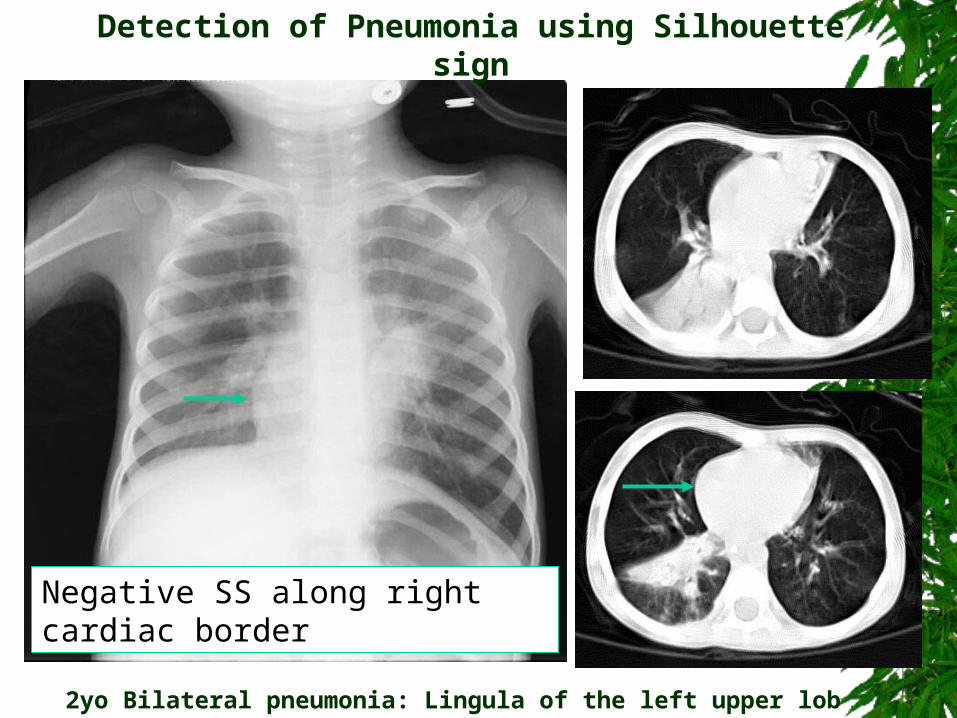
2yo Bilateral pneumonia: Lingula of the left upper lobe, right lower lobe
Negative SS along right cardiac border
Detection of Pneumonia using Silhouette sign
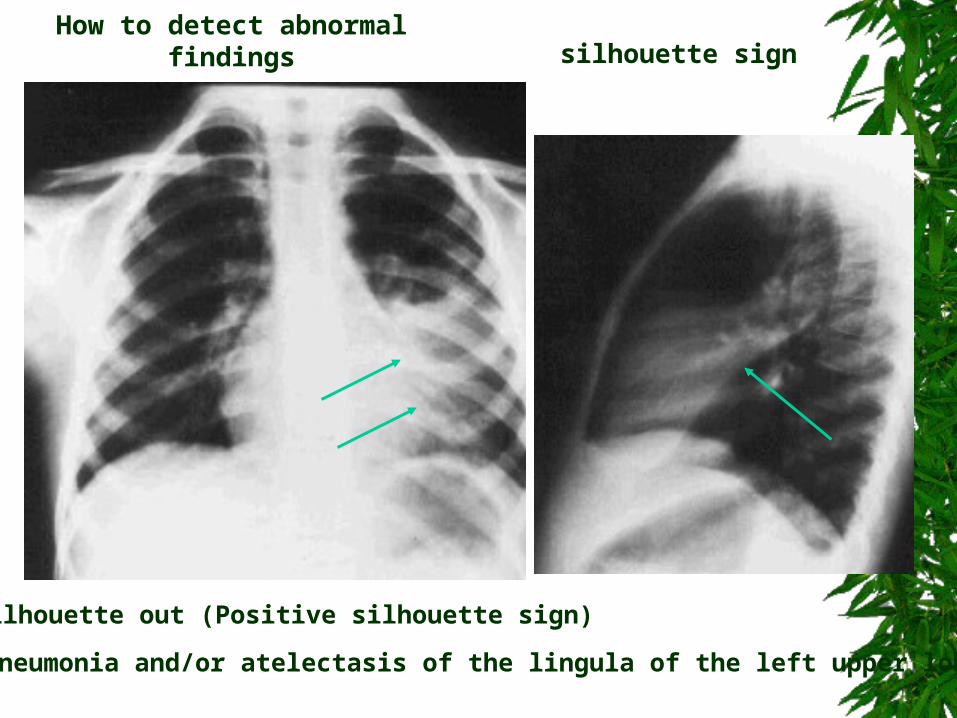
How to detect abnormal findingssilhouette sign
silhouette out (Positive silhouette sign)
Pneumonia and/or atelectasis of the lingula of the left upper lobe
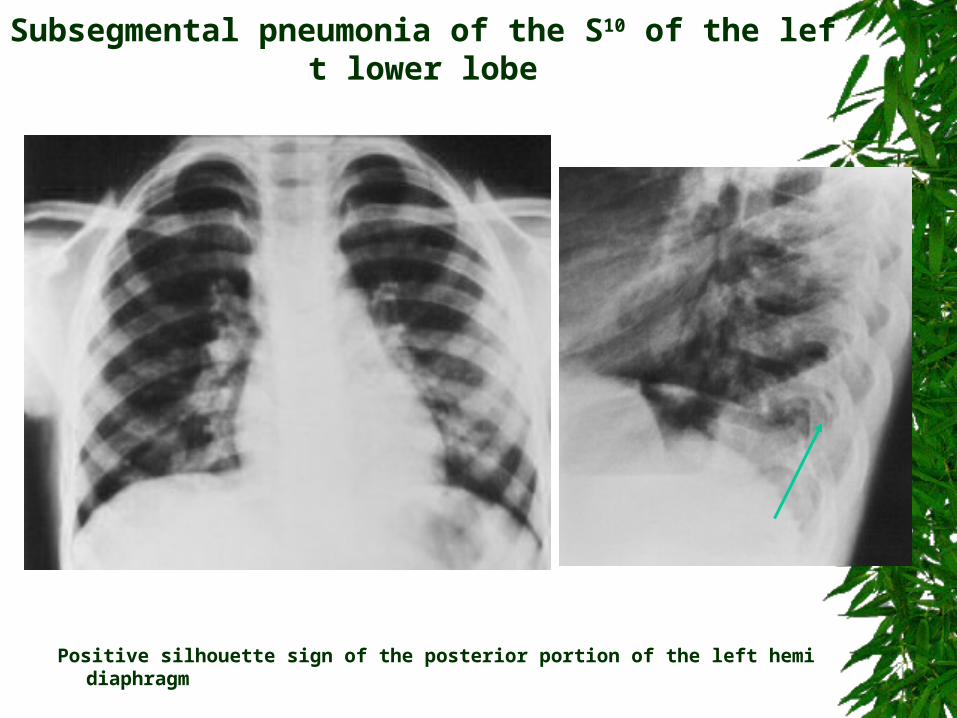
Subsegmental pneumonia of the S10 of the left lower lobe
Positive silhouette sign of the posterior portion of the left hemidiaphragm
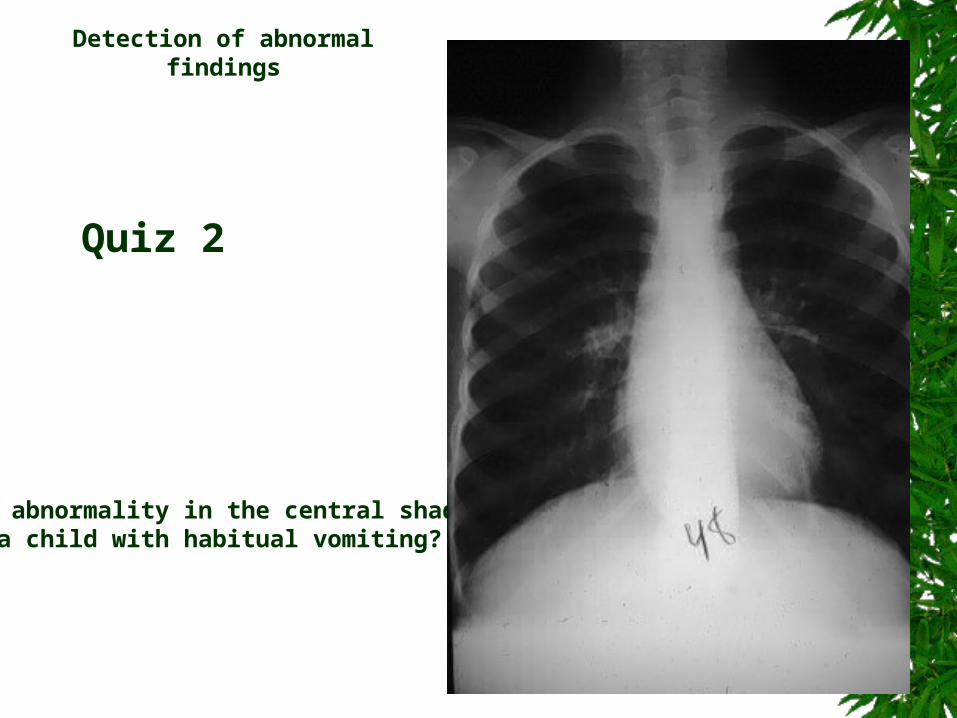
Quiz 2
Detection of abnormal findings
Any abnormality in the central shadow in a child with habitual vomiting?
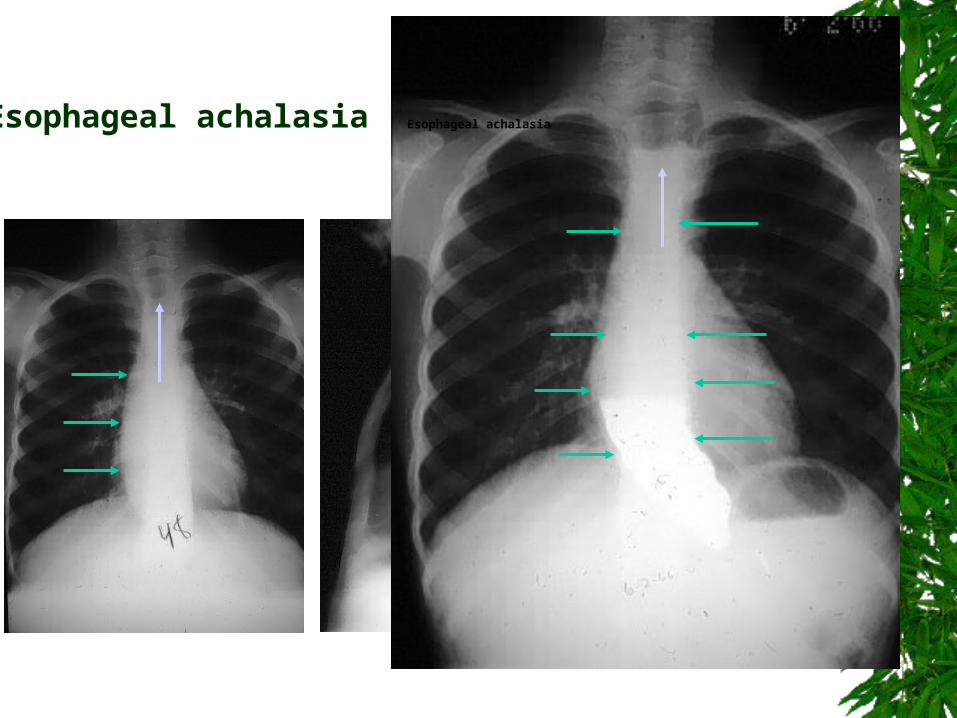
Esophageal achalasia Esophageal achalasia
anterior junction line
posterior junction line
azygoesophageal line
aortic-pulmonic window
aortic pulmonary stripe
left paraspinal line
right paratracheal stripe
posterior tracheal band ( lateral )
tracheo-esophageal stripe ( lateral )
aortic nipple
How to detect abnormal finding
Mediastinal interfaces and lines
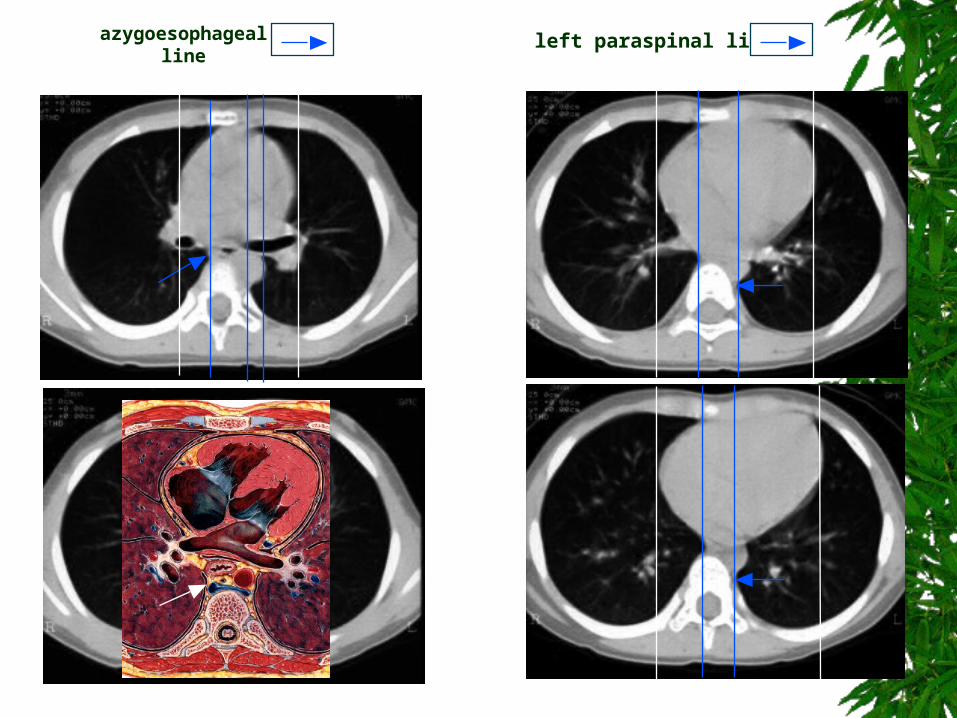
left paraspinal lineazygoesophageal line
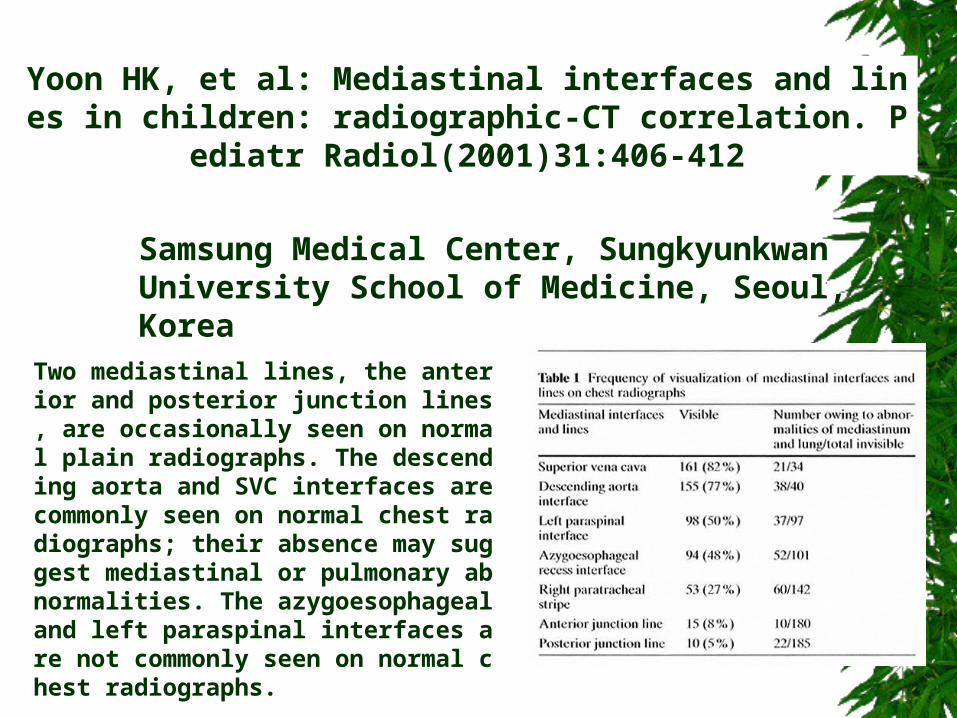
Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
Two mediastinal lines, the anterior and posterior junction lines, are occasionally seen on normal plain radiographs. The descending aorta and SVC interfaces are commonly seen on normal chest radiographs; their absence may suggest mediastinal or pulmonary abnormalities. The azygoesophageal and left paraspinal interfaces are not commonly seen on normal chest radiographs.
Yoon HK, et al: Mediastinal interfaces and lines in children: radiographic-CT correlation. Pediatr Radiol(2001)31:406-412
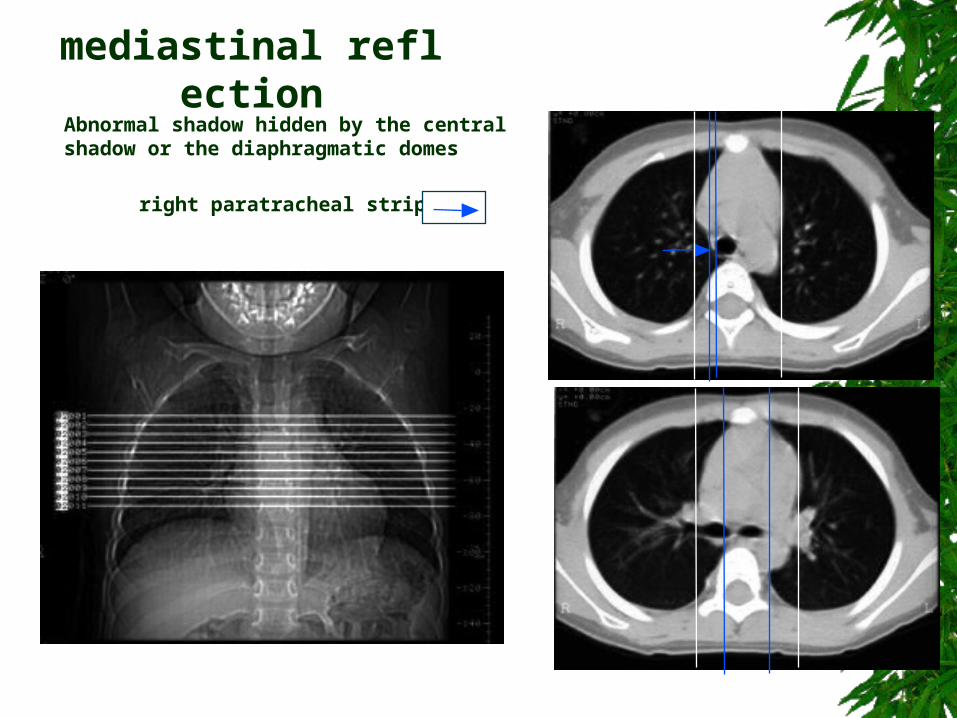
right paratracheal stripe
Abnormal shadow hidden by the central shadow or the diaphragmatic domes
mediastinal reflection
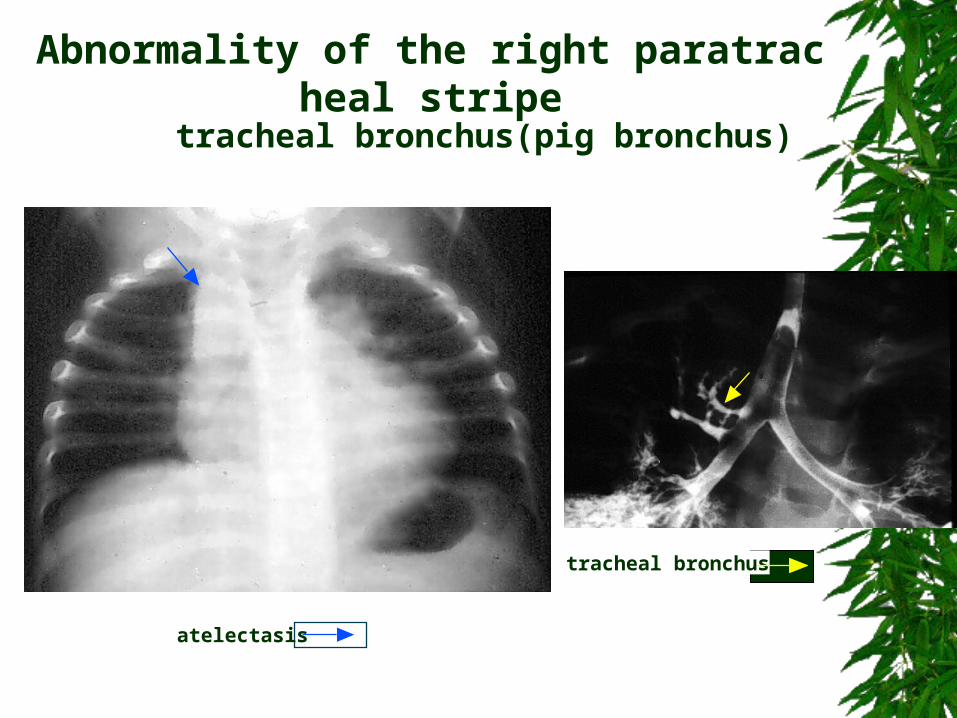
tracheal bronchus(pig bronchus)
tracheal bronchus
atelectasis
Abnormality of the right paratracheal stripe
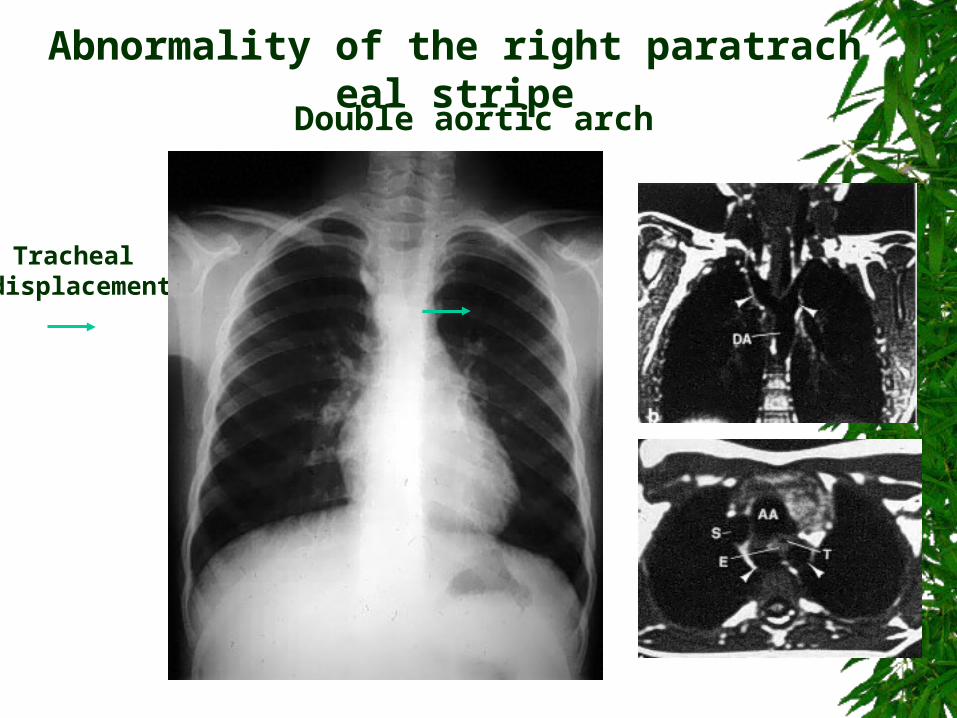
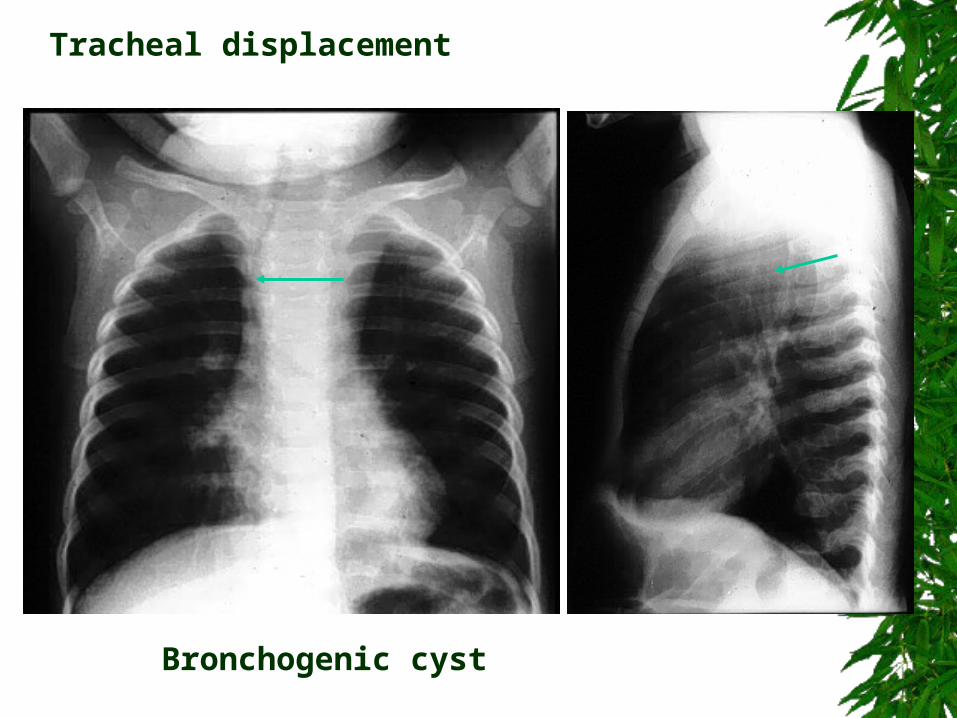
Tracheal displacement
Double aortic arch
Abnormality of the right paratracheal stripe
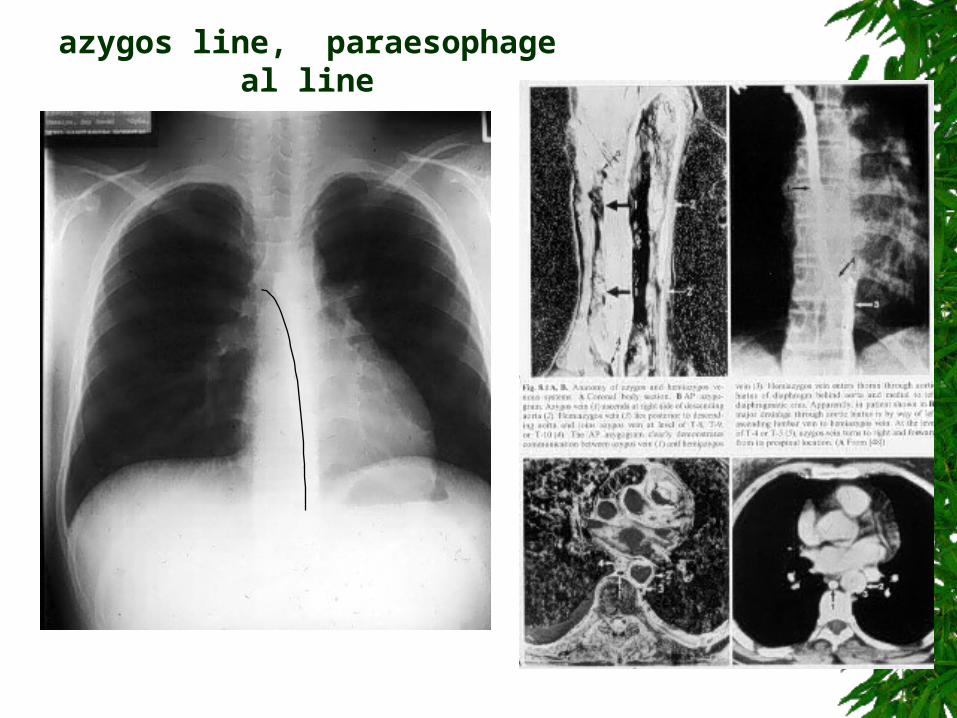
azygos line, paraesophageal line
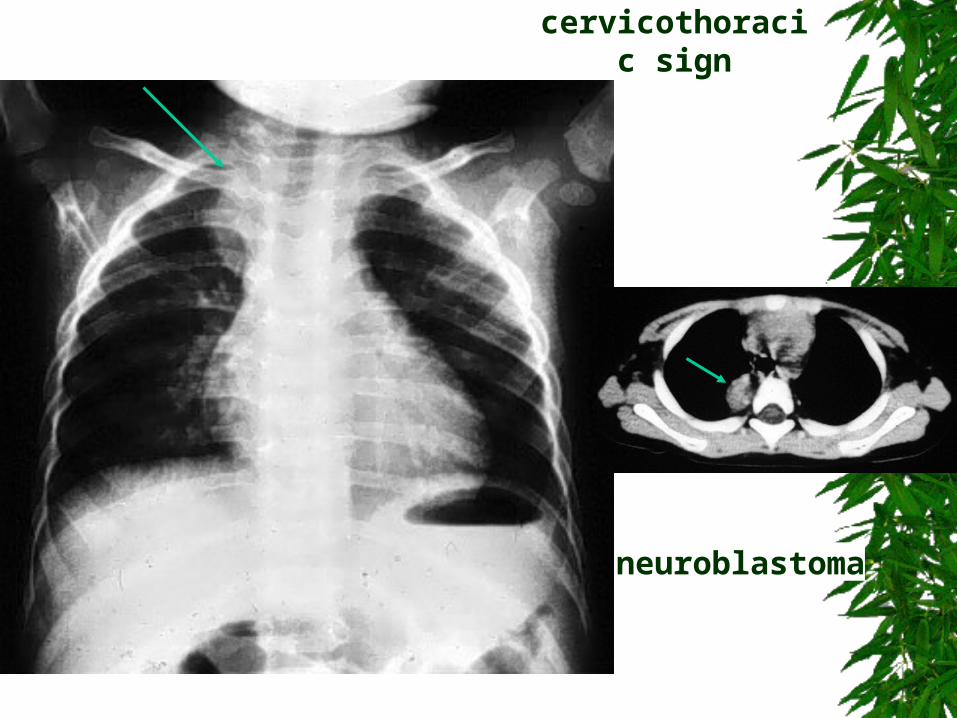
neuroblastoma
cervicothoracic sign
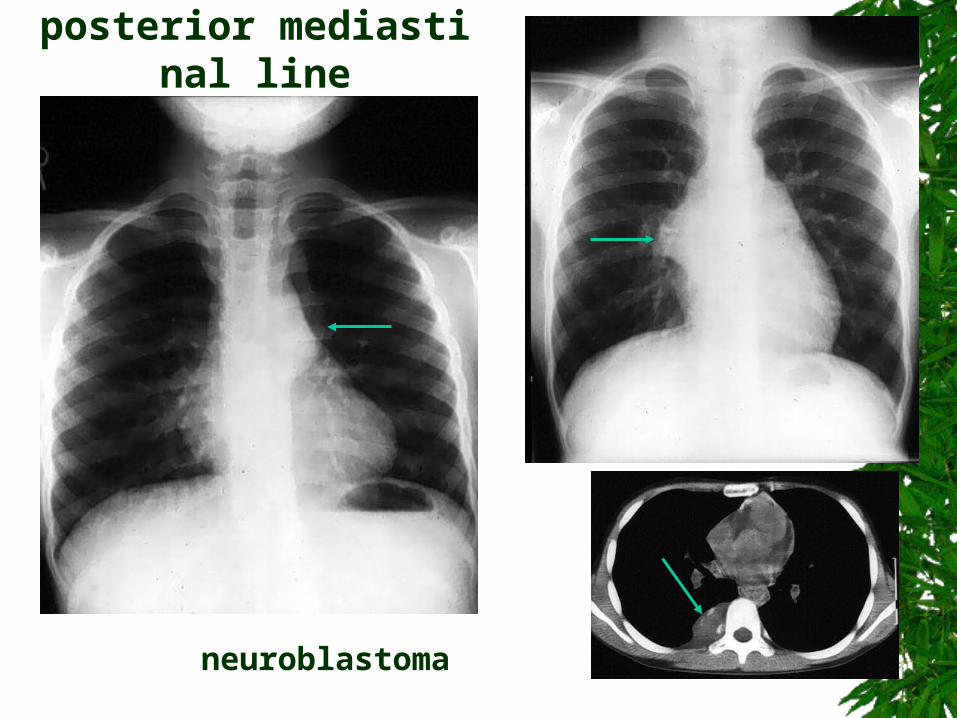
neuroblastoma
posterior mediastinal line
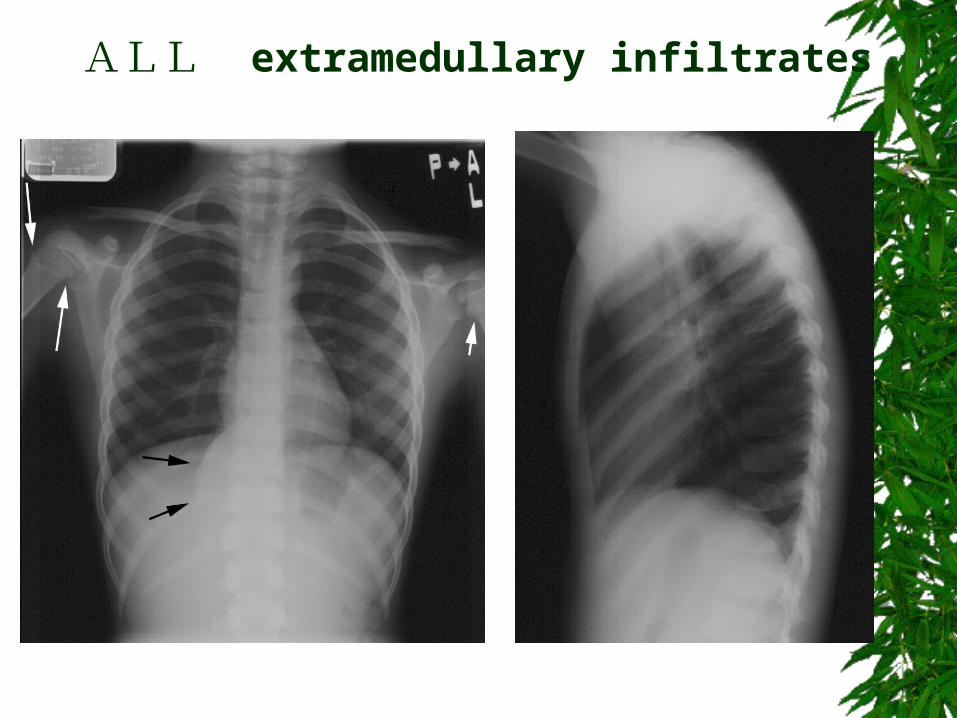
ALL extramedullary infiltrates
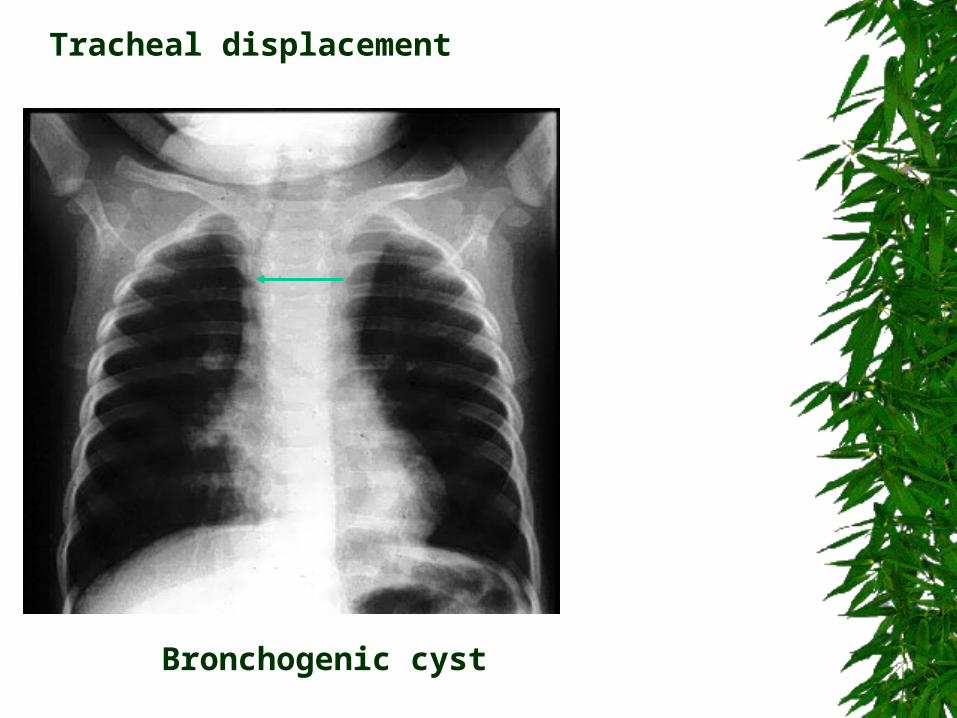
Tracheal displacement
Tracheal displacement
Bronchogenic cyst
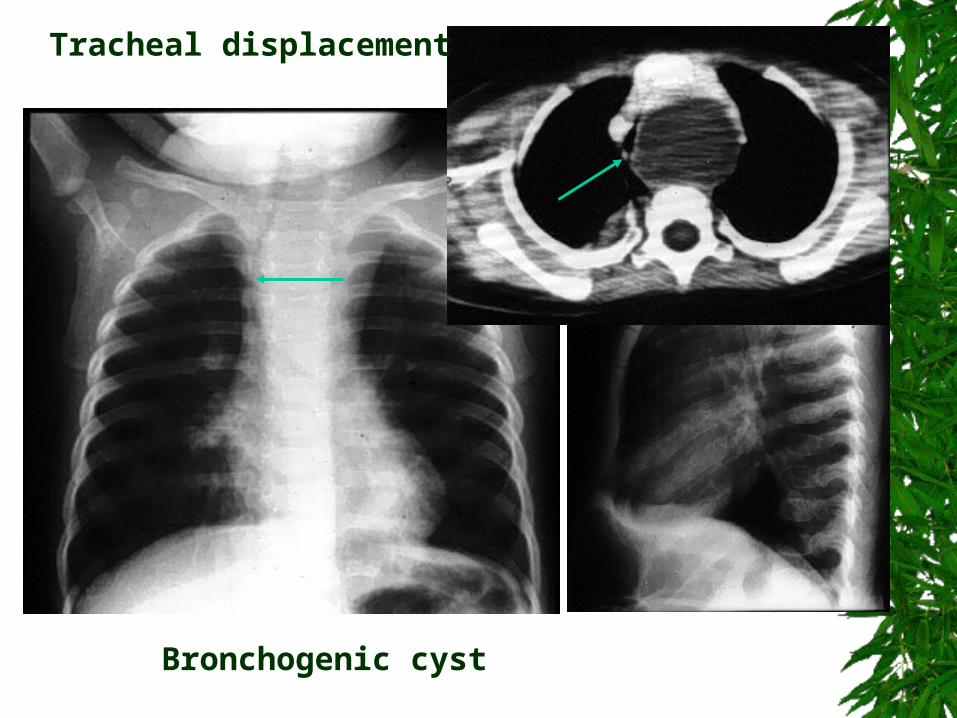
Tracheal displacement
Tracheal displacement
Bronchogenic cyst
Tracheal displacement
Tracheal displacement
Bronchogenic cyst
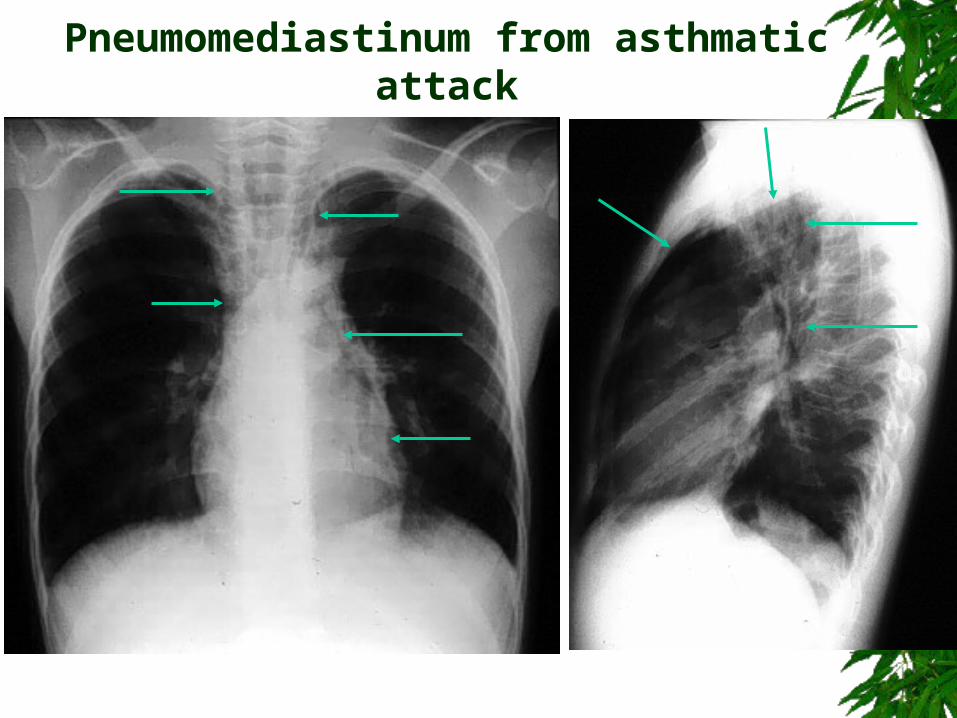
Pneumomediastinum from asthmatic attack
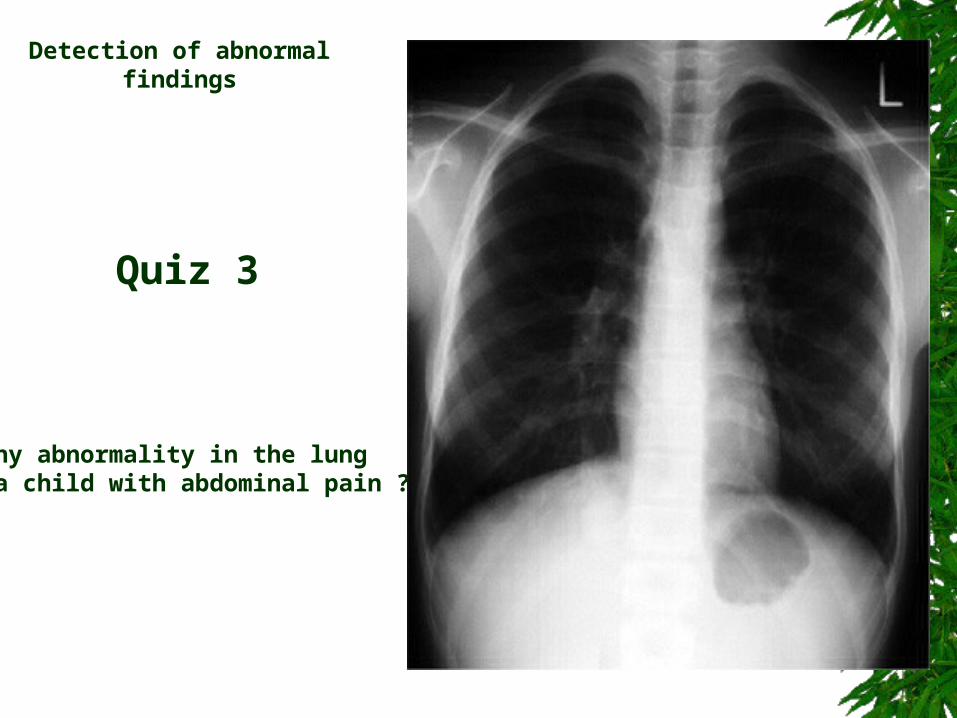
Any abnormality in the lung in a child with abdominal pain ?
Detection of abnormal findings
Quiz 3
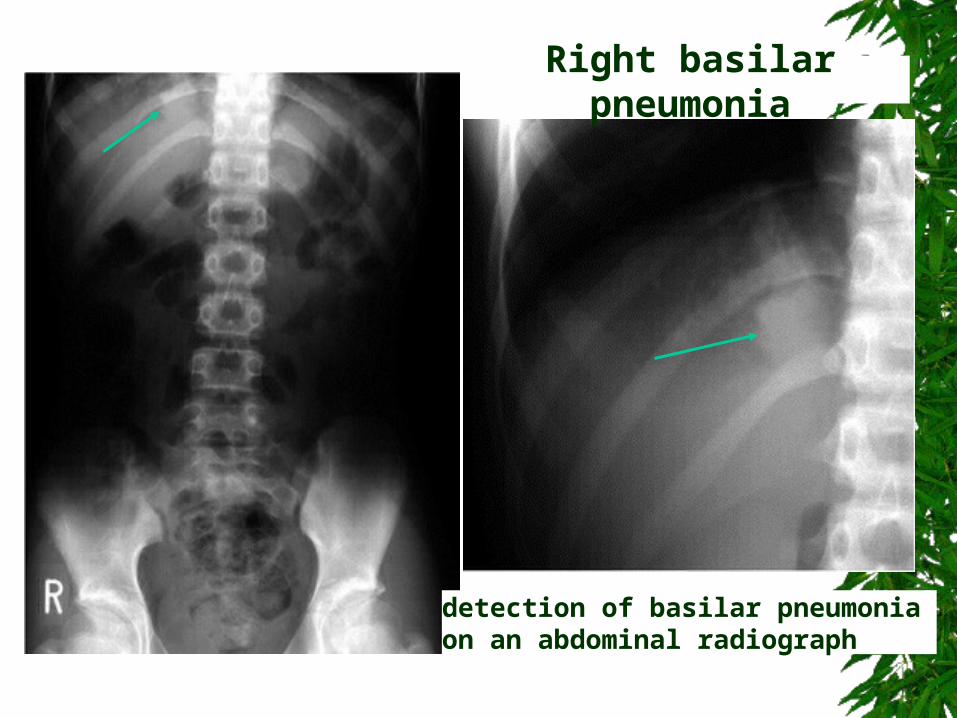
detection of basilar pneumonia on an abdominal radiograph
Right basilar pneumonia
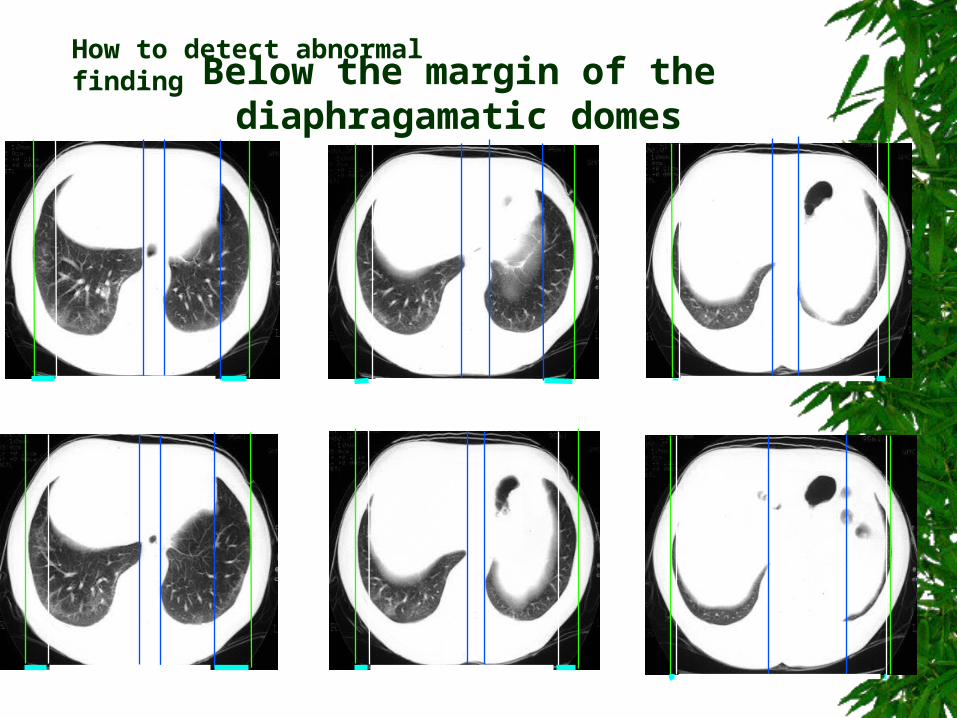
How to detect abnormal finding
Below the margin of the diaphragamatic domes
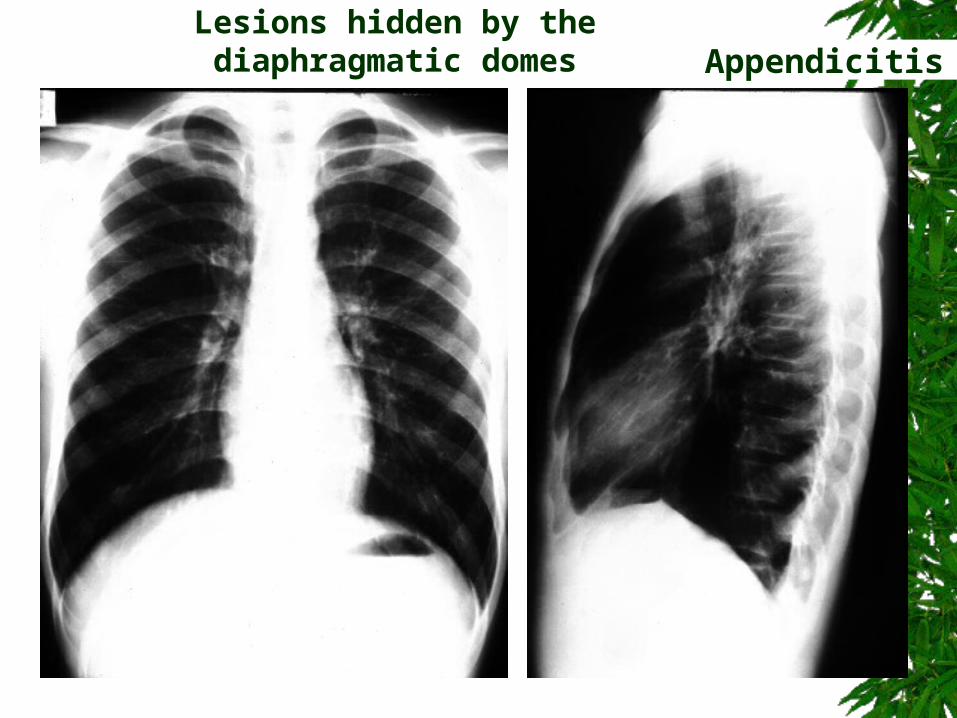
Appendicitis ?Lesions hidden by the diaphragmatic domes
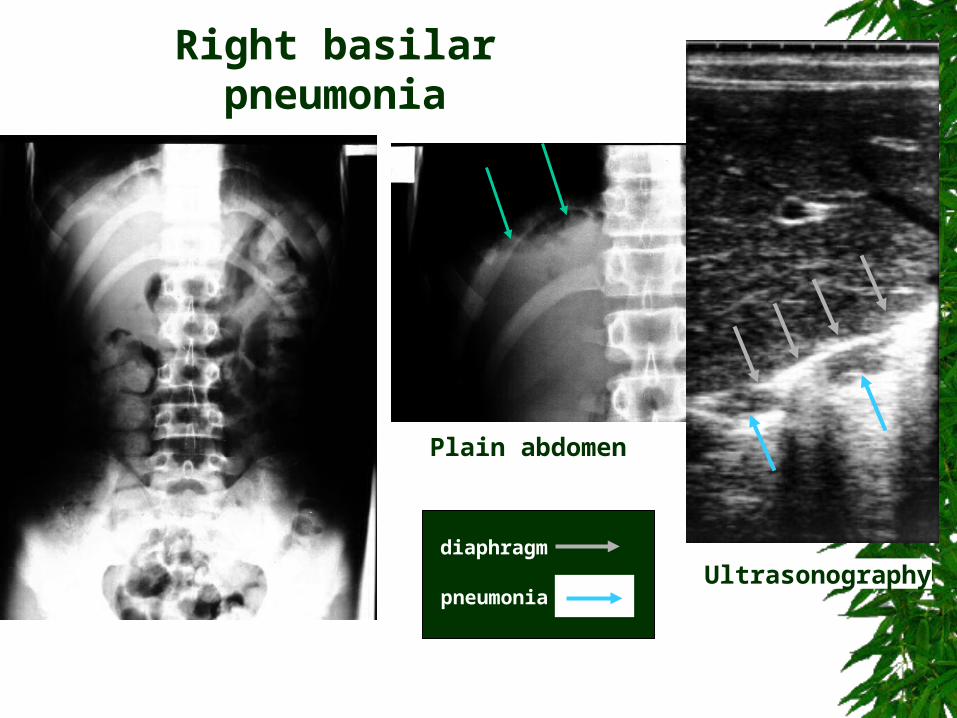
Ultrasonography
Plain abdomen
diaphragm
pneumonia
Right basilar pneumonia
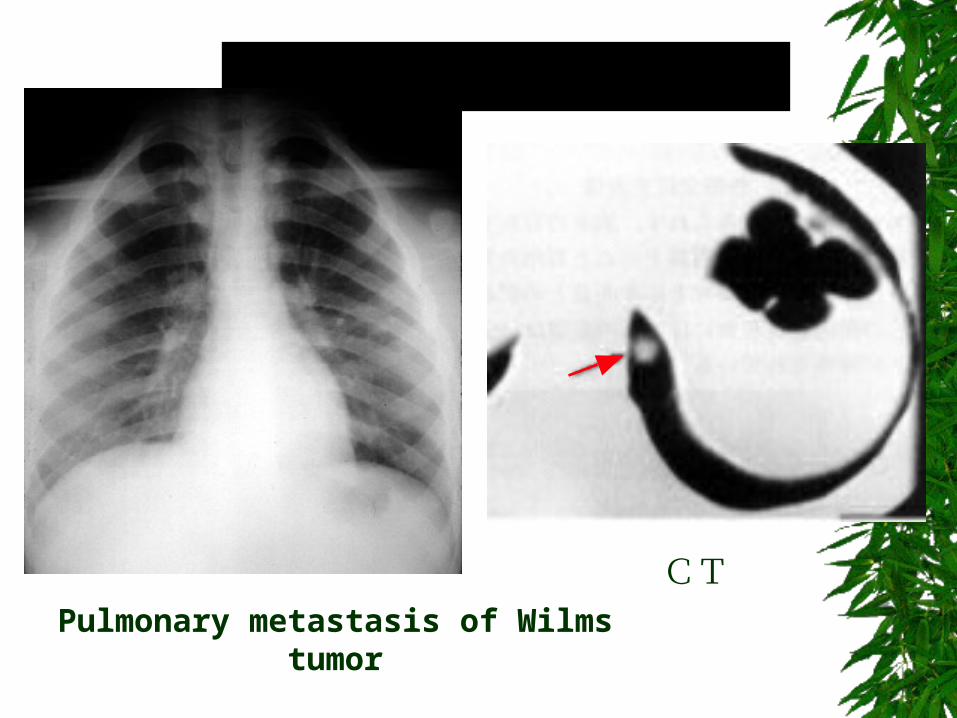
CT
Pulmonary metastasis of Wilms tumor
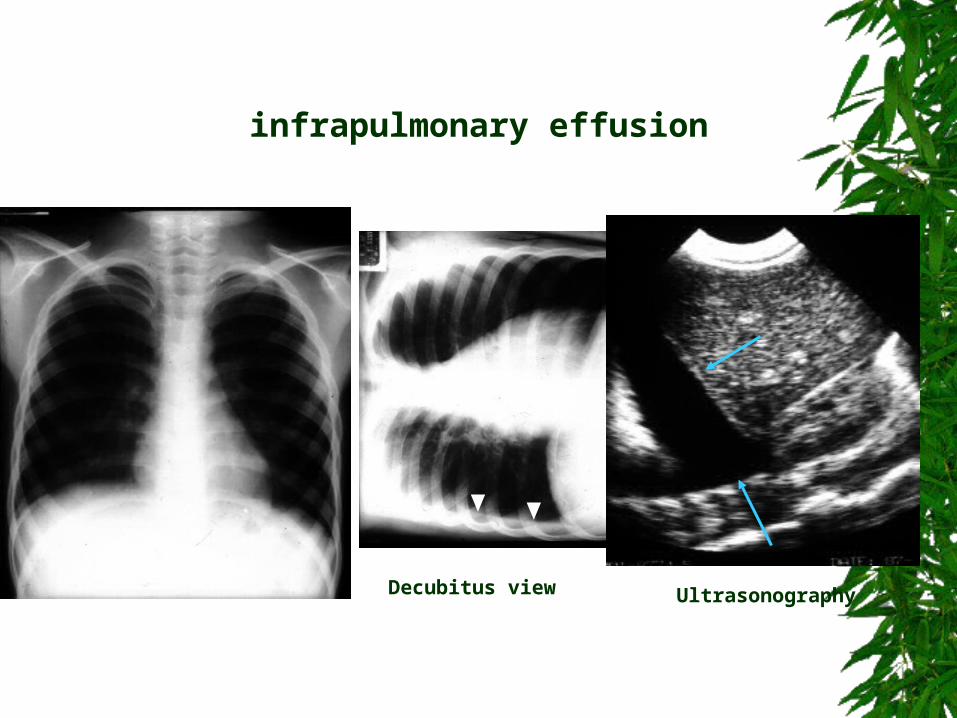
Decubitus view Ultrasonography
infrapulmonary effusion
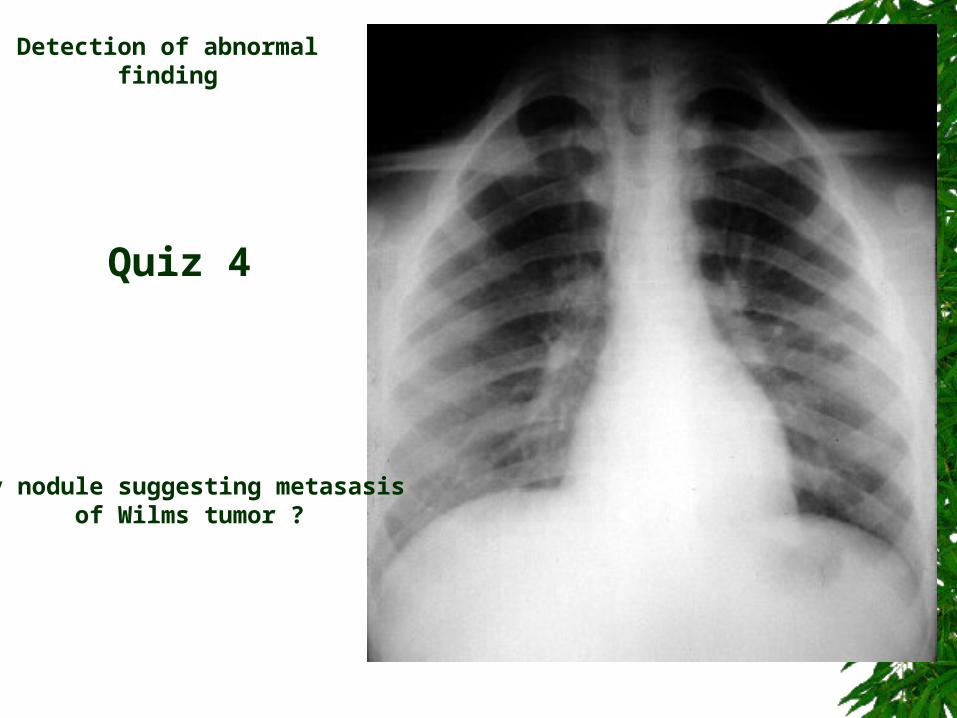
Any nodule suggesting metasasis of Wilms tumor ?
Detection of abnormal finding
Quiz 4
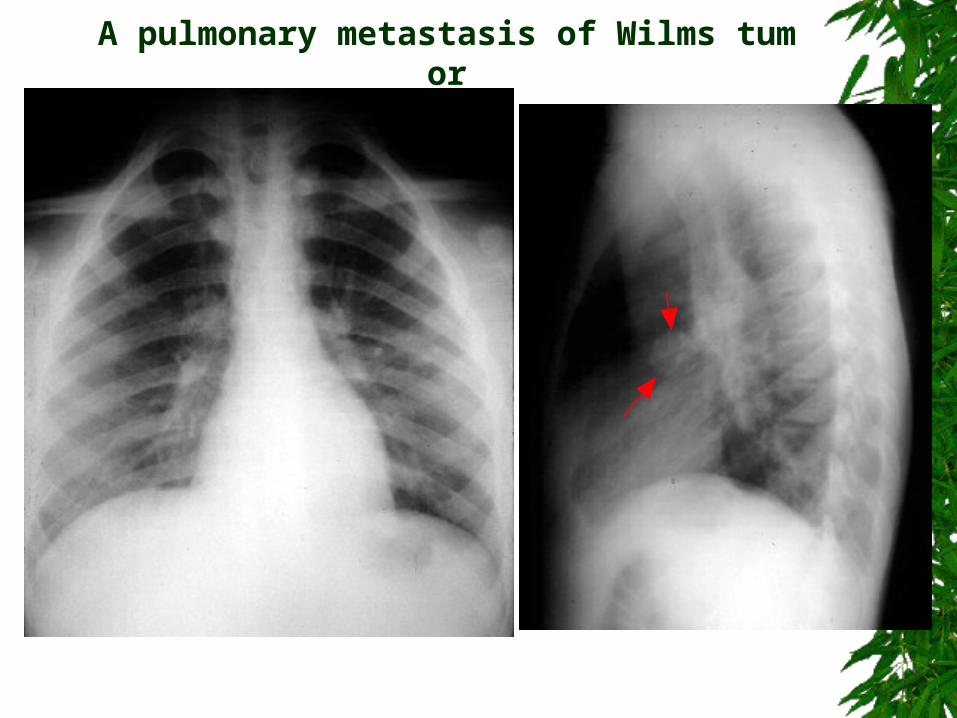
A pulmonary metastasis of Wilms tumor
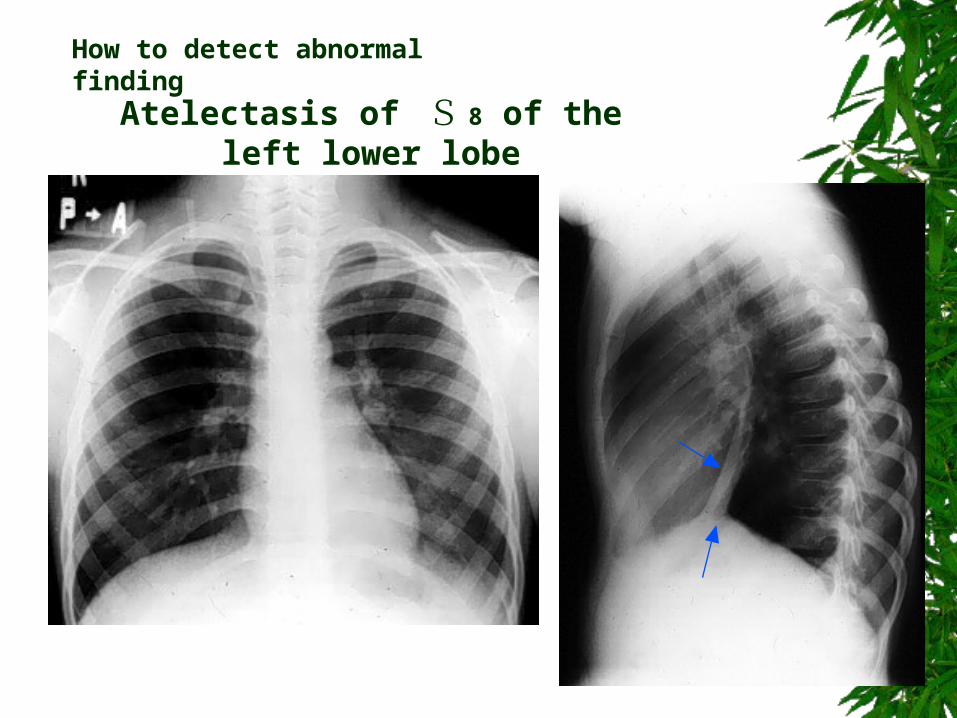
How to detect abnormal finding
Atelectasis of S 8 of the left lower lobe
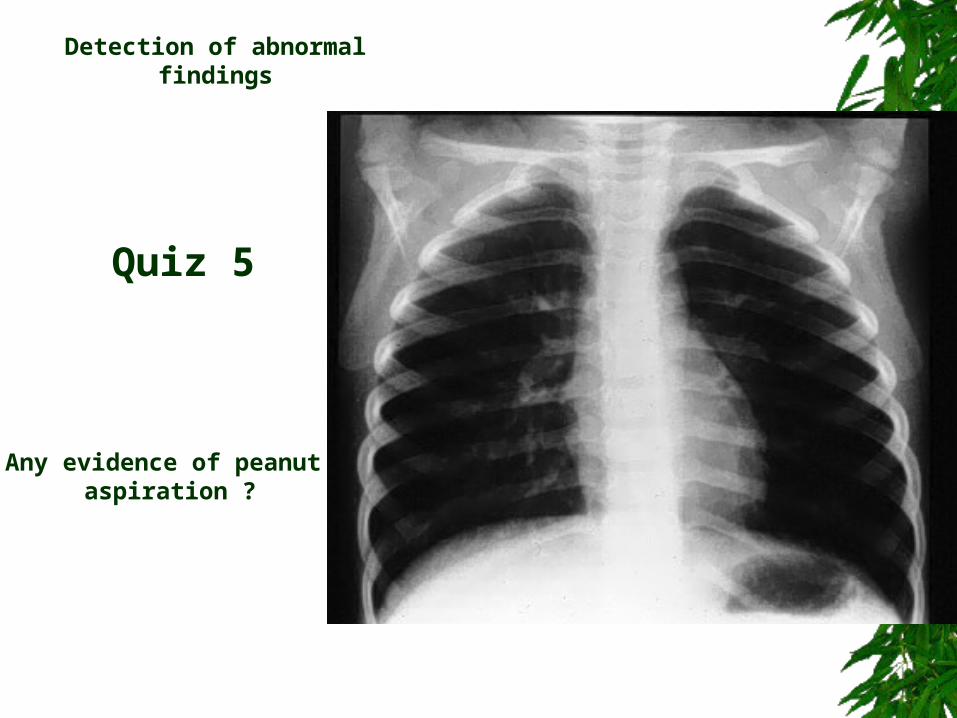
Any evidence of peanut aspiration ?
Detection of abnormal findings
Quiz 5
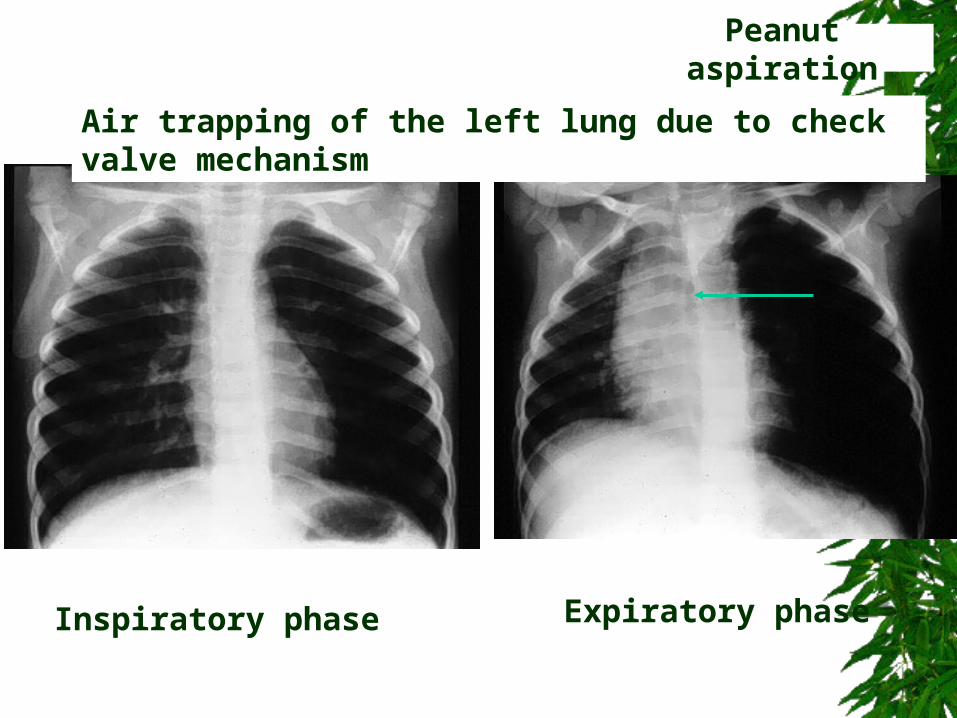
Inspiratory phase Expiratory phase
Air trapping of the left lung due to check valve mechanism
Peanut aspiration
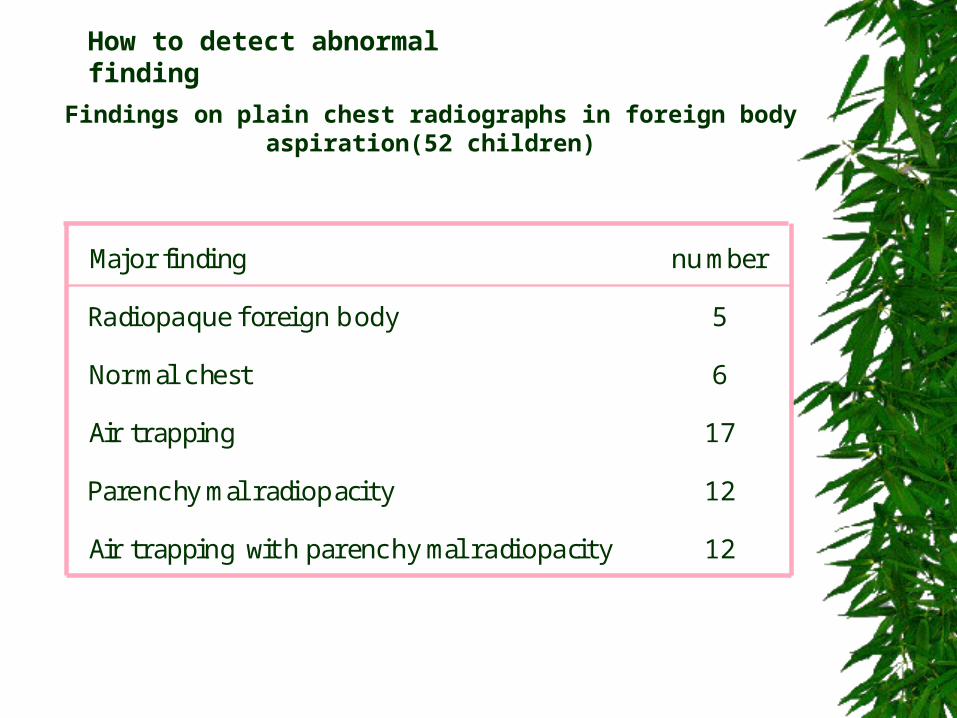
How to detect abnormal finding
Major findin number
Radiopaque foreign body 5
Normal chest 6
Air trapping 17
Parenchymal radiopacity 12
Air trapping with parenchymal radiopacity 12
g
Findings on plain chest radiographs in foreign body aspiration(52 children)
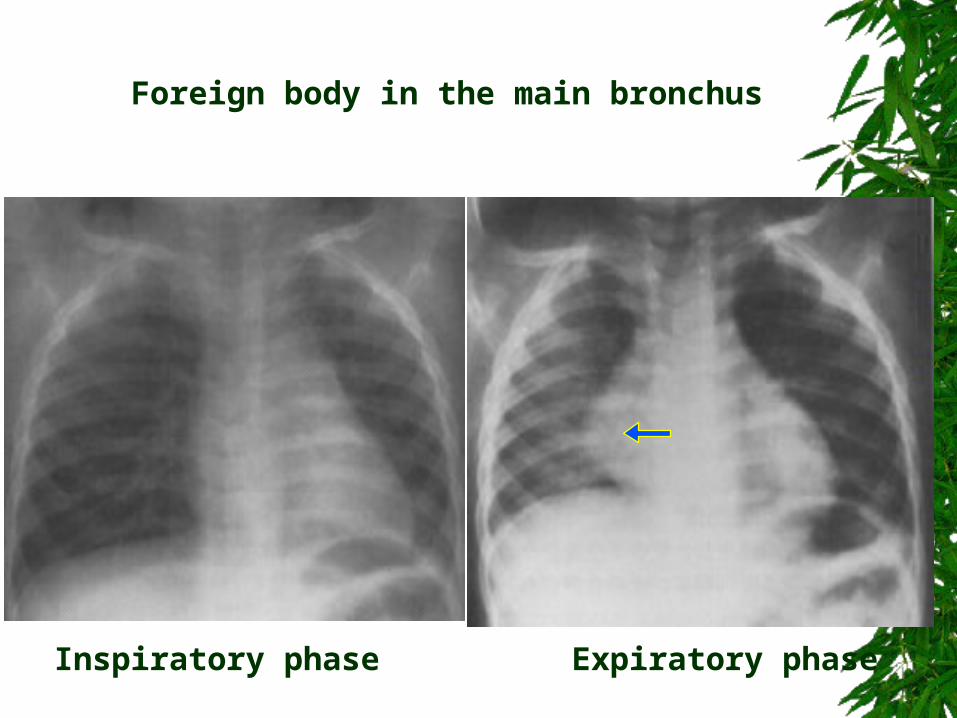
Inspiratory phase Expiratory phase
Foreign body in the main bronchus
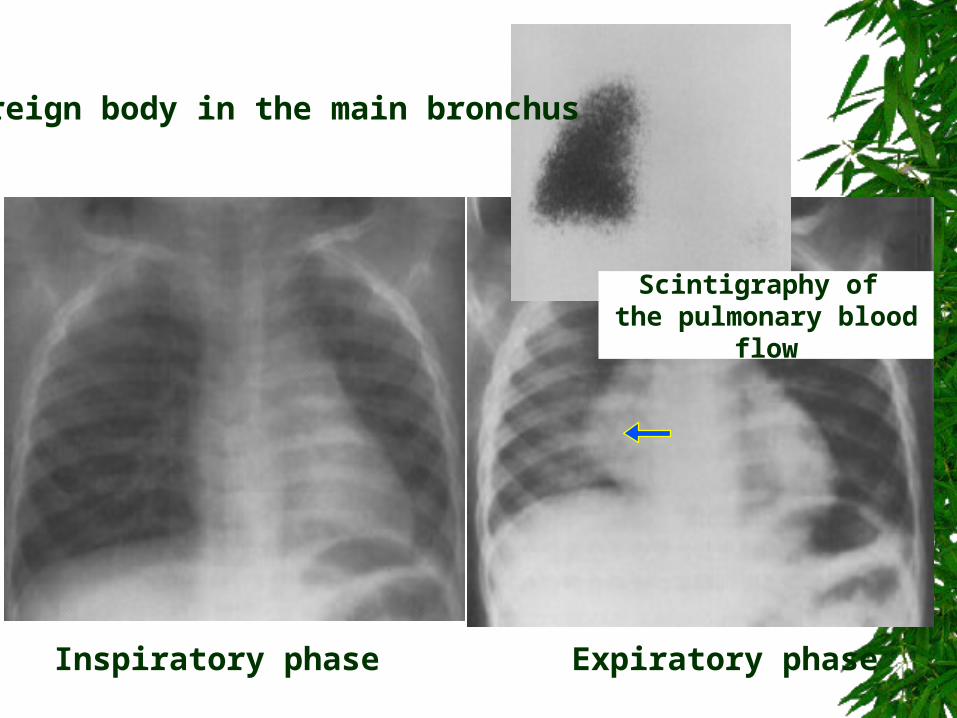
Foreign body in the main bronchus
Inspiratory phase Expiratory phase
Scintigraphy of the pulmonary blood flow
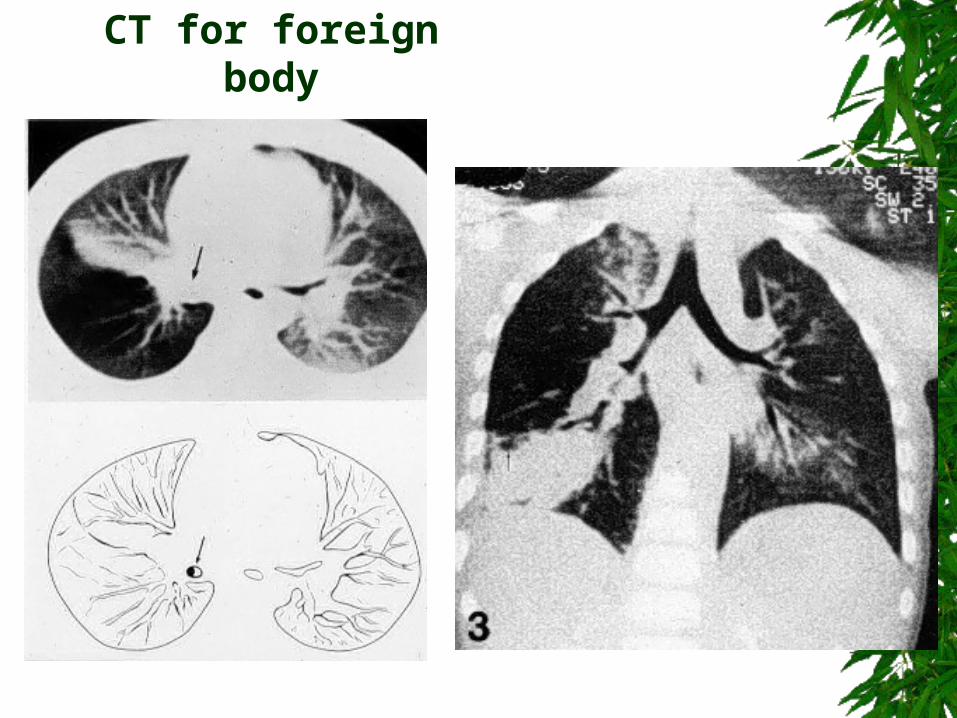
CT for foreign body
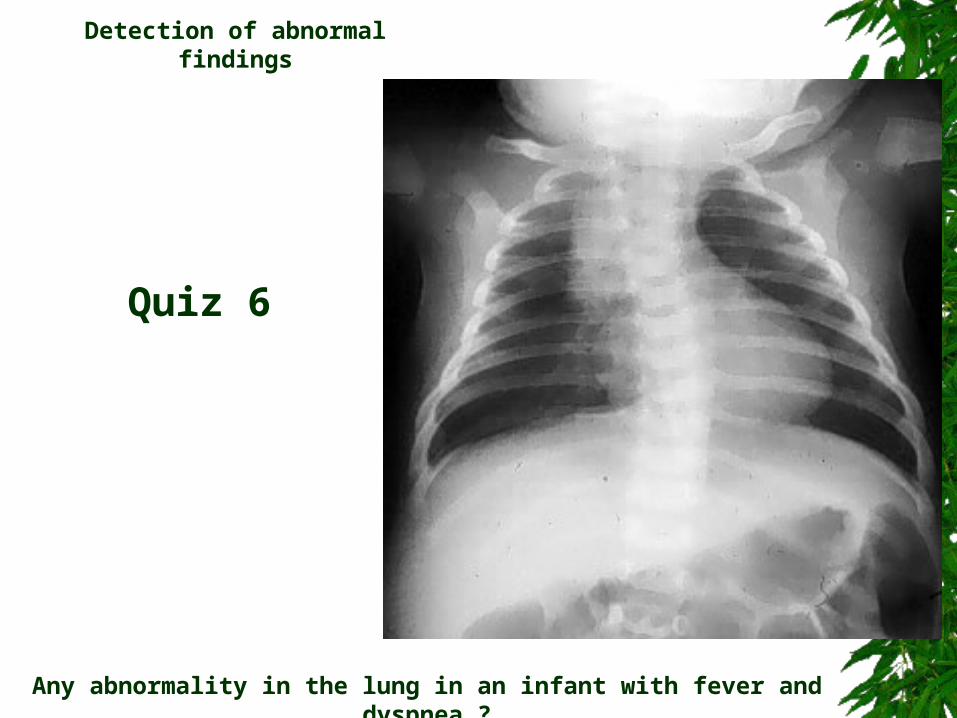
Any abnormality in the lung in an infant with fever and dyspnea ?
Detection of abnormal findings
Quiz 6
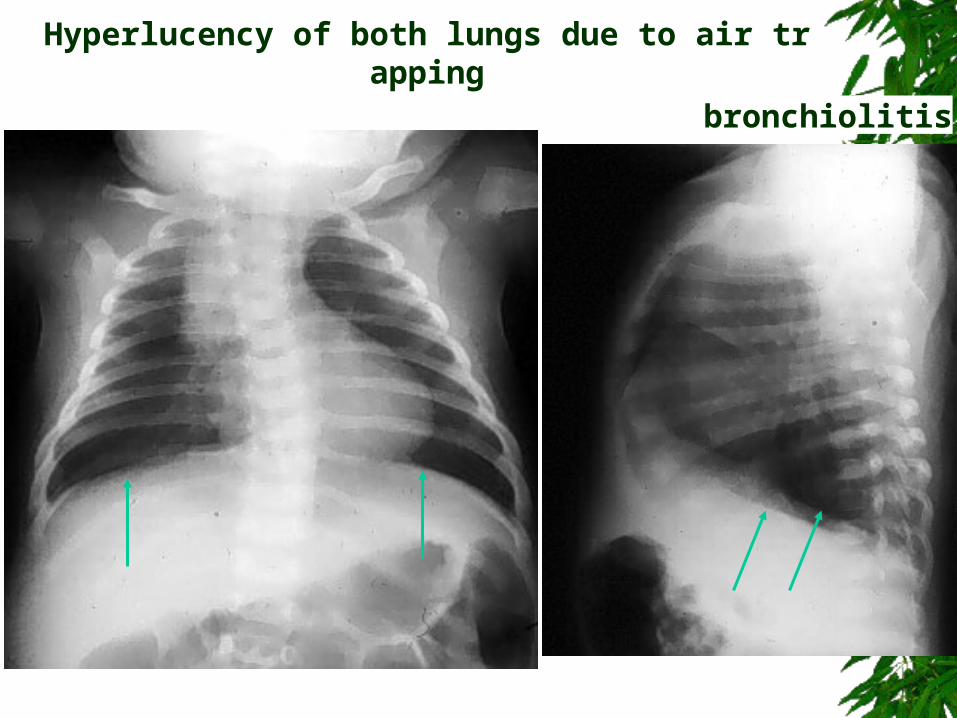
bronchiolitis
Hyperlucency of both lungs due to air trapping
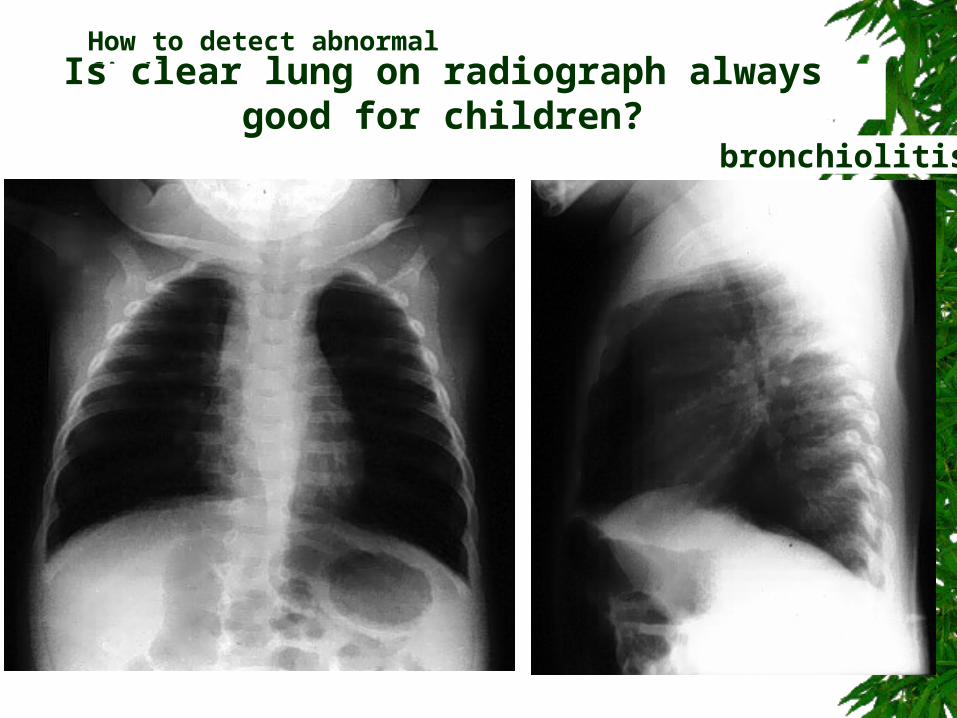
bronchiolitis
How to detect abnormal finding
Is clear lung on radiograph always good for children?
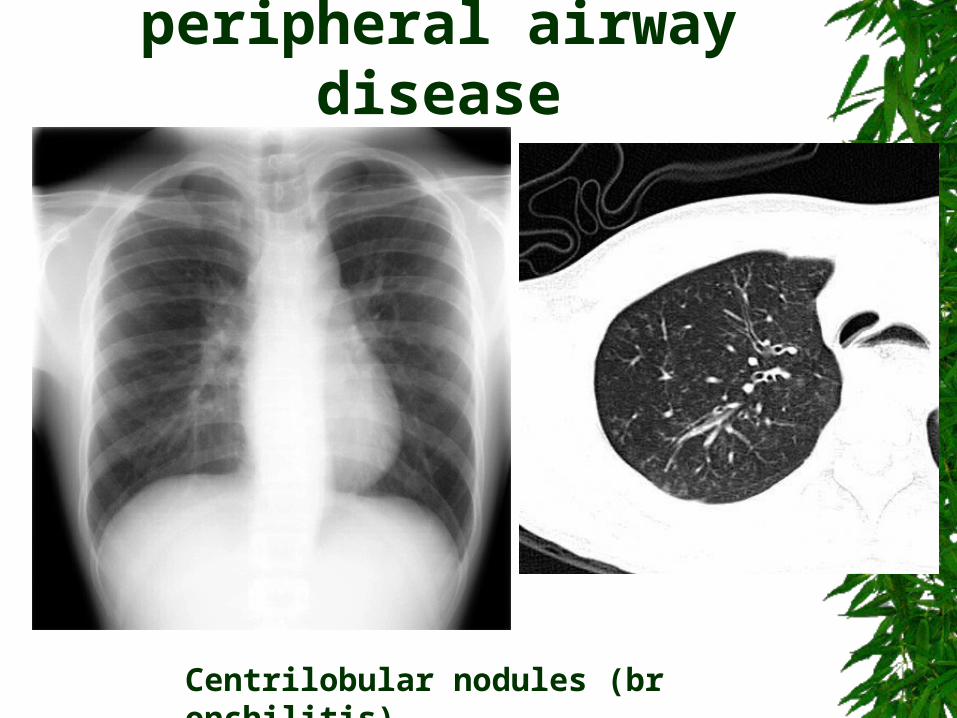
peripheral airway disease
Centrilobular nodules (bronchilitis)
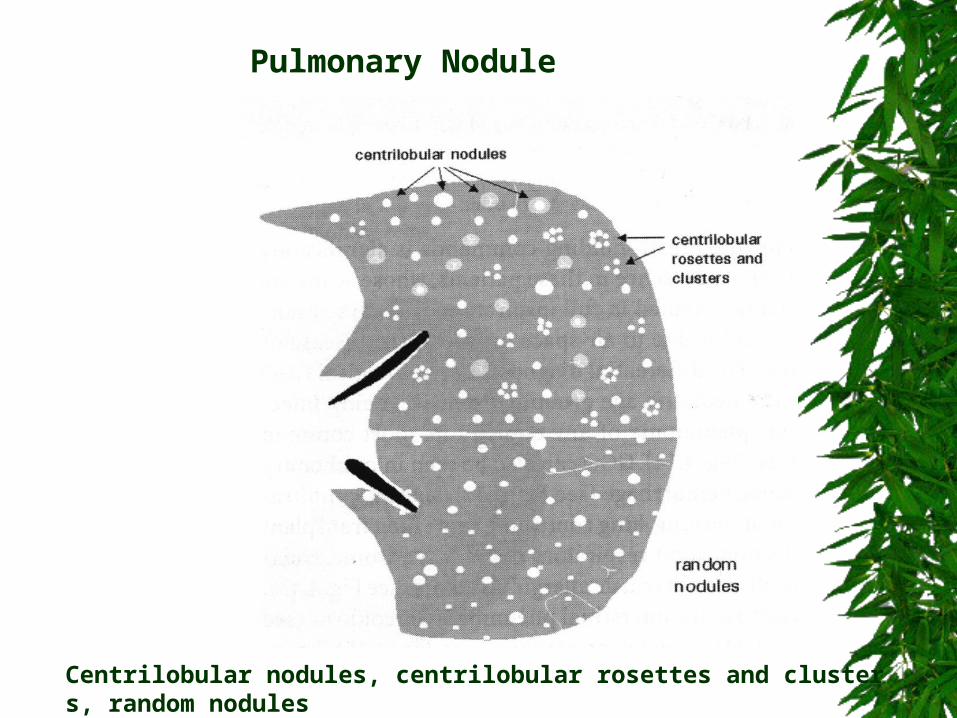
Centrilobular nodules, centrilobular rosettes and clusters, random nodules
Pulmonary Nodule
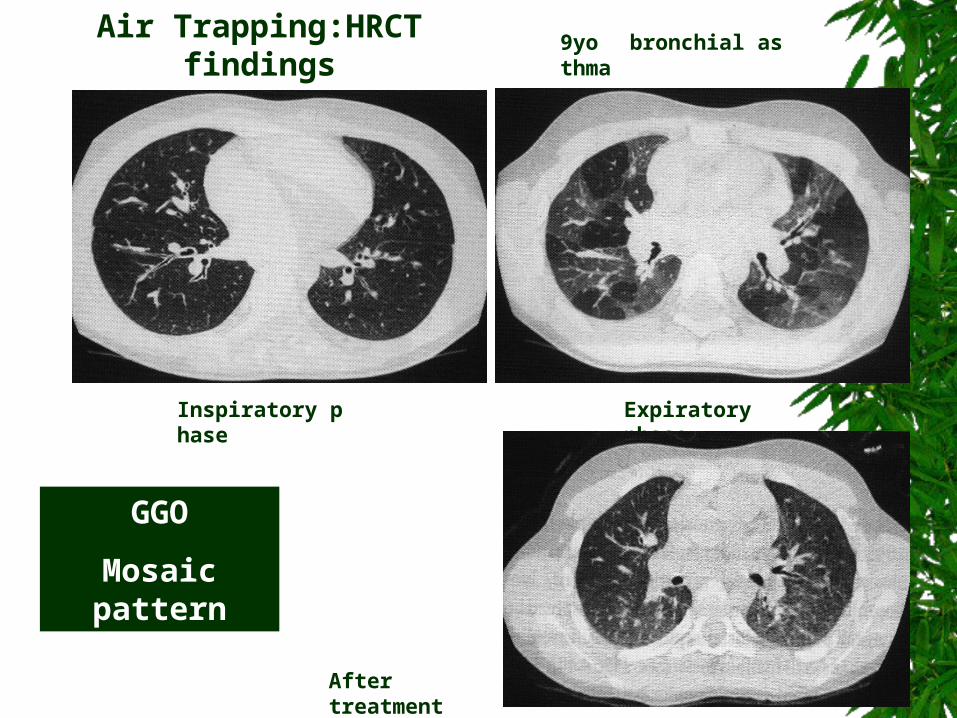
9yo bronchial asthma
Inspiratory phase Expiratory phase
After treatment
Air Trapping:HRCT findings
GGO
Mosaic pattern
Equipment : wider latitude film-screen system, computed radiography(CR) flat panel digital radiography(DR)
Technical factors : high kV, Bucky film
Additional views : lateral view decubitus view, plain abdomen ultrasonography, CT
How to improve the detectablity of the lesions hidden by the central shadow or diaphragmatic domes ?
Reading : silhouette sign, posterior mediastinal lines
Limitaion : ground glass opacity(GGO) peripheral lesions adjacent to the pleura, thin atelectasis perpendicular to the X-ray beam
How to improve the detectablity of the lesions hidden by the central shadow or diaphragmatic domes
Reading : silhouette sign, posterior mediastinal lines
Limitaion : ground glass opacity(GGO) peripheral lesions adjacent to the pleura, thin atelectasis perpendicular to the X-ray beam
CT(HRCT) may easily provide final answer but the indication should be limited only by clinical reasons not merely by radiological reasons!!!!
How to improve the detectablity of the lesions hidden by the central shadow or diaphragmatic domes
1 To make a list of diseases or conditions as many as possible in each category
2 To exclude a specific disease or condition one by one from the list
3 To leave those not to be excluded by former process
Differential diagnosis
Incorrect diagnosis may be lead when the correct diagnosis is not included from beginning
1. Technical
2. Normal
3. Congenital
4. Inflammatory
5. Neoplastic
6. Traumatic or Iatrogenic
Categories to be checked
Differential diagnosis
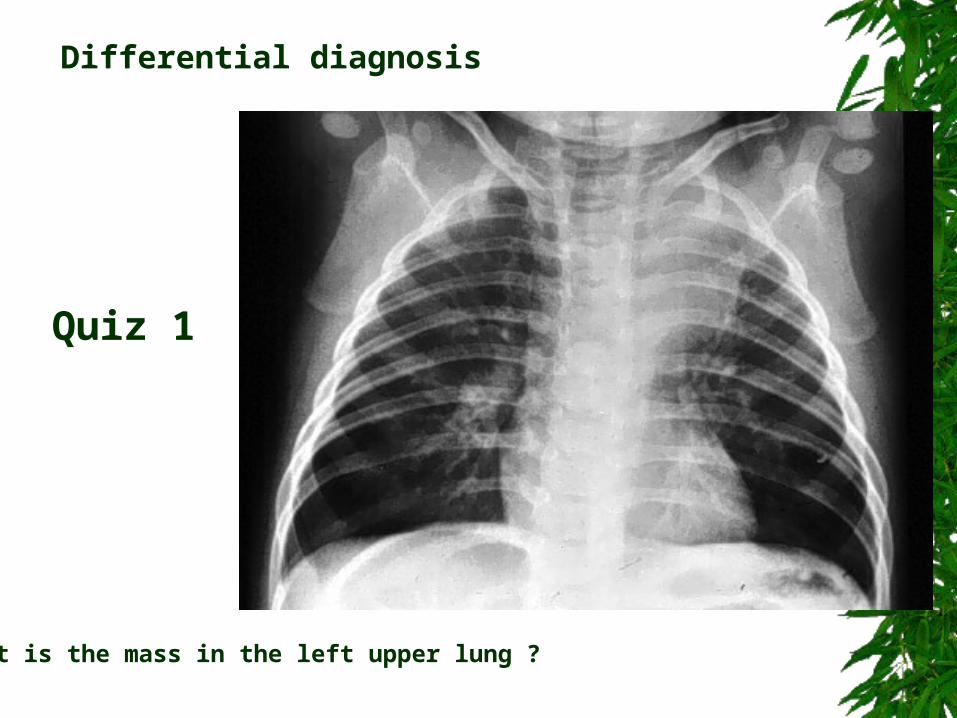
What is the mass in the left upper lung ?
Differential diagnosis
Quiz 1
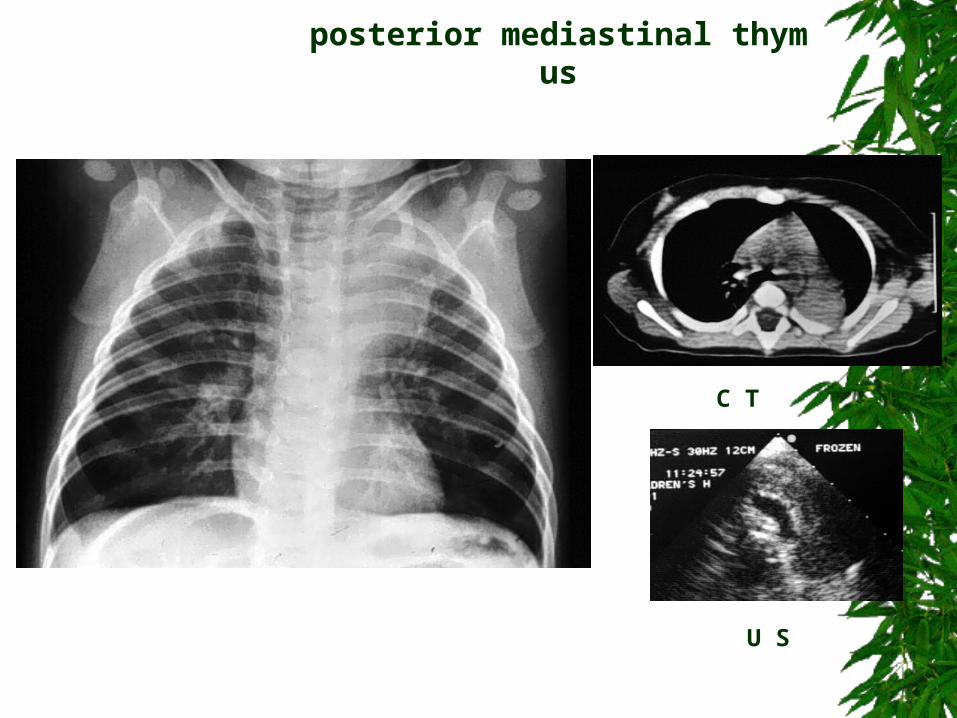
C T
U S
posterior mediastinal thymus
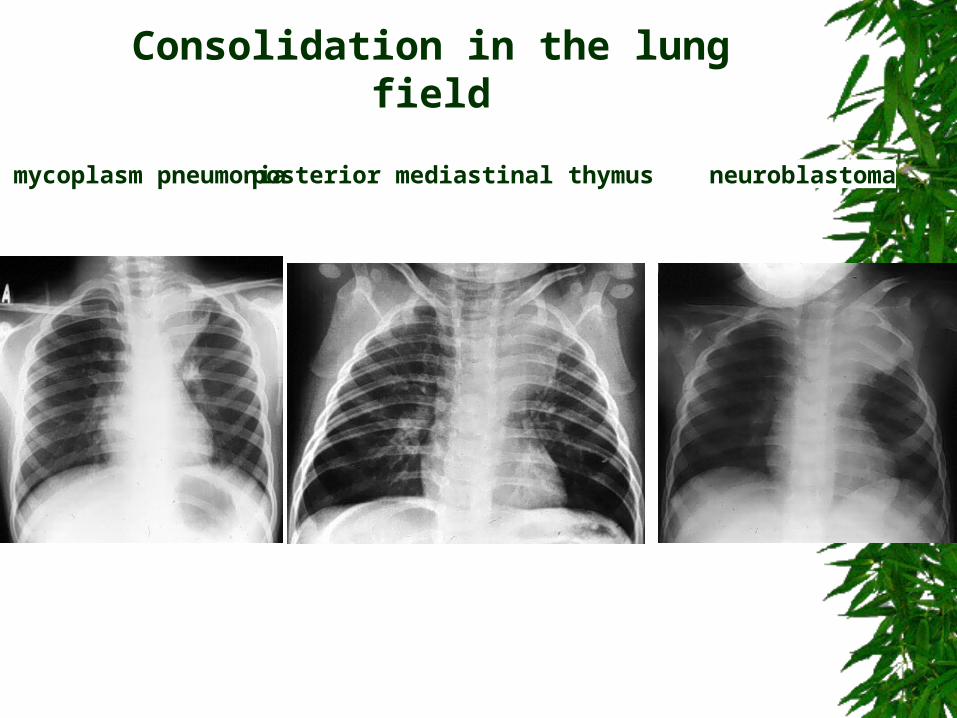
neuroblastomaposterior mediastinal thymusmycoplasm pneumonia
Consolidation in the lung field
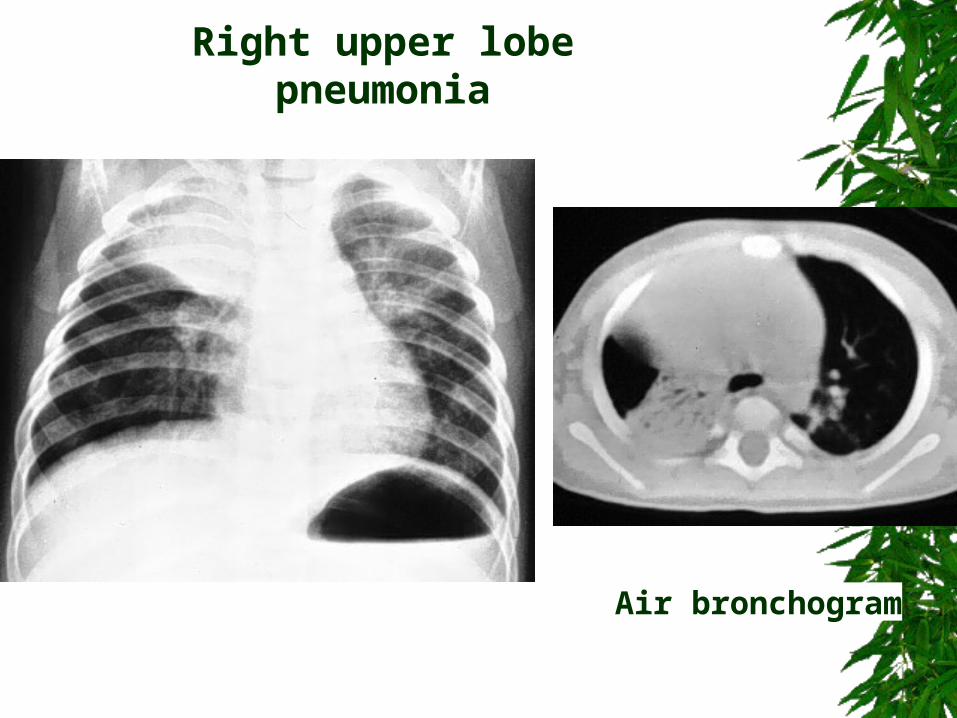
Air bronchogram
Right upper lobe pneumonia
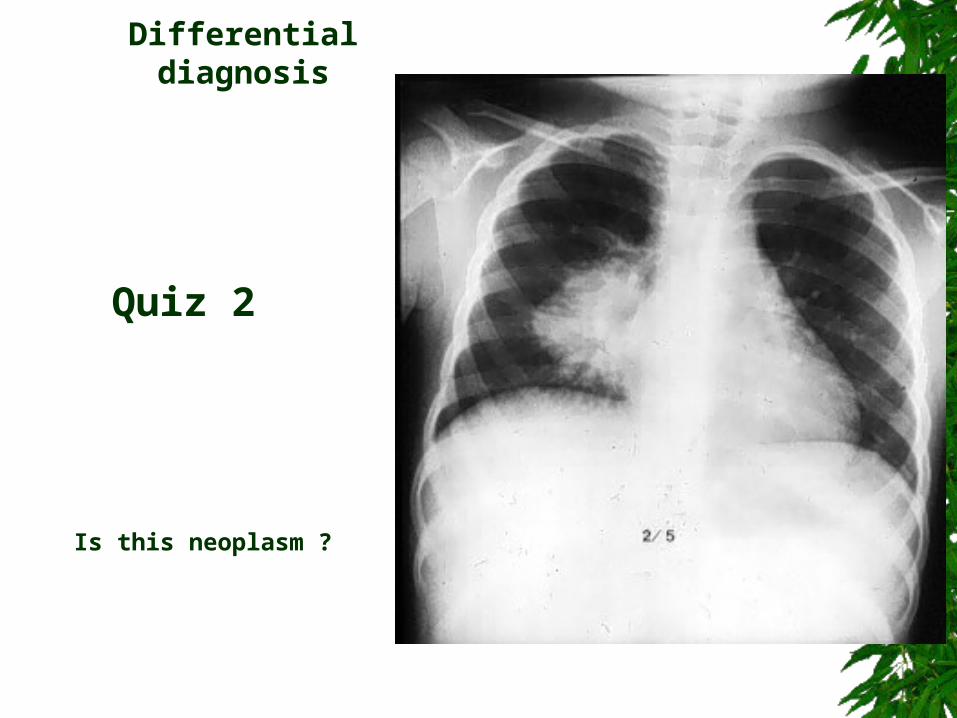
Is this neoplasm ?
Differential diagnosis
Quiz 2
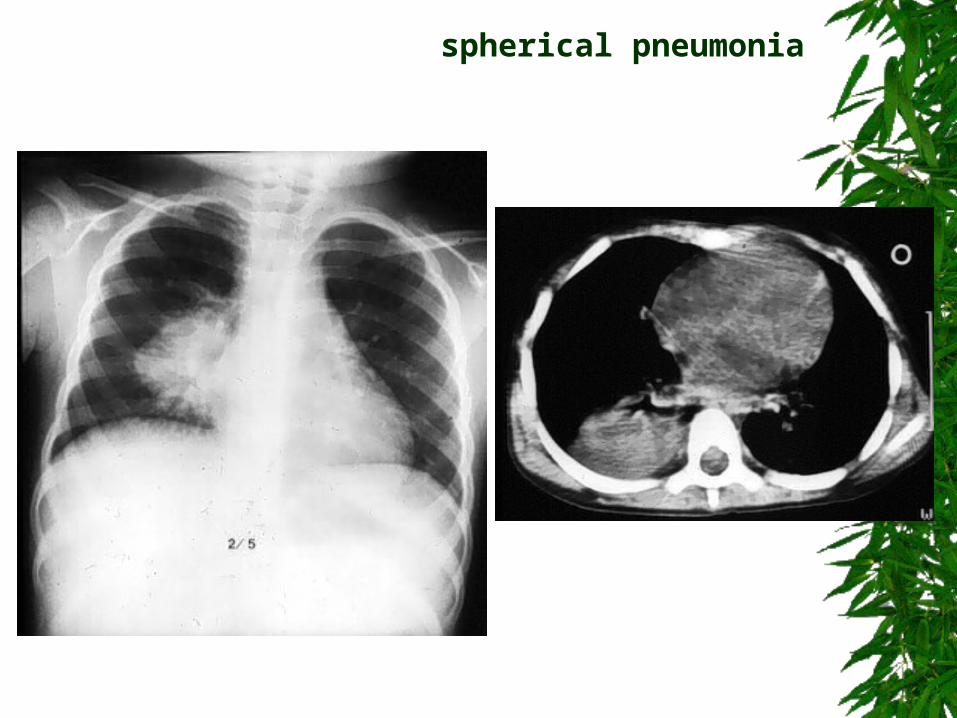
spherical pneumonia
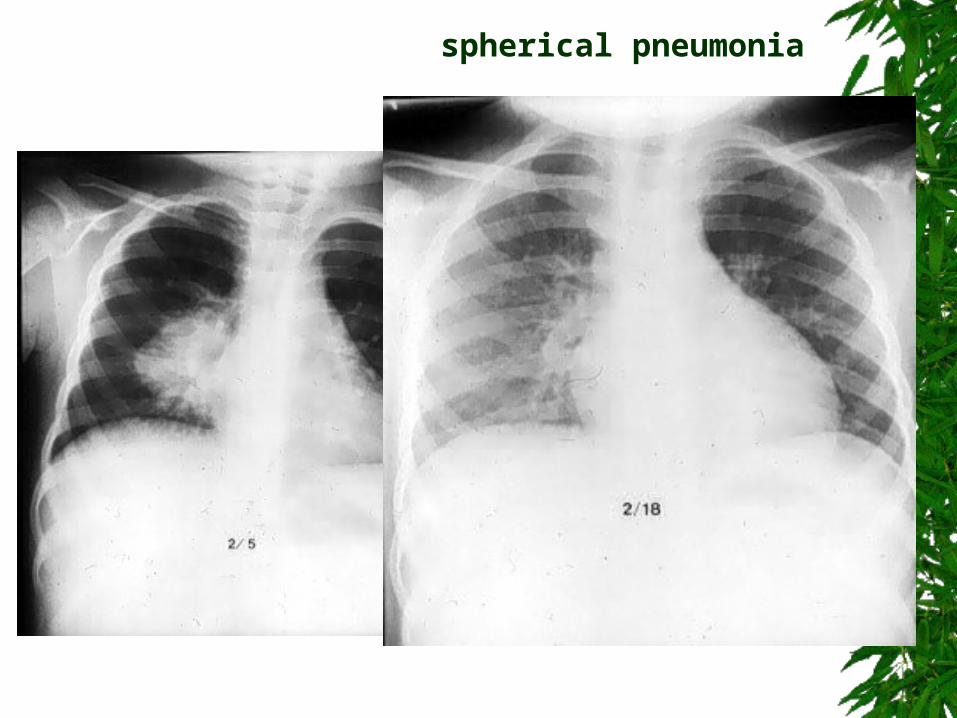
spherical pneumonia
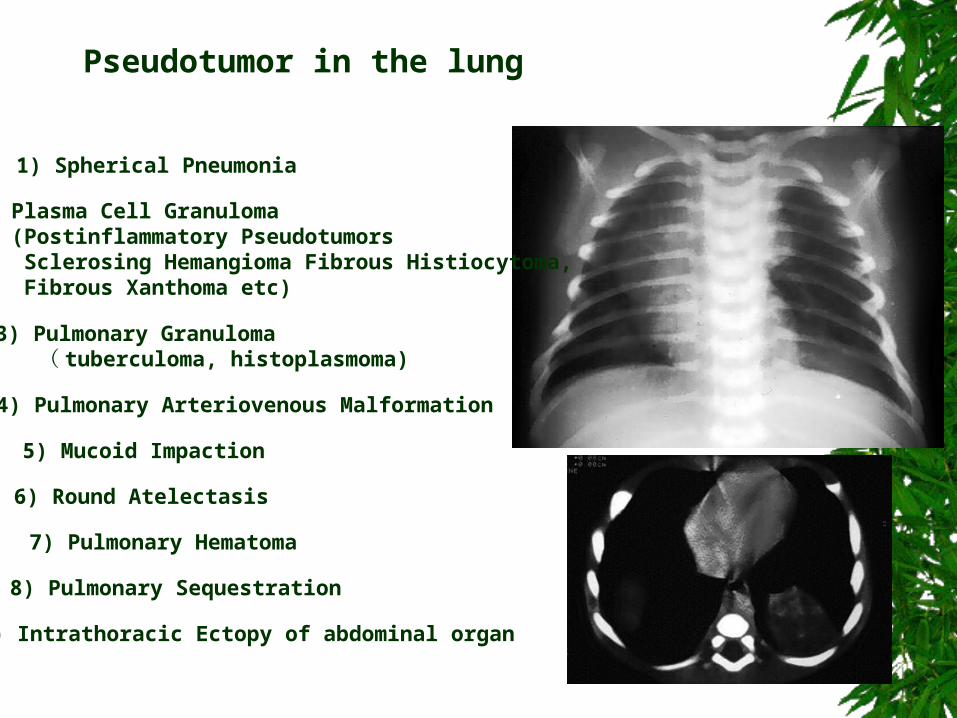
1) Spherical Pneumonia
2) Plasma Cell Granuloma (Postinflammatory Pseudotumors Sclerosing Hemangioma Fibrous Histiocytoma, Fibrous Xanthoma etc)
3) Pulmonary Granuloma ( tuberculoma, histoplasmoma)
4) Pulmonary Arteriovenous Malformation
5) Mucoid Impaction
6) Round Atelectasis
7) Pulmonary Hematoma
8) Pulmonary Sequestration
9) Intrathoracic Ectopy of abdominal organ
Pseudotumor in the lung
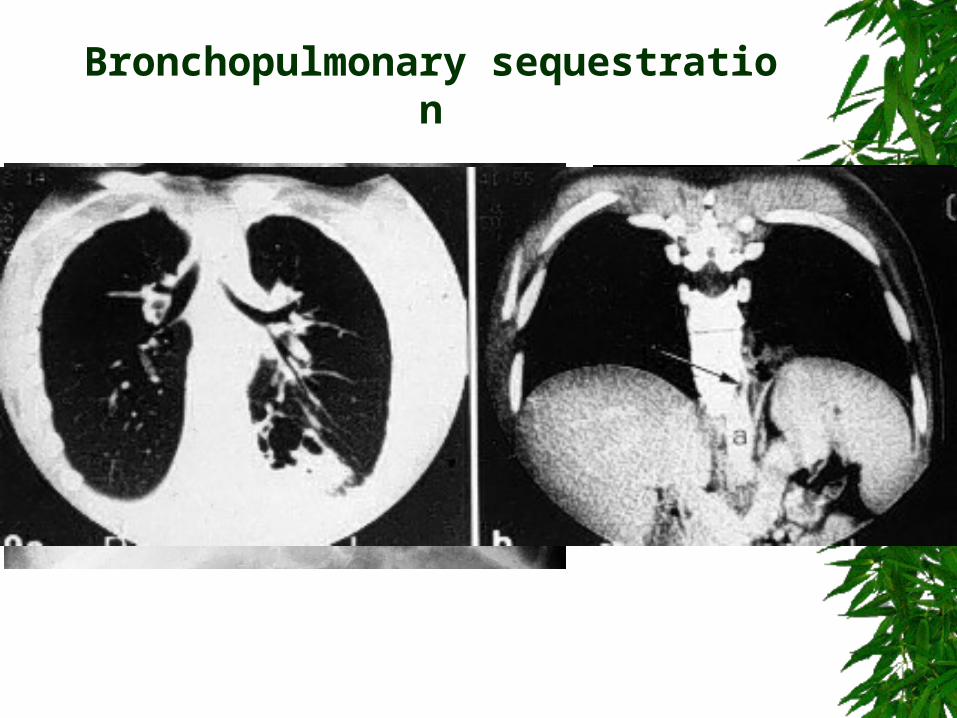
Bronchopulmonary sequestration
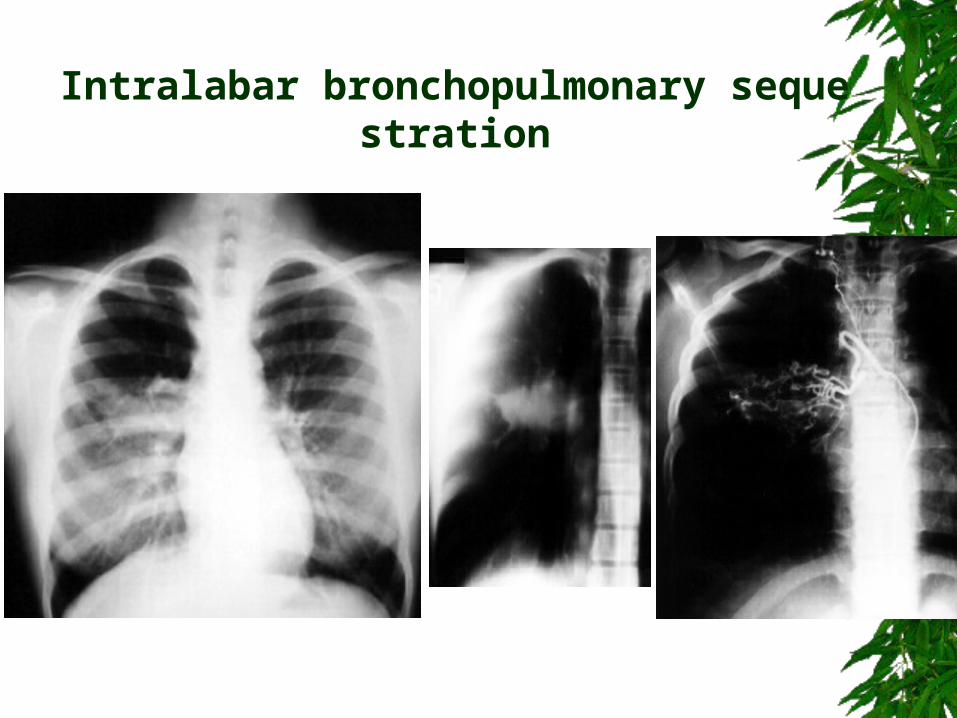
Intralabar bronchopulmonary sequestration
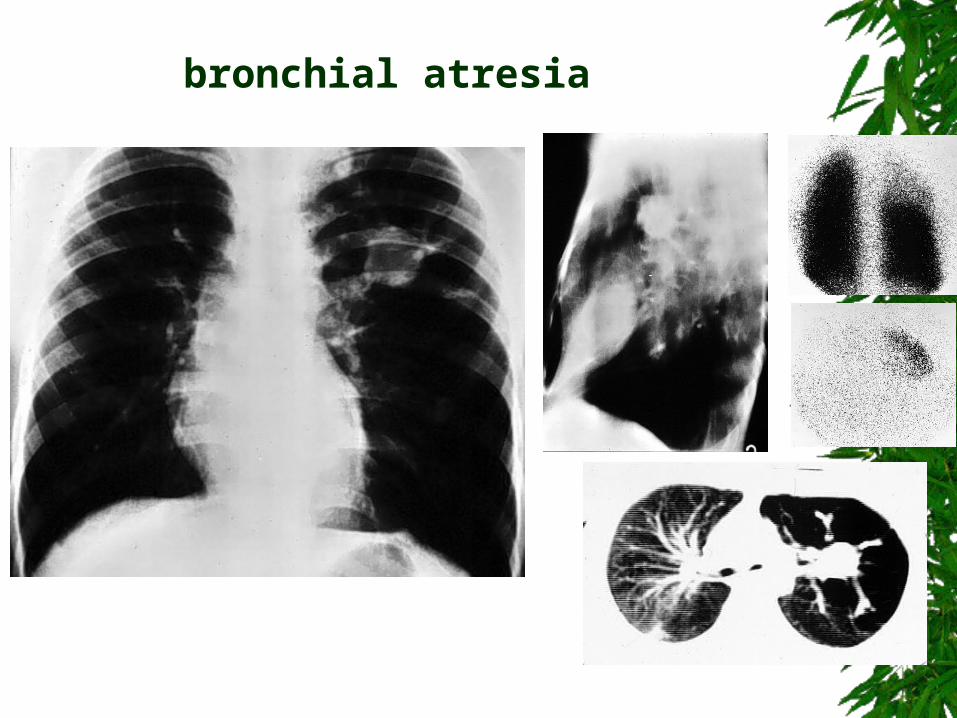
bronchial atresia
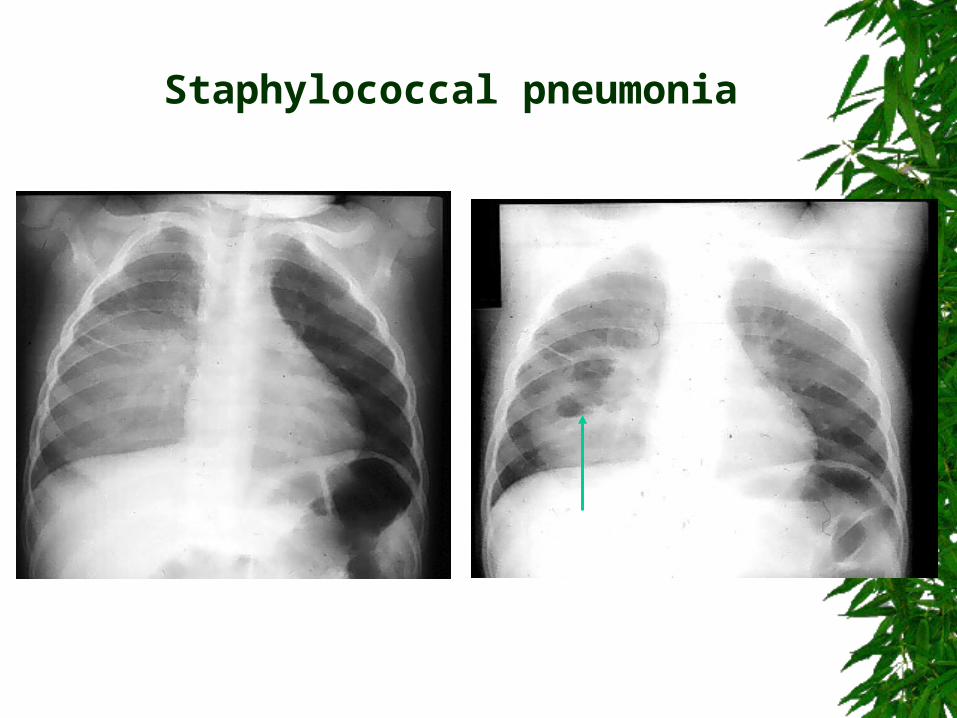
Staphylococcal pneumonia
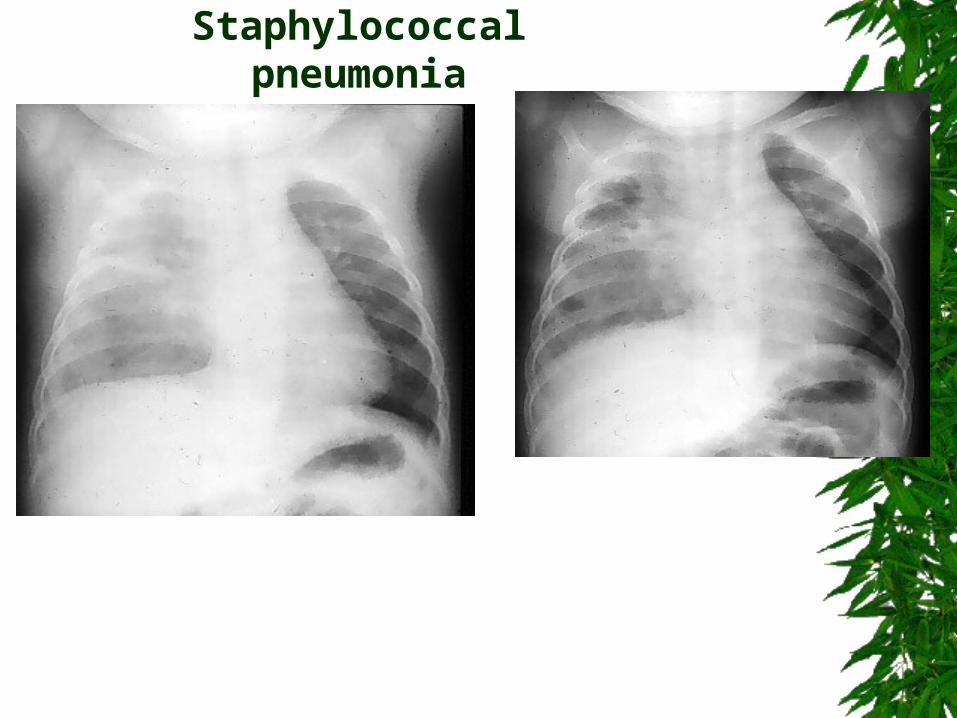
Staphylococcal pneumonia
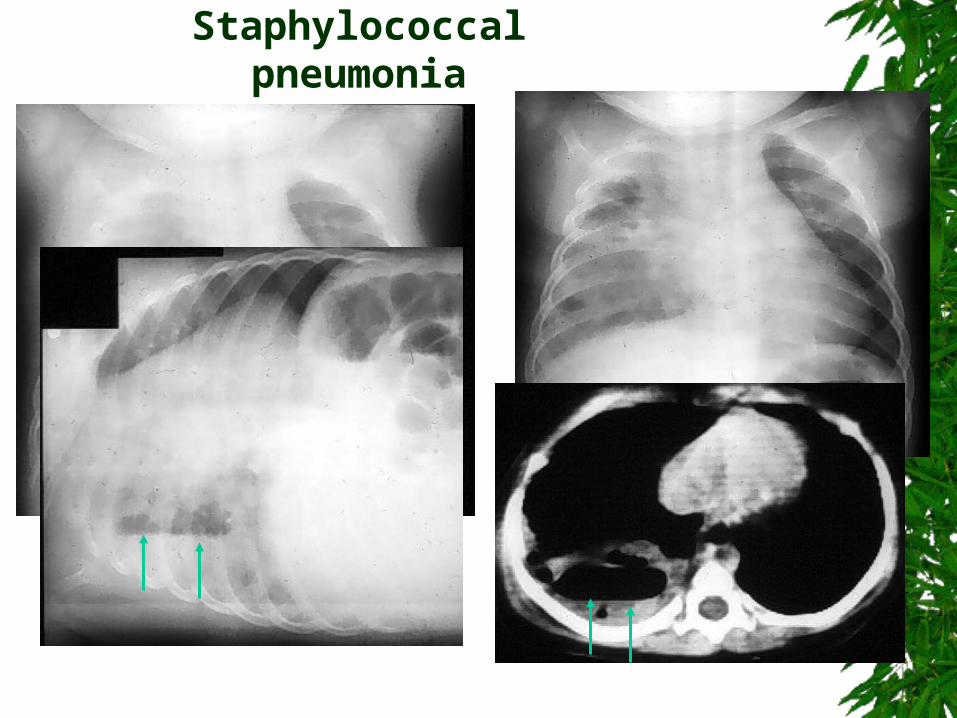
Staphylococcal pneumonia
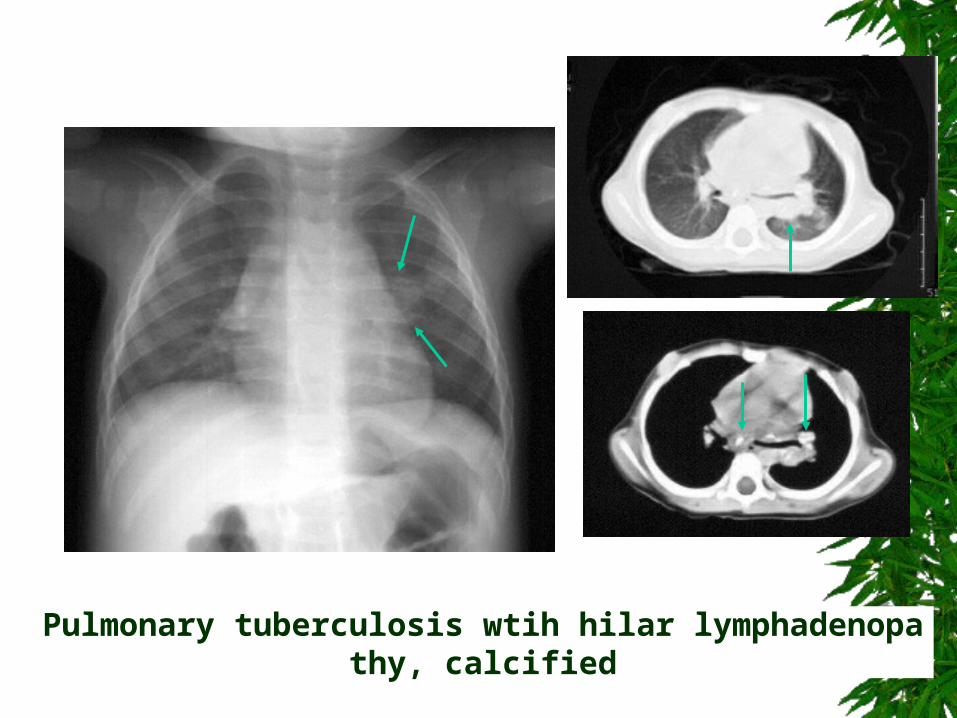
Pulmonary tuberculosis wtih hilar lymphadenopathy, calcified

Primary tuberculosis with calcified lymphnodes
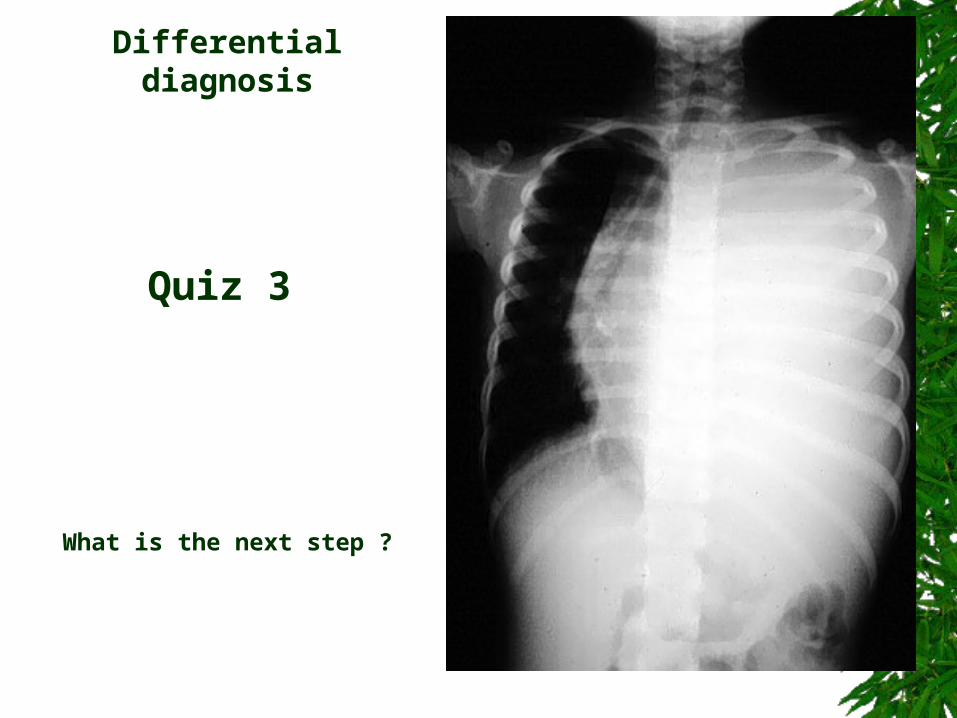
What is the next step ?
Differential diagnosis
Quiz 3
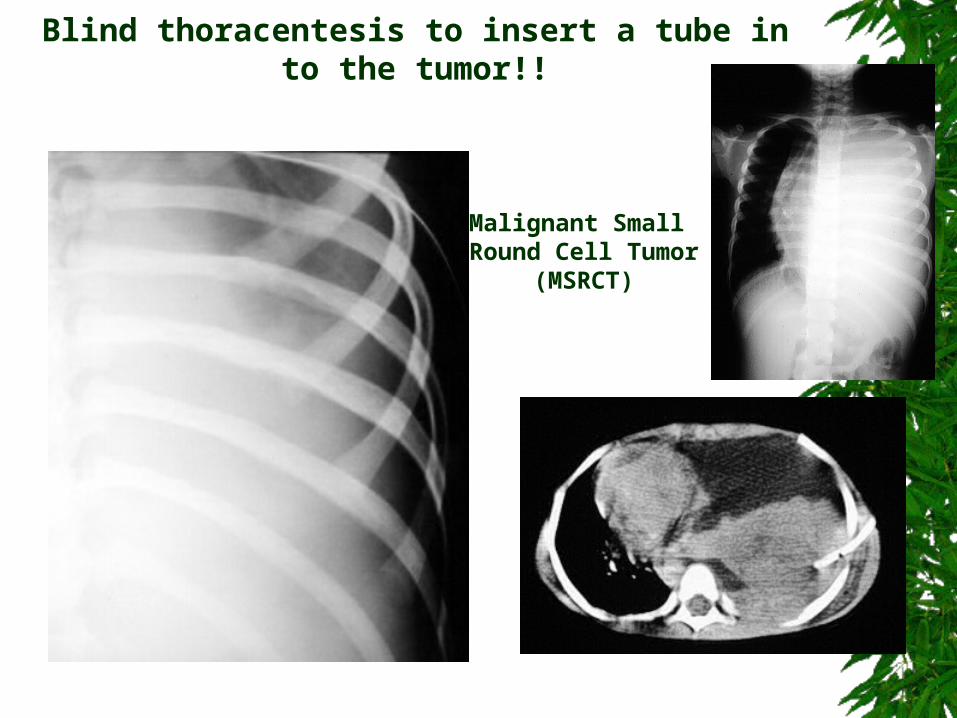
Malignant Small Round Cell Tumor
(MSRCT)
Blind thoracentesis to insert a tube into the tumor!!
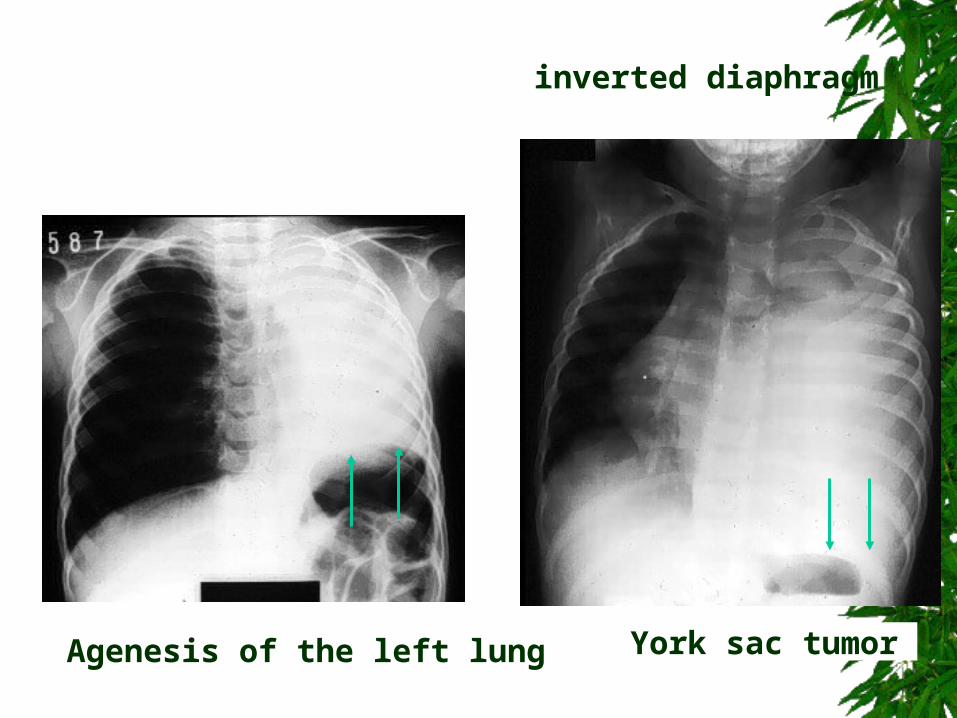
York sac tumor Agenesis of the left lung
inverted diaphragm
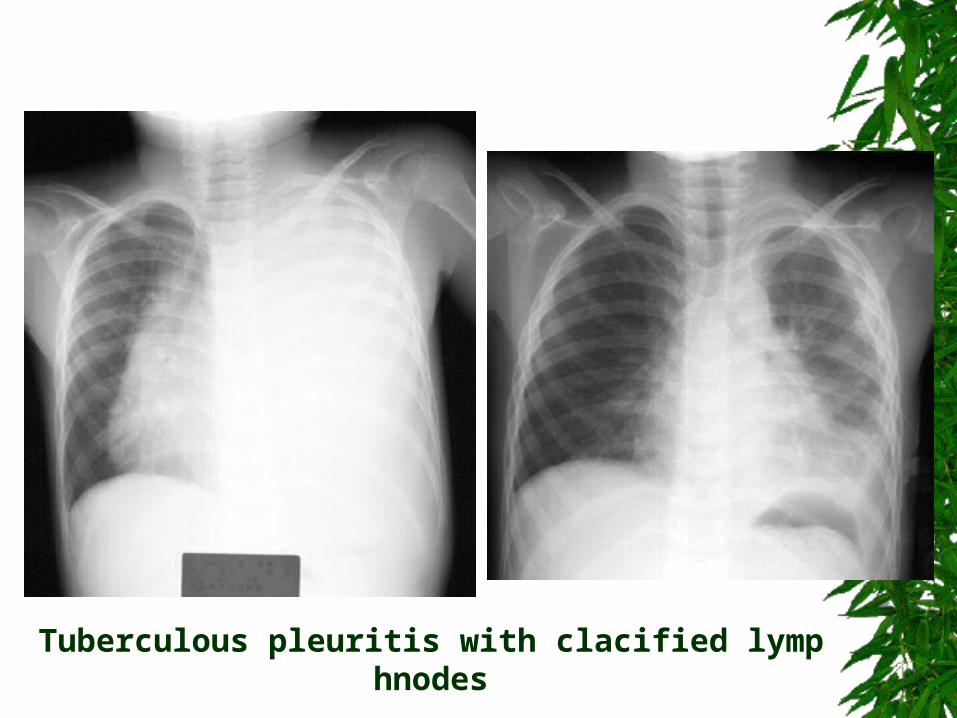
Tuberculous pleuritis with clacified lymphnodes
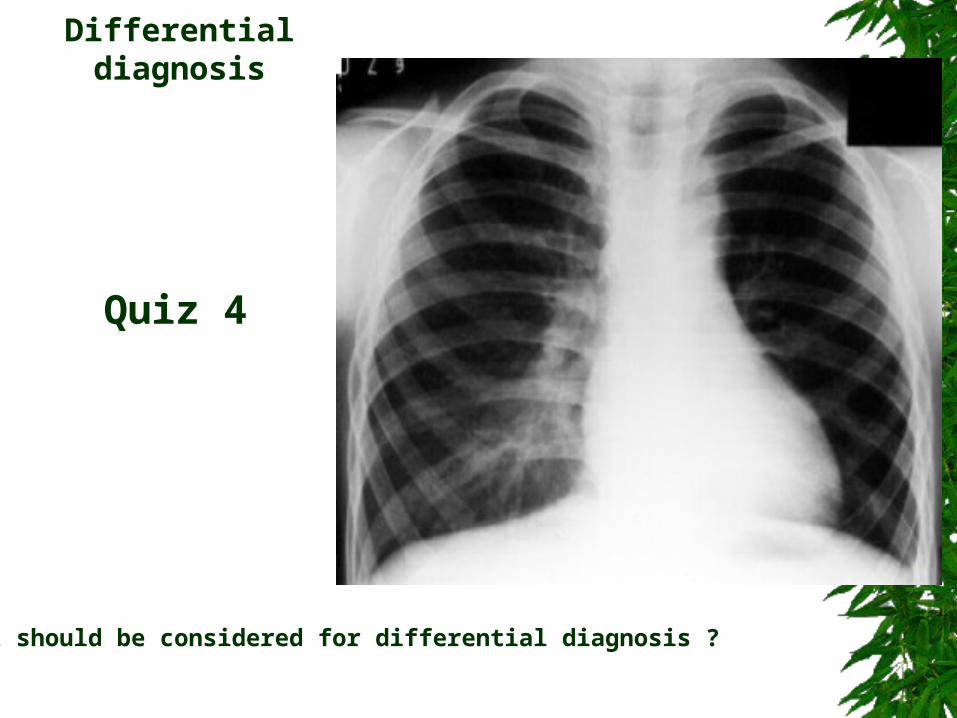
What should be considered for differential diagnosis ?
Differential diagnosis
Quiz 4
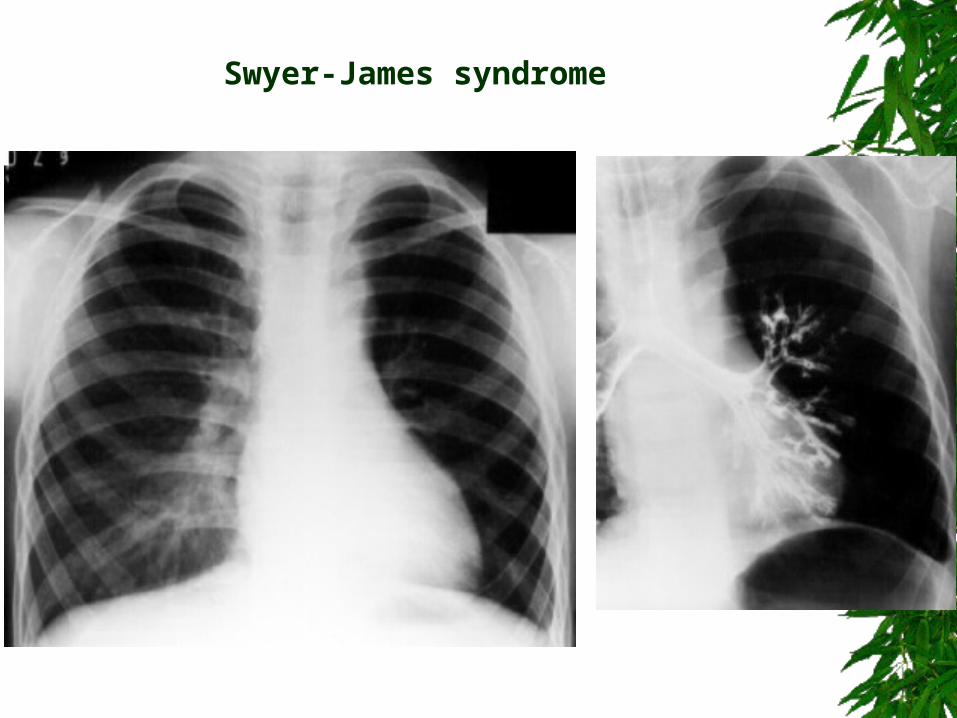
Swyer-James syndrome
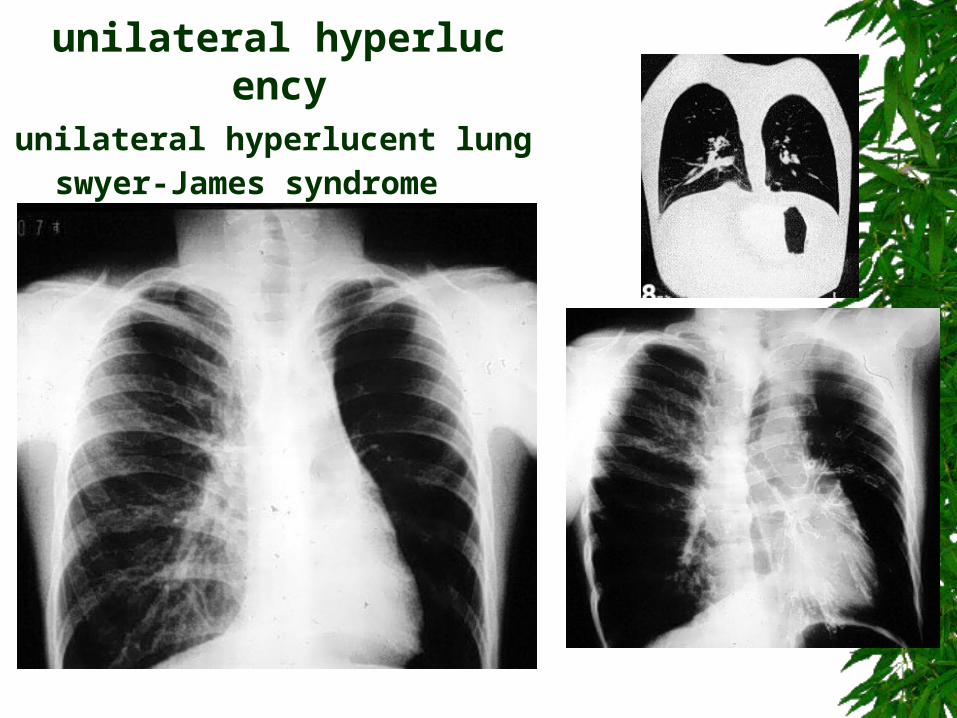
unilateral hyperlucent lungswyer-James syndrome
unilateral hyperlucency
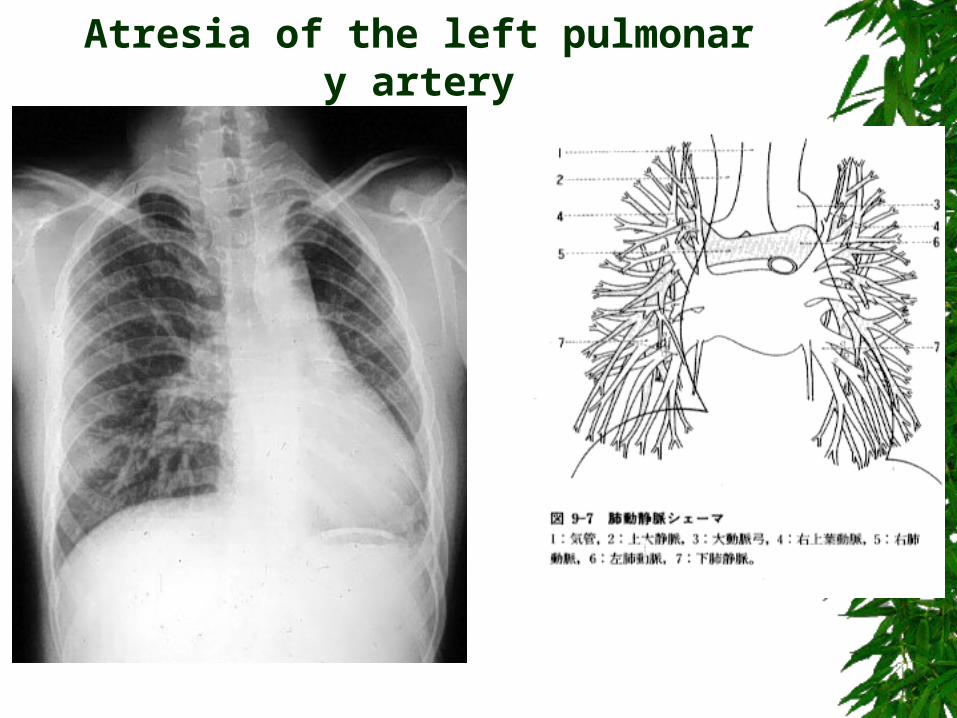
Atresia of the left pulmonary artery
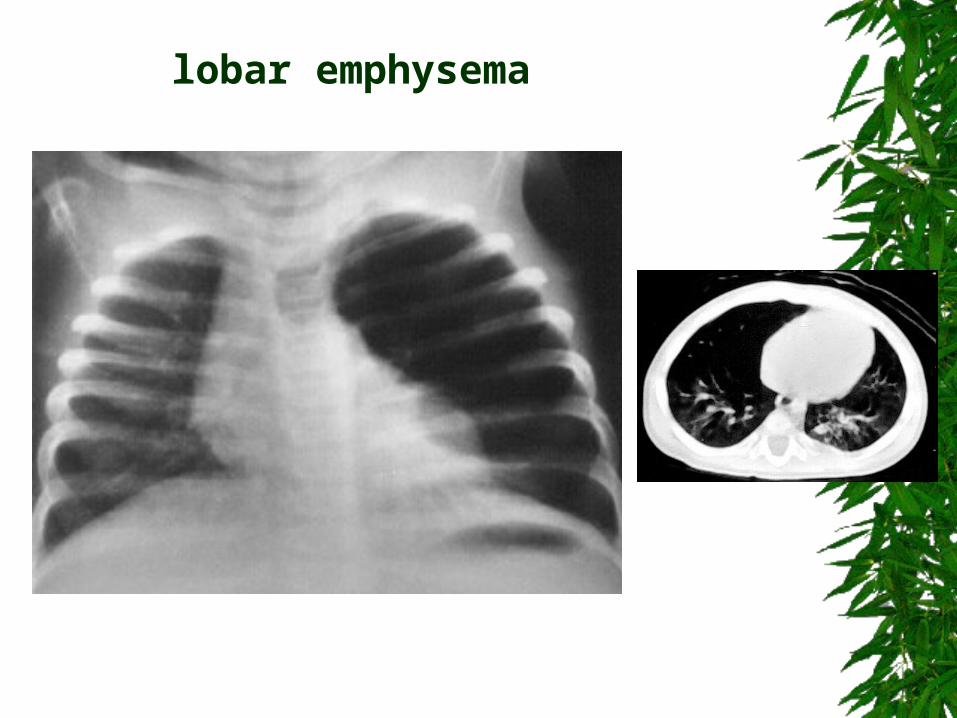
lobar emphysema
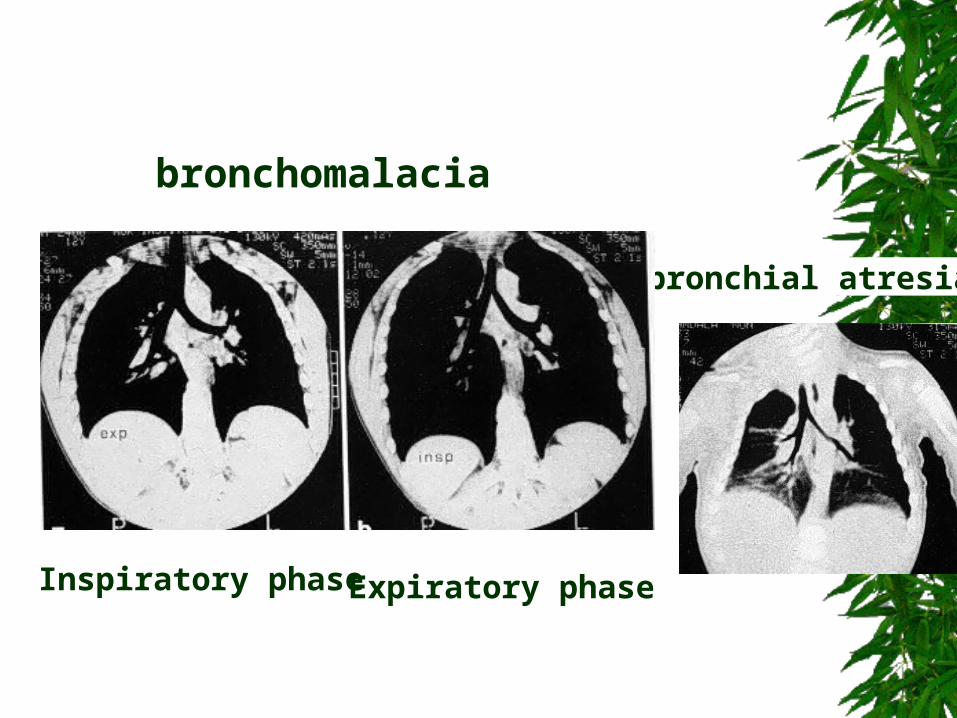
bronchial atresia
Inspiratory phase Expiratory phase
bronchomalacia
1. Technical
2. Normal
3. Congenital
4. Inflammatory
5. Neoplastic
6. Traumatic or Iatrogenic
Check all categories below then you may certainly always reach correct diagnosis!!!
Conclusion
Thank you for your attention!