Embed Size (px)
Citation preview

ANATOMY AND PHYSIOLOGY OF FEMALE REPRODUCTIVE ORGANS
FOR BSc. NURSING STUDENTS, 2013G.C
By :Kihinetu .G
1

I. Anatomy of the female pelvis• Session objectives
By the end of this session, students will be able to
Define pelvis. List the functions of female pelvis Describe the bones, joints and ligaments
of the pelvis Demonstrate pelvic bones, joints and
ligaments.2

pelvis
• The part of the trunk inferoposterior to the abdomen.
• The area of transition between the trunk and the lower limbs.
• Part of the appendicular skeleton of the lower limb.
• The space or compartment surrounded by the pelvic girdle(bony pelvis).
3

Anatomy of the female pelvis
A knowledge of pelvic anatomy is a great importance to the students of midwifery, for during birth the fetus has to traverse the relatively unyielding ring which it forms on its passage from the uterus to the vulva.
The student should be competent enough to recognize a normal pelvis in order to recognize deviation from normal and to refer for better management.
4

Function of pelvis
Adapted for child bearing Allow movement of the body Permits the person to sit and stand Transmits the weight of the trunk to the legAffords protection to pelvic organs and a
lesser extent to the abdominal contents
5

Fun…..
• Provide attachment for the powerful muscles of locomotion and posture.
• Provide attachment for the erectile bodies of the external genitalia.
• Provide attachment for the muscles and membranes that assist in these functions by forming the pelvic floor and filling gaps that exist in or around it.
6

The bones of the pelvis
It is composed of four bones Two innominate or hip bones One sacrum One coccyx
Each innominate bone is formed by fusion of three bones
The ileum The ischium The pubic bone
The three bones fussed at acetabulum
7

Fig. Pelvic bones 8

The ilium
Is the large flared out part of the innominate bone Is made up of a relatively flat of bone above and part of
acetabulum below. the superior, fan-shaped part of the hip bone It has the following characteristics:
The external aspect is gently curved and has a roughened surface to which are attached the gluteal muscles of the buttock.
The greater part of the inner aspect is smooth and concave forming the iliac fosse.
The ridge which surmount these two surface is known as iliac crest, which serves for the attachment of the
muscles of the abdominal wall. 9

iliac crest
• The superior margin of ileum .• the fourth lumbar vertebra.• Used as a surface marking when
performing lumbar puncture.• Ends interiorly in a rounded anterior
superior iliac spine and posterior in a sharp posterior superior iliac spine.
10

The ilium…
Anteriorly the crest ends in the anterior superior iliac spine, a bony prominence which can be palpated under the skin.
Posteriorly iliac crest ends in the posterior superior iliac spine.
Below the anterior superior iliac spine is an other bony prominence the anterior inferior iliac spine, while posteriorly, there is posterior inferior iliac spine.
At its lower most part the ileum forms the upper two- fifths of the acetabulum, where it fuses with ischium and pubis.
11

The ilium…
Behind the acetabulum, the ileum forms the upper part of a large notch, the greater sciatic notch, through which pass the piriforms muscles and the nerves of the sacral plexus, on their way from the front of the sacrum in to the thigh.
On the inner aspect of the bone, the iliac fossa is bounded below by a prominent ridge, which is the iliac part of the ilio pectineal line.
Anteriorly the ilio pectineal line swells into a bony prominence, at the point where the ileum fuses with superior ramus of the pubis, to form the ilio-pectineal eminence.
Posterior to the ilio – pectineal line and above the greater sciatic notch, is a roughened area , where the ileum articulate with the sacrum to form the sacro -iliac joint. 12

The ischium
The lowest constituent bones of the innominate bone
Formed by the following parts;
The head forms the lowest two-fifths of the acetabulum, where it fuses with the ileum and pubis.
Below the acetabulum a thick buttress of bone pass down and terminates in ischial tuberosity the part which the weight of the body rest on when sitting.
Passing up wards and in ward from the ischial tuberosity a small
shaft of the ischium becomes continuous with the inferior ramus of the pubis so forming the public arch.
13

The ischium…
The ischium forms the lower boundary of the large foramen, the obturator foramen or foramen ovale.
On its internal aspect the ischium forms the side wall of the true pelvis.
Protruding in wards from its posterior edge, about 5cm above the tuberosity, is a conspicuous projection known as the ischial spine which is use to estimate the station of fetal head.
Lesser sciatic notch is situated between the ischial spine above and ischial tuberosity below.
14

The pubis
• The smallest of the three bones forming the innominate bone and form the lower one fifth of the acetabulum.
• The right and left pubic bones unite with each other anteriorly at the square shaped pubic bodies. They are fused by a pad of cartilage, the symphysis pubis.
• The upper surface of the body forms a crest, the pubic crest, which ends laterally in the pubic tubercle. 15

The pubis…
• Extending upwards from each pubic body, the superior ramus unites with ilium at ilio-pectineal eminence.
• Below the body of the pubic, the inferior ramus passes down wards and out wards to join the ischium, so forming the upper part of pubic arch
16

The sacrum
Is situated in the posterior part of the pelvis and consists of five fused sacral vertebrae.
The anterior surface is smooth, and is concave from above down wards and slightly so from side to side forming the hollow of the sacrum.
The sacral alae – are the widened out wings of bone on each side of the 1st sacral vertebra.
Promontory of the sacrum – is the center point of the upper border of the 1st sacral vertebrae which with the base of the 5th lumbar vertebra, protrudes over the hollow of the sacrum.
17

The sacrum…
Sacral canal – runs longitudinally through the center of the sacrum and opens at the level of the 5th sacral vertebra.
The posterior surface for the sacrum is rough and irregular and serves for the attachment of the ligaments and muscles of the back.
The sacrum articulates laterally with the ileum at sacroiliac joint and lower margin of it articulate with coccyx at sacro-coccygeal joint. 18

The coccyx
Consists of four fused coccygeal vertebrae. It is triangular in shape with its base uppermost. The 1st coccygeal vertebra articulates with lower
end of the sacrum at the sacro-coccygeal joint. The remaining three vertebrae mere rudimentary
nodules of bone; they are smooth in their inner surface where they support the rectum, while their lowest most tip are attached to the external anal sphincter and ano-coccygeal body.
19

20

Pelvic joints
There are four pelvic joints Two sacro-iliac jointsOne symphysis pubis One sacro-coccygeal joints
21

1. The sacro – Iliac joints
Are the strongest joint in the body. They join the sacrum to the ileum and thus
connect the spine to the pelvis. Their main features are;-The joint cavity is very small The articular surfaces are placed on the inner
surface of the ileum above the greater sciatic notch and on the lateral aspect of the sacrum, extending for the 1st two sacral vertebrae.
22

The sacro – Iliac joints…The supporting ligaments pass from the
sacrum and the fifth lumbar vertebrae to the ileum both anterior and posterior to the joint cavity.
Movements at these joints occur under normal conditions but are very slight. They increase in range during pregnancy and labor when the ligaments become softened under the influence of the hormone relaxin.
23

2. The symphysis pubis
• Is formed at the junction of the pubic bones which are united by a pad of cartilages.
• It is reinforced by supporting ligaments which pass from one pubic bone to the other in front, behind, above and below the disc of cartilage.
24

3. The sacro- coccygeal joint
• Is situated between the lower border of the sacrum and the upper border of the coccyx.
• Slight back ward and forward movement of the coccyx on the lower end of the sacrum occur normally; the back ward movement is greatly increased during labor at the time of the actual birth of the head.
25

The pelvic ligaments
Each of the pelvic joints held together by
ligaments • These are:pubic ligaments sacro-iliac ligament sacro-coccygeal ligaments
26

The pelvic ligaments…
Sacro- tuberous ligaments – is a strong ligament passing from the posterior superior iliac spine and lateral borders of the sacrum and coccyx to the ischial tuberosity. It bridges across the greater and lesser sciatic notches
The sacro- spinous ligament - passes from the side of the sacrum and coccyx across the greater sciatic notch to the ischial spine. It lies in front of the sacro- tuberous ligament. 27

The pelvic ligaments…
The inguinal ligament (pauper’s ligament )-runs from the anterior superior iliac spine to the pubic tubercle forming the groin.
• The sacro- tuberous ligament and sacro- spinous ligaments cross the sciatic notch and form the posterior wall of the pelvic out let.
28

29

30

The regions of the pelvis
The brim of the pelvis divides the pelvis into two parts, the false and true pelvis .
The false pelvis – lies above the pelvic brim and consists mainly of the iliac fosse.
It has little importance in midwifery. The true pelvis – included the pelvic brim and all
the area that lies below- It consists of three constituent parts;
The in let or brim of the pelvis The cavity The out let
31

The pelvic brim
Is round except where the sacral promontory projects in to it.
It appears heart – shaped because of sutting sacral prominence. It is wider transversely than in the anterior-posterior dimension.
It is marked by 8 fixed land marks 1. The promontory of the sacrum 2. The alae of the sacrum 3. The sacro- iliac joint 4. Ilio - pectineal line -(which is the edge formed at the inward
aspect of the ilium)
32

The pelvic brim…
5. Ilion- pectineal eminence-(the superior ramus of the pubic bone meets the ilium)
6. Inner border of the superior ramus of pubic bone.
7. Upper inner border of the body of pubic bone
8. upper inner border of symphysis pubis
33

The pelvic cavityExtends from the in let above to the out let below. Formed by the hollow of the sacrum.
The posterior wall is deeply concave and approximately 12cm in length.
The anterior wall is formed by symphysis pubis and is approximately 4cm long.
The lateral walls comprise the greater sciatic notch, the internal surface of a small portion of the ileum, the body of the ischium and the foramen ovale.
34

The pelvic cavity…
• The plane of the cavity of the pelvis – is an imaginary surface which extends from the mid point of the symphysis pubis in front to the junction of the 2nd and 3rd sacral vertebrae.
• Ischial spine marks the mid plane of the pelvis
35

The pelvic out letTwo out let of the pelvis are described - the
anatomical and the obstetrical. i) The anatomical out let It is diamond in shape . Is formed by the structures which mark the lower
border of the pelvis- these are: The lower border of the symphysis pubis The pubic arch The inner border of the ischial tuberosity. The sacro – tuberous ligament The tip of the coccyx.
36

The pelvic out let…ii) The obstetrical out let – is the constricted lower
portion of the pelvis and not merely its lower bony border.
• It is the segment of the f the pelvis which lies between the anatomical outlet below and an artificial line above.
• Its land marks are:- The lower border of the symphysis pubis The ischial spine The sacro-spinous ligament The lower border of the sacrum
37

The Dimensions of the Normal pelvis
Diameters of the Brim ♥ Anterior – posterior diameters – is a line from the sacral
promontory to the upper border of the symphysis pubis. • When the line taken to the upper most point of the
symphysis it is called the anatomical conjugate or conjugate Vera and it measures 12cm.
• The measurement from the promontory of the sacrum to inner most margin of the symphysis pubis is the obstetrical conjugate and measures 11cm.
38

Dimensions….
♥ The diagonal conjugate – is measured anterior- posteriorly from the lower border of the symphysis pubis to sacral promontory and measures 12-13cm.
• It may be estimated pervaginum as a part of pelvic assessment.
♥ The oblique diameter – passes from the sacro-iliac joints to the opposite ilio- pectineal eminence.
• It measures12cm. ♥ The transverse diameters – is a line between the points
farther most a part on the ilio- pectineal lines and measures 13 cm.
♥ The sacro- cotyloid diameter – is a line passing from the promontary of the sacrum to the ilio- pectineal eminence and it measures 9.5 cm on each side.
39

Dimensions…
The diameters of the cavity - The cavity is circular in shape and all diameter are
equal in length. ♥ Anterior- posterior diameters – posses from the
mid point of symphysis pubis to the junction of the 2nd and 3rd sacral vertebrae and measures 12cm.
♥ The oblique diameter- pass obliquely in the plane of the cavity parallel to the oblique diameters of the brim. It measures 12cm.
♥ The Transverse diameter- passes in the plane of the cavity between the points far most apart in the lateral pelvic walls and measures 12cm.
40

Dimensions…
The diameters of out let ♥ The anterior-posterior diameter – passes from the
lower border of the symphysis pubis to the sacro-coccygeal joint and measures 13cm.
♥ There are two transverse diameters; The 1st is a line passes between the two ischial spines. It
measure 11 cm. The 2nd is a line passing between the inner borders of the
two ischial tuberosities and measures 11cm
♥ The oblique diameters – is said to be between the obturator foramen and the sacrospinous ligament.
It measures 12cm
41

Variations in pelvic shape
Features of normal female pelvis♣ Sacral promontory is not prominent or un
reachable. ♣ Rounded brim♣ The cavity is shallow with straight sides♣ Smooth (blunt) ischial spines ♣ The sacrum is smoothly concave (curved) ♣ Wide sciatic notch. ♣ The pubic arch is round ♣ Sub pubic angle 900
42

Types of pelvis
Based on the shape of the brim, there are four main groups of pelvis
• Gyneacoid • Android • Platypelloid • Anthropoid
43

Gynaecoid pelvis(50%)
It is the normal female type. Inlet is slightly transverse oval. Sacrum is wide with average concavity
and inclination. Side walls are straight with blunt ischial
spines. Sacro-sciatic notch is wide. Subpubic angle is 90-1000.
44

Fig. Gynaecoid pelvis 45

Android pelvis (20%):
♠ It is a male type. ♠ Inlet is triangular or heart-shaped with anterior
narrow apex. ♠ Side walls are converging (funnel pelvis) with
projecting ischial spines. ♠ Sacro-sciatic notch is narrow.
♠ Subpubic angle is narrow <900.
46

Fig .Android pelvis 47

Anthropoid pelvis (25%)
It is ape-like typeAll anteroposterior diameters are long. All transverse diameters are short. Sacrum is long and narrow. Sacro-sciatic notch is wide. Subpubic angle is narrow.
48

fig. Anthropoid pelvis 49

Platypelloid pelvis (5%)
♦ It is a flat female type. ♦ It has kidney shaped brim.♦All anteroposterior diameters are short. ♦All transverse diameters are long. ♦Sacro-sciatic notch is narrow. ♦Subpubic angle is wide.
50

Fig. platypelloid pelvis51

Others rare types of pelvis
Justo-minor pelvis It is similar to Gynaecoid in shape but all diameters are
equally reduced. Found in woman who is less than 1.5M tall. Face difficulties to deliver large baby .
Robert pelvis Has no wings (alae) of the sacrum and there fore
contracted in all diameters It is a type very rarely seen and is the result of congenital
abnormality . Caesarean section is always necessary for delivery
52

Naegele’s pelvis It has one wing of the sacrum This may be due to congenital abnormality but can be caused
by injury .
Delivery by c/s is always indicated .
fig. Robert’s pelvisFig. Naegele’s pelvis
53

Gynaecoid Anthropoid Android 54

The pelvic floor (pelvic diaphragm)
• The pelvic floor is formed by the soft tissue which fill the outlet of the pelvis.
• The urethra, the vagina and the anal canal pass through it.
Function Supports the weight of the abdominal and pelvic organs. Its muscles are responsible for the voluntary control of
micturition, defecation and play a role in sexual inter course.
Maintenance of intra- abdominal pressure. It influences the passive movement of the fetus through
the birth canal.
55

The muscles of the pelvic floor
Superficial pelvic floor muscles- includes
♥ Transverses perinea muscles – arises from the inner surface of ischial tuberosity and passes transversely a cross the out let to meet its follow.
• Helps to fix the position of the perineal body and support the lower part of the vagina.
56

Muscles …
♥ Bulbo-cavernous muscles – arise from the central point of the perineum and pass forwards around the vagina lying superficial to bartholin’s glands and the vestibular bulbs, and deep to the labia.
They are inserted into the corpora cavernous of the clitoris in the upper part of the pubic arch.
Its action is to diminish the size of the vaginal orifice and to cause engorgement of clitoris during sexual activity.
57

Muscles …
♥ Ischio cavernous muscles – pass from the ischial tuberosity a long the pubic arch to the corpora cavernous of the clitoris.
Their function is to cause engorgement of the clitoris.
♥ External anal sphincter – surrounds the anal canal, lying below the internal sphincter and the levator ani.
• Anteriorly it enters in to the formation of the perineal body and posteriorly some of its fibers are attached to the tip of the coccyx.
• Its function is to close the lumen of the anal canal.
58

Muscles…
♥ The membranous sphincter of the urethra – is composed of muscle fibers passing above and below the urethra and attached to the pubic bones.
Deep pelvic floor muscles• Is composed of three pairs of muscles which
together are known as the levator ani muscles. Each lavetor ani muscles consists of the following muscles.
♣Iliococcygeus muscles – arise from the white line of fascia on the inner aspect of each iliac bone and from ischial spine and runs posteriorly to the coccyx.
59

Muscles…
♣Ischiococcygeus muscles – arise from the ischial spine and pass to the upper part of the coccyx and lower border of the sacrum, in front of the sacro-spinous ligament.
It helps to stabilize the sacroiliac and sacro-coccygeal joints.
♣Pubococcygeus muscles- arises from the back of the body of pubic bones.
Its fibers sweep posteriorly below the bladder on either side of the urethra and the lowest third of the vagina, to enter the perineal body.
The longest fibers gain insertions into ano-cocygeal body and the coccyx.
They surround and support the urethra, vagina and rectum. It helps in controlling micturition and defection, as well as
normal sexual function. 60

Fig. Pelvic floor muscles and ligaments 61

The perineal body♦ It is a fibro- muscular pyramid situated between
the lowest third of the vagina in front, the anal canal behind, and the ischial tuberosities laterally.
♦ It is triangular in shape and each side of the triangle is approximately 3.5cm in length.
♦ Structurally it is composed of three layers of tissue;
Outer covering of skin Superficial pelvic floor muscles Bulbo cavernous Transverse perinea Deep pelvic floor muscle-puboccygeus
62

Pelvic fasciaIs a combination of connective tissue, blood
vessels and voluntary and involuntary muscle fibers.
It lines the walls and floor of the pelvic cavity and fills the area between the organs, thus giving additional support. The fascia thickens to form pelvic ligaments. These are Two lateral ligaments – extend from the white
line of the of fascia to the lateral walls of the bladder .
Two pubovesical ligaments – extend from the neck of bladder to the inner surface of each pubic body.
• They form part of the pubo-cervical ligaments. 63

Pelvic fascia…
Two pubovesical ligaments – are attached to the inner surface of each pubic body; they run posteriorly and become attached to the neck of bladder, the vault of the vagina and the supra vaginal cervix.
Transverse cervical ligaments (cardinal or mackenrodt’s) - are attached to the vaginal vault and supravaginal cervix.
• Run transversely across the pelvic floor and run out until they reach the white line of the fasciae.
• They are the strongest of the pelvic ligaments. 64

Pelvic fascia…
Uterosacral ligaments – are attached to the vaginal vault and supravaginal cervix.
They pass posteriorly and attach to the lateral border of the 1st sacral body.
Round ligaments – arise anteriorly from just below the cornu of the uterus and fallopian tubes then take a V, shaped canal before inserting in to each labia major.
The cardinal, uterosacral and round ligaments all contribute to the support of the uterus and maintenance of its position
65

II. The anatomy of the female
Genital Organs
66

The anatomy of the female Genital Organs
♣External Genitalia
Vulva – is formed from the following structures;
Mons pubis – is a pad of fatty tissue situated in front of the symphysis pubis.
It is covered by skin and pubic hair which develop at the time of puberty and appears triangular in distribution.
Purpose – protect the junction of the pubic bone from trauma.
67

External Genitalia…
Labia majora- are two large rounded folds of fatty tissue covered by skin which meet anteriorly at the mons pubis.
Posteriorly each labia majora fuses medially to for in the posterior commissure.
Contains sebaceous glands, sweet glands and hair follicle.
68

External Genitalia…
Labia minora – are two smaller folds of pink skin lying longitudinally with the labia majora.
The area they in close is known as the vestibule Anteriorly they divided in to two folds. The upper folds surround the clitoris and unite to
form the prepuce. The two lower folds are attached to undersurface
of the clitoris and are known as the frenulum. Posteriorly, the labia minora unite to form a thin
fold of skin, the fourchette.
69

External Genitalia…
Clitoris:- is small extremely sensitive erectile structure situated with in the folds of the prepuce and frenulum.
It is about 2.5 cm long and is composed of two corpora covernose.
It consists of the glans, body and two crura. It is analogue to the penis in the male and
highly vascularized
70

71

External Genitalia…
vestibules:- is a triangular space bounded anteriorly by the clitoris, posterior by the fourchette and on either said by labia minus.
• There are four openings in to the vestibule.
1.The urethral meatus – lies 2.5 cm below the clitoris.
2.The vaginal orifice (introitus) – occupies the lower two thirds of the vestibule lying between the labia minora.
72

♫Hymen-is a thin membrane which covers the introitus in virgin.
73

External Genitalia…
3.The bartholin’s ducts and glands:- are situated in the superficial perineal pouch posterior to the vestibular bulb.
• It secretes abundant alkaline mucus during sexual excitement which helps in lubrication.
4.Vestibuler bulb:- are bilateral masses of erectile tissues situated beneath the mucus membrane called vestibule.
• Each bulb lies on either side of the vaginal orifice deep to the labia majora and minora and anterior to bartholin’s glands.
74

External Genitalia…Blood supply:- The vulva is supplied with blood
from two main arteries ♥ The femoral artery in the upper part of the thigh. ♥ The internal pudendal arfery running along the
pubic arch. The veins drain to corresponding veins. Lymphatic drainage: - some drainage in to the inguinal glands and some is in to the external iliac
glands. Never supply:- is from the branches of pudendal
nerve and the perineal nerve.
75

Internal genitalia♥ The vagina Is a tube (canal) which extends from the vulva to
the uterine cervix. It is longer in posterior wall (9cm) than anterior
(7cm). The vault of the vagina is divided in to four fornices
by the projection of the cervix.Anterior PosteriorTwo lateral fornices • The posterior for nix is the largest. • The vaginal walls are pink in appearance and
thrown in to small folds known as rugae.76

The vagina…
Structures• Vaginal wall is composed of four layers. • The layers from in to out wards are :1. Mucus coat lined by stratified squamous
epithelium. 2. Sub mucous layer 3. muscular layer – inner circular and outer
longitudinal 4. fibrous coat
77

The vagina…Contents • There are no glands situated in the wall of the
vagina.• The vagina contains a small amount of fluid
which is derived from two sources;Alkaline mucus which secrete from the glands of
the cervix,The vaginal blood vessels which allow serous
fluid to transude through the vaginal wall into its lumen.
• The vaginal fluid is acidic in reaction having a PH of about 4.5 during reproductive life.
78

The vagina…
Relations Anterior – the bladder and the urethra Posterior – lowest 2/3 perineal body -Middle third rectum -Upper third pouch of Douglas. Lateral – upper 2/3 pelvic fascia at the base of the
brood ligament. - Lowest third – two levator ani muscles - bulbo-cavernosus muscles. Superior – Uterine cervix Inferior – hymen and the structures of the vulva
79

The vagina…Blood supply Arterial supply from the vaginal, the uterine
(descending branch), the middle haemorrodial, the inferior vesical and pedundial arteries
The vain drains in a corresponding manner. Lymphatic drainage The lowest 2/3 drain to the horizontal inguinal
groups along with those of the vulva. Upper 1/3 drain to the internal iliac and sacral
glands. Nerve supply • is from the sympathetic and pelvic splanchnics
nerves 80

The vagina…
Functions Entrance for spermatozoa Exit for menstrual flow and products of
conception Helps to support the uterusOrgans for sexual intercourse Helps to prevent infection
81

The Uterus
Is a hollow, flattened, muscular peer shaped organ situated between the bladder and rectum in non pregnant state.
It is normally anteverted and anteflaxed It measures 8cm in length 5cm width and
2-3 cm thick. Its weight is approximately 57gm.
82

The Uterus…
It consists of the following parts. Body or corpus• Comprise the upper 2/3 of the uterus • Lies between the isthmus and the opening of the
fallopian tubes.CervixForms the lower third of the uterus and measures
about 2.5 cm in length. It is conical in shapeThe cervix projects through the anterior wall of the
vaginal which divides it in to an upper supra vaginal portion and lower vaginal portion.
83

The Uterus…
SUPRA VAGINAL CERVIX – lies out side and above the vagina
Superiorly it meets the border of the uterus at the isthmus.
Is separated in front from the bladder by parametrium.
Posteriorly it is covered by the peritoneum.
84

The Uterus…INFRAVAGINAL CERVIX- is the part which projects in
to the anterior vaginal wall between the anterior and posterior fornices.
• The internal os-opens in to the cavity of the uterus It dilates during labor. In competence of the cervix at this level results in
spontaneous abortion. • The external os – opens in to the vagina at the lower
end of the cervical canal. • The cervical canal – lies between the internal and
external os It is fusiform in shape.
85

The Uterus…
• FUNCTIONS OF THE CERVIX • It helps to prevent infection entering the
uterus. • It dilates and withdraws during labor to
enable vaginal delivery of the fetus and
placenta.
86

The Uterus…
The funds- is the domed upper wall between the insertions of the fallopian tubes.
The cornu- are the upper outer angles of the uterus where the fallopian tubes join.
The cavity- is a potential space between the anterior and posterior walls
It is triangular in shape the base of the triangle being upper most.
The isthmus- is a narrow area between the cavity and the cervix which is 7 mm long.
It enlarges during pregnancy to form the lower uterine segment. 87

The Uterus…
STRUCTURES 1. The mucous membrane (tunica mucosa) –
Endometrium Forms a lining of ciliated epithelium on a base of
connective tissue or stroma. The epithelial cells are cubical in shape and dip
down to form glands which secrete alkaline mucus.
88

The Uterus…
The cervical endometrium is thinner than that of the body and is folded in to a pattern known as the arborvitae (tree of life), this assist the passage of the sperm.
Here the epithelial cells are tall and columnar in shape.
89

The Uterus…
2.The muscular coat (tunica muscularis)- Myometrium.
It is thick in the upper part of the uterus and is more sparse in the isthmus and cervix.
Its fibers are outer longitudinal, middle interlacing oblique and inner circular.
Its muscle fibers are embedded in collagen fibers which enable to stretch in the labor.
90

The Uterus…
3.The serous coat (tunica serosa)- Perimetrium.
Is derived from the peritoneum; it invests the fundus and the whole of the intestinal surface of the uterus, covers the vesical surface as only far as the junction of the body and cervix.
91

The Uterus…
♦ The form, size and situation of the uterus vary at different periods of life and under different circumstances.
In the fetus:- the uterus is contained in the abdominal cavity projecting beyond the superior aperture of the pelvis.
• The cervix is considerably larger than the body.
At puberty- it is pyriform in shape and weights from 14 to 17 gm.
92

The Uterus…
In the adults- the position of the uterus depends on the condition of the bladder and rectum.
When the bladder is empty the entire uterus is directed forward and is at the same time bent on itself at the junction of the body and cervix, so that the body lies up on the bladder.
as the bladder fills the uterus gradually becomes more and more erect until with a fully distended bladder the fundus may be directed back ward toward the sacrum. 93

The Uterus…
During menstruation:-the uterus is enlarged, more vascular, and its surface rounder; the external orifice is rounded, its labia swollen, and the lining membrane of the body thickened, softer, and of a darker color.
94

The Uterus…During pregnancy- the uterus becomes
enormously enraged. By 12th week of pregnancy it rises out of
the pelvis and becomes abdominal organs, by 38th week it reaches the xiphisternum.
It is not longer anteverted and anteflexed but it is becoming vertical.
At full term the uterus is 30cm in length, 23 cm wide and 20cm thick.
Its weight has increased from 57gm to 1000gm.
95

The Uterus…
After parturition-the uterus nearly regains its usual size, weighinig about 42gm; but the cavity is larger than in the virgins state, its vessels are tortuous, and its muscular layers are more defined; the external orifice is more marked, and its edges present one or more fissures.
96

The Uterus…
In old age - the uterus becomes atrophied, and denser in texture, a more distinct separates the body and cervix.
• The internal orifice is frequently, and the external orifice occasionally, obliterated, while the lips almost entirely disappear.
97

The Uterus…
♠ RELATIONS ANTERIOR –uterovesical pouch and
bladder.POSTERIOR- recto uterine pouch of
Douglas and the rectum.LATERAL –broad ligaments, the fallopian
tubes and ovaries. SUPERIOR- the intestines INFERIOR – the vagina.
98

The Uterus…♥ UTERINE SUPPORTS (ligaments) Transverse cervical ligaments and
(mackenrodt’s) Uterosacral ligaments Pubocervical ligaments Broad ligaments Pass from the sides of the uterus to the lateral
walls of the pelvis.Together with the uterus it forms a septum
across the female pelvis dividing the cavity in to two portions.
99

The Uterus…
Between the two layers of each broad ligament are contained;
Uterine tube The round ligament of the uterus The ovary and its ligament The epoophoron and paraoophoron Connective tissue Unstriped muscular fibers Blood vessels and nerves Round ligaments
100

The Uterus…BLOOD SUPPLY From the uterine artery, a branch of the hypo
gastric artery. Veins drains to the corresponding manner. LYMPHATIC DRAINAGE- lymph is drained from
uterine body to the internal illiac glands and also from the cervical area to many other pelvic lymph glands.
Nerve supply -from autonomic nervous system, sympathetic and parasympathetic via sacral plexus
101

The Uterus…
FUNCTION OF THE UTERUS To prepare a bed for the fertilized ovum. To nourish the fertilized ovum for the
gestation period To expel the product of conception at full
term. To involutes following child birth
102

FALLOPIAN TUBES
Are paired structures which are attached with the lateral angle of uterine cavity.
They run along the upper margin of the broad ligament and 10 cm in length.
It has four portions
1.The interstitial portion- is 1.25 cm long and lies within the wall of the uterus.
Its lumen is 1mm wide
103

FALLOPIAN TUBES…
2.The isthmus – is another narrow part which extends for 2.5 cm from the uterus.
It acts as reservoir for spermatozoa because its temperatures is lower than other.
3.The ampulla- is the wider portion where fertilization usually occurs & it is 5 cm in length.
4.The infundibulum- is the funnel shaped fingered end which is composed of many processes know as fimbriae.
104

105

FALLOPIAN TUBES…
RELATIONS
♥ Anterior posterior and superior the peritoneal cavity and the intestine
♥ Lateral the side walls of the pelvis.♥ Inferior the broad ligaments and
ovaries. ♥ Medial the uterus.
106

FALLOPIAN TUBES…LAYERS OF THE TUBE• It consists of three coats
1.The external or serous coat is the peritoneum.
2.Middle or muscular coat- consists of inner circular and outer longitudinal layer of smooth muscles which helps for peristaltic movement of the fallopian tube.
3.The internal or mucous coat-is line by columnar and ciliated epithelium.
Beneath the lining is a layer of vascular connective tissue.
107

FALLOPIAN TUBES…
SUPPORT - by the infundibulo pelvic ligaments. These ligaments are formed from folds of the
broad ligament and run from the infundibulum of the tube to the side walls of the pelvis.
Blood supply:- is via the uterine and ovarian arteries; venous return is by the corresponding veins.
Lymphatic drainage- is in to the lumbar gland. NERVE SUPPLY – is from the ovarian plexus.
108

FALLOPIAN TUBES…
FUNCTIONSPropels the ovum towards the uterus.Receives the spermatozoa as they
travel up wards Provides a site for fertilization Supplies the fertilized ovum with
nutrition during its continued journey to the uterus.
109

THE OVARIES
Are two nodular bodies which produce ova and hormones estrogen and progesterone.
POSITION They are attached to the back of the broad
ligament within the peritoneal cavity Size 3 cm in length, 2 cm in width and
about 1 cm in thickness and weight from about 6gm.
110

THE OVARIES…
RELATIONS Anterior the broad ligament. Posterior the intestine. Lateral the infudibulopelvic ligaments
and the side walls of the pelvis. Superior the fallopian tubes. Medial the uterus and ovarian
ligaments.111

THE OVARIES…
SUPPORTS • From above by the ovarian ligament
medially, and the infundibulo pelvic ligaments laterally.
• Attachment of ovary- infundibulo pelvic ligament to the pelvic wall.
Ovarian ligament- to the uterus.Mesooverium – to the broad ligament
112

THE OVARIES…Structures • The ovary is composed of medulla and
cortex covered with germinal epithelium. The medulla- is the central portion and
point of entry for blood vessels, lymphatic and nerves.
The hilum where these vessels enter lies just where the ovary is attached to the broad ligament and this area is called the mesovarium. 113

THE OVARIES…
The cortex- is the functioning part of the ovaryIt contains the ovarian follicles in
different stage of development surrounded by stroma.
The outer layer is formed of fibrous tissue known as tunica albuginea.
Germinal epithelium lies over the tuinica albuginea.
114

THE OVARIES…
Blood supplyIs from the ovarian arteries and
drains by the ovarian veins.Lymphatic drainage- is to the lumbar
glands. Nerve supply- is from the ovarian
plexus.
115

III. Physiology of the female
reproductive organs
116

III. Physiology of the female reproductive organs
Hormones and their function Hypothalamus produces a specific
releasing and inhibitory hormones or factors which have effect on the production of pituitary hormones.
1.Gonadotrophin releasing hormonesConcerned with the synthesis, storage
and release of gonadotropin hormones (FSH and LH)
117

Hormones…
2.Prolactin inhibitory factor/ hormones3.Thyrotrophin releasing hormone Stimulates the release of TSH4.Corticotrophin releasing hormone Stimulate the release of ACTH5.Growth hormone releasing hormones Stimulate the release of growth
hormones.118

Hormones…
PITUITARY HORMONES
♠ Anterior pituitary (Adenohypothesis)Gonadotropins hormones - FSH and LH.Prolactin hormones- milk production.Others hormones - TSH,ACTH,GH♠ Posterior pituitary – Oxytocin and ADH.
119

Hormones…Ovarian hormones
1.Estrogen - is produced by granulosa cells under the influence of FSH.
Function (actions)Responsible for secondary sexual
characteristics.Inhibition of FSH secretion from ovary
(negative feedback mechanism).Growth of myomentrium, endometrium,
alveoli and ducts of the breast.120

Hormones…
Myometrial stimulation (increase myometrial contractility).
Promotion of female fat distribution.Stimulation of protein synthesis in the liver.Promotion of calcifications of the bone.Angiogenesis (new blood formation).Na and H20 retention by the kindney.
Influences the production of cervical mucus and the structure of the vaginal epithelium.
121

Hormones…
2.Progestrone-produced by the corpus luteum under the influence of LH.
Actions Growth of ducts and lobules of the
breast, inhibition of prolactin synthesis. Relaxation of smooth muscles of the
uterus, blood vessels, GI and urinary tract.
Secretary changes and decasualization of the endometrium.
122

Hormones…
Vasodilatation. Termogenic (increase BBT). Hyperventilation (decrease concentration
of co2 .
3.Androgens - produced by the theca interna cells.
They are source for estrogen synthesis.
4.Inhibin and Relaxin 123

PUBERTY
Is the stage of life at which secondary sexual characteristics appear:
It is marked by neuro-endocrine changes.Pulsative releases of GnRh seen at this
time.Ovarian steroid hormones start to be
secreted.The H-P-O axis becomes coordinated.
124

PUBERTY…
Notable changes at this time are:- Breast development. Marked physical growth.Increase in the transverse diameter of the
pelvis.Growth of pubic and auxiliary hair. Menarche – the 1st menses.
125

The menstrual cycle• is a periodic uterine bleeding in response to cyclic
hormonal changes.• It is hallmark of reproductive year.
Characteristics of normal menses
• Interval 21-35 days• Amount 30-80 ml• Duration 1-8 days, average 5 days• The blood is arterial (85%) oxygenated the rest 10-
15% is deoxygenated.• Color dark red and non clotted in nature 126

The menstrual cycle… Physiology of menstruation
Ovarian follicular developmentThe number of oocytes are 6-7 million by
20 weeks of gestation.1-2 million oocytes remain in the ovary at
birth.At puberty only 300,000 oocytes remains.Only 400-500 will ultimately ovulate and
they will end up at the time of menopause.127

The menstrual cycle… PHASE OF OVARIAN CYCLE1.Follicular phase:- hormonal feedback
promote the development of single dominant follicle.
Its average length is 10-14 days.
2. Luteal phase: - the time from ovulation to the onset of the menses.
Average length 14 days. 128

The menstrual cycle…Hormonal variationAt the beginning of each monthly menstrual
cycle levels of gonadal steroids (progesterone and estrogen) are low and have been decreasing since the end of luteal phase of the previous cycle.
Demise of corpusluteum results FSH level begin to rise.
Causes growing of follicles from the ovary.129

The menstrual cycle…Each growing follicies start to secrete
estrogen hormone; this results uterine endometrial proliferation.
Maximum estrogen level provides negative feedback on pituitary FSH secretion (which begins at midpoint of the follicular phase).
Estrogen also stimulates LH production through the follicular phase.
130

The menstrual cycle…At the end of the follicular phase (just prior to
ovulation) FSH induce LH receptors, then with LH stimulation secretion of progesterone will takes place.
After sufficient degree of estrogenic stimulation the pituitary LH surge is triggered, this is the cause of ovulation then occurs 24- 36 hrs later.
131

The menstrual cycle…Estrogen level begin to rise again as result
of corpusluteum secretion.Progesterone level rise after ovulation, it is
a presumptive sign of ovulation has occurred.
Both estrogen and progesterone level remain elevated till the demise of corpusluteum, then the next cycle will continue.
132

The menstrual cycle…• Phase of endometrial cycle Because of the systemic effects of estrogen, the
endometrium undergoes histologic cyclic changes that culminate in menstruation.
The superficial 2/3 of the endometrium is called the decidua functionalis and is composed of stratum spongiosum – superficial zone.
The decidua basalis- is the deepest region of endometrial and doesn’t undergo significant monthly proliferation. It is the source of endometrial regeneration after each menses.
133

The menstrual cycle… There are three phases in the endometrial
cycle.
1.Menstrual phase:- start from day 1 and usually lasts 3 to 5 days.
During this phase there is irregular sloughing of the superficial 2/3 of endometrium (decidua functionalis) accompanied by blood. Expulsion of the blood is aided by uterine contraction.
134

The menstrual cycle…2.Proliferate phase- starts near the end of the
menstrual phase the basal layer of the endometrium (decidua basalis) under the influence of estrogen; proliferate to regenerate the superficial layer that is shaded during menses.
At the beginning of this phase endometrium is relatively thin (1-2mm)
135

The menstrual cycle…3.Secretary phase- extends from ovulation to the
onset of the next menses. The proliferative endometrium, under the
influence of progesterone is changed to secretary type.
Glands becomes tortuous and exhibit secretary activity
Stromal cells are separated by interstial endometrium
The estrogen receptor cells decreases progressively because of the antagonistic effect of progesterone. As a result there is antagonism of estrogen induced DNA synthesis and cellular mitosis. 136

The menstrual cycle…At post ovulatory day 6-7 secretary activity of
the glands is maximal and endometerium is optimally prepared for implantations of the balastocyst.
Later on the endometrial layer become edematus and 2 days prior to menses there is a dramatic increment of polymorphonuclear lymphocytes “ leukocytic infiltration” it heralds the collapse of the endometrial stroma and menses will start to flow.
137

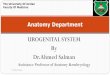
The Menstrual Cycle
138

The menstrual cycle…Mechanism of Menstruation
In the absence of pregnancy, decreasing level of progesterone from the dying corpusluteum, results in dehydration of the stroma, as a result there is increased coiling of the spiral arteries, which supply the superficial layer of the endometrium
139

The menstrual cycle…
Prostaglandin f2@-initiate uterine contraction.
Decreases local uterine blood flow. Physical expel of the blood which result in
menstruation.
140

IV. EMBRYOLOGY
141

IV. EMBRYOLOGYIs a science that deals with the origin and
development of individual organism.FERTILIAZATION- is the union of the ovum
and spermatozoa. Following ovulation as the ovum is extruded
from the graafian follicle it is surrounded by a ring of mucoploysaccharide fluid (the zone pellucid) and a circle of cells (the corona radiate.)
Fertilization usually takes place at the ampulla.
142

Mr.SPERM + Mrs. EGG
143

EMBRYOLOGY cont..
Immediately after penetration of the ovum the chromosomal material of the ovum and the spermatozoa fuse. The resulting structure is called a zygote.
The occurrence of fertilization depends on: Maturation of both sperm and ovum.Ability of the sperm to reach the ovum Ability of the sperm to penetrate the
zonapellucida and cell membrane and achieve fertilization.
144

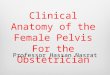
Fertilization and the Events of the First 6 Days of Development
145

EMBRAYOLOGY cont..
IMPLANTATION- is a contact between the blastocyst and the uterine endothelium.
It occurs approximately 8 to 10 Days after fertilization.
Once fertilization is complete the zygote migrates towards the body of the uterus aided by muscular contraction of the fallopian tubes.
146

EMBRYOLOGY cont.. It takes 3 to 4 days for the zygote to reach the body
of the uterus. This time the zygote undergoes mitotic division and consists 16 to 50 cells and is termed as a morula.
When fluid filled cavity appears in the morula a blastocyt is formed, these is after 3 or 4 days.
The cells of a blastocyst are arranged in to layers the outer layer is called the trophoblast which eventually develops in to the placenta and membrane. The inner layer is called the embryoblast which later gives rise to the embryo (fetus). 147

EMBRYOLOGY cont.. All tissue products of conception (embryo, fetus, fetal
membranes and placenta) are called conceptus. On day 4 after fertilization the blastocyst enters in to the
uterine cavity. By day 7 starts embedding it self in to the prepared
endometrium which is now called the deciduas. This process is called implantation.
Once implanted the zygote is an embryo (the period from the end of ovum stage until measurement reaches approximately 3cm, 54-56 days).
Fetus- period end of embryo stage until birth.
148

EMBRYOLOGY cont..
First trimester (0-12 wks) Susceptible to teratogens.Heart function at 3-4 weeks. Eye formation at 4-5 weeks Arm and leg buds at 4-5 weeks Recognizable face at 8 weeks
149

EMBRYOLOGY cont..
Brain rapid grows. External genitalia at 8 weeks.Placenta formed at 12 weeks. Bone ossification at 12 weeks.Fetal circulation function properly
at 8-12 weeks.
150

EMBRYOLOGY cont..
2nd trimester (13-27 weeks) Less danger from teratogens after 12 week.Facial features formed at 16 week.Fetal heart beat heard by 16 to 20 week with
fetoscope.Lanugo appears (hair over the body).Vernix present. Length 10 inches (2.5 cm), weight (05-0.6 Ib)
(0.23-0.27 kg).Most organs become capable of functioning.
151

EMBRYOLOGY cont..
3rd trimester (28-42 weeks) Iron stored. Surfactant production begins in increasing
amount.Size; 15 inches, 2-3 pounds.Testes descend in to scrotum in male at
28-32 week.Calcium stored at 28-32 week.
152

EMBRYOLOGY cont..
Reflexes present at 28-32 week.Subcutaneous fat deposits at 36
week.Lanugo disappears from the body Average size – 18-22 inch, 7.5-8.5 Ib
at 38-40 weeks. Term is reached and birth is due at
38-40 weeks.153

EMBRYOLOGY cont..
THE DECIDUA- is the endometrium after implantation. It has three parts
1.The decidua basalis- the part of the endometrium lying directly under the embryo (the portion where the trophoblast cells establish communication with maternal blood vessels).
2.The decidua capsularis- the portion of endometrium that stretches or encapsulates the surface of the trophoblasts.
3.The decidua vera- the remaining portion of the uterine lining.
154

EMBRYOLOGY cont..
CHORIONIC VILLIAs early as the 11th or 12th day after
conception the tropoblastic cells have sent out processes in to the endometrium. The outgrowths becomes finger like and termed chorionic villi.
The chorionic villi have a central core of loose connective tissue surrounded by a double layer of trophoblastic cells.
155

THE PLACENTA
Is formed from the traphoblast and deciduas basalis.
The placental barrier is formed by the syncitiotrophoblast, cytotrophoblast, the basement membrane and fetal vascular endothelial cells.
The placenta on overage has a diameter of 18 cm, a thickness of 23 mm, a volume of 497ml, a weight of 508 grams and villous surface area of 15m2.
156

THE PLACENTA…
It has two surfaces; maternal and fetal surface.
The maternal surface is made of deciduas basalis and dark red in color.
The fetal surface is smooth, white and is covered by amnion. The branching fetal vessels are visible under the amnion.
157

THE PLACENTA…
FUNCTIONS OF PLACENTA
1.Respiration2.Nutrition- food for the fetus derives from
the mother’s diet and the placenta select those substance required by the fetus.
3.Stordge – the placenta metabolites glucose, stores it in the form of glycogen and reconverts it to glucose as required. It can also store iron and fat-soluble vitamins. 158

THE PLACENTA…
4.Excretion- co2 and bilirubin is excreted through placenta.
5.Protection- placental barrier provides protection against-certain bacteria, virus and maternal immunoglobins in case of Rh-isoimmunization.
159

THE PLACENTA…
6.Endocrine function- placenta secretes certain hormones:
Human chorionic gonadotropin (HCG)- the first hormone to be produced.
• Produced by the cytotrophoblastic layer of chorionic villi.
160

THE PLACENTA…
• Its purpose is to act as fail-safe measure to ensure that the corpus luteum of the ovary continues to produce progesterone and estrogen.
• Forms the basis for pregnancy test. Estrogens – is produced as a 2nd product of the
syncitial cells of the placenta. • It contributes to the mother’s mammary gland
development in preparation for lactation and stimulates the uterus to growth to accommodate the developing fetus. 161

THE PLACENTA…
Progesterone- maintain endometrial lining of the uterus during pregnancy.
• It reduces contractility of the uterine musculature during pregnancy which prevents abortion and premature labor.
162

THE PLACENTA…
Human placental lactogen (HPL) (chorionic somatomamotropin):
• Is produce by placental trophoblasts (as early as 3rd week) and detected in serum by 4th week after ovulation.
• Its main action is resetting of CHO and fat metabolism of mother so as to ensure adequate supply of glucose and energy to the fetus.
163

THE PLACENTA…
• Other action includes. • Gluconeogenesis inhibition. • Inhibitions of peripheral uptake of cellular
glucose and insulin hyper insulinism maintain maternal blood glucose level.
• Increase uptake of amino acid and ketones by placenta.
164

THE PLACENTA…
ANATOMICAL VARATION OF THE PLECENTA AND CORD
1.Succenturiata lobe of placenta A small extra lobe is present, separate from the
main placenta and joined to it by blood vessels which run through the membrane.
Danger – the small lobe may be retained in the utero after delivery and if it is not removed it may lead to hemorrhage and infection.
Identification- on inspection the placenta will appear torn at edge or torn bold vessels may extend beyond the edge of the placenta.
165

THE PLACENTA…
2.Circumvallate placenta- in this situation an opaque ring is seen on the fetal surface.
• It is formed by a doubling back of the chorion and amnion.
3.Bipartite placenta- two completed and separate lobes are present each with a cord leaving it.
• The bipartite cord joins a short distance from the two parts of the placenta.
• Danger- the extra lobe may be retained during delivery. 166

THE PLACENTA…4.A tripartite placenta – is similar to bipartite but
with three distinct lobes. 5.Battledore insertion of the cord- the cord is
attached at the very edge of the placenta • Danger- likely it is detached up on applying
traction during active management of 3rd stage of labor.
6.Velamentous insertion of the cord- it is inserted in to the membrane some distance from the edge of the placenta.
• The umbilical vessels run through the membranous from the cord to the placenta.
• Danger- the vessels may tear with cervical dilatation and would result in sudden blood loss. 167

THE UMBILICAL CORD (FUNIS)
Connects the placenta to the fetus.It has average length of 50 cm (range
30-100 cm) and diameter of 0.8-2 cm.It contains two umbilical arteries, one
umbilical veins and Wharton’s jelly (jelly like substance which surrounds the blood vessels).
168

THE UMBILICAL CORD…
FUNCTIONS
To transport oxygen and nutrients from placenta to the fetus.
To return waste products from the fetus to the placenta
Allows fetal mobility.
169

THE MEMBRANES AND AMMIOTIC FLUID
The membranes (sac) – it has two layers:
1.Chorion - is the smooth opaque outer most fetal membrane.
• Purpose – support the sac that contains amniotic fluid.
2.Amnion – is the inner membranes which is smooth, strong and transparent.
• It lines the chorion and could always be detached from it to the insertion the umbilical cord.
170

THE MEMBRANES AND AMMIOTIC FLUID…
• Its function are:
Offers support to amniotic fluids. It produce the amniotic fluids. It produce phospholipids that
initiates the formation of prostaglandins.
171

THE MEMBRANES AND AMMIOTIC FLUID…
AMNIOTIC FLUID Is a clear fluid in which through the fetus floats
and is also called liquor amnion. It is present in the sac from the early months. The normal amount is from 500cc-1500cc. It is alkaline in reaction and has 99% of water. The remaining 1% contains; mineral salt, urea
from the fetal urine in late pregnancy, trace of protein, fat, CHO, enzymes, lanugo, bile pigments, placental hormones.
172

THE MEMBRANES AND AMMIOTIC FLUID…
ORIGION – is from amnion. Maternal vessels in the decidua. Fetal vessels in the placenta. Fetal urine. APPEARANCE: Its normal color is clear fluid.Meconium stained- sign of fetal distress except
in cases of breech presentation.Golden- sign of hemolytic disease.Milky appearance because of vernix caseosa.
173

THE MEMBRANES AND AMMIOTIC FLUID…
FUNCTIONS: Allows the fetus free movement. Enables fetal limbs to develop and move
without being compressed by each other, the fetal trunk or the walls of the uterus.
Equalizes intra uterine pressure and acts as a shock absorber.
Stablises intrauterine temperature.
174

ORIGIN AND DEVELOPMENT OF ORGAN SYSTEM
From the beginning of the fetal growth, development proceeds in a cephalo- caudal (head to tall) direction.
• PRIMARY GERM LAYERS –the three germ layers which are formed during embryonic stage are:
1. Mesoderm • Forms supporting structures of the body (connective
tissue, cartilage, muscle, bone and tendons).• Upper portion if urinary system; reproductive
system, heart; circulatory system and blood cells.175

ORIGIN AND DEVELOPMENT OF ORGAN SYSTEM…
2.Endoderm • Forms mucous membranes and glands
(lining of the GIT, respiratory tract, tonsils, parathyroid, thyroid, thymus gland).
3.Ectoderm • Forms the nervous system, skin, hair and
nails, sense organs and mucous membranes of the mouth and anus.
176

177

UTERINE MALFORMATION
Various types of structural abnormality can result from failure of fusion of the mullerian ducts.
♥ Double uterus and double vagina- develop when there is complete failure of fusion of the duct.
♥ A single vagina with a double uterus- is the result of fusion at the lower end of the ducts only.
178

UTERINE MALFORMATION…
♥ A bicornuate uterus (one with two horns)- is the result of incomplete fusion at the upper portion of the urogenital area.
♥ Unicornuate uterus -with one horn.♥ Agenesis- complete absence of the
uterus and vagina ♥ Imperforate hymen.
179

UTERINE MALFORMATION…
• EFFECTS OF THE UTERINE ABNORMALITY
Abortion Premature labor abnormal lie of the
fetus Poor uterine contraction Obstructed labor
180

V. Fetal circulation
181

V. Fetal circulation As the placenta acts as the intermiditary organ
of transfer between the mother and fetus, fetal circulation differs from that required for extra uterine existence.
The fetus receives oxygen through the placenta because the lungs do not function as organs of respiration in the uterus.
To meet this situation the fetal circulation contains certain special vessels that shunt the blood around the lungs, with only a small amount circulating through them for nutrition. 182

Fetal circulation cont.. The following functions occur.
The umbilical vein transports blood rich in oxygen and nutrients from the placenta to the fetal body. This vein travels along the anterior abdominal wall of the fetus to the liver and at the porta hepatis, the umbilical vein divides in to two branches.
About ½ of the blood passes in to the liver and the rest enters a shunting vessel called the ductus venosus that by passes the liver. The ducts venosus travels a short distance and joins the inferior vena cava
183

184

Fetal circulation cont.. There, the oxygenated blood from the placenta is
mixed with deoxygenated blood from the lower parts of the fetal body. This blood continues through the vena cava to the right atrium.
As the blood relatively high in oxygen enters the left atrium of the fetal heart, a large proportion of it is shunted directly in to the left atrium through an opening in the artial septum called the foramen ovale.
The more highly oxygenated blood that enters the left atrium through the foramen ovale is mixed with a small amount of deoxygenated blood returning from the pulmonary veins. This mixture moves in to the left ventricle and is pumped in to the aorta.
185

Fetal circulation cont..
Some of this blood reaches the myocardium by means of the coronary arteries and some reaches the tissues of the brain through the carotid arteries
The rest of the blood entering the right atrium as well as the large proportion of the deoxygenated blood entering from the superior vena cava, passes in to the right ventricle and out through the pulmonary artery.
186

Fetal circulation cont.. Enough blood reaches the lung tissues to
sustain them. Most of the blood in the pulmonary artery
bypasses the lungs by entering the ductus arterious which connects the pulmonary artery to the descending portion of the aortic arch.
Some of the blood carried by the descending aorta leads to the various parts in the lower regions of the body
The rest of the blood passes in to the umbilical arteries which branch from the internal iliac arteries and lead to the placenta.
187

VI. The fetal skull Is a bony box like cavity which contains
and protects the delicate brain. It is the most important part of the fetus
because; It contain the delicate brain It is the least compressible part of the fetus. It is the most difficult part to deliver whether it
comes first or last. It is the largest part of fetus.
188

The fetal skull…
♦Division
The fetal skull is divided into three parts:♣ The vault – is the large dome shaped part
above the imaginary line drown from below the occipital protuberance to the orbital ridges.
♣ The face - area extending from the orbital ridges to the junction of the chin and neck.
♣ The base - is composed of bones which are firmly united to protect the vital centers in the medulla.
189

The fetal skull…
Bones of the vault • There are five main bones in the vault of the
fetal skull.
♠ One occipital bones – lies at the back of the head and forms the region of the occiput.
Its ossification center is known as occipital protuberance.
It is roughly triangular in shape. In its lower part it forms the margins of the
foramen magnum. 190

The fetal skull…
♠Two parietal bones – lie on either side of the skull.
The ossification center of each bone is called partial eminence.
They are the largest of the cranial bones. Roughly square in shape and curves as they lie over the
parietal lobes of the brain.
♠Two frontal bones – form the forehead or sinciput.
Their ossification centers are named frontal eminence or frontal bosses.
Fuse in to a single bone by 8 years191

The fetal skull…
Sutures Is an area of membrane between the skull bones where ossification has
not been completed. Overlap during the process of moulding at the time of birth. Types of sutures Lambdoidal suture – separate the occipital bone from the two parietal
bones. It is shaped like the Greek letter Lambda
Sagital suture- runs between the two parietal bones and runs from the anterior fontanel in front to the posterior fontanel behind.
Frontal sutures- runs between the frontal bones, extending from the root of nose below, to the anterior fontanelle above.
Coronal suture- separate frontal bones parietal bones, passing from one temple to the other.
192

The fetal skull…
Fontanels Are areas where two or more suture meet. There are 6 fontanels, but only two are of great
obstetrical importance. ♥ The anterior fontanel or bregma :-is formed
where the sagital, coronal and frontal sutures meet.
It is diamond in shape. It is much longer than posterior fontanel.Pulsation of cerebral vessels can be felt through
it. Normally closes at 18 months of age
193

The fetal skull…
♥ Posterior fontanel occurs at the junction of the
lambdoidal and sagital sutures. It is very small and triangular in
shape It is normally closes by 6 weeks of
age
194

195

The fetal skull…
The Regions of the skull ♦ Vertex –is bounded by the anterior and posterior
fontanels and parietal eminences ♦ Occiput – lies between the foramen magnum and
posterior fontanel.
♦ Sinciput (brow) – extends from the anterior fontanel and coronal suture to the orbital ridge
♦ Face – extends from the orbital ridges and the root of the nose to the junctions of the chin and neck.
The point between the eye brow in known as the glabella.
196

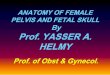
The fetal skull…Land marks of the fetal skull Occipput
VertexSinciput
Posterior fontanel (Lambda)Glabella
Mentum (chin)Anterior fontanel (Bregma)
Occipital protuberance
197

The fetal skull…Diameters of the fetal skull♣ Transverse Diameters Biparietal diameter- between the parietal
eminenences and measures 9.5cm • Engagement occur as this diameter pass through the
plane of the brim. Bi- temporal diameter – runs between the two
extremities of the coronal sutures and is 8.2cm in length.
Bi-acromial diameter – extends between the acromial processes of the scapulae, and measures 11.5cm.
Bi- trochenteric diameter – runs between the greater trochanters of the femur, and measures 9cm in length.
198

The fetal skull…
Anteroposterior or longitudinal diameters Subocipitobregmatic- measured from below the occiput
to the bregma. It measures 9.5cm. Suboccipito frontal – measured from below occipital
protuberance to the center of the frontal sutures, and measures 10cm.
Occipito frontal – measured between the occiput and the glabella. It is 11.5 cm in length
Mento-vertical – measured from the point of the chin to the highest point on the vertex slightly nearer to posterior fontanel then anterior, and it measures 13.5cm.
199

The fetal skull…
Submento vertical – measured from the point where the chin joins the neck to the highest point on the vertex. It is 11.5 cm in length
Submentobregmatic - measure from the point where the chin joins the neck to the center of the bregma and measures 9.5 cm
200

The fetal skull…
The scalp tissue There are five layers of scalp tissue :• Skin containing hairs, (outer covering)• Subcutaneous tissue • Muscle layer – containing the tendon of
Galea• Connective tissue – a loose layer • Periosteum – which coves the skull bones
201

The fetal skull…
Two conditions involving these tissue can arise during labor and both cause a swelling on the infant’s head.
1.Caput succedaneum – is an edematous swelling of the subcutaneous tissues of the fetal skull.
It occurs in early rupture of membranes in the 1st stage of labor, because there is no bag of fore waters to take the pressure of dilating cervix off the fetal head. 202

The fetal skull…
♠ CharacteristicsIt is present at birth Occurs on the part of the head which lies
over the inter as It may lie over a suture line It pits on pressure It disappears with in 24 - 48hrsNo treatment required unless it is
excessive 203

The fetal skull…
2.Cephelo hematoma – this swelling is due to bleeding between the skull bone and periosteum which covers it.
The bleeding occurs because of friction between the skull bones and the periosteum.
♠ Characteristics • It is not present at birth, but appears 2-3 days
after wards .• The swellings is limited by the periosteum and
can there fore only occur over the bone , although it may be bilateral .
• It can not lie over a suture.204

The fetal skull…
• The head is usually red- and bruised in appearance.
• It takes 6 weeks to disappear completely .• Treatment is only required of the
hematoma increase in size over a number of days.
• RX- vit. K, injection to raise the prothrombin level and assist clotting .
205

The fetal skull…
Moulding • Is the change which takes place in the shape of
the fetal skull as pass through the birth canal.• As the head descends through the pelvis in
response to the down ward pressure of uterine contractions, so the skull bones over up each other.
• Molding takes place gradually with out being prolonged, the cerebral membranes and blood vessels are not likely to be demaged .
206

The fetal skull…
• The dangerous types of molding are : Excessive molding Occurs when labor is prolonged or where the
skull bones are not completely ossified ( as in prematurity ).
Upward molding Occurs when the baby delivers in the persistent
occipito posterior position and the after coming head of the breech passes through the pelvis.
It can result in intracranial hemorrhage .207

The fetal skull…
Rapid molding Occurs in a precipitate delivery, and during the
delivery of the head of breach presentation. Results from rapid compression and
decompression of the head which can rupture of the cerebral membrane .
The infant is subjected to severe molding will suffer some degree of asphyxia at birth as a result of intracranial compression, thus they should be seen by pediatrician and get vit .K (0.5-mg/kg). 208

209