Embed Size (px)
DESCRIPTION
PPR Clinical Vetting Session:. November 1 st 2010. Identification of clinically unrelated readmissions designated as preventable. It will always be possible to identify individual cases for which the readmission was a) probably planned or b) probably not preventable - PowerPoint PPT Presentation
Citation preview

PPR Clinical Vetting Session:
November 1st 2010

Identification of clinically unrelated readmissions designated as preventable
• It will always be possible to identify individual cases for which the readmission was a) probably planned or b) probably not preventable
• Identifying exceptions to the PPR logic misses the point of a system that is based on rates, and seeks to identify deviation from expected performance based on peer-hospital rates
• It is precisely because of the impossibility of specifying all possible rules, exceptions, and details for what constitutes a preventable readmission that the PPR system is built upon the comparison of rates.

Identification of clinically unrelated readmissions designated as preventable - 2
• The guiding principle in identifying combinations of initial admissions and readmissions that might be potentially preventable was the following:
– If a hospital has a rate of a particular kind of readmission that is substantially higher than its peer hospitals, then reasonable clinicians would be concerned that a problem with the quality of patient care existed.
• Unless the APR DRG pair that constitutes a potentially preventable readmission can be demonstrated to be typically planned or unpreventable, then the existing logic, which was the product of an intensive iterative process of clinical hypothesis generation and testing, should stand.

How responsible is the discharging hospital for readmissions for the
deterioration of a chronic condition?

Time Interval for Preventable Readmissions

Risk Adjustment – APR DRG Severity of Illness Levels

Top 10 Medical APR DRGs for Frequency of PPRs, by SOI (Florida 2005-2006)
Medical APR DRG All Pts SOI 1 SOI 2 SOI 3 SOI 4
194 Heart FailureChains 15,053 1,304 8,151 4,675 923
Rate 12.5 8.9 11.7 15.0 19.4
140 Chronic Obstructive Lung DiseaseChains 8,271 1,737 3,745 2,416 373
Rate 9.7 7.3 9.3 12.7 17.3
750 SchizophreniaChains 7,592 3,382 3,931 251 28
Rate 17.7 17.1 18.1 20.8 16.8
139 Other PneumoniaChains 7,579 393 3,295 3,394 497
Rate 7.7 2.7 6.5 11.4 16.4
751 Major Depressive DisorderChains 5,608 1,814 3,391 339 64
Rate 10.9 8.3 12.6 16.5 10.8
198Angina Pectoris & Coronary
Atherosclerosis
Chains 5,151 1,414 2,685 982 70
Rate 5.6 3.7 6.2 9.9 17.3
753 Bipolar DisordersChains 4,830 2,366 2,260 179 25
Rate 14.0 12.7 15.3 18.8 11.6
720 Septicemia & Disseminated InfectionChains 4,370 46 881 1,808 1,635
Rate 12.6 3.6 8.3 12.7 19.3
460 Renal FailureChains 4,288 92 471 3,250 475
Rate 12.8 11.0 10.6 12.5 21.1
201 Card Arrhythmia & Conduction DisturbanceChains 4,066 898 1,950 1,070 148
Rate 6.3 4.0 6.4 10.2 16.0
All Other Medical APR DRGsChains 41,412 8,036 15,942 13,011 4,423
Rate 2.9 1.7 2.5 5.0 9.4
Total Medical APR-DRG Chains 108,220 21,482 46,702 31,375 8,661
Rate 5.0 3.2 4.7 7.4 11.7

Top 10 Surgical APR DRGs for Frequency of PPRs, by SOI (Florida 2005-2006)
Surgical APR DRG All Pts SOI 1 SOI 2 SOI 3 SOI 4
175 Percutaneous Cardiovascular Procs w/o AMIChains 7,260 3,222 2,850 1,043 145
Rate 7.9 6.4 9.0 12.7 14.8
221 Major Small & Large Bowel ProceduresChains 3,426 606 1,201 913 706
Rate 9.4 6.0 8.3 11.1 19.5
173 Other Vascular ProceduresChains 3,186 627 1,140 1,075 344
Rate 11.3 6.9 10.2 16.9 23.7
174Percutaneous Cardiovascular Procedures with
AMI
Chains 3,115 791 1,288 648 388
Rate 9.8 6.4 10.0 14.4 18.5
165 Coronary Bypass with Cath or PCIChains 2,638 101 909 1,073 555
Rate 12.3 7.2 9.3 13.9 21.5
301 Hip Joint ReplacementChains 2,870 1,123 1,106 445 196
Rate 6.2 5.1 6.0 8.9 21.4
308Hip/femur Procedure x Joint Replacement d/t
Trauma
Chains 2,395 234 1,115 835 211
Rate 8.0 4.9 6.9 10.6 19.5
302 Knee Joint ReplacementChains 2,373 780 1,323 233 37
Rate 4.0 2.9 4.5 7.4 13.1
161 Cardiac Defibrillator & Heart Assist ImplantChains 2,048 113 614 1,132 189
Rate 9.3 4.9 7.4 11.1 16.9
171 Perm Card Pacemaker w/o AMI, CHF, or ShockChains 2,044 523 1,068 382 71
Rate 8.1 5.5 8.7 12.7 19.6
All Other SurgicalChains 36,608 8,940 13,142 10,196 4,330
Rate 6.1 3.2 6.2 12.4 18.6
Total Surgical APR-DRG Chains 67,963 17,060 25,756 17,975 7,172
Rate 6.8 4.0 6.8 12.3 19.0

Predicted v. Actual Number of PPRs for Reporting Year 2007Florida, Selected APR DRGs (Based on Calendar Year 2005 Rate)
Admission Volume
APR Description SOICY 05
PPR RateRY07
Volume Predicted Actual
540
Cesarean delivery
1 0.03% 56,689 15 16
2 0.06% 17,269 11 9
3 0.09% 4,820 4 2
4 0.98% 295 3 1
Sub Total 0.04% 79,073 33 28
139
Other pneumonia
1 3.14% 6,828 215 246
2 7.38% 21,987 1,622 1,677
3 12.71% 12,314 1,565 1,654
4 17.77% 1,387 246 222
Sub Total 8.58% 42,516 3,648 3,799
175
Percutaneous cardiovascular procedures w/o AMI
1 7.90% 20,312 1,604 1,474
2 11.15% 14,902 1,662 1,596
3 15.84% 4,906 777 761
4 18.04% 639 115 164
Sub Total 10.20% 40,759 4,158 3,995

Predicted v. Actual Number of PPRs for Reporting Year 2007Florida, Selected APR DRGs (Based on Calendar Year 2005 Rate)
APR Description SOI PPR Rate2007
Volume Predicted Actual
194
Heart failure
1 11.04% 4,852 535 591
2 14.61% 24,769 3,618 3,767
3 18.53% 14,833 2,748 2,820
4 18.38% 1,870 344 373
Sub Total 15.64% 46,324 7,245 7,551
750
Schizophrenia
1 21.26% 4,610 980 941
2 22.42% 10,138 2,273 2,407
3 25.44% 791 201 191
4 20.51% 45 9 12
Sub Total 22.23% 15,584 3,464 3,551
460
Renal failure
1 13.76% 387 53 47
2 13.29% 2,283 303 286
3 14.21% 16,040 2,279 2,258
4 18.17% 1,331 242 295
Sub Total 14.36% 20,041 2,878 2,886

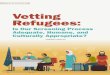
PPR Performance Florida data, FY 2005 vs RY 2006
• Pearson Correlation Coefficient = 0.9976(Calendar year ’05, Reporting year ’07)
• Hospital level R-square = 0.45

“Elective” Admissions as a proxy for planned readmissions

Readmissions with one of these procedures following an Initial Admission for DRG 301 (Total Hip Replacement)
WILL be considered preventable:
0070Revision of hip replacement, both acetabular and
femoral components
0071 Revision of hip replacement, acetabular component
0072 Revision of hip replacement, femoral component
0073Revision of hip replacement, acetabular liner and/or
femoral head only
8153 Revision of hip replacement, not otherwise specified

Readmissions with one of these procedures following an Initial Admission for DRG 301 (Total Hip Replacement) will
be considered PLANNED, and not preventable:
0085 Resurfacing hip, total, acetabulum and femoral head
0086 Resurfacing hip, partial, femoral head
0087 Resurfacing hip, partial, acetabulum
8151 Total Hip Replacement
8152 Partial Hip Replacement

Re DRG 173 (Other Vascular Procedures)
• Readmissions for endovascular grafts following peripheral vascular procedures (procedure 3971) will be classified as planned.
• Re the suggestion that “Some patients cannot physiologically tolerate enough contrast and require 2 different vascular bypass
procedures in order to perform multiple grafting.”
– This is not only an unusually rare group of patients but should be
randomly distributed between hospitals.
– Thus this consideration does not merit excluding the entire group of readmissions, many of which are potentially preventable and should be adequately addressed in a rate-based system.

Re APR DRG 304 (Dorsal and Lumbar Fusion)
• Regarding the suggestion that “These fusion procedures may be done in a staged process requiring 2 separate planned admissions”:
– Based on consultation with orthopedists about this situation, staging is rarely done for dorsal and/or lumbar fusions.