Embed Size (px)
Citation preview

Nutrition and cancer II 137
metabolic alterations. The liver ultrasounds of patientswere done at the beginning and end of the treatment.The patients’ nutritional habits were evaluated as dailyfood consumption frequency in the premorbid period andat the end of the treatment.Results: The metabolic alteration parameters of thepatients before and after chemotherapy are presentedin the table.
Parameter Baseline After 6th cycle p
Body mass index 28.69±5.52 29.13±5.29 0.001Waist/hip ratio 0.826±0.006 0.849±0.063 <0.001Cholesterol level 221.36±48.88 221.32±48.67 0.993Trygliceride level 130.78±74.01 157.59±75.13 <0.001HDL 55.22±10.25 47.35±12.91 <0.001LDL 142.12±42.36 145.81±42.43 0.375Apo A1 153.81±21.28 134.02±21.15 <0.001Fasting blood glucose 106.08±40.54 109.87±38.81 0.488
Without significant alterations in the nutritional habits,TAC regimen caused to induce the risk of developingmetabolic syndrome-X in breast cancer patients. More-over, existence of steatohepatitis in all patients has risenfrom 34% to 55% during chemotherapy period.Conclusion: TAC regimen may give rise to the risk of de-veloping metabolic syndrome-X, which is associated withimportant cardiovascular and metabolic complications inthe future of breast cancer survivors.
Disclosure of Interest: None declared
PP292IN NEWLY DIAGNOSED ESOPHAGEAL CANCERPATIENTS SERUM PGE2 LEVELS ARE REDUCED AFTERNUTRITIONAL INTERVENTION WITH A MEDICAL FOODJ. Faber1,2, V.M. Spaander3, S.C. van Steenbergen4,A.P. Vos1,2, M. Berkhout1, C.H. Lamers4, H.C. Rumke5,H.W. Tilanus6, P.D. Siersema7, A. van Helvoort1, A. vander Gaast8. 1Nutricia Advanced Medical Nutrition,Danone Research, Wageningen, 2Department ofPharmacology & Pathophysiology, Utrecht Institute forPharmaceutical Sciences (UIPS), Utrecht, 3Departmentof Gastroenterology, Erasmus Medical Center,4Laboratory of Clinical and Tumor Immunology, ErasmusMC-Daniel den Hoed Cancer Center, 5VaxinosticsBV, University Vaccine Center Rotterdam Nijmegen,6Department of Surgery, Erasmus Medical Center,Rotterdam, 7Department of Gastroenterology andHepatology, University Medical Center Utrecht, Utrecht,8Department of Medical Oncology, Erasmus UniversityMedical Center, Rotterdam, Netherlands
Rationale: Immune function is compromised in manycancer patients due to host-, tumor- and treatment-related factors, leading to an increased risk of (infec-tious) complications. In the present study, the effectof a nutritionally complete, high protein medical foodenriched with fish oil, specific oligosaccharides andleucine on immune function was investigated in patientswith newly diagnosed esophageal cancer.Methods: In a randomized, double-blind, controlledstudy, 64 newly diagnosed esophageal cancer patients
consumed a daily dose of 400 ml medical food (FortiCareImmunopt™) or routine nutritional support for 4 weeksbefore treatment. Blood samples were taken at day 1(baseline) and day 28 to measure several immune param-eters. Additionally, 40 age-matched healthy volunteerswere included for baseline comparisons.Results: At baseline, patients (61±9 years) had a BMI of25±4 kg/ m2 and had lost 3.4±5.0 kg in the past 3 months.Patients and volunteers did not differ at baseline for exvivo stimulated blood mononuclear cells and no effect ofthe nutritional intervention could be detected. Severalinflammatory serum markers were significantly higher inpatients compared to volunteers at baseline (p < 0.05).After nutritional intervention, the serum PGE2 levels weresignificantly decreased in the medical food group andincreased in the routine group (p = 0.002). In addition,body weight and BMI increased significantly after themedical food intervention and the Eastern CooperativeOncology Group (ECOG) score improved in 17% of thepatients receiving the medical food, compared to 0% inthe routine group (p < 0.05).Conclusion: Nutritional intervention in newly diagnosedesophageal cancer patients with a high protein medicalfood enriched with fish oil, specific oligosaccharides andleucine significantly reduced serum levels of PGE2 andimproved body weight, BMI and ECOG score.
Disclosure of Interest: J. Faber Other: Employee of NutriciaAdvanced Medical Nutrition, Danone Research, Wageningen,The Netherlands, V. Spaander: None declared, S. van Steen-bergen: None declared, A. Vos Other: Employee of NutriciaAdvanced Medical Nutrition, Danone Research, Wageningen,The Netherlands, M. Berkhout Other: Employee of NutriciaAdvanced Medical Nutrition, Danone Research, Wageningen,The Netherlands, C. Lamers: None declared, H. Rumke: Nonedeclared, H. Tilanus: None declared, P. Siersema: None declared,A. van Helvoort Other: Employee of Nutricia Advanced MedicalNutrition, Danone Research, Wageningen, The Netherlands, A.van der Gaast: None declared
PP293PREVENTION OF ORAL AND ESOPHAGEAL RADIATIONMUCOSITIS WITH GLUTAMINE: A RETROSPECTIVE STUDYA. Vidal-Casariego1, A. Calleja-Fernandez1,M.D. Ballesteros-Pomar1, A. Urioste-Fondo1,D. Rodríguez-Domínguez2, E. Sanchez-Aparicio2,P.M. Vinals-Montes2, E. Palacios-Mena2, J.R. Rodríguez-Garrido2, I. Cano-Rodríguez1. 1Department ofEndocrinology and Nutrition, 2Department ofRadiotherapy, Complejo Asistencial de Leon, Leon, Spain
Rationale: Glutamine is a nutraceutic with antioxidantand immune functions that can protect from adverseeffects associated to radiation therapy.Methods: Retrospective, case-control study that includedpatients treated with radiotherapy (RTP) for head andneck cancer (H&N), esophagus (E), lymphoma (LY) orlung cancer (LU) during 2005 2009. Data about glutaminetreatment (initiated before RTP, during RTP, or no glu-tamine), mucositis apparition (oral or esophageal accord-ing WHO criteria), weight loss, malnutrition (BMI < 18.5),and nutrition support were collected. Normal distributionwas assessed using Kolmogorov-Smirnov test; quantitativedata were compared using t Student’s test and ANOVA (or
138 Poster presentations
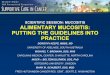
U Mann-Withney and Kruskal-Wallis), and qualitative datausing chi-square test. Odds ratio was calculated with 95%confidence interval (95% CI).Results: 84 patients were included, 77.4% males andmean age 63.9(11) yr; the diagnoses were H&N 73.8%,LU 16.7%, E 7.1%, and LY 2.4%. Treatment beganbefore RTP in 25.2%, during RTP in 44.8%, and 25%received no glutamine. The later had an OR of severemucositis of 3.5 (95% CI 1.3 9.8). The table summa-rizes the relationship between glutamine and mucositis.Weight loss was different according no glutamine, lateor precocious treatment [ 12.9(7.7)% vs 9.6(8.5)% vs5.3(4.7)%; p = 0.018], as well as tube feeding use (20% vs
4.3% vs 0%; p = 0.034). After adjusting for age, sex,previous nutritional status, and diagnosis, glutaminewas associated to less malnutrition (OR 0.001; 95% CI<0.001 0.31).
Glutamine treatment No mucositis(grade 0)
Moderate mucositis(grades 1 2)
Severe mucositis(grades 3 4)
No 9.5% 28.6% 61.9%During RTP 6.5% 60.9% 32.6%Before RTP 29.4% 41.2% 29.4%
p = 0.013
Conclusion: Glutamine may have a protective effect dur-ing RTP, preventing mucositis, weight loss, and nutritionsupport necessity. Prospective surveys are needed.
Disclosure of Interest: None declared
PP294ADHERENCE WITH THE ERAS-PROTOCOL ANDOUTCOMES AFTER COLO-RECTAL CANCER SURGERYU. Gustafsson1, J. Hausel2, A. Thorell2, O. Ljungqvist3,M. Soop4, J. Nygren2. 1Dep. of surgery, Ersta hospital.,2Dep. of surgery, Ersta hospital, Department ofClinical Sciences, Danderyd Hospital, KarolinskaInstitutet, 3Dept of Surgery, Orebro University, Inst. ofMolecular Medicine and Surgery, Karolinska Institutet,Stockholm, Sweden; 4Department of Surgery, Universityof Auckland, Auckland, New Zealand
Rationale: Instead of implementing a more complexmultimodal ERAS (enhanced recovery after surgery)-protocol, many surgical units are introducing selectedparts of the protocol mixed with traditional care. Thisstudy reports the impact of improved adherence to anevidence-based ERAS-protocol, and, the effects of variousERAS-elements on outcomes.Methods: The effect of improved adherence to the ERAS-protocol on postoperative symptoms, complications andlength of stay following major colo-rectal cancer surgerywas studied. Four hundred and sixty-four consecutivepatients treated in 2002 2004 were compared to 489consecutive patients treated in 2005 2007, i.e. beforeand after reinforcement of an ERAS-protocol. All clinicaldata (114 variables) were prospectively recorded.Results: The overall preoperative adherence to the ERAS-protocol improved to 80.6% in 2005 2007 from 54.0% in2002 2004 (p < 0.001). Postoperative complications 165(33.7%) vs. 203 (43.8%), OR 0.73 (95% CI 0.55 0.98)were less common in 2005 2007 compared to 2002 2004.Perioperative intravenous fluid volumes and preoperativecarbohydrate drink were major independent predictors ofthese improvements in clinical outcomes.
Conclusion: Improved adherence to the ERAS-protocolresults in improved clinical outcomes following majorcolo-rectal cancer surgery.
Disclosure of Interest: None declared
PP295LAPAROSCOPIC-ASSISTED AND OPEN HIGH ANTERIORRESECTION WITHIN AN ERAS-PROTOCOLU.O. Gustafsson1, M. Kressner2, A. Thorell1,O. Ljungqvist3, J. Nygren1. 1Dep. of surgery, Erstahospital., Department of Clinical Sciences, DanderydHospital, Karolinska Institutet, 2Dep. of surgery, Erstahospital, Karolinska Inst., Department of MolecularMedicine and Surgery, Karolinska Institutet, 3Dept ofSurgery, Orebro University, Inst. of Molecular Medicineand Surgery, Karolinska Institutet, Stockholm, Sweden
Rationale: Despite no or relatively modest gains inshort-term outcomes comparing laparoscopic and opencolo-rectal surgery, laparoscopy is currently being im-plemented in clinical practise worldwide. In parallel,enhanced recovery after surgery (ERAS) programs areshown to improve postoperative recovery in open colo-rectal surgery. This study reports adherence to the ERAS-protocol and real-life outcomes in laparoscopic and opensurgery.Methods: The association between surgical approach(laparoscopic or open surgery), compliance to the ERAS-protocol, postoperative symptoms, complications andlength of stay following surgery was studied. BetweenJanuary 2007 and December 2009, ninety-six consec-utive patients underwent high anterior resection withlaparoscopic-assisted (n = 49) or open resection (n = 47).All clinical data, (114 variables) were prospectivelyrecorded.Results: The overall preoperative ERAS-protocol compli-ance was 82.7% in the laparoscopic group compared to86.8% in the open group (p < 0.155). There was no signifi-cant difference in postoperative complications 10.2% vs.14.9%, OR 0.69 (95% CI 0.16 3.02) or median hospital stay(4 vs. 5 days) in patients undergoing laparoscopic vs.open resection. The proportion of patients within targetlength of stay �3 was larger in the laparoscopic group,13 (26.5%) vs. 5 (10.6%), OR = 0.29 (95% CI 0.09 0.96).Conclusion: An ERAS setting facilitates the evaluation oflaparoscopic colorectal surgery by providing close auditand a firm framework for the perioperative process.Early recovery was achieved after both laparoscopic andopen resection using the ERAS program. Some recoveryvariables were improved in laparoscopic resection indi-cating benefits from minimally invasive techniques.
Disclosure of Interest: None declared