Embed Size (px)
Citation preview
1
PowerPoint Slides English Spanish Translation
Breast Cancer Survivorship: Diagnosis of Calcifications Video Transcript
Supervivencia al cáncer de mama: diagnóstico de calcificaciones Transcripción del video
Professional Oncology Education Breast Cancer Survivorship: Diagnosis of Calcifications Time: 29:40
Educación Oncológica Profesional Supervivencia al cáncer de mama: diagnóstico de calcificaciones Duración: 29:40
Marita Lazzaro, MSN, RN, ANP-BC Advanced Practice Nurse Cancer Prevention Center The University of Texas MD Anderson Cancer Center
Marita Lazzaro, MSN, RN, ANP-BC Enfermera de práctica avanzada Centro de Prevención del Cáncer Centro para el Cáncer MD Anderson de la Universidad de Texas
Hello. I am Marita Lazzaro, an adult nurse practitioner and women’s health nurse practitioner in the Cancer Prevention Center at [The] University of Texas MD Anderson Cancer Center. And I am going to be presenting today on Breast Cancer Survivorship: the Diagnosis of Calcifications.
Hola, Soy Marita Lazzaro, enfermera especializada en adultos y salud de la mujer en el Centro de Prevención del Cáncer en el Centro para el Cáncer MD Anderson de la Universidad de Texas. El tema de hoy es la supervivencia al cáncer de mama y el diagnóstico de calcificaciones.
2
The objectives of this lecture are upon completion participants will be able to understand the correlation between mammary calcifications and benign proliferative and pre-invasive breast disease; also identify the mammographic terminology associated with the benign and suspicious mammary calcifications; and to realize the importance of the concordance of imaging and pathology.
Los objetivos de hoy son que al finalizar esta disertación los participantes comprendan la correlación entre las calcificaciones mamarias y la patología mamaria benigna, proliferativa y preinvasiva; identificar la terminología mamográfica asociada con las calcificaciones mamarias benignas y sospechosas; y comprender el valor de hacer concordar las imágenes y la patología.
Let’s start with what exactly are calcifications. The term calcification is used to describe the calcified debris from cellular activity. In the breast this can be due to benign fibrocystic activity in the stromal fibrosis tissue or the glandular lobules, or due to a malignant process, in the ducts. Occasionally skin or vascular calcifications can be seen, but these tend to be easily recognizable and of benign etiology. Let’s discuss some of the concerning --- some of the facts concerning calcifications. First, the maj --- majority of calcifications are benign. They are considered a mammographic finding, are not palpable, and are not seen on ultrasound or MRI. A significant --- this is a significant reason why mammograms remain the gold standard of breast screening. Calcifications can be found on mammograms of women of any age, but are most prevalent in postmenopausal women. Calcifications can help identify pre-invasive breast cancer. And that’s why the mammograms continue to be our first line of testing and screening.
Comencemos con la definición de calcificaciones. Este término se utiliza para describir los detritos calcificados de la actividad celular. En la mama, esto puede deberse a la actividad fibroquística benigna en el tejido fibrótico estromal o en los lóbulos glandulares, o a un proceso maligno en los conductos. Ocasionalmente pueden observarse calcificaciones vasculares o de la piel, pero tienden a ser fácilmente reconocibles y de etiología benigna. Analicemos algunos de los datos relativos a las calcificaciones: la mayoría son benignas, se las considera un hallazgo mamográfico, no son palpables, y no se detectan en ecografías o resonancias magnéticas. Esta es una de las principales razones por las que las mamografías continúan siendo el parámetro por excelencia para el diagnóstico mamario. Las calcificaciones pueden encontrarse en mamografías de mujeres de cualquier edad, pero son más frecuentes en las posmenopáusicas. Además, pueden ayudar a identificar el cáncer de mama preinvasivo, y es por eso que son nuestra primera línea de análisis y detección.
3
Calcifications are -- can be of benign etiology. These include breast cysts filled with debris, hyalinizing or involuting fibroadenomas as they age they can form calcified areas. Fibrocystic changes, sclerosing adenosis, ductal hyperplasia without atypia are all forms of active fibrocystic breasts. Secreting lesions include papillomas, duct ectasia filled with debris. Trauma to the breast can also cause calcifications. This is usually in the form of fat necrosis. And, therefore, evid --- evidence of trauma needs to be documented in the chart as much as possible for future clarification. Radiation therapy can also cause calcifications to the breasts as the tissue ages. Again, vascular and dermal calcifications can be seen in the breast, but are usually not concerning for malignancy, as they are easily read as benign.
Las calcificaciones pueden ser de etiología benigna, que incluye quistes mamarios con detritos, y fibroadenomas hialinizados o involutivos, que a medida que envejecen pueden formar áreas calcificadas. Los cambios fibroquísticos como la adenosis esclerosante y la hiperplasia ductal sin atipia son tipos fibrosis mamaria activa. Las lesiones secretoras incluyen papilomas, ectasia ductal con detritos. El traumatismo mamario también puede causar calcificaciones, generalmente en forma de esteatonecrosis. Por eso, la evidencia de traumatismo debe ser documentada en la planilla para referencia futura. La radioterapia también puede causar calcificaciones en las mamas a medida que el tejido envejece. Pueden detectarse calcificaciones vasculares y dérmicas en la mama, pero no son motivo de preocupación, pues suelen ser benignas.
Next, you have suspicious etiology. In this, we get into the proliferative breast disease. This includes atypical proliferation or hyperplasia of the glandular cells of the mammary ducts. This is where you’ll hear people say, “I am very fibrocystic.” Or, multiple biopsies need to be done to determine if the findings on mammogram are benign or not. Flat epithelial atypia is the new terminology that has been --- come out within the last few years, and is felt to be a pre-curser to the next level, which is atypical ductal hyperplasia or commonly called ADH. In some cases, it is felt that flat epithelial atypia and atypical ductal hyperplasia are actually one in the same.
Luego tenemos la etiología sospechosa. Aquí analizamos la patología mamaria proliferativa, que incluye la proliferación atípica o hiperplasia de las células glandulares de los conductos mamarios. Se dice entonces que la paciente es fibroquística. Deben hacerse múltiples biopsias para determinar si los hallazgos en la mamografía son benignos o no. “Atipia epitelial plana” es la nueva terminología que ha surgido en los últimos años, y se le considera precursora del siguiente nivel, la hiperplasia ductal atípica o ADH. En algunos casos, se considera que la atipia epitelial plana y la hiperplasia ductal atípica son la misma enfermedad.
4
Finally, we get into malignant etiology. This is what is commonly called ductal carcinoma in situ, or DCIS. This is a pre-invasive disease. It is intra-ductal carcinoma. And its stage is Stage 0 or Tis, which stands for in situ or still contained within the duct. Usually DCIS is not palpable. It can be felt if there are a number of ducts that have the DCIS present. A cluster of ducts with the DCIS will feel as a vague thickening or mass on the breast exam.
Por último, analicemos la etiología maligna, comúnmente denominada carcinoma ductal in situ o DCIS. Es una enfermedad preinvasiva, un carcinoma intraductal de etapa 0 o Tis, que significa in situ o contenido en el conducto. Generalmente no es palpable, pero se puede sentir si hay varios conductos afectados. Un grupo de conductos con DCIS se siente como un leve engrosamiento o masa en el examen de mamas.
Malignant Etiology: Pre-invasive disease is a dynamic process. Flat epithelial atypia if unchecked will turn into atypical ductal hyperplasia. Fifteen to 20% on biopsy through recent studies have shown that when excised DCIS was found in place or beside the atypical ductal hyperplasia. As you move on, if left alone, DCIS will then become evident. Twelve to 20% of excisions were upgraded to invasive disease. Focal invasion may also be present, and is noted as T1a. It is a dynamic process as stated above. That means it has time to move between the atypical ductal hyperplasia and the focal invasion. An area --- a mass about the size of a pea may take anywhere from one to five years to actually present. DCIS is a pathologic diagnosis. We do not diagnose this by imaging. We just identify areas of concern. Biopsy must be done.
En la etiología maligna, la enfermedad preinvasiva es un proceso dinámico. Si no se le controla, la atipia epitelial plana se convertirá en hiperplasia ductal atípica. En el 15 al 20% de las biopsias tomadas en estudios recientes se detectó, luego de la extirpación, DCIS solo o concomitante con la hiperplasia ductal atípica. Si no se lo trata, el carcinoma ductal in situ se tornará evidente. Del 12 al 20% de las extirpaciones se clasificaron como enfermedad invasiva. La invasión focal también puede estar presente y se la indica como T1a. Es un proceso dinámico, con tiempo para cambiar de hiperplasia ductal atípica a invasión focal. Una masa del tamaño de un guisante puede tardar de uno a cinco años en presentarse. El DCIS es un diagnóstico patológico. No se le diagnostica por imágenes, sino que se identifican áreas dudosas y se realiza una biopsia.
5
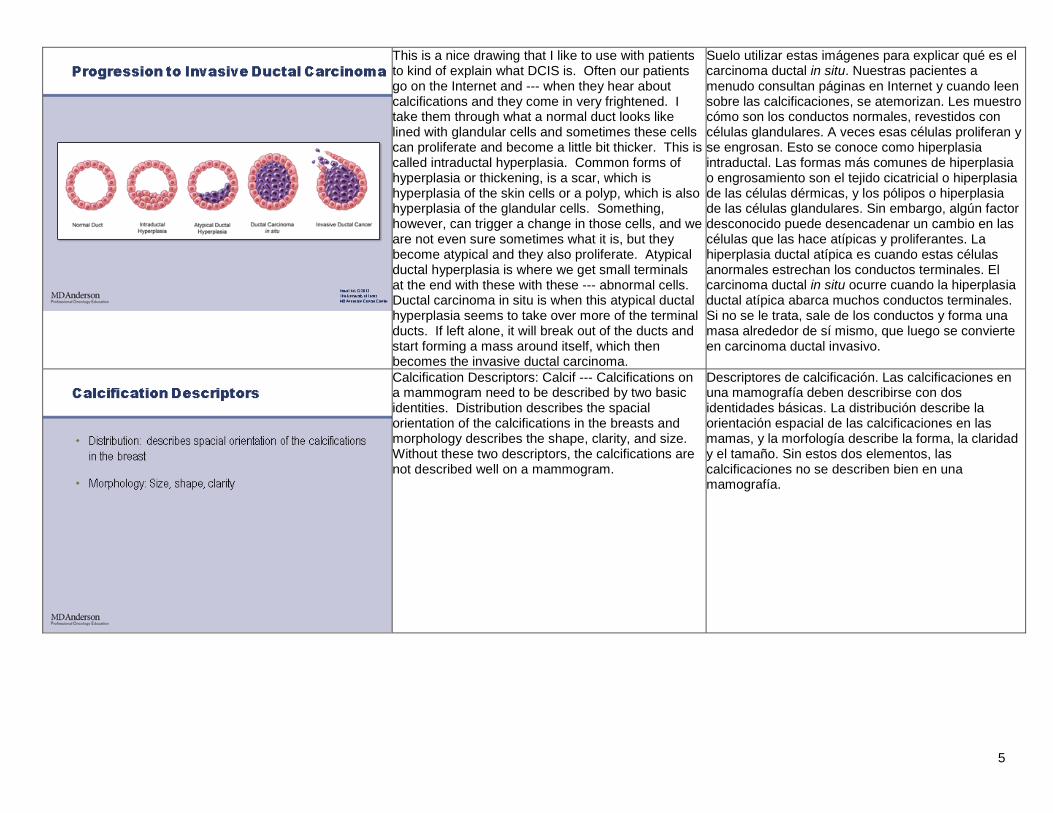
This is a nice drawing that I like to use with patients to kind of explain what DCIS is. Often our patients go on the Internet and --- when they hear about calcifications and they come in very frightened. I take them through what a normal duct looks like lined with glandular cells and sometimes these cells can proliferate and become a little bit thicker. This is called intraductal hyperplasia. Common forms of hyperplasia or thickening, is a scar, which is hyperplasia of the skin cells or a polyp, which is also hyperplasia of the glandular cells. Something, however, can trigger a change in those cells, and we are not even sure sometimes what it is, but they become atypical and they also proliferate. Atypical ductal hyperplasia is where we get small terminals at the end with these with these --- abnormal cells. Ductal carcinoma in situ is when this atypical ductal hyperplasia seems to take over more of the terminal ducts. If left alone, it will break out of the ducts and start forming a mass around itself, which then becomes the invasive ductal carcinoma.
Suelo utilizar estas imágenes para explicar qué es el carcinoma ductal in situ. Nuestras pacientes a menudo consultan páginas en Internet y cuando leen sobre las calcificaciones, se atemorizan. Les muestro cómo son los conductos normales, revestidos con células glandulares. A veces esas células proliferan y se engrosan. Esto se conoce como hiperplasia intraductal. Las formas más comunes de hiperplasia o engrosamiento son el tejido cicatricial o hiperplasia de las células dérmicas, y los pólipos o hiperplasia de las células glandulares. Sin embargo, algún factor desconocido puede desencadenar un cambio en las células que las hace atípicas y proliferantes. La hiperplasia ductal atípica es cuando estas células anormales estrechan los conductos terminales. El carcinoma ductal in situ ocurre cuando la hiperplasia ductal atípica abarca muchos conductos terminales. Si no se le trata, sale de los conductos y forma una masa alrededor de sí mismo, que luego se convierte en carcinoma ductal invasivo.
Calcification Descriptors: Calcif --- Calcifications on a mammogram need to be described by two basic identities. Distribution describes the spacial orientation of the calcifications in the breasts and morphology describes the shape, clarity, and size. Without these two descriptors, the calcifications are not described well on a mammogram.
Descriptores de calcificación. Las calcificaciones en una mamografía deben describirse con dos identidades básicas. La distribución describe la orientación espacial de las calcificaciones en las mamas, y la morfología describe la forma, la claridad y el tamaño. Sin estos dos elementos, las calcificaciones no se describen bien en una mamografía.
6
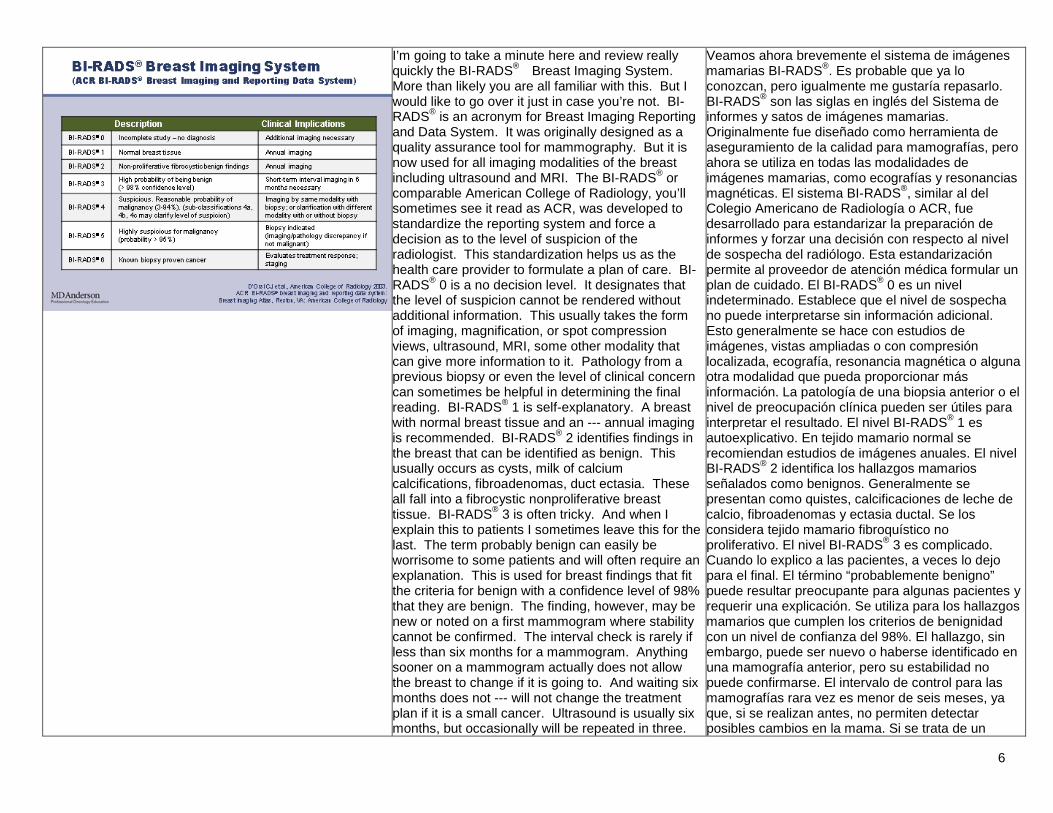
I’m going to take a minute here and review really quickly the BI-RADS® Breast Imaging System. More than likely you are all familiar with this. But I would like to go over it just in case you’re not. BI-RADS® is an acronym for Breast Imaging Reporting and Data System. It was originally designed as a quality assurance tool for mammography. But it is now used for all imaging modalities of the breast including ultrasound and MRI. The BI-RADS® or comparable American College of Radiology, you’ll sometimes see it read as ACR, was developed to standardize the reporting system and force a decision as to the level of suspicion of the radiologist. This standardization helps us as the health care provider to formulate a plan of care. BI-RADS® 0 is a no decision level. It designates that the level of suspicion cannot be rendered without additional information. This usually takes the form of imaging, magnification, or spot compression views, ultrasound, MRI, some other modality that can give more information to it. Pathology from a previous biopsy or even the level of clinical concern can sometimes be helpful in determining the final reading. BI-RADS® 1 is self-explanatory. A breast with normal breast tissue and an --- annual imaging is recommended. BI-RADS® 2 identifies findings in the breast that can be identified as benign. This usually occurs as cysts, milk of calcium calcifications, fibroadenomas, duct ectasia. These all fall into a fibrocystic nonproliferative breast tissue. BI-RADS® 3 is often tricky. And when I explain this to patients I sometimes leave this for the last. The term probably benign can easily be worrisome to some patients and will often require an explanation. This is used for breast findings that fit the criteria for benign with a confidence level of 98% that they are benign. The finding, however, may be new or noted on a first mammogram where stability cannot be confirmed. The interval check is rarely if less than six months for a mammogram. Anything sooner on a mammogram actually does not allow the breast to change if it is going to. And waiting six months does not --- will not change the treatment plan if it is a small cancer. Ultrasound is usually six months, but occasionally will be repeated in three.
Veamos ahora brevemente el sistema de imágenes mamarias BI-RADS®. Es probable que ya lo conozcan, pero igualmente me gustaría repasarlo. BI-RADS® son las siglas en inglés del Sistema de informes y satos de imágenes mamarias. Originalmente fue diseñado como herramienta de aseguramiento de la calidad para mamografías, pero ahora se utiliza en todas las modalidades de imágenes mamarias, como ecografías y resonancias magnéticas. El sistema BI-RADS®, similar al del Colegio Americano de Radiología o ACR, fue desarrollado para estandarizar la preparación de informes y forzar una decisión con respecto al nivel de sospecha del radiólogo. Esta estandarización permite al proveedor de atención médica formular un plan de cuidado. El BI-RADS® 0 es un nivel indeterminado. Establece que el nivel de sospecha no puede interpretarse sin información adicional. Esto generalmente se hace con estudios de imágenes, vistas ampliadas o con compresión localizada, ecografía, resonancia magnética o alguna otra modalidad que pueda proporcionar más información. La patología de una biopsia anterior o el nivel de preocupación clínica pueden ser útiles para interpretar el resultado. El nivel BI-RADS® 1 es autoexplicativo. En tejido mamario normal se recomiendan estudios de imágenes anuales. El nivel BI-RADS® 2 identifica los hallazgos mamarios señalados como benignos. Generalmente se presentan como quistes, calcificaciones de leche de calcio, fibroadenomas y ectasia ductal. Se los considera tejido mamario fibroquístico no proliferativo. El nivel BI-RADS® 3 es complicado. Cuando lo explico a las pacientes, a veces lo dejo para el final. El término “probablemente benigno” puede resultar preocupante para algunas pacientes y requerir una explicación. Se utiliza para los hallazgos mamarios que cumplen los criterios de benignidad con un nivel de confianza del 98%. El hallazgo, sin embargo, puede ser nuevo o haberse identificado en una mamografía anterior, pero su estabilidad no puede confirmarse. El intervalo de control para las mamografías rara vez es menor de seis meses, ya que, si se realizan antes, no permiten detectar posibles cambios en la mama. Si se trata de un
7
Several years ago benign-appearing, but new or increasing calcifications were often followed for a series of six months to show stability, sometimes every six months for two years. But with the advent of the minimally invasive and affordable stereotactic biopsy, calcifications in question now are rarely followed. Biopsy is usually recommended as a definitive diagnosis, and, therefore, reduces the risk of extra radiation, okay, to follow something that is benign. BI-RADS® 3 is now frequently used to show stability of asymmetric tissue on mammograms or benign findings, and is followed with the same imaging modality, such as mammogram follows mammogram in six months, if it is a mammogram finding. And ultrasound follows ultrasound in six months if it is an ultrasound finding. We usually don’t mix the modalities when we are doing stability. BI-RADS® 4 is described as a mammographic finding that requires additional imaging, such as diagnostic mamma --- mammographic views, ultrasound, MRI, and/or biopsy to clarify the level of concern. BI-RADS® 4 carries a reasonable probability of malignancy ranging from 3-94%. As you can see, the range is fairly wide. Therefore, subdivisions of BI-RADS® 4a, b, or c are being proposed by the American College of Radiologists to help clarify for the health care provider what the true level of suspicion is. BI-RADS® 5 is simply a finding that by imaging suggests a cancer with a confidence level of greater than 95%. It should be viewed as a cancer unless proven otherwise. As you know, the diagnosis of malignancy requires tissue sampling and cannot be made by imaging of the breast alone. This level, therefore, requires a biopsy. A benign pathology on biopsy will require either additional biopsies or should be presented in a multiply --- a multiple disciplinary review to --- because it is discordant. The last category, BI-RADS® 6 is used when a cancer has been verified by tissue sampling and monitoring or additional imaging is required. It’s often used for staging to show the extent of the disease in the breast, or to assess treatment response.
cáncer pequeño, una demora de seis meses no alterará el plan de tratamiento. La ecografía suele realizarse cada seis meses, pero puede repetirse cada tres. Hace unos años, las calcificaciones nuevas o crecientes de aspecto benigno solían controlarse a intervalos de seis meses para comprobar su estabilidad, y a veces cada dos años. Con el advenimiento de la biopsia estereotáxica mínimamente invasiva y accesible, en raras ocasiones se realizan seguimientos de calcificaciones. La biopsia generalmente se recomienda como diagnóstico definitivo, ya que reduce el riesgo de radiación adicional para controlar problemas benignos. El nivel BI-RADS® 3 suele utilizarse para comprobar la estabilidad del tejido asimétrico en mamografías o hallazgos benignos. Luego se hacen seguimientos utilizando la misma modalidad: como mamografías de control cada seis meses, si se trata de un hallazgo mamográfico; y ecografías cada seis meses, si se trata de un hallazgo ecográfico. Al controlar la estabilidad, estas modalidades no suelen combinarse. El nivel BI-RADS® 4 se describe como un hallazgo mamográfico que requiere estudios de imágenes adicionales, como mamografías, ecografías, resonancias magnéticas o biopsias, para determinar el nivel de preocupación. BI-RADS® 4 tiene una probabilidad de malignidad del 3 al 94%. Es un rango bastante amplio. El Colegio Americano de Radiología ha propuesto subdividir este nivel en 4a, 4b y 4c para ayudar al profesional médico a determinar el verdadero nivel de sospecha. BI-RADS® 5 es simplemente un hallazgo cuyas imágenes sugieren cáncer con un nivel de confianza superior al 95%. Debe suponerse que es un cáncer, a menos que se demuestre lo contrario. El diagnóstico de malignidad requiere muestras de tejido y no puede basarse solo con imágenes de la mama. Este nivel requiere una biopsia. Una patología benigna en la biopsia requerirá biopsias adicionales o deberá presentarse en una revisión multidisciplinaria por su discordancia. La última categoría, BI-RADS® 6, se utiliza cuando el cáncer ha sido verificado por muestras de tejido. Se requieren monitoreo o estudios de imágenes adicionales. Suele utilizarse para estadificación y
8
mostrar la extensión de la enfermedad en la mama, o para evaluar su respuesta al tratamiento.
As stated previously, subcas --- subclassifications of BI-RADS® 4 is proposed to clarify the level of radiology suspicion. 4a is low and considered a less than 10% probability of malignancy. 4b is to suggest intermediate with a 10-49% probability of cancer. And 4c is of moderate concern carrying a 50-95% probability of cancer. 4c is usually taken to biopsy. Greater than 95%, you jump into BI-RADS® 5 and is considered as highly suspicions. Expect all these calcification --- all these classifications to be finalized and in use by sometime this fall. BI-RADS® reports identifying calcifications should always address the distribution and morphology of the calcifications.
Como ya mencionamos, las subclasificaciones de BI-RADS® 4 se proponen para determinar el grado de sospecha radiológica. 4a es baja, con una probabilidad de malignidad inferior al 10%. 4b sugiere una probabilidad intermedia de cáncer del 10 al 49%. 4c es una preocupación moderada, con una probabilidad de cáncer del 50 al 95%, y generalmente requiere una biopsia. Con una probabilidad superior al 95%, se pasa al nivel BI-RADS® 5 y se considera altamente sospechoso. Estas clasificaciones estarán definidas próximamente y pronto comenzarán a utilizarse. Los informes de BI-RADS® que identifican calcificaciones siempre deben indicar la distribución y morfología de las calcificaciones.
Let’s take a look at benign distribution. When you receive a mammogram report, benign eti --- terminology is such as diffuse, scattered, global. Global means scattered around and not clustered together. Clustering means that they may be actually formed inside a duct. Random calcifications throughout the breast is often used in the mammogram report. It’s usually bilateral and can be minimal to extensive. Usually annual imaging is recommended on these --- these benign --- these calcifications.
Analicemos la distribución benigna. Cuando se recibe un informe de mamografía, la terminología benigna incluye palabras como “difusa”, “dispersa”, “global”, que significa distribuida y no agrupada. Una distribución “agrupada” significa que las calcificaciones pueden estar dentro de un conducto. “Calcificaciones aleatorias en la mama” también se utiliza en los informes mamográficos. Suelen ser “bilaterales” y pueden ser “mínimas” o “extensas”. Para estas calcificaciones se recomiendan estudios de imágenes anuales.
9
Benign Morphology: You’ll see terminology such as coarse or popcorn-like. This tends to be the sclerosing adenosis or the stromal fibrosis. Punctate or round usually tends to be more the milk of calcium, which is also called layering. Dystrophic calcifications tend to go along again with fibrocystic changes, maybe related to injury or trauma. Egg shell or rim, lucent centered, all of these with the distribution as benign go for or end up recommending an annual mammogram.
Morfología benigna. Veremos terminología como “gruesa” o “granular”. Esto tiende a ser la adenosis esclerosante o la fibrosis estromal. “Puntiforme” o “redonda” suelen utilizarse con la leche de calcio, que también se llama estratificación. Las calcificaciones “distróficas” están relacionadas con cambios fibroquísticos, así como con una lesión o traumatismo. “Periférica”, “anular” y “centro radiolucente” se relacionan con la distribución benigna y se recomienda una mamografía anual.
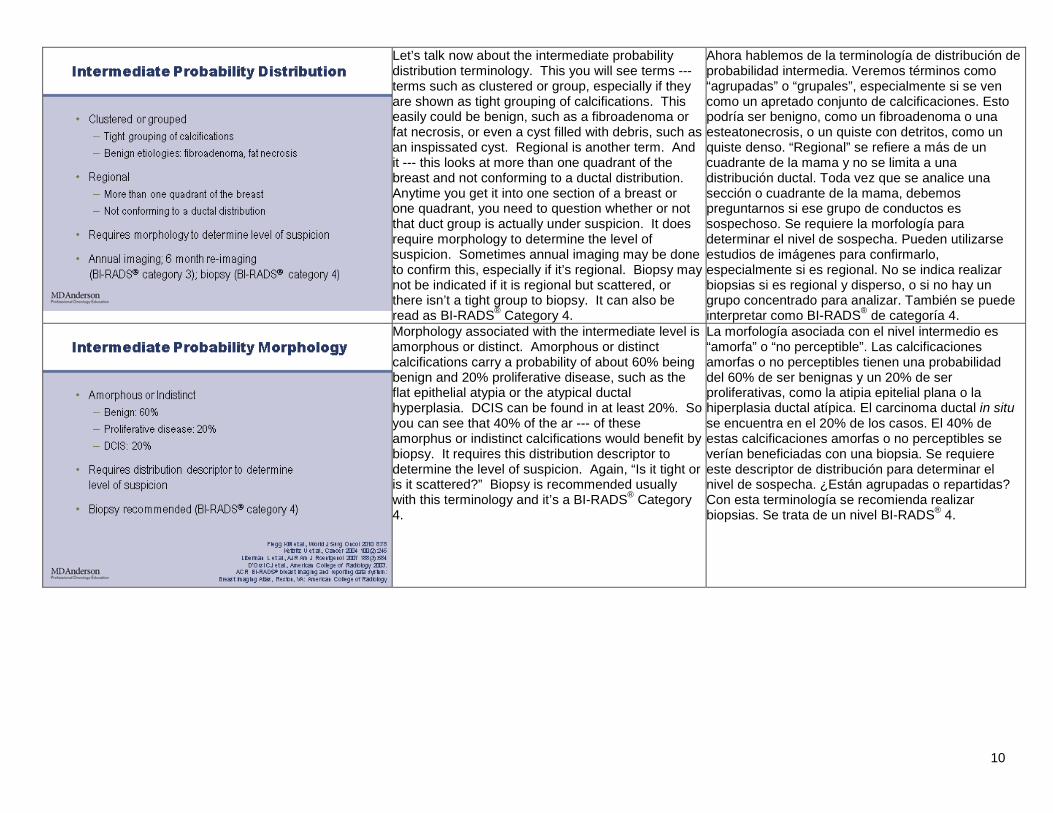
Here is an example of benign ka --- report and what it looks like. Distribution is diffuse and scattered. As you can see, there’s multiple calcifications all around. Here you will see a lucent centered and that’s morphology, or egg shell or rim calcifications. This tends to be a fat necrosis or cystic area and use --- is read as a BI-RADS® 2 requiring annual imaging.
Este es un ejemplo de un informe benigno. La distribución es difusa y dispersa. Hay múltiples calcificaciones en toda la mama. Se observan calcificaciones con centro radiolucente y periféricas. Esto suele ser una esteatonecrosis o área quística de nivel BI-RADS® 2 y requiere estudios de imágenes anuales.
10
Let’s talk now about the intermediate probability distribution terminology. This you will see terms --- terms such as clustered or group, especially if they are shown as tight grouping of calcifications. This easily could be benign, such as a fibroadenoma or fat necrosis, or even a cyst filled with debris, such as an inspissated cyst. Regional is another term. And it --- this looks at more than one quadrant of the breast and not conforming to a ductal distribution. Anytime you get it into one section of a breast or one quadrant, you need to question whether or not that duct group is actually under suspicion. It does require morphology to determine the level of suspicion. Sometimes annual imaging may be done to confirm this, especially if it’s regional. Biopsy may not be indicated if it is regional but scattered, or there isn’t a tight group to biopsy. It can also be read as BI-RADS® Category 4.
Ahora hablemos de la terminología de distribución de probabilidad intermedia. Veremos términos como “agrupadas” o “grupales”, especialmente si se ven como un apretado conjunto de calcificaciones. Esto podría ser benigno, como un fibroadenoma o una esteatonecrosis, o un quiste con detritos, como un quiste denso. “Regional” se refiere a más de un cuadrante de la mama y no se limita a una distribución ductal. Toda vez que se analice una sección o cuadrante de la mama, debemos preguntarnos si ese grupo de conductos es sospechoso. Se requiere la morfología para determinar el nivel de sospecha. Pueden utilizarse estudios de imágenes para confirmarlo, especialmente si es regional. No se indica realizar biopsias si es regional y disperso, o si no hay un grupo concentrado para analizar. También se puede interpretar como BI-RADS® de categoría 4.
Morphology associated with the intermediate level is amorphous or distinct. Amorphous or distinct calcifications carry a probability of about 60% being benign and 20% proliferative disease, such as the flat epithelial atypia or the atypical ductal hyperplasia. DCIS can be found in at least 20%. So you can see that 40% of the ar --- of these amorphus or indistinct calcifications would benefit by biopsy. It requires this distribution descriptor to determine the level of suspicion. Again, “Is it tight or is it scattered?” Biopsy is recommended usually with this terminology and it’s a BI-RADS® Category 4.
La morfología asociada con el nivel intermedio es “amorfa” o “no perceptible”. Las calcificaciones amorfas o no perceptibles tienen una probabilidad del 60% de ser benignas y un 20% de ser proliferativas, como la atipia epitelial plana o la hiperplasia ductal atípica. El carcinoma ductal in situ se encuentra en el 20% de los casos. El 40% de estas calcificaciones amorfas o no perceptibles se verían beneficiadas con una biopsia. Se requiere este descriptor de distribución para determinar el nivel de sospecha. ¿Están agrupadas o repartidas? Con esta terminología se recomienda realizar biopsias. Se trata de un nivel BI-RADS® 4.
11
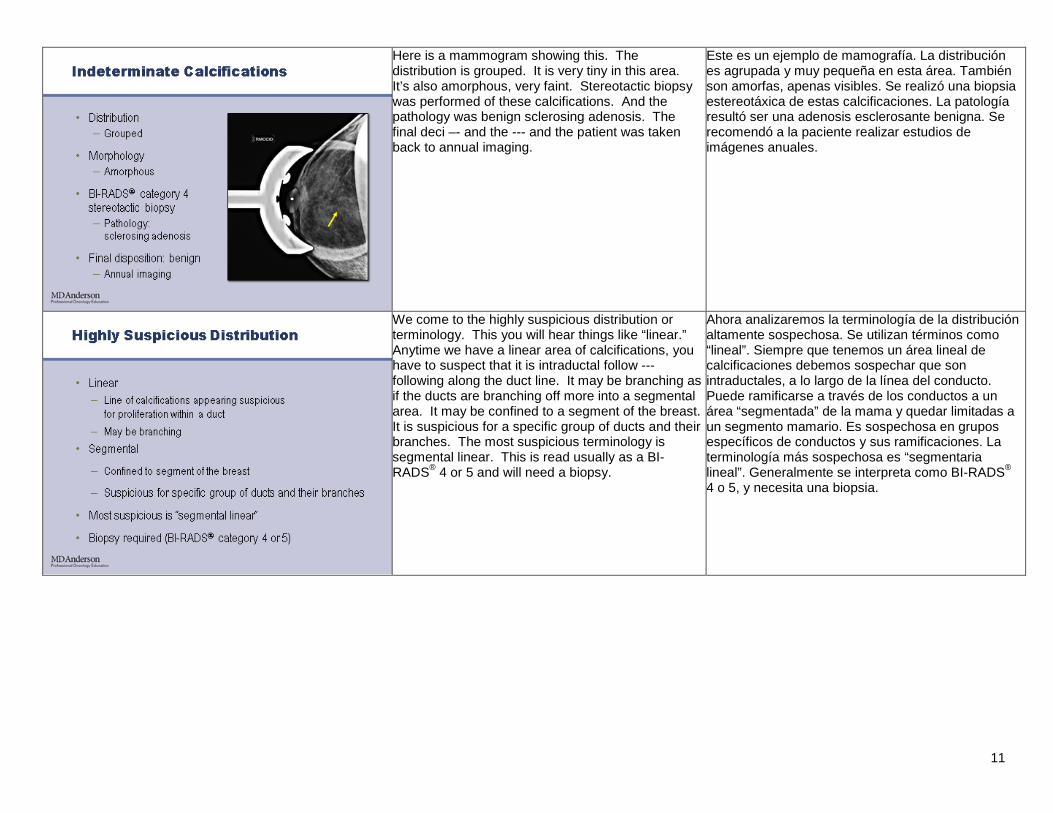
Here is a mammogram showing this. The distribution is grouped. It is very tiny in this area. It’s also amorphous, very faint. Stereotactic biopsy was performed of these calcifications. And the pathology was benign sclerosing adenosis. The final deci –- and the --- and the patient was taken back to annual imaging.
Este es un ejemplo de mamografía. La distribución es agrupada y muy pequeña en esta área. También son amorfas, apenas visibles. Se realizó una biopsia estereotáxica de estas calcificaciones. La patología resultó ser una adenosis esclerosante benigna. Se recomendó a la paciente realizar estudios de imágenes anuales.
We come to the highly suspicious distribution or terminology. This you will hear things like “linear.” Anytime we have a linear area of calcifications, you have to suspect that it is intraductal follow --- following along the duct line. It may be branching as if the ducts are branching off more into a segmental area. It may be confined to a segment of the breast. It is suspicious for a specific group of ducts and their branches. The most suspicious terminology is segmental linear. This is read usually as a BI-RADS® 4 or 5 and will need a biopsy.
Ahora analizaremos la terminología de la distribución altamente sospechosa. Se utilizan términos como “lineal”. Siempre que tenemos un área lineal de calcificaciones debemos sospechar que son intraductales, a lo largo de la línea del conducto. Puede ramificarse a través de los conductos a un área “segmentada” de la mama y quedar limitadas a un segmento mamario. Es sospechosa en grupos específicos de conductos y sus ramificaciones. La terminología más sospechosa es “segmentaria lineal”. Generalmente se interpreta como BI-RADS® 4 o 5, y necesita una biopsia.
12
The morphology associated with this distribution is pleomorphic. That’s one of the most common ones that you’ll see. Heterogeneous or gran --- granular: The probability of malignancy ranges in this group from 40-80% and is dependent upon the distribution characteristics. Such as, if it is linear and segmental and pleomorphic, you are usually reading it as a BI-RADS® Category 5. Fine, linear, or casting is the highest probability for ma --- for malignancy of calcifications, and usually is associated with a high grade ductal carcinoma in situ.
La morfología asociada con esta distribución es “pleomórfica”, que es una de las más comunes, “heterogénea” o “granular”. La probabilidad de malignidad en este grupo oscila entre el 40% y el 80%, y depende de las características de distribución. Por ejemplo, si es lineal, segmentaria y pleomórfica, suele interpretarse como BI-RADS® de categoría 5. Las calcificaciones finas, lineales o segmentarias tienen la probabilidad de malignidad más alta, y se las asocia con un alto grado de carcinoma ductal in situ.
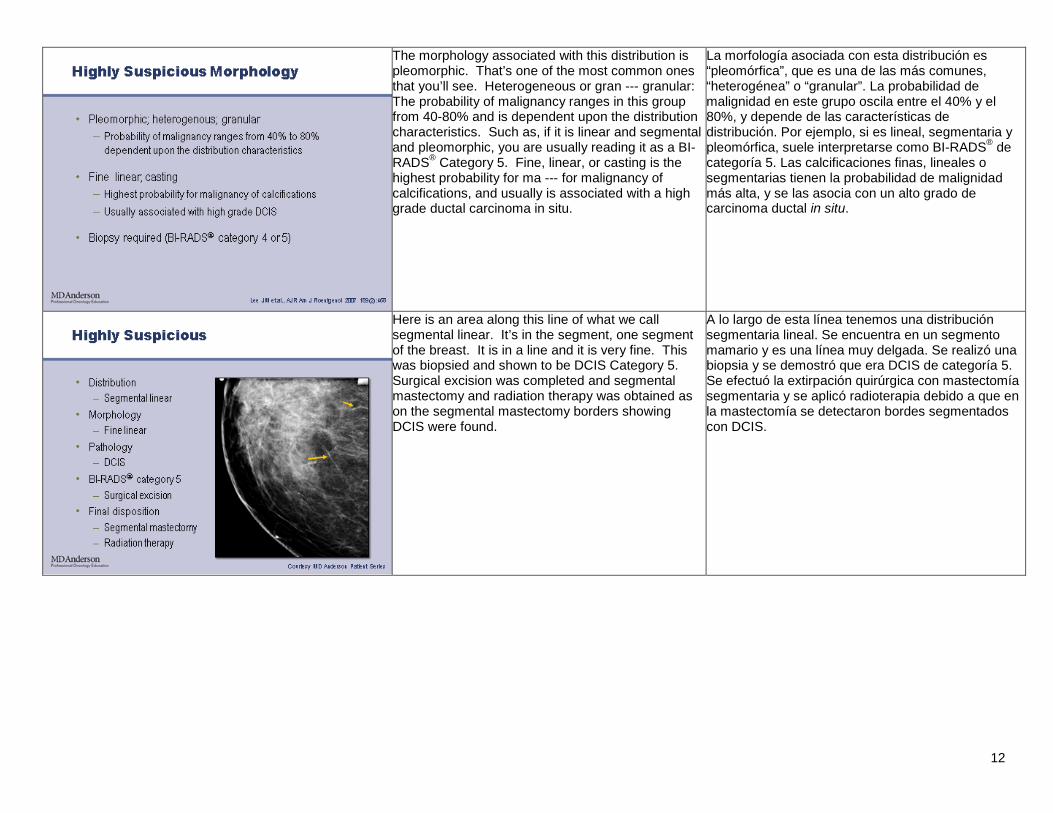
Here is an area along this line of what we call segmental linear. It’s in the segment, one segment of the breast. It is in a line and it is very fine. This was biopsied and shown to be DCIS Category 5. Surgical excision was completed and segmental mastectomy and radiation therapy was obtained as on the segmental mastectomy borders showing DCIS were found.
A lo largo de esta línea tenemos una distribución segmentaria lineal. Se encuentra en un segmento mamario y es una línea muy delgada. Se realizó una biopsia y se demostró que era DCIS de categoría 5. Se efectuó la extirpación quirúrgica con mastectomía segmentaria y se aplicó radioterapia debido a que en la mastectomía se detectaron bordes segmentados con DCIS.
13
As stated earlier, one of the most important things that we need to be concerned with as the health care provider reading this and explaining this and coordinating the plan of care for this patient is concordance of imaging and pathology. The majority of radiologists are as --- are assuming the responsibility, at this time, of addressing the concordance and documenting it on the addendum. However, you need to watch for this. Because if it is not present, then you may be the person to actually contact the pathologist or contact the radiologist as to whether or not, it is concordant or not. The provider must assure that this has been done before a plan of care can be created. If concordance is not there, it may need rebiopsy or you may need additional imaging. The following points will help guide you as to whether concordance is shown. First of all, “Was the sampling adequate?” That should say in the pathology report. “Were calcifications identified on the specimen radiograph?” This is very important and should be present on the films that you receive or have access to. “Were the calcifications identified on the pathology report?” So the calcifications have to be shown on the biopsy sample through mammogram, but they also have to be documented on the pathology report. If either one of them is not showing calcifications, then adequate sampling may not have been achieved. “Was adequacy questioned by the radiologist or pathologist?” Radiologists and pathologists are very sharp nowadays. And they will be the first ones to say we question whether or not this biopsy is adequate and would recommend a repeat. “Is the pathology concordant with the level of concern on imaging?” In other words, if I have a BI-RADS® 5 mammogram with linear and branching calcifications and I have a benign pathology report, that is not concordant. And one of the first things you have to check is whether or not sampling adequacy was achieved. BI-RADS® 4; however, can yield either benign proliferative disease or malignancy. BI-RADS® 5 should always yield malignant path --- pathology. If not, then it is discordant.
Una de las principales preocupaciones como proveedores de atención médica es explicar y coordinar el plan de cuidado de la paciente en concordancia con los estudios de imágenes y la patología. Actualmente, la mayoría de los radiólogos asume la responsabilidad de documentar la concordancia en el apéndice. Debemos estar atentos a esto porque, si no está presente, es posible que debamos comunicarnos con el patólogo o el radiólogo para determinar si es o no concordante. El proveedor debe asegurarse de esto antes de crear el plan de cuidado. Si no hay concordancia, es posible que deban realizarse una biopsia o estudios de imágenes adicionales. Los siguientes puntos servirán de guía para corroborar la concordancia. En primer lugar, ¿fue adecuado el muestreo? Eso debe figurar en el informe patológico. ¿Se identificaron las calcificaciones en la radiografía de la muestra? Esto es muy importante y debe estar presente en las placas que reciban o examinen. ¿Se identificaron calcificaciones en el informe patológico? Las calcificaciones deben aparecer en la muestra de la biopsia con mamografía y también deben documentarse en el informe patológico. Si alguno no muestra calcificaciones, es posible que no se hayan tomado las muestras adecuadas. ¿El radiólogo o patólogo cuestionó la idoneidad? Los radiólogos y patólogos están altamente capacitados y serán los primeros en cuestionar si la biopsia es adecuada o si deben recomendar una repetición. ¿La patología concuerda con el nivel de preocupación de los estudios? Es decir, si tenemos una mamografía BI-RADS® 5 con calcificaciones lineales y ramificaciones, y un informe patológico benigno, no hay concordancia. Primero debemos controlar la idoneidad de las muestras. Sin embargo, en BI-RADS® 4 puede tratarse de enfermedad proliferativa benigna o malignidad. BI-RADS® 5 siempre tiene una patología de malignidad, y si no, es discordante.
14
So what do you do with discordant? You check with a multidisciplinary discussion or a second opinion. At the cancer institutes, we are very privileged to be able to take cases to a multidisciplinary conference. And here at MD --- The University of Texas MD Anderson Cancer Center, we have a set conference to discuss these cases every week. And in this discussion, we have multiple radiologists, multiple pathologists. The surgeon is present and the provider is also present. And we discuss the case clinically through imaging and then also through pathology. And we come up with a final recommendation. It could be it is benign. It could be it needs excision. Or it could be we need more tissue.
¿Qué hacemos con un resultado discordante? Debe programarse una discusión multidisciplinaria o buscar una segunda opinión. En los institutos del cáncer tenemos el privilegio de presentar casos ante una conferencia multidisciplinaria. En el Centro para el Cáncer MD Anderson la Universidad de Texas mantenemos una conferencia semanal en la que discutimos estos casos. Allí contamos con la presencia de varios radiólogos y patólogos, y también asisten el cirujano y el proveedor de atención médica. Discutimos el caso clínicamente a través de las imágenes y la patología, y preparamos una recomendación final. Podría ser benigno, requerir la extirpación o podría requerir más tejido.
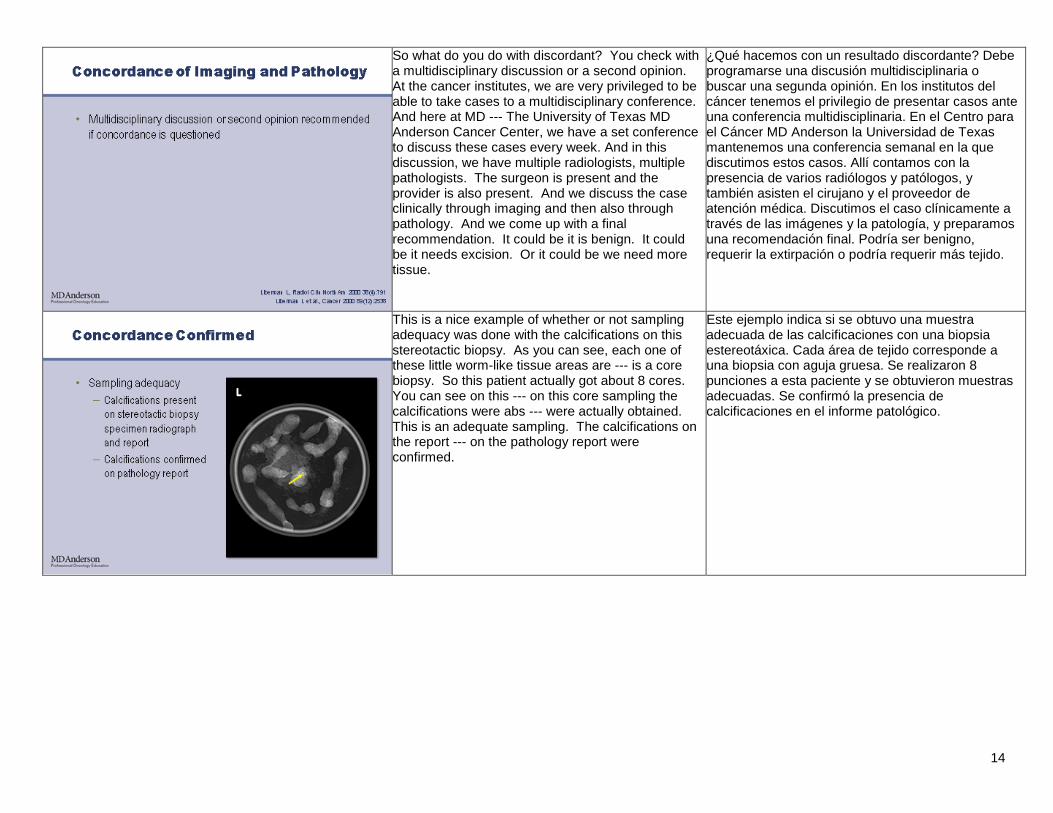
This is a nice example of whether or not sampling adequacy was done with the calcifications on this stereotactic biopsy. As you can see, each one of these little worm-like tissue areas are --- is a core biopsy. So this patient actually got about 8 cores. You can see on this --- on this core sampling the calcifications were abs --- were actually obtained. This is an adequate sampling. The calcifications on the report --- on the pathology report were confirmed.
Este ejemplo indica si se obtuvo una muestra adecuada de las calcificaciones con una biopsia estereotáxica. Cada área de tejido corresponde a una biopsia con aguja gruesa. Se realizaron 8 punciones a esta paciente y se obtuvieron muestras adecuadas. Se confirmó la presencia de calcificaciones en el informe patológico.
15
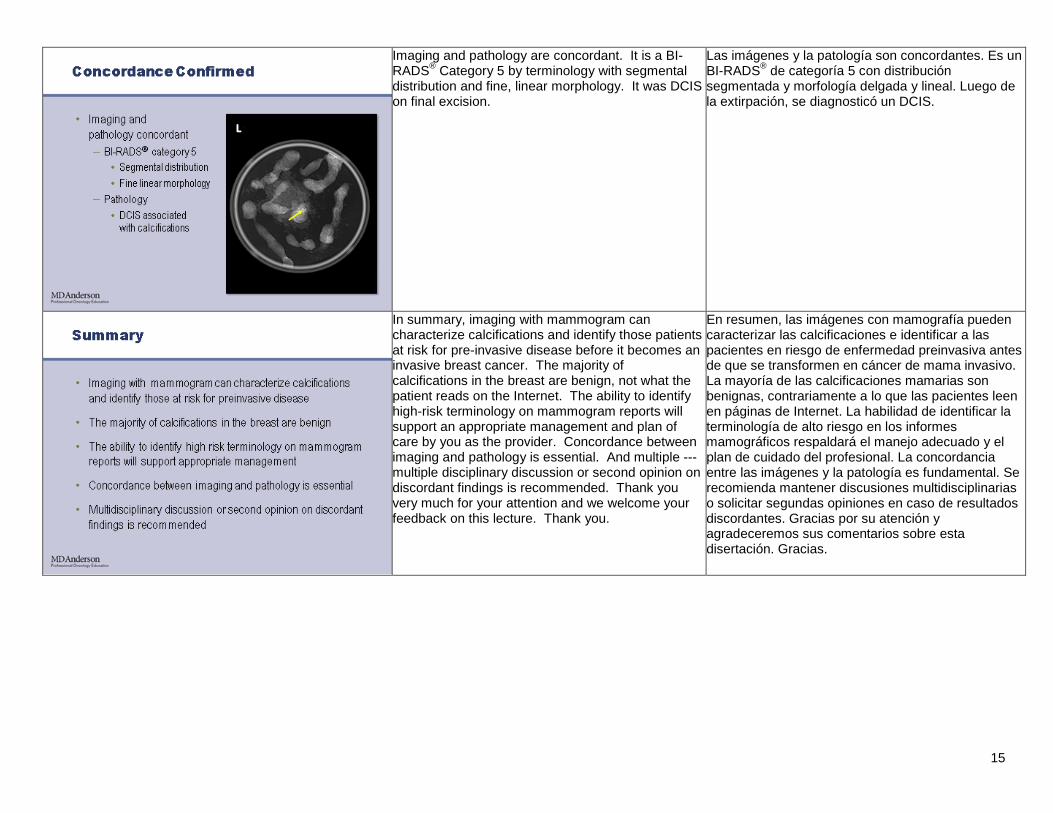
Imaging and pathology are concordant. It is a BI-RADS® Category 5 by terminology with segmental distribution and fine, linear morphology. It was DCIS on final excision.
Las imágenes y la patología son concordantes. Es un BI-RADS® de categoría 5 con distribución segmentada y morfología delgada y lineal. Luego de la extirpación, se diagnosticó un DCIS.
In summary, imaging with mammogram can characterize calcifications and identify those patients at risk for pre-invasive disease before it becomes an invasive breast cancer. The majority of calcifications in the breast are benign, not what the patient reads on the Internet. The ability to identify high-risk terminology on mammogram reports will support an appropriate management and plan of care by you as the provider. Concordance between imaging and pathology is essential. And multiple --- multiple disciplinary discussion or second opinion on discordant findings is recommended. Thank you very much for your attention and we welcome your feedback on this lecture. Thank you.
En resumen, las imágenes con mamografía pueden caracterizar las calcificaciones e identificar a las pacientes en riesgo de enfermedad preinvasiva antes de que se transformen en cáncer de mama invasivo. La mayoría de las calcificaciones mamarias son benignas, contrariamente a lo que las pacientes leen en páginas de Internet. La habilidad de identificar la terminología de alto riesgo en los informes mamográficos respaldará el manejo adecuado y el plan de cuidado del profesional. La concordancia entre las imágenes y la patología es fundamental. Se recomienda mantener discusiones multidisciplinarias o solicitar segundas opiniones en caso de resultados discordantes. Gracias por su atención y agradeceremos sus comentarios sobre esta disertación. Gracias.