Embed Size (px)
Citation preview

ENTERIC PARASITES AND ENTEROAGGREGATIVE ESCHERICHIA
COLI IN CHILDREN UNDER THE AGE OF FIVE, CAÑAZAS DISTRICT OF VERAGUAS
PROVINCE, 2010.
Vanessa Pineda S., Azael Saldaña Patiño, Richard L. Guerrant and Elena Jiménez Gutiérrez
Sección de Parasitología, Instituto Conmemorativo Gorgas de Estudios de la Salud;
Panama Initiative and Center for Global Health, University of Virginia

Although mortality from diarrhea around the globe has decreased significantly over the last four decades, the incidence of diarrhea and the morbidity rates of this disease, with the growing population of impoverished people, appear to have augmented over that same time period.1,2,3 Diarrhea still accounts for 1.6–2.5 million deaths annually worldwide, and each child in the developing world experiences an average of three episodes of diarrhea per year.¹ Persistently high rates of morbidity are of concern, because successive episodes of enteric infection and diarrhea in young children may have long-term effects on linear growth and cognitive development.1,2,3
Giardia lamblia and Ascaris lumbricoides (from left to right), two common gastrointestinal pathogens
BACKGROUND

Of particular interest to this study were enteroaggregative Escherichia coli (EAEC) strains, which are increasingly recognized as a cause of watery diarrhea, occasionally with blood and mucus, in children and adults worldwide.4,6 Several studies have suggested that persistent EAEC infection may produce an inflammatory enteritis in children that is associated with growth impairment and malnutrition.7,8 Although it is not specific for a particular pathogen, the detection of elevated concentrations of fecal lactoferrin, an iron-basedglycoprotein expressed by leukocytes, serves as a sensitive and specific diagnostic marker for the majority of inflammatory diarrheas.9,10,11 The current study therefore utilized fecal lactoferrin as an indicator for intestinal inflammation.
Escherichia coli

According to the Ministry of Health, 76,417 new cases of diarrheal illness occurred in children under the age of five in the Republic of Panama in 2007, and 76,032 new cases ensued in the same population of young children in 2008.12 The present investigation was undertaken to assess the prevalence of gastrointestinal infections with parasites and EAEC in children aged under five in certain impoverished rural communities within Cañazas District of Veraguas Province. In addition, this study aimed to determine whether the children living in these villages experienced growth shortfalls at a young age. Given that the incidence of poverty in Panama’s rural areas comprises approximately 50.7%, in contrast to 17.7% in urban areas, and Veraguas is one of the nation’s most impoverished provinces, with a poverty level of 52%, the study participants were among the poorest inhabitants of Panama.13 As a result of the lack of clean water supply and sanitation, these individuals were also deemed to be at a high risk of acquiring enteric infections.
Schoolchildren in Cañazas

I worked with and under the direct supervision of Vanessa Pineda and Dr. Azael Saldaña in the Department of Parasitology at the Gorgas Memorial Institute of Health Studies in Panama City. We studied young children from four rural communities, Alto y Bala, Calle Lourdes, Polo Sur and San José, within Cañazas District of Veraguas Province. The institute promised to provide diagnostic services for gastrointestinal infections to the children enrolled in the study. Thus, we delivered the written laboratory reports and the antiparasitic medications to the medical personnel of the region's main hospital, San Francisco Javier Hospital, who later proceeded to administer
these drugs to the appropriate children.
SETTING AND SERVICE

What is the prevalence of gastrointestinal infections with parasites and EAEC in children aged under five in four rural communities within Cañazas District of Veraguas Province?
Do these young children experience linear growth shortfalls that may be attributed to their enteric infections?
RESEARCH QUESTIONS

Study population. All eligible members of each dwelling were invited to participate in the study, given a plastic container to collect a stool sample and asked to deliver the stool specimen to the San Francisco Javier Hospital, the main hospital in Cañazas, by the next day. Information concerning age, sex, anthropometry, clinical symptoms, defecation habits, hygiene customs and dwelling characteristics were collected via a questionnaire . From the 174 children invited to join the study, 120 provided stool specimens. Out of these, 100 were less than 5 years of age and were selected to be the study population. Sample collection. At the time of collection, 87 fresh samples contained enough stool to divide each sample into two portions. The first portion was frozen at -20ºC without any additives in a small plastic container. The second portion was stored with a 5% formalin solution in preparation for the fecal parasite concentration processing. The remaining 13 samples were processed with a 5% formalin solution only. Immunochromatography. An immunochromatographic assay for the detection of Cryptosporidium parvum and Giardia lamblia was performed on all of the fresh samples using CERTEST CRYPTO-GIARDIA (Biotec S.L., Zaragoza, Spain), according to the manufacturer’s instructions.Fecal Parasite Concentration. Within a week of collection, the 100 fresh samples were processed by means of a formalin-ethyl acetate sedimentation concentration. Two drops of each specimen were examined under the light microscope, at each end of a slide. The entire smear was examined with the 10X low power objective lens in search of helminth eggs. If necessary, the identity of the eggs was confirmed with 40X magnification. At least a third of each smear was also viewed using the using the 40X high power objective lens to detect cysts of intestinal protozoans.Kinyoun stain. The dry slides were initially fixed with methanol for 10 minutes and rinsed with distilled water until the water flowed off clear. Next the slides were immersed in basic fuchsin solution for 5 minutes and washed with 50% ethanol. Each slide was later submerged in 1% sulfuric acid for 2 minutes and subsequently washed with abundant water. The slides were then stained with methylene blue (1 part volume of 1.4% methylene blue and 2 part volume of distilled water) for 5 minutes and washed with water. Finally, each slide was left to air dry completely at room temperature before being examined under the oil immersion objective lens at 100X magnification. The kinyoun procedure stained the Cryptosporidium spp. oocysts intensely pink over a blue background.DNA Extraction. The DNA was extracted with QIAmp DNA Stool Minikit (Qiagen Inc., Germantown, MD) from 200 mg of each previously frozen stool sample, according to the manufacturer’s instructions, with minor modifications as follows. First 650 µL of Buffer ASL were added to each sample, and the
METHODS

samples were vortexed until stools were homogenized. Then the samples were incubated at 82.5 oC for 5 minutes. Later on, after inhibitors had adsorbed to the matrix of the InhibitEX Tablet, 200 µL of nuclease-free water were added to each sample and the samples were centrifuged at full speed for 2 minutes. The supernatant was pipetted into a new tube with 30 µL of proteinase K, to which 400 µL of Buffer AL were added, vortexed for 15 seconds, and incubated at 70oC for 10 minutes. Then 400 µL of ethanol (100%) were added, and mixed by vortexing. Qiagen’s “Protocol: Isolation of DNA from Stool for Pathogen Detection” was then followed to completion. PCR amplification and sequencing. One of the PCR methods used for sample analysis aimed to amplify aggR, a 308 bp fragment encoding a transcriptional activator of several EAEC virulence genes, using the appropriate forward (5′-CTAATTGTACAATCGATGTA-3′) and reverse (5′-ATGAAGTAATTCTTGAAT-3′) primers.14 The other PCR assay was intended to detect aatA, a 630 bp fragment encoding an outer membrane protein that is part of a protein ABC transporter system, using the corresponding forward (5′-CTGGCGAAAGACTGTATCAT-3′) and reverse (5′-CAATGTATAGAAATCCGCTGTT-3′) primers.14 According to prior studies, these 2 EAEC plasmid borne loci, aggR and aatA are highly specific for this strain of Escherichia coli.14 Both PCR tests were performed in a final reaction volume of 25 µL. Each reaction tube was prepared by adding 4.3 µL of nuclease-free water, 1.6 µL of the forward primer, 1.6 µL of the reverse primer, 12.5 µL of Master Mix and 5 µL of DNA template. For aggR, the amplification was performed with an initial denaturation at 95ºC for 5 minutes followed by 30 cycles of 95ºC for 30 seconds, 43.6ºC for 30 seconds, 72ºC for 30 seconds, and a final extension at 72 ºC for 5 minutes. The cycling conditions were the same for aatA, except the annealing temperature was 53ºC. Negative controls comprised the PCR mixture without the DNA template. An EAEC prototype strain 042 kindly provided by the University of Virginia was included in each test as a positive control. Electrophoresis on 1.5% agarose gels and staining with 5 µL of ethidium bromide in 100 mL was used for visualization of amplified targets.Fecal lactoferrin testing. An ELISA test for the qualitative detection of lactoferrin, a marker of fecal neutrophils and an indicator of intestinal inflammation, was performed on the previously frozen stool samples using IBD-CHECK (Techlab, Blacksburg, VA), according to the manufacturer’s instructions. The samples with positive results for the original ELISA were then assayed using IBD-SCAN (Techlab, Blacksburg, VA), a quantitative ELISA for measuring concentrations of fecal lactoferrin, according to the manufacturer’s instructions. Height-for-age, weight-for-age and weight-for-height z-scores. Algorithms provided by the World Health Organization via an SPSS version were used to calculate the corresponding indicators of attained growth standards. These algorithms were based on the 2006 World Health Organization (WHO) international growth reference.

The study population included 52 female and 48 male children ranging from 4.4 to 59.4 months of age with a median age of 35.1 months. On questioning, 47% of the participants’ parents reported living in a house with an earth floor and 52% indicated that they had no electricity in their homes. The survey revealed that 93% of the participants had access to a latrine and only 10% had a private toilet. The region’s aqueduct with unchlorinated water served as the sole water source for 86% of the participants. There was an average of 6 people per household.
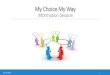
On further questioning, 37% of the parents reported having been aware of prior intestinal helminthic infections in their children. Out of these 37 children, only 24 (65%) had received medical treatment for their illness at the time. A health care provider, in the form of a nurse, a nutritionist or a physician, had informed the parents of 42% of the participants that these children were underweight. The results of the stool tests are shown in Figure 1. Intestinal pathogens were detected in 61% of the participating children, Giardia lamblia in 32%, Ascaris lumbricoides in 14%, Enteroaggregative Escherichia coli in 13%, Entamoeba coli in 12%, Iodamoeba büstchlii in 8%, Entamoeba histolytica/Entamoeba dispar complex in 4%, and Uncinaria, Hymenolepis nana, Cryptosporidium parvum, Cyclospora cayetanensis and Endolimax nana in 1% each. Since only 87 stool samples were frozen, genetic targets for EAEC were amplified for only these specimens and thus percentage of infections, exactly 12.6%, represented 11 positive results out of a total of 87 tests. The rest of the percentages were determined out of a total of a 100.
RESULTS AND DISCUSSION

Giard
ia la
mbl
ia
Ascar
is lu
mbr
icoi
des
Enter
oagg
rega
tive
Esche
richi
a co
li*
Entam
oeba
Col
i
Ioda
moe
ba b
ütsc
hlii
Entam
oeba
histo
lytic
a/Ent
amoe
ba d
ispa
r com
plex
Unc
inar
ia
Hym
enol
epis n
ana
Cryst
ospo
ridiu
m p
arvu
m
Cyclo
spor
a ca
yeta
nens
is
Endol
imax
nan
aAny
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
32
14 11 128
4 1 1 1 1 1
61
Intestinal infections in study participants
Figure 1. Intestinal infections in study participants from Cañazas, Veraguas, on June 31, 2010. * The percentage of EAEC infections, exactly 12.6%, represented 11 positive specimens for the corresponding EAEC genetic markers out of a total of 87 frozen samples. The rest of the percentages were calculated out of a total of a 100, which comprised the number of fresh stool specimens examined. Therefore, these last percentages are identical to the numbers displayed within each bar in the figure.

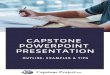
As shown in Figure 2, the height-for-age z-scores of the study participants younger than 18 months of age experienced a significant decline with a slope of -0.2407 (95% CI = -0.3653 to -0.1161; P = 0.0016) from a relatively normal number at approximately 4 months of age (4.37 months of age with a height-for-age z-score of 0.16) to a z-value more than 3 standard deviations below the mean of the reference population at roughly over 16 months of age (16.39 months with a height-for-age z-score of -3.56). The reasons for this sharp decline may be due to a combination of factors, including an insufficient diet and a high burden of enteric infections as a result of the weaning process and exposure to contaminated water. Given the high rate of gastrointestinal infections in the study population, it is highly probable that many of the participants, regardless of whether or not they presented with enteric pathogens on this occasion, were infected in the past. These infections may have contributed to their current linear growth deficits. As a group, the children in the study who were older than 18 months did not seem to recover from the aforementioned sharp decline in their height-for-age z-scores during earlier months. Although Figure 2 does not depict a statistically significant level of decline in these values for the children whose ages span from over 18 months to nearly 5 years (exactly from age 18.79 to 59.40 months), with a slope of -0.006549 (95% CI = -0.02991 to 0.01681; P = 0.5780), the data does demonstrate a height-for-age z-score mean of -1.449 (95% CI = -1.729 to -1.169; P < 0.0001), which is more than 1 standard deviation below the international reference mean value.

Figure 5. Height-for-age z-scores of all study participants according to age in months. Out of a 100 subjects, two were excluded from this analysis, for anthropometric data was not collected from them.
HAZ-scores for children < 5 years old
10 20 30 40 50 60
-6
-5
-4
-3
-2
-1
0
1
2
3
4
5
6
Age in months
He
igh
t-fo
r-a
ge
z-s
co
res

Further longitudinal research could track the children’s growth, capture seasonal variations, and detect a wider spectrum of enteric bacteria and parasites. Another future study could evaluate anthropometric measurements of adults living in the aforementioned communities to derive correlations between stunting early in childhood and obesity later on in life. In collaboration with the San Francisco Javier Hospital and perhaps other clinics and/or hospitals in the area, another research project could entail reviewing medical records to calculate the incidence, morbidity and mortality rates of distinct enteric infections as well as the healthcare costs associated with these diarrheal illnesses. A future health-related environmental investigation could entail testing the water from its source and at different points along the aqueduct system in Cañazas for common enteric pathogens to determine whether or not this water is a source of intestinal infection in the children. With current living conditions, eradication of the enteric infections and the growth shortfalls in these children seems very challenging. In order to prevent childhood stunting, most interventions should target children under 18 months of age because this early period seems to be a crucial stage for linear growth. These strategies could include improvements in water quality and sanitation, increased breastfeeding, better weaning practices, and better health care access.
Acknowledgments: I extend my gratitude to Vanessa Pineda, Dr. Azael Saldaña, Dr. Richard Guerrant, Jones Barbosa Lima Neto and April Ballard for their invaluable support and guidance throughout this research process. I thank Dr. Brad Brown and Dr. Jeanita W. Richardson for their very helpful advice. I am also grateful to Relana Pinkerton for her help in the statistical analysis and to Dr. Vivian E. Thomson for her logistical assistance.
Financial support: This work received financial support from the University of Virginia’s Panama Initiative Student Scholar Program and the Center for Global Health-University Scholar Award Program.
RECOMMENDATIONS

CONTACT INFORMATION
UVa mentors: Dr. Richard L. Guerrant, M.D. Thomas H. Hunter Professor of International Medicine Infectious Diseases and International Health Director, Center for Global Health [email protected] Brad Brown, Ph.D. Associate Professor of Commerce Director of International Affairs [email protected] Jeanita W. Richardson, Ph.D.
Associate ProfessorMedical Education and Public Health Sciences
Division of Public Health Policy and Practice Department of Public Health Sciences [email protected]
Host mentor:• Dr. Azael Saldaña Patiño Director, Section of Parasitology Gorgas Memorial Institute of Health Studies [email protected]
My contact information:[email protected]
Personal Background: I was born and raised in San José, Costa Rica. Prior to attending college in the United States, I studied for a year and a half at the University of Costa Rica and worked as a laboratory intern at this university’s Cellular and Molecular Biology Research Center. Subsequently, I obtained a Bachelor of Science degree in clinical laboratory science from the University of North Carolina at Chapel Hill. Throughout my college years, I took part in various service and advocacy non-profit organizations. After graduation, I worked as a medical technologist at the University of North Carolina Hospitals’ Transfusion Medicine Service Laboratory for a year. I then shadowed physicians full-time through the internal medicine, pediatrics, and gynecology services at the Mexico Hospital in Costa Rica for six months. Overall, my research experiences and clinical laboratory science courses stimulated my interest in medical investigation as a way to serve others. My undergraduate volunteer activities and later clinical exposure also increased my awareness of health inequalities and strengthened my resolve to work with underserved populations around the world.

1. Kosek M, Bern C, Guerrant RL. The global burden of diarrhoeal disease, as estimated from studies published between 1992 and 2000. Bull WHO. 2003; 81(3):197–204.
2. Guerrant RL, Oria R, Bushen OY, et al. Global impact of diarrheal diseases that are sampled by travelers: the rest of the hippopotamus. Clin Infect Dis. 2005; 41(Suppl 8):S524–30.
3. Guerrant RL, Kosek M, Moore S, et al. Magnitude and impact of diarrheal diseases. Arch Med Res. 2002; 33(4):351–5.
4. Kaper JB, Nataro JP, Mobley HL. Pathogenic Escherichia coli. Nat Rev Microbiol. 2004; 2(2):123-40.5. Nataro JP, Steiner T, Guerrant RL. Enteroaggregative Escherichia coli. Emerg Infect Dis. 1998;
4(2):251-61.6. Harrington SM, Dudley EG, Nataro JP. Pathogenesis of enteroaggregative Escherichia coli infection.
FEMS Microbiol Lett. 2006; 254(1):12-8.7. Roche JK, Cabel A, Sevilleja J, et al. Enteroaggregative Escherichia coli (EAEC) Impairs Growth while
Malnutrition Worsens EAEC Infection: A Novel Murine Model of the Infection Malnutrition Cycle. J Infect Dis. 2010; 202(4):506-14.
8. Steiner TS, Lima AAM, Nataro JP, et al. Enteroaggregative Escherichia coli produce intestinal inflammation and growth impairment and cause interleukin-8 release from intestinal epithelial cells. J Infect Dis. 1998; 177: 88-96.
9. Gadewar S, Fasano A. Current concepts in the evaluation, diagnosis and management of acute infectious diarrhea. Current Opinion in Pharmacology. 2005; 5(6):559-65.
10. Kane SV, Sandborn WJ, Rufo PA, et al. Fecal Lactoferrin is a sensitive and specific marker in identifying intestinal inflammation. American J Gastroenterology. 2003; 98(6):1309-14.
11. Huicho L, Campos M, Rivera J, et al. Fecal screening tests in the approach to acute infectious diarrhea: a scientific overview. Pediatr Infect Dis J. 1996; 15(6):486-94.
12. Benítez L, Tejada I, Ruiloba AM. Boletín Estadístico de Salud 2008. Ministerio de Salud, República de Panamá. 2009; 58.
13. Encuesta de Niveles de Vida 2008. Contraloría General de la República, Instituto Nacional de Estadística y Censo, República de Panamá. 2008; 2.
14. Monteiro BT, Campos LC, Sircili MP, et al. The dispersin-encoding gene (aap) is not restricted to enteroaggregative Escherichia coli. Diagnost Micro Infect Dis. 2009; 65:81–84.
15. Venkataraman S, Ramakrishna BS, Kang G, et al. Faecal lactoferrin as a predictor of positive faecal culture in south Indian children with acute diarrhoea. Annals Trop Paediatr. 2003; 23(1):9-13.
16. Huicho L, Garaycochea V, Uchima N, et al. Fecal lactoferrin, fecal leukocytes and occult blood in the diagnostic approach to child hood invasive diarrhea. Pediatr Infect Dis J. 1997; 16:644–7.
REFERENCES