Embed Size (px)
Citation preview

9/19/2017
1
Palliative Radiotherapy We Can Actually
Afford: A New Program Designed to Help
Patients and Caregivers Save Resources
1
Christopher Abraham, MD
Assistant Professor
Department of Radiation Oncology
Washington University School of Medicine
Patrick White, MD, HMDC, FACP, FAAHPM
Chief Medical Officer, BJC Home Care
Assistant Professor of Medicine
Washington University School of Medicine
Disclosure: There are no relevant financial
relationships to disclose regarding
this presentation
2
Patrick White, MD
Chris Abraham, MD
1) Describe 3 potential benefits of palliative radiation
2) Identify 3 obstacles to the use of palliative radiation in
the hospice setting
3) Describe how a new program can make palliative
radiation available to all hospice patients
Objectives
3

9/19/2017
2
My Background
• Internal Medicine-
Washington
University/BJH
• PhD Program, Clinical and
Translational Science,
University of Pittsburgh
• Co-Chief Medical Officer,
University of Pittsburgh’s
Hospice Program
• Chief Medical Officer, BJC
Home Care
My Background
5
• MD, Saint Louis
University
• Radiation Oncology
Residency, Barnes-
Jewish Hospital
• Assistant Professor,
Department of
Radiation Oncology
Washington University
in St. Louis
States Worse Than Death Among Hospitalized
Patients With Serious Illnesses
6
Rubin EB, Buehler AE, Halpern SD. States Worse Than Death Among Hospitalized Patients With Serious Illnesses. JAMA Intern Med. 2016 PMID 24479808

9/19/2017
3
Radiotherapy Basics
• Radiotherapy utilizes high energy radiation to damage DNA
– X-rays, gamma rays, charged particles
– DNA damage is not specific to cancer cells alone
• Radiotherapy may be delivered locally or systemically
• Local radiotherapy may be delivered externally or internally
• Radiation dose is prescribed in Gray and fractions
• Fractionation is utilized to:
– Minimize normal tissue toxicity
– Increase the likelihood DNA damage
Radiotherapy Basics
• Radiotherapy may be given with definitive OR palliative
intent
• Nearly 50% of all radiotherapy is given with palliative
intent
• Radiotherapy prescription dichotomy:
– Local control IS impacted by dose
• Locally advanced lung cancer: 60Gy/30 fractions
– Palliative effect IS NOT impacted by dose
• Bone metastasis: 8Gy/1 fraction
Historical Perspective
• “When the initial objective of
radiation therapy is palliation,
new ground rules must be
applied. Possible serious
complications or even slowly
self-limiting side effects of
treatment are no longer
acceptable. Overall treatment
time must be short. Cost must
be minimized. Convenience of
treatment must be
considered.” - JAMA, 1964

9/19/2017
4
Palliative Radiotherapy
• Palliative radiotherapy:
– Effective at improving symptoms
• Pain
• Dysphagia / odynophagia
• Bleeding
• Obstruction
– Improves quality of life
– Safe with limited side effects
– Time-efficient
– Cost-effective
– Convenient
Palliative Radiotherapy Indications
• Primary Sites of Disease
– Brain – headaches, neurologic dysfunction
– Head and neck – pain, bleeding, dysphagia, SOB
– Lung – pain, hemoptysis, SVC, post-obstructive PNA
– GU – pain, hematuria, obstruction
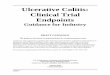
– GI – pain, bleeding, tenesmus, obstruction
• Secondary Sites of Disease
– Bone – pain, cord compression
– Skin, subcutaneous tissues
– Spleen – pain, early satiety
– Overlap with primary sites of disease
Palliative Radiotherapy Exclusions
• Patient
– Imminent death
– Inability to provide consent
– Multiple progressive systems
• Treatment
– Side effects > risks
– Unsafe
• Health Care System
– Cost
– Transportation

9/19/2017
5
Site Specific Treatment
14
Bone Metastases
Bone Metastasis
Palliative Radiotherapy Trials for Bone Metastasis: A Systematic Review
Chow, JCO 2007
• Meta-analysis including 16 randomized trials
• >5000 patients in total
• Randomized between single fraction vs. multiple fractions– 8Gy / 1 fraction vs 20Gy/5, 30Gy/10, etc
• Multiple pathologic types included
• Multiple outcomes assessed:– Overall response
– Complete response
– Re-treatment

9/19/2017
6
Bone Metastasis
• Overall response
– Single fraction: 58%, Multi fraction: 59%
Bone Metastasis
• Complete response
– Single fraction: 23%, Multi fraction: 24%
Bone Metastasis
• Re-treatment
– Single fraction: 20%, Multi fraction: 8%

9/19/2017
7
Bone Metastasis: Re-treatment
Single versus multiple fractions of repeat radiation for
painful bone metastasis: a randomized controlled, non-
inferiority trial
Chow, Lancet Onc 2014
• RCT of 8Gy / 1fx vs. 20Gy / 5 fx RT for re-treatment
• No difference in overall pain response
• Acute radiation related toxicities higher in multi-fraction
• No difference in cord compression or pathologic fracture
Bone Metastasis: End of Life
Efficacy of radiotherapy for painful bone metastases
during the last 12 weeks of life: results from Dutch
Bone Metastasis Study
Meeuse, CA 2010
• RTC of single vs multi fraction radiotherapy
• Cohort of patients who died within 12 weeks after
randomization
• Results
– Pain response 45% overall
– Median time to relief 2 weeks

9/19/2017
8
Bone Metastasis Conclusions
• For bone metastasis:
– Radiotherapy is effective at improving pain
– Single fraction is equivalent to multi fraction:
• Overall response
• Complete response
– Re-treatment rates are 2.5 times with single fraction
radiotherapy
• When re-treatment:
– Re-treatment is effective at improving pain
– Single fraction is equivalent to multi fraction
• Palliative radiotherapy is effective at the end of life
Spinal Cord Compression
Spinal Cord Compression
8Gy single dose radiotherapy is effective in metastatic
spinal cord compression: Results of a phase III
randomized multicenter Italian trial
Maranzano, Rad Onc 2009
• RCT of 8Gy / 1 fraction vs 8Gy / 2 fractions for MSCC
• Patients with short life expectancy
• No difference in response
– Pain
– Motor and sphincter function
• No difference in duration of response

9/19/2017
9
Other sites
Thoracic
Palliative Thoracic Radiotherapy for Lung Cancer: A
Systematic Review
Fairchild, JCO 2007
• Meta-analysis including 13 randomized trials
• >3000 patients
• Randomized patients to short or long course
• Multiple outcomes assessed
– Symptom palliation
– Survival
– Toxicity
– Re-irradiation rate
Thoracic (Hemoptysis)

9/19/2017
10
Thoracic (Cough)
Thoracic (Chest Pain)
Esophageal Stricture
Single-dose brachytherapy verus metal stent
placement for palliation of dysphagia from
oesophageal cancer: multicenter randomized trial
Homs, Lancet 2004
• Prospective randomized trial
• Randomized between stent and brachytherapy
• >200 patients
• Results:
– Stent more rapid relief
– Brachy more long relief, improved QOL
– Brachy fewer complications

9/19/2017
11
Large Pelvic Masses
Phase II study of multiple daily fractionations in palliation of advanced pelvic malignancies: preliminary report of RTOG 8502
Spanos, IJROBP 1989
• 152 pts with advanced pelvic malignancies– Gyn, colorectal, GU, misc
• 3.7Gy BID x 2 days, 3-6 weeks off, repeat x2
• Total of 44.4Gy
• After completion of 3 courses:– CR – 15%
– PR – 32%
– Stable - 35%
Conclusions
• Palliative radiotherapy is:
– Effective
– Safe
– Time efficient
• Radiotherapy is useful for:
– Primary and secondary disease
– Multiple anatomic sites
• Single fraction radiation is often reasonable and
appropriate means for palliation
• Perception
– Hospice Provider’s Perception
– Radiation Oncologists Perception
• Barriers
– Educational Barriers
– Economic Barriers
– Research Barriers
• Outcome
– Less than 3% of hospice patients receive radiation therapy
Barriers to Radiation Therapy in Hospice Care
33
Lutz ST, Jones J. Chow E. Role of radiation therapy in palliative care of the patient with
cancer. J Clin Onc. 2014; 32(26):2913-9.

9/19/2017
12
Question % Yes
1) Is radiation therapy (RT) important in palliative care? 87%
2) Do you feel sufficiently trained for when to use RT? 52%
3) Is RT available to your patients? 74%
4) Do you have access to a radiation oncologist to discuss your patients?
75%
5) Would you be willing to attend palliative RT lectures? 94%
Barriers to Radiation Therapy in Hospice Care:
Survey of Hospice Providers (Easy Questions)
34
Lutz S, Spence C, Chowe E, Janjan N, Connor S. Survey on use of palliative radiotherapy in
hospice care. J Clin Oncol. 2004; 22(17):3581-3586.
Question % Yes
1) Do you feel radiation oncologists are sufficiently trained in palliative care to render opinions regarding treatment of hospice cancer patients?
56%
2) Are radiation oncologists resistant to prescribing single-fraction treatments?
76%
3) Would you be willing to recruit hospice patients into trials measuring the worth of palliative radiotherapy in certain circumstances?
59%
Barriers to Radiation Therapy in Hospice Care:
Survey of Hospice Providers (Hard Questions)
35
• Lack of formal palliative care training for radiation
oncology residents
• Lack of radiotherapy training for palliative care
professionals
• Minimal protected time at national meetings for palliative
oncology topics
• Lack of training for hospice clinicians in identifying
situations where radiation therapy may improve QOL
Educational Barriers
36
Lutz ST, Jones J. Chow E. Role of radiation therapy in palliative care of
the patient with cancer. J Clin Onc. 2014; 32(26):2913-9.

9/19/2017
13
• Economic incentives to prescribe protracted courses of
radiation therapy
• Radiotherapy costs several times the average hospice
per diem
• Transportation costs are often borne by hospice
organizations and may even be more expensive than the
radiotherapy itself
• Caregivers may not be able to take the time off work to
complete protracted course of radiation therapy
Economic Barriers
37
Lutz ST, Jones J. Chow E. Role of radiation therapy in palliative care of the
patient with cancer. J Clin Onc. 2014; 32(26):2913-9.
Economic Impact of Single-fraction Versus
Multi-fraction Radiotherapy
38
International Variation in Practice Patterns Comparing
Single-Fraction to Multi-fraction Radiotherapy
39

9/19/2017
14
• Paucity of experienced research teams in hospice and
palliative care programs
• Missing data points because of declining health or death
of accrued patients
• Lack of federal funds dedicated to end-of-life studies
• Paucity of clinical trials comparing different radiation
regimens for many conditions (outside of painful bone
metastases)
Research Barriers
40
Lutz ST, Jones J. Chow E. Role of radiation therapy in palliative
care of the patient with cancer. J Clin Onc. 2014; 32(26):2913-9.
• More focused collaborations between radiation
oncologists and hospice/palliative care physicians
• Emphasis on hypofractionated courses for patients with
poor prognoses
• Formalized training for both radiation oncology residents
and palliative care fellows on the nuances of palliative
radiotherapy
• Formation of more radiotherapy overuse guidelines and
quality measures and increased accountability
Improving Access to Radiotherapy
41
Hospice / Palliative Logistics
for New Palliative
Radiotherapy Clinic at CHNE

9/19/2017
15
Who- Any hospice patient with painful bone metastases or
spinal cord compression regardless of hospice provider
What-Palliative radiation clinic specializing in single fraction
radiotherapy
Where-Christian Hospital Northeast in Saint Louis
When-Now!
Why-Need for inexpensive, single fraction radiation therapy
to help improve quality of life while reducing the burdens on
patients and caregivers
New Palliative Radiation Oncology Clinic
43
• Reduced Professional Fee-Washington University
Radiation Oncology has agreed to bill only a 99203
($290.52) which is a level 3 visit with low complexity
• Christian Hospital will allow a single fraction without a CT
simulation or additional imaging to keep costs ($328.13)
minimal.
• Total costs for the technical fee and professional fee and
imaging will be $618.65 (adjusted for Medicare Fee
Schedule) and the entire process will typically be
conducted in one visit!
• This could result in reduced ambulance costs, lower
caregiver burden, decreased transportation discomfort,
longer hospice LOS, etc.
What Makes This Radiotherapy Practical
44
• Is the patient able to lie flat?
– (okay if not but need to know)
• Is the patient able to follow instructions, can the safely
be placed on a treatment table?
• Is the patient decisional to sign consent for treatment?
– if not POA must be present for consult and treatment to give
consent.
Information Needed From the Referring Hospice
45

9/19/2017
16
Logistics
Hospice determines radiotherapy need
Case discussed with Radiation Oncology
Formal referral rendered
Continued assessment of need
Radiation Oncology assessment
Simulation
Quality Assurance
Delivery of single fraction radiotherapy
Transportation
Pre-medication
• Conway JL, Yurkowski E, Glazier J, et al. Comparison of Patient-reported Outcomes with a Single
Versus Multiple Fraction Palliative Radiotherapy for Bone Metastasis in a Population-based Cohort. Radiother Oncol. 2016; 119(2):202-207.
• Chow E, van der Linden YM, Roos D, et al. Lancet Oncol. Single Versus Multiple Fractions of Repeat Radiation for Painful Bone Metastases: a Randomized, Controlled, Non-inferiority Trial.
2014 Feb;15(2):164-71.
• Collinson L, Kvizhinadze G, Nair N, McLeod M, Blakely T. Economic Evaluation of Single-fraction
Versus Multiple-fraction Palliative Radiotherapy for Painful Bone Metastases in Breast, Lung and
Prostate Cancer. J Med Imaging Radiat Oncol. 2016; 60(5):650-660.
• Chow E, Hahn CA, Lutz ST, Global Reluctance to Practice Evidence-based Medicine Continues in
the Treatment of Uncomplicated Painful Bone Metastases Despite Level 1 Evidence and Practice Guidelines. Int J Radiat Oncol Bio Phys. 2012;83(1):e117-120.
• Saito T, Toya R, Semba A, et al. Influence of the Treatment Schedule on the Physicians' Decisions
to Refer Bone Metastases Patients for Palliative Radiotherapy: a Questionnaire Survey of
Physicians in Various Specialties. Nagoya J Med Sci. 2016; 78(3):275-84.
• Fairchild A, Barnes E, Ghosh S, et al. International Patterns of Practice in Palliative Radiotherapy
for Painful Bone Metastases: Evidence-based Practices? Int. J. Radiation Oncology Biol. Phys.
2009;75(5):1501-1510.
• Thavarajah N, Zhang L, Wong K, Bedard G. Patterns of Practice in the Prescription of Palliative
Radiotherapy for the Treatment of Bone Metastases at the Rapid Response Radiotherapy Program Between 2005 and 2012. Curr Oncol. 2013 Oct;20(5):e396-405.
References
47
• McDonald R, Ding K, Brundage M, et al. Effect of Radiotherapy on Painful Bone Metastases: A
Secondary Analysis of the NCIC Clinical Trials Group Symptom Control Trial SC.23. JAMA Oncol. 2017. Epub ahead of print.
• Howell DD, James JL, Hartsell WF, Suntharalingam M. Single-fraction Radiotherapy Versus Multi-fraction Radiotherapy for Palliation of Painful Vertebral Bone Metastases-equivalent Efficacy, Less
Toxicity, More Convenient: a Subset Analysis of Radiation Therapy Oncology Group trial 97-14.
Cancer. 2013; 119(4):888-96.
• Moghanaki D, Cheuk AV, Fosmire H, Anscher MS. Availability of Single-fraction Palliative
Radiotherapy for Cancer Patients Receiving End-of-life Care Within the Veterans Healthcare Administration. J Palliat Med. 2014;17(11):1221-5.
• Lutz ST, Jones J, Chow E. Role of Radiation Therapy in Palliative Care of the Patient with Cancer. J Clin Oncol. 2014; 32(26):2913
• Lutz S, Spence C, Chow E, Janjan N, Connor S. Survey on Use of Palliative Radiotherapy in
Hospice Care. J Clin Oncol. 2004; 22(17):3581-6.
• McCloskey SA, Tao ML, Rose CM, Fink A, Amadeo AM. National Survey of Perspectives of
Palliative Radiation Therapy: Role, Barriers, and Needs. Cancer J. 2007; 13(2):130-7.
References (continued)
48