Embed Size (px)
Citation preview

1/20/2015
1
Best Practices for
Optimal Dementia Care
Terry R. Barclay, PhD Director, HealthPartners Neuropsychology
Objectives
• Review Minnesota’s ACT on Alzheimer’s
• Discuss rationale for timely detection
• Recognize key management priorities throughout the dementia continuum
– Accompanying evidence-based tools
• Learn how to help patients and family access services to improve function and promote wellness
2
Introduction to
ACT on Alzheimer’s

1/20/2015
2
ACT on Alzheimer’s
statewide
collaborative
volunteer
driven
60+ O R G A N I Z A T I O N S
300+ I N D I V I D U A L S
I M P A C T S O F A L Z H E I M E R ’ S
BUDGETARY SOCIAL PERSONAL
4
sustain
caregivers
raise
awareness
& reduce
stigma
Goals of ACT
identify &
invest in
promising
approaches
increase
detection &
improve care
equip communities
ACT Tool Kit
• Consensus-based, best practice standards for Alzheimer’s care
• Tools and resources for:
– Primary care providers
– Care coordinators
– Community agencies
– Patients and families
6

1/20/2015
4
Cognitive Screening
10
Base Rates
• 1 in 9 people 65+ (11%)
• 1 in 3 people 85+ (32%)
11
Age Range Percent with Alzheimer’s
< 65 4%
65 -74 13%
75 -84 44%
85 + 38%
Is Screening Good Medicine?
2014 US Preventative Services Task Force (USPSTF)
• Purpose: Systematically review the diagnostic accuracy of brief cognitive screening instruments and the benefits/harms of medication and non-medication interventions for early cognitive impairment.
• Limitation: Limited studies in persons with dementia other than AD and sparse reporting of important health outcomes.
• Conclusion: Brief instruments to screen for cognitive impairment can adequately detect dementia, but there is no empirical evidence that screening improves decision making.
12
1/20/2015
5
Provider Perspective
“Avoiding detection of a serious and life changing medical condition just because there is no cure or ‘ideal’ medication therapy seems, at worst, incredibly unethical, and, at best, just bad medicine.”
George Schoephoerster, MD Family Practice Physician
13
If we don’t diagnose, does it still exist?
“Beyond mountains, there are mountains.”
Haitian Proverb
Diagnostic Challenges

1/20/2015
6
Clinical Provider Practice Tool
• Easy button workflow for:
1. Screening
2. Dementia work-up
3. Treatment / care www.actonalz.org/provider-practice-tools
16
Cognitive Screening
• Initial considerations
– Timing
• Routine, annual check-ups or only when patients become obviously symptomatic?
– Best practice recommendation: Annual screening at 65+
– Screening meant to uncover insidious disease
– Doesn’t add much if you can already detect impairment in basic conversation
– Research
• Which tools are best?
• Balance b/w time and sensitivity/specificity
Cognitive Screening
– Clinic flow
• Who will administer screen? – Rooming nurses, social workers, allied health professionals,
MDs
• What happens when patients fail?
18

1/20/2015
7
Screening Measures
• Wide range of options
– Mini-Cog (MC)
– Mini-Mental State Exam (MMSE)
– St. Louis University Mental Status Exam (SLUMS)
– Montreal Cognitive Assessment (MoCA)
• All but MMSE free, in public domain, and online
Screening Administration
• Try not to: – Use the word “test”
• Instead: “We’re going to do something next that requires some concentration”
– Allow patient to give up prematurely or skip questions
– Deviate from standardized instructions
– Offer multiple choice answers
– Be soft on scoring – Score ranges already padded for normal errors
– Deduct points where necessary – be strict
Mini-Cog
Contents • Verbal Recall (3 points)
• Clock Draw (2 points)
Advantages • Quick (2-3 min)
• Easy
• High yield (executive fx, memory, visuospatial)
Subject asked to recall 3 words Leader, Season, Table
Subject asked to draw clock, set hands to 10 past 11
+3
+2

1/20/2015
8
22
DATE_________ ID_________________________AGE____GENDER M F LOCATION ______________________TESTED BY________
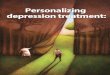
MINI-COG ™
1) GET THE PATIENT’S ATTENTION, THEN SAY: “I am going to say three words that I want you to remember now and later. The words are
Banana Sunrise Chair. Please say them for me now.” (Give the patient 3 tries to repeat the words. If unable after 3 tries, go to next item.)
(Fold this page back at the TWO dotted lines BELOW to make a blank space and cover the memory words. Hand the patient a pencil/pen).
2) SAY ALL THE FOLLOWING PHRASES IN THE ORDER INDICATED: “Please draw a clock in the space below. Start by drawing a large
circle.” (When this is done, say) “Put all the numbers in the circle.” (When done, say) “Now set the hands to show 11:10 (10 past 11).” If
subject has not finished clock drawing in 3 minutes, discontinue and ask for recall items.
-------------------------------- -------------------------------- -------------------------------- -------------------------------- -------------------------------- -------------------------------- --------------
-------------------------------- -------------------------------- -------------------------------- -------------------------------- -------------------------------- -------------------------------- -------------
3) SAY: “What were the three words I asked you to remember?”
_ (Score 1 point for each) 3-Item Recall Score
Score the clock (see other side for instructions): Normal clock 2 points Clock Score
Abnormal clock 0 points
Total Score = 3-item recall plus clock score 0, 1, 2, or 3 = clinically important cognitive impairment likely;
4 or 5 = clinically important cognitive impairment unlikely
23
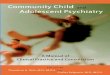
CLOCK SCORING
NORMAL CLOCK
A NORMAL CLOCK HAS ALL OF THE FOLLOWING ELEMENTS: All numbers 1-12, each only once, are present in the correct
order and direction (clockwise). Two hands are present, one pointing to 11 and one pointing to 2.
ANY CLOCK MISSING ANY OF THESE ELEMENTS IS SCORED ABNORMAL. REFUSAL TO DRAW A CLOCK IS SCORED
ABNORMAL.
SOME EXAMPLES OF ABNORMAL CLOCKS (THERE ARE MANY OTHER KINDS)
Abnormal Hands Missing Number
................................ ................................ ................................ ................................ ................................ ................................ ................................ .
Mini-CogTM, Copyright S Borson. Reprinted with permission of the author, solely for clinical and teaching use. May not be modified or
used for research without permission of the author ([email protected]). All rights reserved.
Mini-Cog
Pass
• > 4
Fail
• 3 or less
Borson S., Scanlan J, Brush M et al. 2000. The Mini-Cog: A cognitive “vital signs”
measure for dementia screening in multi-lingual elderly. Int J Geriatr Psychiatry, 15,
1021-1027.

1/20/2015
9
Mini-Cog Research
• Performance unaffected by education or language • Borson Int J Geriatr Psychiatry 2000
• Sensitivity and specificity similar to MMSE (76% vs. 79%; 89% vs. 88%)
• Borson JAGS 2003
• Does not disrupt workflow & increases rate of diagnosis in primary care
• Borson JGIM 2007
• Failure associated with inability to fill pillbox • Anderson et al Am Soc Consult Pharmacists 2008
Mini-Cog: Sam
26
http://youtu.be/CRQEighdb0w
SLUMS
1/20/2015
10
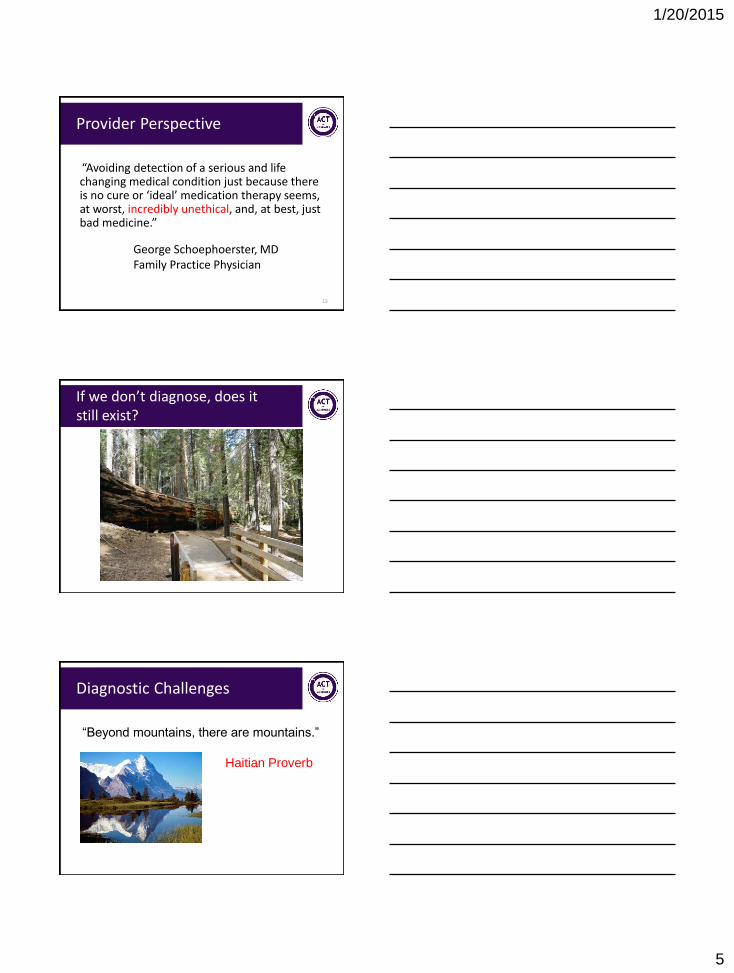
SLUMS
High School Diploma Less than 12 yrs education
Pass > 27 > 25
Fail 26 or less 24 or less
28
Tariq SH, Tumosa N, Chibnall et al. Comparison of the Saint Louis University mental
status examination and the mini-mental state examination for detecting dementia
and mild neurocognitive disorder--a pilot study. Am J Geriatr Psychiatry. 2006
Nov;14(11):900-10.
MoCA
MoCA
Pass
• > 26
Fail
• 25 or less
30
Nasreddine ZS, Phillips NA, Bédirian V, et al. The Montreal Cognitive Assessment
(MoCA©): A Brief Screening Tool For Mild Cognitive Impairment. J Am Geriatr Soc
53:695–699, 2005

1/20/2015
11
Screening Tool Selection
Montreal Cognitive Assessment (MoCA) • Sensitivity: 90% for MCI, 100% for dementia
• Specificity: 87%
St. Louis University Mental Status (SLUMS) • Sensitivity: 92% for MCI, 100% for dementia
• Specificity: 81%
Mini-Mental Status Exam (MMSE) • Sensitivity: 18% for MCI, 78% for dementia
• Specificity: 100%
Larner et al Int Psychogeriatr 2012; Nasreddine et al J Am Geriatr Soc 2005; Tariq et al Am J Geriatr Psychiatry
2006; Ismail et al Int J Geriatr Psychiatry 2010
Cognitive Screening Flow Chart
32
Cognitive Impairment Identification Flow Chart
33

1/20/2015
12
Dementia Work-up and Diagnosis
34
Dementia Work-Up
35
36

1/20/2015
13
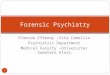
Dementia Diagnoses
Alzheimer’s Disease
Vascular Dementia
Lewy Body Dementia
FTD
Alzheimer’s disease: 60-80 % • Includes mixed AD + VD
Lewy Body Dementia: 10-25 % – Parkinson spectrum
Vascular Dementia: 6-10 % – Stroke related
Frontotemporal Dementia: 2-5 % – Personality or language
disturbance
Delivering the Diagnosis
• General guidelines:
– Include a family member in the visit if at all possible
– Talk directly to the person with dementia
– Speak at a slower, relaxed pace using plain words • Try not to fill the time with words – less is more
– Explain why tests were ordered and what results mean
– Ask at least 3 times whether the patient / family has any questions
– Acknowledge how overwhelming the information feels; provide empathy, support, reassurance
38
Delivering the Diagnosis
• Focus on wellness, healthy living, and optimizing function
– Sleep
– Exercise
– Social and mental stimulation
– Nutrition and hydration
– Stress reduction
– Increase structure at home
39
Zaleta AK and Carpenter BD. Patient-Centered Communication During the Disclosure of a Dementia
Diagnosis. AM J ALZHEIMERS DIS OTHER DEMEN 2010, 25: 513

1/20/2015
14
Delivering the Diagnosis
• Connect patient/family to community resources – Care for both patient and caregiver
– Examples: Senior linkage line, Alzheimer’s Association
• Discuss follow-up – Want to see patient and family member at regular
intervals (e.g., q 6 months) for proactive care
– Discuss involvement of care coordinator
• Provide written summary of visit 40
Common Questions
• How is Alzheimer’s different from dementia?
• Is there any treatment? What can we do?
• How fast is this going to progress?
• How often do we see you?
• What’s next?
41
Delivering the Diagnosis: Sam
42
https://www.youtube.com/watch?v=vy2ZC5ZSZL8

1/20/2015
15
Dementia Care and Treatment
43
Care and Treatment
44
45
Care and Treatment

1/20/2015
16
Care and Treatment
• The care for patients with Alzheimer’s has very little to do with pharmacology and much to do with psychosocial interventions
• Involve care coordinator • Connect patient and family to experts in the
community – Example: Alzheimer’s Association – Refer every time, at any stage of disease, and for
every kind of dementia – Stress this is part of their treatment plan and you
expect to hear about their progress at next visit
46
ACT EMR Tools
• Use EMR to automate and standardize:
– Screening
– Work-up
– After visit summary with dementia education
– Orders and referrals
– Community supports www.actonalz.org/provider-practice-tools
47
Screening
48

1/20/2015
17
Labs and Orders
49
Consults and Referrals
50
Consults and Referrals
51

1/20/2015
18
Pharmacological Treatment
52
Managing Mid to Late Stage Dementia
53
Managing Dementia Across the Continuum
54
www.actonalz.org/provider-practice-tools

1/20/2015
19
Mood and Behavioral Symptoms
• Neuropsychiatric symptoms common: – 60% of community dwelling patients with
dementia
– > 80% of nursing home residents with dementia
• Nearly all patients with dementia will suffer from mood or behavioral symptoms during the course of their illness
Ferri, CP et al. Lancet 2005
Jeste, DV. ,Neuropsychopharmacology. 2008 55
56
ACT to the Rescue!
57
1/20/2015
20
Systematic Approach to Management
• Step 1: Define behavior
• Step 2: Categorize target symptom
• Step 3: Identify reversible causes
• Step 4: Use non-drug interventions first to treat target symptoms
58
Step 3: Identify Reversible Causes
• Unmet needs – Boredom – Meaning, purpose – Over/under stimulation – Pain/discomfort – Safety – Environmental stressors
• Caregiver reactions
– Limited knowledge about disease process or behaviors
59
Step 4: Non-pharmacologic Interventions
• Teach family caregivers to:
– Validate Join Distract
– Understand that behavior = communication
– Think like a behavioral analyst • Is this really a problem, and for whom?
• What is the feeling or underlying message this behavior is trying to communicate?
• How can I address the underlying need?
• How long will this solution last?
60

1/20/2015
21
Optimizing Medication Therapy
61
Top 5 Resources
62
Top 5 Resources
• Promoting wellness and function
63

1/20/2015
22
Top 5 Resources
• Addressing behavioral challenges
64
Top 5 Resources
• One stop shop for caregiver support:
Alzheimer’s Association 800.272.3900 | www.alz.org/mnnd
Care Consultation
Support Groups (Memory Club)
24/7 Helpline
65
Top 5 Resources
• Intensive Caregiver Training:
Family Memory Care
800.272.3900
66

1/20/2015
23
Top 5 Resources
• Polypharmacy:
PharmD Consult
67