Embed Size (px)
Citation preview

27.01.2018
1
Bivirkninger etter utskrivelse fra
Dagkirurgi Smerte, kvalme,kognitiv svikt, delir og fatigue etter dagkirurgi
Johan Ræder Avd. for Anestesiologi - Ullevål
Akuttklinikken, OUS
First: General considerations -------------------------------------------------- Then: 1) Pain 2) Nausea and vomiting 3) Fatigue 4) Cogn. Dysfunction, Delirium 5) Orthostatic hypotention 6) Sleep disorders 7) Surgical Complications 8) Others: nutrition, activity of daily living, mood
Ambulatory surgery post-discharge problems:
What are they and
how should we deal with them?
Brennan T: Pain 2001:152:S33-40
Pain after Outpatient surgery
- open hernia repair
Discharge to home
- 732 ambulatory patients, 8 weeks survey - Orthopedic, Lap.Cholecystectomy, Lap. Gynaecology - 298 patients (41%) made unscheduled contact with health care contacts
20% pain related 13% wound related 4% Nausea/vomiting
-355 patients, 4 weeks survey, hernia repair/arthroscopy/breast augmentation 1% (3 patients) readmitted 9% unsceduled contacts with health care 4% pain, 4% wound, 1 % other
-355 patients, 4 weeks survey, hernia repair/arthrsocopy/breast augmentation
Preop 1 week 2 weeks 4 weeks Pain 39% 43% 27% 19% Mobility problems 31% 41% 29% 17% Mood depression 11% 9% 5% 4% Sleep problems 16% 15% 9% 5%

27.01.2018
2
At home –different from Hospital:
• No iv line
• No health care personnel
• Expectation of better and improving function
Resumption of more vigorous activities
Expectations from others
• Local anaesthesia, blocks, drugs given in hospital Wean out!
Preparation for post-discharge period
• Minimize interference with normal homeostasis
• Minimize surgical trauma
+ Long acting local anaesthesia in wounds
• Minimize anaesthesia trauma – drug load
– Recovery aspects of all drugs given
– Adequate prophylaxis for pain/PONV
Risk factors present? (pain – nausea/vomit)
Post Operative Nausea/Vomiting (PONV) and PAIN: RISK FACTORS
MULTIMODALITY !!
side-effects
side-effects
side-
effects EFFECT drug A
drug B
drug C
PONV - Female - Previous PONV - Frequent travel sickness - Non-smoker - Opioid drugs - Young age - Inhalational anaesthesia - Brain nerves involved (surgical area) (type of surgery) ( stress response inflammation?)
PAIN - Female - Young age - Pre-surgical pain - Pre-surgcal opioids - Catastophizing
personality - Psycho-social
problems - Extent of surgery (stress response, inflammation?) - Nerve damage/ cutting If high risk:
1) MULTIMODAL PROPHYLAXIS!! Premedication, Preparation, Surgical method, Anaesthesia, Drugs, Others........... 2) High vigilance of SYMPTOMS: proper, rapid algorithms
1) Pain 2) Nausea and vomiting 3) Fatigue 4) Cogn. Dysfunction, Delirium 5) Orthostatic hypotention 6) Sleep disorders 7) Surgical Complications 8) Others: nutrition, activity of daily living, mood
Ambulatory surgery post-discharge problems: The “list” :
Ambulatory post-discharge pain
Ambulatory post-discharge pain
Basic prophylaxis and patient prescription:
- Paracetamol
- NSAID / Cox-II inhibitor
- Opioids «on-top» initially

27.01.2018
3
Paracetamol + NSAID Romundstad L et al. Pain 2005:177-183
paracetamol+ NSAID > NSAID > paracetamol > placebo
PARACETAMOL - oral vs. rectal (1 gr dose)
Serum
Conc.
2 4 hours
oral
rectal
Korpela et al. Acta Anaesth Scand 1999:43:245-7
Optimal, oral (70 kg) - 2 g start - 1 g x 4
22 studies, 2 307 patients:
Significant reducton with NSAID vs placebo:
-Nausea: ↓ 12%
-Vomiting: ↓ 32%
-Sedation: ↓ 29%
Cox – I inhibition
Cox – II inhibition
Indometacin (Indocid)
Ketorolac (Toradol)
Naproxen (Naprosyn)
Ibuprofen (Ibux, Brufen etc)
Diclofenac (Voltaren, Diklofenak)
Celecoxib (Celebra)
Parecoxib (Dynastat)
Rofecoxib (Vioxx))
Etoricoxib (Arcoxia)
Lumiracoxib ((Prexige))
Cox II better: • Gastrointestinal side-effects
• Cardiovascular side-effects ?
• Allergy, Asthma
• Renal
• (Bleeding ?)
• Bone/tendon/tissue (i.e.gut) healing
-------------------------------- • Importance of dose, duration and intervals
• Animal experiments vs human
• Prospective versus retrospective cohort studies
• Data versus regulatory decisions

27.01.2018
4
A cohort of 446 763 individuals including 61 460 with acute myocardial infarction was acquired.
It is shown that all traditional NSAIDs, including naproxen, appear to be associated with an increased risk of acute myocardial infarction The risk with celecoxib does not seem to be greater than that with traditional
NSAIDs. Onset of risk occurs in the first week
A cohort of 446 763 individuals including 61 460 with acute myocardial infarction was acquired.
It is shown that all traditional NSAIDs, including naproxen, appear to be associated with an increased risk of acute myocardial infarction The risk with celecoxib does not seem to be greater than that with traditional
NSAIDs. Onset of risk occurs in the first week
??? Risk of alternatives, i.e. opioids??
Inflammation! good for healing bad for pain
Anesthesia Analgesia 2007:105:481-6.
Adding dexamethasone 16 mg to
paracetamol and rofecoxib and local anaesthesia
45% Pain Free during day 1-3
120 patients scheduled for thyroid surgery were randomly assigned to: - dexamethasone 0.30 mg/kg, - dexamethasone 0.15 mg/kg - placebo.
Minor inflammation??

27.01.2018
5
A single i.v. perioperative dose of dexamethasone had small but statistically significant analgesic benefits.
No increase in infection or delayed wound healing with dexamethasone
Blood glucose levels were higher at 24 h
Forty-five studies involving 5796 patients receiving dexamethasone 1.25–20 mg
Regional blocks after discharge?
Prolonged effect after discharge? Better if done pre-operatively, i.e. preventive= before surgical trauma?
All patients pooled: - Pain was described as very strong at block resolution (8-12 hrs) in 27 (63%) patients - 26 (76%) had episodes of mild pain after 6 months.
ING. FIELD BLOCK vs. GENERAL AN. for Hernia repair, 60 patients
(Aasbø V, Thuen A,Ræder J. Acta Anaesth Scand 2002:46:674-678 )
ING. FIELD BLOCK vs. GENERAL AN. for Hernia repair, 60 patients
Aasbø V, Thuen A,Ræder J. Acta Anaesth Scand 2002:46:674-678 )
Sign. better with reg.field block (ropiva. 0,5% 50ml):
• analgesia at 0, 1h, 2h, 48h
• less analgesics day 1, 2 and 2-7
• recovery unit:
– able to sit at 18 min (vs. 72)
– able to stand/walk at 33 min (vs. 115)
– discharge ready at 102 min (vs. 280)
• better daylife function at 24h and 48 h
• more satisfied patients at 48h and day 7
No rebound pain! Analgesia beyond block duration!
Nerve block Tourniquet Injury Inflammation
Hernia
Ongoing study: - Perioperative: paracetamol+NSAID+ Glucocorticoid - Supraclavicular block

27.01.2018
6
Prolonged duration of loco-regional anaesthesia?
• Adjuncts to the (ropivacaine/bupivacaine)mixture:
– Ketorolac, dexamethasone, (clonidine?)
• Wound catheters
Few hours extra analgesia?
Until next day?
Anesth Analg 2010;110:1191–4
- Bupivacaine 2.5 mg/mL, 20 mL given every third hour for 72 hours postoperatively - Through 2 thin catheters placed on the donor site - Double-blind placebo-controlled study consisting of 2 x 20 patients.
The bupivacaine group had significantly reduced pain at rest and during coughing. The placebo group needed 2 to 3 times more opioids in the 72-hour period.
Prolonged duration of loco-regional anaesthesia?
• Adjuncts to the (ropivacaine/bupivacaine)mixture:
– Ketorolac, dexamethasone, (clonidine?)
• Wound catheters
Liposomal bupivacaine (slow release)?
Three randomized controlled trials (RCTs) and two non-randomized controlled trials (Non-RCTs), including 1214 patients significant differences (VAS) score at 24 h and 48 h Reduced morphine equivalent consumption on POD 1 Reduced incidence of nausea and vomiting .
Ceiling of effect? 13 mg bupivacaine/ml release during 48-72 hrs i.e. 0.2-0.3 mg/ml/hour released
Tramadol - more norepineprine - more serotonin - opioid Tapentadol - more norepineprine - opioid Amitryptiline
NSAID Cox-II Steroid
Ketamine Gabapentinoid
Descending control Inhibit Stimulate
To Thalamus Brainstem
Pain enhancement Pain inhibition
From Periphery
Pain Pract 2017:17:678-700 ≈ 2200 tapentadol patients vs controls (5 studies)

27.01.2018
7
Tapentadol: - Opioid sparing? vs oxycodone - Less serotonerg effects less nausea vs tramadol
More studies needed: post.operative pain, ambulatory setting
The opioids...
215 140 opioid-naive individuals 18 to 64 years of age who had undergone 1 of 8 common surgical procedures Length of initial prescription for opioid pain medication The median prescription lengths were: 4 days for appendectomy and cholecystectomy 5 days for inguinal hernia repair 4 days for hysterectomy 5 days for mastectomy, 5 days for anterior cruciate ligament repair and rotator cuff repair, 7 days for discectomy 7-day limits on initial opioid prescriptions are likely adequate Identify the 10% to 30% of patients who will require more
Other analgesics?? Optimal multimodal? Even shorter!! Individualize
Mastectomy, lumpectomy, thoracotomy, total knee/hip replacement 6% of patients continued on new opioids 150 days after surgery. Preoperative factors predicted prolonged opioid use after surgery: - legitimate prescribed preop. opioid use - self-perceived risk of addiction - depressive symptoms Each of these factors was a better predictor of prolonged opioid use than postoperative pain duration or severity
Opioids at home after ambulatory surgery:
Oral !!
- Morphine low, variable absorbed
- Codeine low/high metabolizers
- Oxycodone
- 91 women - IV oxycodone or morphine before the end of
laparoscopic hysterectomy - Continued with patient-controlled analgesia
oxycodone vs morphine for 24 h postoperatively

27.01.2018
8
Morphine vs Oxycodone PCA 2 x 45 gynaec. patients
Lenz H, Raeder J et al, Anesth Analg. 2009:109:1279-83.
Less initial pain
Less sedation
Opioid ”problems”
• Tolerance • Hyperalgesia ( chronic pain??) • Immunosuppressive (cancer, infection) • Side-effects
– Nausea, constipation, abuse, sedation, sleep disturbances, itching, urinary retention, respiratory depression
• Individual variations in receptors (genetic) • Variable enteral absorption • Less efficacy by movement induced pain but....... • Still often needed «on top»
Ibuprofen 800 mg bid 3 vs paracetamol 800 mg + 60 mg codeine bid 3, Day 0-3: 10 % «unwilling» to participate in study with codeine No differences in pain (rest, provocation, day/night) More constipation with codeine:
- 22% no defecation (vs 6%) - Less overall satisfaction
More nausea/vomiting with codeine
The two groups received as pre-medication and twice daily for 3 days. Either: - oxycodone 10 mg 25% no defecation or - Oxycodone 10 mg + naloxone 5 mg 20% no defecation
Further options - analgesia?
• Local anestesia • Paracetamol • NSAID • Coxib (cox-II spesific NSAID) • Corticosteroids • Gabapentinoid (gabapentin, pre-gabalin) (neuropatic pain) • Alfa-2 agonists (clonidin, dexmedethomidin) • Anticonvulsiva (neuropatic pain) • Antidepressiva (neuropatic pain) • Opioids • Ketamin / S-ketamin • Lidokain iv
50 patients, placebo-controlled study of 150 mg pregabalin administered before lumbar discectomy
With pregabalin: Lower VAS scores for pain at rest 0-4 h Lower morphine consumption 0-4 h No differences at 24 h and 7 days after surgery. Preoperative anxiety significantly lower
27.01.2018
9
Seventy-four studies were included. Pregabalin reduced pain scores at 2 hours in all categories: cardiothoracic, ENT, gynecologic, laparoscopic cholecystectomy, orthopedic, spine, miscellaneous procedures Pregabalin reduced 24-hour morphine consumption in gynecologic,laparoscopic cholecystectomy, orthopedic, spine and miscellaneous procedures. Pregabalin resulted in significant sedation in all surgical categories except ENT, laparoscopic cholecystectomy, and gynecologic procedures.
Pregabalin/Gabapentine – side-effects
Very common side effects (affect more than 1 in 10 people) • Sleepiness. • Dizziness. • Headache. Common side effects (affect between 1 in 10 and 1 in 100 people) • Fatigue or lethargy. • Confusion, feeling disorientated. • Shaky movements and unsteady walk. • Tremor, abnormal coordination. • Blurred or double vision.
For ambulatory?? - Selected cases - Start preoperatively - Information!! (pregabalin 75-150 mgx2)
Prospect project http://www.postoppain.org
- Procedure specific* evidence based recommendations on postoperative pain management
- Expert surgeons + anasthesiologists: Evidence based Cochrane approach (Grade A-D evidence)
- Putting evidence together to a “full package” with alternatives added
- Advice on pre-, per- and post-operative measures - Advice on surgical methods, anaesthesia methods, drugs,
adjuvants, other relevant aspects.....
*Patients AND procedures are different!! Inflammation? Neuropatic components?
http://www.anzca.edu.au
http://fpm.anzca.edu.au/documents/apmse4_2015_final
Ambulatory post-discharge nausea and vomiting (PDNV):

27.01.2018
10
- The prevalence of PDNV was 56.9%. (of 248 patients) - Antiemetic were used by a minority - Non-pharmacologic techniques of self-management used by some - The presence of PDNV affects overall quality of life, patient functioning,
and patient satisfaction.
Post Discharge Nausea and Vomiting PDNV
Risk factors: - Female gender
- Age less than 50 yrs
- History of previous post-operative nausea or vomiting (PONV) or travel sickness
- Use of opioids post-operatively
- Occurence of PONV while in the hospital
Total score: 0 7% risk of PDNV
5 89% risk of PONV
Apfel et al. Anesthesiology 2012:117:475-86
The period 8th – 120th hours postop. incidences for: postdischarge nausea: 57% (intraop ondansetron ony) vs 20%, postdischarge vomiting 20% (intraop ondansetron ony) vs 3%,
Adding: Dexamethasone iv + Oral ondansetron post-discharge
100 non-smoking female patients, gynecological laparoscopic surgery: - Palonosetron group (n = 50) 0.075 mg bolus iv - Ondansetron group (n = 50). 8 mg bolus iv + 16 mg addedd to IV-PCA Similar incidence of PONV during 48 h after operation (26% rescue in both groups) Less vomiting in the palonosetron group (18% vs. 4%, P = 0.025). No differences were observed in side effects between the groups.
93 patients, laparoscopic gynaecology, either: - Single intravenous injection of 0.075-mg palonosetron or - 40-mg oral aprepitant Similar PONV during 0–48 hours after surgery palonosetron 26% vs aprepitant 23% 0 and 2 h after administration, 40-mg aprepitant significantly less nausea severity At 6 and 24 h. less fentanyl consumption with 40-mg aprepitant
96 patients: - ondansetron disintegrating tablets 8 mg bid 2 for 3 days vs placebo
Ondansetron Placebo
Nausea 0-24 h 48% 28% Nausea 24-72 h 35% 21% Vomiting 0- 24 h 12% 8% Vomiting 24-72 h 13% 9%
Not significant Low power, confounders?

27.01.2018
11
60 ASA I and II patients, outpatient gynecological laparoscopy All patients received a prophylactic dose of ondansetron 4 mg IV at induction Immediately before discharge: ondansetron ODT 8 mg or identical placebo tablet 12 h later: second dose
Post Discharge Nausea and Vomiting PDNV
Prophylaxis/treatment: - Non-opioid analgesia post-operatively - Residual effect of hospital given anti-emetics:
- 5-HT3 block, neuroleptic, ephedrine up to 24 hr - Aprepitant, Palonosetron 48 hrs - Dexamethasone, scopolamine patch up 2-3 days
- Non-pharmaocological measures: - Adjust fluid, food intake: timing – amount - Resting, fresh air, cold forehead dressing, acupressure
- Drugs taken at home: - Tablets? Mixtures? - Orally disintergrating ondansetron - Suppositories (neuroleptics, metoclopramide)
Fatigue ??
State of:
- Physical and/or mental tiredness or weakness
- Feeling worn out, low in energy
Christensen Fatigue Scale
• NRS-scale (1-10)
• Four verbal anchors
Fatigue Assessment in a Surgical Population
• Identity-Consequences Fatigue Scale (ICFS)1
– Specifically developed for postoperative fatigue – 31 items
• ICFS 10-ShortForm (10-SF)2
– 10 items – Retains 98% of information in original ICFS
• Christensen Fatigue Scale3
– Single-item scale – NRS (1-10) with 4 anchors
1) Paddison J: J.Psycosom.Res. 2006 2) Nostdal T: J.Psycosom.Res. 2016 3) Christensen T: Br.J.Surg. 1982

27.01.2018
12
Fatigue 0-100 (0=none); Propofol vs.
Thiopentone and Desflurane
34
60
52
37
21
35
60
51
38
24
0
10
20
30
40
50
60
70
80
90
100
Preop. Day 1 Day 3 Day 6 Day 30
Desflurane (-SD) Propofol (+SD)
No difference between the groups
Fatigue; 0-100 Males vs. Females
33
52* 46
36
22
35
62*
52
38
23
0
10
20
30
40
50
60
70
80
90
100
Preop Day 1 Day 3 Day 6 Day 30
Male (-SD) Female (+SD)
Sex difference; Females report more fatigue than males at Day 1 (*p = 0.046)
Post-operative fatigue
POFS > 50 ≈ patient feel a significant «impact» on activities
Day 1 Day 3 Day 6 day 30
Post-operative fatigue
- Relevant and frequent - Not influenced by TIVA versus Inhalational - Slightly more frequent in females - No difference with: age - (others: Related to extent of surgery, tissue damage, inflammation)
- MORE RESEARCH NEEDED!!
- Epidemiology (regional vs general an?) - Benefit* from Glucocorticoids?? (Anti-inflammation) *Paulsen O, J Clin Oncol 2014 Oct 10;32(29):3221-8
Ambulatory surgery and
post-discharge cognitive function
27.01.2018
13
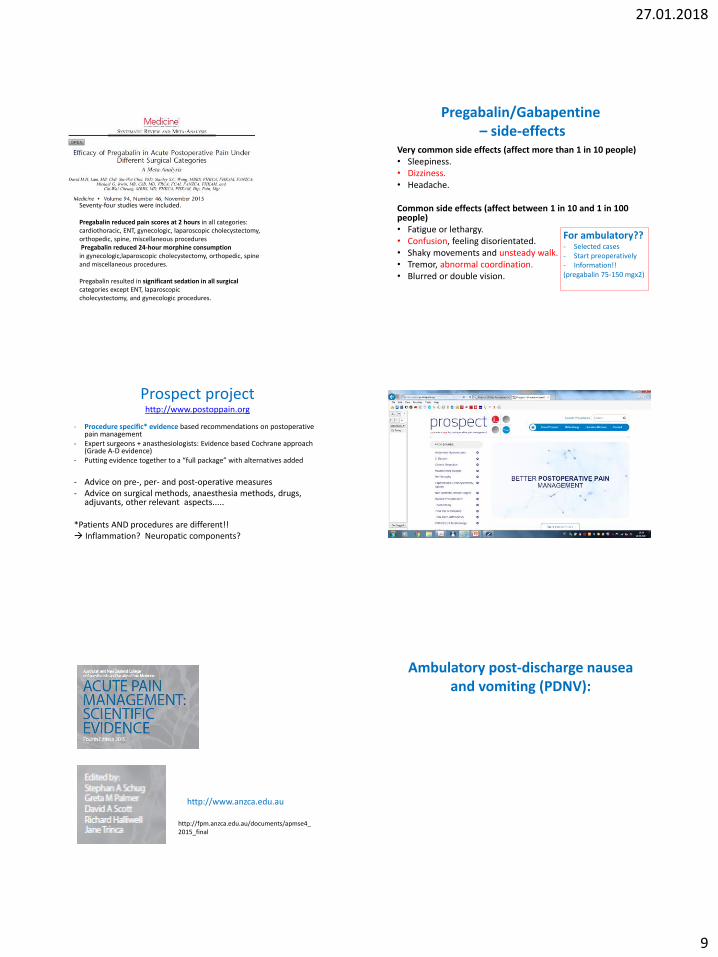
ANESTHESIOLOGY 2012; 116:1176 – 8.
J Neurosurg Anesthesiol 2013;25:33–42
Current Opinion in Anesthesiology 2011, 24:665–669
Cognitive dysfunction:
Reduced cognitive abilities on complex tasks seen during first days last for week(s), months
Delirium:
Confusion; silent or noisy
acute, often immediate last for hours, (few) days
1218 patients > 60 years Postoperative cognitive dysfunction was present: - 26% after 1 week - 10% after 3 months (controls ≈ 3%)
- Increasing age and duration of anaesthesia, little education, a second operation,
postoperative infections, and respiratory complications were risk factors for early postoperative cognitive dysfunction
- Age was only risk factor for late postoperative cognitive dysfunction.
Cognitive dysfunction, Ambulatory vs. inpat. surgery:
ISPOCD-2, 372 pat, Canet J, Raeder et al.
Acta Anaesthesiol Scand. 2003;47:1204-10.
In.pat . ambul. control
1 week: 9.8%* 3.8% 3.4%
3 months: 8.8%** 4.5% 2.8%
*P=0.03 **P=0.14
Cognitive dysfunction:
Reduced cognitive abilities on complex tasks seen during first days last for week(s), months
Delirium:
Confusion; silent or noisy
acute, often immediate last for hours, (few) days
225 non-demented patients , mean age of 70 yr undergoing either THA or TKA in a fast-track set-up The mean LOS was 2.6 days (range 1–8 days).
Twenty-two patients received general anaesthesia, and the rest had spinal anaesthesia.
No patients developed PD

27.01.2018
14
225 non-demented patients , mean age of 70 yr undergoing either THA or TKA in a fast-track set-up The mean LOS was 2.6 days (range 1–8 days).
Twenty-two patients received general anaesthesia, and the rest had spinal anaesthesia.
No patients developed PD
J Am Geriatr Soc 2014; 62:94–102,
Delirium in: 54% of the participants in Oslo 39% in Edinburgh
In a study of 400 adult patients, mixed non-cardiac surgery, admitted in the post-anesthesia care unit, presence of delirium signs : 31% of patients at admission, 15% at 30 minutes 15% at 1h 4% at PACU discharge
After discharge in the ambulatory patients? Confidential data suggests a very low rate, but there are cases
Orthostatic hypotention
• «Traditional» fainting: – Dehydration, pain, drugs (clonidine, pregabalin, gabapentin)
• Postoperative Orthostatic Tolerance – In 12-60% of patients, more with extensive surgery,
females,opioids, regular antihypertensive medication
– Resolves within 24-48 hrs
– Pathophysiology (tissue destruction? Inflammation?):
Attenuated endogenous vasopressor response,
increased vagal output
- Testing? Subcutaneous ephedrine?
Strategies for future improvement should include: - studies on high-dose steroids, - the influence of anesthesia techniques on
baroreflex function - reduction in the use of perioperative
opioids - potential preventive effect of different
alpha-1 agonists (e.g.) midodrine.
Sleep Disorders
• Low quality sleep first night
– Disturbed day-night rythme, less REM sleep (opioids)
• Increased day-time sleep
• Night 2-3: «catch-up» sleep with more REM sleep, dreams, movements (hypoxia?)
27.01.2018
15
Obstructive sleep apnoea syndrome
- Patient selection and preop evaluation!! - Patients using CPAP at home should be instructed to bring their device with them - If CPAP: should be used several days/nights after surgery, including during daytime naps - Avoid opioids/residual opioids post-operatively
- Sleep in a chair (or lateral position) - If needed: Observe opioid tolerance in the recovery unit delay discharge admit for overnight stay (and surveillance!) if in any doubt
Obstructive sleep apnoea syndrome
Post-discharge issues in
out-patient surgery Conclusions
We should prepare our patients: - What we do in the hospital - What we plan for discharge - Patient and/or relative information
- Oral - Written - Web cites
1) Pain 2) Nausea and vomiting 3) Fatigue 4) Cogn. Dysfunction, Delirium 5) Orthostatic hypotention 6) Sleep disorders 7) Surgical Complications 8) Others: nutrition, activity of daily living, mood