Embed Size (px)
Citation preview

FIMDP 2013
DEPT OF COMMUNITY MEDICINE
SRM MEDICAL COLLEGE ,SRM UNIVERSITY
&
UNSW AUSTRALIA
9TH & 10TH JAN 2013

School of Public Health and Community Medicine
Seminar on Health Care Management
9th and 10th of January, 2013
Department of Community Medicine
SRM Medical College Hospital &
Research Centre
SRM University
Clinical governance and risk
management
Why do we need clinical governance?
Hospital medicine used to be simple, ineffective
and relatively safe.
Now it is complex, effective and potentially
dangerous.
Chantler C. The role and education of doctors in the delivery of healthcare. Hollister Lecture delivered at the Institute of Health Services \
Research, Northwestern University, Illinois, USA, October 1998. Lancet 1999;353:1178–81.
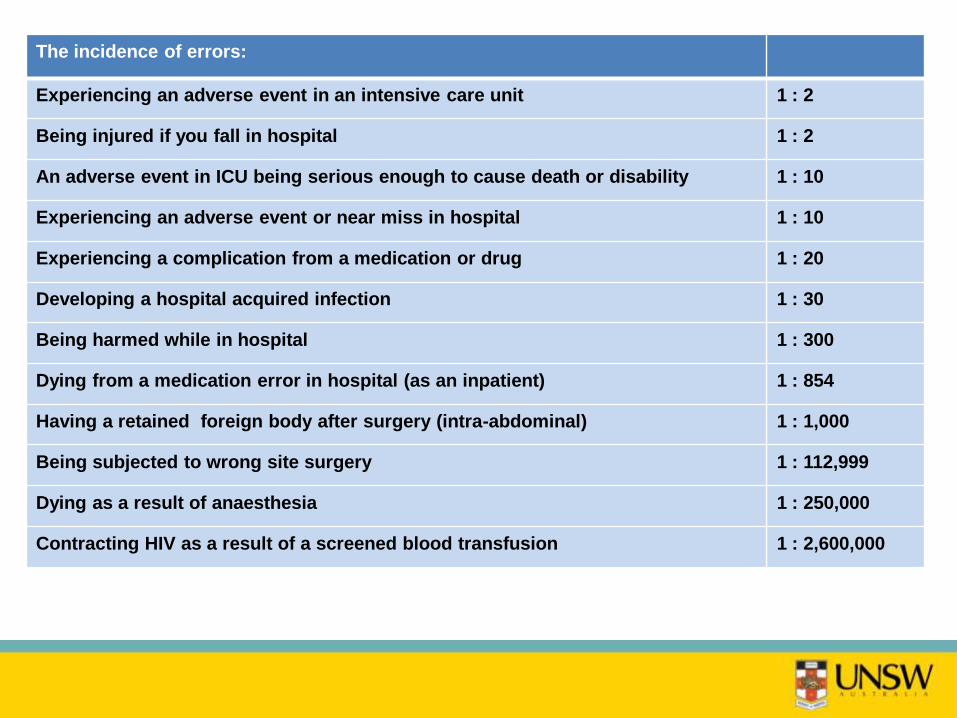
The incidence of errors:
Experiencing an adverse event in an intensive care unit 1 : 2
Being injured if you fall in hospital 1 : 2
An adverse event in ICU being serious enough to cause death or disability 1 : 10
Experiencing an adverse event or near miss in hospital 1 : 10
Experiencing a complication from a medication or drug 1 : 20
Developing a hospital acquired infection 1 : 30
Being harmed while in hospital 1 : 300
Dying from a medication error in hospital (as an inpatient) 1 : 854
Having a retained foreign body after surgery (intra-abdominal) 1 : 1,000
Being subjected to wrong site surgery 1 : 112,999
Dying as a result of anaesthesia 1 : 250,000
Contracting HIV as a result of a screened blood transfusion 1 : 2,600,000
Rates of medical errors
• United States: (lowest estimate) 44,000 - 98,000 preventable
deaths per year as a result of medical errors
• CDC estimated in 2000 that approximately 90,000 people die of
nosocomial infections alone, per year in the US
• United Kingdom: A total of 45% of patients experienced some
medical mismanagement and 17% suffered errors giving longer
hospital stay or more serious problems
• Australia: approximately18,000 preventable deaths, 50,000
permanently disabled patients per year
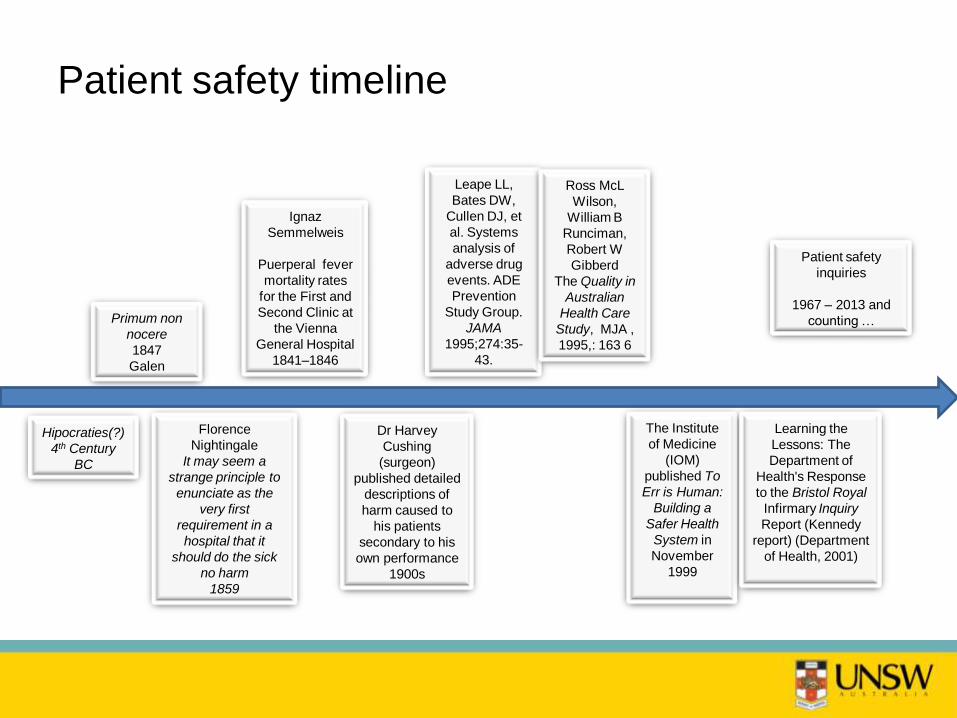
Patient safety timeline
Primum non
nocere
1847
Galen
Hipocraties(?)
4th Century
BC
Florence
Nightingale
It may seem a
strange principle to
enunciate as the
very first
requirement in a
hospital that it
should do the sick
no harm
1859
Dr Harvey
Cushing
(surgeon)
published detailed
descriptions of
harm caused to
his patients
secondary to his
own performance
1900s
The Institute
of Medicine
(IOM)
published To
Err is Human:
Building a
Safer Health
System in
November
1999
Leape LL,
Bates DW,
Cullen DJ, et
al. Systems
analysis of
adverse drug
events. ADE
Prevention
Study Group.
JAMA
1995;274:35-
43.
Ignaz
Semmelweis
Puerperal fever
mortality rates
for the First and
Second Clinic at
the Vienna
General Hospital
1841–1846
Ross McL
Wilson,
William B
Runciman,
Robert W
Gibberd
The Quality in
Australian
Health Care
Study, MJA ,
1995,: 163 6
Learning the
Lessons: The
Department of
Health's Response
to the Bristol Royal
Infirmary Inquiry
Report (Kennedy
report) (Department
of Health, 2001)
Patient safety
inquiries
1967 – 2013 and
counting …
Patient safety ten years on ...
• Institute of Medicine To err is human
• Bristol Royal Infirmary Inquiry
But
• Patient safety has been a concern since the origins of medicine
(Hippocratic oath/Florence Nightingale)
• Concerns raised in the 1800s (eg hand hygiene) continue to this day
and for very similar reasons –
• „we can cure childhood cancer, but we can‟t get clinicians to
wash their hands‟

What is clinical governance?
Clinical governance is a systematic approach to
maintaining and improving the quality of patient
care within health systems
Why did clinical governance
emerge?
The emergence of clinical governance …
Links between corporate and clinical
governance
• Scally and Donaldson: “a system through which NHS organisations
are accountable for continually improving the quality of their services
and safeguarding high standards of care by creating an environment
in which excellence in clinical care will flourish.”2 (p. 62)
• Western Australian Government: “a systematic and integrated
approach to assurance and review of clinical responsibility and
accountability that improves quality and safety resulting in optimal
patient outcomes” (2001: 2)
Characteristics of events sparking
inquiries
• Widespread loss of life
• Threats to public health or safety
• Failure by the state in its duty to protect
• Failure in regulation
• Shocking events
Landmark Chambers, 2009
Study of eight inquiries: the need for CQI
• Eight inquiries, six countries:
– Bristol Royal Infirmary (UK)
– Campbelltown and Camden (Australia)
– Celjie Hospital (Slovenia)
– Glasgow‟s Victoria Infirmary (UK)
– King Edward Memorial Hospital (Australia)
– Royal Melbourne Hospital (Australia)
– Southland DHB Mental Health Services (New Zealand)
– Winnipeg Health Services Centre (Canada)
• Paediatric cardiac surgery, tertiary care, ED, pathology, gynaecology and obstetrics,
mental health services
Hindle, Braithwaite, Travaglia (2006)
Culture of high risk healthcare
• Quality healthcare is not evenly distributed;
• Health care can continue to operate far below standard for years, and sometimes
decades;
• Quality improvement processes are often deficient;
• Lack of supervision and monitoring;
• Lack of balance between professional autonomy and individual, team or professional
responsibility;
• Deficient teamwork, including lack of understanding and respect for other
professions;
• Denial or suppression of early warning signs;
• Dismissal of patient and clinician concerns;
• Failure of timely transmission of vital information to responsible individuals;
• Suppression and abuse of whistleblowers;
• Routine circumventing of existing procedures and protocols.
Hindle, Braithwaite, Travaglia (2006)
• The Ely Hospital, Wales (1967) - long stay patients, elderly
• Banstead Hospital, Cowley Road Hospital, Friern Hospital, St. James's Hospital, StorthesHall Hospital, St. Lawrence's Hospital, Springfield Hospital, UK (1968) – elderly
• Normansfield Hospital, Middlesex, UK (1978) people with learning disabilities
• Inquiries into the circumstances of the death of various children and others and the first Ashworth Inquiry Ashworth, UK (1985-96) –children
• Stanley Road Hospital, Wakefield, UK (1986) –elderly patients
• Cervical screening services, Cartwright Inquiry, NZ (1987 – 1988) – women
• Chelmsford Royal Commission, NSW (1990) –psychiatric patients
• Ashworth Special Hospital Inquiry, UK (1999) -criminal psychiatric patients
• Rodney Ledward, UK (1999) – women
• Grantham and Kesteven Hospital, Allitt -Clothier Report (1992, 1994) - children
• Winnipeg Health Services Centre, Canada (1995 – 1998) – children
• Cervical screening services at Kent and Canterbury Hospitals Trust - Wells Report, UK (1997) – women
• Royal Liverpool Children’s Inquiry (Alder Hey –Ashton report), UK (2000) – children
• King Edward Memorial Hospital, WA (2000 –2001) – women
• Bristol Royal Infirmary, Kennedy Report, UK (2001) – children
• The Victoria Climbié Inquiry, UK (2001) – child
• RMH, Victoria (2002) - the elderly
• Southland DHB, NZ (2001-2002)- psychiatric patient
• Three Inquiries: The Kerr/Haslam, Ayling, Neale, Inquiries (2003-2004) – psychiatric patients, women
• Camden and Campbelltown Hospitals, NSW(2002-2003)– locational disadvantage, lower SES, people from NESB
• Shipman, UK (2005) - elderly women, isolated individuals
• Healthcare Commission, Clostridium difficile(Stoke Mandeville, Maidstone and TumbridgeWells), UK (2006)
• Bundaberg, Patel Inquiries, Queensland (2006) –locational disadvantage, lower SES, Aboriginal and Torres Strait Islander patients
• E.coli Inquiry, South Wales (2006) – child
• Garling Inquiry Reeves, NSW (2008) – women;
• Garling Inquiry (acute healthcare), NSW (2008)
• Stafford General Hospital, UK (2010) – ED, elderly, confused, dying patients
Patient safety inquiries

Francis Inquiry into Stafford Hospital (2010)
• target-driven priorities which generated fear
• disengagement between clinicians and management
• low staff morale
• isolation
• lack of openness
• acceptance of poor standards of conduct
• reliance on external assessments
• denial
• bullying
• lack of information about patients‟ care or condition
• lack of involvement in decisions
• failure of communication between staff
• lack of engagement with families and friends

Inquiry recommendations range up to several
hundred. Most suggest variations on three
strategies:
• Organisational, service or team restructuring;
• Policy and guideline development;
• Staff training.
18

What does clinical
governance involve?
The key elements of clinical governance
• Recognisably (ie publicly available) high
standards of care
• Transparent responsibility and
accountability for those standards
• A constant dynamic of improvement (CQI)
Braithwaite and Travaglia (2008)
Links made between
corporate and clinical
governance
Strategies to ensure the effective
exchange of knowledge and
expertise
Sponsoring of a patient centred
approach to service delivery
Structures to improve quality and safety and
manage risk
Focus on quality assurance and
continuous improvement
Other aspects of CG
• Education and training
• Clinical audit
• Clinical effectiveness
• Research and development
• Openness
• Risk management
• Information Management

Link between corporate and
clinical governance
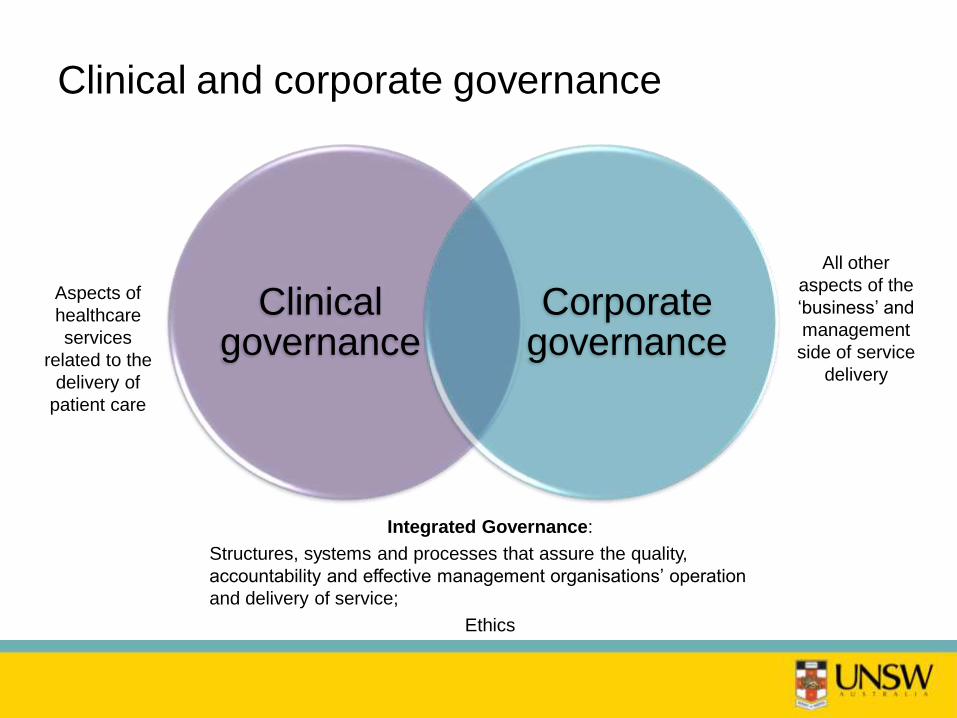
Clinical and corporate governance
Clinical governance
Corporate governance
Integrated Governance:
Structures, systems and processes that assure the quality,
accountability and effective management organisations‟ operation
and delivery of service;
Ethics
Aspects of
healthcare
services
related to the
delivery of
patient care
All other
aspects of the
„business‟ and
management
side of service
delivery
What is the link between clinical and corporate
governance?
Errors and adverse events are:
Either the result of incompetent clinicians
Or they are the result of incompetent managers
Or option 3:
They are the result of a failure to implement evidence based practice
AND evidence based management
I believe patient safety must be a fundamental component
of a modern health service.
It is closely connected with issues such as clinical
governance and evidence-based practice.
The culture of the NHS must change from a closed blame-
centred culture, to an open learning one.
We must not only ask the question „who made the
mistake‟? But what features of the health
organisation created the conditions where mistakes are
more likely‟?
CMO Sir Liam Donaldson
The importance of knowledge
exchange
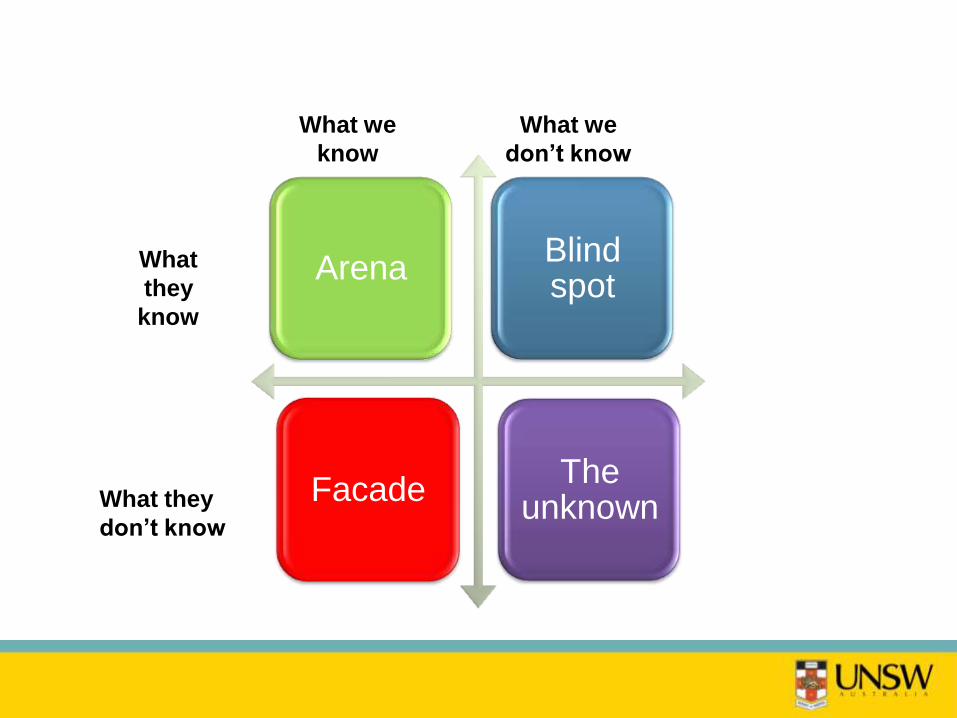
Arena
Facade
Blind spot
The unknown
What we
don’t know
What
they
know
What they
don’t know
What we
know
What we know most about
• Types of errors [for certain groups]
• Rates of errors
• Systems/technical causes of errors
• Experience of clinicians {?}
• Errors of commission
• Types of patients who experience errors
• Differential rates of errors
• Errors of omission
• Sustained quality improvements
To distinguish:
• Data: are collections of facts, figures, statistics:
the building blocks (can be usable or not)
• Information: are data with a meaning by way of
a relational context (organised or processed
data – the who, what, when and where)
• Knowledge: is the appropriately applied data
and information (relevant, actionable) – the how
• Wisdom: evaluated understanding (discern,
judge)
Requirements of wisdom
• Emotional regulation – coping
• Knowing what‟s important
• Moral reasoning
• Compassion
• Humility (epistemic, cultural and other)
• Altruism
• Patience
• Dealing with uncertainty
(Hall, S.S. (2010) Wisdom: from philosophy to neuroscience. QUP: St Lucia.
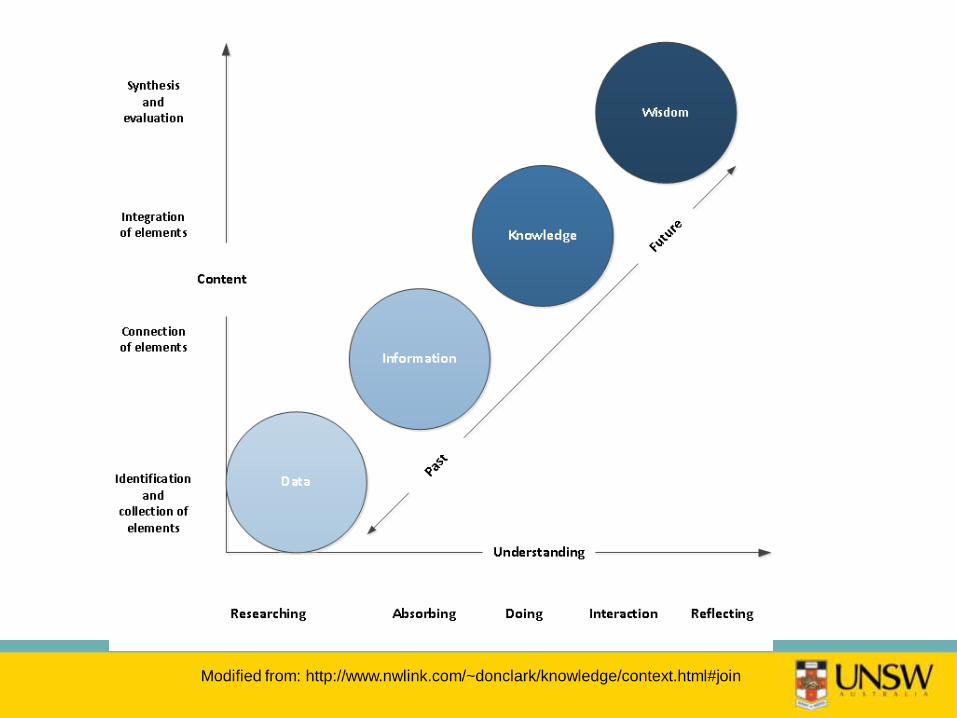
Modified from: http://www.nwlink.com/~donclark/knowledge/context.html#join

The five tasks of health managers*
1. Generating new knowledge
2. Accessing/discovering existing knowledge
3. Capturing, representing and embedding knowledge
4. Facilitating knowledge development and application
5. Transferring knowledge across individuals, teams,
units, services and systems
Adapted from Helen Bevan’s work on from knowledge management

Patient/person centred
approach to care
Patient centred care
Health care that establishes a partnership
among practitioners, patients, and their families
(when appropriate) to ensure that decisions
respect patients’ wants, needs, and preferences
and that patients have the education and
support they need to make decisions and
participate in their own care
Institute of Medicine (2001) Crossing the Quality Chasm
Patient centred care focuses on:
• Whole-person care
• Coordination and communication
• Patient support and empowerment
• Ready access
Bechtel C.If You Build it, Will They Come? Designing Truly Patient-Centered Health Care. Health
Affairs.
Background – definition
• Risk has been defined as a central cultural construct of recent
times
• Risk can be understood as the possibility (or chance) of harm of
loss to an individual or group, the magnitude of that loss or harm
and the probability of its occurrence.
• Risk appears throughout the patient safety literature. There are the
risks associated with most medical treatments, often categorised
as „side-effects‟, complications or adverse events.
• In this context risk involves “... accepting that some degree of harm
may be unavoidable in many clinical situations is clearly
appropriate where the risks are weighed against the expected
benefits.”
• In comparison, vulnerability in healthcare has been
called the elephant in the room of healthcare (Hurst:
2008)
• Unlike the concept of risk, which has undergone
sustained examination over a decade, vulnerability has
proven difficult to define and is under-researched.
• While risk of harm is well understood, less is known
about patients‟ (either as individuals or in groups)
vulnerability to harm.
What is vulnerability?
• Vulnerability has been defined as susceptibility to any kind of
harm, whether physical, moral or spiritual, at the hands of an
agent or agency, a factor which … needs to be recognised
and negotiated in health care transactions. (Hurst: 2008)
• A functional definition of vulnerability is an individual or
groups' susceptibility to risk of harm.
• Vulnerability can be identified as occurring as a result of one
or more social, structural, situational or [we will argue]
systems causes
• Theoretically, the risk of injury and death as a result of
unexpected, unconsidered, incompetent, or incomplete
actions is equal for all patients.
• Yet there are indicators from patient safety studies to
suggest that certain individuals and groups may be
particularly vulnerable to errors, when social factors
(such as ethnicity, disability, gender and socio-economic
status) are considered.
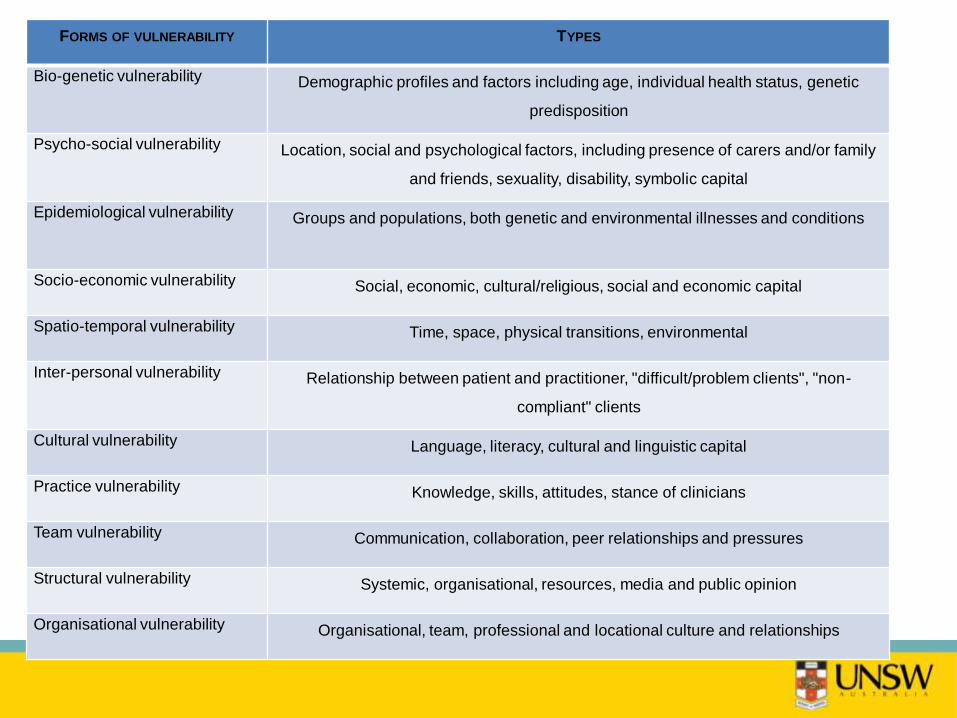
FORMS OF VULNERABILITY TYPES
Bio-genetic vulnerability Demographic profiles and factors including age, individual health status, genetic
predisposition
Psycho-social vulnerability Location, social and psychological factors, including presence of carers and/or family
and friends, sexuality, disability, symbolic capital
Epidemiological vulnerability Groups and populations, both genetic and environmental illnesses and conditions
Socio-economic vulnerability Social, economic, cultural/religious, social and economic capital
Spatio-temporal vulnerability Time, space, physical transitions, environmental
Inter-personal vulnerability Relationship between patient and practitioner, "difficult/problem clients", "non-
compliant" clients
Cultural vulnerability Language, literacy, cultural and linguistic capital
Practice vulnerability Knowledge, skills, attitudes, stance of clinicians
Team vulnerability Communication, collaboration, peer relationships and pressures
Structural vulnerability Systemic, organisational, resources, media and public opinion
Organisational vulnerability Organisational, team, professional and locational culture and relationships
Roux-Dufort
What is it within all our systems that
makes us at risk for lower quality care
and poor outcomes?
Who is vulnerable within healthcare?
Participants‟ responses were allocated to four categories of high risk
groups:
1. Clinicians;
2. Individuals with bio-medical conditions;
3. Patients with liminal status; and
4. Socially vulnerable groups
Braithwaite, Travaglia, Nugus (2006)
Vulnerable patients
• The elderly and frail
• Indigenous communities and individuals
• People from culturally and linguistically diverse backgrounds and
refugees
• People with disabilities, especially cognitive impairments, mental
illnesses and sensory disabilities
• Children and youth
• Patients with literacy and communication problems
• People from lower SES
• Geographically isolated individuals
• Socially isolated individuals
• The homeless
• The frail and malnourished
• Patients with co-morbidities and chronic illness
• Patients with high acuity
Phase 2: vulnerable patients
• Patients with liminal status:
• Rapidly deteriorating patients;
• Patients in transit;
• Patients discharged early;
• Patients in emergency departments and Intensive Care
Units;
• Prisoners; and
• Certain locations and times
Braithwaite, Travaglia, Nugus (2006)
Structural responses and CQI
responses to patient safety

Structures to improve the quality and safety and management of risk
Modern patient safety
movement
Recognition of errors as a
major cause of death and disability Introduction
of error reporting systems
Protection of staff who
report errors
Performance standards (at
different levels)
Creation of safety
systems (including
clinical governance)
Comprehensive approach
to QI and safety
Focus on finding error
causes
Use of team training and simulation
Building leadership
and knowledge

Conclusion
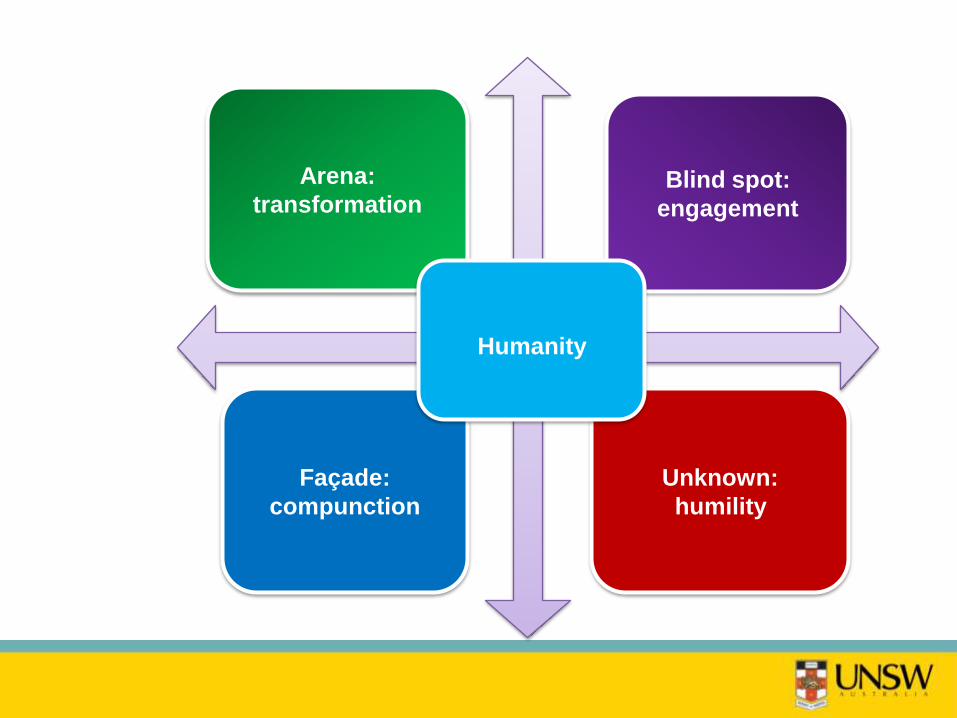
Arena:
transformationBlind spot:
engagement
Façade:
compunction
Unknown:
humility
Humanity
THANK YOU





























