Embed Size (px)
Citation preview
2/26/2013
1
Jennifer A. Greene, MD Assistant Professor, Associate Program Director
University of South Carolina School of Medicine
Department of Obstetrics and Gynecology
February 22nd, 2013
Infanticide
o Earliest recorded means
• control family size
o Safe and effective
o Methods
• Suffocation
• Exposure/Neglect
• Drowning
Moran, Dianne R., Infanticide. Encyclopedia of Death and Dying. www.deathreference.com Sept. 11, 2006.
Abortion
o “Potions”
• Colonial “home medical” guides
• Recipes for "bringing on the menses"
• Herbs:
• grown in one's garden
• easily found in the woods
• Commercial preparations:
• Mid eighteenth
• Widely available
• Often fatal
Pollitt, Katha. Abortion in American History. The Atlantic Online. May 1997

2/26/2013
2
Abortion
o Potions
• 1820’s-1830’s--first statutes regulating abortion
• Banned commercial abortifacients
• More like poison-control laws
• Abortion per se was not banned
• 1840s abortion business was booming
• Legal until the late 1900’s—before quickening (4 months)
Pollitt, Katha. Abortion in American History. The Atlantic Online. May 1997
Abortion
o Surgical
o 1723—France
• Modern curette
• French verb, curer, "to cleanse“
• Developed for general surgery
o 1842—France--J. Recamier
• Utilized curette for uterine application
• Reintroduced the vaginal speculum
o 1870s—Germany--Alfred Hegar
• Created cervical dilators “Hegars”
• Dilation and curettage (D&C)
• widely practiced during the last quarter of the nineteenth century
Boston Women’s Health Book Collective. Our Bodies Ourselves For The New Century. May 4, 1998.
Abortion o Surgical o Antisepsis:
• Not discovered until the late 1860’s
• Joseph Lister, based on Luis Pasteur’s
o D&C for abortion: eventually • More effective and safe
• Compared to common herbal remedies • 19th century
• Posed greater danger • when performed by unskilled abortionists
• or without adherence to proper antiseptic techniques.
o 1940’s: Penicillin • Routinely used in medical practice
Boston Women’s Health Book Collective. Our Bodies Ourselves For The New Century. May 4, 1998.

2/26/2013
3
Abortion
o Surgical
• Mid 19th century—
abortion outlawed
• 1973: U.S. Supreme Court:
Roe v. Wade
• the ``right of privacy...founded in
the Fourteenth Amendment's
concept of personal liberty...is
broad enough to encompass a
woman's decision whether or not to
terminate her pregnancy.'‘
• Availability: safe abortion
Boston Women’s Health Book Collective. Our Bodies Ourselves For The New Century. May 4, 1998.
First recorded use 1850 BC
o Ancient Egypt
• Crocodile dung pessary
• Fermented dough
o Various other formulations through history
• Acacia berries, honey, dates, wool
• Barrier effect +/- acidity of berries
1800’s
o Laboratory research
• Inhibitors of sperm motility
• Line of thinking led to modern spermicides
• Predecessor:
• Lysol® - feminine hygiene
- post coital douche (70% failure)

2/26/2013
4
Foam
Gel
Cream
Film
Suppository
Tablet
Nonoxyl-9 o 1960’s
o $8 per package
o Various forms--vehicle
o Only spermicide (USA)
o Non-ionic Surfactant • Attacks acrosomal membrane
• Sperm immobilization
o Perfect use 1st year failure: 15% o Typical use 1st year failure: 26%
Foam
Gel
Cream
Film
Suppository
Tablet
Nonoxyl-9 o Added benefits:
• Greater STI protection • N. g., C. t., HIV
o FDA: 2003 • Package warning
• No decrease risk • N. g., C. t.
• Increased risk HIV (UNAIDs) • Epithelial disruption
• >once daily
• Vagina/Rectum
• Increased risk N. gonorrhea • JAMA (2002)
o Increased risk HPV
Van Dame L. Advances in topical microbicides. Presented at the XIII International AIDS Conference, July 9--14, 2000, Durban, South Africa
New Warning for Nonoxynol-9 OTC Contraceptive Products re: STDs and HIV/AIDS. FDA.GOV. 2009.
Marais D, Carrara H, Kay P, Ramjee G, Allan B, Williamson AL. The impact of the use of COL-1492, a nonoxynol-9 vaginal gel, on the presence of cervical human papillomavirus in
female sex workers. Virus Res. 2006 Nov;121(2):220-2. Epub 2006 Jul 24.
WHO/CONRAD Technical Consultation on Nonoxyl-9. Summary Report. Geneva. October, 2001.
Cochrane Review-2008.
Nonoxyl-9 o WHO, FDA, CDC
• Due to HIV risk:
• Not suitable for:
• Women at high risk for STI
• Sex workers, multiple partners, frequent coitus
• Use more than once daily
• Rectal use
• Better
• Than no method
• As a secondary method; in addition to:
• Diaphragm
• Cervical cap
• Condom

2/26/2013
5
Today Sponge® o 1983
o OTC
o $13-19 (package #3)
o Plastic foam sponge + Nonoxyl-9 (1000mg) • Effective x 24 hours
• Barrier + Spermicide + Absorption
o Nulliparous: Perfect use: 9%; Typical use: 26%
o Multipara: Perfect use: 16%; Typical use: 32%
o Availability: • Removed: 1994; Produced: 2005
• Removed: 2007; Re-launched: 2009
o Made famous by Seinfeld’s—Elaine • “Sponge-worthy”
Today Sponge® o Toxic Shock Syndrome
• CDC: MMWR
• 4 reported cases 1983--Staph aureus
• 37 days PP
• 32 hours in place
• 5 days
• Fragmented removal
• JAMA: 1986 --13 total cases
• 13 confirmed cases
• Risk low overall
• Increased association
• Menses
• Use in the puerperium
• Delayed/incomplete removal
1) MMWR. February 03, 1984 / 33(4);43-4,49
2) Faich, G. etal. JAMA. 1986 Jan 10;255(2):216-8.
Today Sponge® o Toxic Shock Syndrome
• FDA mandated package warning (Dec. 1983)
• Outer box--highlighted
• Package insert
• “uncertain risk” TSS
• Not to be left in >30 hours
• Not to be used during menses
• Medical attention:
• Fragmented/incomplete removal
• S&S TSS:
• fever, rash, N/V, confusion
• myalgia, vaginal D/C
• Medical consultation prior to use:
• h/o prior TSS
• Recently post partum

2/26/2013
6
Male Condom: o 1000 B.C. - ancient Egypt
• Images:
• Linen, leather, oiled silk paper sheathes
• Thin hollow horns
• Protection vs. Ritual
o 1500’s - Gabrielle Fallopius (Italy)
• Linen sheaths useful for prevention of Syphilis and pregnancy
o 1844 - Vulcanization of “rubber”
• Condoms mass-produced
• Stronger and more elastic
• Washed and re-used!!
Cichocki, Mark. The History of Condoms. Ask.Com. April, 2007
Male Condom: o 1912 - Latex Condoms-developed
• Cheap and disposable; single-use condom is born
• World War II, mass produced • provided to troops worldwide
o 1950’s - Latex Condoms-improved • Thinner, tighter and lubricated
• Reservoir tip introduced; semen collection • decrease leakage and unintended pregnancy
o 1990’s – Polyurethane Condoms-developed • Alternative to latex
• Less allergenic, permissible with oil based lubricants
• No odor, less storage restrictions
• Less elastic; more slippage/breakage, less “natural” feel
Cichocki, Mark. The History of Condoms. Ask.Com. April, 2007

2/26/2013
7
o Male Condom: o OTC
o Synthetic: Latex, Polyurethane
• $5 and up (package #3)
o Natural: Lamb (cecum)
• >$3 per single condom
• Proposed decreased STI protection
• Intestinal pores; no conclusive data
o Perfect use: 2%
o Typical use: 18%
• Motivation/consistency*
o Male Condom: o Added benefit:
• Proven STI protection
• N. g., C. t., HIV
• some HPV
• Synthetic: Highly effective
• Natural: Less effective
• 3-5% slippage/breakage
• Increased w/polyurethane
• 2.6-5 times
o Decrease failure rates by coupling with EC*
o Male Condom: o Spermicide: Nonoxyl-9
• No improved protection
• Pregnancy vs alternate lubricants
• Increased risk:
• N. gonorrhea, C. trachomatis, HIV
o Phased out after 2001
• No protection from STIs (N. g., C. t.)
• Increased risk of HIV & N. g.
• Unsafe for high risk individuals
• Multiple partners, frequent intercourse, high STI locale
• Better than no condom at all
WHO/CONRAD Technical Consultation on Nonoxyl-9. Summary Report. Geneva. October 2001

2/26/2013
8
Female Condom: o Polyurethane
• (1990)
• FC-1 (FDA 2003)
• Expensive
• Noisy • Poor acceptance
o Synthetic Nitrile
• (2005)
• FC-2 (FDA 2009)
• Less noise
• Thinner
• Less expensive
• Any lubricant
o FC female condom ®
• FC-1
o Reality®
o Femy®
o Femidom®
o FC -2®
o Care®
o Dominique®
o Myfemy®
o Protectiv®
Beksinska, M et al (2010) 'Female condom technology: new products and regulatory issues', Contraception, published online 14th September 2010.
Female Condom: • $5.99 3-pack
• Perfect use: 5%
• Typical use: 21%
Limitation:
o Acceptability • Up to 90% (WHO)
• West < Worldwide
Decrease failure rates by coupling with EC*
Hoffman, Susie. The Future of the Female Condom. International Family Planning Perspectives. Guttmacher Institute. Volume 30,
Number 3, September 2004.
Choi K-H et al., Patterns and predictors of female condom use among ethnically diverse women attending family planning clinics, Sexually
Transmitted Diseases, 2003, 30(1):91-98.
Cervical Cap: o 19th century
• Friedrich Wilde—Germany
• Custom made rubber cervical caps
• Prior to vulcanization of rubber
• high rates of degradation
o 20th century
• 1927—Vimule® Cap--rubber->latex
• 1930’3—Prentif® Cap—rubber->latex
• 1940’s—Dumas® Cap—plastic->latex
• 1960’s--Dramatic decrease in use
• introduction COC
Cervical Caps". Cervical Barrier Advancement Society. March 2005. http://www.cervicalbarriers.org/information/cervicalcaps.cfm. Retrieved 2008-04-26. Weiss BD, The Cervical Cap. In reply. American Family Physician. 1991 Oct; 44(4):1139.
2/26/2013
9
Cervical Cap: o FemCap® (FemCap, Inc.--2003)
• $60
• Silicone
• Rx—must be fitted • Planned Parenthood/Gen OB/GYN
• 22mm, 26mm, 30mm
• At least 6-8 hours post coitus
• Max: 48 hours
• TSS not reported • Avoid during menses
o Perfect use: 5%
o Typical use: 21% • Should be combined with spermicide
• Proven Infectious benefits: • Decreased: N. g., C. t.
• No protection from HIV
Lauersen, NH., etal. The Cervical Cap: Effectiveness, Safety and Acceptability as a Barrier Contraceptive. Mt Sinai J Med. 1986 Apr; 53(4): 233-8.
Diaphragm o 1844—USA--Charles Goodyear—Vulcanization of Rubber
o 1880s—Germany--C. Haase—(P.J. Mensinga) • first to describe
• rubber contraceptive device
• spring molded into the rim
• The Mensinga diaphragm—
• only brand available for many decades
o 1860’s—USA--Edward Bliss Foote • designed an early form
• "womb veil" released
o 1940: 33% U.S. married couples using the diaphragm
o 1960’s—use dropped dramatically • Introduction:
• IUD & COCs
o 1965—10% U.S. married couples using the diaphragm
Evolution and Revolution: The Past, Present, and Future of Contraception". Contraception Online (Baylor College of
Medicine) 10 (6). February 2000
Diaphragm o Ortho All-FlexTM ($15-75)
• Silicone
• Must be fitted/ordered
• Planned Parenthood
• General OB/GYN
• 24-30 hours
• Proven Infectious benefits:
• Decreased: N. g., C. t., HPV
• No protection from HIV
o Perfect use: 5%
o Typical use: 21% • Should be combined with spermicide
• Risk: TSS
• Avoid during menses
2/26/2013
10
Combination Oral Contraceptives (COCs)
o 1957—FDA approved
• Not for contraception
• Only for “severe menstrual disorders”
• Substantial increase in severe menstrual disorders
o 1960--approved for contraceptive use
o 1963--2.3 million U.S. women “on the pill”
o 1964—remains illegal in 8 states
o 1965—6.5 million U.S. women using the pill
• Most popular form of birth control U.S.
o 1972—Supreme Court legalized pill use
• Regardless of marital status
o Few warnings/little publicity regarding side effects
Nicolchev, Alexandra. A brief history of the birth control pill. www.pbs.org. May 7, 2010
Combination Oral Contraceptives (COCs)
o 1960’s—Early Formulations
• Mestranol {→ Ethinyl Estradiol (EE)}
• 1st orally active estrogen
• High doses →ensure:
• clinical efficacy/pregnancy prevention
• 150 μg mestranol
• (10 mg norethynodrel)
• Side effects:
• Minor:
• Nausea, breast tenderness, fluid retention
• Mood changes, weight gain, melasma
• Major:
• VTE/PE, CVA—not widely publicized
• Ethinyl Estradiol (EE)
• More potent—remains most potent orally active EE
• Dosing adjustments, down
Mishell, Daniel. An Oral Contraceptive with 3 Approved Indications. The Journal of Reproductive Medicine. Volume 53., No. 9. (Supplement) September 2008.
2/26/2013
11
Combination Oral Contraceptives (COCs) o 1970’s
• Concerns for pill safety prompt Senate Hearings
• Doctors Case Against the Pill—Barbara Seaman
• VTE: dose dependent
• ↑ risk > 50μg
• FDA mandated: package insert/warnings
• After 1975: All formulations
• PG < 3mg; EE < 50 μg
• No decrease in efficacy
o 1988
• original high dose formulations
• removed from the market
American Experience. The Pill. Timeline. www.pbs.org/wgbh/amex/pill/timeline/timeline2.html
Combination Oral Contraceptives (COCs) o Current:
• Progestin: 0.5-1.5 mg (10 mg)
• EE: 10-35 μg (150 μg)
• 50 μg EE:
• Ovral, Ogestrel, Demulen 1/50
• Zovia 1/50E, Ovcon 1/50
• 50 μg Mestranol—limited availability
• Norinyl 1+50, Ortho Novum 1/50, Necon 1/50
o $ few dollars to $50+/pack/month
o Perfect use: 0.3%
o Typical use: 9%
Progestins
o 19-Nortestosterone derivatives—more closely resemble testosterone
• Greater androgenic activity
• 17α-acetoxyprogesterone derivatives
• Medroxyprogesterone acetate(Provera)/Megestrol Acetate(Megace)
• First Generation: (Estranes—1960’s)
• levonorgestrel, norgestimate(norelgestromin{patch}), norethistrone
• Second Generation: (Gonanes-1970’s)
• norethindrone , norethindrone acetate, ethynodiol diacetate
• Third Generation: (Estranes)
• gestodene, desogestrel {etonorgestrel (ring)} norgestimate
• Less androgenic
• Fourth Generation: Spironolactone derivative
• drosperinone
• Anti-androgenic, anti-mineralocorticoid effect
Gomes, Marcelo, P.V. Risk of Venous Thromboembolic Disease Associated with Hormonal Contraceptives and
Hormone Replacement Therapy, A Clinical Review. Arch Intern Med. 2004; 164 (18).
2/26/2013
12
COCs
o Mechanism of Action:
• Suppression:
• FSH/LH: Anterior Pituitary-gonadotropins
• Ovulation
• Progestin: inhibition of LH
• CVX—thickened mucous
• EM—atrophy
• Fallopian tubes—decreased
motility of cilia
• Folliculogenesis
• Estrogen: inhibition of FSH
• Level of EM—decreased BTB
• GnRH: Hypothalamus
Katz, etal. Comprehensive Gynecology, 5th Ed. 281-287. Mosby 2007
COCs
o Dosing: Cyclic • 21/7
• Arbitrarily chosen—1960s-2007
• Scheduled, monthly bleeding
• Assurance against pregnancy
• Higher dose formulations
• EE/PG-not cleared HFI—contd. LH/FSH suppression
• 24/4
• Decreased hormone dosing (20 EE)
• EE/PG cleared 2-3 days into HFI
• Absent EE: Permits ↑ FSH & potential follicular development
• Absent PG: Permits ↑ LH & ovulation if re-start is delayed
• Shorter HFI/pill free interval
• Greater inhibition of follicular development
• Decreased risk of ovulation & reduced menstrual side effects
• Yaz®, LoEstrin®, LoLoestrin®, Beyaz®
Mishell, Daniel. An Oral Contraceptive with 3 Approved Indications. The Journal of Reproductive Medicine. Volume 53., No. 9. (Supplement) September 2008. Katz, etal. Comprehensive Gynecology, 5th Ed. 281-287. Mosby 2007
COCs
o Dosing: Cyclic + Novel placebo substitutes
• LoEstrinFe® (Warner Chilcott)
• 24 days-20 μg EE/1mg NETA
• 4 days-ferrous fumarate
• GeneressFe® (Watson)
• 24 days-25 μg EE/0.8mg NETA
• 4 days-ferrous fumarate
• Beyaz® (Bayer)
• 24 days-20 μg EE/3mg Drsp/0.451mg levomefolate Ca++
• 4 days-0.451mg levomefolate Ca++
• Sayfral® (Bayer)
• 21 days-20 μg EE/3mg Drsp/0.451mg levomefolate Ca++
• 7 days-0.451mg levomefolate Ca++
2/26/2013
13
COCs
o Dosing: Cyclic + Novel placebo substitutes +
Lowest EE + shortest HFI
• Lo LoEstrinFe® (Warner Chilcott)
• FDA 2010
• 24 days-10 μg EE/1mg NETA
• 2 days-10 μg EE
• 2 days-ferrous fumarate
• Lowest dose of EE yet
• Thus expected decrease in EE related S&S
• Comparable efficacy to other low dose OCPs
• Similar side effect profile—similar BTB
22501 Loestrin Clinical PREA - Food and Drug Administration
www.fda.gov/.../DevelopmentApprovalProcess/.../UCM243787.pdf
COCs
o Dosing: Cyclic/Extended Cycle
• Quarterly
• Seasonale®(Duramed-2003)/Jolessa® (Barr Labs)
• 84 days-30 μg EE/0.15 mg LNG
• 7 days-placebo
• Quasense® (Watson)
• 84 days-30 μg EE/0.15 mg LNG
• 7 days-placebo
o Another variation to decrease:
• Ovulation
• # HFI
• Episodes of menstrual bleeding
• Menstrual related symptoms:
• dysmenorrhea, etc.
COCs
o Dosing: Continuous
o No HFI—low dose EE only
• Seasonique®(Duramed--2003)
• 84 days-30 μg EE/0.15 mg LNG
• 7 days-10 μg EE
• Minimal BTB; similar to Seasonale
• Avg. 3 days per 91 pill cycle
• LoSeasonique®(Duramed--2007)
• 84 days-20 μg EE/0.1 mg LNG
• 7 days-10 μg EE
• Avg. 2-3 days per 91 pill cycle
o Decrease EE withdrawal symptoms
• HA, dysmenorrhea/pelvic pain, PMS
• Trials are ongoing
o Quarterly menses expected
Extended-Cycle Oral Contraceptive Pills With 10 µg Ethinyl Estradiol ...
www.medscape.com/viewarticle/564690_6 LOSEASONIQUE dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?id=57764

2/26/2013
14
COCs
o No HFI/Continuous Dosing
• Lybrel®(Wyeth-2007)
• 28-pill pack
• 20 μg EE/0.09 mg LNG
• No scheduled HFI
• No expected routine menstrual bleeding
• Unscheduled bleeding:
• most often during the first seven pill packs
• decreases with subsequent pill packs
• 60% of women had bleeding/spotting during the 6th pill pack
• 48% by the 9th pill pack
• 41% during pill pack 13
• 18% stopped Lybrel® at least in part, due to unscheduled bleeding/spotting
LYBREL (levonorgestrel and ethinyl estradiol) - DailyMed dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?id=39528
COCs
o Novel Progestin:
o Dropsperinone (2007) 4th Generation
• 17 α-spironolactone derivative
• Anti-mineralocorticoid
• Anti-0androgenic
• Closely resembles natural progesterone
• Small increased risk:
• VTE
• Hyperkalemia
• Yasmin: 21/7 (Bayer)/Ocella-generic
• 21: 30 μg EE/3mg drosperinone
• 7: placebo
• Yaz: 24/4 (Bayer)
• 24: 20 μg EE/3mg drosperinone
• 4: placebo
Novel Estrogen:
o Natazia® (Bayer-2010)
• 1st quadriphasic COC
• 28 tablets:
• 2d-3 mg estradiol valerate (E2V)
• 5d-2 mg E2V and 2 mg dienogest
• 17d-2 mg E2V and 3 mg dienogest
• 2d-1 mg E2V
• 2d-placebo
• 2 day HFI:
• Decrease bleeding, menstrual symptoms compared to conventional COCs
• Decrease total steroid exposure compared to monophasic COCs
• Head to head studies comparing EE & E2V are currently lacking
2/26/2013
15
Side Effects: o EE:
• Nausea, breast tenderness, fluid retention, melasma
• Depression:
• more likely a result of PG than EE
• Less problematic with Low Dose COCs
• VTE-dose dependent • Due to EE effects on hepatic globulin synthesis
• Factor V, VIII, X, fibrinogen--VTE
• Hypertension • Activation RAA—increased hepatic Angiotensin production
• 1:200 women will develop clinical HTN
• Smokers > 35 years
• Increased risk arterial clots: MI/CVA
• Increased risk with # cigarettes/day (>10)
• CVA-ischemic/MI
• Overall low risk
• Dose dependent (EE); relatively small differences in risk according to progestin type • 0.9 to 1.7: 20 μg COC
• 1.3 to 2.3: 30 to 40 μg COC
Lidegaard Ø, Løkkegaard E, Jensen A et al. Thrombotic stroke and myocardial infarction with hormonal
contraception. N Engl J Med 2012; 366:2257-66.
Side Effects:
o EE:
• Slightly increased risk
• Cervical squamous cell and adenocarcinoma
• Uncertain mechanism, routine pap testing recommended
• Hepatocellular adenoma
• No longer clinically relevant
• Prolonged use and high dose pills—specifically mestranol
• Gallbladder disease—no longer supported with Low Dose COCs
• Lipid Profile—effects seen with high dose COCs
• EE: ↑ HDL, ↓ LDL, ↑ triglycerides & total Cholesterol
• PG: ↓ HDL, ↑ LDL, ↑ triglycerides
• Negligible change in lipid metabolism, uncertain clinical significance COCs
Katz, etal. Comprehensive Gynecology, 5th Ed. 281-287. Mosby 2007
Side Effects:
o EE:
• Breast Cancer:
• 1996—large international collaborative group re-analyzed
• worldwide epidemiologic data
• COCs and breast cancer
• 54 studies, 25 countries
• 53,000—women with breast cancer; 100,000 controls
• While taking COCs—small increased risk of breast cancer diagnosis
• RR: 1.24 [CI 1.15-1.30]
• This risk declined after cessation of therapy;
• back to baseline by 10 years post use
• NOTE: of Cancers diagnosed:
• less clinically advanced than in non-users
Collaborative Group on Hormonal Factors in Breast Cancer and hormonal contraceptives: Collaborative reanalysis of individual data on 53, 297
women with breast cancer and 100,239 women without breast cancer from 54 epidemiological studies. Lancet 347:1713, 1996
2/26/2013
16
Side Effects:
o PG:
• Depression:
• Newer studies suggest greater PG effect on mood vs. EE
• Data not conclusive
• Less problematic with current Low Dose COCs
• Weight gain:
• Felt to be due to the anabolic effects of PG
• Stimulation of appetite
• Acne:
• Via androgenic properties of PG
• May develop or worsen
• Amenorrhea:
• With COCs is the result of PG
• EM atrophy & ↓ regulation of EE receptors in EM by PG
Katz, etal. Comprehensive Gynecology, 5th Ed. 281-287. Mosby 2007
Benefits COCs
o Prevention of unintended pregnancy
o Decreased
• Epithelial ovarian cancer
• Suppression of ovulation
• Colon Cancer
• Endometrial cancer
• Functional ovarian cysts
• necessitating surgery/hospitalization
• Menstrual associated symptoms
• Acne
• PMS
• Dysmenorrhea
• Pelvic pain
• Menorrhagia
Katz, etal. Comprehensive Gynecology, 5th Ed. 281-287. Mosby 2007
Resources: o Medical eligibility
• WHO medical eligibility criteria (2009)
• www.WHO.INT/reproductivehealth/publications/family _planning/
• CDC (2010)
• www.cdc.gov/mmwr/pdf/rr/rr59e0528.pdf
2/26/2013
17
Ortho Evra Patch® (Janssen-2008)
o 4.5 x 4.5 cm adhesive patch
o 3 weeks active/1 week off
• Per patch:
• 6 mg-Norelgestromin/75 μg-EE
• Daily dose:
• 20 μg-EE/150 μg-Norelgestromin
o $ 3 patches(1 month)=just over 1 pack brand name COCs
www.orthoevra.com
Ortho Evra Patch®
o Typical use: 0.3-0.6%
o Perfect use: 0.8%
o ↓ efficacy: ↑ weight (<198lbs)
o VTE risk:
• 60% more EE exposure with patch vs 35 μg EE COC
• Results: multiple independent studies
• Range: approximate doubling of risk to no increase in risk
• ORTHO EVRA® compared to women using 35 μg EE COC
• FDA mandated warning
• Should not be used >35 years
www.orthoevra.com
Nuva Ring® (Merk)
o FDA: 2001/2002
o 5.4 cm flexible ring
• ethylene vinylacetate polymer
o $ equal to pack of pills
o Daily dose:
• 15 μg-EE/150 μg-Etonogestrel
• (desogestrel—3rd gen.)
• Steady state 35 days
o 3 weeks intra-vaginal /1 week out
• Off label: cont. dosing
www.nuvaring.com

2/26/2013
18
Nuva Ring®(Merk)
o Overall pregnancy rates
• First year users: 0.3%
• No typical use data
VTE risk:
o Studies 3rd generation CHC
• containing etonogestrel (3rd gen.)
• higher risk vs 2nd generation COCs
• approximate two-fold increased risk
• additional 1-2 VTE per 10,000 women-years of use
• Not all studies have revealed the same risk*
www.nuvaring.com
Progesterone only pills (POPs) • Thicken cervical mucous
• Decrease tubal motility
• Inhibition ovulation
• ~ 50% cycles
• Dosing compliance imperative
• Limitations:
• Dosing/compliance
• Benefits:
• No EE related SE
• HTN, CVD
• DM, Melasma
• Smokers > 35 years
• h/o VTE
• Lactation

2/26/2013
19
Progesterone only pills (POPs)
o Norethindrone 0.35mg
• Micronor®
• Nor-QD ®
• Camilla ®
• Errin ®
• Jolivette ®
• Nora-Be ®
o Perfect use: 0.3%
o Typical use: 8%
Progesterone only pills (POPs)
o “Progestogen only” products:
• conferred no increased risk of CVA-ischemic or MI
• whether taken as:
• low dose norethisterone pills
• desogestrel only pills
• Not available in the US
• or in the form of hormone releasing “implants” or
“intrauterine devices”
• Risks were conferred by estrogen—COCs
Lidegaard Ø, Løkkegaard E, Jensen A et al. Thrombotic stroke and myocardial infarction with hormonal contraception. N Engl J Med 2012; 366:2257-66.
Progestins
o VTE risk:
• <1995: PG role VTE uncertain
• More recent studies:
• Small but increased risk
• 2nd vs 3rd generation COCs
• 2nd: levonorgestrel, norgestrel, norethistrone
• 3rd: gestodene, desogestrel, norgestimate
• 4th: drosperinone
• Baseline COC use: Low risk VTE: 1:10,000 woman years
• Doubled risk: remains small 2:10,000 woman years
Gomes, Marcelo, P.V. Risk of Venous Thromboembolic Disease Associated with Hormonal Contraceptives
and Hormone Replacement Therapy, A Clinical Review. Arch Intern Med. 2004; 164 (18).
2/26/2013
20
Progesterone only pills/DMPA/LNG/ETG Implant/LNG IUS
o History of DVT 2
o Acute DVT/PE 3
o DVT/PE established anticoagulation
2
o First degree relatives with VTE/PE
2
o Major surgery
• Prolonged immobilization 1
• Minimal immobilization 1
WHO Medical Eligibility Criteria, Fourth Edition. 2009
Depot Medroxyprogesterone Acetate (DMPA)
o Depot Provera®
o (Pfizer—1992)
o Standard
• 150 mg=1cc
• IM deltoid/gluteus maximus
• 13 weeks
o Typical use: 0.3-0.6%
o Perfect use: 0.8%
Depot Medroxyprogesterone Acetate (DMPA-SQ)
o (Pfizer—2004)
• Depot Provera-subQ®
• Developed to replace office visit, with home SQ self administration
o Subcutaneous
• 104 mg=0.65cc
• SQ anterior thigh/abdomen
• 14 weeks
o Typical use: 0.3-0.6%
o Perfect use: 0.8%
2/26/2013
21
Depot Medroxyprogesterone Acetate (DMPA)
o FDA “black box” warning 2004
o A meta-analysis of 12 studies involving
• 1,039 DMPA users (IM formulation) and 2,086 controls
• Average Z-score--DMPA users
• decreased <1 SD vs nonusers
• BMD reductions stabilized
• after 3 to 4 years of use
• Bone loss reversed with discontinuation
• similar to those in women having never used DMPA
• Loss is comparable to that seen with lactation
o ACOG/AAP: no limit on duration of use
o Adolescents/Menopause
• Benefit/risk unintended pregnancy
• Ca++/Weight bearing exercise most days/week
Tang OS, etal. Further evaluation on long-term depot-medroxyprogesterone acetate use and bone mineral density. Contraception.2000; 62: 161-164.
Norplant® (Wyeth—1990)
o 6 rod implant—LNG—5 years
o Predecessor to
• Implanon® (Merk 2001)
• Nexplanon® (Merk 2011)
• Removed from the market 2000
• Multiple consumer suits
• No warning about side effects:
• Irregular menses, headaches, nausea, depression
• No suits were lost
Norplant II/Jadelle® (Wyeth—1996)
o 2 rod implant system—LNG—3 years
o 2000-concerns for lot efficacy
o Removed from US markets
• Remains in use Internationally
Subcommittee for Workshop on Implant Contraceptives, Committee on Contraceptive Research and Development, Division
of Health Policy, Institute of Medicine (March 9, 1998). "Appendix B: Norplant: historical background". In Harrison, Polly F.;
Rosenfield, A.
Implanon® (Merk—2001) o $595/$262
o 4 cm x 2 mm
o Ethylene vinyl acetate
o 68mg Etonogestrel implant • 60 μg/day
• 25-30 μg/day (end 3rd year)
o No pregnancies in earliest studies
Nexplanon® (Merk—2011) o Modified device introducer
o Greater ease of provider placement
o Typical use: 0.5%
o Perfect use: 0.5%
2/26/2013
22
Intrauterine Device (IUD):
o 1960’s: manufactured & released USA
o 1975: Dalkon Shield® (Dalkon Corp.)
• Recalled:
• Infertility/sterility
• thousands of users
• Braided string
• Increased upper genital tract infections
• Resultant PID & infertility
o All IUDs removed from the market
• Litigation fear
Intrauterine System (IUS)
o ParaGard® T380A (Teva—1984)
• $475
• T-shape
• Polyethylene arms/radiopaque
• Copper wire wrapped stem
• Surface area copper=380mm²
• Duration: 10 years
o Typical use: 0.6%
o Perfect use: 0.8%
o 10 year cumulative failure rates: 2.1-2.8%

2/26/2013
23
Intrauterine System (IUS)
o Mirena® (Berlex Labs—2000)
• $843
• 3.2 cm x 3.2 cm silastic T
• 52mg LNG
• 20 μg/day
• 14 μg/day (after 5 years)
• Duration: 5 years
• Added benefits:
• decreased menstrual bleeding, dysmenorrhea
• amenorrhea
o Typical use: 0.1%
o Perfect use: 0.1%
o 5 year cumulative failure rate : 0.7%
Bilateral Tubal Ligation (BTL)
o Total annual cases of tubal sterilization
• 1995: 687,000
• 2006: 643,000
• despite 4% population increase
• Interval sterilizations
• decreased 12%
• Post partum sterilizations
• stable; following 8%-9% live births
• more common
• Black and Latino
• lower income, lower education, higher parity
• Southern geography
Chan LM, etal. Tubal Sterilization Trends in the United States. Fertil Steril. 2010 Jun; 94(1): 1-6.

2/26/2013
24
Bilateral Tubal Ligation (BTL) Cumulative 10 yr. failure rates
o Post-partum/Cesarean delivery
• Modified Pomeroy 0.8%
• Modified Parkland 0.8%
o Laparoscopy
• Modified Pomeroy 0.8%
• Filshie Clip® 0.9%
• Fallope Ring® (silastic band) 1.8%
• Bipolar cautery 2.5%
• Fistula formation→ectopic pregnancy
Hysteroscopic Tubal Occlusion
o Essure®(Conceptus—2009)
• $950 (device)
• Essure® flexpay plan
• Nickel Coil
• Polyesther fibers (PET)
• 99.8% effective; 99.7% at 5 years
• Tubal occlusion after 3 months
• Verification with HSG
• OR vs Office
Hysteroscopic Tubal Occlusion
o Essure®(Conceptus—2009)
• Combined data from the phase II and pivotal trials
• NO pregnancies in 643 study participants
• 29,357 women-months of follow-up
• Average surveillance time of 42.5 months
• No pregnancies have been reported following documented bilateral tubal
occlusion in these trials
• Kerin, etal. analyzed 37 reported pregnancies, worldwide, 1997-2004
• 6 (16%): were pregnant prior to device placement
• 7 (19%): misinterpreted HSGs
• 21 (57%): inadequate post-procedure follow-up
Kerin JF, Cooper JM, Price T, et al. Hysteroscopic sterilization using a micro-insert device: results of a multicentre phase II study. Hum Reprod.
2003;18:1223–1230.
Kerin JF. Pregnancies in women who have the Essure hysteroscopic sterilization procedure: a summary of 37 cases. J Minim Invasive Gynecol.
2005;12(suppl):28. Abstract 67.

2/26/2013
25
Hysteroscopic Tubal Occlusion
o Essure® (Conceptus—2009)
o August 1st, 2012:
• U.S. Department of Health and Human Services
• FDA approved birth control
• including permanent birth control procedures--Essure®
• must be provided by insurance companies
• without cost to patients
• Co-pay, co-insurance, deductible
US DHHS. A statement by U.S. Department of Health and Human Services Secretary Kathleen Sebelius. New Release. Jan 2012.
Hysteroscopic Tubal Occlusion
o Adiana® (Hologic—2009)
• Increase office application
• Hysteroscopic
• Tubes cannulated
• Low level radiofrequency energy
• Insertion polymer matrix
• Previously treated area
• Tubal occlusion after 3 months
• Verification with HSG
• OR vs Office
• 3 year cumulative failure rates: 1.6%
James B. Presthus. Bridging the Use of Adiana Permanent Contraception from Clinical Trials to Community Practice. OBG Management. Supplement. 2011 Jan; S1.

2/26/2013
26
Progesterone only
o Plan B®
o Next Choice®
Yupze method
o COCs
Copper IUS
o Paragard®
Urlipristal
o Ella®
Yuzpe
o 1997—FDA off label use approval
o 2 high doses COC (Alesse, Ovral, Levlen, LoOvral, Triphasil, Trilevlen)
• > 100 μg EE
• 100 μg Norgestrel
• 50 μg Levonorgestrel
• Norethindrone=slightly less effective
• Within 120 hours unprotected coitus/method failure
• 2nd dose 12 hours later
• Pregnancies/100 women:
• Early: (<12 h) 0.5%
• Late: 24-72 h) 4.2%
• Avg: 2-3.2%
Zieman, Mimi, etal. Managing Contraception. Sept 2011; 74-79.
Copper IUS (ParaGard®)
o ParaGard T380A®(Teva)
o Up to 5 days post intercourse
• Up to 8 days post ovulation
o Pregnancies/100 women: 0.1%
o Good long term, reversible contraceptive option
2/26/2013
27
Levonorgestrel Only
o Plan B® (Teva—2006), Next Choice®(Watson—2009)
• OTC > 18 years
• 2 doses (0.75mg LNG ) 12 hours apart
• $35-60
• Delayed ovulation via high dose PG
• Pregnancy reduction 89%
• within 72 hours
• Effective up to 120 hours
• More effective/less side effects than combination Yuzpe
o Levonorgestrel
• Generic Plan B—Rite Aid
FDA/CDERm, 2006a; Duramed Pharmaceuticals, 2006.
Levonorgestrel Only
o Plan B One-Step®(Teva—2009)
o Next Choice One-Dose ®(Watson—2012)
• OTC > 17 years with ID
• 1 dose (1.5mg LNG )
• $35-60
• Pregnancies/100 women:
• Early: (<12 h) 0.4%
• Late: (24-72 h) 2.7%
• Avg: 1.1%
Zieman, Mimi, etal. Managing Contraception. Sept 2011; 74-79.
Ulipristal o Ella®(Watson—2010)
• Progesterone agonist/antagonist
• Preventing ovulation
• Rx only
• 2 Trials: Phase III
• USA >18 years: 2.10% (study) vs 5.53% (expected)
• USA/Europe >16 years : 1.78% (study) vs 5.54% (expected)
• $40-60
• 30mg Ulipristal ASAP post contraceptive failure
• Effective 120 hours/5 days
• Less effective: BMI >30 kg/m²
• More effective compared to LNG EC over full 120 hours
Glasier, Anna F. et al. "Ulipristal Acetate versus levonorgestrel for emergency contraception: a
randomized non-inferiority trial and meta-analysis". The Lancet, 365, 555-562. (2010).

2/26/2013
28
Pregnancy evaluation
o If: menses has not resumed 21 days after EC
Progesterone only EC available OTC regardless of age:
o Alaska, California, Hawaii
o Maine, New Hampshire, New Mexico
o Vermont Washington State
Emergency Contraception: US states with pharmacies that provide LNG EC regardless of age. ec.princeton.edu. 2012

2/26/2013
29
Latex Female Condom
o (Current—nitrile, improvement over polyurethane)
o Single use latex barrier
o Less expensive
• Improved access for developing countries
o Thinner, more natural feel
o Phase III trials in progress (WHO)
SILCS Diaphragm
o Novel single-size barrier device
o Reusable
o Fit most women comfortably
o Phase III contraceptive trial
• SILCS diaphragm with Buffer Gel® or Nonoxynol-9
• Enrolled 450 couples at six U.S. sites
• Study completed; data analysis is underway
Conrad Progress Report 2008-2010
2/26/2013
30
Testosterone undecanoate+Norethistrone enanthate
o (TU/NET-EN )
o Male hormonal contraceptive
o Phase IIb trial
• WHO & CONRAD collaboration
• Organization (WHO) to determine the safety and efficacy of a long-acting
o Combination:
• testosterone (testosterone undecanoate [TU])
• long-acting progestin (norethisterone enanthate [NET-EN])
• sperm suppression
o Injection: 2 months
o Ten sites/seven countries
o 2008 enrolling participants in 2008
o Results for contraceptive efficacy are expected in 2013
Conrad Progress Report 2008-2010
Cyclofem®
o Female injectable hormonal contraceptive
o Highly effective combined monthly injectable
• medroxyprogesterone acetate (MPA) 25 mg
• estradiol cypionate (E2C) 5mg
• long-acting ester of estradiol
• developed for effective reversible contraception
• Studied/used extensively throughout the world
• Not currently FDA approved
• Approval process underway
• Lunelle: former name
• FDA approved 2000
• marketed and distributed in U.S.
• Removed from the market due to production issues
Conrad Progress Report 2008-2010
Cyclofem®
o Investigators at Eastern Virginia Medical School:
• Ongoing clinical trial
o Trial objectives
• assess the pharmacokinetic parameters:
• medroxyprogesterone acetate
• estradiol cypionate
• during the third month of use and for two months post-use
• compare to historical data of Lunelle in U.S. women
• Endpoints:
• MPA and E2C levels
• Return of ovulation after cessation
o Enrollment is ongoing
Conrad Progress Report 2008-2010

2/26/2013
31
Antares Pharma and the Population Council
o International, nonprofit research organization
o Combination: Low dose Transdermal
• Progestin: Nestorone®
• Estrogen: 17β-estradiol (E2)
• Potential for superior safety profiles compared to other common preps
o Gel formulation
• Metered-dose pump
• Rapid absorption, no residue
• slow steady passage from skin into the systemic circulation
• Once-daily application
• upper arms, shoulders, abdomen or internal parts of the thighs
• Unscented, clear
• Key benefit of ATD™ gels: excellent local skin tolerance
• Over patches/adhesives
Antares Pharma and the Population Council
o Nestorone®
• No oral activity
• Absorbed well trans-dermally
• Highly effective at ovulation suppression at low dosing
• No androgenic activity
• (e.g. acne, weight gain, and altered cholesterol levels)
• Particularly applicable for breastfeeding
o Estradiol
• much less potent estrogen via transdermal application
• potentially lower VTE risk, better side effect profile
2/26/2013
32
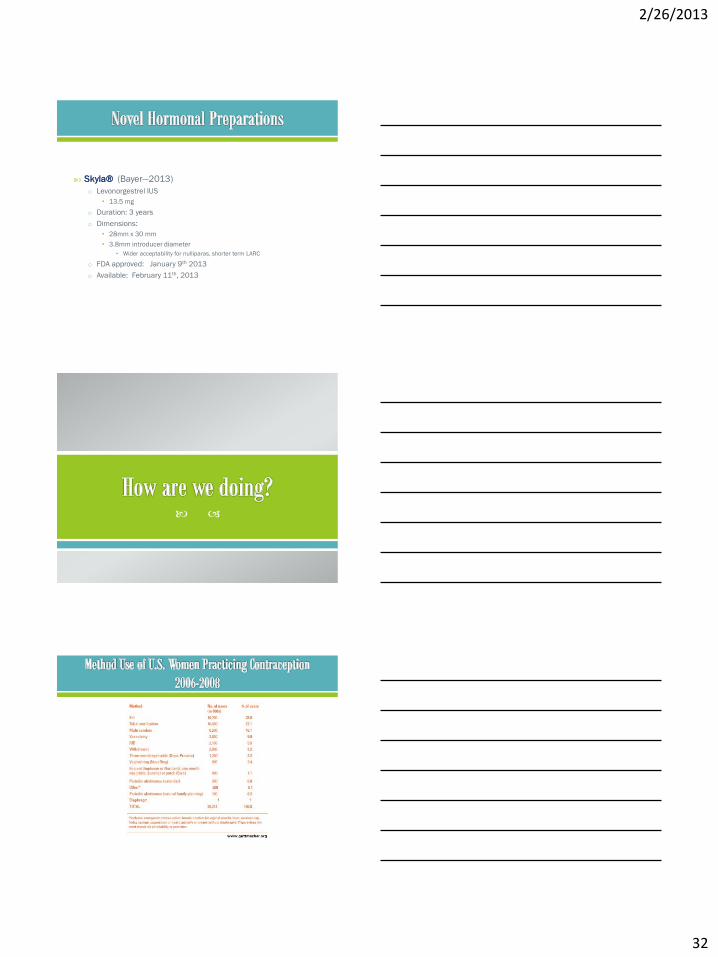
Skyla® (Bayer—2013)
o Levonorgestrel IUS
• 13.5 mg
o Duration: 3 years
o Dimensions:
• 28mm x 30 mm
• 3.8mm introducer diameter
• Wider acceptability for nulliparas, shorter term LARC
o FDA approved: January 9th 2013
o Available: February 11th, 2013

2/26/2013
33
o No improvement past 20 years
• 1994-2001: 49.2% to 48%
• 2006: 49%
o Unintended pregnancy rate:
• 2001: 50 per 1000 women aged 15-44 years
• 2006: 52 per 1000 women aged 15-44 years
• Notable decline: teens (15-17 years)
o Unintended pregnancies ending in abortion
• 2001: 47%
• 2006: 43%
Finer, LB and Zolna, MR. Unintended pregnancy in the United States: incidence and disparities, 2006, Contraception, 2011, 84(5):478–485
Educate
o Benefits of family planning, scheduled pregnancy
o Dosage/administration
o Side effects
o Newest products
Follow up
o Ensure compliance/tolerability
o Evaluate for unacceptable side effects
o Change method
Maximize protection/coverage
o Recommend EC

2/26/2013
34