Embed Size (px)
Citation preview
Power Doppler Imaging in PreoperativePlanning and Postoperative Monitoring ofMuscle Flaps
Nyu-nyu Loh, MD,1 Ian Y. Ch’en, MD,1 Eric Olcott, MD,1,2 R. Brooke Jeffrey, Jr., MD,1
Kenneth C. Hui, MD,3 Barbara Persons, MD,3 William C. Lineaweaver, MD3
1 Department of Radiology, Stanford University Medical Center, 300 Pasteur Drive, Stanford, California 943052 Veterans Affairs, Palo Alto Health Care System, 301 Miranda Avenue, Palo Alto, California 943043 Division of Plastic Surgery, Stanford University Medical Center, 300 Pasteur Drive, Stanford, California 94305
Received 15 November 1996; accepted 4 June 1997
ABSTRACT: Purpose. We assessed the utility of powerDoppler imaging (PDI) in preoperative planning andpostoperative evaluation of microvascular tissuetransfers.
Methods. Twenty-five PDI studies were performedon 23 patients using a 5–10-MHz linear-array trans-ducer. Thirteen patients were assessed preoperativelyfor patency of the desired donor vessel; 8 of them hadsurgical scars overlying the desired vascular territory.Twelve patients (including 2 from the first group) wereevaluated postoperatively for patency of the vascularanastomoses and adequacy of the blood supply to thetransferred tissue.
Results. Twelve of the 13 patients assessed preop-eratively had successful flap transfers. Four of the 8patients with scars over the desired vascular territo-ries had absent or aberrant arteries, necessitating achange in the operative plan. None of these patientshad operative complications. Eight of the 12 patientsscanned postoperatively had patent anastomoses. In2 of these patients, impending surgery was avertedwhen the adequacy of the tissue blood supply wasestablished with PDI. In 4 patients, PDI showed arterialor venous compromise, which was confirmed at sur-gery.
Conclusions. PDI is a useful technique in microsur-gical tissue transfer for assessing the patency of de-sired donor vessels preoperatively and for postopera-tive evaluation of blood supply. © 1997 John Wiley &Sons, Inc. J Clin Ultrasound 25:465–471, 1997.
Keywords: power Doppler imaging; muscle flap trans-fer
The failure rates for microsurgical reconstruc-tions (microvascular tissue transfers) report-
edly range from 5% to 10% in experienced cen-ters.1–3 Because flap losses are almost entirelyattributable to vascular compromise, a reliablemethod of detecting tissue vascularity and perfu-sion that can be used for surgical planning andpostoperative monitoring is desirable. Vessels inthe planned flap pedicle and derivative perforat-ing vessels can be absent or aberrant because ofanatomic variations or surgical or traumatic dis-ruption.4–6 Such vascular abnormalities, if unde-tected preoperatively, can lead to intraoperativeabandonment of the procedure. Postoperatively,the value of early detection of blood supply prob-lems can be substantial since early correctivemeasures can achieve flap salvage rates of 70–100%.7,8
Current methods for postoperative monitoringof flaps all have significant limitations. Directclinical observation can be misleading or impos-sible (eg, ‘‘buried’’ flaps preclude direct visualiza-tion), and techniques such as electromagneticflowmetry, thermocouple probes, and transcuta-neous oxygen monitoring are complex and/or in-vasive.9 While spectral waveform analysis andconventional color Doppler imaging (CDI) afforddirect assessment of flap vascularity and mayprovide information about blood flow directionand velocity, their major drawback is that theirsensitivity for the detection of flow varies with themean Doppler frequency shift and is Dopplerangle dependent. Consequently, CDI may not ac-
Correspondence to: R.B. Jeffrey, Jr.
© 1997 John Wiley & Sons, Inc. CCC 0091-2751/97/090465-07
465VOL. 25, NO. 9, NOVEMBER/DECEMBER 1997

curately assess tissue blood supply despite effortsto maximize Doppler flow sensitivity settings.
Power Doppler imaging (PDI) is a promisingcolor Doppler technique that maximizes flow sen-sitivity because it color-encodes the entire inte-grated power of the Doppler signal rather thanjust the mean Doppler frequency shift.10 PDI’sability to detect tissue vascularity is thus less de-pendent on the Doppler angle, which results inincreased sensitivity to low-volume flow. PDI issuperior to CDI in depicting low-volume flow11
and adds diagnostic confidence when used as anadjunct to duplex scanning in renal and gastroin-testinal flow-related conditions (eg, pyelonephri-tis and bowel ischemia).12,13 A single report ofPDI studies of reimplanted digits and flap recipi-ent site vessels has indicated the potential utilityof this technique in acute and elective microsur-gical tissue transfer.14 The aim of the present pro-spective study was to assess the utility of PDI inpreoperative patient selection and planning andpostoperative monitoring of microsurgical tissueflaps.
PATIENTS AND METHODS
Patients
Twenty-five PDI studies were performed on 23patients (12 women and 11 men; mean age, 51years) referred from the plastic and reconstruc-tive surgery service from September 1, 1995, toMarch 5, 1996. All 23 patients underwent chestwall, head or neck, or extremity reconstructivesurgery using rectus abdominis muscle flaps (20patients), a free radial forearm flap (1 patient), apectoralis major flap (1 patient), or a free flapfrom the thigh (1 patient). There were 2 groups ofpatients: group 1 consisted of 13 patients who un-derwent PDI as an integral part of their preop-erative workup (Figure 1), and group 2 consistedof 12 patients who had PDI for postoperative flapevaluation (Figures 2 and 3). Two patients hadboth pre- and postoperative evaluation by PDI.
The preoperative PDI examinations were per-formed mainly to identify the deep inferior epi-gastric artery (DIEA) and/or the deep superiorepigastric artery (DSEA) and to verify the bloodsupply to the rectus abdominis muscle. Eight pa-tients had surgical scars overlying the vascularterritory of the donor or recipient site from previ-ous surgery to the chest wall (eg, cardiac bypasssurgery) or abdomen/pelvis (eg, cesarean section,hysterectomy, herniorrhaphy, or trauma). PDIwas used to identify aberrant or absent arteries inthese patients. PDI was performed postopera-
tively because of clinical concerns about vascularpatency. Two of the 12 patients studied postop-eratively had serial PDI examinations. All post-operative studies were performed using a por-table scanner in the intensive care unit within 6days of surgery.
Technique
All PDI studies were performed with a commer-cially available scanner equipped with a 5–10-MHz linear-array transducer (Acuson XP, Moun-tain View, CA; or ATL HDI 300, Bothell, WA).Specific PDI parameters (scale and dB settings)were optimized for low-volume flow. The powerDoppler gain was adjusted to be just below noiselevels to maximize flow sensitivity.15 The colorbox was kept as small as possible to minimizeflash artifacts. Spectral Doppler waveform trac-ings were routinely obtained to confirm arterial orvenous flow. Resistance indices, however, werenot calculated.
Preoperatively, the native DIEA can be readilyvisualized with PDI on transverse scans 3–4 cmfrom the midline approximately midway betweenthe umbilicus and symphysis pubis. Longitudinalscans can trace this vessel from its external iliacartery origin (near the inguinal crease) into thebelly of the rectus abdominis muscle to approxi-mately 2 cm above the level of the umbilicus.Small, tortuous perforating vessels arborize withvessels from the DSEA in the rectus abdominismuscle. The DSEA, the terminal branch of theinternal thoracic (mammary) artery, is identifiedcoursing caudally in the xiphoid/sternal areaalong the inferior costal margin.
Postoperative evaluations are expedited whenthe sites of surgical anastomosis are known to thesonologist. Our studies were guided by sketchesor markers placed over the anastomotic site or bythe surgeon’s being present during imaging. Us-ing PDI, the areas of the venous and arterialanastomoses were interrogated, and the vascular-ity of the muscle flap was assessed. Abnormalfluid collections were identified, and their rela-tionship to surrounding vessels was determined.Vessels in the flap were assessed for patency andfor expected course. Spectral Doppler waveformsconfirmed arterial or venous flow. If no flow wasdetected in a vessel, with or without the presenceof a visible clot, the vessel was determined to beoccluded. If the course of the vessel deviated fromexpected arterial anatomy (as delineated above),the vessel was designated as aberrant, suggestiveof collateral formation. Vessel size was measuredfrom both gray-scale and PDI images. However,
LOH ET AL
466 JOURNAL OF CLINICAL ULTRASOUND
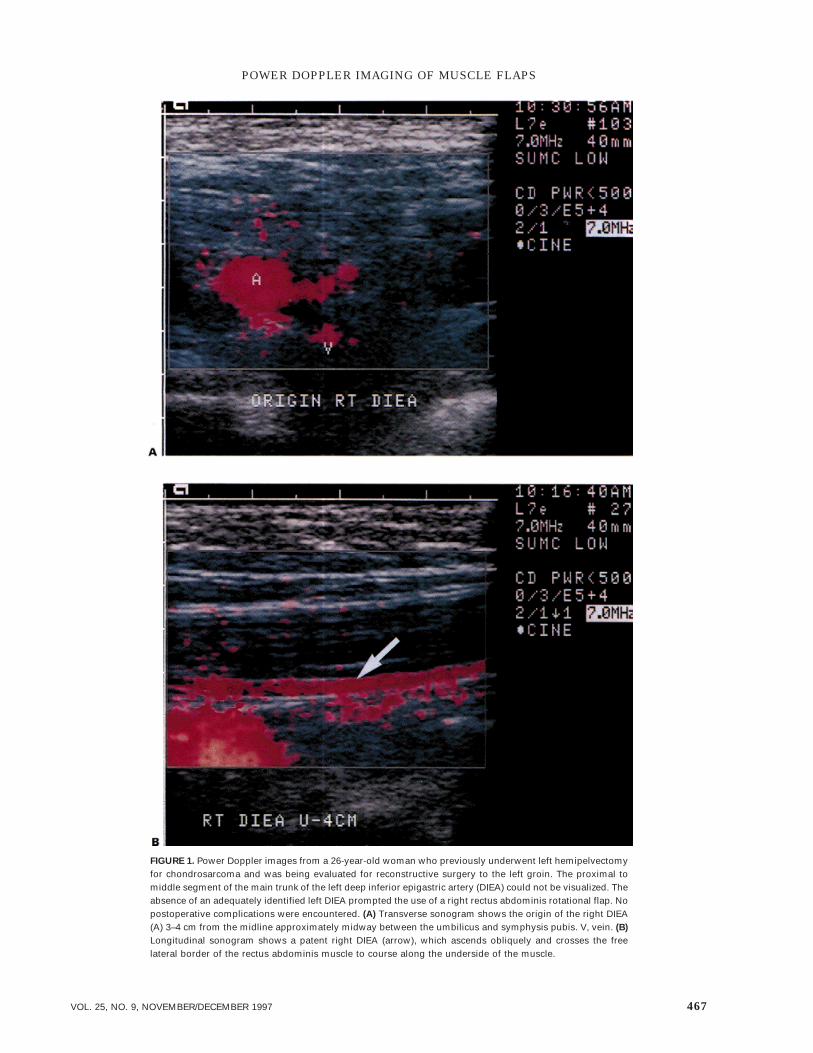
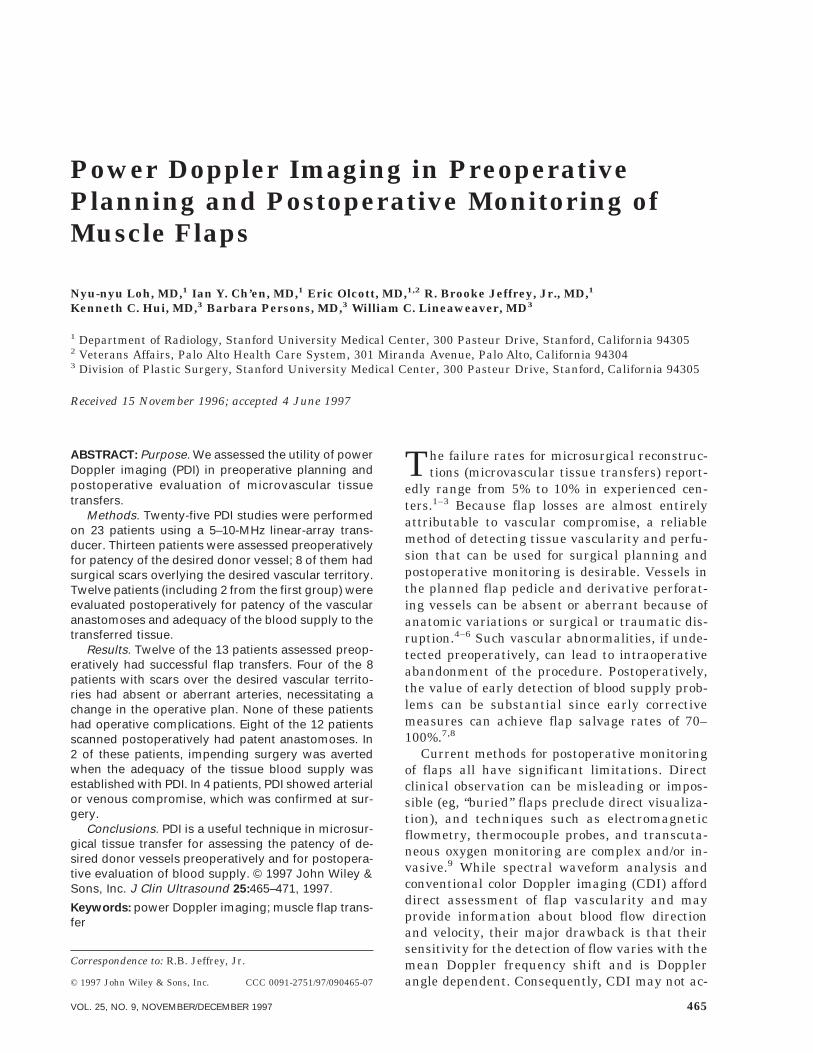
FIGURE 1. Power Doppler images from a 26-year-old woman who previously underwent left hemipelvectomyfor chondrosarcoma and was being evaluated for reconstructive surgery to the left groin. The proximal tomiddle segment of the main trunk of the left deep inferior epigastric artery (DIEA) could not be visualized. Theabsence of an adequately identified left DIEA prompted the use of a right rectus abdominis rotational flap. Nopostoperative complications were encountered. (A) Transverse sonogram shows the origin of the right DIEA(A) 3–4 cm from the midline approximately midway between the umbilicus and symphysis pubis. V, vein. (B)
Longitudinal sonogram shows a patent right DIEA (arrow), which ascends obliquely and crosses the freelateral border of the rectus abdominis muscle to course along the underside of the muscle.
POWER DOPPLER IMAGING OF MUSCLE FLAPS
467VOL. 25, NO. 9, NOVEMBER/DECEMBER 1997

the ‘‘blooming’’ effect of PDI may result in over-estimation of vessel size, so vascular patency wasdetermined solely on the basis of the presence orabsence of flow and confirmation with spectralDoppler waveforms.
RESULTS
Nine of 13 preoperative studies showed patentDIEAs or DSEAs based on the presence of bloodflow. The main vascular trunk ranged in diameterfrom 1.3 to 3.6 mm. Four examinations revealedabsent or aberrant arteries and led to alterationsin the surgical approach: 2 patients had left DIEAcompromise [1 who had had left inguinal nodaldissection for vulvar cancer and 1 who had hadwound dehiscence following left hemipelvectomyfor chondrosarcoma (Figure 1)] and required rightDIEA rectus abdominis flaps for left inguinal re-construction, and 2 patients with chronic sternalwound infections following previous surgerieslacked DSEAs and received a pectoralis majorflap or a free flap from the thigh rather than arectus abdominis flap. The other 4 patients withsurgical scars over the thoracoabdominal wallhad normal arterial vasculature. Twelve of the 13patients scanned preoperatively had successfulflap transfers, with flap survival confirmed clini-cally. In the 1 case of flap failure, a large inter-costal vessel was mistaken for a patent DSEA onPDI, the DSEA was found intraoperatively to be
occluded, and attempted flap rotation based onthe intercostal vessels failed.
Postoperative PDI showed patent vascularanastomoses and the presence of arterial and ve-nous flow in 8 of 12 patients. In 2 of these cases,impending surgical exploration for clinical suspi-cion of vascular compromise was averted. In 4 pa-tients, problems with flap viability were con-firmed with PDI (Figure 2), which directlyprompted open exploration. Two of these patientsdid not demonstrate intrinsic flap vascularity andwere surgically confirmed to have arterial occlu-sion. The other 2 patients showed either absentflap venous flow (due to venous compression) orflow seen only during augmentation in associa-tion with adjacent fluid collections suggestive ofhematoma (surgically confirmed) (Figure 3). In allof these cases, findings on PDI prompted earlyflap revision, which resulted in a 50% flap salvagerate. The 2 failed cases were 1 arterial and 1 ve-nous thrombosis, also confirmed at surgery.
DISCUSSION
PDI has proven to be a useful adjunct to CDI fora variety of clinical applications.15 Because it isbased on the properties of the total integratedDoppler power spectrum rather than the meanDoppler frequency shift (as in conventional CDI),PDI affords higher sensitivity in low flow statesand vessels that are tortuous or perpendicular tothe axis of the ultrasound beam.
FIGURE 2. Power Doppler image from a 73-year-old woman who underwent reconstruction with a right rectusabdominis pedicled flap and split-thickness skin graft to repair a left chest wall defect secondary to localabscess. On postoperative day 5, the patient’s rectus flap became dusky, and power Doppler examinationrevealed absence of perfusion in the lateral portion of the flap, as shown here. This finding was confirmedsurgically. The flap was salvaged after revascularization.
LOH ET AL
468 JOURNAL OF CLINICAL ULTRASOUND
In our study, PDI was effective in delineatingblood flow in small vessels and assessing flapblood supply. Preoperative verification of pro-posed donor vessels such as the DIEA or DSEAcan directly alter clinical management: 4 (31%) of13 patients in this pilot series required an alter-native surgical approach when the absence of the
main donor vessel was determined using PDI.PDI is particularly useful in confirming vessel pa-tency in patients who have had previous surgicalincisions or trauma in the vicinity of the proposeddonor site and is often helpful in selecting an al-ternative donor site. In this study, 12 (92%) of the13 patients evaluated preoperatively had success-
FIGURE 3. Power Doppler images from a 26-year-old man who underwent free radial forearm flap reconstruc-tion of the palate to correct an oronasal fistula and experienced increasing swelling of the left neck. (A)
Transverse scan shows a large, complex mass representing a hematoma (arrow) adjacent to the graft anas-tomosis. The flap survived after surgical drainage of the hematoma. A, patent artery; V, vein. (B) Longitudinalscan shows flow in a dilated vein graft (arrow). Dilatation of the vein was believed to be due to compressionby the hematoma.
POWER DOPPLER IMAGING OF MUSCLE FLAPS
469VOL. 25, NO. 9, NOVEMBER/DECEMBER 1997

ful flap transfers. The single failure was in a pa-tient who required a rotational muscle flap forchronic sternal infection after previous coronaryartery bypass surgery. PDI identified a 1.7-mm-diameter vessel with arterial flow in the rightparasternal area that was believed to be the rightDSEA. During surgery, however, it was discov-ered that the right DSEA had been surgically li-gated at the time of the coronary artery bypassand that the sonographic finding corresponded toa well-developed arterial collateral (superolateralmarginal artery). The rotational muscle flapbased on this vessel subsequently failed. Thus,meticulous scanning techniques should be fol-lowed in demonstrating the origin of the vessel ofinterest in order to avoid confusion with othervessels in the area, especially in patients withprevious surgery and resultant distortion of theregional vascular anatomy. Actual mapping of do-nor vessels with planning of flaps to include thelargest perforators can also be performed withPDI, as has been done with CDI.9
PDI has the potential to improve postoperativeflap monitoring. For this study, only patients inwhom tissue viability was a concern based on theclinical scenario were evaluated by sonography.While conventional CDI can accurately detectflow in larger vessels, PDI could demonstrate flaptissue vascularity, in addition to the patency ofanastomosed vessels, and provide enough reas-surance to the surgeons to opt for conservativemanagement. Impending surgery was avoided in2 patients who did not have major vascular com-promise based on PDI findings. Furthermore,early diagnosis of vascular compromise helped tosalvage 2 of 4 thrombosed flaps. Postoperativeevaluation and monitoring of buried flaps, inwhich direct visualization of tissue color and vas-cularity is not possible, may be another potentialapplication of PDI, in conjunction with CDI.
A limitation of this study is the small patientpopulation, which was a result of the patient se-lection process, ie, including only patients withpotential problems (such as ligated donor vesselsor occluded vessels postoperatively). Another pos-sible limitation is that patients found by PDI tohave absent or abnormal vasculature in the ter-ritory of the initially desired donor site did notundergo angiographic or surgical confirmation ofthe ultrasound findings. Postoperatively, patientswho were clinically stable were not referred forsonographic evaluation. Furthermore, interroga-tion by ultrasound was not performed until obvi-ous clinical signs were present, which may ac-count for the 50% salvage rate.
This pilot study suggests that PDI is useful in
evaluating tissue vasculature both before and af-ter microsurgical transfer. Further study isneeded to determine the efficacy of this techniquein comparison with established methods for pre-operative planning and postoperative monitoringof microsurgical reconstructions.
REFERENCES
1. Jones NF: Postoperative monitoring of microsurgi-cal free tissue transfers for head and neck recon-struction. Microsurgery 1988;9:159.
2. Gross JE, Friedman JD: Soft tissue reconstruction.Monitoring. Orthop Clin North Am 1993;24:531.
3. Lineaweaver W, Hui KCW, Heutz UR, et al: Theevolution of the role of microsurgical flap proce-dures in the medical center. In Proceedings of the12th Symposium of the International Society of Re-constructive Microsurgery. Singapore, Interna-tional Society of Reconstructive Microsurgery,1996, p. 177.
4. Whitney TM, Lineaweaver WC, Billys JB, et al:Improved salvage of complicated microvasculartransplants monitored with quantitative fluorom-etry. Plast Reconstr Surg 1992;90:105.
5. Neligan PC: Monitoring techniques for the detec-tion of flow failure in the postoperative period. Mi-crosurgery 1993;14:162.
6. Rand RP, Cramer MM, Strandness DJ: Color-flowduplex scanning in the preoperative assessment ofTRAM flap perforators: a report of 32 consecutivepatients. Plast Reconstr Surg 1994;93:453.
7. Hallock GG, Brown CL, DeSantis MJ: Preoperativeidentification of perforating vessels to the skin bycolor duplex imaging. J Ultrasound Med 1995;14:263.
8. Canales FL, Furnas H, Glafkides M, et al: Micro-surgical transfer of the rectus abdominis muscleusing the superior epigastric vessels. Ann PlastSurg 1990;24:534.
9. Rubin JM, Bude RO, Carson PL, et al: Power Dopp-ler US: a potentially useful alternative to meanfrequency-based color Doppler US. Radiology 1994;190:853.
10. Dacher JN, Pfister C, Monroc M, et al: PowerDoppler sonographic pattern of acute pyelonephri-tis in children: comparison with CT. AJR Am JRoentgenol 1996;166:1451.
11. Clautice-Engle T, Jeffrey RB Jr, Li KC, et al:Power Doppler imaging of focal lesions of the gas-trointestinal tract: comparison with conventionalcolor Doppler imaging. J Ultrasound Med 1996;15:63.
12. Chen CN, Cheng TJ, Tang YB, et al: Power Dopp-ler ultrasound—a new tool for small vessel assess-ment in microsurgery. In Proceedings of the 12th
LOH ET AL
470 JOURNAL OF CLINICAL ULTRASOUND

Symposium of the International Society of Recon-structive Microsurgery. Singapore, InternationalSociety of Reconstructive Microsurgery, 1996, p.391.
13. Bude RO, Rubin JM: Power Doppler sonography[editorial]. Radiology 1996;200:21.
14. Berg WA, Chang BW, DeJong MR, et al: ColorDoppler flow mapping of abdominal wall perforat-
ing arteries for transverse rectus abdominis myo-cutaneous flap in breast reconstruction: methodand preliminary results. Radiology 1994;192:447.
15. Amerhauser A, Moelleken BR, Mathes SJ, et al:Color flow ultrasound for delineating microsurgicalvessels: a clinical and experimental study. AnnPlast Surg 1993;30:193.
POWER DOPPLER IMAGING OF MUSCLE FLAPS
471VOL. 25, NO. 9, NOVEMBER/DECEMBER 1997