Embed Size (px)
Citation preview
ARTICLE IN PRESS
EXPERIMENTAL
ANDTOXICOLOGIC
PA THOLOGY
0940-2993/$ - se
doi:10.1016/j.et
$Encouraged
in the Develo
Clinical Aspect
ogy, June 29–Ju�CorrespondE-mail addr
Experimental and Toxicologic Pathology 56 (2004) 103–112
www.elsevier.de/etp
Potential stem cell therapy and application in neurotrauma$
M. Brodhuna,�, R. Bauerb, S. Patta
aInstitute of Pathology, Friedrich Schiller University, Bachstrasse 18, Jena 07740, GermanybInstitute of Pathophysiology and Pathobiochemistry, Friedrich Schiller University, Jena, Germany
Received 19 March 2004; accepted 29 April 2004
Abstract
Traumatic brain injury results from a sudden and external physical insult to the head, which is often accompanied bymotor and cognitive impairment. Neurotrauma is characterized not only by focal abnormalities, but rather by multifocal,or even global structural and functional disturbances of the brain network. The impact initially causes necrotic cell deathin the underlying tissue, followed by apoptotic cell death in the surrounding tissue due to multiple subsequent events,such as ischemia, excitotoxicity and altered gene expression. These pathological conditions are associated with highmorbidity and mortality. Despite the high medical and economical relevance of neurotrauma there are currently nosufficient treatments. Supplementary therapeutic strategies have to be established. Many types of stem cells have theability to engraft diffusely and become integral members of structures throughout the host CNS. Intrinsic factors appearto derive spontaneously from stem cells and seem to be capable of neuroprotective and/or neuroregenerative functions.Furthermore stem cells can be readily engineered to express specific genes. Such observations suggest that stem cellsmight participate in reconstructing the molecular and cellular milieu of traumatized brains. In this paper, the state ofstem cell research is reviewed and its possible application in neurotrauma will be discussed.r 2004 Elsevier GmbH. All rights reserved.
Keywords: Stem cells; Neurotrauma; Spinal cord injury
Introduction
Stem cells (SC) have the ability to self replicate forindefinite periods often throughout the life of theorganism (van der Kooy and Weiss, 2000). Underappropriate conditions, or given the right signals,stem cells can originate different cell types throughasymmetric cell division. Differences in stem cells
e front matter r 2004 Elsevier GmbH. All rights reserved.
p.2004.04.004
by suggestions at the Symposium ‘‘Traumatic Injury
ping Brain: Biomechanical, Pathophysiological and
s’’ at the 4th International Congress of Pathophysiol-
ly 5, 2002, Budapest, Hungaria.
ing author.
ess: [email protected] (M. Brodhun).
depend on their location and differentiation potential(Gage, 2000; Fuchs and Segre, 2000; Weissman, 2000).There is a multitude of different types of stem cell typeswithin the human body, including blood stem cells,muscle/bone stem cells, brain stem cells, and liver stemcells (Blau et al., 2001).Biologic therapies derived from such cells are
expected to be effective in treatment of a wide rangeof medical conditions. The ability of stem cells frommultiple sources to regenerate tissue may increase theflexibility and applicability of therapeutic strategies. Inneurological diseases the aim of cell therapy is toreplace, repair, or enhance the biological function ofdamaged cells in order to restore or receive brainfunctions (Gage, 1998). This may occur through
ARTICLE IN PRESS
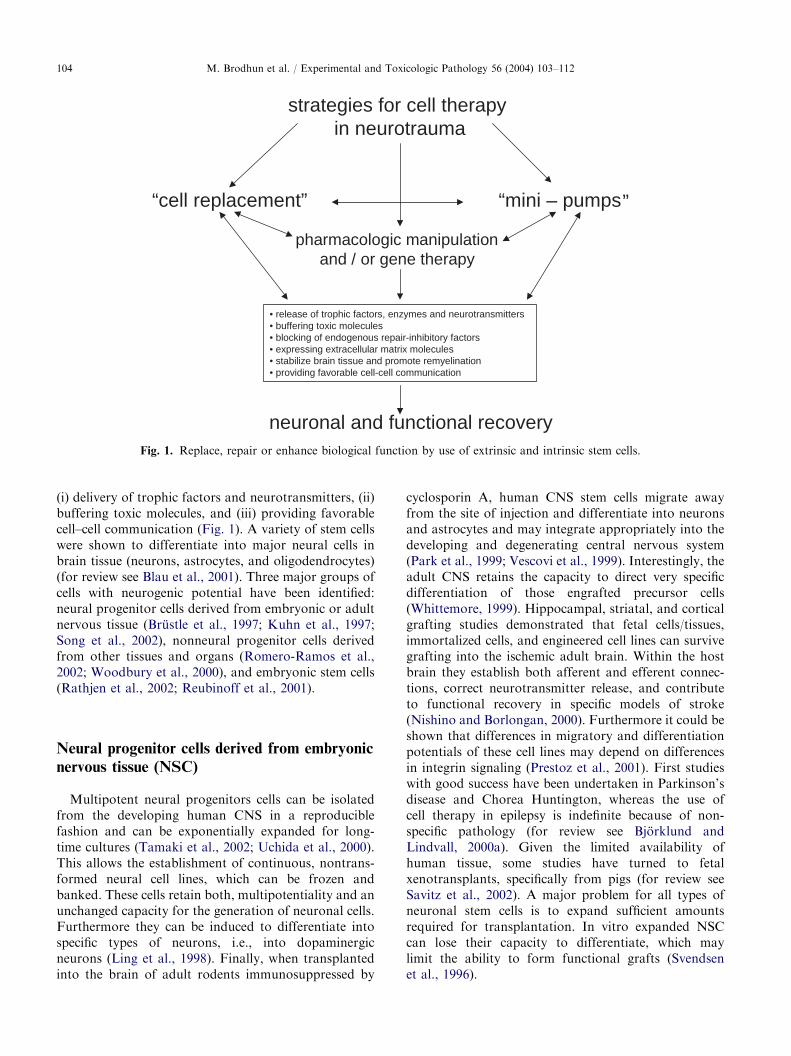
strategies for cell therapy in neurotrauma
“cell replacement” “mini – pumps
neuronal and functional recovery
• release of trophic factors, enzymes and neurotransmitters• buffering toxic molecules• blocking of endogenous repair-inhibitory factors• expressing extracellular matrix molecules• stabilize brain tissue and promote remyelination• providing favorable cell-cell communication
pharmacologic manipulationand / or gene therapy
“
Fig. 1. Replace, repair or enhance biological function by use of extrinsic and intrinsic stem cells.
M. Brodhun et al. / Experimental and Toxicologic Pathology 56 (2004) 103–112104
(i) delivery of trophic factors and neurotransmitters, (ii)buffering toxic molecules, and (iii) providing favorablecell–cell communication (Fig. 1). A variety of stem cellswere shown to differentiate into major neural cells inbrain tissue (neurons, astrocytes, and oligodendrocytes)(for review see Blau et al., 2001). Three major groups ofcells with neurogenic potential have been identified:neural progenitor cells derived from embryonic or adultnervous tissue (Brustle et al., 1997; Kuhn et al., 1997;Song et al., 2002), nonneural progenitor cells derivedfrom other tissues and organs (Romero-Ramos et al.,2002; Woodbury et al., 2000), and embryonic stem cells(Rathjen et al., 2002; Reubinoff et al., 2001).
Neural progenitor cells derived from embryonic
nervous tissue (NSC)
Multipotent neural progenitors cells can be isolatedfrom the developing human CNS in a reproduciblefashion and can be exponentially expanded for long-time cultures (Tamaki et al., 2002; Uchida et al., 2000).This allows the establishment of continuous, nontrans-formed neural cell lines, which can be frozen andbanked. These cells retain both, multipotentiality and anunchanged capacity for the generation of neuronal cells.Furthermore they can be induced to differentiate intospecific types of neurons, i.e., into dopaminergicneurons (Ling et al., 1998). Finally, when transplantedinto the brain of adult rodents immunosuppressed by
cyclosporin A, human CNS stem cells migrate awayfrom the site of injection and differentiate into neuronsand astrocytes and may integrate appropriately into thedeveloping and degenerating central nervous system(Park et al., 1999; Vescovi et al., 1999). Interestingly, theadult CNS retains the capacity to direct very specificdifferentiation of those engrafted precursor cells(Whittemore, 1999). Hippocampal, striatal, and corticalgrafting studies demonstrated that fetal cells/tissues,immortalized cells, and engineered cell lines can survivegrafting into the ischemic adult brain. Within the hostbrain they establish both afferent and efferent connec-tions, correct neurotransmitter release, and contributeto functional recovery in specific models of stroke(Nishino and Borlongan, 2000). Furthermore it could beshown that differences in migratory and differentiationpotentials of these cell lines may depend on differencesin integrin signaling (Prestoz et al., 2001). First studieswith good success have been undertaken in Parkinson’sdisease and Chorea Huntington, whereas the use ofcell therapy in epilepsy is indefinite because of non-specific pathology (for review see Bjorklund andLindvall, 2000a). Given the limited availability ofhuman tissue, some studies have turned to fetalxenotransplants, specifically from pigs (for review seeSavitz et al., 2002). A major problem for all types ofneuronal stem cells is to expand sufficient amountsrequired for transplantation. In vitro expanded NSCcan lose their capacity to differentiate, which maylimit the ability to form functional grafts (Svendsenet al., 1996).

ARTICLE IN PRESSM. Brodhun et al. / Experimental and Toxicologic Pathology 56 (2004) 103–112 105
Neural progenitor cells derived from adult
nervous tissue (NSC)
In the adult brain generation of new neurons fromneuronal stem and progenitor cells predominantlyoccurs in two brain regions, in the subventricular zone(SVZ) of the lateral ventricle and in the subgranularzone of the dentate gyrus (for review see Gould andGross, 2002). In the SVZ new interneurons aregenerated for the olfactory bulb, whereas new granulecells, which migrate into the granule cell layer andestablish axonal projections to area CA3 along themossy fiber tracts, are formed in the subgranular zone ofthe dentate gyrus (Bjorklund and Lindvall, 2000b,Kempermann, 2002b). These newly formed neuronshave electrophysiological properties indistinguishablefrom older neurons (van Praag et al., 2002). A study ofCameron and McKay (2001) indicated that approxi-mately �9000 progenitor cells exist in the dentate gyruswhich have a cell cycle time approximately of 24 h.However, an exact estimation of NSC numbers in theadult brain is always limited by technical/methodologi-cal problems (Gould and Gross, 2002). Adult neurogen-esis shows a continuous turnover. Furthermore newneurons may arise from cells with glial characteristics(Doetsch et al., 1999; Seri et al., 2001). Because the totalnumber of neurons in the adult brain does notdramatically increase, function of these new cellsremains unclear to date. The most favorable hypothesisis that they serve as gatekeeper for memory function(Kempermann, 2002a). It is also speculated thatdisturbances in neurogenesis may contribute to thepathogenesis of neurodegenerative and mood disorders(Kempermann, 2002b; Armstrong and Barker, 2001). Inother parts of the central nervous system (frontal,temporal and parietal cortex, in the striatum, septumand spinal cord) a quiescent potential of neuronal stemcells has been described (Gu et al., 2000; Jiang et al.,2001; Magavi et al., 2000; Palmer et al., 1995).Adult neurogenesis can be modulated by external and
internal factors. Enriched environment (Kempermann,2002a, b) and estrogens (Tanapat et al., 1999) enhancesthe survival of newly generated cells in the hippocam-pus, whereas stress (Gould and Tanapat, 1999) andincreased glucocorticoid levels (Tanapat et al., 2001)inhibit the proliferation of these cells. Furthermore itcould be shown that neuronal stem cells proliferatefollowing neuronal lesions, i.e., acute ischemia, pro-longed damage and mechanical injury (Parent andLowenstein, 2002). Following 5 or 10min of globalischemia in the adult gerbil there is a tenfold increase inthe birth of new cells in the subgranular zone of dentategyrus of the hippocampus as assessed using BrdUincorporation (Sharp et al., 2002). This begins at 7 days,peaks at 11 days, and decreases thereafter (Sharp et al.,2002). Over the next month approximately 25% of the
newborn cells disappear. Of the remaining cells, 60%migrate into the granule cell layer where two-thirdsbecome neurons. The other 40% of these cells migrateinto the dentate hilus where 25% of these becomeastrocytes. Interestingly, others have observed low levelsof cortical neurogenesis after transient middle cerebralartery occlusion and after reversible photothromboticstroke (Gu et al., 2000; Jiang et al., 2001).In vivo procedure for the induction of massive
proliferation, directed migration, and neurodifferentia-tion in the damaged adult central nervous system wouldhold promise for the treatment of a variety ofneurological diseases. Indeed the neurogenic responsecan be enhanced by application of exogenous sub-stances. Fallon et al. (2000) could show a rapidproliferation of forebrain stem cells using a combinationof 6-hydroxydopamine lesions of the substantia nigradopaminergic neurons and infusions of transforminggrowth factor alpha (TGFa) into forebrain structures.These were followed by a timed migration with anincrease of neuronal and glial progenitors directedtoward the region of the TGFa infusion site. Further-more, intracerebroventricular administration of hepar-in-binding epidermal growth factor like growth factor(HB-EGF) in adult rats increased BrdU labeling in thesubventricular zone and in the subgranular zone ofdentate gyrus (Jin et al., 2002). Different effects of FGFand EGF on proliferation and differentiation have beendescribed (Kuhn et al., 1997). However, there is still adebate, whether endogenous progenitor cells trans-planted following differential types of brain injury arecapable to replace the variety of damaged neuronal cellsand whether these cells are functionally integrated. It isalso conceivable that they are aberrantly integrated andform abnormal connections, that increase the initialfunctional impairment (for review see Kruger andMorrison, 2002).
Nonneural progenitor cells derived from other
tissues and organs
Hematopoietic stem cells (HSC)
Lymphohematopoietic cells are constantly replen-ished by common precursors called hematopoietic stemcells (Till et al., 1964). HSC give rise to progeny thatinclude all other blood cell types, including additionalHSC. These cells are the principal known cellsresponsible for developing and maintaining of theblood-forming and the immune system during ontogenyand after bone marrow transplantation. Multiple tissuesources, including bone marrow, umbilical cordblood and peripheral blood, contain HSC. In mice,HSC have been phenotypically isolated and extensively

ARTICLE IN PRESSM. Brodhun et al. / Experimental and Toxicologic Pathology 56 (2004) 103–112106
characterized both in vitro and in vivo (Morrison et al.,1995). Hematopoietic stem cells retain the capacity todifferentiate into cell types other than blood cells.Both, primitive hematopoietic progenitors (CD117+,Sca-1+) and more committed hematopoietic progeni-tors (CD117+, Sca-1�) can be induced to developtowards ependymocytes and to express oligodendrocyte,neuronal and astroglial markers after injection into thetelencephalon of P0 C3H/He mice (Bonilla et al., 2001).During the last years transdifferentiation of bonemarrow cells into neuronal cells in vivo has been proven(for review see Mezey et al., 2000). However, severalsome groups (Castro et al., 2002; Castro et al., 2003;Wagers et al., 2002) have shown that transdifferentia-tion of circulating HSC and/or their progeny in vivointo nonhematopoietic cells is an extremely rare event, ifit occurs at all. Demonstration of bone marrow derivedcells in the brain may depend on the experimentalsystem used and on technical problems. Research has tobe continued to solve this controversy. Furthermore,little is known about the molecular mechanismsresponsible for the HSC phenotype and the genesinvolved in the decision of self-renewal and differentia-tion (Terskikh et al., 2000). Despite the ability to culturehematopoietic progenitors, in vitro culture of long-termself-renewing pluripotent HSCs has not been achieved.
Bone marrow stroma cells (BMSC)
In addition to hematopoietic cells bone marrowcontains cells that meet the criteria for stem cells ofnonhematopoietic tissues (Chen et al., 2001). These cellswere first characterized by Friedenstein et al. (1968)demonstrating their adherent, clonogenic, nonphagocy-tic, and fibroblastic properties (colony-forming units-fibroblastic, CFU-Fs). They can easily be obtainedfollowing a simple bone marrow aspiration procedureallowing the subsequent expansion in culture through asmany as 50 population passages (Devine, 2002). BMSCshave attracted interest because of their capacity for self-renewal in a number of nonhematopoietic tissues andtheir multipotentiality for differentiation (Chen et al.,2001; Pittenger et al., 1999). BMSCs can engraft inmultiple tissues and produce fibrous tissue, bone, orcartilage and muscle when implanted into appropriatetissue in vivo (Pereira et al., 1995). There is also evidencethat BMSCs can also adopt the fate of endodermal andectodermal cell types (Zhao et al., 2002). Woodbury et al.(2000) described a protocol for in vitro differentiation ofBMSCs into neuron like cells. BMSCs also possess thecapacity to pass the blood-brain barrier and migrate intothe forebrain and cerebellum (Kopen et al., 1999).Differentiation into astrocytes and neurons has beenshown after injection in neonatal mouse brain (Kopenet al., 1999). Recently, also functional improvement has
been described after human and rat BMSCs transplanta-tion following focal brain ischemia in rats (Chen et al.,2001; Li et al., 2001; Zhao et al., 2002). However, thenumber of cells with neuronal phenotype after transplan-tation of BMSC is low and transplanted animals hadno differences in infarct volume compared with controls(Li et al., 2000) suggesting neuroprotective effects aremore related to trophic factor support (‘‘mini pumps’’) byBMSC than to cell replacement. These cells in BMSChave the advantages that they might be delivered toinjured brain tissue without need for invasive stereotacticoperations and show less immunologic problems, whenobtained from the patient itself. However, suitableparenteral application strategies have to be developedto accumulate a sufficient amount of BMSC into theinjured brain with minimal distribution in other organs.
Embryonic stem cells (ES)
Embryonic stem cells are pluripotent cells isolatedfrom the inner cell mass of blastocystes (Gerlach et al.2002), which can differentiate to all cells in the organism(Nagy et al. 1993). ES cells possess the capacity togenerate neurons and glial cells, which in some instancesexpress markers characteristic of specific classes ofneurons (Hynes and Rosenthal, 2000). Arborized axonaland dentritic morphologies of ES have been observedunder in vitro and in vivo conditions (Brustle et al., 1997).With regard to Parkinson0s disease several groups areexploring the possibilities of using embryonic and fetalstem cells to produce dopaminergic cells (Storch et al.,2001; Chung et al., 2002). To date more than 300Parkinson patients have been transplanted with embryo-nic ventral mesenchephalic neurons worldwide with atleast partly satisfying results (Hagell and Brundin 2001;Lindvall and Hagell 2001). The most severe problemsrelated to this stem cell therapy are (i) interindividualvariation in therapeutic benefits depending on theintegration of transplanted cells, (ii) side-effects in theform of ‘‘off’’ dyskinesias, and (iii) control of prolifera-tion and differentiation of these cells with the risk oftumor formation (Hagell et al., 1999). Moreover, use ofES is restricted because of ethical and governmentalrestrictions but also technical and logistical issues.
Strategies for neurotrauma
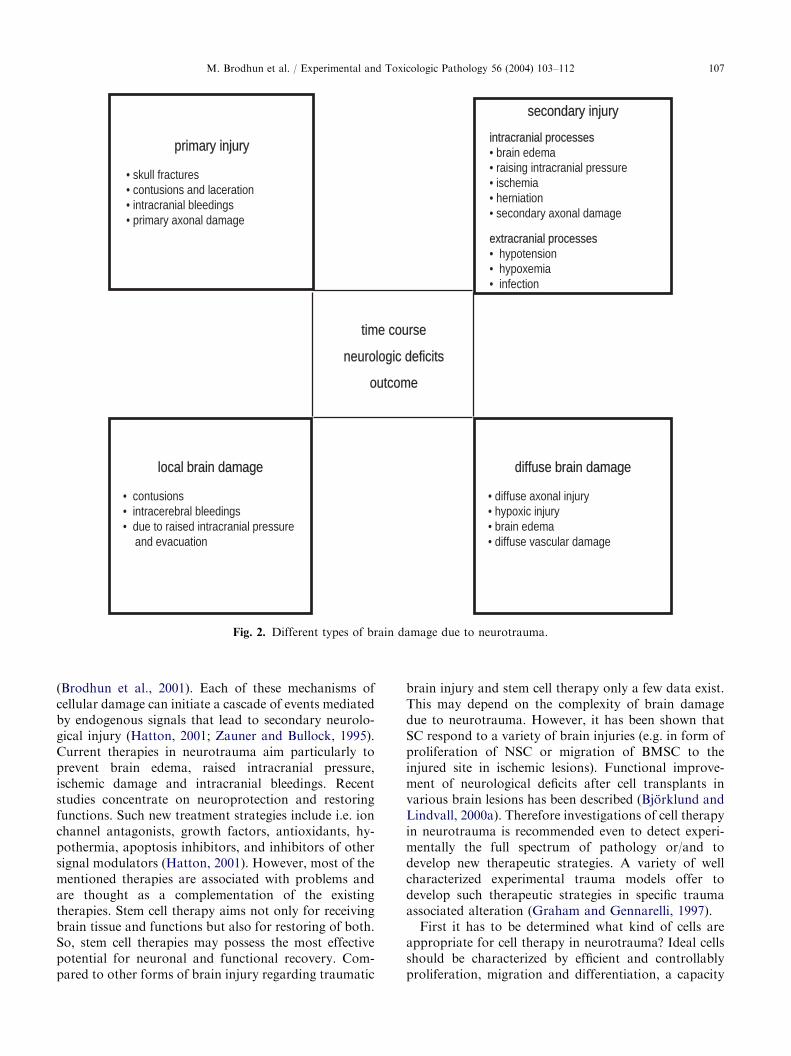
Neuropathological, brain trauma can be differen-tiated in local and diffuse lesions as well as in primaryand secondary injuries (Fig. 2; Patt and Brodhun, 1999).Depending on the type of brain injury, the intensity andthe success of resuscitation, necrosis, apoptosis, inflam-matory and excitotoxic cellular damage can be observed
ARTICLE IN PRESS
diffudiffuse braiain damn damagage
• diffuse axonal injury• hypoxic injury• brain edema• diffuse vascular damage
primaprimary iy injurjury
• skull fractures• contusions and laceration• intracranial bleedings• primary axonal damage
sesecocondandary i injurnjury
intracracraninialal processes processes• brain edema• raising intracranial pressure• ischemia• herniation• secondary axonal damage
extextracraniacranialal processesprocesses• hypotension • hypoxemia• infection
time coursetime course
neurologic deficitsneurologic deficits
outcomeoutcome
locallocal braibrain damdamagage
• contusions• intracerebral bleedings• due to raised intracranial pressure
and evacuation
Fig. 2. Different types of brain damage due to neurotrauma.
M. Brodhun et al. / Experimental and Toxicologic Pathology 56 (2004) 103–112 107
(Brodhun et al., 2001). Each of these mechanisms ofcellular damage can initiate a cascade of events mediatedby endogenous signals that lead to secondary neurolo-gical injury (Hatton, 2001; Zauner and Bullock, 1995).Current therapies in neurotrauma aim particularly toprevent brain edema, raised intracranial pressure,ischemic damage and intracranial bleedings. Recentstudies concentrate on neuroprotection and restoringfunctions. Such new treatment strategies include i.e. ionchannel antagonists, growth factors, antioxidants, hy-pothermia, apoptosis inhibitors, and inhibitors of othersignal modulators (Hatton, 2001). However, most of thementioned therapies are associated with problems andare thought as a complementation of the existingtherapies. Stem cell therapy aims not only for receivingbrain tissue and functions but also for restoring of both.So, stem cell therapies may possess the most effectivepotential for neuronal and functional recovery. Com-pared to other forms of brain injury regarding traumatic
brain injury and stem cell therapy only a few data exist.This may depend on the complexity of brain damagedue to neurotrauma. However, it has been shown thatSC respond to a variety of brain injuries (e.g. in form ofproliferation of NSC or migration of BMSC to theinjured site in ischemic lesions). Functional improve-ment of neurological deficits after cell transplants invarious brain lesions has been described (Bjorklund andLindvall, 2000a). Therefore investigations of cell therapyin neurotrauma is recommended even to detect experi-mentally the full spectrum of pathology or/and todevelop new therapeutic strategies. A variety of wellcharacterized experimental trauma models offer todevelop such therapeutic strategies in specific traumaassociated alteration (Graham and Gennarelli, 1997).First it has to be determined what kind of cells are
appropriate for cell therapy in neurotrauma? Ideal cellsshould be characterized by efficient and controllablyproliferation, migration and differentiation, a capacity

ARTICLE IN PRESSM. Brodhun et al. / Experimental and Toxicologic Pathology 56 (2004) 103–112108
to produce high numbers of cells from minor donormaterial under simple growth conditions, long timestorability, low risk of immunological reactions, a greatpotential for good integration in neuronal circuits,localization-depended specific differentiation and relia-bility to improve neurologic deficits after administrationwithout side effects. Moreover, they should not berestricted to ethical issues.In spinal cord injury a few studies (Liu et al., 2000;
Senior, 2000) have shown that embryonic stem cellssurvive and differentiate into astrocytes, oligodendrocytesand neurons, and migrate away from the lesion. Gaitanalysis demonstrated that transplanted rats showedbetter motor performance compared with ‘sham-oper-ated’ controls or control rats transplanted with adultmouse neocortical cells (McDonald et al., 2000). Choppet al. (2000) also found significant functional improve-ment in rats treated with BMSC transplantation afterspinal cord injury 2–5 weeks postinjury.In brain trauma, however, contusions probably could be
replaced through stem cell implantations similar to thestudies in focal and global ischemia (Bjorklund andLindvall, 2000a). This may occur with SCs with a lowerneuronal differential potential (e.g. BMSC or HSC) as‘‘mini-pumps’’ to generate a neuroprotective milieu oreven with SCs with higher neuronal differential potential(NSC, ES) for ‘‘cell replacement’’ (Fig. 1). As ‘‘minipumps’’ cells have the capacity to release of trophic factorsand enzyms and to buffer toxic molecules. Therefore a fullneuronal differentiation of used stem cells seems notalways to be essential for reaching neurological improve-ment. As examples for ‘‘mini pumps’’ BMSC and HSCtransplants will be accompanied without provocation ofimmunological reactions when patient’s own cells are used.However, long time surviving and functional integration ofthese grafts into brain tissue of such transplants will be lesscompared to NSC or ES transplants as typical candidatesfor cell replacement strategies. Using the lateral controlledcortical contusion model in mice Tate et al. (2002) showedthat NSCs injected into the injury cavity lined the injurypenumbra. Furthermore, cells applied together with afibronectin-containing matrix showed increased survivaland migration after 3 weeks relative to injections of cellsalone (Tate et al., 2002). Interestingly, striatal transplantsin the same model had lower numbers of surviving cells(Tate et al., 2002). Riess et al. (2002) showed significantlyimproved motor function after both ipsi- or contralateraltransplantation of NSC clone C17.2 at 3 days after lateralcontrolled cortical impact brain injury, whereas cognitivedysfunction was unaffected. Grafted cells survived as longas 13 weeks after transplantation (whole experimentalperiod). A differentiation of transplanted cells to oligoden-drocytes has not been observed. Immortalized neuronalstem cells (HiB5) that have been retrovirally transducedto produce NGF can markedly improve neuromotor aswell as cognitive function and rescue hippocampal CA3
neurons after lateral fluid percussion brain injury whentransplanted into the injured brain 24 hours postinjury(Philips et al., 2001). The latter study supports the‘‘mini-pump’’-hypothesis.
Ischemic lesions in trauma may be positively influ-enced by intravenous or intraarterial application of SCs.Lu et al. (2001) showed that intraarterial transplantationof BMSCs in adult rats was a suitable route forintracerebral administration of BMSCs following trau-matic brain injury (TBI). BMSCs infused intraarteriallyafter TBI survived and migrated into the brain whenapplied 24hours after TBI. BrdU-positive BMSC werelocalized to the boundary zone of the lesion, corpuscallosum and cortex of the ipsilateral hemisphere. Thenumber of BrdU-positive cells was significantly higher inthe ipsilateral hemisphere than in the contralateralhemisphere. Interestingly, more intraarterially infusedBMSCs engrafted after culturing with NGF and BDNF.The expression of neuronal and astrocytic markers wasgreater when the cells were precultured with NGF andBDNF. On the other hand, HSC seem not totransdifferentiate into neuronal cells in experimentalcortical stab injury and cortical contusions injury(Castro et al., 2002). Neuroprotective effects of bothBMSC and HSC are more related to trophic factorsupport than to cell replacement suggesting that theyserve as ‘‘mini-pumps’’. Using cells as ‘‘mini-pumps’’apoptotic and other forms of secondary brain injurymay also be prevented (Tatton et al., 1997).To activate endogenous stem cells is—beside implanta-
tion of neuronal or embryonic stem cells into ischemic brainlesions—another strategy for ‘‘cell replacement’’ with theaim to create new connections in the neuronal network.Using the fluid percussion injury model in rats and BrdU-staining of neuronal progenitor cells Chirumamilla et al.(2002) showed that the total number of proliferating cellswas immediately increased in the injury group for both theSVZ and the hippocampus. However, the proliferating cellsin the SVZ did not express any neuronal markers. Incontrast, there was a significant increase in the number ofimmature astrocytes and activated microglia in thehippocampus. These results may indicate that progenitorcells might not have begun to differentiate into a neuronalphenotype. However, more reliable results may be achievedby providing an extracellular brain matrix or by addinggrowth factors to stimulate proliferation, differentiation andmigration (Gage, 1998). Furthermore, some studies havedescribed a quiescent potential of neuronal stem cells inmany parts of the central nervous system outside the knownproliferation zones (Gu et al., 2000; Jiang et al., 2001;Magavi et al., 2000; Palmer et al., 1995). Specificpharmacological modulation of these quiescent neuronalstem cells may lead to a successful treatment of focal andglobal brain lesions.
Diffuse or traumatic axonal injury is a frequentoccurring damage in brain- and spinal cord-trauma

ARTICLE IN PRESSM. Brodhun et al. / Experimental and Toxicologic Pathology 56 (2004) 103–112 109
and associated with severe neurological deficits (Pov-lishock and Christman, 1995). Therefore it is importantto estimate, whether diffuse axonal injury may berepaired by SC. Intraspinal transplants (e.g., fetalneuronal cells, progenitor stem cells, and olfactoryensheathing cells) have been used to restore intraspinalcircuitry or to serve as a ‘‘bridge’’ for damaged axons.Among these transplants, olfactory ensheathing cellsprovide a particularly favorable substrate for spinalaxonal regeneration because these cells can secreteextracellular molecules and neurotrophic factors andhave the ability to migrate into gliotic scar tissue, animportant attribute that might be associated with highpotential for axonal regeneration (Lu and Ashwell,2002). Using an in vitro model of axotomy of theentorhino-hippocampal pathway, del Rio et al. (2002)showed that Cajal-Retzius cells triggered the regenera-tion of the axotomized entorhino-hippocampal path-way. Furthermore, the regrowth induced by Cajal-Retzius cells was robust and its pattern was indis-tinguishable from that of the unlesioned entorhino-hippocampal pathway (del Rio et al., 2002). NSCs and afew types of glial precursors have shown the capabilityto differentiate into oligodendrocytes and to remyeliatedemyelinated axons in the CNS, an important conditionfor restoring white matter damage. But the functionalextent of remyelination achieved by these transplants islimited to date (Cao et al., 2002). Predifferentiation and/or genetic modification of stem cells cultures prior totransplantation may lead to the generation of high cellnumbers of the desired phenotype following transplan-tation (Park et al., 2002). New strategies derive frominvestigations of CNS myelin components, that inhibitregenerating axons, including NogoA, myelin associatedglycoprotein (MAG; Domeniconi et al., 2002; Liu et al.,2002), and oligodendrocyte myelin glycoprotein (Omgp;Wang et al., 2002). All these proteins seem to effect onthe Nogo receptor (NgR) which is proposed to play acritical regulatory role in inhibition of axonal regenera-tion in the adult CNS (Kruger and Morrison, 2002).Functional blocking of endogenous inhibitory factorssuch as Nogo-A or proteoglycans (Jones and Tuszynski,2002) by genetic or even pharmacological modificationof SC may promote axonal growth and functionalrecovery. First studies in animal models of spinal cordinjury were successful (GrandPre et al., 2002).Another potential application of cell therapy may be
the prevention or restoration of vascular damage due totraumatic injuries. BMSC and human umbilical cordblood cells have been shown as a source of endothelialcells (Hess et al., 2002; Lu et al., 2002).However, stem cell therapy is probably not sufficient
by itself. It is possibly necessary to combine stem celltherapy with other established treatment strategies.Furthermore, cell therapy may not be equally good forall types of brain injury in neurotrauma (Fig. 2). It is
already known, that the choice of stem cells fortransplantation depends on many factors: the type,extend and degree of brain lesion, the desired differ-entiation of the stem cells, their properties, the ability tocultivate these cells, the number of cells needed etc.(Gage, 1998; Nishino et al., 2000; Whittemore, 1999).The ability of stem cells to establish reciprocal connec-tions with the host brain also depends on the age of thehost (Bjorklund and Lindvall, 2000a). Olfactory celldivision rate decreases in relation to age, especiallyduring the first months of life (Fung et al., 1997; Ohtaand Ichimura, 2000; Ducray et al., 2002). This appearsto be linked to the reduced expression level of numerouscell cycle regulators in relation to age (Legrier et al.,2001). These effects were also observed for neuralprecursors in the brain (Kuhn and Dickinson-Anson,1996). Moreover, in vitro culturing of such cells fromhuman post mortem brain showed a decreased numberof cell cycles periods in relation with the donor age(Palmer et al., 2001). This data suggest that potentialefficiency of cell therapy in infants may be moreefficient.A prerequisite for the clinical use of stem cells is the
determination of the safety characteristics of the donorcells in terms of tumorgenicity, viability, sterility, andantigenic compatibility far in advance of the scheduledday of surgery (Vescovi et al., 1999). Even thoughtumorgenicity seems to be a minor problem with fetal oradult stem cells compared to ES and immortilized cellsources, proliferation has to be estimated in long termtrials in experimental models before clinical use. One ofthe most serious challenges after non autologues celltransplantation is the destruction of the implant by thehost immune system which also may cause secondarybrain injury to the primary lesion. Regarding to stemcell therapy in brain disease generally only very fewdetailed data exist and have to be evaluated urgently(Modo et al., 2002). Even though the brain and thespinal cord may have decreased immune responsiveness,the implanted cells might trigger systemic immunologi-cal processes, if the blood-brain barrier is compromiseddue to brain lesions or the surgery procedure used. Waysto handle immunological reactions may include encap-sulation, genetic modifications of tranplanted cells andimmunosuppression. Producing specific cell types frompatient0s own stem cells would provide immunologicaladvantages (Gerlach et al., 2002).
Conclusion
The ideal stem cell do not exist to date. However, ithas been shown that a wide range of stem cells canimprove neurological functions in a variety of brainlesions. Therefore cell therapy may serve as a future
ARTICLE IN PRESSM. Brodhun et al. / Experimental and Toxicologic Pathology 56 (2004) 103–112110
restorative therapy for neurotrauma. Further studies arenecessary to analyze whether stem cells have a putativetherapeutic role as supportive cells, by their own or asvehicles of gene delivery, and to what extend these cellsare capable for neuronal remodeling. For the most celltypes it is still unknown, what percentage of trans-planted or stimulated progenitor cells differentiate intoterminal neurons versus glial cells. Moreover it has to beshown, in which dimension transplanted cells areintegrated in neuronal circuits, promote functionalrecovery and whether grafts survive for longer periodsof time. For neurotrauma, it has to be demonstrated,which cells are more safe and effective in the differentlesions, which cells are more useful for treatment ofwhite matter and underlying axonal damage, which timepoints and application forms, which numbers of cells arethe best and what type of immunosuppression is needed.It has also to be determined which trauma patientsshould undergo transplantation, what trauma lesionsand location sites (cortex, white matter, direct intocontusion area or neighborhood, contralateral hemi-sphere, parenteral) are amenable to cell therapy, and towhat extend therapeutic benefits justify side effects ofcell therapy. Although clinical trials in Parkinson’sdisease and stroke are currently underway, only little isknown about the basic biology of transplanted cells.Standardized investigation protocols have to be devel-oped for better comparison of the different donor cellsand application forms with regard to different lesiontypes of neurotrauma.
References
Armstrong RJ, Barker RA. Neurodegeneration: a failure of
neuroregeneration? Lancet 2001;6:1174–6.
Bjorklund A, Lindvall O. Cell replacement therapies for
central nervous system disorders. Nature Neurosci
2000a;3:537–44.
Bjorklund A, Lindvall O. Self-repair in the brain. Nature
2000b;405:892–5.
Blau HM, Brazelton TR, Weimann JM. The evolving concept
of a stem cell: entity or function? Cell 2001;105:829–41.
Bonilla S, Alarcon P, Verde RV, et al. From hematopoietic
stem cells to neural stem cells Int. J Dev Biol 2001;45:67–8.
Brodhun M, Fritz H, Walter B, et al. Immunomorphological
sequelae of fluid-percussion induced severe brain injury
in juvenile pigs – Effects of mild hypothermia. Acta
Neuropathol 2001;101:424–34.
Brustle O, Spiro AC, Karram K, et al. In vitro-generated
neuronal precursors participate in mammalian brain devel-
opment. Proc Natl Acad Sci USA 1997;94:14809–14.
Cameron HA, McKay RD. Adult neurogenesis produces a
large pool of new granule cells in the dentate gyrus. J Comp
Neurol 2001;435:406–17.
Cao Q, Benton RL, Whittemore SR. Stem cell repair of central
nervous system injury. J Neurosci Res 2002;68:501–10.
Castro RF, Jackson KA, Goodell MA, et al. ‘‘Failure of bone
marrow cells to transdifferentiate into neural cells in vivo’’.
Science 2002;297:1299.
Castro RF, Jackson KA, Goodell MA, et al. Response to
Comment on Failure of Bone Marrow Cells to Trans-
differentiate into Neural Cells in Vivo. Science 2003;299:
1184.
Chen J, Li Y, Wang L, et al. Therapeutic benefit of
intravenous administration of bone marrow stromal cells
after cerebral ischemia in rats. Stroke 2001;32:1005–11.
Chirumamilla S, Sun D, Bullock MR, et al. Traumatic brain
injury induced cell proliferation in the adult mammalian
central nervous system. J Neurotrauma 2002;19:693–703.
Chopp M, Zhang XH, Li Y, et al. Spinal cord injury in rat:
treatment with bone marrow stromal cell transplantation.
Neuroreport 2000;13:3001–5.
Chung S, Sonntag KC, Andersson T, et al. Genetic engineering
of mouse embryonic stem cells by Nurr1 enhances
differentiation and maturation into dopaminergic neurons.
Eur J Neurosci 2002;16:1829–38.
del Rio JA, Sole M, Borrell V, et al. Involvement of Cajal-
Retzius cells in robust and layer-specific regeneration of the
entorhino-hippocampal pathways. Eur J Neurosci 2002;15:
1881–90.
Doetsch F, Caille I, Lim DA, et al. Subventricular zone
astrocytes are neuronal stem cells in the adult mammalian
brain. Cell 1999;97:703–16.
Domeniconi M, Cao Z, Spencer T, et al. Myelin-associated
glycoprotein interacts with the Nogo66 receptor to inhibit
neurite outgrowth. Neuron 2002;35:283–90.
Ducray A, Bondier JR, Michel G, et al. Recovery following
peripheral destruction of olfactory neurons in young and
adult mice. Eur J Neurosci 2002;15:1907–17.
Fallon J, Reid S, Kinyamu R, et al. In vivo induction of
massive proliferation, directed migration, and differentia-
tion of neural cells in the adult mammalian brain. Proc Natl
Acad Sci USA 2000;97:14686–91.
Friedenstein AJ, Petrakova KV, Kurolesova AI, et al.
Heterotopic transplants of bone marrow. Analysis of
precursor cells of osteogenic and hematopoietic tissues.
Transplantation 1968;6:230–47.
Fuchs E, Segre JA. Stem cells: a new lease on life. Cell
2000;100:143–55.
Fung KM, Peringa J, Venkatachalam S, et al. Coordinate
reduction in cell proliferation and cell death in mouse
olfactory epithelium from birth to maturity. Brain Res
1997;761:347–51.
Gage FH. Cell therapy. Nature 1998;392:18–24.
Gage FH. Mammalian neuronal stem cells. Science
2000;287:1433–8.
Gerlach M, Braak H, Hartmann A, et al. Current state of
stem cell research for the treatment of Parkinson’s disease.
J Neurol 2002;249:III33–5.
Gould E, Tanapat P. Stress and hippocampal neurogenesis.
Biol Psychiat 1999;1:1472–9.
Gould E, Gross CG. Neurogenesis in adult mammals: some
progress and problems. J Neurosci 2002;22:619–23.
Graham DI, Gennarelli TA. Trauma. In: Graham DI, Lantos
PL, editors. Greenfield’s Neuropathology,. 6th ed. London:
Arnold; 1997. p. 198–262.
ARTICLE IN PRESSM. Brodhun et al. / Experimental and Toxicologic Pathology 56 (2004) 103–112 111
GrandPre T, Li S, Strittmatter SM. Nogo-66 receptor
antagonist peptide promotes axonal regeneration. Nature
2002;417:547–51.
Gu WG, Brannstrom T, Wester P. Cortical neurogenesis in
adult rats after reversible photothrombotic stroke. J Cerebr
Blood Flow Metabol 2000;20:1166–73.
Hagell P, Schrag A, Piccini P, et al. Sequential bilateral
transplantation in Parkinson’s disease: effects of the second
graft. Brain 1999;122:1121–32.
Hagell P, Brundin P. Cell survival and clinical outcome
following intrastriatal transplantation in Parkinson disease.
J Neuropathol Exp Neurol 2001;60:741–52.
Hatton J. Pharmacological treatment of traumatic brain
injury: a review of agents in development. CNS Drugs
2001;15:553–81.
Hess DC, Hill WD, Martin-Studdard A, et al. Bone marrow as
a source of endothelial cells and NeuN-expressing cells after
stroke. Stroke 2002;33:1362–8.
Hynes M, Rosenthal A. Embryonic stem cells go dopaminer-
gic. Neuron 2000;28:11–4.
Jiang W, Gu WG, Brannstrom T, et al. Cortical neurogenesis
in adult rats after transient middle cerebral artery occlu-
sion. Stroke 2001;32:1201–7.
Jin K, Mao XO, Sun Y, et al. Heparin-binding epidermal
growth factor-like growth factor: hypoxia-inducible expres-
sion in vitro and stimulation of neurogenesis in vitro and in
vivo. J Neurosci 2002;22:5365–73.
Jones LL, Tuszynski MH. Spinal cord injury elicits expression
of keratan sulfate proteoglycans by macrophages, reactive
microglia, and oligodendrocyte progenitors. J Neurosci
2002;22:4611–24.
Kempermann G. Why new neurons? Possible functions for
adult hippocampal neurogenesis. J Neuroscience 2002a;22:
635–8.
Kempermann G. Regulation of adult hippocampal neurogen-
esis – implications for novel theories of major depression.
Bipolar Disorders 2002b;4:17–33.
Kopen GC, Prockop DJ, Phinney DG. Marrow stroma cells
migrate throughout forebrain and cerrebellum, and they
differentiate into astrocytes after injection into neonatal
mouse brains. Proc Natl Acad Sci USA 1999;96:10711–6.
Kruger GM, Morrison S. Brain Repair by endogenous
progenitors. Cell 2002;110:3402–999.
Kuhn HG, Dickinson-Anson H, et al. Neurogenesis in the
dentate gyrus of the adult rat: age-related decrease of
neuronal progenitor proliferation. J Neurosci 1996;16:
2027–33.
Kuhn HG, Winkler J, Kempermann G, et al. EGF and FGF-2
have different effects on neuronal progenitors in the adult
rat brain. J Neuroscience 1997;17:5820–9.
Legrier ME, Ducray A, Propper A, et al. Cell cycle regulation
during mouse olfactory neurogenesis. Cell Growth Differ
2001;12:591–601.
Li Y, Chopp M, Chen J, et al. Intrastriatal transplantation of
bone marrow nonhematopoietic cells improves functional
recovery after stroke in adult mice. J Cereb Blood Flow
Metab 2000;20:1311–9.
Li Y, Chen J, Wang L, et al. Treatment of stroke in rat with
intracarotid administration of marrow stromal cells.
Neurology 2001;56:1666–72.
Lindvall O, Hagell P. Cell therapy and transplantation in
Parkinson’s disease. Clin Chem Lab Med 2001;39:
356–61.
Ling ZD, Potter ED, Lipton JW, et al. Differentiation of
mesencephalic progenitor cells into dopaminergic neurons
by cytokines. Exp Neurol 1998;149:411–23.
Liu S, Qu Y, Stewart TJ, et al. Embryonic stem cells
differentiate into oligodendrocytes and myelinate in culture
and after spinal cord transplantation. Proc Natl Acad Sci
USA 2000;97:6126–31.
Liu BP, Fournier A, GrandPre T, et al. Myelin-associated
glycoprotein as a functional ligand for the Nogo-66
receptor. Science 2002;16:1190–3.
Lu D, Li Y, Wang L, et al. Intraarterial administration of
marrow stromal cells in a rat model of traumatic brain
injury. J Neurotrauma 2001;18:813–9.
Lu J, Ashwell K. Olfactory ensheathing cells: their potential
use for repairing the injured spinal cord. Spine
2002;27:887–92.
Lu D, Sanberg PR, Mahmood A, et al. Intravenous
administration of human umbilical cord blood reduces
neurological deficit in the rat after traumatic brain injury.
Cell Transplant 2002;11:275–81.
Magavi S, Leavitt BR, Macklis JD. Induction of neurogenesis
in the neocortex of adult mice. Nature 2000;405:951–5.
McDonald JW, Liu XZ, Qu Y, et al. Transplanted embryonic
stem cells survive, differentiate and promote recovery in
injured rat spinal cord. Nat Med 2000;6:358.
Mezey E, Chandross KJ, Harta G, Maki RA, McKercher SR.
Turning blood into brain: cells bearing neuronal antigens
generated in vivo from bone marrow. Science 2000;290:
1779–82.
Modo M, Rezaie P, Heuschling P, et al. Transplantation of
neural stem cells in a rat model of stroke: assessment of
short-term graft survival and acute host immunological
response. Brain Res 2002;958:70–82.
Morrison SJ, Uchida N, Weissman IL. The biology of
hematopoietic stem cells. Annu Rev Cell Dev Biol
1995;11:35–71.
Nagy A, Rossant J, Nagy R, et al. Derivation of completely
cell culture-derived mice from early passage embryonic
stem cells. Proc Natl Acad Sci USA 1993;90:8424–8.
Nishino H, Borlongan CV. Restoration of function by neural
transplantation in the ischemic brain. Prog Brain Res
2000;127:461–76.
Ohta Y, Ichimura K. Immunohistochemical localization of
proliferating cells and epidermal growth factor receptors in
mouse olfactory epithelium. ORL J Otorhinolaryngol Relat
Spec 2000;62:20–5.
Palmer TD, Ray J, Gage FH. FGF-2-responsive neuronal
progenitors reside in proliferative and quiescent regions of
the adult brain. Mol Cell Neurosci 1995;6:474–86.
Palmer TD, Schwartz PH, Taupin P, et al. Cell culture.
Progenitor cells from human brain after death. Nature
2001;411:42–3.
Parent JM, Lowenstein DH. Seizure-induced neurogenesis: are
more new neurons good for an adult brain? Prog Brain Res
2002;135:121–31.
Park KI, Liu S, Flax JD, et al. Transplantation of neural
progenitor and stem cells: developmental insights may
ARTICLE IN PRESSM. Brodhun et al. / Experimental and Toxicologic Pathology 56 (2004) 103–112112
suggest new therapies for spinal cord and other CNS
dysfunction. J Neurotrauma 1999;16:675–87.
Park KI, Ourednik J, Ourednik V, et al. Global gene and cell
replacement strategies via stem cells. Gene Ther 2002;9:
613–24.
Patt S, Brodhun M. Neuropathological sequelae of traumatic
injury in the brain. An overview. Exp Toxicol Pathol 1999;
51:119–23.
Pereira RF, Halford KW, O0Hara MD, et al. Cultured
adherent cells from marrow can serve as long-lasting
precursor cells for bone, cartilage, and lung in irradiated
mice. Proc Nat Acad USA 1995;92:4857–61.
Philips MF, Mattiasson G, Wieloch T, et al. Neuroprotective
and behavioral efficacy of nerve growth factor-transfected
hippocampal progenitor cell transplants after experimental
traumatic brain injury. J Neurosur 2001;94:765–74.
Pittenger MF, Mackay AM, Beck SC, et al. Multilineage
potential of adult human mesenchymal stem cells. Science
1999;284:143–7.
Povlishock JT, Christman CW. The pathobiology of trauma-
tically induced axonal injury in animals and humans: a
review of current thoughts. J Neurotrauma 1995;12:
555–64.
Prestoz L, Relvas JB, Hopkins K, et al. Association between
integrin-dependent migration capacity of neural stem cells
in vitro and anatomical repair following transplantation.
Mol Cell Neurosci 2001;18:473–84.
Rathjen J, Haines BP, Hudson KM, et al. Directed differ-
entiation of pluripotent cells to neural lineages: homo-
geneous formation and differentiation of a neurectoderm
population. Development 2002;129:2649–61.
Reubinoff BE, Itsykson P, Turetsky T, et al. Neural
progenitors from human embryonic stem cells. Nat
Biotechnol 2001;19:1134–40.
Riess P, Zhang C, Saatman KE, et al. Transplanted neural
stem cells survive, differentiate, and improve neurological
motor function after experimental traumatic brain injury.
Neurosurgery 2002;51:1043–52.
Romero-Ramos M, Vourc’h P, Young HE, et al. Neuronal
differentiation of stem cells isolated from adult muscle.
J Neurosci Res 2002;15:3999–4002.
Savitz SI, Rosenbaum DM, Dinsmore JH, et al. Cell
transplantation for stroke. Ann Neurol 2002;52:266–75.
Seri B, Garcia-Verdugo JM, McEwen BS, et al. Astrocytes give
rise to new neurons in the adult mammalian hippocampus.
J Neurosci 2001;21:7153–60.
Senior K. Embryonic stem cells used to remyelinate injured rat
spinal cord neurons. Lancet 2000;355:1890.
Sharp FR, Liu J, Bernabeu R. Neurogenesis following brain
ischemia. Brain Res Dev Brain Res 2002;31:23–30.
Song HJ, Stevens CF, Gage FH. Neural stem cells from adult
hippocampus develop essential properties of functional
CNS neurons. Nat Neurosci 2002;5:438–45.
Svendsen CN, Clarke DJ, Rosser AE, et al. Survival and
differentiation of rat and human epidermal growth factor-
responsive precursor cells following grafting into the
lesioned adult central nervous system. Exp Neurol 1996;
137:376–88.
Tamaki S, Eckert K, He D, Sutton R, et al. Engraftment of
sorted/expanded human central nervous system stem cells
from fetal brain. J Neurosci Res 2002;69:976–86.
Tanapat P, Hastings NB, Reeves AJ, et al. Estrogen stimulates
a transient increase in the number of new neurons in the
dentate gyrus of the adult female rat. J Neurosci 1999;
19:5792–801.
Tanapat P, Hastings NB, Rydel TA, et al. Exposure to fox
odor inhibits cell proliferation in the hippocampus of
adult rats via an adrenal hormone-dependent mechanism.
J Comp Neurol 2001;437:496–504.
Tate MC, Shear DA, Hoffman SW, et al. Fibronectin
promotes survival and migration of primary neural stem
cells transplanted into the traumatically injured mouse
brain. Cell Transplant 2002;11:283–95.
Tatton WG, Chalmers-Redman RM, Ju WY, et al. Apoptosis
in neurodegenerative disorders: potential for therapy by
modifying gene transcription. J Neural Transm Suppl
1997;49:245–68.
Terskikh A, Lukyanov S, Diatchenko S, et al. Hunting
hematopoietic stem cell-specific genes using PCR-select
cDNA subtraction CLONTECHniques 2000; 1: 33–34.
Till JE, McCulloch EA, Siminovitch L. A stochastic model of
stem cell proliferation, based on the growth of spleen
colony-forming cells. Proc Natl Acad Sci USA
1964;51:29–36.
Uchida N, Buck DW, He D, Reitsma MJ, Masek M, Phan TV,
Tsukamoto AS, Gage FH, Weissman IL. Direct isolation of
human central nervous system stem cells. Proc Natl Acad
Sci USA 2000;97:14720–5.
van der Kooy D, Weiss S. Why stem cells? Science
2000;287:1439–41.
van Praag H, Schinder AF, Christie BR, et al. Functional
neurogenesis in the adult hippocampus. Nature 2002;417:
1030–4.
Vescovi AL, Gritti A, Galli R, et al. Isolation and intracerebral
grafting of nontransformed multipotential embryonic hu-
man CNS stem cells. J Neurotrauma 1999;16:689–93.
Wagers AJ, Sherwood RI, Christensen JL, et al. Little evidence
for developmental plasticity of adult hematopoietic stem
cells. Science 2002;297:2256–9.
Wang KC, Koprivica V, Kim JA, et al. Oligodendrocyte-
myelin glycoprotein is a Nogo receptor ligand that inhibits
neurite outgrowth. Nature 2002;417:941–4.
Weissman IL. Stem cells: units of development, units of
regeneration, and units in evolution. Cell 2000;100:157–68.
Whittemore SR. Neuronal replacement strategies for spinal
cord injury. J Neurotrauma 1999;16:667–73.
Woodbury D, Schwarz EJ, Prokop DJ, et al. Adult rat and
human bone marrow stromal cells differentiate into
neurons. J Neurosci Res 2000;61:364–70.
Zauner A, Bullock R. The role of excitatory amino acids in
severe brain trauma: opportunities for therapy: a review.
J Neurotrauma 1995;12:547–54.
Zhao LR, Duan WM, Reyes M, et al. Human bone marrow
stem cells exhibit neuronal phenotypes and ameliorate
neurological deficits after grafting into ischemic brain of
rats. Exp Neurol 2002;174:11–20.