Embed Size (px)
Citation preview

Postural Tachycardia Syndrome (POTS) – What? Why? How?
Satish R Raj MD MSCI FACC FHRS FRCPC Associate Professor of Cardiac Sciences University of Calgary Adjunct Associate Professor of Medicine Autonomic Dysfunction Center Vanderbilt University School of Medicine October 2014

Case Presentation - AP n ONSET
q Age 26 years; SWF; works in music industry q Dx “Pneumonia” -> inhalers q Developed “spells of tachycardia” q Cardiologist #1 proposed EP Study/Ablation q Cardiologist #2 -> Tilt Test q Associated Symptoms
n Lightheaded/presyncope (standing) n Intermittent stabbing chest pains (standing) n Mental clouding (“brain fog”) n Severe fatigue
SR Raj, Circulation 2013

Case Presentation – AP (2)
Position HR (bpm) BP (mmHg) Supine – 15 min 73 103/72 Upright – 1 min 106 109/80 Upright – 3 min 105 106/83 Upright – 5 min 122 118/75
Upright – 10 min 121 118/78
Orthostatic Challenge

WHAT is POTS?

Postural Tachycardia Syndrome - Common Criteria
n Orthostatic tachycardia > 30 bpm q >40 bpm required if <18 years
n No consistent orthostatic hypotension q ΔBP > 20/10 mmHg
n Symptoms of sympathetic activation q Worse upright; better recumbent
n Chronic symptoms > 6 months
Phillip Low MD Mayo Clinic

POTS - Mimics & Associations n Mimics
q Acute infections q Multiple sclerosis q Sjogren’s syndrome
n Associations q Joint Hypermobility Syndrome
n Ehlers Danlos Syndrome – Hypermobility q Fibromyalgia q Chronic Fatigue Syndrome

POTS - Common Symptoms
n Rapid Heartbeat n Chest Discomfort n Short of Breath n Lightheaded
n Exercise Intolerance
n Mental Clouding n Headache n Nausea n Tremulousness
n Fatigue n Sleep Complaints
Cardiac Non-Cardiac

POTS Control Heart Rate (bpm)
Blood Pressure (mmHg)
Tilt Angle (deg)
200
200 0
50
60
0
Tilt Testing
SR Raj, Indian Pacing Electrophysiol J. 2006;6:84-99

POTS: Feel awful when upright
0 10 20 30
05
101520253035
POTSControl
Tilt (60°) Time
Sym
ptom
s S
core
(au
)
SR Raj & RS Sheldon, Tilt Table Testing in S Saksena & AJ Camm Electrophysiological Disorders of the Heart 2nd Ed. (2011)

POTS – Who is affected?
n Prevalence ½ million in USA n Female (~80-85%) n Typically aged 13-50 years
n Significant functional disability

Quality of Life in POTS
Kanika Bagai

Health Related Quality of Life (SF-36) – Chronic Illnesses
Physical Mental0
25
50
75
100 Back PainESRD
SF36 Sub-Scores
Scor
eDialysis

Health Related Quality of Life (SF-36) – Chronic Illnesses
Physical Mental0
25
50
75
100
POTSBack PainESRD
SF36 Sub-Scores
Scor
e
Modified from K Bagai et al., J Clin Sleep Med 2011
Dialysis

Sleep Problems Correlate with Poor HRQL
HealthyPOTS
0 25 50 75 100MOS Sleep Problems Index
10
20
30
40
50
60
70
SF36
Phy
sica
l
R-Square = 0.62
HealthyPOTS
0 25 50 75 100MOS Sleep Problems Index
10
20
30
40
50
60
SF36
Men
tal
R-Square = 0.60
Physical Mental
R2=0.62 R2=0.60
Modified from K Bagai et al., J Clin Sleep Med 2011

WHY do they have POTS?
… ‘final common pathway’ of hundreds of genetic and acquired autonomic and cardiovascular entities
- David Robertson
David Robertson

Pathophysiology of POTS – The Challenge

Blind men and the Elephant n It was six men of Hindustan
To learning much inclined, Who went to see the Elephant (Though all of them were blind), That each by observation Might satisfy his mind
n They conclude that the elephant is like a wall, snake, spear, tree, fan or rope, depending upon where they touch.
Ancient Hindu Parable retold by John Godfrey Saxe (1816–1887)

Pathophysiology of POTS
Satish

POTS - Pathophysiologies
n Mast Cell Activation n Partial Autonomic Neuropathy n Leg Blood Flow Abnormalities n Hypovolemia n Hyperadrenergic
q Increased Release q Decreased Clearance
n Antibodies are Evil…

POTS and Mast Cells
n Spot (4 hour) urine collection n If syncopal/flushing attack, 1-2 hour urine
collection n Mast cell activation disorder n Often aspirin sensitivity n Therapy:
q H1 + H2 blockade q ASA q Alpha-methyldopa Italo Biaggioni
C Shibao et al., Hypertension 2005

Neuropathic POTS
Normal nPOTS Giris Jacob
§ Reduced NE Spillover in legs
§ Abnormal sweat test (QSART) in legs
G Jacob et al., N Engl J Med. 2000;343:1008-14

Leg Blood Flow May Identify Different Subpopulations of POTS
Julian Stewart
Stewart J M et al. AJP Heart Circ Physiol 2003;285:H2749-H2756

Blood Volume & Renin-Angiotensin-Aldosterone System in POTS

Plasma Volume is Low in POTS
Adapted from SR Raj et al., Circulation 2005;111:1574-1582
Control POTS
-25-20-15-10-505
1015
P<0.001
PV D
evia
tion
(%)

Plasma Renin Activity & Aldosterone are inappropriately low in POTS…when one would expect them elevated
Supine Standing0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5 P=0.941P=0.996POTS Control
Ren
in ((
ng/m
l)/hr
)
Supine Standing0
250
500
750
1000POTS Control
Ald
oste
rone
(pM
)
P=0.019P=0.017
Adapted from SR Raj et al., Circulation 2005;111:1574-1582

RAAS Schema in POTS
AGT ANG I ANG II Aldo
Blood Volume
PRA ACE
ANG (1-7) ACE2
Adapted from HI Mustafa et al., Heart Rhythm. 2011;8:422-8.

Conclusions – RAAS in POTS n Things are screwy n Unusual RAAS profile in POTS
q Low blood volume q Low plasma renin activity q Low aldosterone
n More work is needed to understand physiology q Decreased ACE2 activity? q Elevated ANG II due to less degradation? q Why are aldosterone levels low?
n Can the kidney not hold onto sodium in POTS? q May explain the need for high sodium diets and low
blood volume in POTS.

Hyperadrenergic POTS – Increased SNS Nerve Firing
Normal hPOTS

Hyperadrenergic POTS – Decreased NE Clearance

A Norepinephrine Synapse
NET
Slide courtesy of Alex Nackenoff
(Vanderbilt)

A Norepinephrine Synapse
NET
Slide courtesy of Alex Nackenoff
(Vanderbilt)
SNS Tone

Shannon JR, NEJM 2000; 342:541-9.
.
P
P P P
P
S-S
P
V69I
T99I
V245IV449I
G478SA457PN292T
V356L
A369P N375S
K463R
F528C
Y548H

Reaction at Vanderbilt
n Excitement
n The cause of POTS has been found!!!

POTS Patients with NET mutations: 2000-2010
n n n n
No other patients had this mutation. We had just about given up hope in NET defects as a cause of POTS…

Variable Expression of NET Protein in POTS
Courtesy of Murray Esler, Baker IDI (Melbourne, Australia)

Lambert E et al. Circ Arrhythm Electrophysiol 2008;1:103-109
Decreased NET Protein Expression in some POTS Patients

Role of Antibodies in POTS
1. AChR Antibody 2. Adrenergic Antibodies

Ganglionic Acetylcholine Receptor Ab n Discovered at Mayo Clinic
q Steve Vernino & Vanda Lennon
n Loss of function Ab at Autonomic Ganglia
n Prevalence in POTS q Mayo: ~7-14% of POTS patients
n Now reportedly lower per Dr. P Low (Mayo)
q Vanderbilt: 0% of POTS patients
n Presentation is usually Autonomic Failure q Orthostatic hypotension q Constipation, pupil findings
Schroeder C et al. NEJM 2005;353:1585-1590

POTS Patient serum stimulates adrenergic receptors
H Li et al., JAHA 2014; 3(1):e000755.

Beta-receptor activation from POTS sera β2
-AR
med
iate
d
cAM
P re
leas
e β1
-AR
med
iate
d
cAM
P re
leas
e
H Li et al., JAHA 2014; 3(1):e000755.

The Model
How could the Ab contribute to the POTS phenotype?
H Li et al., JAHA 2014; 3(1):e000755.

POTS – HOW to Manage?
Investigation & Treatment

POTS: Investigations
n History & Physical Examination n Orthostatic Vital Signs n CBC, BMP n Autonomic Reflex Testing n Echocardiogram n Blood Volume Assessment n Exercise Capacity Assessment

POTS: Treatment Approaches n Exercise n Increase Blood Volume
q Oral Water q Increase Salt (diet vs. tablets) q Fludrocortisone q Octreotide q IV Saline q Acute DDAVP-H2O
n Hemodynamic Agents q Midodrine q Propranolol q Pyridostigmine q Ivabradine (emerging)
n Behavioral Therapies

Exercise in POTS
n Historically q “good thing to do” q Many patients could not/would not
n excessive fatigue (~days) and intolerance q Anecdotally, those patients that did exercise
did better over time n Cause/effect vs. selection bias
n Now q Recent data on effects of exercise training in
POTS from Dallas, Vienna, & Mayo…

Exercise Study in POTS - Design
Screening
Blood Volume Measurement
Maximal Exercise Test
45-min 60° Upright Tilt
Cardiac MRI
Maximal Exercise Test
45-min 60° Upright Tilt
Blood Volume Measurement
Cardiac MRI
3 months of exercise training

Exercise in POTS - Benefits
n Short-term exercise training in POTS q Increases fitness levels q Increases blood volume q Cardiac Remodeling q Normalizes Sympathetic Activity q Decreases Orthostatic Tachycardia
Qi Fu et al., JACC 2010;55:2858-68

Exercise in POTS – How To? n Focus on Aerobic Activity
q Some resistance training focused on thighs n Must be Regular
q Every other day (4/week) n 30min/session -> 45-60min/session n NO UPRIGHT EXERCISES
q Rowing machines q Recumbent Cycles q Swimming
n Takes 4-5 weeks to start seeing benefits Qi Fu et al., JACC 2010;55:2858-68

POTS: Treatment Approaches n Exercise n Increase Blood Volume
q Oral Water q Increase Salt (diet vs. tablets) q Fludrocortisone q Octreotide q IV Saline q Acute DDAVP-H2O
n Hemodynamic Agents q Midodrine q Propranolol q Pyridostigmine q Ivabradine (emerging)
n Behavioral Therapies

G Jacob et al. Circulation 1997;96:575-580
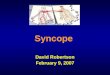
IV Saline (1L) Acutely Decreases Orthostatic Tachycardia…a LOT!!

DDAVP+H2O reduces standing HR
Pre 1H 2H 3H 4H859095
100105110115120125 DDAVP+H2O Placebo
PTime=0.001
PDrug=0.001
PINT =0.001
Time Post Dose
Hea
rt R
ate
(bpm
)
ST Coffin et al., Heart Rhythm. 2012;9:1484-90

POTS: Treatment Approaches n Exercise n Increase Blood Volume
q Oral Water q Increase Salt (diet vs. tablets) q Fludrocortisone q Octreotide q IV Saline q Acute DDAVP-H2O
n Hemodynamic Agents q Midodrine q Propranolol q Pyridostigmine q Ivabradine (emerging)
n Behavioral Therapies

Jacob, G. et al. Circulation 1997;96:575-580
Midodrine Decreases Orthostatic Tachycardia…a little bit.

Beta-Blockers in POTS
n PRO q Intuitively appealing
n High HR -> Lower it
n CON q Stewart et al. studied IV esmolol and found
that it DID NOT improve orthostatic tolerance q Many patients report “intolerance to beta-
blockers”

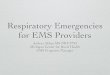
Pre 1H 2H 3H 4H70
80
90
100
110
120
130 Propranolol Placebo
PDrug <0.001PInt <0.001
Time Post Dose
Hea
rt R
ate
(bpm
)Propranolol 20mg lowers Orthostatic Tachycardia
Pre 1H 2H 3H 4H0
10
20
30
40 Propranolol Placebo
PDrug <0.001
Time Post Dose
Cha
nge
in H
eart
Rat
e (b
pm)
Standing HR Orthostatic Increase in HR
SR Raj et al. Circulation 2009;120:725-734

Symptoms
Pre 2H 4H12
14
16
18
20
22
24
26 Propranolol Placebo
PInt =0.04
Time Post Dose
Sym
ptom
s (a
.u.)
Propranolol Improves Symptoms…
SR Raj et al. Circulation 2009;120:725-734

Propranolol 20mg Propranolol 80mg
-15
-10
-5
0
P =0.041Wilcoxon
Δ S
ympt
oms
Scor
e (a
.u.)
…but Less is More
SR Raj et al. Circulation 2009;120:725-734

Acetylcholinesterase Inhibition
n Pyridostigmine q Peripheral AChEI q Increases availability of synaptic ACh q Ganglionic Nicotinic Receptor
n ↑ SNS & ↑ PNS q Postganglionic Muscarinic Receptor
n ↑ PNS
n Might decrease tachycardia in POTS

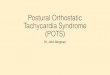
Pre 2H 4H9095
100105110115120125130135 Pyridostigmine Placebo
P=0.001 P=0.160
P<0.001
P<0.001
Time Post Dose
Hea
rt R
ate
(bpm
)Acetylcholinesterase Inhibition
Standing Heart Rate Symptoms
SR Raj et al., Circulation 2005;111:2734-2740
Pyridostigmine Placebo
-15
-10
-5
0
5
P=0.025
Cha
nge
in S
ympt
om S
core
(au)

Norepinephrine Transporter Inhibition
Standing
Pre 1H 2H 3H 4H90
100
110
120
130 Atomoxetine Placebo
PInt <0.001
A
Time Post Dose
Hea
rt R
ate
(bpm
)
EA Green et al., JAHA 2013;2:e000395
Seated
Pre 1H 2H 3H 4H70
75
80
85
90
95
100
PInt =0.029
B
PlaceboAtomoxetine
Time Post Dose
Hea
rt R
ate
(bpm
)

Norepinephrine Transporter Inhibition
Orthostatic Change
Pre 1H 2H 3H 4H15
20
25
30
35
40 Atomoxetine Placebo
PInt =0.001
C
Time Post Dose
Δ H
eart
Rat
e (b
pm)
Symptoms: 0 to 2h
Atomoxetine Placebo
-8
-6
-4
-2
0
2
4
6
P =0.028Δ
Sym
ptom
s Sc
ore
(a.u
.)
EA Green et al., JAHA 2013;2:e000395

POTS: Treatment Approaches n Exercise n Increase Blood Volume
q Oral Water q Increase Salt (diet vs. tablets) q Fludrocortisone q Octreotide q IV Saline q Acute DDAVP-H2O
n Hemodynamic Agents q Midodrine q Propranolol q Pyridostigmine q Ivabradine (emerging)
n Behavioral Therapies

What Type of POTS Do I Have?
Challenges: 1. Overlapping Subsets 2. Lost in Translation

Hyperadrenergic POTS Neuropathic POTS
Hypovolemic POTS
What Type of POTS Do I Have?

Hyperadrenergic POTS Neuropathic POTS
Hypovolemic POTS
What Type of POTS Do I Have?

Lost in Translation
Not my M-I-L

Prognosis of POTS
“Prediction is very difficult, especially about the future.” Niels Bohr (1885-1962); Nobel Prize (Physics) 1922

POTS – Take Home Messages n POTS
q chronic disorder associated with significant disability
q Syndrome…not one disease n Multiple pathophysiologies
n Treatment q Exercise q Volume expansion q Heart rate control q Manage the “living with a chronic illness”

Questions?