Embed Size (px)
Citation preview

Postural CareGentle Respectful Effective
Sarah Clayton, Postural Care CIC2nd April 2014

How to participate today

Sarah Clayton
Sarah Clayton – Sarah started working with families whose children were using nighttime positioning in 1998, this work was published in Physiotherapy in 2000. In 2004 she co-wrote the accredited Postural Care courses using her skills as a fully qualified teacher. In September 2007 Sarah’s oldest daughter Abigail was diagnosed with a malignant brain tumour aged just 6, she has undergone extensive treatment. Abi is currently in remission and continues to do well although her future is by no means certain.

The Principles of Postural Care
There are 24hours in a day
Out of 8,760 hours of the year, a person with movement problems will spend
approximately:-
1,140 hours in school, this will be slightly longer if you are at work
7,620 with their family and supporters 3,640 in bed

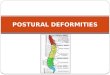
Patterns of Distortion of the Legs
• the knees together • the knees out to the side • A “windswept” position, with both
knees to one side
Once the hips and knees lose the ability to straighten fully the legs will adopt an avoidable position with either:-




Protecting the hips….
There is a lot of information about protecting hips at
www.hipdysplasia.org

The hip joint is formed by the head of the femur (thigh bone) and the acetabulum (part of the pelvis).

When the hips are strong the they are held tightly together by tight ligaments….
If we don’t support the weight of a persons legs these ligaments become loose and the hips are at
risk of dislocation…

The evidence demonstrates that position is both a cause of distortion and the key to developing the hips in the first few months of life
“Cultures that hold infants with the hips apart have very low rates of hip dysplasia”
“Cultures that keep infants’ hips extended on a cradleboard or papoose board have high rates of hip dysplasia in their children”
International Hip Dysplasia Institute

For children and adults with movement difficulties the hips may be subject to ongoing destructive forces and damage

X ray shows how much the ligaments have stretched and how the head of the femur is coming
out of the acetabulum
this is called the “Percentage Migration”
33% is called subluxed …..75% is dislocated
Scrutton D , Baird G Arch Dis Child 1997;76:381-384

The direction of dislocation will depend on the position the person lies in as a habit

The direction of dislocation will depend on the position the person lies in as a habit

or anteriorly(to the front)
posteriorly (to the back)

In Wakefield, UK hip dislocations have been dramatically reduced…
GMFCS Gross Motor Function Classification Scale
1 Children who can walk, run, jump and climb stairs but who have some impairment of speed, balance and/or coordination
2 Children who can walk in and outdoors and climb stairs but have some difficulties with such things as uneven ground or crowds 3 Children who use walking aids but use wheelchairs for long distances
4 Children who use walking aids for short distances but use wheelchairs most of the time 5 Children who use wheelchairs for all mobility and need postural support in order to be able to sit comfortably
Number of children supported by the service
75% Migration over 75% of femoral head uncovered by acetabulum
Wakefield 122 106 46 274 0Pontefract 48 79 50 177 2

(CIPOLD 2013) Recommendation 9:-
“CCGs must ensure they are commissioning sufficient and sufficiently expert, preventative services for people with learning disabilities regarding their high risk of respiratory illness.
This would include expert, proactive postural care support”

Some people may need support to correct established problems such as chest rotation

De-rotating the Chest



The answer does not lie in equipment.
The answer lies in the development of co-
produced, asset based, problem solving, creative solutions that have a clear person-centred outcome

Michael’s StoryAge 29
Age 34

Coleen’s StoryAge 19
Age 22

Postural Care Pathway – “It’s My Life!”
Available to download at:
https://www.dropbox.com/s/d9nvb08e5d6gvx9/It%27s%20My
%20Life%202014.pdf

“Unless someone like you
cares a whole awful lot,
nothing is going to get better.
It's not.”
Dr Seuss, The Lorax

Any questions?

Further information and contact details
www.in-control.org.uk/webinarschedule2014
www.in-control.org.uk/stayconnected