Embed Size (px)
Citation preview

PostScript..............................................................................................
LETTERS
Conjunctival changes associatedwith yellow nail syndromeThe yellow nail syndrome (YNS) is a rareclinical entity characterised by slow growingyellow discoloured nails in association withperipheral lymphoedema, pulmonary mani-festation (bronchiectasis, pleural effusions),and chronic sinusitis.1 About 100 cases of YNShave been described in the literature but it hasnever been associated with ocularmanifestations.2 We report one patient withYNS in whom chronic chemosis and conjunc-tival degenerative lesion was observed.
Case reportA 61 year old man was referred with a 2month history of ocular irritation in the lefteye. His past medical history was significativefor yellowish slow growing nails, chronicmaxillary sinusitis, and bronchiectasis for 5years diagnosed as YNS. On examination,nails of both hands and feet showed yellowdiscoloration and thickening (Fig 1). He alsohad oedema over the lower limbs andsubacute bronchial infection for 2 months. Onocular examination, corrected visual acuitywas 20/20 in both eyes. Slit lamp examinationof the left eye revealed an area of conjunctivalinjection and thickening in the palpebralfissure adjacent to nasal limbus. A mild nasalchemosis and superficial corneal micropan-nus were also observed (Fig 2 top). Tear secre-tion was normal. Examination of the anterior
and posterior segment in both eyes was unre-markable. Treatment with topical cortico-steroid (dexamethasone 0.1%, four times perday) and artificial tears was begun. Two weeksafter presentation the patient reported anincomplete resolution of the irritation on theleft eye and conjunctival lesion persisted.Computed tomographic scan of the brain andthe orbits was normal. A conjunctival biopsyspecimen showed multilayered epithelium,nuclear pleomorphism with malpighian dif-ferentiation. The underlying connective tissuewas normal (Fig 2 bottom). Ocular symptomsimproved rapidly and postoperative antibioticand steroid eye drops where discontinuedafter 2 weeks. There was no recurrence of theconjunctival lesion but a mild chemosispersist in the left eye and appeared in theright eye.
CommentYNS was first described by Samman andWhite in 1964.1 The syndrome has been
defined as the complete triad of slow growingyellow nails, lymphoedema, and pleural effu-sions but today it is accepted that the presenceof two of the three symptoms is sufficient toestablish the diagnosis, even though theabnormalities may appear separately withintervals of several years.2
The aetiology of YNS is obscure, whilepathogenesis seems to involve impaired lym-phatic drainage.3 Ocular involvement hasnever been described in the YNS. However,conjunctival chemosis observed in our patientcould be related to YNS which may involve thepleura, the lungs, but also other serosal ormucosal membranes such as the conjunctiva.Moreover, ocular symptoms and corneal mi-cropannus appeared at the same time of a riseof pulmonary symptoms. An inflammatorycomponent, which could alter blood flow andcapillary permeability, has not been excludedand, interestingly, topical dexamethasoneused to treat chemosis is efficient.
There is very little information on his-topathological findings observed in the YNS.Nail biopsies demonstrated features of matu-ration disarray in the nail bed epitheliumassociated with dense, fibrous tissue replacingsubungual stroma.4 The changes that weobserved in the conjunctival epithelium aresimilar to that in the nail bed in YNS.
Since it appears that there is a pathogenicassociation between the YNS and ocular find-ings, this association is probably not coinci-dental and could be the first report of ocularmanifestation of YNS.
T Bourcier, M Baudrimont, V Borderie,C Mayaud, L Laroche
Quinze-Vingts National Center of Ophthalmologyand Department of Pneumology, Tenon Hospital,
Paris, France
Correspondence to: Tristan Bourcier, MD, PhD,Service du Professeur Laroche, CHNO des
Quinze-Vingts, 28 rue de Charenton 75012 Paris,France; [email protected]
Accepted for publication 28 January 2002
References1 Samman PD, White WF. The “yellow nail
syndrome.” Br J Dermatol 1964;76:153–7.2 Hershko A, Hirshberg B, Nahir M, et al.
Yellow nail syndrome. Postgrad Med J1997;73:466–8.
3 Bull RH, Fenton DA, Mortimer PS. Lymphaticfunction in the yellow nail syndrome. Br JDermatol 1996;134:307–12.
4 DeCoste SD, Imber MJ, Baden HP. Yellownail syndrome. J Am Acad Dermatol1990;22:608–11.
Bilateral anterior uveitis as apresenting manifestation ofsarcoidosis and syphilisWe report an unusual case of bilateral acuteanterior uveitis in an asymptomatic patient inwhich ophthalmic examination and labora-tory tests showed the diagnosis of syphilis andsarcoidosis.
Case reportA previously healthy 34 year old Hispanicwoman with a 2 week history of blurredvision was referred for evaluation. The patienthad no systemic complaints. On examinationher best corrected visual acuity was 20/30 in
If you have a burning desire to respond toa paper published in the BJO, why notmake use of our “rapid response” option?
Log on to our website(www.bjophthalmol.com), find the paperthat interests you, and send your responsevia email by clicking on the “eLetters”option in the box at the top right handcorner.
Providing it isn’t libellous or obscene, itwill be posted within seven days. You canretrieve it by clicking on “read eLetters”on our homepage.
The editors will decide as beforewhether to also publish it in a futurepaper issue.
Figure 1 Yellow nail syndrome. Noteyellow discoloration, increased curvature,and thickening of the nail plates infingernails.
Figure 2 Anterior segment photograph ofthe left eye, showing conjunctival injection,conjunctiva thickening, and micropannusadjacent to nasal limbus. A mild nasalchemosis was also observed (top).Photomicrograph of conjunctival biopsy. Thelesion shows multilayered epithelium, nuclearpleomorphism with malpighiandifferentiation. The underlying connectivetissue was normal (haematoxylin-eosin-safran,magnification ×300) (bottom).
Br J Ophthalmol 2002;86:930–943930
www.bjophthalmol.com
on 15 July 2018 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.86.8.930-a on 1 August 2002. D
ownloaded from
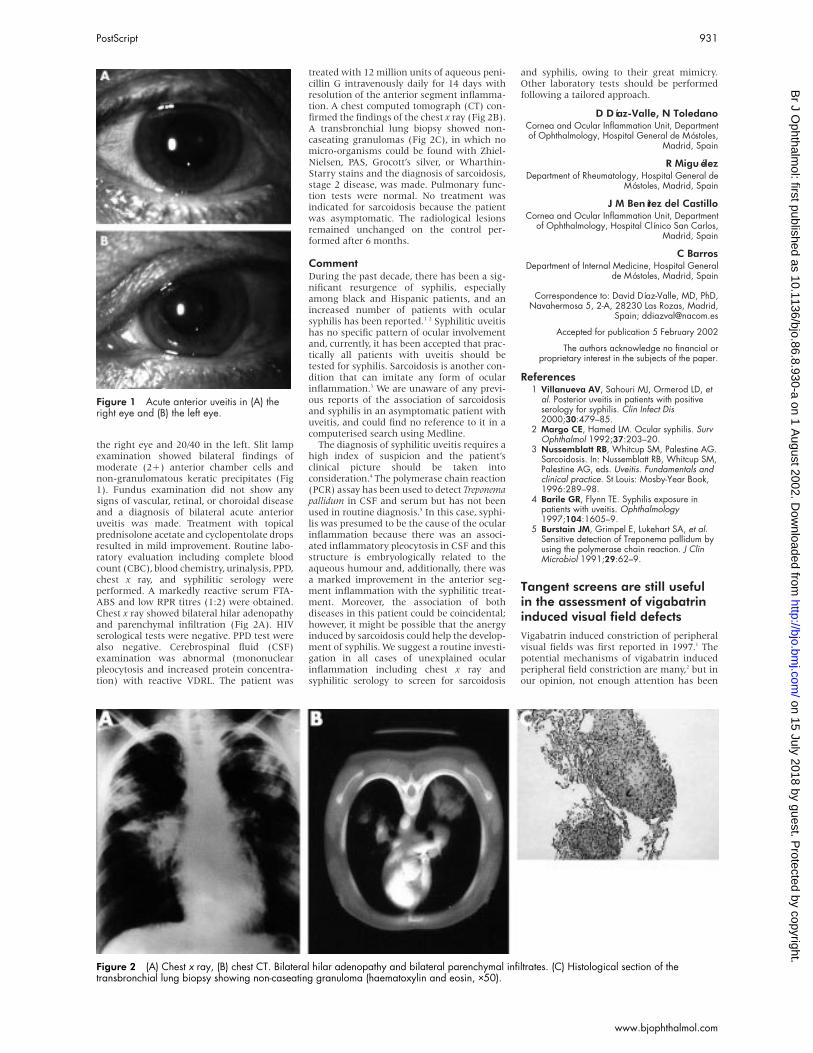
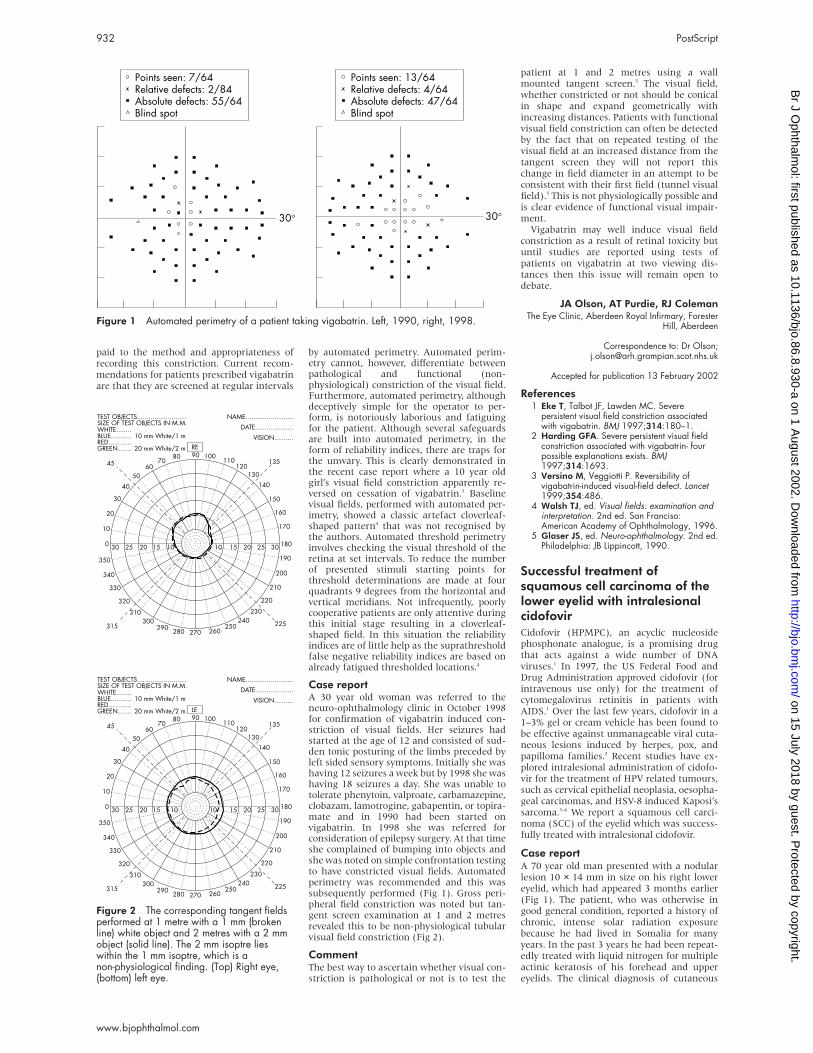
the right eye and 20/40 in the left. Slit lampexamination showed bilateral findings ofmoderate (2+) anterior chamber cells andnon-granulomatous keratic precipitates (Fig1). Fundus examination did not show anysigns of vascular, retinal, or choroidal diseaseand a diagnosis of bilateral acute anterioruveitis was made. Treatment with topicalprednisolone acetate and cyclopentolate dropsresulted in mild improvement. Routine labo-ratory evaluation including complete bloodcount (CBC), blood chemistry, urinalysis, PPD,chest x ray, and syphilitic serology wereperformed. A markedly reactive serum FTA-ABS and low RPR titres (1:2) were obtained.Chest x ray showed bilateral hilar adenopathyand parenchymal infiltration (Fig 2A). HIVserological tests were negative. PPD test werealso negative. Cerebrospinal fluid (CSF)examination was abnormal (mononuclearpleocytosis and increased protein concentra-tion) with reactive VDRL. The patient was
treated with 12 million units of aqueous peni-cillin G intravenously daily for 14 days withresolution of the anterior segment inflamma-tion. A chest computed tomograph (CT) con-firmed the findings of the chest x ray (Fig 2B).A transbronchial lung biopsy showed non-caseating granulomas (Fig 2C), in which nomicro-organisms could be found with Zhiel-Nielsen, PAS, Grocott’s silver, or Wharthin-Starry stains and the diagnosis of sarcoidosis,stage 2 disease, was made. Pulmonary func-tion tests were normal. No treatment wasindicated for sarcoidosis because the patientwas asymptomatic. The radiological lesionsremained unchanged on the control per-formed after 6 months.
CommentDuring the past decade, there has been a sig-nificant resurgence of syphilis, especiallyamong black and Hispanic patients, and anincreased number of patients with ocularsyphilis has been reported.1 2 Syphilitic uveitishas no specific pattern of ocular involvementand, currently, it has been accepted that prac-tically all patients with uveitis should betested for syphilis. Sarcoidosis is another con-dition that can imitate any form of ocularinflammation.3 We are unaware of any previ-ous reports of the association of sarcoidosisand syphilis in an asymptomatic patient withuveitis, and could find no reference to it in acomputerised search using Medline.
The diagnosis of syphilitic uveitis requires ahigh index of suspicion and the patient’sclinical picture should be taken intoconsideration.4 The polymerase chain reaction(PCR) assay has been used to detect Treponemapallidum in CSF and serum but has not beenused in routine diagnosis.5 In this case, syphi-lis was presumed to be the cause of the ocularinflammation because there was an associ-ated inflammatory pleocytosis in CSF and thisstructure is embryologically related to theaqueous humour and, additionally, there wasa marked improvement in the anterior seg-ment inflammation with the syphilitic treat-ment. Moreover, the association of bothdiseases in this patient could be coincidental;however, it might be possible that the anergyinduced by sarcoidosis could help the develop-ment of syphilis. We suggest a routine investi-gation in all cases of unexplained ocularinflammation including chest x ray andsyphilitic serology to screen for sarcoidosis
and syphilis, owing to their great mimicry.Other laboratory tests should be performedfollowing a tailored approach.
D Díaz-Valle, N ToledanoCornea and Ocular Inflammation Unit, Departmentof Ophthalmology, Hospital General de Móstoles,
Madrid, Spain
R MiguélezDepartment of Rheumatology, Hospital General de
Móstoles, Madrid, Spain
J M Benítez del CastilloCornea and Ocular Inflammation Unit, Department
of Ophthalmology, Hospital Clínico San Carlos,Madrid, Spain
C BarrosDepartment of Internal Medicine, Hospital General
de Móstoles, Madrid, Spain
Correspondence to: David Díaz-Valle, MD, PhD,Navahermosa 5, 2-A, 28230 Las Rozas, Madrid,
Spain; [email protected]
Accepted for publication 5 February 2002
The authors acknowledge no financial orproprietary interest in the subjects of the paper.
References1 Villanueva AV, Sahouri MJ, Ormerod LD, et
al. Posterior uveitis in patients with positiveserology for syphilis. Clin Infect Dis2000;30:479–85.
2 Margo CE, Hamed LM. Ocular syphilis. SurvOphthalmol 1992;37:203–20.
3 Nussemblatt RB, Whitcup SM, Palestine AG.Sarcoidosis. In: Nussemblatt RB, Whitcup SM,Palestine AG, eds. Uveitis. Fundamentals andclinical practice. St Louis: Mosby-Year Book,1996:289–98.
4 Barile GR, Flynn TE. Syphilis exposure inpatients with uveitis. Ophthalmology1997;104:1605–9.
5 Burstain JM, Grimpel E, Lukehart SA, et al.Sensitive detection of Treponema pallidum byusing the polymerase chain reaction. J ClinMicrobiol 1991;29:62–9.
Tangent screens are still usefulin the assessment of vigabatrininduced visual field defectsVigabatrin induced constriction of peripheralvisual fields was first reported in 1997.1 Thepotential mechanisms of vigabatrin inducedperipheral field constriction are many,2 but inour opinion, not enough attention has been
Figure 1 Acute anterior uveitis in (A) theright eye and (B) the left eye.
Figure 2 (A) Chest x ray, (B) chest CT. Bilateral hilar adenopathy and bilateral parenchymal infiltrates. (C) Histological section of thetransbronchial lung biopsy showing non-caseating granuloma (haematoxylin and eosin, ×50).
PostScript 931
www.bjophthalmol.com
on 15 July 2018 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.86.8.930-a on 1 August 2002. D
ownloaded from
paid to the method and appropriateness ofrecording this constriction. Current recom-mendations for patients prescribed vigabatrinare that they are screened at regular intervals
by automated perimetry. Automated perim-etry cannot, however, differentiate betweenpathological and functional (non-physiological) constriction of the visual field.Furthermore, automated perimetry, althoughdeceptively simple for the operator to per-form, is notoriously laborious and fatiguingfor the patient. Although several safeguardsare built into automated perimetry, in theform of reliability indices, there are traps forthe unwary. This is clearly demonstrated inthe recent case report where a 10 year oldgirl’s visual field constriction apparently re-versed on cessation of vigabatrin.3 Baselinevisual fields, performed with automated per-imetry, showed a classic artefact cloverleaf-shaped pattern4 that was not recognised bythe authors. Automated threshold perimetryinvolves checking the visual threshold of theretina at set intervals. To reduce the numberof presented stimuli starting points forthreshold determinations are made at fourquadrants 9 degrees from the horizontal andvertical meridians. Not infrequently, poorlycooperative patients are only attentive duringthis initial stage resulting in a cloverleaf-shaped field. In this situation the reliabilityindices are of little help as the suprathresholdfalse negative reliability indices are based onalready fatigued thresholded locations.4
Case reportA 30 year old woman was referred to theneuro-ophthalmology clinic in October 1998for confirmation of vigabatrin induced con-striction of visual fields. Her seizures hadstarted at the age of 12 and consisted of sud-den tonic posturing of the limbs preceded byleft sided sensory symptoms. Initially she washaving 12 seizures a week but by 1998 she washaving 18 seizures a day. She was unable totolerate phenytoin, valproate, carbamazepine,clobazam, lamotrogine, gabapentin, or topira-mate and in 1990 had been started onvigabatrin. In 1998 she was referred forconsideration of epilepsy surgery. At that timeshe complained of bumping into objects andshe was noted on simple confrontation testingto have constricted visual fields. Automatedperimetry was recommended and this wassubsequently performed (Fig 1). Gross peri-pheral field constriction was noted but tan-gent screen examination at 1 and 2 metresrevealed this to be non-physiological tubularvisual field constriction (Fig 2).
CommentThe best way to ascertain whether visual con-striction is pathological or not is to test the
patient at 1 and 2 metres using a wallmounted tangent screen.5 The visual field,whether constricted or not should be conicalin shape and expand geometrically withincreasing distances. Patients with functionalvisual field constriction can often be detectedby the fact that on repeated testing of thevisual field at an increased distance from thetangent screen they will not report thischange in field diameter in an attempt to beconsistent with their first field (tunnel visualfield).5 This is not physiologically possible andis clear evidence of functional visual impair-ment.
Vigabatrin may well induce visual fieldconstriction as a result of retinal toxicity butuntil studies are reported using tests ofpatients on vigabatrin at two viewing dis-tances then this issue will remain open todebate.
JA Olson, AT Purdie, RJ ColemanThe Eye Clinic, Aberdeen Royal Infirmary, Forester
Hill, Aberdeen
Correspondence to: Dr Olson;[email protected]
Accepted for publication 13 February 2002
References1 Eke T, Talbot JF, Lawden MC. Severe
persistent visual field constriction associatedwith vigabatrin. BMJ 1997;314:180–1.
2 Harding GFA. Severe persistent visual fieldconstriction associated with vigabatrin- fourpossible explanations exists. BMJ1997;314:1693.
3 Versino M, Veggiotti P. Reversibility ofvigabatrin-induced visual-field defect. Lancet1999;354:486.
4 Walsh TJ, ed. Visual fields: examination andinterpretation. 2nd ed. San Franciso:American Academy of Ophthalmology, 1996.
5 Glaser JS, ed. Neuro-ophthalmology. 2nd ed.Philadelphia: JB Lippincott, 1990.
Successful treatment ofsquamous cell carcinoma of thelower eyelid with intralesionalcidofovirCidofovir (HPMPC), an acyclic nucleosidephosphonate analogue, is a promising drugthat acts against a wide number of DNAviruses.1 In 1997, the US Federal Food andDrug Administration approved cidofovir (forintravenous use only) for the treatment ofcytomegalovirus retinitis in patients withAIDS.1 Over the last few years, cidofovir in a1–3% gel or cream vehicle has been found tobe effective against unmanageable viral cuta-neous lesions induced by herpes, pox, andpapilloma families.2 Recent studies have ex-plored intralesional administration of cidofo-vir for the treatment of HPV related tumours,such as cervical epithelial neoplasia, oesopha-geal carcinomas, and HSV-8 induced Kaposi’ssarcoma.3–6 We report a squamous cell carci-noma (SCC) of the eyelid which was success-fully treated with intralesional cidofovir.
Case reportA 70 year old man presented with a nodularlesion 10 × 14 mm in size on his right lowereyelid, which had appeared 3 months earlier(Fig 1). The patient, who was otherwise ingood general condition, reported a history ofchronic, intense solar radiation exposurebecause he had lived in Somalia for manyyears. In the past 3 years he had been repeat-edly treated with liquid nitrogen for multipleactinic keratosis of his forehead and uppereyelids. The clinical diagnosis of cutaneous
Figure 1 Automated perimetry of a patient taking vigabatrin. Left, 1990, right, 1998.
Figure 2 The corresponding tangent fieldsperformed at 1 metre with a 1 mm (brokenline) white object and 2 metres with a 2 mmobject (solid line). The 2 mm isoptre lieswithin the 1 mm isoptre, which is anon-physiological finding. (Top) Right eye,(bottom) left eye.
932 PostScript
www.bjophthalmol.com
on 15 July 2018 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.86.8.930-a on 1 August 2002. D
ownloaded from

SCC was confirmed by the histological exam-ination of a punch biopsy. As the patientrefused conventional surgery, after obtainingwritten consent the lesion was treated with adose of cidofovir 0.1 ml (7.5 mg of active prin-ciple). The drug was injected both intralesion-ally and perilesionally with a fine needle (26gauge). Care was taken to avoid intravascularinoculation. Erythema and ulceration wereevident after 3 days, then the lesion becameprogressively smaller and flatter until itdisappeared within the month. A skin punchbiopsy was performed after 12 months on theprevious lesional area, but revealed no pres-ence of neoplastic cells. No systemic sideeffects were noted and the cosmetic result wasexcellent (Fig 2). The patient is free fromrecurrences after a 24 month follow up.
CommentSurgical excision is the treatment of choice forSCC.7 Alternatively, liquid nitrogen, electro-cautery, radiotherapy, or laser photocoagula-tion may be used. Decisions regarding treat-ment depend on the age of the patient, thelocation, extension, and severity of the neo-plasm. For cases in which surgery or alterna-tive cytodestructive techniques are not practi-cal, local treatment with 5-fluorouracil,nitrogen mustard, bleomycin, mitomycin C,photodynamic therapy, or imiquimod may beconsidered as an alternative therapeuticoption.7 Recent studies have showed thatcidofovir exerts tumoricidal activity towardsHPV related cervical intraepithelial neoplasia,3
oesophageal and respiratory papillomatoustumours,4 5 or HSV-8 related Kaposi’s sarcoma.6
To our knowledge, the regression of SCC afterthe intralesional injection of cidofovir has notpreviously been reported.
The mechanism of cidofovir as an anti-neoplastic agent is unknown. The involutionof the neoplastic tissue could be due to theinhibition of rapidly proliferating cellsthrough a decrease in DNA thymidine incor-poration, the activation of tumour suppressorgenes, the induction of apoptosis, and theinhibition of angiogenesis.8–10
Systemic administration of cidofovir is bur-dened with serious, dose related side effects.
Kidney toxicity is the most common but lessfrequently uveitis, macular oedema, neutrope-nia, thrombocytopenia, nausea, fever, hairloss, and muscle pain have also beenobserved.2 When administered topically orintralesionally cidofovir has not, to date,shown systemic toxicity.
Surgical excision remains the best possibletreatment for SCC, as it is usually curative andpermits the histopathological evaluation ofmargins. However, the successful outcomewith intralesional cidofovir in this case mightbe worth considering.
D CalistaDepartment of Dermatology, “M Bufalini” Hospital,
Cesena, Italy
L RiccioniPathology Unit, “M Bufalini” Hospital
L CocciaPrivate practice, ophthalmologist, Ascoli Piceno,
Italy
Correspondence to: Donato Calista, MD,Department of Dermatology, “M Bufalini” Hospital,
47023 Cesena, Italy; [email protected]
Accepted for publication 15 February 2002
References1 De Clercq E. Therapeutic potential of
cidofovir for the treatment of DNA virusinfection. Verh K Acad Geneeskd Belg1996;58:19–49.
2 Zabawski EJ, Cockerell CJ. Topical andintralesional cidofovir: a review ofpharmacology and therapeutic effects. J AmAcad Dermatol 1998;39:741–5.
3 Snoeck R, Noel JC, Muller C, et al. Cidofovir,a new approach for the treatment of cervixintraepithelial neoplasia grade III (CIN III).J Med Virol 2000;60:205–9.
4 Van Cutsem E, Snoeck R, Van Ranst M, et al.Successful treatment of a squamous papillomaof the hypopharynx-esophagus by localinjections of (S)-1-(3-hydroxy-2-phosphonylmethoxypropyl) cytosine. J Med Virol1995;45:230–5.
5 Pranky SM, Magit AE, Kearns DB, et al.Intralesional cidofovir for recurrent respiratorypapillomatosis in children. Arch OtolaryngolNeck Surg 1999;125:1143–8.
6 Fife K, Gill J, Bourboulia D, et al. Cidofovirfor the treatment of Kaposi’s sarcoma in anHIV negative homosexual man. Br J Dermatol1999;141:1148–9.
7 Wennberg AM. Basal cell carcinoma: newaspects of diagnosis and treatment. ActaDerm Venereol Suppl (Stockh)2000;209:5–25.
8 Andrei G, Snoeck R, Schols D, et al. Inductionof apoptotic cell death following treatment oftumor cells with acyclic nucleosidephosphonate. 37th ICAAC, Toronto 28September–1 October 1997. Poster 187-H.
9 DeClercq E, Andrei G, Balzarini J, et al.Antitumor potential of acyclic nucleosidephosphonates. Nucleosides Nucleotides1999;18 :759–71.
10 Liekens S, Andrei G, Vandeputte M, et al.Potent inhibition of hemangioma formation inrats by the acyclic nucleoside phosphonateanalogue cidofovir. Cancer Res1998;58:2562–7.
Multiple iridociliary cysts inpatients withmucopolysaccharidosesThe mucopolysaccharidoses (MPSs) are rarehereditary diseases. They are classified into sixtypes by the distinct lysosomal accumulationsof glycosaminoglycans, which give rise to theprogressive clinical features with involvementof multisystems. Ophthalmic complications,such as corneal stromal opacity, pigmentary
retinal degeneration, optic nerve atrophy, andglaucoma, are common in patients withMPSs.
Cysts in various organs have been reportedin patients with MPSs—for example, multipledentigerous cysts, multifocal large cysts in thewhite matter and arachnoid of the brain, andbone cysts.1 2 In the eye, membrane boundvacuoles in the non-pigmented epithelium ofthe ciliary processes have been observed byelectron microscopy.3 However, iridociliarycysts have never been reported in patientswith MPSs.
We present two cases of multiple iridocili-ary cysts in two patients with MPSs, one withScheie syndrome and the other withMaroteaux-Lamy syndrome.
Case reportsCase 1A 18 year old woman, who was diagnosedwith Scheie syndrome (MPS type IS) byenzyme assay. The activity of α-L-iduronidasein peripheral blood lymphocytes was notdetectable. She had bilateral corneal stromalopacities, shallow anterior chambers, andhigh intraocular pressures. On 6 April 1998her corrected visual acuity was 20/50 in botheyes. Her right intraocular pressure was 24mm Hg and the left was 20 mm Hg with topi-cal medication. Ultrasound biomicroscopyrevealed multiple round cystic lesions withuniformly low echoic density similar to ante-rior chamber fluid in all quadrants of the pos-terior iris, iridociliary sulcus, and pars plicataof both eyes (Fig 1).
Case 2A 23 year old woman, who was diagnosedwith Maroteaux-Lamy syndrome (MPS typeVI). The activity of arylsulphatase B in theperipheral blood lymphocytes was signifi-cantly low. At the age of 13 years, she under-went penetrating keratoplasty on her righteye because of corneal stromal opacity. At theage of 23 years, she underwent deep lamellarkeratoplasty on her left eye. On 10 December1997, slit lamp examination disclosed a cleargraft and the shallow anterior chamber inboth eyes. The corrected visual acuity in herright eye was 20/30 and left was 20/400. Herright intraocular pressure was 12 mm Hg andleft was 18 mm Hg without medication.
Ultrasound biomicroscopy revealed multi-ple round low echoic lesions in the posterioriris and ciliary body similar to case 1 in botheyes (Fig 2).
We examined an additional two patientswith Scheie syndrome; however, no iridocili-ary cysts were found in either patient.
CommentWe have demonstrated the presence of multi-ple round cystic lesions. From this echo-graphic finding, we interpret these lesions asmultiple iridociliary cysts. In previous reports,there is a wide gap in the incidence of ciliarybody cysts on the posterior ciliary bodybecause of the difficulty in detecting them byconventional methods. Marigo et al retrospec-tively reported that cystic lesions were identi-fied in 108 eyes of 88 out of 4632 patients byultrasound biomicroscopy and the incidenceof the multiple cysts occupying more than180º was 13.3%.4 Kunimatsu et al studied theciliary body in 232 eyes of 116 healthy peopleby ultrasound biomicroscopy. They reportedthat ciliary body cysts were detected in 54.3%,and all the cysts were located at the iridocili-ary sulcus or pars plicata.5 The cysts in ourpatients were located at the posterior iris as
Figure 1 Cutaneous squamous cellcarcinoma of the lower right eyelid.
Figure 2 The same patient 24 months later.
PostScript 933
www.bjophthalmol.com
on 15 July 2018 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.86.8.930-a on 1 August 2002. D
ownloaded from

well as in the iridociliary sulcus and pars pli-cata, and the number of cysts was much largerthan that of healthy people in the previousreports.
Also, the reports concerning cysts in otherorgans in MPSs patients support the notionthat iridociliary cysts in MPSs patients weredifferent from usual cysts in normal patients.Because no evidence of the progression of theiris cysts was obtained, neither pathologicalexamination nor the analysis of contents ofcysts was performed in our cases.
All of our patients were diagnosed withglaucomas or ocular hypertension. It has beensuggested that the high intraocular pressurewas due to a blockage of the trabecular mesh-work by the glycosaminoglycan, or a falsehigh ocular pressure because of the higherrigidity of the cornea in the MPSs patients. Onthe other hand, angle closure that is caused bymultiple iridociliary cysts in a patient withoutMPS has been reported.6 So we suggest thatangle closure by the cysts may be anothercause for the high intraocular pressure insome MPSs cases.
In summary, some of the patients withMPSs with shallow anterior chamber demon-strated the presence of multiple iridociliarycysts and ultrasound biomicroscopy is veryuseful tool for finding the cysts.
S Sato, N Maeda, H Watanabe, Y TanoDepartment of Ophthalmology, Osaka University
Medical School, Japan
Y InoueDepartment of Ophthalmology, Tottori University
Faculty of Medicine, Japan
Y ShimomuraDepartment of Ophthalmology, Kinki University
Medical School, Japan
A TanakaDepartment of Pediatrics, Osaka City University
Graduate School of Medicine, Japan
Correspondence to: Shigeru Sato, MD, Departmentof Ophthalmology, Osaka University Medical
School, Room E7, Yamadaoka 2-2, Suita, Osaka565-0871, Japan; [email protected]
Accepted for publication 25 February 2002
References1 Roberts MW, Barton NW, Constantopoulos
G, et al. Occurrence of multiple dentigerouscysts in a patient with the Maroteaux-Lamysyndrome (mucopolysaccharidosis, type VI).Oral Surg Oral Med Oral Pathol1984;58:169–75.
2 Lamon JM, Trojak JE, Abbott MA. Bone cystsin mucopolysaccharidosis I-S (Scheiesyndrome). Johns Hopkins Med J1980;146:73–5.
3 Topping TM, Kenyon KR, Goldberg MF, etal. Ultrastructural ocular pathology of Hunter’ssyndrome. Arch Ophthalmol1971;86:164–77.
4 Marigo FA, Esaki K. Differential diagnosis ofanterior segment cysts by ultrasoundbiomicroscopy. Ophthalmology1999;106:2131–5.
5 Kunimatsu S, Araie M. Ultrasoundbiomicroscopy of ciliary body cysts. Am JOphthalmol 1999;127:48–55.
6 Tanihara H, Akita J, et al. Angle closurecaused by multiple bilateral iridociliary cysts.Acta Ophthalmol Scand 1997;75:216–17.
A case of encephalocranio-cutaneous lipomatosisEncephalocraniocutaneous lipomatosis(ECCL) is a rare neurocutaneous syndromecharacterised by cranial and facial asymme-try, cutaneous lesions, central nervous systemabnormalities, and ocular abnormalities.
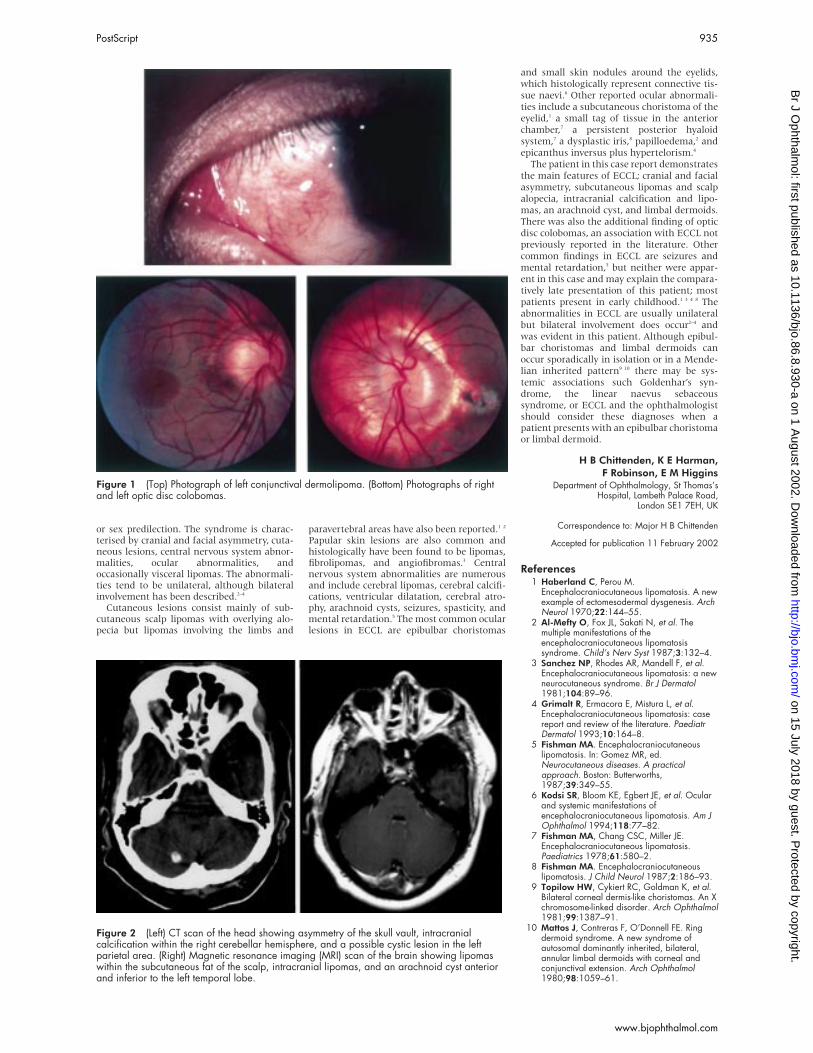
A case is described of a young man whopresented with limbal dermoids, subcutan-eous lipomas, and scalp alopecia. Furtherinvestigation revealed cranial and facial asym-metry, intracranial lipomas, and calcificationand an arachnoid cyst, supporting a diagnosisof ECCL. This patient also had the additionalocular abnormality of bilateral optic disc colo-bomas, an association with ECCL not previ-ously reported in the literature.
Case reportA 23 year old Asian man first presented to theeye clinic aged 16 with a left conjunctivallesion. On examination he had bilateralconjunctival dermolipomas, preauricular lipo-mas, and bilateral optic disc colobomas.Surgery was not advised at this time and nofollow up was arranged, although photo-graphs were taken (Fig 1). Aged 20, hepresented to the eye clinic again. Before exci-sion biopsy of the left conjunctival dermol-ipoma, a computed tomograph (CT) scan ofthe head was requested to delineate theposterior extent of the lesion. This revealedsome asymmetry of the skull vault, intracra-nial calcification within the right cerebellarhemisphere, and a possible cystic lesion in theleft parietal area (Fig 2 (left)). Subsequentexamination by a neurologist was entirelynormal with no stigmata of the phacoma-toses. Histology of the conjunctival lesionconfirmed a complex corneoscleral choris-toma comprising collagenous tissue with fatand a focus of cartilage.
Three years later the patient was seen by adermatologist complaining of a lesion on hisleft eyebrow, which was clinically a lipoma.Skull and facial x rays revealed asymmetry ofthe skull vault and facial bones including thezygomatic arches. Further investigation in theform of an magnetic resonance imaging(MRI) scan of the brain showed lipomaswithin the subcutaneous fat of the scalp andalso intracranial lipomas. In addition, therewas an arachnoid cyst anterior and inferior tothe left temporal lobe (Fig 2 (right)). Therewas no connection between the soft tissuetumour on the left eyebrow and the intracra-nial cavity. Subsequent histology of theexcised lesion revealed a lipoma.
Review of the patient’s childhood medicalrecords revealed that since birth he had hadlarge patches of scalp alopecia and aged 7 hewas noted to have a large suprapubic fat pad.A final diagnosis of ECCL was made based onthe findings of limbal dermoids, subcutan-eous lipomas, scalp alopecia, cranial and facialasymmetry, intracranial lipomas and calcifica-tion, and an arachnoid cyst.
CommentECCL is a rare neurocutaneous syndrome ofunknown aetiology, first described by Haber-land and Perou in 1970.1 All cases described inthe literature have been sporadic and theredoes not appear to be any geographic, racial,
Figure 1 Cross sectional appearance of the iris by ultrasound biomicroscopy in case 1.Multiple iridociliary cysts are seen in the posterior iris of both eyes: (A) 1.2 mm diameter cystin the right eye; (B) 0.8 mm diameter cyst in the left eye.
Figure 2 Cross sectional view of the iris by ultrasound biomicroscopy in case 2. Multipleiridociliary cysts are seen in the posterior iris of both eyes: (A) 0.8 mm, 0.4 mm, and 0.8 ×1.3 mm diameter cysts in the right eye; (B) 1.1 mm and 1.0 mm diameter cysts in the left eye.
934 PostScript
www.bjophthalmol.com
on 15 July 2018 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.86.8.930-a on 1 August 2002. D
ownloaded from
or sex predilection. The syndrome is charac-terised by cranial and facial asymmetry, cuta-neous lesions, central nervous system abnor-malities, ocular abnormalities, andoccasionally visceral lipomas. The abnormali-ties tend to be unilateral, although bilateralinvolvement has been described.2–4
Cutaneous lesions consist mainly of sub-cutaneous scalp lipomas with overlying alo-pecia but lipomas involving the limbs and
paravertebral areas have also been reported.1 2
Papular skin lesions are also common andhistologically have been found to be lipomas,fibrolipomas, and angiofibromas.3 Centralnervous system abnormalities are numerousand include cerebral lipomas, cerebral calcifi-cations, ventricular dilatation, cerebral atro-phy, arachnoid cysts, seizures, spasticity, andmental retardation.5 The most common ocularlesions in ECCL are epibulbar choristomas
and small skin nodules around the eyelids,
which histologically represent connective tis-
sue naevi.6 Other reported ocular abnormali-
ties include a subcutaneous choristoma of the
eyelid,1 a small tag of tissue in the anterior
chamber,7 a persistent posterior hyaloid
system,7 a dysplastic iris,8 papilloedema,2 and
epicanthus inversus plus hypertelorism.4
The patient in this case report demonstrates
the main features of ECCL; cranial and facial
asymmetry, subcutaneous lipomas and scalp
alopecia, intracranial calcification and lipo-
mas, an arachnoid cyst, and limbal dermoids.
There was also the additional finding of optic
disc colobomas, an association with ECCL not
previously reported in the literature. Other
common findings in ECCL are seizures and
mental retardation,5 but neither were appar-
ent in this case and may explain the compara-
tively late presentation of this patient; most
patients present in early childhood.1 3 4 8 The
abnormalities in ECCL are usually unilateral
but bilateral involvement does occur2–4 and
was evident in this patient. Although epibul-
bar choristomas and limbal dermoids can
occur sporadically in isolation or in a Mende-
lian inherited pattern9 10 there may be sys-
temic associations such Goldenhar’s syn-
drome, the linear naevus sebaceoussyndrome, or ECCL and the ophthalmologistshould consider these diagnoses when apatient presents with an epibulbar choristomaor limbal dermoid.
H B Chittenden, K E Harman,F Robinson, E M Higgins
Department of Ophthalmology, St Thomas’sHospital, Lambeth Palace Road,
London SE1 7EH, UK
Correspondence to: Major H B Chittenden
Accepted for publication 11 February 2002
References1 Haberland C, Perou M.
Encephalocraniocutaneous lipomatosis. A newexample of ectomesodermal dysgenesis. ArchNeurol 1970;22:144–55.
2 Al-Mefty O, Fox JL, Sakati N, et al. Themultiple manifestations of theencephalocraniocutaneous lipomatosissyndrome. Child’s Nerv Syst 1987;3:132–4.
3 Sanchez NP, Rhodes AR, Mandell F, et al.Encephalocraniocutaneous lipomatosis: a newneurocutaneous syndrome. Br J Dermatol1981;104:89–96.
4 Grimalt R, Ermacora E, Mistura L, et al.Encephalocraniocutaneous lipomatosis: casereport and review of the literature. PaediatrDermatol 1993;10:164–8.
5 Fishman MA. Encephalocraniocutaneouslipomatosis. In: Gomez MR, ed.Neurocutaneous diseases. A practicalapproach. Boston: Butterworths,1987;39:349–55.
6 Kodsi SR, Bloom KE, Egbert JE, et al. Ocularand systemic manifestations ofencephalocraniocutaneous lipomatosis. Am JOphthalmol 1994;118:77–82.
7 Fishman MA, Chang CSC, Miller JE.Encephalocraniocutaneous lipomatosis.Paediatrics 1978;61:580–2.
8 Fishman MA. Encephalocraniocutaneouslipomatosis. J Child Neurol 1987;2:186–93.
9 Topilow HW, Cykiert RC, Goldman K, et al.Bilateral corneal dermis-like choristomas. An Xchromosome-linked disorder. Arch Ophthalmol1981;99:1387–91.
10 Mattos J, Contreras F, O’Donnell FE. Ringdermoid syndrome. A new syndrome ofautosomal dominantly inherited, bilateral,annular limbal dermoids with corneal andconjunctival extension. Arch Ophthalmol1980;98:1059–61.
Figure 1 (Top) Photograph of left conjunctival dermolipoma. (Bottom) Photographs of rightand left optic disc colobomas.
Figure 2 (Left) CT scan of the head showing asymmetry of the skull vault, intracranialcalcification within the right cerebellar hemisphere, and a possible cystic lesion in the leftparietal area. (Right) Magnetic resonance imaging (MRI) scan of the brain showing lipomaswithin the subcutaneous fat of the scalp, intracranial lipomas, and an arachnoid cyst anteriorand inferior to the left temporal lobe.
PostScript 935
www.bjophthalmol.com
on 15 July 2018 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.86.8.930-a on 1 August 2002. D
ownloaded from

Bilateral non-specific orbitalinflammation (orbital“pseudotumour”), posteriorscleritis, and anterior uveitisassociated with hypothyroidismin a childPosterior scleritis and non-specific orbitalinflammation (NSOI), also known as orbital“pseudotumour,” are rarely seen inchildren.1–3 Paediatric posterior scleritis andNSOI seldom have an underlying systemicassociation and, to our knowledge, hypo-thyroidism has not been reported as anassociation,1 4 although thyroid abnormalitiesare recognised in adults.
We present a case of a child with bilateralanterior NSOI, posterior scleritis, and anterioruveitis who was also found to be hypothyroid.
Case reportA previously fit and well 13 year old girlpresented with a 3 week history of bilateralred eyes and painless puffy left upper andlower lids for 1 week. She had had a headachefor 10 days which had failed to respond to oralantibiotics. Systemic inquiry revealed a sorethroat for 10 days but no other symptoms, inparticular no thyroid related symptoms. Hervisual acuity was 6/9 right, and 6/18 unaided,improving to 6/12 with pinhole in the left eye.She read all the Ishihara plates with the righteye, but missed three out of 17 plates with theleft. No relative afferent pupillary defect(RAPD) was present. She had mild left perior-bital swelling which was not erythematous ortender. There was no proptosis. She had fullextraocular movements with no diplopia. Theright eye had signs of mild anterior uveitiswith 1+ of cells while the left eye had 2+ ofcells in the anterior chamber. There was noevidence of posterior segment involvement,with normal vitreous and fundi.
She was commenced with 2 hourly dexam-ethasone eye drops to both eyes and on review3 days later her vision improved to 6/6 in botheyes. A week later, she returned with pain andincreasing periorbital swelling, left eye greaterthan right. Her visual acuity was reduced to6/12 (right eye) and 6/60 improving to 6/18with a pinhole (left eye). A mild left RAPDwas present. Significant non-tender, mildlyerythematous periorbital swelling waspresent in the left eye. She had 2 mm leftrelative proptosis, with generalised restrictionof extraocular movements. There was mildbilateral anterior uveitis. The left disc wasmore swollen than the right and retinal striaewere present in both eyes (Fig 1). There was noevidence of vitreous or chorioretinal inflamma-tion. An orbital computed tomograph (CT)
scan suggested a diagnosis of bilateral ante-rior NSOI without enlargement of the ex-traocular muscles (Fig 2). B-mode ultrasonog-raphy showed bilateral diffuse thickening ofthe posterior coats of the eyes (maximum leftthickness of 4.4 mm) and fluid in Tenon’scapsule consistent with scleritis.
Full blood count, urea, and electrolytes, liverfunction tests, serum angiotensin convertingenzyme, serum calcium, autoantibodies (in-cluding ANA, ANCA, and rheumatoid factor), Creactive protein (CRP), and chest x ray werenormal. She had negative serology for Borrelia,HTLV-1, and HTLV-2. Her erythrocyte sedimen-tation rate (ESR) was 32 mm in the first hourand a mildly raised Ig M was found. She wasbiochemically hypothyroid (raised TSH of 25.5mU/l (0.4–4.0) and T4 of 10.6 pmol/l (9–20))with positive anti-thyroid M antibodies. Thyro-trophin releasing hormone stimulation testconfirmed primary hypothyroidism.
Treatment was commenced with pred-nisolone 50 mg which was reduced graduallyover 3 months with resolution of her symp-toms and signs. She had no relapse at 1 yearfollow up. She was also treated with thyroxinefor her hypothyroidism.
CommentThe distinction between posterior scleritis anddiffuse anterior NSOI is not always clear. As inthis case, they commonly have evidence ofinflammatory changes of the posterior coatsof the eye and periocular tissues.2 4 5
In a series of 29 paediatric NSOI cases, therewas an association with peripheral bloodeosinophilia, raised ESR, and positive ANA.Normal thyroid function tests (TFTs) werepresent in all of the nine children tested.4
Other reports of paediatric NSOI do not statewhether TFTs were performed.6 7 Similarly,children with posterior scleritis tend not tohave any clinical or laboratory evidence ofassociated systemic disease, but TFTs are notspecifically mentioned.1 8 This is in contrastwith our patient who was found to bebiochemically hypothyroid. There is some evi-dence of thyroid autoimmunity in adultpatients with NSOI, as shown by Atabay et alwho found antibodies to eye muscle mem-brane antigens and thyroid microsomal anti-gen in patients with NSOI. Each of their caseswas clinically and biochemically euthyroid.3
NSOI and scleritis in children may be asso-ciated with iritis, unlike the adult form of thisdisorder.6 9 Bloom et al report that childrenwith NSOI and anterior uveitis tend to have aworse prognosis and increased recurrence.6
Our patient responded well to steroid treat-ment with no relapse at 1 year.
Scleritis with uveitis, although rare in chil-dren, should be recognised as part of the dif-ferential diagnosis of acute paediatric orbitalinflammation. Hypothyroidism may be anincidental finding in our case, but the role ofthyroid autoimmunity in children with NSOIand scleritis needs to be further investigated.
J M Uddin, C A Rennie, A T MooreDepartment of Ophthalmology, Addenbrooke’s
Hospital, Cambridge, UK
Correspondence to: Jimmy Uddin, Department ofOphthalmology, Addenbrooke’s Hospital, Hills
Road, Cambridge CB2 2QQ, UK;[email protected]
Accepted for publication 27 February 2002
References1 Woon WH, Stanford MR, Graham EM.
Severe idiopathic posterior scleritis inchildren. Eye 1995;9:570–4.
2 Benson WE. Posterior scleritis. SurvOphthalmol 1988;32:297–316.
3 Atabay C, Tyutyunikov A, Scalise D, et al.Serum antibodies reactive with eye musclemembrane antigens are detected in patientswith nonspecific orbital inflammation.Ophthalmology 1995;102:145–53.
4 Mottow-Lippa L, Jakobiec FA, Smith M.Idiopathic inflammatory orbital pseudotumorin childhood. II. Results of diagnostic tests andbiopsies. Ophthalmology 1981;88:565–74.
5 Rootman J, Nugent R. The classification andmanagement of acute orbital pseudotumors.Ophthalmology 1982;89:1040–8.
6 Bloom JN, Graviss ER, Byrne BJ. Orbitalpseudotumor in the differential diagnosis ofpediatric uveitis. J Pediatr OphthalmolStrabismus 1992;29:59–63.
7 Hertle RW, Granet DB, Goyal AK, et al.Orbital pseudotumor in the differentialdiagnosis of pediatric uveitis. J PediatrOphthalmol Strabismus 1993;30:61.
8 Wald KJ, Spaide R, Patalano VJ, et al.Posterior scleritis in children. Am J Ophthalmol1992;113:281–6.
9 McCluskey PJ, Watson PG, Lightman S, et al.Posterior scleritis: clinical features, systemicassociations, and outcome in a large series ofpatients. Ophthalmology 1999;106:2380–6.
Unilateral enlargement of theblind spot: a diagnostic dilemmaUnilateral blind spot enlargement occurs asan isolated entity (acute idiopathic blind spotenlargement) or in association with otherconditions such as multiple evanescent whitedot syndrome, multifocal choroiditis withpanuveitis, or punctate inner choroidopathy.It remains controversial whether blind spotenlargement in these conditions serves tounify them as a diagnostic group. The patientpresented here had clinical features suggest-ing “diagnostic overlap” with some of theseconditions, suggesting that diagnostic “lump-ing” of these diseases may have more logicthan “splitting” them.
Case reportA 30 year old female patient presented to us inSeptember 2000 with a blind spot close to thecentre of vision in her left eye. She was uncer-tain as to how long it had been present,having noticed it only when the other eye wastemporarily covered by chance. She was fitand well, with no recent viral illness or previ-ous eye problems. Her acuity with myopic cor-rection (−3.00 dioptre sphere right, −3.25dioptre sphere left) was recorded at 6/6 rightand left, and discrete foci of chorioretinalscarring were noted above and nasal to theoptic disc in the left eye (Fig 1). There was noevidence of vitreous inflammatory activity in
Figure 1 Fundus photograph of the left eyeshowing a swollen optic disc, tortuous retinalvessels, and multiple retinal striae.
Figure 2 CT scan showing bilateral softtissue thickening of the posterior coats of theglobe and periocular tissues. This ispredominantly intraconal and adjacent to theleft globe. The extraocular muscles appearnormal.
936 PostScript
www.bjophthalmol.com
on 15 July 2018 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.86.8.930-a on 1 August 2002. D
ownloaded from
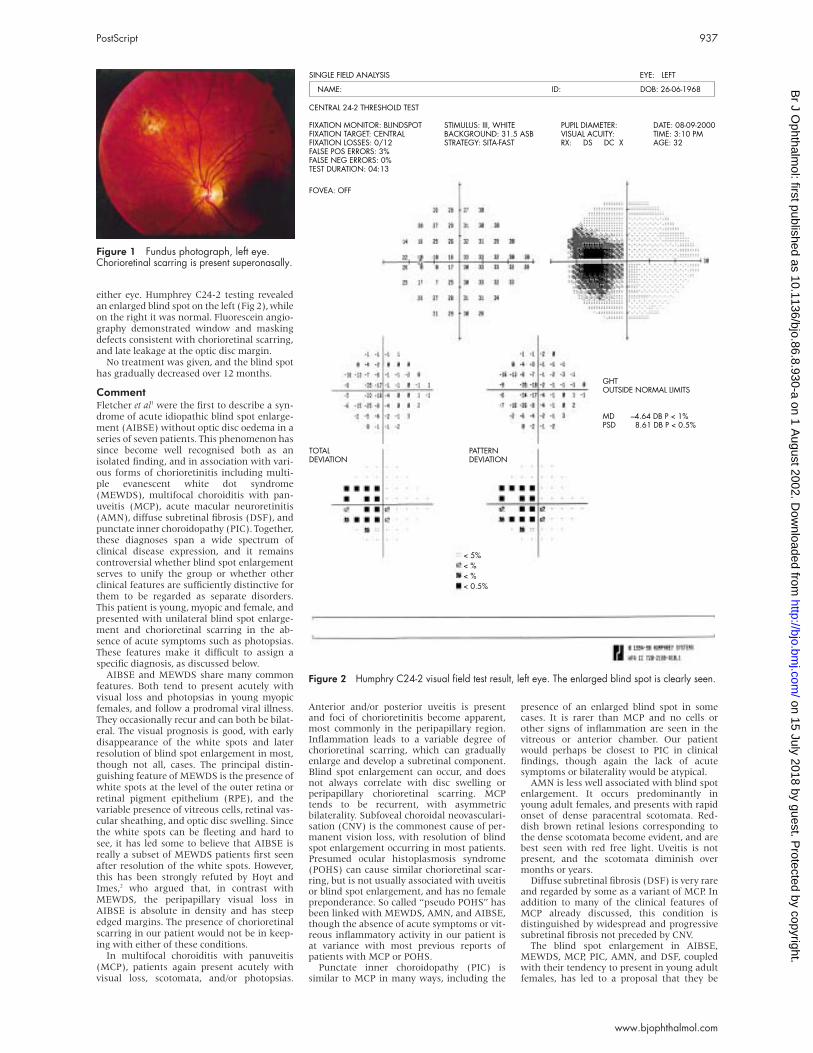
either eye. Humphrey C24-2 testing revealedan enlarged blind spot on the left (Fig 2), whileon the right it was normal. Fluorescein angio-graphy demonstrated window and maskingdefects consistent with chorioretinal scarring,and late leakage at the optic disc margin.
No treatment was given, and the blind spothas gradually decreased over 12 months.
CommentFletcher et al1 were the first to describe a syn-drome of acute idiopathic blind spot enlarge-ment (AIBSE) without optic disc oedema in aseries of seven patients. This phenomenon hassince become well recognised both as anisolated finding, and in association with vari-ous forms of chorioretinitis including multi-ple evanescent white dot syndrome(MEWDS), multifocal choroiditis with pan-uveitis (MCP), acute macular neuroretinitis(AMN), diffuse subretinal fibrosis (DSF), andpunctate inner choroidopathy (PIC). Together,these diagnoses span a wide spectrum ofclinical disease expression, and it remainscontroversial whether blind spot enlargementserves to unify the group or whether otherclinical features are sufficiently distinctive forthem to be regarded as separate disorders.This patient is young, myopic and female, andpresented with unilateral blind spot enlarge-ment and chorioretinal scarring in the ab-sence of acute symptoms such as photopsias.These features make it difficult to assign aspecific diagnosis, as discussed below.
AIBSE and MEWDS share many commonfeatures. Both tend to present acutely withvisual loss and photopsias in young myopicfemales, and follow a prodromal viral illness.They occasionally recur and can both be bilat-eral. The visual prognosis is good, with earlydisappearance of the white spots and laterresolution of blind spot enlargement in most,though not all, cases. The principal distin-guishing feature of MEWDS is the presence ofwhite spots at the level of the outer retina orretinal pigment epithelium (RPE), and thevariable presence of vitreous cells, retinal vas-cular sheathing, and optic disc swelling. Sincethe white spots can be fleeting and hard tosee, it has led some to believe that AIBSE isreally a subset of MEWDS patients first seenafter resolution of the white spots. However,this has been strongly refuted by Hoyt andImes,2 who argued that, in contrast withMEWDS, the peripapillary visual loss inAIBSE is absolute in density and has steepedged margins. The presence of chorioretinalscarring in our patient would not be in keep-ing with either of these conditions.
In multifocal choroiditis with panuveitis(MCP), patients again present acutely withvisual loss, scotomata, and/or photopsias.
Anterior and/or posterior uveitis is presentand foci of chorioretinitis become apparent,most commonly in the peripapillary region.Inflammation leads to a variable degree ofchorioretinal scarring, which can graduallyenlarge and develop a subretinal component.Blind spot enlargement can occur, and doesnot always correlate with disc swelling orperipapillary chorioretinal scarring. MCPtends to be recurrent, with asymmetricbilaterality. Subfoveal choroidal neovasculari-sation (CNV) is the commonest cause of per-manent vision loss, with resolution of blindspot enlargement occurring in most patients.Presumed ocular histoplasmosis syndrome(POHS) can cause similar chorioretinal scar-ring, but is not usually associated with uveitisor blind spot enlargement, and has no femalepreponderance. So called “pseudo POHS” hasbeen linked with MEWDS, AMN, and AIBSE,though the absence of acute symptoms or vit-reous inflammatory activity in our patient isat variance with most previous reports ofpatients with MCP or POHS.
Punctate inner choroidopathy (PIC) issimilar to MCP in many ways, including the
presence of an enlarged blind spot in somecases. It is rarer than MCP and no cells orother signs of inflammation are seen in thevitreous or anterior chamber. Our patientwould perhaps be closest to PIC in clinicalfindings, though again the lack of acutesymptoms or bilaterality would be atypical.
AMN is less well associated with blind spotenlargement. It occurs predominantly inyoung adult females, and presents with rapidonset of dense paracentral scotomata. Red-dish brown retinal lesions corresponding tothe dense scotomata become evident, and arebest seen with red free light. Uveitis is notpresent, and the scotomata diminish overmonths or years.
Diffuse subretinal fibrosis (DSF) is very rareand regarded by some as a variant of MCP. Inaddition to many of the clinical features ofMCP already discussed, this condition isdistinguished by widespread and progressivesubretinal fibrosis not preceded by CNV.
The blind spot enlargement in AIBSE,MEWDS, MCP, PIC, AMN, and DSF, coupledwith their tendency to present in young adultfemales, has led to a proposal that they be
Figure 1 Fundus photograph, left eye.Chorioretinal scarring is present superonasally.
Figure 2 Humphry C24-2 visual field test result, left eye. The enlarged blind spot is clearly seen.
GHTOUTSIDE NORMAL LIMITS
MDPSD
PATTERN DEVIATION
< 5%< %< %< 0.5%
TOTAL DEVIATION
FIXATION MONITOR: BLINDSPOTFIXATION TARGET: CENTRALFIXATION LOSSES: 0/12FALSE POS ERRORS: 3%FALSE NEG ERRORS: 0%TEST DURATION: 04:13
CENTRAL 24-2 THRESHOLD TEST
SINGLE FIELD ANALYSIS EYE: LEFT
NAME: ID: DOB: 26-06-1968
STIMULUS: III, WHITEBACKGROUND: 31.5 ASBSTRATEGY: SITA-FAST
PUPIL DIAMETER:VISUAL ACUITY:RX: DS DC X
DATE: 08-09-2000TIME: 3:10 PMAGE: 32
FOVEA: OFF
–4.64 DB P < 1% 8.61 DB P < 0.5%
PostScript 937
www.bjophthalmol.com
on 15 July 2018 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.86.8.930-a on 1 August 2002. D
ownloaded from
grouped under the term “acute zonal occultouter retinopathy” (AZOOR).3 Added to theclinical similarities already described, Jacob-sen et al4 demonstrated electroretinographic(ERG) abnormalities in a group of 24 AZOORpatients, though in some cases there wereonly subtle intereye differences detected. Itwas concluded that ERG findings help tounify this diagnostic group, as well as indicat-ing that the primary pathophysiology lies atthe level of the photoreceptor outer segment.This view was not supported by Jampol andWiredu, who argued that the above entitieswere sufficiently distinctive to warrant “split-ting” rather than “lumping.”5
Our patient does not fit neatly into any ofthe diagnoses discussed above, and theprincipal clinical features of blind spot en-largement with chorioretinal scarring in theabsence of acute symptoms or evidence of vit-ritis suggest that there is a degree of diagnos-tic overlap in her case. To the extent that asingle case report can inform this debate, itdoes indicate that some patients do not fitneatly into diagnostic groups, strengtheningthe case for those who would “lump” thesediagnoses rather than “split” them. Perhapsthere are other cases which remain unre-ported because of this diagnostic uncertainty.
R H GrayTaunton and Somerset Hospital, Musgrove Park,
Taunton TA1 5DA, UK
Accepted for publication 25 March 2002
References1 Fletcher WA, Imes RK, Goodman D, et al.
Acute idiopathic blind spot enlargement. Abig blind spot syndrome without optic discoedema. Arch Ophthalmol 1988;106:44–9.
2 Hoyt WF, Imes RK. Multiple evanescent whitedot syndrome, reply to letter. Arch Ophthalmol1988;106:1163.
3 Gass JDM. Acute zonal occult outerretinopathy. J Clin Neuro-Ophthalmol1993;13:79–97.
4 Jacobson SG, Morales DS, Sun XK, et al.Pattern of retinal dysfunction in acute zonaloccult outer retinopathy. Ophthalmology1995;102:1187–98.
5 Jampol LM, Wiredu BS. MEWDS, MFC, PIC,AMN, AIBSE, and AZOOR: one disease ormany. Retina 1995;15:373–8.
Acquired ocular toxoplasmosisin pregnancyWe describe the management of a case ofacquired ocular toxoplasmosis that occurredin the first trimester of pregnancy.
Case reportA 27 year old apparently healthy Pakistaniwoman, at 9 weeks’ gestation, presented tothe Birmingham and Midland Eye Centre
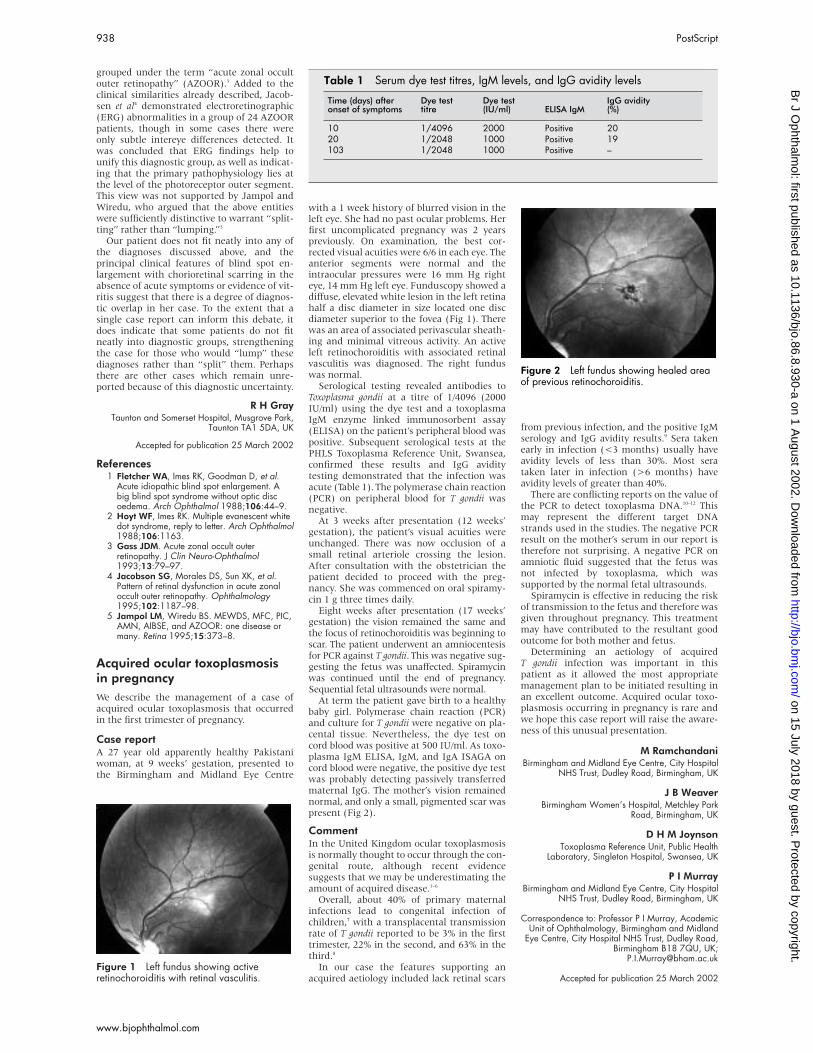
with a 1 week history of blurred vision in theleft eye. She had no past ocular problems. Herfirst uncomplicated pregnancy was 2 yearspreviously. On examination, the best cor-rected visual acuities were 6/6 in each eye. Theanterior segments were normal and theintraocular pressures were 16 mm Hg righteye, 14 mm Hg left eye. Funduscopy showed adiffuse, elevated white lesion in the left retinahalf a disc diameter in size located one discdiameter superior to the fovea (Fig 1). Therewas an area of associated perivascular sheath-ing and minimal vitreous activity. An activeleft retinochoroiditis with associated retinalvasculitis was diagnosed. The right funduswas normal.
Serological testing revealed antibodies toToxoplasma gondii at a titre of 1/4096 (2000IU/ml) using the dye test and a toxoplasmaIgM enzyme linked immunosorbent assay(ELISA) on the patient’s peripheral blood waspositive. Subsequent serological tests at thePHLS Toxoplasma Reference Unit, Swansea,confirmed these results and IgG aviditytesting demonstrated that the infection wasacute (Table 1). The polymerase chain reaction(PCR) on peripheral blood for T gondii wasnegative.
At 3 weeks after presentation (12 weeks’gestation), the patient’s visual acuities wereunchanged. There was now occlusion of asmall retinal arteriole crossing the lesion.After consultation with the obstetrician thepatient decided to proceed with the preg-nancy. She was commenced on oral spiramy-cin 1 g three times daily.
Eight weeks after presentation (17 weeks’gestation) the vision remained the same andthe focus of retinochoroiditis was beginning toscar. The patient underwent an amniocentesisfor PCR against T gondii. This was negative sug-gesting the fetus was unaffected. Spiramycinwas continued until the end of pregnancy.Sequential fetal ultrasounds were normal.
At term the patient gave birth to a healthybaby girl. Polymerase chain reaction (PCR)and culture for T gondii were negative on pla-cental tissue. Nevertheless, the dye test oncord blood was positive at 500 IU/ml. As toxo-plasma IgM ELISA, IgM, and IgA ISAGA oncord blood were negative, the positive dye testwas probably detecting passively transferredmaternal IgG. The mother’s vision remainednormal, and only a small, pigmented scar waspresent (Fig 2).
CommentIn the United Kingdom ocular toxoplasmosisis normally thought to occur through the con-genital route, although recent evidencesuggests that we may be underestimating theamount of acquired disease.1–6
Overall, about 40% of primary maternalinfections lead to congenital infection ofchildren,7 with a transplacental transmissionrate of T gondii reported to be 3% in the firsttrimester, 22% in the second, and 63% in thethird.8
In our case the features supporting anacquired aetiology included lack retinal scars
from previous infection, and the positive IgMserology and IgG avidity results.9 Sera takenearly in infection (<3 months) usually haveavidity levels of less than 30%. Most serataken later in infection (>6 months) haveavidity levels of greater than 40%.
There are conflicting reports on the value ofthe PCR to detect toxoplasma DNA.10–12 Thismay represent the different target DNAstrands used in the studies. The negative PCRresult on the mother’s serum in our report istherefore not surprising. A negative PCR onamniotic fluid suggested that the fetus wasnot infected by toxoplasma, which wassupported by the normal fetal ultrasounds.
Spiramycin is effective in reducing the riskof transmission to the fetus and therefore wasgiven throughout pregnancy. This treatmentmay have contributed to the resultant goodoutcome for both mother and fetus.
Determining an aetiology of acquiredT gondii infection was important in thispatient as it allowed the most appropriatemanagement plan to be initiated resulting inan excellent outcome. Acquired ocular toxo-plasmosis occurring in pregnancy is rare andwe hope this case report will raise the aware-ness of this unusual presentation.
M RamchandaniBirmingham and Midland Eye Centre, City Hospital
NHS Trust, Dudley Road, Birmingham, UK
J B WeaverBirmingham Women’s Hospital, Metchley Park
Road, Birmingham, UK
D H M JoynsonToxoplasma Reference Unit, Public Health
Laboratory, Singleton Hospital, Swansea, UK
P I MurrayBirmingham and Midland Eye Centre, City Hospital
NHS Trust, Dudley Road, Birmingham, UK
Correspondence to: Professor P I Murray, AcademicUnit of Ophthalmology, Birmingham and Midland
Eye Centre, City Hospital NHS Trust, Dudley Road,Birmingham B18 7QU, UK;
Accepted for publication 25 March 2002Figure 1 Left fundus showing activeretinochoroiditis with retinal vasculitis.
Table 1 Serum dye test titres, IgM levels, and IgG avidity levels
Time (days) afteronset of symptoms
Dye testtitre
Dye test(IU/ml) ELISA IgM
IgG avidity(%)
10 1/4096 2000 Positive 2020 1/2048 1000 Positive 19103 1/2048 1000 Positive –
Figure 2 Left fundus showing healed areaof previous retinochoroiditis.
938 PostScript
www.bjophthalmol.com
on 15 July 2018 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.86.8.930-a on 1 August 2002. D
ownloaded from
References1 Burnett AJ, Shortt SG, Isaac-Renron JL, et al.
Multiple cases of acquired toxoplasmosisretinitis presenting in an outbreak.Ophthalmology 1998;105:1032–6.
2 Bowie WR, King AS, Werker DH, et al.Outbreak of toxoplasmosis associated withmunicipal drinking water. Lancet1997;350:173–7.
3 Glasner PD, Silveira C, Kruszon-Moran D, etal. An unusually high prevalence of oculartoxoplasmosis in southern Brazil. Am JOphthalmol 1992;114:136–44.
4 Holland GN. Perspective. Reconsidering thepathogenesis of ocular toxoplasmosis. Am JOphthalmol 1999;128:502–5.
5 Gilbert RE, Dunn DT, Lightman S, et al.Incidence of symptomatic toxoplasma eyedisease: aetiology and public healthimplications. Epidemiol Infect1999;123:283–9.
6 Bosch-Driessen EH, Rothova A. Recurrentocular disease in postnatally acquiredtoxoplasmosis. Am J Ophthalmol1999;128:421–5.
7 Desmonts G, Couvreur J. Congenitaltoxoplasmosis. N Engl J Med1974;290:1110–6.
8 Wallon M, Dunn D, Slimani D, et al.Diagnosis of congenital toxoplasmosis at birth:what is the value of testing for IgM and IgA?Eur J Pediatr 1999;158:645–9.
9 Liesenfeld O, Montoya JG, Kinney S, et al.Effect of testing for IgG avidity in thediagnosis of Toxoplasma gondii infection inpregnant women: experience in a US referencelaboratory. J Infect Dis 2001;183:1248–53.
10 Guy EC, Joynson DH. Potential of the polymerasechain reaction in the diagnosis of activeToxoplasma infection by detection of parasitein blood. J Infect Dis 1995;172:319–22.
11 Garweg J, Boehnke M, Koerner F. Restrictedapplicability of the polymerase chain reactionfor the diagnosis of ocular toxoplasmosis. GerJ Ophthalmol 1996;5:104–8.
12 Bou G, Figueroa MS, Marti-Belda P, et al.Value of PCR for detection of toxoplasmagondii in aqueous humor and blood samplesfrom immunocompetent patients with oculartoxoplasmosis. J Clin Microbiol1999;37:3465–8.
Spontaneous reduction in myopiccorrection following varicelladisciform stromal keratitisWe present the case of an 11 year old myopicgirl who developed significant refractivechanges due to corneal scarring followingvaricella disciform stromal keratitis in herright eye. This has markedly reduced themyopia in her right eye and resulted insignificant anisometropia.
Case reportThis 11 year old girl presented to her generalpractitioner with a red and painful right eyewith reduced vision. She had had anuneventful episode of primary varicella zosterinfection (chickenpox) 3 weeks earlier, fromwhich she had made a full recovery. The
general practitioner diagnosed her as havingconjunctivitis and she was treated withtopical chloramphenicol. One week later, theredness and pain had settled but her visionremained hazy. As a result she was referred tothe eye department. Examination confirmed areduction of visual acuity to 6/24 (Snellen) inthe right eye and 6/6 in the left with spectaclecorrection. She was wearing a correction formyopia with a prescription of −4.75/−0.75 ×110° in the right eye and −6.00/−0.50 × 90° inthe left eye. There was right superficialdisciform stromal scar in the central corneaover the visual axis extending towards theperiphery at 6 o’clock. Corneal sensation wasintact and equal in both eyes. There was noactive inflammation with white conjunctivaand quiet anterior chambers. The intraocularpressures were normal. Fundus examinationrevealed no abnormality. As there was no
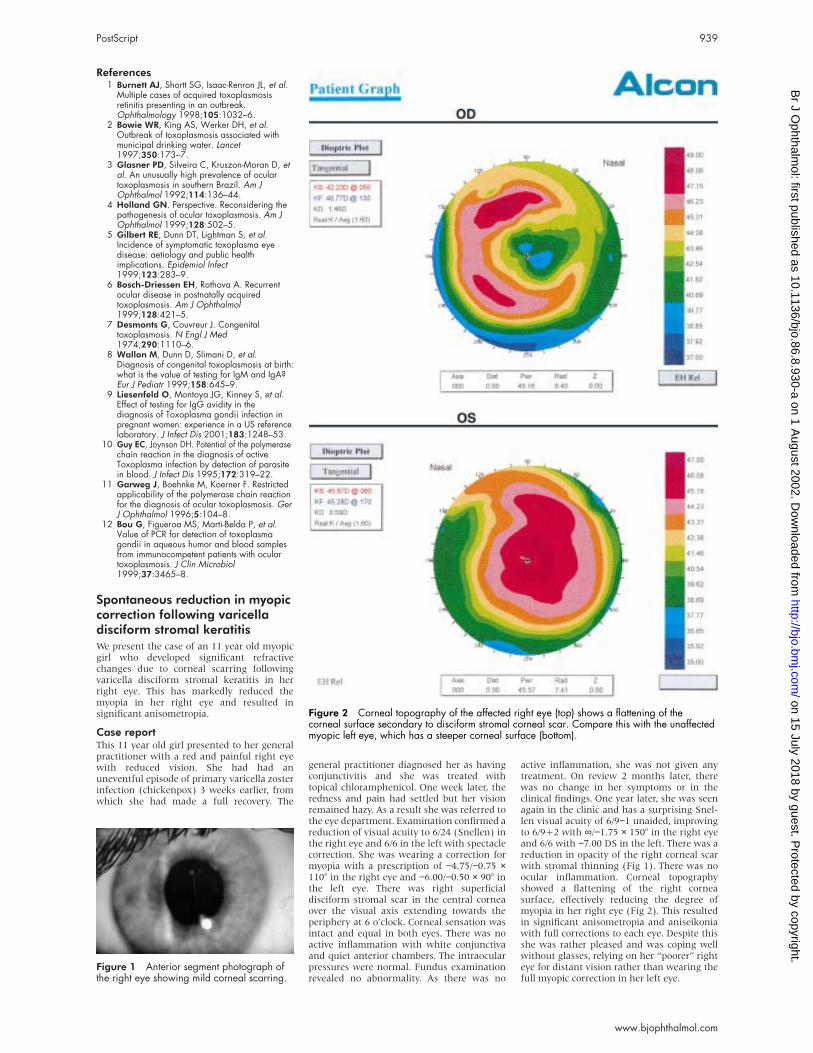
active inflammation, she was not given anytreatment. On review 2 months later, therewas no change in her symptoms or in theclinical findings. One year later, she was seenagain in the clinic and has a surprising Snel-len visual acuity of 6/9−1 unaided, improvingto 6/9+2 with ∞/−1.75 × 150° in the right eyeand 6/6 with −7.00 DS in the left. There was areduction in opacity of the right corneal scarwith stromal thinning (Fig 1). There was noocular inflammation. Corneal topographyshowed a flattening of the right corneasurface, effectively reducing the degree ofmyopia in her right eye (Fig 2). This resultedin significant anisometropia and aniseikoniawith full corrections to each eye. Despite thisshe was rather pleased and was coping wellwithout glasses, relying on her “poorer” righteye for distant vision rather than wearing thefull myopic correction in her left eye.
Figure 1 Anterior segment photograph ofthe right eye showing mild corneal scarring.
Figure 2 Corneal topography of the affected right eye (top) shows a flattening of thecorneal surface secondary to disciform stromal corneal scar. Compare this with the unaffectedmyopic left eye, which has a steeper corneal surface (bottom).
PostScript 939
www.bjophthalmol.com
on 15 July 2018 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.86.8.930-a on 1 August 2002. D
ownloaded from
CommentThis is an unusual case of spontaneousmyopia correction following corneal scarringsecondary to varicella zoster disciform stro-mal keratitis. Primary varicella zoster infec-tion (chickenpox) is a diffuse vesicular skinrash mainly affecting children and is usuallyself limiting. Common ocular findings areeyelid vesicles or marginal erosions and acuteconjunctivitis.1 Corneal changes are infre-quent but can occur during the first week ortwo after the onset of chickenpox. Disciformstromal keratitis is an unusual but well recog-nised complication of primary varicella zosterinfection.2 3 Varicella viral antigen and intra-cellular viral inclusions has been found in thecorneal epithelium of affected eyes. Wilhemuset al reported five cases and reviewed theliterature and found that this condition istypically unilateral, has a delayed onset,typically several weeks after the onset of skinrash.4 The complications following disciformstromal keratitis identified in this review arecorneal scarring, neurotrophic keratopathy,iridocyclitis with secondary glaucoma, andiris stromal atrophy. The principal cause ofloss of vision is corneal scarring. In our case,the corneal scarring had resulted in theflattening of the corneal surface thus reduc-ing the degree of myopia significantly. Thiswas highly unusual and had contributed toimproving the unaided visual acuity in heraffected eye. The effect on the cornea wassimilar to post LASIK (laser assisted in situkeratomileusis) and PRK (photorefractivekeratectomy) in that the cornea appearancewas similar as was the topography. Inaddition, the degree of cornea haze waslimited and there had been a degree of stabil-ity for a period of over 1 year.
She was unable to tolerate the full refractivecorrections because of the significant ani-sometropia and aniseikonia. Despite this shewas pleased as she can see 6/9 unaided andwould rather not wear her rather high myopicspectacle correction. In view of her young age,the uncertainty of the long term stability ofher refractive state and her lack of visualcomplaint, contact lens and refractive surgerywere not considered as appropriate treatmentat present. However, they may have possibleroles in her future management.
Topical corticosteroid therapy and antiviralagents have a role in the management of her-petic stromal disease following herpes sim-plex and herpes zoster infection.5 However,their roles in the treatment of stromal kerati-tis following primary varicella zoster are con-troversial and have not been determined.4 Inour patient, the keratitis settled despitehaving neither topical corticosteroid nor anti-viral agent.
Y F Choong, N R HawksworthEye Department, Royal Glamorgan Hospital,
Ynysmaerdy, Llantrisant, CF72 8XR, UK
Accepted for publication 29 October 2001
References1 Liesegang TJ. The varicella-zoster virus:
systemic and ocular features. J Am AcadDermatol 1984;11(2 Pt 1):165–91.
2 Uchida Y, Kaneko M, Hayashi K. Varicelladendritic keratitis. Am J Ophthalmol1980;89:259–62.
3 Nesburn AB, Borit A, Pentelei-Molnar J, et al.Varicella dendritic keratitis. Invest Ophthalmol1974;13:764–70.
4 Wilhelmus KR, Hamill MB, Jones DB.Varicella disciform stromal keratitis. Am JOphthalmol 1991;111:575–80.
5 McGill J. The enigma of herpes stromaldisease. Br J Ophthalmol 1987;71:118–25.
Presumed ocular candidiasis indrug misusers after intravenoususe of oral high dosebuprenorphine (Subutex)Heroin drug misusers are a high risk group fordisseminated candidiasis.1 Recently, an oralsubstitute for heroin with oral methadone orhigh dose sublingual buprenorphine tablets(Subutex) (HDSB) has proved to be effectivein management of opioid addiction.2 Wereport the first four cases of presumedcandida endophthalmitis following intra-venous injection of HDSB.
Case reportsCase 1A 22 year old man, HIV negative, formerheroin misuser, was seen complaining ofblurry vision in his right eye. He used HDSBintravenously, after dissolution in saliva. Oneweek following an injection, he presentedwith a febrile septicaemic syndrome associ-ated with scalp nodules. Funduscopy revealeda moderate vitritis and a white tiny perifoveo-lar lesion with few white snowballs (Fig 1).The bacterial and fungal cultures from bothblood and anterior chamber tap were nega-tive. Treatment was begun with intravenousfluconazole associated with three intravitrealamphotericin B injections (IVT). After 15 daysof therapy, he was discharged on oral flucona-zole. Ten days later, the endophthalmitisrelapsed with development of a secondparamacular necrotising lesion. A posteriorvitrectomy was performed. The vitreous cul-tures were negative for Candida albicans. Hewas treated again with intravenous ampho-tericin B, along with amphotericin B IVT withsuccess.
Case 2A 27 year old man, a former heroin misuser,was receiving HDSB substitution therapy.
Occasionally, he injected a preparation ofHDSB diluted with preserved lemon juice. Twoweeks following such an injection, he devel-oped a skin abscess in which cultures revealedC albicans, posterior cervical lymphadenopa-thy, nodules of the scalp, and arthritis of theleft wrist. Three weeks later he complained ofdecreased vision in his right eye. Funduscopyrevealed a yellowish-white macular lesion andfew white snowballs (Fig 2) Treatment wasinstituted with intravenous amphotericin Band flucytosine but the patient left the hospi-tal against medical advice 4 days later.
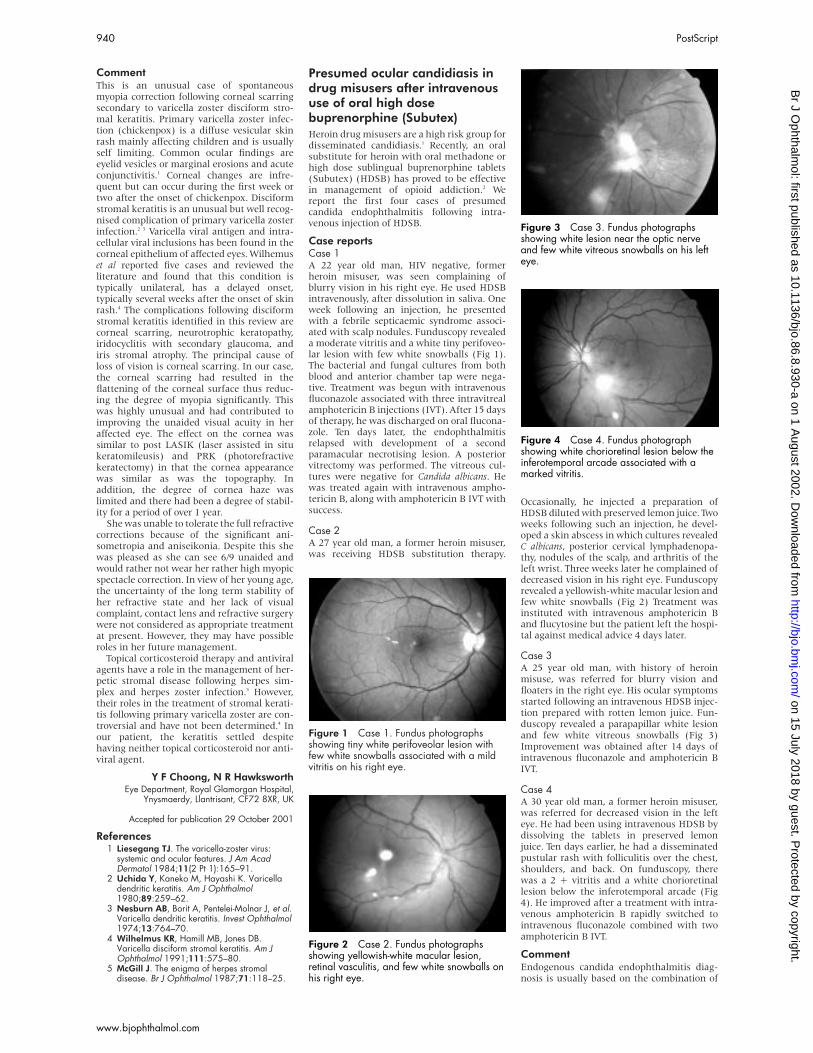
Case 3A 25 year old man, with history of heroinmisuse, was referred for blurry vision andfloaters in the right eye. His ocular symptomsstarted following an intravenous HDSB injec-tion prepared with rotten lemon juice. Fun-duscopy revealed a parapapillar white lesionand few white vitreous snowballs (Fig 3)Improvement was obtained after 14 days ofintravenous fluconazole and amphotericin BIVT.
Case 4A 30 year old man, a former heroin misuser,was referred for decreased vision in the lefteye. He had been using intravenous HDSB bydissolving the tablets in preserved lemonjuice. Ten days earlier, he had a disseminatedpustular rash with folliculitis over the chest,shoulders, and back. On funduscopy, therewas a 2 + vitritis and a white chorioretinallesion below the inferotemporal arcade (Fig4). He improved after a treatment with intra-venous amphotericin B rapidly switched tointravenous fluconazole combined with twoamphotericin B IVT.
CommentEndogenous candida endophthalmitis diag-nosis is usually based on the combination of
Figure 1 Case 1. Fundus photographsshowing tiny white perifoveolar lesion withfew white snowballs associated with a mildvitritis on his right eye.
Figure 2 Case 2. Fundus photographsshowing yellowish-white macular lesion,retinal vasculitis, and few white snowballs onhis right eye.
Figure 3 Case 3. Fundus photographsshowing white lesion near the optic nerveand few white vitreous snowballs on his lefteye.
Figure 4 Case 4. Fundus photographshowing white chorioretinal lesion below theinferotemporal arcade associated with amarked vitritis.
940 PostScript
www.bjophthalmol.com
on 15 July 2018 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.86.8.930-a on 1 August 2002. D
ownloaded from

clinical setting (febrile septicaemia following
an intravenous injection, skin typical lesions)
and typical fundus lesions.3 Isolation of the
fungus from a vitrectomy specimen could
provide a definitive diagnosis but this is not
routinely performed or required.4 In our cases,
the diagnosis of presumed candida endoph-
thalmitis was based on (1) the characteristic
clinical setting, (2) the typical ocular involve-
ment that was characterised by creamy-white
chorioretinal lesions with white balls and vit-
ritis, and (3) the response to antifungal
therapy. Vitrectomy was performed only in
one case. It was not performed in three
patients because they presented an isolated
chorioretinitis or associated with a mild
vitritis and a characteristic clinical
presentation.5 6 Patients were treated with
intravenous amphotericin B or intravenous
fluconazole and intravitreal injections of
amphotericin B, except in one patient who
refused intraocular injections.
In the mid-1980s, in France, an outbreak of
candidiasis followed the introduction on the
drug market of a new brown heroin.7 The
hypothesis that the lemon juice used to
dissolve the heroin might have been contami-
nated with C albicans was demonstrated.8 Our
cases also seem to confirm that the fungi
probably come from the lemon juice or the
patient himself rather than from the bu-
prenorphine itself. Since March 1995,
substitution therapy with HDSB tablets
(Subutex) is approved for licence in France.
Unfortunately, 8% of the patients enrolled in
substitution programmes continued to use
the intravenous route.9 This drug is now
widely prescribed in France. Recently,
in Europe, this treatment obtained the
authorisation for commercialisation in 13
European countries. Our report demonstrates
the need to inform general practitioners,
pharmacists, and patients of the risks in-
volved with the intravenous use of substitute
agents.
N Cassoux, B Bodaghi, P LehoangDepartment of Ophthalmology, Pitié-SalpêtrièreHospital 47–83 bd de l’Hôpital, 75651 Paris,
cedex 13, Paris, France
Y EdelDepartment of Public Health, ECIMUD (Hospitalised
Drug Abusers Medical and Psychiatric SupportTeam) Pitié-Salpêtrière Hospital 47–83 bd de
l’Hôpital, 75651 Paris, cedex 13, Paris, France
Correspondence to: Phuc Lehoang;[email protected]
Accepted for publication 6 March 2002
References1 Mellinger M, De Beauchamp O, Gallien C,
et al. Epidemiological and clinical approachto the study of candidiasis caused by Candidaalbicans in heroin addicts in the Paris region:analysis of 35 observations. Bull Narc1982;34:61–81.
2 Bouchez J, Beauverie P, Touzeau D.Substitution with buprenorphine in methadone-and morphine sulfate-dependent patients.Preliminary results. Eur Addict Res1998;4(Suppl 1):8–12.
3 Aguilar GL, Blumenkrantz MS, Egbert PR, etal. Candida endophthalmitis after intravenousdrug abuse. Arch Ophthalmol1979;97:96–100.
4 Pettit T, JE Edwards, EP Purdy, et al.Endogenous fungal endophthalmitis. In:Pepose J, Holland G, Wilhelmus K, eds.Ocular infection and immunity. St Louis:Mosby, 1996:1262–85.
5 Barza M. Treatment options for candidalendophthalmitis. Clin Infect Dis1998;27:1134–6.
6 Martinez-Vazquez C, Fernandez-Ulloa J,Bordon J, et al. Candida albicansendophthalmitis in brown heroin addicts:response to early vitrectomy preceded andfollowed by antifungal therapy. Clin Infect Dis1998;27:1130–3.
7 Dupont B, Drouhet E. Cutaneous, ocular, andosteoarticular candidiasis in heroin addicts:new clinical and therapeutic aspects in 38patients. J Infect Dis 1985;152:577–91.
8 Leen CL, Brettle RP. Fungal infections in drugusers. J Antimicrob Chemother 1991;28(SupplA):83–96.
9 Bouchez J, Vignau J. The Frenchexperience—the pharmacist, generalpractitioner and patient perspective. EurAddict Res 1998;4(Suppl 1):19–23.
Aetiology of microbial keratitisin northern TanzaniaThe incidence of corneal blindness caused bymicrobial keratitis in the developing world isfar higher than that in the developed world.1
Microbial keratitis has become a more promi-nent cause of corneal blindness in east Africaas the uptake of measles immunisation
improves, reducing measles keratitis scarring,
and with improved recognition and treatment
of vitamin A deficiency, reducing its associ-
ated xerophthalmia and subsequent corneal
scarring.
It has been shown that in tropical climates,
keratitis of fungal aetiology is much more
prevalent than in temperate climates.2 3 Little
information is available about microbial
keratitis in east Africa. The aim of this study
was to identify the causative organisms of the
condition seen in patients presenting to the
Kilimanjaro Christian Medical Centre
(KCMC) hospital in northern Tanzania, east
Africa. KCMC is one of the largest hospitals
in Tanzania, situated on the foothills ofMount Kilimanjaro, serving five regions innorthern and central Tanzania—Kilimanjaro,Arusha, Singida, Tanga, and Dodoma with apopulation of approximately eight millionpeople.
Clinical casesPatients referred to, or presenting for the firsttime to, KCMC with clinical signs of microbialkeratitis, were prospectively recruited to thestudy, between May 1997 and April 1998.
Table 1 Details of 44 patients presenting with microbial keratitis at KCMC
Characteristics Range Median
Age (years) 8–97 44Time from onset of symptoms to presentation (days) 1–90 10
Number %
SexMale 29 65.9Female 15 34.1
OccupationAgricultural 22 50Student/school 6 13.6Driver/conductor 4 9.1Maasai* 4 9.1Retired 4 9.1Soldier/guard 1 2.3Miner 1 2.3Teacher 1 2.3Businessman 1 2.3
Treatment before presentation at KCMC of all cases (culture negative cases only)Nil 11 (6) 25Local remedy 4 (2) 9.1Inappropriate treatment 3 (1) 6.8“Appropriate”† treatment, inadequate intensity 18 (5) 40.9“Appropriate”† treatment 4 (2) 9.1Unknown 4 (2) 9.1
HistoryVegetative trauma 14 32All trauma 17 38.6Previous corneal scar 14 32Lid problems 2 4.6Nil 11 25
Organisms culturedFungi
Fusarium solani 4 9.1Fusarium sp 5 11.4Aspergillus fumigatus 1 2.3Cladosporium sp + Bacillus sp 1 2.3Unidentified fungus + Staph epidermidis 1 2.3All fungi 12 27.3
Gram positive bacteriaStaphylococcus epidermidis 3 6.8Staphylococcus aureus 2 4.6
Gram negative bacteriaPseudomonas aeruginosa 6 13.6Proteus sp 1 2.3
No organism cultured 20 45.5
*Tribal herdsmen.†Empirical treatment with broad spectrum topical antibiotic.
PostScript 941
www.bjophthalmol.com
on 15 July 2018 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.86.8.930-a on 1 August 2002. D
ownloaded from

Patients with corneal ulceration without
infiltration were excluded. These consisted of
three patients with herpes simplex keratitis,
two patients with Mooren’s ulcer, and one
patient with a neurotrophic ulcer. Two pa-
tients with secondary infection of a recent
penetrating corneal injury were excluded. Two
children were unable to undergo slit lamp
examination and corneal scraping for micro-
biology specimens and were also excluded
from the study.
Forty four corneal ulcers were seen.
Thirty eight of the patients had visual acuity
in the affected eye of 6/60 or worse, and the
mean greatest diameter of the infiltrate on
presentation was 5.1 mm. Organisms were
cultured from 24 of the 44 ulcers (54.6%).
Fifty per cent of positive cultures were fungal.
Larger diameter ulcers were more likely to be
culture positive and have poorer outcomes:
mean ulcer diameter was 6.0 mm in culture
positive ulcers and 3.7 mm in culture
negative ulcers. Fungal growth had been pre-
dicted by positive microscopy for fungal
elements in nine of the 12 cases that grew
fungi (75%), and there was never positivefungal microscopy without fungal growth.All five Gram positive isolates had had Grampositive cocci identified on Gram staininginitially but, in contrast, there were threecases where Gram positive cocci were initiallyseen on Gram staining, but cultures hadgrown other organisms (two fungi, one Gramnegative bacilli). Full details are shown inTable 1.
CommentIn this study fungal keratitis accounted for50% of culture positive cases of microbialkeratitis in northern Tanzania, with themajority of these cases (42%) yielding purefungal isolates on culture. These figures aresimilar to those published from west Africa,where 56% of microbial keratitis was causedalone or in part by fungi.3 As in studies fromthe United States,4 west Africa,3 and southernIndia,2 the most common genus of fungusisolated was that of the filamentous fungusFusarium.
There may have been a bias towards fungalulcers in this study. KCMC is a referral centre,receiving severe ulcers from primary care cen-tres, where topical antibacterial treatmentsare generally available and topical antifungaltreatments are generally not. If the culturenegative ulcers were predominantly bacterialulcers, the relative frequency of fungal kerati-tis in this study would be artificially high.However culture negative ulcers had had asimilar range of treatments to culture positiveulcers before presenting to KCMC, as can beseen from Table 1. There is no evidence to sug-gest the culture negative ulcers were predomi-nantly of (treated) bacterial rather thanfungal aetiology.
Study design limitations precluded anyestimation of prevalence of microbial kerati-tis in the region, which would have been use-ful. The findings relate to northern and partof central Tanzania; with a similar climate,risk factors and primary care set up, theaetiology of microbial keratitis is likelyto be similar in the wider region. The studyset out to test for acanthamoeba antigen aspart of the microbiological examination, butthis became impossible after logistical diffi-culties.
The most important factor in outcome wasthe initial size of the ulcer on examination.Larger ulcers were more likely to be culture
positive and to have a poor outcome, such as a
blinding corneal scar or requiring eviscera-
tion. Culture results were nevertheless useful
in ascertaining antibiotic sensitivities, and in
adding antifungal treatment where necessary.
Any patient undergoing evisceration had usu-
ally been an inpatient for several weeks with a
painful blind eye, had tried multiple treat-
ment regimens, and had often requested evis-
ceration himself. The overall rate of eviscera-
tion was 25%. Although there is little
published material on outcomes of microbial
keratitis in the developing world, this figure
compares with a series of culture positive
fungal ulcers in Madurai, India, where 20%
were classified as “severe, with little prospect
of recovery”.5
Clearly, awareness of proper treatment
regimens in northern Tanzania is paramount,
particularly at the place of first contact, the
village health centre, to prevent this overall
picture of severe corneal ulcers with very
poor visual prognosis. Treatment regimens
should also take into account the high
proportion of fungal keratitis. Microscopy
looking specifically for fungal elements is a
simple, quick, and useful test that could help
direct initial treatment, along with clinical
appearances suggestive of fungal infection.
This might be more economically viable
and practical than blanket coverage of all
keratitis with an antifungal topical treatment
in the first line therapy. Unfortunately
consistently effective antifungal topical treat-
ments are not widely available in this part of
Africa.
Future studies could examine the efficacy
of current treatments for fungal keratitis and
how best to improve awareness of appropriate
treatment regimens in the region.
Acknowledgements
This work was supported by grants from the British
Council for the Prevention of Blindness and The
Ulverscroft Foundation.
We are grateful to the hospital director, the staff, and
the patients of KCMC for their collaboration in the
above study.
T R G Poole, D L HunterDepartment of Ophthalmology, Kilimanjaro
Christian Medical Centre, Moshi, Tanzania, Africa
E M K MaliwaDepartment of Microbiology
A R C RamsayClinical Laboratory
Correspondence to: Mr Poole; [email protected] for publication 10 April 2002
References1 Whitcher JP, Srinivasan M. Corneal
ulceration in the developing world—a silentepidemic. Br J Ophthalmol 1997;81:622–3.
2 Srinivasan M, Gonzales CA, George C, etal. Epidemiology and aetiological diagnosisof corneal ulceration in Madurai, south India.Br J Ophthalmol 1997;81:965–71.
3 Hagan M, Wright E, Newman M, et al.Causes of suppurative keratitis in Ghana. Br JOphthalmol 1995;79:1024–8.
4 Leisegang TJ, Forster RK. Spectrum ofmicrobial keratitis in South Florida. Am JOphthalmol 1980;90:38–47.
5 Rahman MR, Minassian DC, Srinivasan M, etal. Trial of chlorhexidine gluconate for fungalcorneal ulcers. Ophthalmic Epidemiol1997;4:141–9.
BOOK REVIEW
Oculoplastic Surgery Atlas. Eyelid Disor-ders. Eds Geoffrey J Gladstone, Evan H
Black, Shoib Myint, Brian G Brazzo. Pp 130;£66.50. Heidelberg: Springer-Verlag, 2001.ISBN 0-387-95316-7.
This CD video atlas with accompanying text isthe first in a series of three such atlases bythese authors and is the first such oculoplasticatlas available. The atlas consists of 95 pagesof text supplemented with black and whitedrawings in six chapters. Two CDs contain allthe video sequences and these follow thesame chapter layout as the text; surgical anat-omy of the eyelid, entropion, ectropion, eyelidretraction, ptosis, and eyelid reconstruction.
There are a total of 17 video procedurestypically lasting between 3 and 5 minutes anda 10 minute cadaveric anatomy sequence. Thevideo quality is very acceptable for individualviewing but does not project as successfully.All sequences are well narrated and informa-tive, covering basic and some more advancedoculoplastic procedures. The need for free skingrafting in one of the cases demonstrated isperhaps questionable but this does not detractfrom the educational value of the atlas. Anumber of associated procedures are coveredin the videos—for example, harvesting skin/cartilage; however, these cannot be instantlylocated from the menus and an additionalseparate section including such procedurescould perhaps have been usefully included.
The text is clearly written and concise but isnot comprehensive and provides limitedinformation relating to patient and procedureselection. A good deal of the text is covered inthe narration accompanying the video.
The atlas is aimed at all those who have aninterest in oculoplastic surgery but is particu-larly relevant to the ophthalmic surgeon. Itwill be a valuable asset for teaching residentsand fellows and should make interestingviewing for all those routinely practising ocu-loplastic surgery.
From a personal point of view, I am alwaysfascinated to watch other surgeons at work, astechnical approaches to the same problem/operation are often quite diverse. This is one ofthe best ways to keep up to date and improveyour own surgery.
Overall, this atlas will be a valuable asset toall those in training and a useful tool for thosepractising oculoplastic surgical procedures. Ilook forward to the next two atlases in theseries and to further editions.
Garry Shuttleworth
NOTICES
Patient careThe latest issue of Community Eye Health (No41) discusses patient care with both ophthalo-molgists’ and patients’ views given. Forfurther information please contact: Journal ofCommunity Eye Health, International Centre
942 PostScript
www.bjophthalmol.com
on 15 July 2018 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.86.8.930-a on 1 August 2002. D
ownloaded from

for Eye Health, Institute of Ophthalmology,11–43 Bath Street, London EC1V 9EL, UK (tel:+44 (0)20 7608 6910; fax: +44 (0)20 72503207; email: [email protected]; website:www.jceh.co.uk). Annual subscription (4 is-sues) UK£25/US$40. Free to workers in devel-oping countries.
International Centre for EyeHealthThe International Centre for Eye Health haspublished a new edition of the Standard List ofMedicines, Equipment, Instruments and OpticalSupplies (2001) for eye care services indeveloping countries. It is compiled by theTask Force of the International Agengy for thePrevention of Blindness. Further details: SueStevens, International Centre for Eye Health,11–43 Bath Street, London EC1V 9EL, UK (tel:+44 (0)20 7608 6910; email: [email protected]).
Second SightSecond Sight, a UK based charity whose aimsare to eliminate the backlog of cataract blindin India by the year 2020 and to establishstrong links between Indian and British oph-thalmologists, is regularly sending volunteersurgeons to India. Details can be found at thecharity website (www.secondsight.org.uk) orby contacting Dr Lucy Mathen ([email protected]).
SPecific Eye ConditionS (SPECS)SPecific Eye ConditionS (SPECS) is a not forprofit organisation which acts as an umbrellaorganisation for support groups of any condi-tions or syndrome with an integral eye disor-der. SPECS represents over fifty differentorganisations related to eye disorders rangingfrom conditions that are relatively common tovery rare syndromes. We also include groupswho offer support of a more general nature tovisually impaired and blind people. Support
groups meet regularly in the Boardroom atMoorfields Eye Hospital to offer support toeach other, share experiences and explore newways of working together. The web sitewww.eyeconditions.org.uk acts as a portalgiving direct access to support groups ownsites. The SPECS web page is a valuableresource for professionals and may also beof interest to people with a visual impairmentor who are blind. For further details aboutSPECS contact: Kay Parkinson, SPECS Devel-opment Officer (tel: +44 (0)1803 524238;email: [email protected]; www.eyeconditions.org.uk).
The British Retinitis PigmentosaSocietyThe British Retinitis Pigmentosa Society(BRPS) was formed in 1975 to bring togetherpeople with retinitis pigmentosa and theirfamilies. The principle aims of BRPS are toraise funds to support the programme ofmedical research into an eventual cure for thishereditary disease, and through the BRPSwelfare service, help members and their fami-lies copy with the everyday concerns causedby retinitis pigmentosa. Part of the welfareservice is the telephone helpline (+44(0)1280 860 363), which is a useful resourcefor any queries or worries relating to theproblems retinitis pigmentosa can bring. Thisservice is especially valuable for those recentlydiagnosed with retinitis pigmentosa, and allcalls are taken in the strictest confidence.Many people with retinitis pigmentosa havefound the Society helpful, providing encour-agement, and support through the Helpline,the welfare network and the BRPS branchesthroughout the UK. (tel: +44 (0)1280 821334; email: [email protected]; website: www.brps.demon.co.uk)
Ophthalmic Anesthesia Society(OAS) 16th Scientific MeetingThe 16th Scientific Meeting of the OAS will beheld on 4–6 October 2002 in The Westin,
Michigan Avenue, 909 North Michigan Av-enue, Chicago, USA (reservations +1 800 2283000). Further details: OAS, 793-A FoothillBlvd, PMB 110, San Luis Obispo, CA 93405,USA (tel: +1 805 771 8300; web site: www.eyeanesthesia.org).
BEAVRS MeetingThe next BEAVRS meeting will be held in theDalmahoy Hotel near Edinburgh on 31 Octoberto 1 November 2002. Further details: SusanCampbell, Medical Secretary, Gartnavel Gen-eral Hospital (email: [email protected]).
Cornea 2002—Celebrating 50Years of EyebankingThe Cornea 2002 meeting will be held in LeMeridien Hotel, London, Gatwick on 14–15November 2002. Subjects to be covered willinclude eye banking, penetrating and lamellarkeratoplasty, stem cell restoration, keratopros-thesis, advanced keratoplasty techniques, pae-diatric cornea, keratorefractive surgery, andintraocular refractive surgery. Spaces are lim-ited and a beneficial package rate is availableprior to 30 September 2002. Further details:CORNEA 2002 organiser at the Corneo PlasticUnit, The Queen Victoria Hospital, HoltyeRoad, East Grinstead, West Sussex, RH19 3DZ(tel: 01342 410 210 ext 560; fax: 01342 317181; email: [email protected]).
CORRECTION
An error occurred in the article: Bilateralcircumscribed haemangioma of the choroidnot associated with systemic vascular syn-drome. Br J Ophthalmol 2001;85:1260. Theauthors should have been listed as P Perri, CIncorvaia, C Costagliola, F Parmeggiani, GLamberti, B Paduano, A Sebastiani.
PostScript 943
www.bjophthalmol.com
on 15 July 2018 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.86.8.930-a on 1 August 2002. D
ownloaded from





























