Embed Size (px)
Citation preview

25ACQUIRED AND CONGENITAL HEMOSTATIC DISORDERS IN
PREGNANCY AND THE PUERPERIUM
R. V. Ganchev and C. A. Ludlam
During normal pregnancy, a series of progres-sive changes in hemostasis occur that are overallprocoagulant and help prevent excessive bleed-ing at the time of delivery. The concentrationsof coagulation factors V, VII, VIII, IX, X, XIIand von Willebrand factor (vWF) rise signifi-cantly (Table 1) and are accompanied by a pro-nounced increase in fibrinogen levels (up totwo-fold from non-pregnant levels). Factor XIIIlevels tend to decrease in late pregnancy after aninitial increase in the beginning of pregnancy.Markers of coagulation activation such asprothrombin fragments (PF1+2), thrombin–antithrombin complexes (TAT) and D-dimerare increased, while a decrease in physiologicalanticoagulants is manifested by a significantreduction in protein S activity and acquiredactivated protein C (APC) resistance. Fibrinoly-sis is inhibited not only by the rise in endothe-lium-derived plasminogen activator inhibitor-1(PAI-1) but also by placenta-derived PAI-2.Microparticles derived from maternal endo-thelial cells and platelets, and from placental
trophoblasts may contribute to the pro-coagulant effect1. Although concentrations ofsoluble tissue factor (TF) remain constantduring normal pregnancy2, monocyte TFactivity and expression are lower whencompared with those in non-pregnant women,possibly acting to counterbalance the pro-coagulant changes3,4. Local hemostasis at theplacental trophoblast level is characterized byincreased TF expression and low expressionof tissue factor pathway inhibitor (TFPI)1.Approximately 4 weeks’ post-delivery, thehemostatic system returns to that of thenon-pregnant state5.
Although the overall balance shifts towardshypercoagulability, occasionally medical condi-tions coincident with pregnancy and complica-tions of pregnancy itself put excessive demandson maternal physiology and may result in ableeding tendency. This chapter describesacquired and congenital hemostatic disordersthat may lead to hemorrhagic complications inthe obstetric patient.
209
Increased Decreased No change
Systemic changesProcoagulant factorsAnticoagulant factorsAdhesive proteinsFibrinolytic proteinsTissue factor (TF)Microparticles (MP)
I, V, VII, VIII, IX, X, XIIsoluble TMvWFPAI-1, PAI-2
MP
XIIIPS
t-PAmonocyte TF
PC, AT
soluble TF
Local placental changes TF TFPI
TM, thrombomodulin; PS, protein S; PC, protein C; AT, antithrombin; vWF, von Willebrand factor; PAI,plasminogen activator inhibitor; t-PA, tissue plasminogen activator; TFPI, tissue factor pathway inhibitor.Adapted from Brenner B. Haemostatic changes in pregnancy. Thromb Res 2004;114:409–14
Table 1 Coagulation system changes in normal pregnancy
231Z:\Sapiens Publishing\A5211 - Postpartum Hemorrhage\Make-up\Postpartum Hemorrhage - Voucher Proofs #T.vp30 August 2006 14:21:07
Color profile: Generic CMYK printer profileComposite Default screen

ACQUIRED DISORDERS OFHEMOSTASIS
Thrombocytopenia
Thrombocytopenia is the most common hemo-static abnormality and may complicate up to10% of all pregnancies. The normal plateletcount ranges from 150 to 400 × 109/l, andthrombocytopenia is defined as a count ofless than 150 × 109/l. The platelet count maydecline by approximately 10% during normalpregnancy6. Spontaneous bleeding is unusualunless the count has fallen to below 30 × 109/l,but surgical bleeding or postpartum hemor-rhage may occur as a consequence of plateletsless than 50 × 109/l. Thrombocytopenia in preg-nancy may result from variety of causes (Table2). The timing of onset of these disordersduring pregnancy and their clinical manifesta-tions often overlap, making the identificationof individual causes of thrombocytopeniasometimes problematic.
It is important to consider spurious thrombo-cytopenia as a possible cause of decreasedplatelet count before embarking on extensiveinvestigations or treatment. This is a laboratoryartefact due to EDTA-induced platelet aggrega-tion in vitro and can be diagnosed by visualinspection of the blood film, when plateletchanges are readily visible.
Gestational thrombocytopenia
Gestational, or incidental, thrombocytopenia(GT) is the most common cause of
thrombocytopenia in pregnancy, affecting 5%of all pregnant women and accounting for morethan 75% of cases of pregnancy-associatedthrombocytopenia7,8. It presents as a mild tomoderate thrombocytopenia (100–150 × 109/l),which is detected incidentally often for the firsttime during the third trimester of pregnancy.The platelet count returns to normal within 7days of delivery. GT is the physiologic thrombo-cytopenia that accompanies normal pregnancyand is thought to be due to hemodilution and/oraccelerated platelet clearance7,8. It is an entirelybenign condition, which is not associated withmaternal hemorrhage or fetal or neonatalthrombocytopenia. It is, however, necessary tomonitor the platelet count during pregnancyand, if it falls below 100 × 109/l, the diagnosismust be reviewed. Rare cases, subsequentlyconfirmed as GT, have had counts as low as50 × 109/l9. Epidural anesthesia is consideredsafe if the maternal platelet count is greater than80 × 109/l. Delivery should proceed accordingto obstetric indications and the cord plateletcount should be checked. GT is difficult todistinguish from idiopathic thrombocytopenicpurpura, when thrombocytopenia is identifiedfor the first time during pregnancy and noprevious counts have been documented.
Idiopathic thrombocytopenic purpura
Idiopathic thrombocytopenic purpura (ITP)accounts for one to five cases of thrombocyto-penia per 10 000 pregnancies10 and 5% of casesof pregnancy-associated thrombocytopenia7; it
210
POSTPARTUM HEMORRHAGE
Pregnancy-specific Not pregnancy-specific
Gestational (incidental) thrombocytopeniaPre-eclampsiaHELLP syndrome (hemolysis, elevated liver enzymes
and low platelets)Acute fatty liver of pregnancy (AFLP)
Idiopathic thrombocytopenic purpura (ITP)Thrombotic thrombocytopenic purpura (TTP)Hemolytic uremic syndrome (HUS)Systemic lupus erythematosusViral infection (HIV, CMV, EBV)Antiphospholipid antibodiesConsumptive coagulopathyDrug-induced thrombocytopeniaType 2B von Willebrand diseaseCongenital
From McCrae KR. Thrombocytopenia in pregnancy: differential diagnosis, pathogenesis and management.Blood Rev 2003;17:7–14
Table 2 Causes of pregnancy-associated thrombocytopenia
232Z:\Sapiens Publishing\A5211 - Postpartum Hemorrhage\Make-up\Postpartum Hemorrhage - Voucher Proofs #T.vp30 August 2006 14:21:08
Color profile: Generic CMYK printer profileComposite Default screen

is the most common cause of significantthrombocytopenia in the first trimester. ITP ischaracterized by premature clearance of plate-lets by antiplatelet antibodies and consequentincreased production of platelets by the bonemarrow. The most common presentation is thefinding of an asymptomatic thrombocytopeniaon a routine blood count, when the distinctionfrom GT may be difficult. Patients occasionallypresent for the first time with severe thrombo-cytopenia in pregnancy, and women withpreviously diagnosed ITP often experience anexacerbation in pregnancy11. Symptomaticpatients present with minor bruises orpetechiae, bleeding from mucosal surfaces, orrarely fatal intracranial bleeding.
As in the non-pregnant patient, ITP is a diag-nosis of exclusion with thrombocytopenia andnormal or increased megakaryocytes in the bonemarrow in the absence of other causes. There isno confirmatory laboratory test, and documen-tation of a low platelet count outside pregnancyis invaluable. Practically, however, in theabsence of a platelet count prior to pregnancy,significant thrombocytopenia (< 100 × 109/l) inthe first trimester, with a declining plateletcount as gestation progresses, is most consistentwith ITP. In contrast, mild thrombocytopeniadeveloping in the second or the third trimesterand not associated with hypertension orproteinuria most likely represents GT12. Bonemarrow examination is unnecessary unlessthere is suspicion of leukemia, lymphoma ormalignant infiltration.
The decision to treat a pregnant woman withITP is based on assessment of the risk of signifi-cant maternal hemorrhage. The count usuallyfalls as pregnancy progresses, with a nadir in thethird trimester11, and active treatment may haveto be instituted to ensure a safe platelet countat the time of delivery. The incidence of ante-partum hemorrhage is not increased in maternalITP, but there is a small increased risk of post-partum hemorrhagic complications, not fromthe placental bed but from surgical incisionssuch as episiotomies and from soft-tissuelacerations13.
Asymptomatic patients with platelet counts> 20 × 109/l do not require treatment untildelivery is imminent but should be carefullymonitored. Platelet counts of > 50 × 109/l are
regarded as safe for normal vaginal delivery, andthose > 80 × 109/l are safe for Cesarean section,spinal or epidural anesthesia14.
The major treatment options for maternalITP are corticosteroids or intravenous immuno-globulin (IVIg). There is no evidence, however,that either of these treatment modalities admin-istered to the mother affects the platelet countin the fetus or neonate. If the duration of treat-ment is likely to be short, i.e. starting in thethird trimester, corticosteroids are an effectiveoption. An initial dose of 1 mg/kg prednisolone(based on pregnancy weight) is recom-mended11,14, which can be subsequentlytapered. In addition to their toxicities in non-pregnant individuals, such as osteoporosis andweight gain, corticosteroids increase theincidence of pregnancy-induced hypertensionand gestational diabetes, and may promotepremature rupture of the fetal membranes.
Concerns about potential adverse maternaleffects of steroids have led some to use IVIgas a first-line therapy in pregnancy15,16. Othersreserve this treatment for patients in whomsteroid therapy is likely to be prolonged or inwhom an unacceptably high maintenance doseis required (> 7.5 mg prednisolone daily). Theconventional dose of IVIg is 0.4 g/kg/day for 5days, although 1 g/kg/day for 2 days has beenused successfully and may be more conve-nient11. A persistent and predictable response isobtained in 80% of the cases. The response totherapy usually occurs within 24 h (more rapidthan with steroids) and is maintained for 2–3weeks. After an initial response, repeat singleinfusions can be used to prevent hemorrhagicsymptoms and ensure an adequate plateletcount for delivery.
Therapeutic options for those women withseverely symptomatic ITP refractory to oralsteroids or IVIg include high-dose intravenousmethylprednisolone (1.0 g), perhaps combinedwith IVIg, or azathioprine14, but these shouldonly be considered after careful assessment ofthe potential risks. Splenectomy is now rarelyperformed in pregnancy. It remains an option ifall other attempts to increase the platelet countfail and is best performed in the secondtrimester.
The offspring of mothers with ITP may alsodevelop thrombocytopenia, as a result of the
211
Acquired and congenital hemostatic disorders
233Z:\Sapiens Publishing\A5211 - Postpartum Hemorrhage\Make-up\Postpartum Hemorrhage - Voucher Proofs #T.vp30 August 2006 14:21:08
Color profile: Generic CMYK printer profileComposite Default screen

transplacental passage of maternal antiplateletIgG7,12. The incidence of severe neonatalthrombocytopenia (< 50 × 109/l) has beenreported between 9 and 15%, with intracranialhemorrhage occurring in 0–1.5% of infants17.Due to the inability of maternal clinical charac-teristics to predict neonatal thrombocytopenia,antenatal (cordocentesis) and perinatal (fetalscalp blood sampling) procedures for determi-nation of fetal platelet count have been consid-ered in the past. Cordocentesis carries amortality of 1–2%, however, whereas scalpblood sampling is associated with artefactuallylow results and risk of significant hemorrhage.For these reasons, both procedures are nowlargely abandoned in the management ofITP in pregnancy. The most reliable predictorof fetal thrombocytopenia is a history ofthrombocytopenia at delivery in a priorsibling18.
In view of the very low risk of seriousneonatal hemorrhage, it is now agreed that themode of delivery in ITP should be determinedby purely obstetric indications11,14. If thematernal platelet count remains low at thetime of delivery, despite optimal antenatalmanagement, platelet transfusion may berequired to treat maternal bleeding. Motherswith thrombocytopenia are unlikely to bleedfrom the uterine cavity after the third stageof labor, provided that there are no retainedproducts of conception. However, bleeding mayoccur from surgical wounds, episiotomies orperineal tears. Non-steroidal anti-inflammatorydrugs should be avoided for postpartum analge-sia. ITP should not exclude women fromconsideration for peripartum thrombosis pro-phylaxis. Prophylactic doses of low-molecularweight heparin are generally safe if the plateletcount is greater than 50 × 109/l. Followingdelivery, a cord blood platelet count shouldbe determined in all cases. Since the neonatalplatelet count may decline for 4–5 days afterdelivery11, daily monitoring is indicated. Infantsshould be closely observed and treatment israrely required. In those with clinical hemor-rhage or platelet count < 20 × 109/l, treatmentwith IVIg produces a rapid response. Life-threatening hemorrhage should be managedwith platelet transfusion combined withIVIg11.
Secondary autoimmunethrombocytopenia
Antiphospholipid syndrome
The diagnosis of primary antiphospholipidsyndrome requires the coexistence of clinicalmanifestations (either vascular thrombosis orpregnancy morbidity) with laboratory evidenceof reproducible antiphospholipid antibodies(either lupus anticoagulant or anticardiolipinantibody)19. Primary antiphospholipid syn-drome is associated with autoimmunethrombocytopenia in 20–40% of cases20.Thrombocytopenia is rarely severe and usuallydoes not require treatment. If treatment is nec-essary, management options during pregnancyare similar to those for primary ITP. However,primary antiphospholipid syndrome is associ-ated with recurrent spontaneous abortionsbefore 10 weeks of gestation, and women withthe condition are at risk of intrauterine fetalgrowth restriction or death, pre-eclampsia andmaternal thrombosis19,21.
A combination of low-dose aspirin andlow-dose subcutaneous heparin is helpful inpreventing recurrent spontaneous abortionsin antiphospholipid syndrome22. Antenatal andpostnatal thrombosis prophylaxis is indicated inwomen with antiphospholipid syndrome and ahistory of thrombosis23. Moderate thrombo-cytopenia should not alter decisions aboutantiplatelet or antithrombotic therapy inantiphospholipid syndrome20.
Systemic lupus erythematosus
Immune platelet destruction may occur in sys-temic lupus erythematosus (SLE) because ofantiplatelet antibodies or immune complexes,but thrombocytopenia is seldom severe; lessthan 5% of cases have platelet count< 30 × 109/l during the course of the disease13.Thrombocytopenia is often the first presentingfeature and may precede any other manifesta-tions of the condition by months or years. It isdifficult to document any special effect of preg-nancy on SLE; the general consensus is thatpregnancy does not affect the long-term prog-nosis of SLE, but that pregnancy itself may beassociated with more flare-ups, particularly inthe puerperium24. The management of isolated
212
POSTPARTUM HEMORRHAGE
234Z:\Sapiens Publishing\A5211 - Postpartum Hemorrhage\Make-up\Postpartum Hemorrhage - Voucher Proofs #T.vp30 August 2006 14:21:08
Color profile: Generic CMYK printer profileComposite Default screen

thrombocytopenia associated with SLE in preg-nancy is governed by the principles outlinedfor ITP. Women with SLE are also at risk forpre-eclampsia which may be complicated bythrombocytopenia.
HIV-associated thrombocytopenia
HIV-related thrombocytopenia can be causedby increased platelet destruction by antiplateletantibodies or immune complexes, commonlyduring early-onset HIV. In advanced disease,drugs and infection may lead to marrow dys-function that results in thrombocytopenia.In one series of HIV-positive women, approxi-mately 3% were thrombocytopenic and, inmost cases, thrombocytopenia was believed tobe directly related to HIV infection25. Slightlyfewer than half of the thrombocytopenic womenhad a platelet count < 50 × 109/l, and 20% hadhemorrhagic complications25.
Treatment with antiretroviral therapy tendsto improve the defective thrombopoiesis andincrease the platelet count in HIV-positivepatients, but some antiretroviral drugs may alsocause thrombocytopenia. When immune des-truction is believed to be a significant componentof thrombocytopenia, IVIg may be required totreat hemorrhagic symptoms or to increase theplatelet count before delivery in thrombocyto-penic HIV-positive women25. Corticosteroidsare also effective but may be associated withincreased risk of further immunosuppressionand infection. Thrombotic thrombocytopenicpurpura is found more frequently in HIV-infected patients and should be treatedaccordingly. Cesarean delivery reduces the riskof transmission of HIV from mother to fetus.
Drug-induced thrombocytopenia
Drug-induced thrombocytopenia may becaused by immune- or non-immune-mediatedplatelet destruction or suppression of plateletproduction. Both are uncommon in pregnancy,but drug-induced causes should be consideredand excluded. Drugs which are commonly asso-ciated with thrombocytopenia are shown inTable 3.
A unique form of drug-induced thrombo-cytopenia is heparin-induced thrombocytopenia
(HIT). It occurs in 1–5% of patients receivingunfractionated heparin but is considerably lesscommon in patients treated with low-molecularweight heparins. HIT is caused by an antibodydirected against the heparin–platelet factor 4complex, which can induce platelet activationand aggregation in vivo. Unlike other thrombo-cytopenias, HIT is complicated by arterialand/or venous thrombosis which may be life-threatening. Laboratory tests are available toconfirm the diagnosis. HIT has been reported inpregnancy26,27, although it may be less commonin pregnant than in non-pregnant individuals28.Fetal thrombocytopenia does not occur becauseheparin does not cross the placenta. Heparinshould be withdrawn immediately on clinicalsuspicion of HIT. If ongoing anticoagulation isurgently required, the heparinoid danaparoidmay be used in most patients. Danaparoid hasbeen used successfully to treat HIT in preg-nancy27. Hirudin is an alternative in non-pregnant patients, but experience is limited in
213
Acquired and congenital hemostatic disorders
A. Immune mediatedAcetaminophenAminosalicylic acidAmiodaroneAmphotericin BCimetidineDiclofenacGold/gold saltsLevamisoleMethyldopaQuinine and quinidineRanitidineSulfasalazineVancomycin
B. Unique antibody-mediated processHeparin
C. Suppression of platelet productionAnagrelideValproic acid
D. Suppression of all hematopoietic cellsChemotherapeutic agents
Adapted from George JN, Raskob GE, Shah SR,et al. Drug-induced thrombocytopenia: a systematicreview of published case reports. Ann Intern Med1998;129:886–90
Table 3 Drugs causing thrombocytopenia
235Z:\Sapiens Publishing\A5211 - Postpartum Hemorrhage\Make-up\Postpartum Hemorrhage - Voucher Proofs #T.vp30 August 2006 14:21:08
Color profile: Generic CMYK printer profileComposite Default screen

pregnancy and its use is not recommendedunless there is no suitable alternative29. Platelettransfusion should be avoided in patientswith HIT. Because HIT is potentially life-threatening, all women must have a plateletcount before treatment with heparin begins.The count must be repeated on day 4 of firstexposure to heparin or day 1 of repeat exposureand then at least weekly for the first 3 weeks.
Thrombocytopenia with microangiopathy
Several syndromes are associated with thrombo-cytopenia as a result of platelet activation, redcell fragmentation, and a variable degree ofhemolysis (microangiopathic hemolytic anemia,MAHA). Some syndromes are unique toobstetric practice. The differential diagnosisis particularly pertinent for obstetricians and isimportant because management options differ.The differential diagnosis is summarized inTable 4.
Pre-eclampsia and HELLP syndrome
Pre-eclampsia affects approximately 6% of allpregnancies, most often those of primigravidasless than 20 or greater than 30 years of age7.The criteria for the condition include hyperten-sion and proteinuria > 300 mg/24 h developing
after 20 weeks of gestation6. Although the clini-cal manifestations of pre-eclampsia generally donot become evident until the third trimester, thelesions underlying this disorder occur early inpregnancy and involve deficient remodelling ofthe maternal uterine vasculature by placentaltrophoblast cells30,31. Thrombocytopenia devel-ops in approximately 50% of patients, with theseverity usually proportional to the severity ofthe pre-eclampsia. Occasionally, the onset ofthrombocytopenia precedes other manifesta-tions of pre-eclampsia7. Current understandingof the pathogenesis of thrombocytopenia inpre-eclampsia is that it is due to excessiveplatelet activation, adhesion of platelets todamaged or activated endothelium, and/orclearance of IgG-coated platelets by thereticuloendothelial system7.
Activation of the coagulation cascade occursin most patients with pre-eclampsia; however,screening coagulation tests such as activatedpartial thromboplastin time (APTT), pro-thrombin time (PT) and fibrinogen are usuallynormal. Regardless, more sensitive markers ofhemostatic activity such as D-dimer and TATcomplexes are often elevated. In severepre-eclampsia, the activation of coagulationresults in consumption of clotting factors andtherefore prolongation of the clotting test timesand a fall in plasma fibrinogen.
214
POSTPARTUM HEMORRHAGE
Diagnosis TTP HUS HELLP Pre-eclampsia AFLP
Time of onsetHemolysisThrombocytopeniaCoagulopathyLiver diseaseRenal diseaseHypertensionCNS diseaseEffect of delivery
on diseaseManagement
2nd trimester++++++-±±rare+++none
early plasmaexchange
postpartum++++-±+++±±none
supportive± plasmaexchange
3rd trimester++++±++++±±recovery
supportiveconsider plasmaexchange if persists
3rd trimester+++±±++++±recovery
supportiveplasma exchangerarely required
3rd trimester++/±++++++±±+recovery
supportive
TTP, thrombotic thrombocytopenic purpura; HUS, hemolytic uremic syndrome; HELLP, hemolysis,elevated liver enzymes, and low platelets; AFLP, acute fatty liver of pregnancy.Adapted from Horn EH. Thrombocytopenia and bleeding disorders. In James DK, Steer PJ, Weiner CP,Gonik B, eds. High-Risk Pregnancy: Management Options, 3rd edn, Elsevier, 2006:901–24
Table 4 Differentiation of pregnancy-associated microangiopathies
236Z:\Sapiens Publishing\A5211 - Postpartum Hemorrhage\Make-up\Postpartum Hemorrhage - Voucher Proofs #T.vp30 August 2006 14:21:08
Color profile: Generic CMYK printer profileComposite Default screen

The HELLP (hemolysis, elevated liverenzymes and low platelets) syndrome is oftenconsidered to be a variant of pre-eclampsia andis the most common cause of severe liver diseasein pregnant women32. Criteria for the HELLPsyndrome include microangiopathic hemolyticanemia, aspartate aminotransferase (AST)> 70 U/l and thrombocytopenia, with a plateletcount < 100 × 109/l33. Patients may presentwith severe epigastric and right upper quadrantpain, which need not be accompanied byhypertension and proteinuria. Exacerbation ofHELLP syndrome may occur postpartum andthere is a recurrence risk of approximately 3% insubsequent pregnancies. The syndrome occa-sionally presents postpartum, usually within48 h, but rarely as late as 6 days after delivery.Despite their similarities, HELLP is associatedwith significantly greater maternal and fetalmorbidity and mortality than pre-eclampsia7.
Management of pre-eclampsia/HELLP syn-drome is supportive and should be focused onstabilizing the patient medically prior to earlydelivery of the fetus. Platelet transfusions maybe needed if bleeding occurs or if thrombo-cytopenia is severe and Cesarean delivery isplanned, though the survival time of transfusedplatelets in patients with pre-eclampsia is dimin-ished6. If required, the consumptive coagulo-pathy resulting from pre-eclampsia should betreated with fresh frozen plasma (FFP). Con-sumptive coagulopathy severe enough to resultin depletion of fibrinogen is uncommon in thesedisorders, but, if severe hypofibrinogenemia ispresent, plasma fibrinogen levels can be raisedwith cryoprecipitate. In most cases, the clinicalmanifestations of pre-eclampsia resolve withinseveral days after delivery, although the plateletcount may decline for additional 24–48 h34. Ifsevere thrombocytopenia, hemolysis or organdysfunction persists after delivery, plasmaexchange may be considered35, but thediagnosis should also be reviewed.
Thrombotic thrombocytopenic purpura andhemolytic uremic syndrome
Thrombotic thrombocytopenia (TTP) andhemolytic uremic syndrome (HUS) share thecentral features of microangiopathic hemolyticanemia and thrombocytopenia. Though neither
disease occurs exclusively during pregnancy, theincidence of both is increased in this setting,and up to 10% of all cases of TTP occur inpregnant patients6.
TTP is defined by a pentad of symptoms thatinclude MAHA, thrombocytopenia, neurologi-cal abnormalities, fever, and renal dysfunction,although the complete pentad is present at thetime of diagnosis in less than 40% of patients34.The clinical manifestations of HUS are similar.Neurological abnormalities are particularly afeature of patients with TTP; renal dysfunctionis more severe in patients with HUS. Congenitalor acquired deficiency of a specific von Wille-brand factor-cleaving protease, ADAMTS 13,and the consequent increased level of high-molecular weight multimers of vWF play acentral role in the pathogenesis of TTP. Inter-estingly, levels of ADAMTS 13 decrease duringnormal pregnancy, perhaps accounting, at leastin part, for the predisposition to development ofthrombotic microangiopathy in this setting36.
TTP and HUS may be difficult to discernfrom one another, as well as from otherpregnancy-associated microangiopathies suchas pre-eclampsia or the HELLP syndrome. Theextent of microangiopathic hemolysis is gener-ally more severe in TTP or HUS than inpre-eclampsia or HELLP, and the former disor-ders are not associated with hypertension. Thetime of onset of these disorders is also helpfulin differentiating between them. TTP usuallypresents in the second trimester, HUS in thepostpartum period and pre-eclampsia andthe HELLP syndrome almost exclusively in thethird trimester7,34,37. Plasma antithrombin lev-els are normal in TTP and HUS and reduced inpre-eclampsia and HELLP34. Another featuredistinguishing these disorders is their responseto delivery. Whereas pre-eclampsia and theHELLP syndrome usually improve followingdelivery, the courses of TTP and HUS do not.Hence, pregnancy termination should not beconsidered therapeutic in patients with TTP orHUS38. However, TTP responds equally well toplasma exchange in pregnant and non-pregnantpatients with > 75% of patients achieving remis-sion6. Plasma exchange should be instituted assoon as possible after the diagnosis of TTP.Daily plasma exchange should continue until atleast 48 h after complete remission is obtained.
215
Acquired and congenital hemostatic disorders
237Z:\Sapiens Publishing\A5211 - Postpartum Hemorrhage\Make-up\Postpartum Hemorrhage - Voucher Proofs #T.vp30 August 2006 14:21:08
Color profile: Generic CMYK printer profileComposite Default screen

Repeated plasma exchange cycles are usuallymaintained until delivery. Management of HUSis supportive and includes renal dialysis and redcell transfusion. Plasma exchange has no provenbenefit in the treatment of HUS.
The placental ischemia and increased inci-dence of premature delivery that complicatepregnancies in patients with TTP and HUSmay lead to poor fetal outcomes, but these aremarkedly improved by good management ofthese conditions.
Acute fatty liver of pregnancy
Acute fatty liver of pregnancy affects one ofevery 5000–10 000 pregnancies and is mostcommon in primagravidas during the thirdtrimester39. The cause of the condition isunknown in the majority of instances, but somepatients may have a long-chain 3-hydroxy-acylCoA dehydrogenase (LCHAD) deficiency40.
Patients present with overt signs of hepaticdamage and may have hemorrhagic manifesta-tions, perhaps the result of decreased synthesisof clotting factors and consumptive coagulo-pathy. Evidence for consumptive coagulopathyis provided by thrombocytopenia, prolongedAPTT and PT and by decrease in fibrinogenand antithrombin levels.
AFLP is most aptly viewed as part of thepregnancy-associated microangiopathies; up to50% of patients with AFLP may also meetcriteria for pre-eclampsia. The extent of micro-angiopathic hemolysis and thrombocytopenia isgenerally mild compared to that observed inHELLP, TTP, or HUS41.
Delivery is the most important aspect ofmanagement, as it starts the reversal of thepathological process. Coagulation defects aremanaged supportively with fresh frozen plasma,cryoprecipitate and platelet concentrates. Inthese patients, normalization of hemostaticabnormalities may not occur for up to 10 daysafter delivery. Fetal mortality in this disorderapproaches 15%, though maternal mortalityoccurs in less than 5% of cases39.
CONSUMPTIVE COAGULOPATHY
Consumptive coagulopathy (disseminatedintravascular coagulation) is an acquired
clinicopathologic syndrome, characterized byactivation of the coagulation system, and result-ing in widespread intravascular deposition offibrin-rich thrombi. Consumption of clottingfactors usually leads to a bleeding diathesis,although a small percentage of affected individ-uals may go on to develop widespread thrombo-sis with peripheral organ ischemia. Some degreeof consumptive coagulopathy accompaniesmost forms of obstetric hemorrhage; however,the greater risk of coagulopathy usually arisesfrom consumption of clotting factors and plate-lets as a result of massive obstetric hemorrhage.The combination of massive hemorrhage andcoagulation failure is recognized as one of themost serious complications in pregnancy.
Obstetric consumptive coagulopathy is usu-ally acute in onset (except as an uncommon latecomplication of retained dead fetus) and can becaused by a variety of disease processes. Itis triggered by several mechanisms includingrelease of TF into the circulation, endothelialdamage to small vessels and production ofprocoagulant phospholipids in response tointravascular hemolysis42 (Table 5). Blood loss
216
POSTPARTUM HEMORRHAGE
A. Injury to vascular endotheliumPre-eclampsiaHypovolemic shockSepticemic shock
B. Release of tissue factor (TF)Placental abruptionAmniotic fluid embolismRetained dead fetusPlacenta accretaAcute fatty liver
C. Production of procoagulantFetomaternal hemorrhagePhospholipidsIncompatible blood transfusionSepticemiaIntravascular hemolysis
From Anthony J. Major obstetric hemorrhage anddisseminated intravascular coagulation. In JamesDK, Steer PJ, Weiner CP, Gonik B, eds. High-RiskPregnancy: Management Options, 3rd edn. Elsevier,2006:1606–23
Table 5 Mechanism of consumptive coagulopathyin pregnancy
238Z:\Sapiens Publishing\A5211 - Postpartum Hemorrhage\Make-up\Postpartum Hemorrhage - Voucher Proofs #T.vp30 August 2006 14:21:09
Color profile: Generic CMYK printer profileComposite Default screen

itself with transfusion and volume replacementmay also trigger consumptive coagulopathy.With obstetric complications associated withcoagulation failure, there may be interaction ofseveral mechanisms.
These triggers lead to the generation ofthrombin, cause defects in inhibitors of coagula-tion and suppress fibrinolysis. Thrombin pro-motes platelet activation and aggregates form,which occlude the microvasculature and resultin thrombocytopenia. Thrombin becomesbound to antithrombin (AT) and thrombo-modulin, and these proteins are soon con-sumed. Following binding to thrombomodulin,thrombin activates the anticoagulant protein C,which also becomes depleted, predisposingto microvascular thrombosis. In consumptivecoagulopathy secondary to sepsis, increased lev-els of C4b-binding protein result in the bindingof more free protein S, and therefore render itunavailable to be a cofactor of the anticoagulantprotein C. PAI-1 is increased out of proportionto the level of tissue plasminogen activator(tPA), resulting in depressed fibrinolysis. Fibrinis formed, but its removal is impaired, leadingto thrombosis of small and middle-size vessels.The passage of erythrocytes through partiallyoccluded vessels leads to red cell fragmentationand microangiopathic hemolytic anemia.
Placental abruption is the most commoncause of obstetric consumptive coagulopathy(60% of cases; 5% of all abruptions), but thesyndrome is uncommon unless the abruptionis severe enough to cause fetal death. Initially,increased intrauterine pressure forces TF-richdecidual fragments into the maternal circula-tion. However, in severe abruption, hypo-volemic shock, large volume transfusion andhigh levels of fibrin degradation products(FDPs) that act as anticoagulants themselvesexacerbate the situation. Retained dead fetusmay cause chronic consumptive coagulopathyby release of TF from the dead fetus into thematernal circulation, but generally only if thefetus is at least 20 weeks’ size and the periodof death is more than 4 weeks. Amniotic fluidembolism occurs during labor, Cesarean sectionor within a short time of delivery. Amniotic fluidis rich in TF and may enter uterine veins whenthere has been a tear in the uterine wall. Thecondition may lead to maternal death as a result
of severe pulmonary hypertension followingembolization of the pulmonary vessels by fetalsquames. If the mother survives this acuteevent, there may be an anaphylactoid reactionto the presence of the fetal tissues in the mater-nal circulation associated with cardiovascularcollapse, pulmonary edema and the develop-ment of consumptive coagulopathy. Sepsiscauses consumptive coagulopathy via therelease of proinflammatory cytokines such astumor necrosis factor α (TNF-α), interleukin 1(IL-1) and IL-6, which may trigger TF expres-sion by monocytes and endothelial cells43.Severe pre-eclampsia with intense vasospasmand resulting ischemia causes endothelial injuryand expression of TF.
Acute consumptive coagulopathy in preg-nancy presents almost invariably with bleeding –either as a genital tract bleeding from theplacental site or bleeding from the woundafter Cesarean section. There may be excessivebleeding from venepuncture sites.
Laboratory investigations are essential toestablish the diagnosis of consumptive coagulo-pathy. The characteristic changes are a low orfalling platelet count and a prolongation of theAPTT and PT. Fibrinogen level falls with theprogression of the coagulopathy; the normalrange in late pregnancy is 4–6 g/l which is sig-nificantly higher than the non-pregnant range,2–4 g/l; coagulation fails at levels < 1 g/l. FDPsare increased, reflecting the excessive deposi-tion of fibrin and enhanced fibrinolysis. TheD-dimer is the most commonly used parameterto assess FDP levels, as it is specific for fibrinbreakdown. Normal D-dimer levels are under200 ng/ml, but often exceed 2000 ng/ml incases of consumptive coagulopathy. The bloodfilm may show evidence of microangiopathichemolysis with fragmentation of red cells.
The basic principles in treatment of con-sumptive coagulopathy are removal of theprecipitating cause if possible, correction ofaggravating factors, and replacement of missingcoagulation factors and platelets. Correction ofaggravating factors such as shock and hypoxia isimportant. This includes red cell transfusion ifnecessary and oxygen administration. Intra-venous antibiotics should be given if sepsis issuspected. Replacement of clotting factors ismost effectively done with fresh frozen plasma.
217
Acquired and congenital hemostatic disorders
239Z:\Sapiens Publishing\A5211 - Postpartum Hemorrhage\Make-up\Postpartum Hemorrhage - Voucher Proofs #T.vp30 August 2006 14:21:09
Color profile: Generic CMYK printer profileComposite Default screen

If there is severe hypofibrinogenemia, cryo-precipitate may be required. Platelets shouldbe maintained > 50 × 109/l in the presence ofactive bleeding by the administration of bloodgroup-compatible platelets. Any etiologicalcondition should be promptly treated; it oftenrequires delivery of the fetus. Heparin use oftenleads to excessive bleeding and therefore doesnot usually have a role in obstetric consumptivecoagulopathy except in the cases of a retaineddead fetus. Similarly, antifibrinolytic drugs(tranexamic acid, aprotinin) are not helpful andare usually contraindicated because they inhibitthe removal of deposited fibrin by fibrinolysis.
The usual regimen, when there is coagulationfailure in obstetric practice, includes adminis-tration of FFP, platelets and cryoprecipitate.FFP contains fibrinogen and all coagulationfactors. Each unit is approximately 250 ml andthe usual requirement is 4–6 units. Plateletconcentrates are used to increment plateletcount. A unit of platelets is approximately 60 mlin volume; it should raise the platelet count by5000 × 109/l and the usual dose is five packs.Cryoprecipitate is enriched in fibrinogen, factorVIII and vWF and is particularly useful forthe treatment of hypofibrinogenemia. Ten bags(each 30 ml) of cryoprecipitate should increasethe fibrinogen level by 1 g/l. One 250 ml unit ofFFP contains a similar amount of fibrinogen(500 mg) as one 30 ml bag of cryoprecipitate(435 mg).
The D-dimer, platelet count and fibrinogenlevel are clinically useful tests in monitoringreplacement therapy if the patient is bleeding.The aim should be to achieve a platelet count> 50 × 109/l, a fibrinogen level > 1.0 g/l andsignificant shortening of the APTT and PT toapproach their normal values.
Although recombinant activated factor VII(rFVIIa) is not licensed for use in pregnancy,it has been used in obstetric patients with con-sumptive coagulopathy and severe bleeding notresponsive to other treatment options44,45 (seeChapter 26). Consumptive coagulopathy is nota contraindication to the use of rFVIIa if mas-sive bleeding is occurring. However, cautionshould be used in patients with major consump-tive coagulopathy because there are occasionalreports of thrombosis and consumptivecoagulopathy after the use of rFVIIa46.
Recombinant activated protein C (raPC) hasbeen successfully used in sepsis-related obstetricconsumptive coagulopathy at a dose of 24 µg/kg/h in a 96-h infusion47,48. Caution is neededin patients with severe thrombocytopenia(< 30 × 109/l) because of the increased inci-dence of intracerebral hemorrhage associatedwith its use; monitoring of the platelet countand transfusion of platelets as necessary areimportant considerations. In addition to actingas an anticoagulant, raPC has direct anti-inflammatory and anti-apoptotic properties49.This may explain in part why the other endo-genous anticoagulants (antithrombin and tissuefactor pathway inhibitor) used in severe sepsishave not shown such good efficacy.
The treatment of such underlying conditionssuch as abruptio placentae, uterine ruptureand fetal death require immediate obstetricattention. Usually, there has been extensivehemorrhage and red cell transfusion is neededin addition to correction of the coagulationfailure.
FACTOR VIII INHIBITORS
Acquired hemophilia is due to the developmentof an autoantibody to factor VIII (FVIII). Theestimated incidence is approximately 1 per1 000 000 per annum. Most cases occur inhealthy individuals without discernible riskfactors, but the condition is associated withautoimmune conditions such as rheumatoidarthritis and SLE, inflammatory bowel disease,multiple sclerosis and malignancies. In up to11% of cases, the associated factor is a recent orongoing pregnancy50.
Acquired hemophilia may occur in relation toany pregnancy, but the risk appears to be great-est after the first delivery. Onset is usually atterm or within 3 months postpartum, but mayonly become evident 12 months post-delivery51.Clinical manifestations do not necessarily corre-late with inhibitor levels and can range fromspontaneous bruising to life-threatening hemor-rhage. FVIII inhibitors may cross the placentaand persist in the neonate for up to 3 months,but neonatal complications are rare51. Sponta-neous resolution occurs in almost 100% ofwomen first diagnosed in the postpartum periodafter 30 months50.
218
POSTPARTUM HEMORRHAGE
240Z:\Sapiens Publishing\A5211 - Postpartum Hemorrhage\Make-up\Postpartum Hemorrhage - Voucher Proofs #T.vp30 August 2006 14:21:09
Color profile: Generic CMYK printer profileComposite Default screen

Basic coagulation studies in acquired hemo-philia demonstrate a prolonged APPT with anormal PT and thrombin time (TT). If plasmafrom the patient is mixed with normal plasma,the APPT remains prolonged due to the inhibi-tor antibody neutralizing the FVIII in thenormal plasma. FVIII inhibitors must be differ-entiated from a lupus inhibitor by specific testsbecause the clinical implications are profoundlydifferent. Quantification of FVIII inhibitor is bythe Bethesda assay, and checking this level mayhelp in determining the choice of therapy andmonitoring the progress of the patient.
Treatment is aimed at control of bleedingand accelerating the elimination of inhibitors.Hematological measures to minimize blood lossaim to compensate for the loss of FVIII. Choiceof product to attempt to normalize hemostasisdepends on various considerations, includingthe severity of bleeding, availability of clottingfactor concentrates, inhibitor level and cross-reactivity of inhibitor to porcine FVIII. HumanFVIII may be effective if the titer of inhibitor islow, i.e. less than 10 Bethesda units. At higherlevels, use of porcine FVIII which may notcross-react with the inhibitor, and recombinantFVIIa or prothrombin complex concentrate(PCC) becomes necessary52.
Inhibiting the production of the inhibitor isthe second management aim. Prednisolone atdose of 1 mg/kg is associated with a loss ofinhibitor in 50% of patients with acquiredhemophilia52. Other immunosuppressivesshould be considered if there is no responseto steroids. Addition of cyclophosphamide(2.0–3.0 mg/kg) should be considered at 3weeks if there is no decline in the inhibitor titer,or earlier if there is continued bleeding. Othermethods to reduce inhibitor levels includeazathioprine, plasma exchange or infusion ofIVIg.
ANTICOAGULANT THERAPY DURINGPREGNANCY AND THE PERIPARTUMPERIOD
Anticoagulant therapy is indicated duringpregnancy in the following cases:
(1) Prevention and treatment of venousthromboembolism (VTE);
(2) Prevention and treatment of systemicembolism in patients with mechanical heartvalve prostheses;
(3) Prevention of pregnancy complications inwomen with antiphospholipid syndrome(APS) or other thrombophilia and priorpregnancy complications.
The anticoagulants currently available forthe prevention and treatment of VTE andarterial thromboembolism include heparinand heparin-like compounds (unfractionatedheparin (UFH), low-molecular weight heparin(LMWH), and heparinoids) and coumarinderivatives, e.g. warfarin. The ‘direct’ thrombininhibitors, such as hirudin, cross the placentaand have therefore not yet been evaluatedduring pregnancy53.
Heparins are the anticoagulant of choiceduring pregnancy for situations in which theirefficacy is established. Neither UFH, LMWHnor heparinoids cross the placenta54. Heparinsare not associated with any known teratogenicrisk, and the fetus is not anticoagulated as aresult of maternal heparin use. LMWHs havepotential advantages over UFH during preg-nancy because they have a longer plasmahalf-life and a more predictable dose-responsethan UFH, with the potential for once-dailyadministration. In addition, LMWHs are asso-ciated with a lower risk of HIT and osteoporosisthan UFH.
Coumarin derivatives such as warfarin crossthe placenta and have the potential to causeteratogenicity as well as anticoagulate the fetuspredisposing to bleeding in utero. It is probablethat oral anticoagulants are safe during the first6 weeks of gestation, but there is an approxi-mately 5% risk of developmental abnormalitiesof fetal cartilage and bone if they are takenbetween 6 and 12 weeks’ gestation55. The risk ofwarfarin embryopathy is dose-dependent, withan increased risk when the daily warfarin doseexceeds 5 mg56. Fetal intracranial bleeds in uteroare a well-established complication after expo-sure to these drugs during any trimester. Ingeneral, coumarins should not be used for theprevention or treatment of VTE in pregnancy,but they remain the anticoagulants of choicefor the management of pregnant women withmechanical heart valve prostheses. Because of
219
Acquired and congenital hemostatic disorders
241Z:\Sapiens Publishing\A5211 - Postpartum Hemorrhage\Make-up\Postpartum Hemorrhage - Voucher Proofs #T.vp30 August 2006 14:21:09
Color profile: Generic CMYK printer profileComposite Default screen

the hemorrhagic risk to both mother and fetus,warfarin should be avoided beyond 36 weeksgestation.
LMWHs are currently widely used for theprevention and treatment of gestational VTE.In our institution, women on prophylactic dosesof LMWH are advised to have the dose of theLMWH tailed off at the end of pregnancy andomit their dose if labor is suspected. Women ona therapeutic dose of LMWH are admitted inadvance of planned induction to be converted tothe therapeutic dose of intravenous UFH. Theyshould omit LMWH on the day of admissionand should be started on UFH, aiming for anAPTT ratio of 1.5–2.0. UFH should be reducedto 500 IU/h when contractions start, aiming foran APTT ratio < 1.5 and should be stopped atthe second stage of labor or earlier if it appearsthat a Cesarean section may be required. In thelatter case, protamine sulfate may be neededfor reversal of UFH if the APTT ratio remains> 1.5. Postpartum, the heparin infusion can berestarted 4 h post-delivery at 500 IU/h, provid-ing there is no bleeding. Patients are restartedon a therapeutic dose of LMWH 2–3 days afterdelivery. Warfarin can be started 4–5 days post-partum, and LMWH should be continued untilan international normalized ratio (INR) of 2.0or greater is reached on two consecutive days.Breastfeeding is safe on UFH, LMWH andwarfarin.
Epidural anesthesia is generally safe inwomen following discontinuation of UFH, pro-viding their coagulation screen is normal andtheir platelet count is > 80 × 109/l. It remainsunclear what period of time should elapsebetween the last dose of LMWH and insertionor removal of an epidural or spinal catheter, orhow long the time interval should be until thenext dose. In practice, it is reasonable to allow atleast 12 h to elapse after a prophylactic dose ofLMWH before inserting an epidural or spinalcatheter, but a delay up to 24 h may be neces-sary in patients on therapeutic doses of LMWH.At least 2 h should elapse after insertion of thecatheter before LMWH is given again. If therehave been difficulties with the procedure, thenit is prudent to delay prior to giving furtherprophylaxis.
Pregnant women with prosthetic heart valvespose a problem because of the lack of reliable
data regarding the efficacy and safety ofantithrombotic therapy during pregnancy.However, it appears reasonable to adopt one ofthe following three approaches:
(1) Oral anticoagulants throughout pregnancy;
(2) Replacing oral anticoagulants with UFHfrom weeks 6 to 12;
(3) UFH throughout pregnancy.
In the first two regimens, heparin is usuallysubstituted for the oral anticoagulant close toterm. The use of LMWH for anticoagulationin patients with artificial heart valves is stilldebatable.
As Walker57 has so succinctly stated, deci-sions about the most appropriate anticoagulantregimen during pregnancy for women withmechanical heart valve prostheses must bemade on an individual patient basis after carefulcounseling, and should be based as far as possi-ble on the relative risks of the various thrombo-prophylaxis regimens and on whether thepatient is perceived to be at higher or lowerthromboembolic risk.
Women with the older type of mechanicalprostheses (e.g. Starr-Edwards or Bjork-Shiley),women with a prosthesis in the mitral position,women with multiple prosthetic valves andwomen with atrial fibrillation may be regardedas being at high thromboembolic risk. Womenwith newer and less thrombogenic valves (e.g.St Jude’s or Duromedics), particularly if theyare in the aortic position and providing they arein normal sinus rhythm, may be regarded asbeing at lower thromboembolic risk.
With the information currently available, itwould be prudent to advise women in thehigh-thromboembolic-risk category to use anoral anticoagulant with an INR target of3.5 throughout pregnancy, although some maychoose to substitute adjusted doses of heparinbetween 6 and 12 weeks’ gestation. Warfarinshould be avoided close to term and UFH orLMWH substituted. However, if labor com-mences in a woman on warfarin, intravenousvitamin K or fresh frozen plasma can be used toreverse its effect.
On the basis of one report that the risk offetal complications with warfarin appears to bedose-related56, women with mechanical heart
220
POSTPARTUM HEMORRHAGE
242Z:\Sapiens Publishing\A5211 - Postpartum Hemorrhage\Make-up\Postpartum Hemorrhage - Voucher Proofs #T.vp30 August 2006 14:21:10
Color profile: Generic CMYK printer profileComposite Default screen

valves in the lower thromboembolic risk cate-gory may feel reassured about the relatively lowrisk to their fetus if they use warfarin throughoutpregnancy, or with substitution of UFH orLMWH from weeks 6 to 12 if their daily warfa-rin requirement does not exceed 5 mg. Womenin this category requiring higher daily dosesof warfarin may wish to minimize the risk offetal complication, and be prepared to rely onadjusted doses of UFH and LMWH, but theymust be made aware that there is less goodevidence to support the use of these latterregimens. In general, women with bioprostheticvalves do not require anticoagulation, butanticoagulation may be necessary for otherindications.
Clear recommendations for heparin use dur-ing labor and delivery in women with artificialheart valves are not available. Intravenous UFHat therapeutic doses may be administered until6 h before delivery. If the UFH is to be reversed,it is usually sufficient to stop the infusion (as thehalf-life of the UFH is approximately 1 h). Ifmore rapid reversal is necessary, protamine sul-fate is used. One mg of protamine sulfate neu-tralizes 100 IU of heparin if the latter has beengiven within the previous 30 min. Protaminesulfate should be given slowly at 5 mg/min, witha maximum single dose of 50 mg. Protaminesulfate is much less effective in reversal ofLMWH.
Warfarin is initiated in the postpartum periodin patients with mechanical valves. Antico-agulation with intravenous UFH while awaitingtherapeutic levels of warfarin is probably notwarranted. The risk of bleeding, particularlyafter Cesarean section, exceeds the risk ofthrombotic complications58. SubcutaneousUFH in prophylactic doses (5000–7500 unitstwice daily) may be given.
CONGENITAL DISORDERS OFHEMOSTASIS
Congenital platelet disorders
Bernard–Soulier syndrome is a rare autosomalrecessive platelet disorder due to a variety ofmutations in membrane glycoproteins Ib, IXand V. Patients usually present early in life withspontaneous bruising, epistaxis or bleeding after
minor trauma; menorrhagia is a commonpresentation. Laboratory findings includethrombocytopenia, large platelets, prolongedbleeding time and poor platelet aggregation invitro to ristocetin.
Eleven cases of Bernard–Soulier syndrome inpregnant women have been described to date59.Most have been diagnosed prior to pregnancy,and postpartum hemorrhage has been morecommon than antepartum bleeding60. Manage-ment of bleeding in Bernard–Soulier syndromein pregnancy is debatable; single-donor platelettransfusions (preferably HLA-matched),desmopressin (DDAVP) and antifibrinolyticagents have been successfully used60.
Glanzmann’s thrombasthenia is due to aspectrum of mutations in platelet membraneGP IIb/IIIa, resulting in failure to bindfibrinogen. It is characterized by excessivemenstrual blood loss, bleeding from mucousmembranes, and major hemorrhage followingtrauma or surgery. The platelet count is normal,but clot retraction is greatly impaired and agentssuch as adenosine diphosphate (ADP), epi-nephrine and collagen fail to induce plateletaggregation. Patients with this condition are atincreased risk of primary postpartum hemor-rhage. Single-donor platelets (again, HLA-matched if possible) and recombinant activatedFVII have been used to control bleeding duringthe peripartum and the postpartum period61.
The May-Hegglin anomaly is a rare auto-somal dominant condition with thrombo-cytopenia and giant platelets. Platelet countvaries between 40 and 80 × 109/l, but plateletfunction appears normal. Excess hemorrhageis uncommon, but patients may need aplatelet transfusion to achieve hemostasis atdelivery62.
von Willebrand disease
von Willebrand disease (vWD) is the most com-mon of the inherited bleeding disorders, foundin approximately 1% of the general populationwithout ethnic variations. It is caused by areduced plasma concentration of structurallynormal von Willebrand factor (vWF) or thepresence of a structurally abnormal moleculewith reduced activity. vWF is the carrier proteinin plasma for FVIII, and it also acts as a bridge
221
Acquired and congenital hemostatic disorders
243Z:\Sapiens Publishing\A5211 - Postpartum Hemorrhage\Make-up\Postpartum Hemorrhage - Voucher Proofs #T.vp30 August 2006 14:21:10
Color profile: Generic CMYK printer profileComposite Default screen

between platelets and subendothelial collagenfibers.
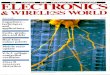
vWF is synthesized in endothelial cells as apolypeptide of 2813 amino acids, which under-goes initial dimerization and then multimerizat-ion up to a multimer with a molecular weightof 20 000 kDa. High-molecular weight (HMW)multimers are functionally more effective inpromoting platelet adhesion and aggregation.The vWF protein is released into the plasma,and is also stored in Weibel–Palade bodies inthe endothelial cells. vWF is also synthesized inmegakaryocytes, stored in the platelet α-gran-ules and, on activation, secreted by the plateletrelease reaction. This allows accumulation ofvWF at the site of vascular injury where it canpromote further platelet adhesion and thushemostasis. The mature vWF protein possessesa number of specific binding sites, which repre-sent its different activities (Figure 1). Circulat-ing HMW multimers are cleaved by a protease,known as ADAMTS 13, which is lacking inpatients with the rare congenital thromboticthrombocytopenic purpura.
vWD is subclassified into six categories(Table 6), which correspond to distinctpathophysiological mechanisms and are impor-tant in determining therapy. Of all the catego-ries, about approximately 70–80% of patientshave type 1 disease.
The condition commonly presents as a mildto moderate bleeding disorder, typically with
easy bruising or bleeding from mucosal sur-faces. The most frequent problem found in thenon-pregnant female is menorrhagia, whichmay be quite severe. Patients with mild abnor-malities may be asymptomatic, with the diag-nosis made only after significant hemostaticchallenges such as operations and trauma.
Laboratory tests in patients with vWDshow prolonged bleeding time and may showa prolonged APTT. More definitive diagnostictests depend on the finding of reduced vWFactivity measured by ristocetin cofactor activity
222
POSTPARTUM HEMORRHAGE
Figure 1 The von Willebrand factor. The protein consists of a series of domains with different bindingsites for factor VIII, heparin, collagen and platelet glycoprotein (Gp) Ib and IIb/IIIa. The sites of genemutations giving rise to different subtypes of VWD are marked. From Green D, Ludlam CA. VWD inbleeding disorders. Health Press 2004, pp. 63–69
Type 1
Type 2Type 2A
Type 2B
Type 2M
Type 2N
Type 3
Partial quantitative deficiency ofapparently normal vWFQualitative deficiency of vWFQualitative variants with decreasedHMW multimersQualitative variants with increasedaffinity for platelet GP IbQualitative variants with normal HMWmultimers appearanceQualitative variants with markedlydecreased affinity for factor VIIIVirtually complete deficiency of vWF
VWF, von Willebrand factor; HMW multimers,high-molecular weight multimersAdapted from Sadler JE. Thromb Haemost1994;71:520–5
Table 6 Classification of von Willebrand disease(VWD)
244Z:\Sapiens Publishing\A5211 - Postpartum Hemorrhage\Make-up\Postpartum Hemorrhage - Voucher Proofs #T.vp30 August 2006 14:21:13
Color profile: Generic CMYK printer profileComposite Default screen

(vWF:RCo) and collagen-binding assay(vWF:CB), accompanied by variable reductionsin vWF antigen (vWF:Ag) and FVIII. Severalfurther tests that aid in classification includeanalysis of ristocetin-induced platelet aggrega-tion (RIPA), vWF multimer and assay of FVIIIbinding to vWF63. The diagnosis may not bestraightforward, as one or more of the activitiesof FVIII and vWF may be borderline and evennormal. It is often necessary to repeat theestimations on at least three occasions. Stress,physical exercise, recent surgery and pregnancyall increase plasma vWF levels and FVIII levels,and diagnosis may be difficult in these circum-stances64. When investigating patients with bor-derline results, it should be taken into accountthat FVIII and vWF levels are 15–20% lower inindividuals with blood group O compared toindividuals with blood group A64.
The aim of therapy for vWD is to correctthe impaired primary hemostasis and impairedcoagulation. Treatment choice depends on theseverity and the type of disease, and on theclinical setting. Treatment options usuallyinclude DDAVP and vWF-containing bloodproducts65.
DDAVP, a synthetic vasopressin analogue,releases vWF from endothelial stores; there isalso an increase in the plasma FVIII level. It isusually given by slow intravenous infusion of0.3 µg/kg over 20 min, which can be repeatedevery 4–6 h on two or three occasions. The drugcan also be given subcutaneously or as a nasalspray. Side-effects include hypotension, facialflushing, fluid retention for up to 24 h and con-sequent hyponatremia. DDAVP can safely beused during pregnancy66 and after delivery. It iseffective in securing in many situations in type 1vWD with a 3–5-fold increase in the plasmavWF and FVIII levels. It is of no therapeuticbenefit in type 3 vWD because of the very lowbasal levels of vWF and FVIII. The response intypes 2 is less predictable. DDAVP is contrain-dicated in patients with type 2B because it mayexacerbate the coexisting thrombocytopenia.Patients should have a test of DDAVP (ifpossible when not pregnant) to see if it iseffective in their individual case.
Plasma-derived vWF concentrates are neces-sary in patients who do not respond adequatelyto DDAVP or in whom it is contraindicated.
The loading dose is 40–60 IU/kg, and thiscan be followed by repeat doses every 12–24 hto maintain vWF activity (vWF:RCoF) > 50%.All currently available concentrates are derivedfrom plasma. As at least one viral inactivationstep is included in their manufacture, they areunlikely to transmit hepatitis or HIV, but thereis still a risk of parvovirus infection.
von Willebrand disease and pregnancy
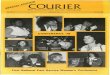
von Willebrand disease is the most commoncongenital hemostatic disorder in pregnancy. Ina normal pregnancy, both FVIII and vWF levelsprogressively increase (Figure 2)67. vWF startsto rise as early as the 6th week and by the thirdtrimester may have increased three- to fourfold.FVIII and vWF levels also increase in mostwomen with vWD, which may explain the fre-quent improvement in minor bleeding manifes-tations during pregnancy. The hemostaticresponse to pregnancy depends on both the typeand severity of disease. Most women with type 1vWD have an increase in FVIII and vWF levelsinto the normal non-pregnant range, which maymask the diagnosis during pregnancy. However,levels may remain low in severe cases. FVIII andvWF antigen levels often increase in pregnantwomen with type 2 vWD with minimal orno increase in vWF activity levels. In type 2BvWD, the increase in the abnormal vWF cancause progressive and severe thrombocytopenia,but intervention is not usually required. Mostwomen with type 3 vWD have no improvementin FVIII or vWF levels during pregnancy68.
After delivery, FVIII and vWF in normalwomen fall slowly to baseline levels over aperiod of 4–6 weeks. However, the postpartumdecline of these factors may be rapid and signifi-cant in women with vWD68. As the individualhemostatic response to pregnancy is variable,vWF and FVIII levels should be monitoredduring pregnancy and 3–4 weeks after delivery.
Antepartum hemorrhage is uncommon inwomen with vWD, but may occur after sponta-neous miscarriage or elective termination,occasionally as the initial presentation of vWD.Women with vWD are at substantial risk forsecondary postpartum hemorrhage, especially3–5 days after delivery. vWD may also exacer-bate bleeding due to other obstetric causes, such
223
Acquired and congenital hemostatic disorders
245Z:\Sapiens Publishing\A5211 - Postpartum Hemorrhage\Make-up\Postpartum Hemorrhage - Voucher Proofs #T.vp30 August 2006 14:21:14
Color profile: Generic CMYK printer profileComposite Default screen

as uterine atony or a trauma to the birth canal.Other pregnancy-associated reasons for bleed-ing in women with vWD include extensivebruising and hematomas at intramuscularinjection, episiotomy and surgical wound sites.
For patients whose vWD profile has normal-ized in pregnancy, no specific hemostatic sup-port is required. Regional analgesia mayproceed in these patients after discussion withan obstetric anesthetist. Although neonatalbleeding is rare, ventouse delivery and high-cavity forceps should be avoided. Careful andprompt repair of episiotomy wounds or perinealtears is advisable.
For patients whose vWF activity (vWF:RCo)has not normalized, decisions about regionalanalgesia should be individualized69. Hemo-static supportive therapy with DDAVP or vWFconcentrate should be given to cover delivery orCesarean section if the FVIII level is less than50% or if vWF:RCo has not normalized66.Because of the high incidence of secondarypostpartum hemorrhage in patients with vWD,efforts should be made to ensure that placenta iscomplete upon expulsion or removal.
After delivery, all patients should be closelyobserved for postpartum hemorrhage anduncorrected hemostatic defects treated. Inresponsive patients, DDAVP is the treatment ofchoice to prevent and treat mild to moderatepostpartum bleeding70. FVIII and vWF:RCoshould be checked a few days postpartumbecause they may fall rapidly after delivery.
FVIII and vWF:RCo should be maintained inthe normal range for at least 3–7 days afterCesarean section. It is difficult and unnecessaryto diagnose vWD in the neonate, except whentype 3 vWD is suspected. Generally, diagnosiscan be postponed until later in childhood.
HEMOPHILIAS
Hemophilias A and B are the most commonsevere congenital bleeding disorders associatedwith reduced or absent coagulation FVIII andFIX, respectively. The incidence of hemophiliaA is around 1 in 10 000 live male births. Hemo-philia B is about five times less common thanhemophilia A. The genes for both conditionsare located on the X-chromosome; they aretherefore sex-linked disorders that almost exclu-sively affect males. Clinically, the hemophiliashave an identical presentation and can only bedistinguished by measuring plasma levels of thespecific clotting factors. The clinical severity isdirectly related to plasma concentrations ofFVIII/FIX. Individuals with levels of below 1%of normal have severe hemophilia and the mostfrequent bleeds. Females in families with a his-tory of hemophilia may be obligate, potential orsporadic carriers, depending on the details ofthe pedigree71. An obligate carrier is a womanwhose father has hemophilia, or a woman whohas family history of hemophilia and who hasgiven birth to a hemophiliac son, or a womanwho has more than one child with hemophilia.
224
POSTPARTUM HEMORRHAGE
050
100150200250300350400450
13 18 23 28 33 38 Post Basal
Fact
or le
vel i
u/dl
Weeks gestation
FVIIIvWF:Ag
Figure 2 Levels of factor VIII and vWF in normal pregnancy. From Giangrande PL. Management ofpregnancy in carriers of haemophilia. Haemophilia 1998;4:779–84
246Z:\Sapiens Publishing\A5211 - Postpartum Hemorrhage\Make-up\Postpartum Hemorrhage - Voucher Proofs #T.vp30 August 2006 14:21:14
Color profile: Generic CMYK printer profileComposite Default screen

A potential carrier of hemophilia is a womanwho has a maternal relative with the disorder. Awoman with one affected child and no familyhistory may be a sporadic carrier71. Female car-riers of hemophilia may have reduced FVIII/IXlevels because of random inactivation of theX-chromosome (lyonization). If the FVIII/IXlevel is less than 50%, abnormal bleeding mayoccur after trauma or surgery.
There are two main risks for a female carrierof hemophilia in pregnancy. First, women witha low FVIII/IX level may be at risk of bleedingafter delivery or during invasive proceduresin the first trimester. Second, there is a 50%chance of each son inheriting hemophilia and50% of her daughters being carriers.
As discussed earlier, the levels of FVIII andvWF rise during normal pregnancy (Figure 2).The increase is particularly marked during thethird trimester, when levels of FVIII may rise todouble that of the normal baseline value. Simi-larly, the vast majority of carriers of hemophiliaA will have increased their FVIII production towithin the normal range by late gestation; factorreplacement therapy is thus only rarely requiredduring pregnancy in carriers of hemophilia A.By contrast, the level of FIX does not increasesignificantly during pregnancy, and thus awoman with a low initial baseline FIX is morelikely to require replacement to control bleedingcomplications during delivery.
All women who are obligate or potentialcarriers of hemophilia should be offered genetictesting and counseling. In particular, theyshould have their carrier status determinedto allow for the optimal management oftheir pregnancies. Genetic testing should beoffered when the individual is able to under-stand the issues concerned (usually at age of13–15 years) and after having given informedconsent72. In many individuals in the UK withhemophilia A and B, the causative mutationhas been identified. If the mutation within thefamily is known, it is straightforward to screenthe potential carrier. If, on the other hand, themutation is not known, then linkage analysisusing informative genetic polymorphisms maybe possible. If neither of these approachesis suitable, then direct mutation detectionmay be possible by sequencing the FVIII/FIXgene.
Coagulation studies should also be carriedout to identify carriers with low FVIII/FIX lev-els. Phenotypic data may be helpful in assessingthe statistical risk of carrriership if moleculardiagnosis is not possible. However, normal lev-els of FVIII/FIX do not exclude carriership72.Women who have low levels of FVIII may havea useful hemostatic response to DDAVP. Toestablish whether this response is occurring, atrial of intravenous DDAVP can be attempted,with measurement of the response in FVIIIlevels over the next 24 h.
Once carriership has been established,women should be offered prepregnancy coun-seling to provide them with the information nec-essary to make informed reproductive choices.A new technique of preimplantation diagnosisis potentially useful for carriers of hemophiliawho, after counseling, do not wish to contem-plate bringing up a hemophilic child, but wouldnot consider termination. Following in vitrofertilization (IVF) treatment, it is possible toremove a single embryonic cell at the 8–16-cellstage and carry out genetic diagnosis. Female orunaffected male embryos can then be trans-ferred into the uterus. In the UK, each such testrequires a license from the Human Fertilizationand Embryology Authority.
If prenatal diagnosis is requested, testingis usually carried out by chorionic villus sam-pling (CVS) at 11–12 weeks’ gestation; DNAextracted from fetal cells is analyzed. The prin-cipal advantage of this procedure is that it maybe applied during the first trimester, so that, iftermination of the pregnancy is required, thisis easier to carry out. The main adverse eventrelated to CVS is miscarriage, which is esti-mated at about 1–2%. Fetal cells are karyotypedso that the fetal sex is established. If the fetus isfemale, no further tests are done. If the fetus ismale, additional tests are conducted to establishwhether the affected gene has been inherited.Cells for karyotyping and as a source of DNAcan also be obtained from amniotic fluid(amniocentesis) after 15 weeks’ gestation; here,the miscarriage rate is about 0.5–1%. Fetoscopyto allow for fetal blood sampling is rarely per-formed; it can only be performed after about 16weeks’ gestation and has a substantial risk offetal death (1–6%). The use of prenatal diag-nosis is decreasing in developed countries. As
225
Acquired and congenital hemostatic disorders
247Z:\Sapiens Publishing\A5211 - Postpartum Hemorrhage\Make-up\Postpartum Hemorrhage - Voucher Proofs #T.vp30 August 2006 14:21:14
Color profile: Generic CMYK printer profileComposite Default screen

hemophilia care improves, more couples arewilling to contemplate bringing up a child withhemophilia67. When prenatal diagnosis has notbeen carried out but there is a risk that the childmay have hemophilia, fetal sex should be diag-nosed by ultrasonography67. This information isnecessary for the obstetrician even if the parentsdo not wish to know the sex of the infant.
Factor VIII/IX levels in female carriers ofhemophilia should be monitored regularly inpregnancy. It is particularly important to mea-sure coagulation factor levels toward the end ofthe third trimester (34–36 weeks) to plan man-agement of delivery67. If maternal FVIII/FIXlevels remain low at 34–36 weeks in hemophiliacarriers, treatment is necessary for delivery67. AFVIII/FIX plasma level of 40% is safe for vagi-nal delivery, and a level of 50% or greater is safefor Cesarean section. Epidural anesthesia maybe used if coagulation defects have been cor-rected67. Recombinant FVIII/FIX or DDAVP(for carriers of hemophilia A only) shouldbe used. Plasma-derived factor concentrateproducts, including those subjected to dual-inactivation processes, have the potential totransmit non-lipid coated viruses, e.g. parvo-virus, and should not be used. Infection of thefetus with parvovirus may result in hydropsfetalis and fetal death.
If the fetus is a known hemophiliac, is maleand of unknown hemophilia status, or is ofunknown sex, care should be taken to avoidtraumatic vaginal delivery. Routine Cesareandelivery is unnecessary67, but should be carriedout if obstetric complications are anticipated.
Most bleeding problems in carriers of hemo-philia occur postpartum. Replacement therapyshould be given immediately after delivery tomothers with uncorrected hemostatic defect.Treatment options at this stage are the sameas those during labor and delivery. Supportivetherapy to maintain hemostasis should becontinued for 3–4 days after vaginal deliveryand for 5–10 days after Cesarean section73.
In the infant, intramuscular injections shouldbe avoided until hemophilia has been excluded.Cord blood should be obtained for FVIII/FIXassays74. Routine administration of coagulationfactor concentrates to neonates with hemophiliais unnecessary if delivery has been atraumaticand there are no clinical signs of hemorrhage74.
RARE COAGULATION DISORDERS
Fibrinogen deficiency
The hypo- and dysfibrinogenemias comprisea collection of disorders that are usuallydominantly inherited and associated with bothbleeding and venous thrombotic manifestations.Women are at risk of recurrent miscarriage, andboth antenatal and postnatal hemorrhage. Inhypofibrinogenemia, both antigenic and func-tional fibrinogen levels are reduced. Thediagnosis of dysfibrinogenemia is made bydemonstrating a prolonged TT with a normalantigenic fibrinogen level.
Prophylaxis with fibrinogen concentratesimproves pregnancy outcome and preventsantepartum and postpartum hemorrhage inwomen with hypo- and dysfibrinogenemia.Cryoprecipitate is a good source of fibrinogenbut should not usually be used, as it is not virallyinactivated. Its use may be considered in anemergency situation if no other alternatives areavailable. The half-life of infused fibrinogen is3–5 days, and treatment is unlikely to be neededmore often than on alternate days. Levels above1.5 g/l are required toward the end of pregnancyand at the time of delivery75.
Factor VII deficiency
Congenital FVII deficiency is the most commonof the rare inherited coagulation disorders withan estimated prevalence of 1 in 500 000. It isinherited in an autosomal recessive manner andits frequency is significantly increased in coun-tries where there are consanguineous marriages.FVII levels are usually less than 10% in homo-zygotes and around 50% in heterozygotes.Although there is a poor correlation betweenFVII levels and bleeding risk, hemorrhagesoccur in patients with factor VII levels below10–15%76. Individuals with a moderate FVIIdeficiency often bleed from the mucousmembranes, and epistaxis, bleeding gums andmenorrhagia are common. In severe FVII defi-ciency (FVII level < 2%), bleeding into the cen-tral nervous system very early in life leads to ahigh morbidity and mortality. Congenital FVIIdeficiency is usually suspected when an isolatedprolongation of the PT is found in a patient
226
POSTPARTUM HEMORRHAGE
248Z:\Sapiens Publishing\A5211 - Postpartum Hemorrhage\Make-up\Postpartum Hemorrhage - Voucher Proofs #T.vp30 August 2006 14:21:14
Color profile: Generic CMYK printer profileComposite Default screen

without liver disease, and a normal APTT andfibrinogen level.
The FVII level may increase up to four-foldduring normal pregnancy76. However, it isunknown whether FVII levels increase to thesame degree in pregnant women with congenitalFVII deficiency as they do in normal preg-nancy77. FVII deficiency during pregnancy is arisk factor for postpartum hemorrhage. Bleed-ing may occur from the placental implantationsite, episiotomies, lacerations to the birth canal,or surgical trauma occurring with Cesareandelivery78.
Recombinant activated FVII (rFVIIa) hasbeen approved in the European Union for use incongenital FVII deficiency79. In places wherethis product is not available, fresh frozenplasma, prothrombin complex concentrates(PCCs) or plasma-derived FVII concentratemay be used. Because the patient may poten-tially need a Cesarean delivery and because peri-neal trauma cannot be anticipated, prophylaxisis usually recommended at the time of deliv-ery78. Recombinant FVIIa has been given as aninitial bolus injection of 20–50 µg/kg, followedby further boluses of 10–35 µg/kg every 4–6hours to cover vaginal delivery or Cesareansection in patients with congenital FVII defi-ciency78,80. It has also been used as an initialbolus injection of 13 µg/kg with subsequentcontinuous infusion at 1.7–3.3 µg/kg/h for 4days76 (see Chapter 26).
Factor X deficiency
Congenital FX deficiency is an autosomalrecessive disorder. The prevalence of the severe(homozygous) form is 1 : 1 000 000 in the gen-eral population and is much higher in countrieswhere consanguineous marriages are morecommon. The prevalence of heterozygous FXdeficiency is about 1 : 500, but individualsare usually clinically asymptomatic. Severe FXdeficiency (FX level < 1%) is associated with asignificant risk of intracranial hemorrhage in thefirst weeks of life and umbilical stump bleeding.The most frequent symptom is epistaxis, whichis seen with all severities of deficiency.Menorrhagia occurs in half of the women.Severe arthropathy may occur as a result ofrecurrent joint bleeds. Mild deficiency is
defined by FX levels of 6–10%; these individu-als are often diagnosed incidentally but mayexperience easy bruising or menorrhagia. Thediagnosis of FX deficiency is suspected follow-ing the finding of a prolonged APTT and PTand is confirmed by measuring plasma FX levels.
Thirteen pregnancies in eight patients withisolated FX deficiency have been reported inthe literature81. The complications describedinclude spontaneous abortions, placentalabruptions, premature births and postpartumhemorrhage. FX levels increase during preg-nancy and antenatal replacement therapy is notusually needed. However, women with severeFX deficiency and a history of adverse outcomein pregnancy may benefit from aggressivereplacement therapy75. As the half-life of FXis 24–40 h, a single daily infusion is usuallyadequate. FX levels of 10–20% are generallysufficient for hemostasis75 and are required atthe time of delivery.
FX is present in intermediate-purity FIX con-centrates (prothrombin complex concentrates,PCCs). FX levels should be monitored as cau-tion is required because of the prothromboticproperties of these concentrates. Fresh frozenplasma may be an alternative when prothrombincomplex concentrates are not available.
Combined deficiencies of the vitaminK-dependent factors II, VII, IX and X
Congenital combined deficiency of factors II,VII, IX and X is an autosomal recessive bleed-ing disorder. It is caused by deficiency ofenzymes associated with vitamin K metabolism(e.g. γ-glutamyl carboxylase) as a result ofhomozygous genetic mutations. Muco-cutaneous and postoperative related bleedinghave been reported. Severe cases may presentwith intracranial hemorrhage or umbilical cordbleeding in infancy. Some individuals haveassociated skeletal abnormalities (probablyrelated to abnormalities in bone vitaminK-dependent proteins such as osteocalcin).Severe bleeding is usually associated withactivities of the vitamin K-dependent factors of< 5%. Affected individuals show prolongationof the APTT and PT associated with variablereductions in the specific activities of factors II,VII, IX and X.
227
Acquired and congenital hemostatic disorders
249Z:\Sapiens Publishing\A5211 - Postpartum Hemorrhage\Make-up\Postpartum Hemorrhage - Voucher Proofs #T.vp30 August 2006 14:21:14
Color profile: Generic CMYK printer profileComposite Default screen

The clinical picture and response to vitaminK is variable, some responding to low-dose oralvitamin K but others are non-responsive even tohigh-dose intravenous replacement. In thoseindividuals who are non-responsive to vitaminK, prothrombin complex concentrates are theproduct of choice.
There is a single report of a pregnancy pro-gressing to term in an individual with severecongenital vitamin K-dependent clotting factordeficiency managed with oral vitamin K 15 mgdaily throughout pregnancy. Bleeding from anepisiotomy wound in this case required freshfrozen plasma82.
Factor XI deficiency
FXI deficiency is an autosomally inherited con-dition, which is particularly common in Ashke-nazi Jews in whom heterozygote frequency is8%. Overall, the prevalence of severe deficiencyis approximately 1 : 1 000 000 but partial defi-ciency is much more common. FXI deficiency isunlike most of the other rare coagulation disor-ders in that heterozygotes may have a significantbleeding tendency that is poorly predictedby the FXI level. Spontaneous bleeding isextremely rare, even in those with undetectableFXI levels. Bleeding is provoked by injury orsurgery, particularly in areas of high fibrinolyticactivity (e.g. genitourinary tract). Menorrhagiais common, and women with FXI deficiencymay be diagnosed as a consequence of this. FXIdeficiency rarely results in bleeding duringpregnancy, but women with severe or partialdeficiency may suffer postpartum bleeding75.
The APTT is usually prolonged and diag-nosis is confirmed by finding a low FXI level.The deficiency is classified as severe if the FXIlevel is less than 15% and partial at 15–70%; thelower limit of the normal range is 70%. There iscontroversy about changes in FXI levels duringnormal pregnancy, some studies demonstratingan increase and others a decrease83. Changesin FXI levels in women with FXI deficiencyhave been inconsistent during pregnancy84. It istherefore recommended that FXI levels shouldbe checked at the initial visit, and during thethird trimester in FXI-deficient women.
In women with partial FXI deficiency andno bleeding history but previous hemostatic
challenge, treatment is not usually requiredduring vaginal delivery. In women with partialdeficiency and significant bleeding history or noprevious hemostatic challenges, tranexamic acidis often used for 3 days, with the first dose beingadministered during labor. Tranexamic acid isalso used to manage prolonged mild intermit-tent secondary postpartum hemorrhage whichis a common presentation of FXI-deficientpatients84. FXI concentrate is needed forseverely deficient women to cover vaginaldelivery and also for Cesarean section. The aimis to maintain the FXI level > 50% during laborand for 3–4 days after vaginal delivery and 7days after Cesarean section. FXI concentrate ispotentially thrombogenic; the single doseshould not exceed 30 IU/kg with the aim ofraising FXI level to no greater than 70%84.Concurrent use of tranexamic acid or otherantifibrinolytic drugs with FXI concentrateshould be avoided. Fresh frozen plasma can beused, but, in patients with severe deficiency, it isdifficult to produce a sufficient rise (to morethan 30%) without the risk of fluid overload75.Recombinant FVIIa has been used successfullyto manage adult patients with FXI deficiencyundergoing surgery, although it is not licensedfor this indication75.
Factor XIII deficiency
Congenital FXIII (fibrin stabilizing factor)deficiency is an autosomal recessive disorder.It is characterized by features of delayedand impaired wound healing with bleedingoccurring 24–36 h after surgery or trauma.Umbilical bleeding in the first few weeks of lifeis very suggestive of the disorder. Soft tissuebleeds are more common than hemarthroses,which usually only occur after trauma. Sponta-neous intracranial bleeds are a characteristicfeature. Spontaneous abortions occur in earlypregnancy because FXIII is required forsuccessful implantation. Women with FXIIIdeficiency are also at increased risk of postnatalbleeding75. The severity of the bleeding statevaries markedly between individuals with appar-ently similar FXIII plasma levels. The routinetests (APTT and PT) are normal and the FXIIIlevel has to be specifically requested of thelaboratory.
228
POSTPARTUM HEMORRHAGE
250Z:\Sapiens Publishing\A5211 - Postpartum Hemorrhage\Make-up\Postpartum Hemorrhage - Voucher Proofs #T.vp30 August 2006 14:21:15
Color profile: Generic CMYK printer profileComposite Default screen

FXIII has a half-life of 7–10 days and there-fore only needs to be given at 4–6-weekly inter-vals to maintain a level > 3% which is necessaryto prevent spontaneous intracranial bleeds. Upto 50% of severely (FXIII level < 1%) affectedwomen may miscarry without appropriate FXIIItreatment75. All severely affected individualsshould be started on monthly infusions of plasma--derived FXIII concentrate from the time of diag-nosis to prevent intracranial bleeds and theseshould be continued during pregnancy75. FXIIIlevels fall throughout pregnancy and should bemonitored, aiming to keep the trough level > 3%.
FXIII deficiency may also cause life-threatening hemorrhage in the neonate withlevels < 3%. The disorder can be diagnosedfrom cord or peripheral blood samples. Treat-ment of an acute bleeding episode is with FXIIIconcentrate at a dose of 20 IU/kg75.
References
1. Brenner B. Haemostatic changes in pregnancy.Thromb Res 2004;114:409–14
2. Bellart J, Gilabert R, Miralles RM, et al.Endothelial cell markers and fibrinopeptide A toD-dimer ratio as a measure of coagulation andfibrinolysis balance in normal pregnancy.Gynecol Obstet Invest 1998;46:17–21
3. Øian P, Omsjø I, Maltau JM, Østerud B.Reduced thromboplastin activity in blood mono-cytes and reduced sensitivity to stimuli in vitro ofblood monocytes from pregnant women. Br JHaematol 1985;59:133–7
4. Holmes VA, Wallace JMW, Gilmore WS, et al.Tissue factor expression on monocyte sub-populations during normal pregnancy. ThrombHaemost 2002;87:953–8
5. Holmes VA, Wallace JM. Haemostasis in normalpregnancy: a balancing act? Biochem Soc Trans2005;33:428–32.
6. McCrae KR. Thrombocytopenia in pregnancy:differential diagnosis, pathogenesis and manage-ment. Blood Rev 2003;17:7–14
7. McCrae KR, Samuels P, Schreiber AD.Pregnancy-associated thrombocytopenia: patho-genesis and management. Blood 1992;80:2697–714
8. Shehata N, Burrows RF, Kelton JG. Gestationalthrombocytopenia. Clin Obstet Gynecol 1999;42:327–34
9. Guidelines for the investigation and manage-ment of idiopathic thrombocytopenic purpura in
adults, children and in pregnancy. Br J Haematol2003;120:574–96
10. Kessler I, Lancet M, Borenstein R, et al. Theobstetrical management of patients with immu-nologic thrombocytopenic purpura. Int JGynaecol Obstet 1982;20:23–8
11. Burrows RF, Kelton JG. Thrombocytopeniaduring pregnancy. In Greer IA, Turpie AG,Forbes CD, eds. Haemostasis and Thrombosis inObstetrics and Gynaecology. London: Chapman &Hall, 1992
12. Gill KK, Kelton JG. Management of idiopathicthrombocytopenic purpura in pregnancy. SemHematol 2000;37:275–83
13. Letsky EA. In de Swiet, ed. Coagulation Defects inMedical Disorders in Obstetric Practice, 4th edn.Oxford: Blackwell Science, 2002:61–96
14. Letsky EA, Greaves M. Guidelines on theinvestigation and management of thrombocyto-penia in pregnancy and neonatal alloimmunethrombocytopenia. Maternal and NeonatalHaemostasis Working Party of the Haemostasisand Thrombosis Task Force of the British Soci-ety for Haematology. Br J Haematol 1996;95:21–6
15. Crowther MA, Burrows RF, Ginsberg J,Kelton JG. Thrombocytopenia in pregnancy:diagnosis, pathogenesis and management. BloodRev 1996;10:8–16
16. Gill KK, Kelton JG. Management of idiopathicthrombocytopenic purpura in pregnancy. SemHematol 2000;37:275–83
17. Bussel JB, Druzin ML, Cines DB, Samuels P.Thrombocytopenia in pregnancy. Lancet 1991;337:251
18. Godelieve C, Christiaens ML, NieuwenhuisHK, Bussel JB. Comparison of platelet counts infirst and second newborns of mothers withimmune thrombocytopenic purpura. ObstetGynecol 1997;90:546–52
19. Miyakis S, Lockshin MD, Atsumi T, et al. Inter-national consensus statement on an update of theclassification criteria for definite antiphospho-lipid syndrome (APS). J Thromb Haemost 2006;4:295–306
20. Galli M, Finazzi G, Barbui T. Thrombocyto-penia in the antiphospholipid syndrome: patho-physiology, clinical relevance and treatment. AnnMed Intern 1996;147:24–7
21. Harris EN. A reassessment of the antiphospho-lipid syndrome. J Rheumatol 1990;17:733–5
22. Rai R, Cohen H, Dave M, Regan L. Randomisedcontrolled trial of aspirin and aspirin plus hepa-rin in pregnant women with recurrent miscar-riage associated with phospholipid antibodies (or
229
Acquired and congenital hemostatic disorders
251Z:\Sapiens Publishing\A5211 - Postpartum Hemorrhage\Make-up\Postpartum Hemorrhage - Voucher Proofs #T.vp30 August 2006 14:21:15
Color profile: Generic CMYK printer profileComposite Default screen

antiphospholipid antibodies). BMJ 1997;314:253–7
23. Royal College of Obstetricians and Gynaecolo-gists: Guidelines. Thromboprophylaxis duringpregnancy, labour and after vaginal delivery.Guidelines No. 37. London, RCOG Press,2004
24. de Swiet M. Antiphosholipid syndrome, systemiclupus erythematosus and other connective tissuediseases. In de Swiet, ed. Medical Disorders inObstetric Practice, 4th edn. Oxford: BlackwellScience, 2002:267–81
25. Mandelbrot L, Schlienger I, Bongain A, et al.Thrombocytopenia in pregnant women infectedwith human immunodeficiency virus: maternaland neonatal outcome. Am J Obstet Gynecol1994;171:252–7
26. van Besien K, Hoffman R, Golichowski A.Pregnancy associated with lupus anticoagulantand heparin induced thrombocytopenia: man-agement with a low molecular weight heparinoid.Thromb Res 1991;62:23–9
27. Greinacher A, Eckhardt T, Mussmann J,Mueller-Eckhardt C. Pregnancy complicated byheparin associated thrombocytopenia: manage-ment by a prospectively in vitro selectedheparinoid (Org 10172). Thromb Res 1993;71:123–6
28. Fausett MB, Vogtlander M, Lee RM, et al.Heparin-induced thrombocytopenia is rare inpregnancy. Am J Obstet Gynecol 2001;185:148–52
29. Huhle G, Geberth M, Hoffmann U, et al.Management of heparin-associated thrombo-cytopenia in pregnancy with subcutaneousr-hirudin. Gynecol Obstet Invest 2000;49:67–9
30. Khong TY, De Wolf F, Robertson WB, BrosensI. Inadequate maternal vascular response toplacentation in pregnancies complicated bypreeclampsia and by small for gestational ageinfants. Am J Obstet Gynecol 1987;157:360–3
31. Goldman-Wohl D, Yagel S. Regulation oftrophoblast invasion: from normal implantationto preeclampsia. Mol Cell Endocrinol 2002;187:233–8
32. Tank PD, Nadanwar YS, Mayadeo NM. Out-come of pregnancy with severe liver disease. Int JGynaecol Obstet 2002;76:27–31
33. Sibai BM. The HELLP syndrome (hemolysis,elevated liver enzymes, and low platelets): muchado about nothing? Am J Obstet Gynecol 1990;162:311–16
34. McCrae KR, Cines DB. Thrombotic micro-angiopathy during pregnancy. Sem Hematol1997;34:148–58
35. Martin JN, Files JC, Blake PG, et al. Plasmaexchange for preeclampsia: Postpartum use forpersistently severe preeclampsia-eclampsia withHELLP syndrome. Am J Obstet Gynecol 1990;162:126–37
36. Mannucci PM, Canciani T, Forza I, et al.Changes in health and disease of the metallo-protease that cleaves von Willebrand Factor.Blood 2001;98:2730–5
37. Lain KY, Roberts JM. Contemporary conceptsof the pathogenesis and management ofpreeclampsia. JAMA 2002;287:3183–6
38. Esplin MS, Branch DW. Diagnosis and manage-ment of thrombotic microangiopathies duringpregnancy. Clin Obstet Gynecol 1999;42:360–8
39. Bacq Y. Acute fatty liver of pregnancy. SemPerinatol 1998;22:134–40
40. Tyni T, Ekholm E, Pihko H. Pregnancycomplications are frequent in long-chain3-hydroxyacyl-coenzyme A dehydrogenase defi-ciency. Am J Obstet Gynecol 1998;178:603–8
41. Vigil-De Gracia P. Acute fatty liver and HELLPsyndrome: two distinct pregnancy disorders. IntJ Gynaecol Obstet 2001;73:215–21
42. Anthony J. Major obstetric hemorrhage anddisseminated intravascular coagulation. In JamesDK, Steer PJ, Weiner CP, Gonik B, eds. HighRisk Pregnancy: Management Options, 3rd edn.Amsterdam: Elsevier, 2006:1606–23
43. Levi M. Current understanding of disseminatedintravascular coagulation. Br J Haematol 2004;124:567–76
44. Moscardo F, Perez F, de la Rubia J, et al.Successful treatment of severe intra-abdominalbleeding associated with disseminated intra-vascular coagulation using recombinant acti-vated factor VII. Br J Haematol 2001;114:174–6
45. Zupancic Salek S, Sokolic V, Viskovic T, et al.Successful use of recombinant factor VIIa formassive bleeding after caesarean section dueto HELLP syndrome. Acta Haematol 2002;108:162–3
46. Ludlam CA. The evidence behind inhibitortreatment with recombinant factor VIIa. Pato-physiol Haemost Thromb 2002;32(Suppl 1):13–18
47. Maclean A, Almeida Z, Lopez P. Complicationsof acute fatty liver of pregnancy treated with acti-vated protein C. Arch Gynecol Obstet 2005;273:119–21
48. Mikaszewska-Sokolewicz M, Mayzner-Zawadzka E. Use of recombinant humanactivated protein C in treatment of severe sepsisin a pregnant patient with fully symptomaticovarian hyperstimulation syndrome. Med SciMonit 2005;11:27–32
230
POSTPARTUM HEMORRHAGE
252Z:\Sapiens Publishing\A5211 - Postpartum Hemorrhage\Make-up\Postpartum Hemorrhage - Voucher Proofs #T.vp30 August 2006 14:21:15
Color profile: Generic CMYK printer profileComposite Default screen

49. Toh CH, Dennis M. Disseminated intravascularcoagulation: old disease, new hope. BMJ 2003;327:974–7
50. Kashyap R, Choudhry VP, Mahapatra M, et al.Postpartum acquired haemophilia: clinical rec-ognition and management. Haemophilia 2001;7:327–30
51. Porteous AO, Appleton DS, Hoveyda F, LeesCC. Acquired haemophilia and postpartumhaemorrhage treated with internal pudendalembolisation. Br J Obstet Gynaecol 2005;112:678–9
52. Boggio LN, Green D. Acquired hemophilia. RevClin Exp Hematol 2001;5:389–404
53. Bates SM, Ginsberg JS. How we manage venousthromboembolism during pregnancy. Blood2002;100:3470–8
54. Bates SM, Greer IA, Hirsh J, Ginsberg JS. Useof antithrombotic agents during pregnancy.Presented at the Seventh ACCP Conferenceon Antithrombotic and Thrombolytic Therapy.Chest 2004;126:627–44
55. Ginsberg JS, Hirsh J, Turner C, et al. Risks to thefetus of anticoagulant therapy during pregnancy.Thromb Haemost 1989;61:197–203
56. Vitale N, De Feo M, De Santo LS, et al. Dose-dependent fetal complications of warfarin inpregnant women with mechanical heart valves.J Am Coll Cardiol 1999;33:1637–41
57. Walker ID. In O’Shaughnessy D, Makris M andLillicrap D, eds. Obstetrics in Practical Hemostasisand Thrombosis, 1st edn. Oxford: BlackwellPublishing, 2005:139–48
58. Kearon C, Hirsh J. Management of anticoagu-lation before and after elective surgery. N Engl JMed 1997;336:1506–11
59. Rahimi G, Rellecke S, Mallmann P, Nawroth F.Course of pregnancy and birth in a patient withBernard–Soulier syndrome – a case report. Pato-physiol Haemost Thromb 2002;32(Suppl 1):13–18
60. Kriplani A, Singh BM, Sowbernika R,Choudhury VP. Successful pregnancy outcomein Bernard–Soulier syndrome. J Obstet GynaecolRes 2005;31:52–6
61. Kale A, Bayhan G, Yalinkaya A, Yayla M.The use of recombinant factor VIIa in aprimigravida with Glanzmann’s thrombastheniaduring delivery. J Perinat Med 2004;32:456–8
62. Pajor A, Nemes L, Demeter J. May Hegglinanomaly and pregnancy. Eur J Obstet GynecolReprod Biol 1999;85:229–31
63. Favaloro EJ. Laboratory assessment as a criticalcomponent of the appropriate diagnosis andsub-classification of von Willebrand’s disease.Blood Rev 1999;13:185–204
64. Laffan M, Brown SA, Collins PW, et al. Thediagnosis of von Willebrand disease: a guidelinefrom the UKHCDO. Haemophilia 2004;10:199–217
65. Pasi KJ, Collins PW, Keeling DM, et al.Management of von Willebrand disease: a guide-line from the UKHCDO. Haemophilia 2004;10:218–31
66. Mannucci PM. How I treat patients with vonWillebrand disease. Blood 2001;97:1915–19
67. Giangrande PL. Management of pregnancy incarriers of haemophilia. Haemophilia 1998;4:779–84
68. Kujovich JL. Von Willebrand disease andpregnancy. J Thromb Haemost 2005;3:246–53
69. Stedeford JC, Pittman JA. Von Willebrand’sdisease and neuroaxial anaesthesia. Anaesthesia2000;55:1228–9
70. Horn EH. Thrombocytopenia and bleedingdisorders. In James DK, Steer PJ, Weiner CP,Gonik B, eds. High-Risk Pregnancy: ManagementOptions, 3rd edn. Amsterdam: Elsevier, 2006:901–24
71. Miller R. Counselling about diagnosis and inher-itance of genetic bleeding disorders: haemophiliaA and B. Haemophilia 1999;5:77–83
72. Ludlam CA, Pasi KJ, Bolton-Maggs P, et al.A framework for genetic service provision forhaemophilia and other inherited bleedingdisorders. Haemophilia 2005;11:145–63
73. Walker ID, Walker JJ, Colvin BT, et al. Investi-gation and management of haemorrhagic disor-ders in pregnancy. J Clin Pathol 1994;47:100–8
74. Kulkarni R, Lusher JM, Henry RC, Kallen DJ.Current practices regarding newborn intracranialhaemorrhage and obstetrical care and mode ofdelivery of pregnant haemophilia carriers: asurvey of obstetricians, neonatologists andhaematologists in the United States, on behalf ofthe National Hemophilia Foundation’s Medicaland Scientific Advisory Council. Haemophilia1999;5:410–15
75. Bolton-Maggs PH, Perry DJ, Chalmers EA, et al.The rare coagulation disorders – review withguidelines for management from the UKHCDO.Haemophilia 2004;10:593–628
76. Jimenez-Yuste V, Villar A, Morado M, et al.Continuous infusion of recombinant activatedfactor VII during caesarean section delivery ina patient with congenital factor VII deficiency.Haemophilia 2000;6:588–90
77. Fadel HE, Krauss JS. Factor VII deficiency andpregnancy. Obstet Gynecol 1989;73:453–4
78. Eskandari N, Feldman N, Greenspoon JS.Factor VII deficiency in pregnancy treated with
231
Acquired and congenital hemostatic disorders
253Z:\Sapiens Publishing\A5211 - Postpartum Hemorrhage\Make-up\Postpartum Hemorrhage - Voucher Proofs #T.vp30 August 2006 14:21:15
Color profile: Generic CMYK printer profileComposite Default screen

recombinant factor VIIa. Obstet Gynecol 2002;99:935–7
79. Mariani G, Konkle BA, Ingerslev J. Congenitalfactor VII deficiency: therapy with recombinantactivated factor VII – a critical appraisal. Haemo-philia 2006;12:19–27
80. Muleo G, Santoro R, Iannaccaro PG, et al.The use of recombinant activated factor VII incongenital and acquired factor VII deficiencies.Blood Coagul Fibrinolysis 1998;9:389–90
81. Romagnolo C, Burati S, Ciaffoni S, et al. Severefactor X deficiency in pregnancy: case report andreview of the literature. Haemophilia 2004;10:665–8
82. McMahon MJ, James AH. Combined deficiencyof factors II, VII, IX, and X (Borgschulte–Grigsby deficiency) in pregnancy. Obstet Gynecol2001;97:808–9
83. David AL, Paterson-Brown S, Letsky EA. FactorXI deficiency presenting in pregnancy: diagnosisand management. Br J Obstet Gynaecol 2002;109:840–3
84. Kadir RA, Economides DL, Lee CA. Factor XIdeficiency in women. Am J Hematol 1999;60:48–54
232
POSTPARTUM HEMORRHAGE
254Z:\Sapiens Publishing\A5211 - Postpartum Hemorrhage\Make-up\Postpartum Hemorrhage - Voucher Proofs #T.vp30 August 2006 14:21:15
Color profile: Generic CMYK printer profileComposite Default screen