Embed Size (px)
Citation preview
1
Postpartum Complication:PPHMargie Bridges, DNP, ARNP-BC, RNC-OBPerinatal Clinical Nurse SpecialistOverlake Hospital
PPH OBJECTIVES
NORMAL ADAPTATION
RECOGNITION
READINESS
RESPONSE
2
Physiologic Adaptation of Pregnancy Provides Protection
Antepartum Volume Expansion
Uterine Contractility
Autotransfusion
Hypercoagulopathy
Normal Adaption
Uterus
Normal Involution Weight
Size
Fundal position
After pains
Breastfeeding
3
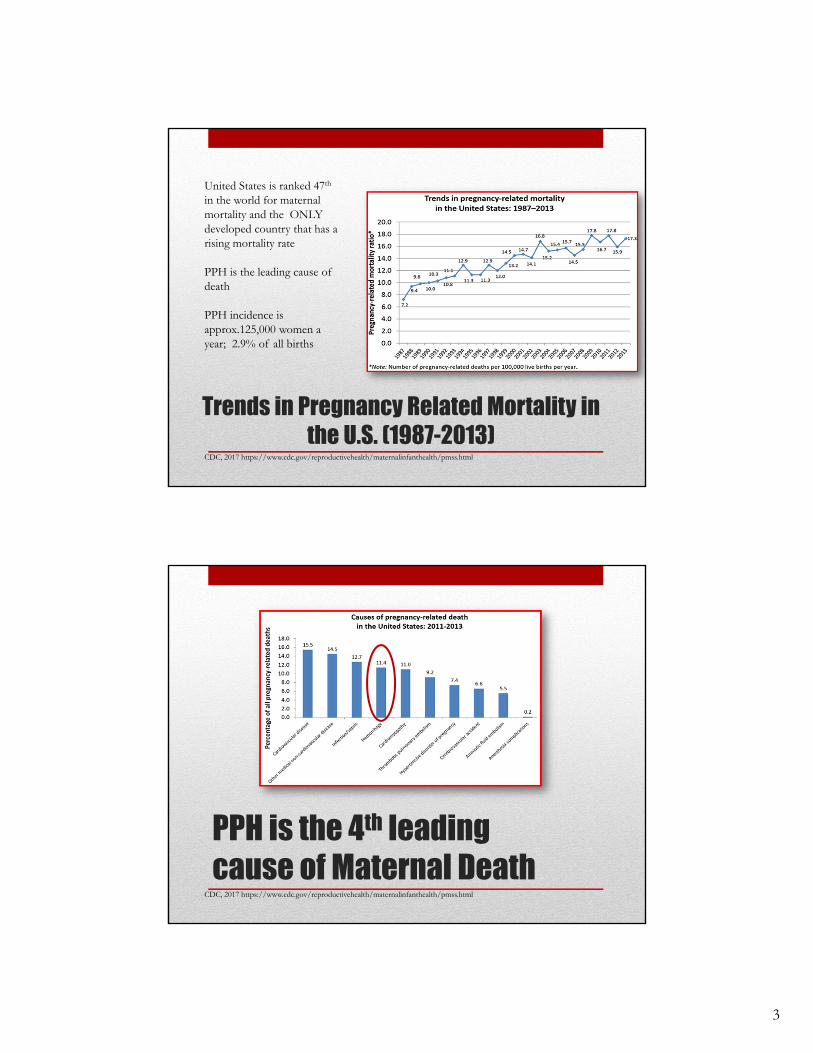
Trends in Pregnancy Related Mortality in the U.S. (1987-2013)
CDC, 2017 https://www.cdc.gov/reproductivehealth/maternalinfanthealth/pmss.html
United States is ranked 47th
in the world for maternal mortality and the ONLY developed country that has a rising mortality rate
PPH is the leading cause of death
PPH incidence is approx.125,000 women a year; 2.9% of all births
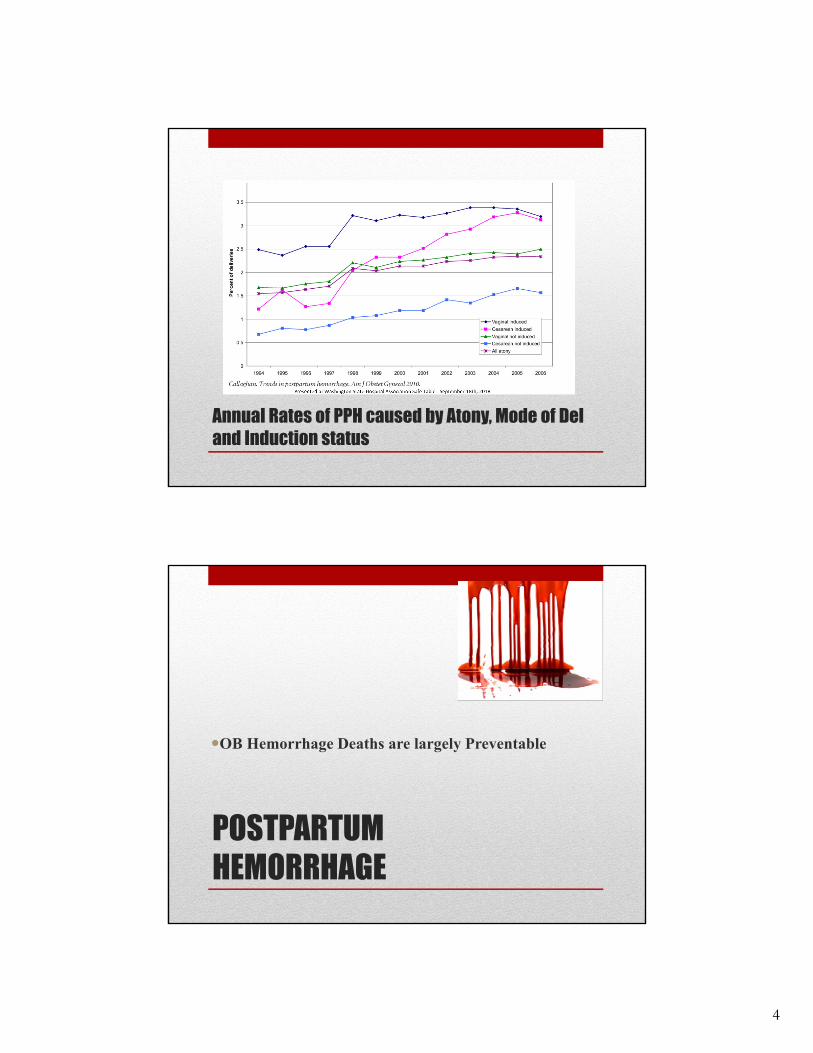
PPH is the 4th leading cause of Maternal Death
CDC, 2017 https://www.cdc.gov/reproductivehealth/maternalinfanthealth/pmss.html
4
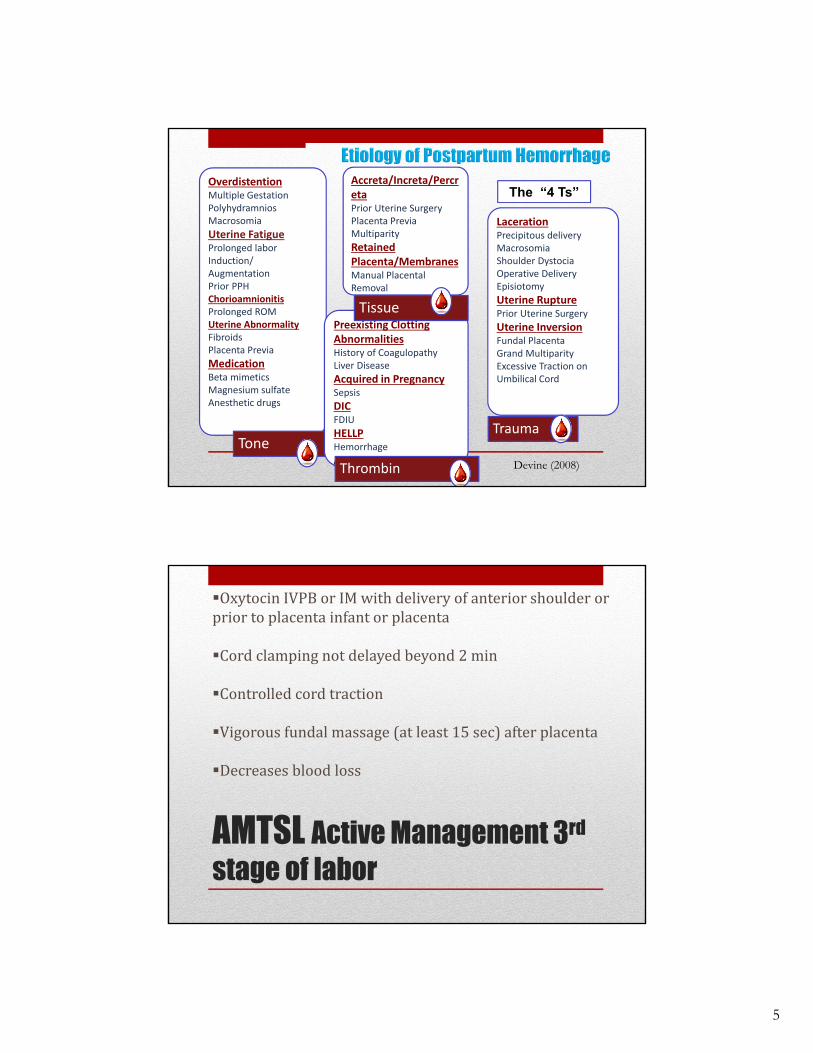
Annual Rates of PPH caused by Atony, Mode of Del and Induction status
POSTPARTUM HEMORRHAGE
OB Hemorrhage Deaths are largely Preventable
5
OverdistentionMultiple GestationPolyhydramniosMacrosomia
Uterine FatigueProlonged laborInduction/AugmentationPrior PPHChorioamnionitisProlonged ROMUterine AbnormalityFibroidsPlacenta Previa
MedicationBeta mimeticsMagnesium sulfateAnesthetic drugs
Tone
Preexisting Clotting AbnormalitiesHistory of Coagulopathy Liver Disease
Acquired in PregnancySepsis
DICFDIU
HELLPHemorrhage
Anticoagulation
LacerationPrecipitous deliveryMacrosomiaShoulder DystociaOperative DeliveryEpisiotomy
Uterine RupturePrior Uterine Surgery
Uterine InversionFundal PlacentaGrand MultiparityExcessive Traction on Umbilical Cord
Accreta/Increta/PercretaPrior Uterine SurgeryPlacenta PreviaMultiparity
Retained Placenta/MembranesManual Placental Removal
Tissue
Thrombin
Trauma
The “4 Ts”
Devine (2008)
AMTSL Active Management 3rd
stage of labor
Oxytocin IVPB or IM with delivery of anterior shoulder or prior to placenta infant or placenta
Cord clamping not delayed beyond 2 min
Controlled cord traction
Vigorous fundal massage (at least 15 sec) after placenta
Decreases blood loss
6
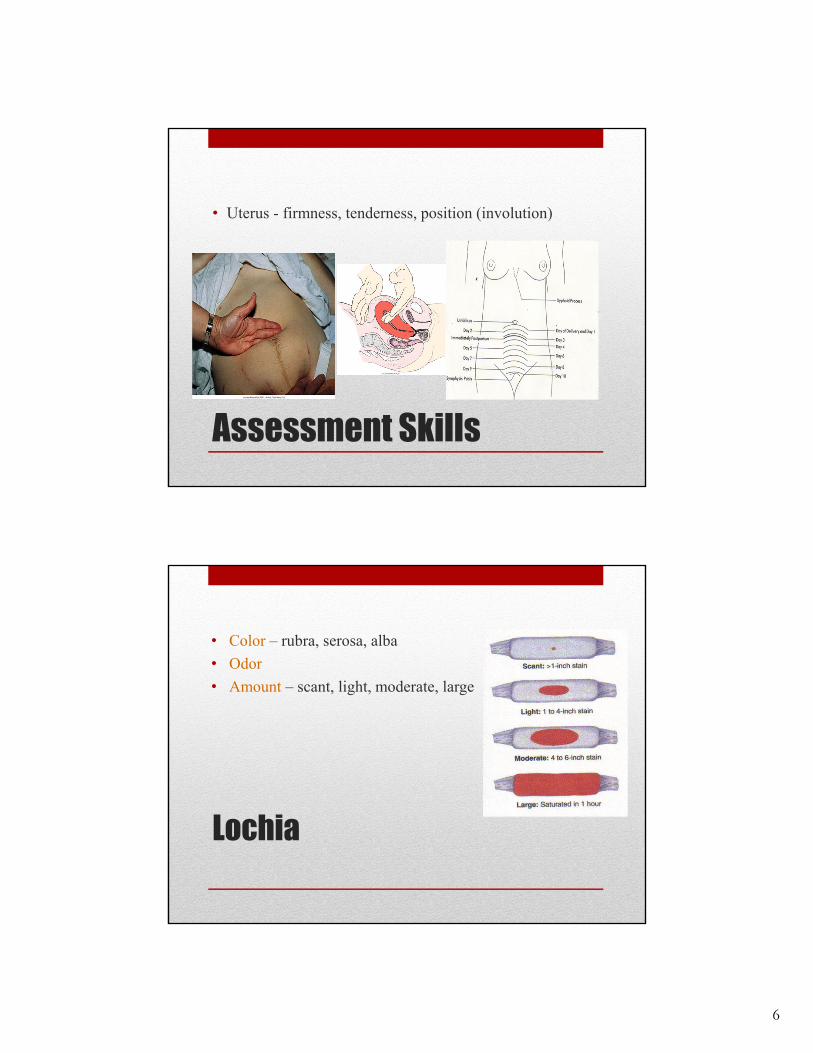
Assessment Skills
• Uterus - firmness, tenderness, position (involution)
Lochia
• Color – rubra, serosa, alba
• Odor
• Amount – scant, light, moderate, large
7
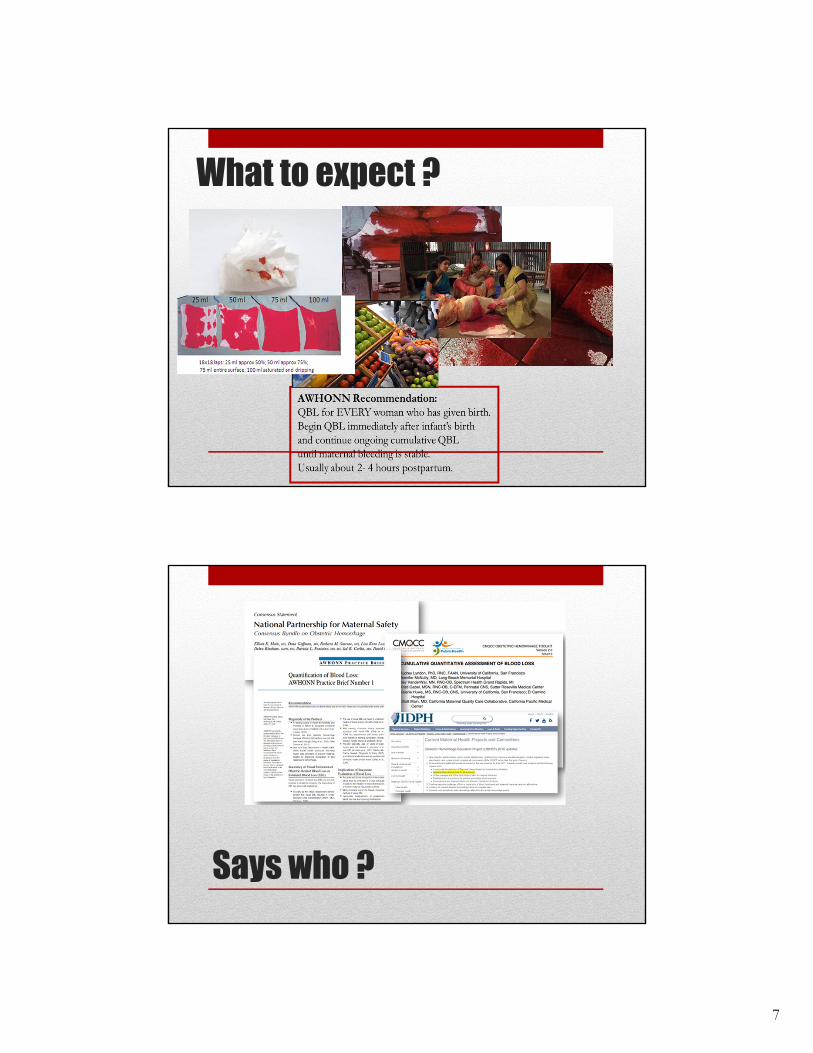
What to expect ?
Says who ?
8
WHAT ?
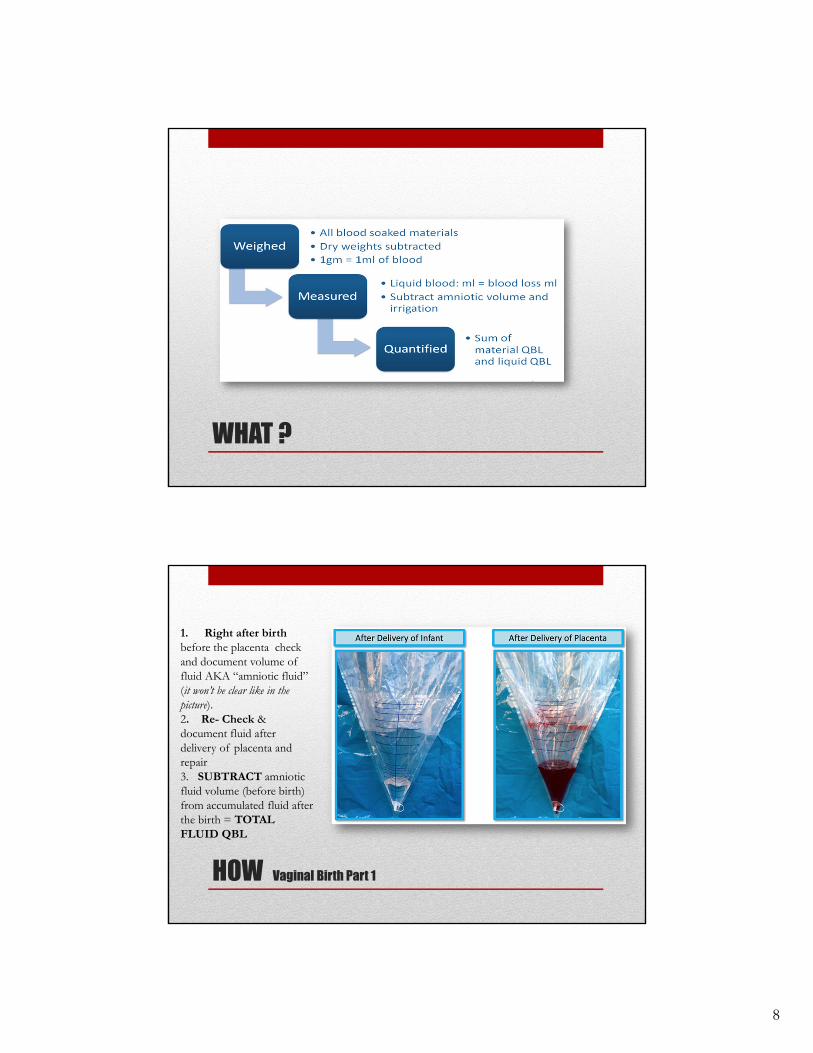
HOW Vaginal Birth Part 1
1. Right after birthbefore the placenta check and document volume of fluid AKA “amniotic fluid” (it won’t be clear like in the picture).2. Re- Check & document fluid after delivery of placenta and repair 3. SUBTRACT amniotic fluid volume (before birth) from accumulated fluid after the birth = TOTAL FLUID QBL
9
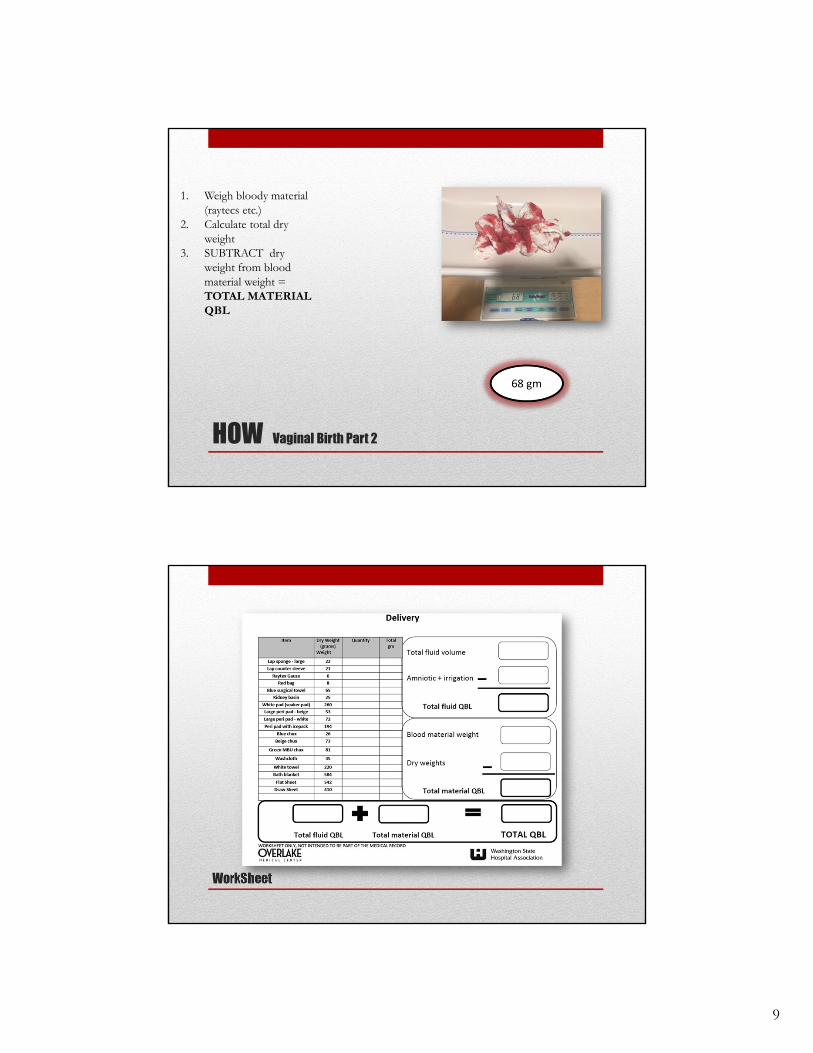
HOW Vaginal Birth Part 2
1. Weigh bloody material (raytecs etc.)
2. Calculate total dry weight
3. SUBTRACT dry weight from blood material weight = TOTAL MATERIAL QBL
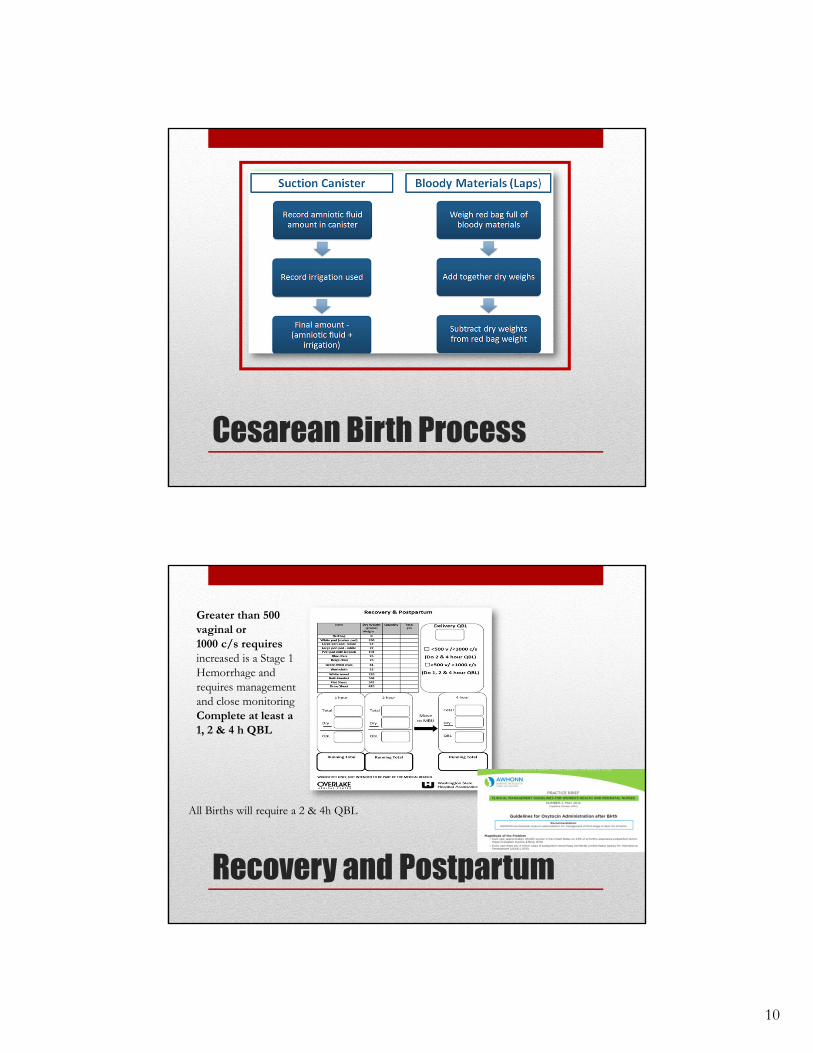
WorkSheet
10
Cesarean Birth Process
Recovery and Postpartum
Greater than 500 vaginal or1000 c/s requires increased is a Stage 1 Hemorrhage and requires management and close monitoringComplete at least a 1, 2 & 4 h QBL
All Births will require a 2 & 4h QBL
11
EBL vs QBLMath not Magic
LET’S PRACTICE !!!
“The clinical symptoms of blood loss (low blood pressure, fast pulse, pallor and sweating, signs of hypovolemia and impeding shock) are often the primary indicators for intervention. However, relying on the onset of such symptoms may lead to delayed intervention, resulting in increased morbidity and mortality.”
B.S. Kodkany and R.J. Derman. Pitfalls in Assessing Blood Loss and Decision to Transfer
PPH Triggers
12
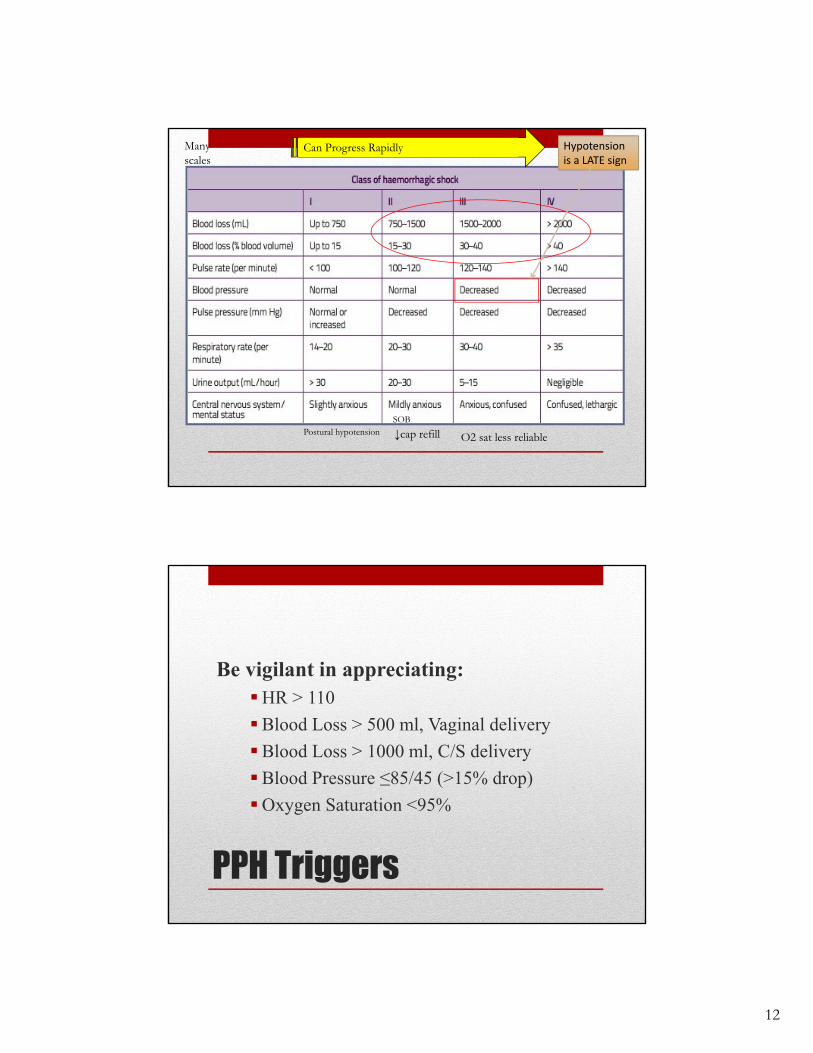
Postural hypotension
Can Progress Rapidly Hypotension is a LATE sign
Many scales
↓cap refillSOB
O2 sat less reliable
PPH Triggers
Be vigilant in appreciating:HR > 110
Blood Loss > 500 ml, Vaginal delivery
Blood Loss > 1000 ml, C/S delivery
Blood Pressure ≤85/45 (>15% drop)
Oxygen Saturation <95%
13
Be prepared with Triggers!
When triggers present:
Mobilize help Continue calculation of blood loss Confirm T & S done Confirm status of blood availability Confirm T & S done; Confirm blood availability Have uterotonics readily available PPH Cart
5 Major Causes
• Uterine Atony
• Lacerations
• Retained Placental Tissue/Fragments
• Hematoma
• Subinvolution
14
Signs and Symptoms of Uterine Atony
• Marked hypotonia of the uterus• Leading cause of PPH – 80-90% of all cases
Signs and Symptoms:• Boggy, large uterus• Heavy, bright red vaginal flow• Expelled clots
Causes of Atony ?Marked hypotonia of the uterus
• Long Labor• Induction/augmentation of labor• Large Baby • Multiple Gestation• Uterine myomas or fibromas• High parity• MgSo4• Full bladder• Infection• Retained Placenta• HX PPH• Infection• History of PPH
Interventions???
Usual suspect…..
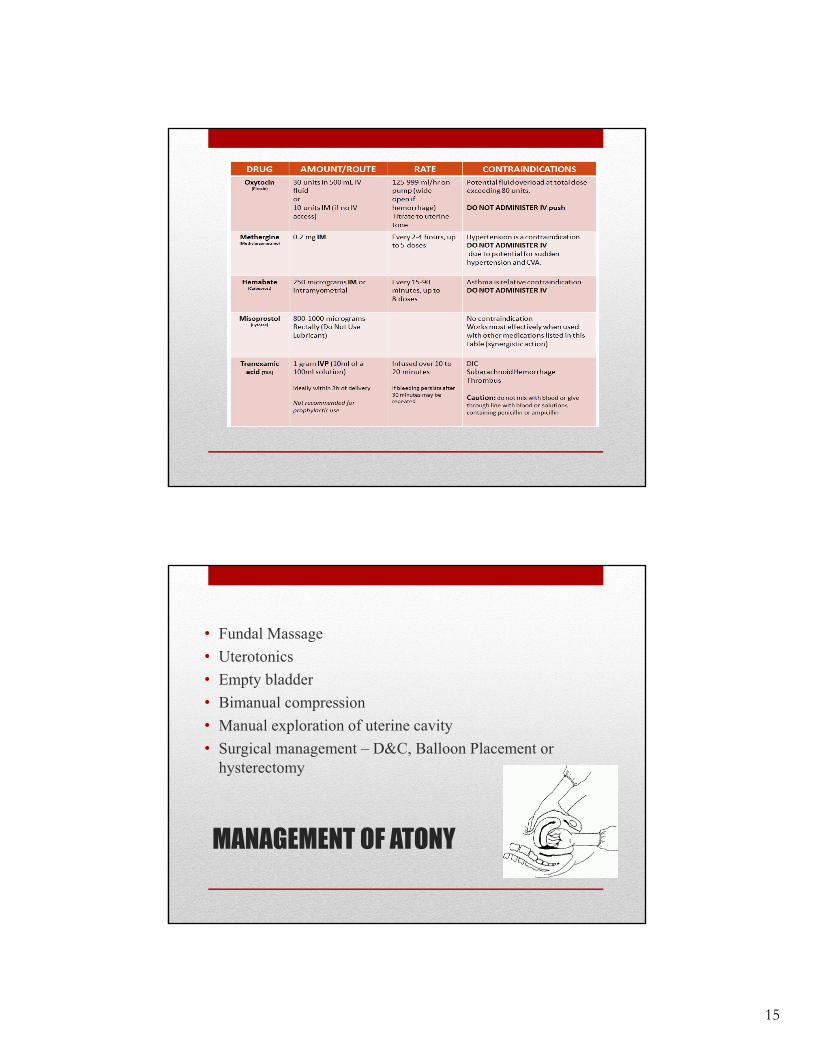
15
MANAGEMENT OF ATONY
• Fundal Massage
• Uterotonics
• Empty bladder
• Bimanual compression
• Manual exploration of uterine cavity
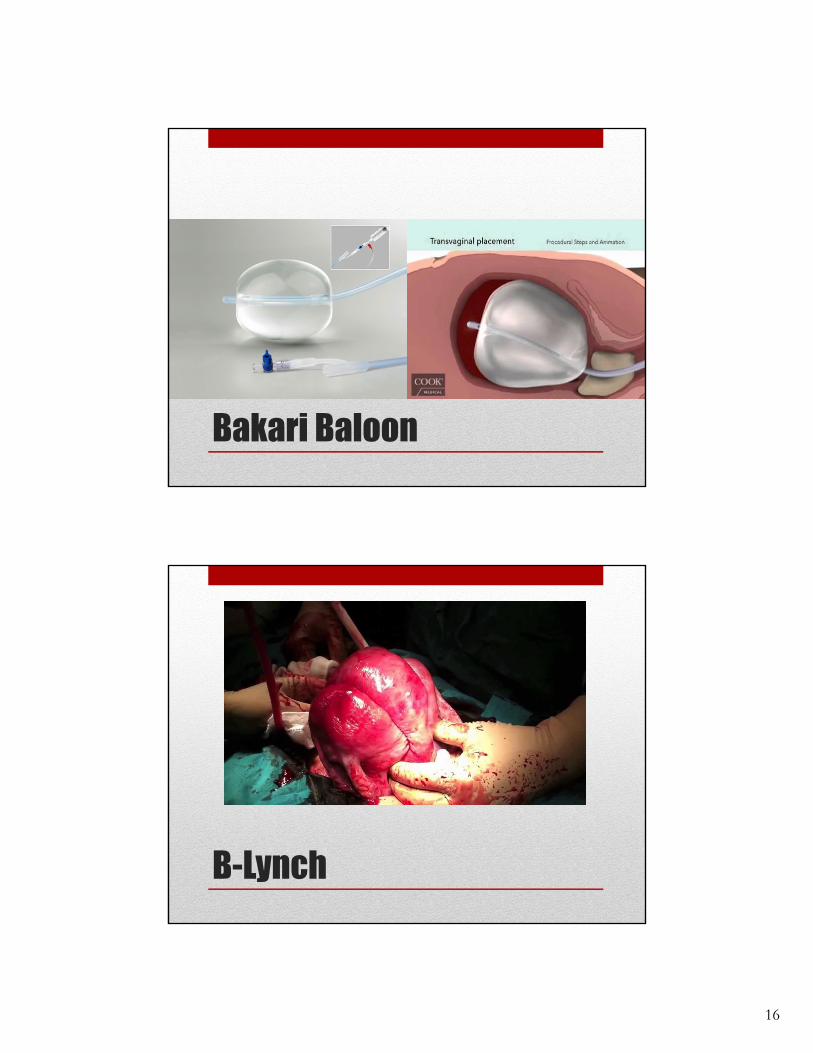
• Surgical management – D&C, Balloon Placement or hysterectomy
16
Bakari Baloon
B-Lynch
17
Lacerations
Location: cervix, vagina and perineum
Signs and Symptoms:
• Bright red/heavy bleeding with a firmly contracted uterus
• Steady stream or trickle of unclotted blood or comes in spurts
Laceration Causes Large fetal head for size of
pelvis
Difficult second stage
Operative vaginal delivery
Scars from infections, surgery or injury
Precipitous delivery
Perineal or vaginal varicesInterventions?
18
Causes of PPH- Retained Placental Fragments
• Manual removal of placenta
• Abnormal adherence of the placenta
• Over distension of uterus
• Prolonged labor with maternal exhaustion
• High parity
• Abruptio placenta
S & S of Retained Placental/Membrane Fragments
• Uterus remains large
• Heavy vaginal flow, usually beginning more than 24 hours after birth (around 7 days postpartum)
• Abnormal progression of lochia
INTERVENTIONS?

19
Hematomas
Prolonged pressure of the fetal head on vaginal mucosa
Operative vaginal delivery
Nicking of blood vessel during episiotomy or laceration repair
A collection of blood in the connective tissue due to vessel wall damage: can be vulvar, vaginal, or retroperitoneal
Signs and Symptoms of Hematoma
• Complaints of severe perineal or pelvic pain
• Unilateral, tense bulging mass at opening of vagina or labia
• Unilateral bluish or reddish discoloration of the skin of the perineum or buttocks
• Hemodynamic instability
Interventions???
20
Nursing Interventions for PPH
Fundal massage Record VS, O2 sat every 5 minutes Record cumulative blood loss, weigh pads Empty bladder: consider indwelling catheter IV access: at least 18 gauge: obtain labs with IV start Increase intravenous fluid Increase or start oxytocin Add other uterotonics as needed Determine and treat etiology – Confirm blood availability Order 2 units RBCs if ongoing bleeding; Consider ordering plasma
• I & O: hourly urine output• Maintain adequate ventilation: pulse oximeter and oxygen per mask as needed at 6-10
liters• Draw blood for type and crossmatch and hematocrit/hemoglobin• Give plasma expanders and packed RBC/blood products as ordered• Keep warm• At risk for Disseminated Intravascular Coagulation
GO TO OR
If uterotonics and bedside interventions do not control the bleeding Move to the OR
Consider D&C, intrauterine balloon, or other surgical intervention
Labs – CBC and coag studies repeat every 30 minutes with ongoing bleeding Order needs to be place in Epic
Repeat hemabate as often as every 15 minsDO NOT wait for labs to transfuse
Transfuse for clinical signs/symptoms
21
OB MTP
Obstetrical Massive Hemorrhage Protocol OB Hemorrhage Phone Tree
Algorithm ( On OB Anesthesiologist Role Card)
STAFF ROLE CARDS
Lab Requisition Form
Bleeding Emergency Flow Sheet
Baseline Lab Tube packets ( blue and lavender tubes for DIC panel)
OB MTP JOB AID
22
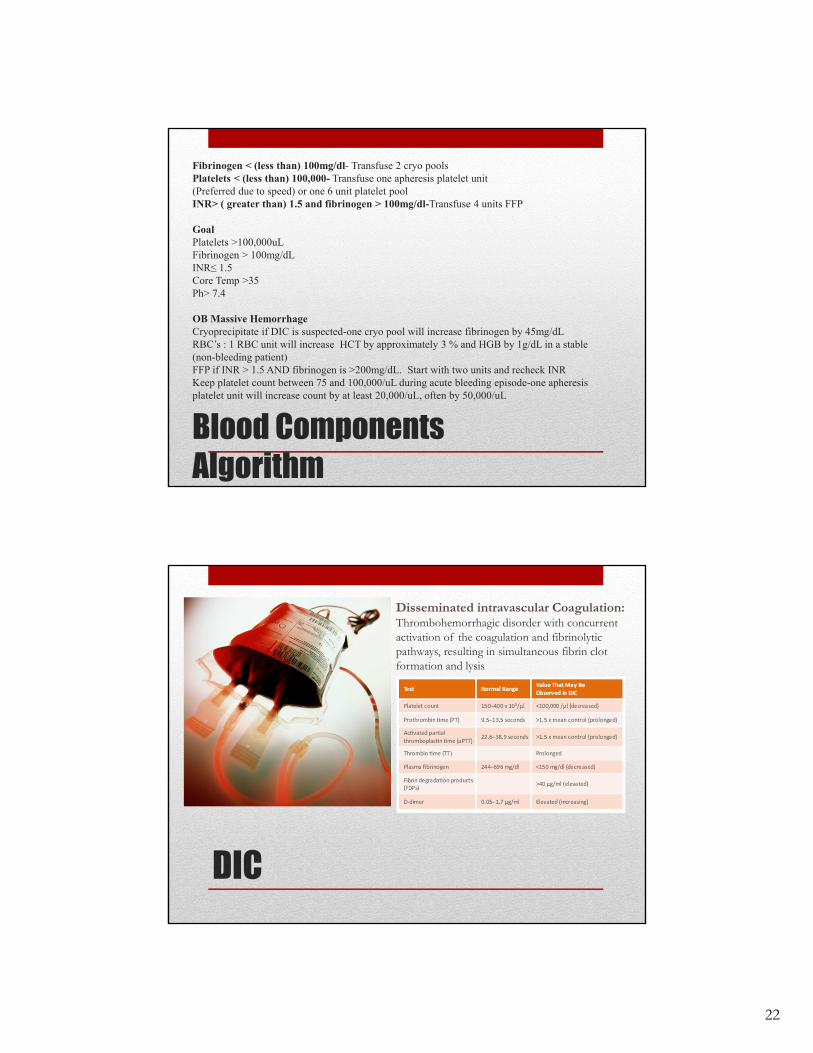
Blood Components Algorithm
Fibrinogen < (less than) 100mg/dl- Transfuse 2 cryo poolsPlatelets < (less than) 100,000- Transfuse one apheresis platelet unit (Preferred due to speed) or one 6 unit platelet poolINR> ( greater than) 1.5 and fibrinogen > 100mg/dl-Transfuse 4 units FFP
GoalPlatelets >100,000uLFibrinogen > 100mg/dLINR≤ 1.5Core Temp >35Ph> 7.4
OB Massive HemorrhageCryoprecipitate if DIC is suspected-one cryo pool will increase fibrinogen by 45mg/dLRBC’s : 1 RBC unit will increase HCT by approximately 3 % and HGB by 1g/dL in a stable (non-bleeding patient)FFP if INR > 1.5 AND fibrinogen is >200mg/dL. Start with two units and recheck INRKeep platelet count between 75 and 100,000/uL during acute bleeding episode-one apheresis platelet unit will increase count by at least 20,000/uL, often by 50,000/uL
DIC
Disseminated intravascular Coagulation:Thrombohemorrhagic disorder with concurrent activation of the coagulation and fibrinolytic pathways, resulting in simultaneous fibrin clot formation and lysis
23
Long-term complications of PPH
Blood Component transfusion reactions/complications Temporary of permanent kidney failure Anemia Fluid overload ( pulmonary edema, Dilutional
coagulopapthy) Sepsis Asherman’s Syndrome (intrauterine scaring/adhesions) Infertility Death
Don’t miss the boat! Look early , look often, work fast……
24
How can we help?The ability to give compassionate care will hold you up
• The unexpected will happen
Questions?